 Kim Z. Rokamp
Kim Z. Rokamp Niels H. Secher
Niels H. Secher Jonas Eiberg
Jonas Eiberg Lars Lønn3
Lars Lønn3 Henning B. Nielsen
Henning B. Nielsen- 1Departments of Anesthesia, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark
- 2Vascular Surgery, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark
- 3Interventional Radiology, Rigshospitalet, University of Copenhagen, Copenhagen, Denmark
This study addresses three questions for securing tissue oxygenation in brain (rScO2) and muscle (SmO2) for 100 patients (age 71 ± 6 years; mean ± SD) undergoing vascular surgery: (i) Does preoxygenation (inhaling 100% oxygen before anesthesia) increase tissue oxygenation, (ii) Does inhalation of 70% oxygen during surgery prevent a critical reduction in rScO2 (<50%), and (iii) is a decrease in rScO2 and/or SmO2 related to reduced blood pressure and/or cardiac output?Intravenous anesthesia was provided to all patients and the intraoperative inspired oxygen fraction was set to 0.70 while tissue oxygenation was determined by INVOS 5100C. Preoxygenation increased rScO2 (from 65 ± 8 to 72 ± 9%; P < 0.05) and SmO2 (from 75 ± 9 to 78 ± 9%; P < 0.05) and during surgery rScO2 and SmO2 were maintained at the baseline level in most patients. Following anesthesia and tracheal intubation an eventual change in rScO2 correlated to cardiac output and cardiac stroke volume (coefficient of contingence = 0.36; P = 0.0003) rather to a change in mean arterial pressure and for five patients rScO2 was reduced to below 50%. We conclude that (i) increased oxygen delivery enhances tissue oxygenation, (ii) oxygen supports tissue oxygenation but does not prevent a critical reduction in cerebral oxygenation sufficiently, and (iii) an eventual decrease in tissue oxygenation seems related to a reduction in cardiac output rather than to hypotension.
Introduction
Monitoring regional cerebral oxygenation (rScO2) by near infrared spectroscopy (NIRS) is used for both cardiac and non-cardiac surgery (Casati et al., 2005; Murkin and Arango, 2009) and suggested as an index for how well the circulation is managed (Murkin, 2011). A decrease in intraoperative rScO2 to less than 80% of the preoperative value, or to a level lower than 50% have been associated with postoperative complications such as cognitive dysfunction (Casati et al., 2005; Slater et al., 2009), stroke (Olsson and Thelin, 2006) and increased length of stay in hospital (Casati et al., 2005). Furthermore, patients with a preoperative rScO2 below 50% demonstrate increased probability for 1-year postoperative mortality (Heringlake et al., 2011). Thus, it appears to be an advantage to maintain rScO2 during surgery but with induction of general anesthesia subsequent reduction in blood pressure may affect regional blood flow and in turn tissue oxygenation (Petrozza, 1990). Yet, in patients undergoing minor surgery such as mastectomy, thyroidectomy or parathyroidectomy, a low blood pressure does not appear to affect rScO2 as determined by NIRS (Nissen et al., 2009). During surgery mean arterial pressure (MAP) is maintained often above 60 mmHg that is considered to represent the level that secures cerebral autoregulation (Paulson et al., 1990). On the other hand, during certain types of surgery deliberate reduction of MAP to below 60 mmHg may be initiated to limit hemorrhage (Martin and Galliano, 1965; Beaussier et al., 2000; Boonmak et al., 2013).
Patients undergoing vascular surgery are supplemented with O2 to prevent arterial desaturation (Dixon et al., 2005) and a high intraoperative inspired O2 fraction has the potential to improve postoperative outcome (Niinikoski, 1969; Hunt and Pai, 1972; Greif et al., 2000; Fries et al., 2005; Turtiainen et al., 2011). Raised inspired O2 fraction might affect regional blood flow to the brain (Nielsen et al., 1999; Smith et al., 2012) and skeletal muscle (Welch et al., 1977; Pedersen et al., 1999) and we aimed to assess influence of O2 supplementation on rScO2 and muscle oxygenation (SmO2) in a cohort of vascular surgical patients. It was addressed whether (i) preoxygenation (inhaling 100% oxygen before anesthesia) increases tissue oxygenation, (ii) inhalation of 70% oxygen during surgery prevents a critical reduction in ScO2 to below 50%, and (iii) a decrease in rScO2 and/or SmO2 is related to reduced blood pressure or cardiac output (CO).
Materials and Methods
Using a non-randomized single-center retrospective study-design we included vascular surgical patients enrolled in a cohort as approved by the Danish Data Protection Agency (2009-41-3617) and by the local ethical committee (H-4-2012-FSP). The evaluation included, arbitrarily, 100 patients (71 males; age 71 ± 6 years, height 171 ± 12 cm, weight 75 ± 16 kg; mean ± SD) in whom vascular surgery was performed between March 2009 and August 2011. Patients were planned for open (n = 23) or endovascular aortic repair (EVAR) (n = 56) of an abdominal aortic aneurysm, lower limb by-pass surgery (n = 6), an iliaco-femoral (n = 9) or axillo-femoral bypass (n = 1), open surgery for arterial mesenteric stenosis (n = 2), or EVAR of a thoracic aortic aneurysm (n = 3). Fifty-nine patients were in treatment for arterial hypertension and medication included an ACE antagonist (n = 36), adrenergic β-receptor blockade (n = 23), a calcium channel inhibitor (n = 18), and diuretics (n = 25). Ten patients were diabetics and for 14 patients suffered from chronic obstructive lung disease.
The patients were exposed to at least 6 h of fast and orally intake of clear fluids was stopped 2 h before surgery. Three-lead electrocardiography monitored heart rate (HR) and pulse oximetry assessed arterial hemoglobin O2 saturation (SpO2). A peripheral vein was used for administration of fluid and anesthetics. In accordance to local guidelines, a radial artery catheter (20 gauge; 1.1 mm) was, after local anesthesia, inserted in the arm with the highest non-invasively determined systolic blood pressure. The catheter was kept patent by isotonic saline (3 ml/h) through to a transducer (Edwards Life Sciences, Irving, CA, USA) positioned at the level of the heart. A two channel cerebral oximeter (INVOS 5100C, Somanetics, Troy, MI, USA) was used to detect rScO2 and SmO2. The reported values are taken to represent hemoglobin oxygen saturation in the tissue beneath the sensor as the ratio between deoxygenated hemoglobin and the sum of deoxygenated and oxygenated hemoglobin. Thus, as approved by the US Food and Drug Administration (510k-080769), the INVOS 5100C- determined rScO2 is considered a trend monitor of the hemoglobin O2 saturation for skin, scalp, and cortical tissue. With the NIRS-probe applied to the forehead it is assumed that capillaries within the frontal lobe contribute most to light absorbance (Madsen and Secher, 1999) but the skin, subcutaneous tissue and the scalp also contribute to change the INVOS-determined rScO2 (Davie and Grocott, 2012; Soerensen et al., 2012). The rScO2 was determined with a sensor attached to the forehead as least 2 cm above the eyebrows and that position is considered to limit an influence from the frontal sinus on rScO2 (Tubbs et al., 2002). Monitoring a change in NIRS-determined SmO2 indicates an early warning of an acute blood loss (Madsen et al., 1995) but the decision to apply a NIRS sensor to the middle part of the right biceps muscle was made by the anesthesiologist in charge and SmO2 is therefore reported for only 61 patients. The SmO2 value reflects both hemoglobin/oxyhemoglobin and myoglobin (Madsen and Secher, 1999).
Modelflow methodology (Nexfin, bmeye B.V, Amsterdam, The Netherlands) (Bogert and van Lieshout, 2005) was used to assess CO and cardiac stroke volume (SV) from the pressure curve and heart rate (HR) and MAP were monitored through the arterial line. Neuromuscular blockade was evaluated with “train of four” (Organon Dublin, Ireland). Lactated Ringer and Macrodex (Fresenius Kabi, Bad Homburg, Germany) were administered to support the central blood volume according to a goal-directed strategy (Bundgaard-Nielsen et al., 2007) as guided by SV and CO and by central venous O2 hemoglobin saturation in patients instrumented with a central venous catheter (via the internal jugular vein as guided by an ultrasound image). Administration of red blood cells was initiated in bleeding patients when hemoglobin was below 6 mmol/L.
The patients received no sedating drugs and in accordance to local guidelines inhalation of O2 was introduced using a bilateral nasal catheter. Thereafter a facial mask was applied for continued O2 breathing until anesthesia was induced with propofol (1 mg/kg) and fentanyl (1 μ g/kg). Cisatracurium (0.1–0.15 mg/kg) facilitated oral tracheal intubation and anesthesia was maintained with propofol (0.08 mg/kg/min) and remifentanil (0.3–0.4 μ g/kg/min). For ventilation a Dräger CATO (M32040, Lübeck, Germany) in volume-controlled mode was adjusted to an end-tidal CO2 tension of 4–4.5 kPa and a positive end-expiratory pressure of 5 cm H2O was used. When the patient was intubated, the inspiratory O2 fraction was set to 0.7 for maintenance of tissue oxygenation whereby the incidence of surgical site infections may decrease (Greif et al., 2000; Turtiainen et al., 2011). In 16 patients arterial blood was obtained for immediate blood gas analysis (ABL 725; Radiometer, Copenhagen, Denmark) to secure that changes in SpO2 reflected those in SaO2.
Values were recorded: (a) with the patient breathing room air, (b) after breathing O2 enriched air, (c) following induction of anesthesia, and finally (d) after tracheal intubation. Reported values during surgery represent the lowest noted rScO2 with the associated values for SmO2, HR, SV, CO, and MAP.
Statistics
For normally distributed data, One-Way analysis of variance (ANOVA) with repeated measures was used. In the case of a significant main effect, a Tukey-test based post-hoc evaluation was applied. Correlations among variables were evaluated by Spearman's test. A GLM matrix analysis was use to locate the factor that had the statistically strongest influence on rScO2. A P-value < 0.05 was considered statistical significant.
Results
Breathing O2 enriched air increased arterial O2 tension (from 10 ± 2 to 34 ± 12 kPa), SpO2 (95.3 ± 2.4 to 99.7 ± 1.1%), arterial hemoglobin O2 saturation (from 96.2 ± 2.0 to 99.7 ± 0.2%), and the arterial CO2 tension (from 5.1 ± 0.6 to 5.4 ± 0.7 kPa; all P < 0.05). In all patients O2 breathing increased rScO2 (Figure 1) and SmO2 while there was no effect on cardiovascular variables (Table 1). Statistically, SpO2 contributed most to rScO2 (P < 0.0001): changes in tissue oxygenation correlated to those in SpO2 (rScO2, r = 0.50; SmO2, r = 43. P < 0.05) as provoked by breathing O2 enriched air before anesthesia.
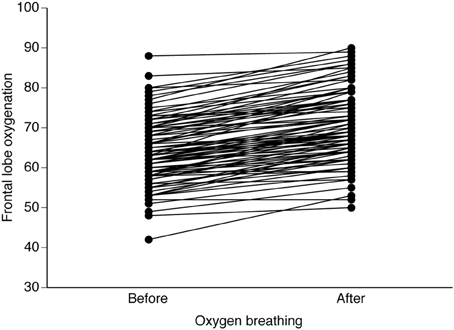
Figure 1. Effects of O2 breathing on NIRS determined frontal lobe oxygenation. Data are individual responses from vascular surgical patients exposed to preoperative facial mask breathing with 100% O2.
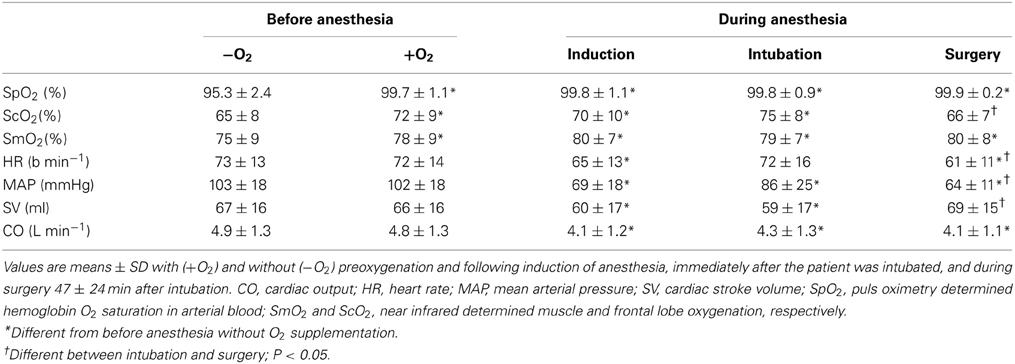
Table 1. Cardiovascular and blood gas variables for vascular surgical patients.
Following induction of anesthesia, MAP, HR, and CO lowered, while rScO2 and SmO2 remained elevated. For three patients rScO2 was reduced by more than 10% indicative of a potentially critical reduction in regional cerebral O2 supply. During surgery with an end-tidal CO2 pressure of 4.4 ± 0.4 kPa, SV, and CO were at the levels before anesthesia, SmO2 remained elevated and rScO2 was not significantly changed as compared to the preoperative level. In seven patients, however, rScO2 decreased by more than 10% and for five of these patients rScO2 was below 50%. In the patients demonstrating a significant drop in rScO2, CO was reduced by 1.6 ± 1.2 L/min but rScO2 appeared independent of MAP when CO was maintained or increased (Figure 2). Thus, there was no statistical significant relation between rScO2 and MAP but ScO2 was correlated to SV and CO (Table 2). Also rScO2 correlated to age, while SmO2 correlated only to SV and CO before but not after induction of anesthesia (P = 0.0025).
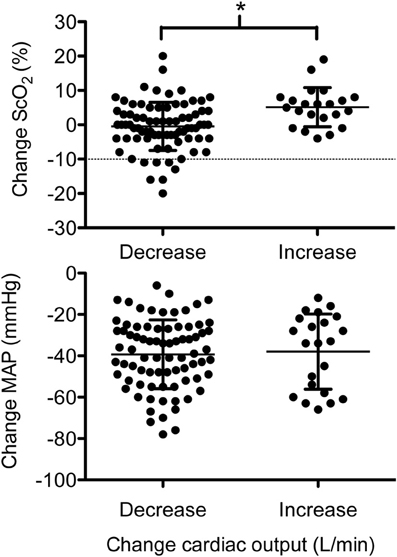
Figure 2. The surgical changes in frontal lobe oxygenation (ScO2) and mean arterial pressure (MAP) related to cardiac output (CO; decrease is CO below the preoperative level and increase is CO above the preoperative level). The dotted line straight line (upper panel) at −10% represents the change in ScO2 considered to be critical. *Different value; P < 0.05.
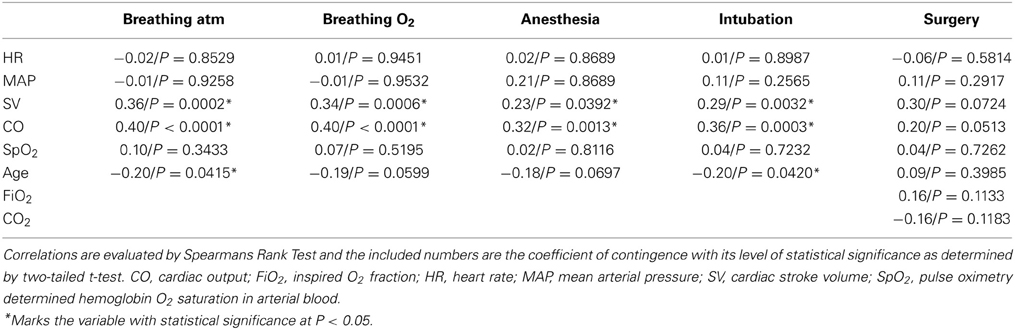
Table 2. Relationship between frontal lobe oxygenation and cardiovascular variables.
Discussion
This study aimed to answer three questions: (i) Does preoxygenation (inhaling 100% oxygen before anesthesia) increase tissue oxygenation? (ii) Does inhalation of 70% oxygen during surgery prevent a reported critical reduction in ScO2 to 50%? and (iii) When ScO2 and/or SmO2 decrease, is the decrease then related to reduced blood pressure and/or cardiac output? In vascular surgical patients, administration of elevated inspiratory O2 fraction increased oxygenation of both the cerebral frontal lobe (rScO2) and skeletal muscle (SmO2) (by 10 and 3%, respectively). Importantly, this increase in tissue oxygenation appeared protective for development of tissue hypoxemia following induction of anesthesia, although the incidence of critical reduction in rScO2 remained 5%. The third important observation was that during anesthesia a correlation between tissue oxygenation and a decrease in MAP was not observed indicating that for vascular surgical patients, as for patients scheduled for other types of surgery (Nissen et al., 2009), a transient drop in blood pressure to below what is often considered the lower limit of cerebral autoregulation does not affect rScO2. On the other hand, rScO2 correlated to a reduction in CO and SV.
It has not been evaluated whether it is profitable to control flow-related variables (SV, CO, or SvO2) in conjunction with an effort to maintain rScO2 during surgery. With fluid administration according to an “individualized goal-directed regime,” SV and hence CO is optimized to a level considered to represent normovolemia (Bundgaard-Nielsen et al., 2010). In the present study, the cardiovascular variables reported during surgery represent situations where rScO2 reached a minimum and the associated CO may reflect that fluid resuscitation was about to be initiated.
A correlation between rScO2 and CO supports a link to blood flow (Ide et al., 1999) and as cardiovascular capacity decline with advancing age (Proctor and Joyner, 1997), this view is further supported by a correlation between rScO2 and age. Seven patients suffered a critical reduction in rScO2 when CO dropped (Figure 2) and if O2 supplementation had not induced a 10% increase in rScO2, it is likely that rScO2 would have been reduced to a critical level in more patients. We did not find indication for that a low MAP affected rScO2 and in ASA class I patients, a 30% reduction in MAP with a minimum MAP of 50 mmHg, is considered acceptable (Yamada et al., 1988; Petrozza, 1990). In this evaluation 32 of 100 patients undergoing vascular surgery at one stage of the operation developed a MAP < 60 mmHg, apparently without affecting rScO2. Even when MAP was below 50 mmHg (n = 12), rScO2 was maintained.
Administration of an O2 enriched atmosphere was introduced to reduce the incidence of complications after colorectal surgery (Greif et al., 2000) and vascular surgery (Turtiainen et al., 2011). Yet, not all follow-up studies support that a high O2 fraction reduces surgical site infections (Pryor et al., 2004; Belda et al., 2005; Meyhoff et al., 2009; Bustamante et al., 2011) and O2 supplementation may provoke formation of O2 free radicals (García-de-la-Asunción et al., 2011). Furthermore, surgical site infection, atelectasis, pneumonia, and respiratory failure occur at similar frequencies in patients with an inspired O2 fraction of 0.80 compared to 30% O2 (Meyhoff et al., 2009). The tendency for O2 breathing to provoke pulmonary atelectasis (Hedenstierna, 2012) suggests the use of positive end expiratory pressure as applied in this evaluation. Also the relevance for using O2 supplementation is likely to vary among groups of patients. For vulnerable patients a reduction in tissue oxygenation may provoke ischemic stroke after surgery (Waggoner et al., 2001; Cheng-Ching et al., 2010). Importantly, vascular surgical patients often present with coronary artery or cerebrovascular disease (Hertzer et al., 1984) and hypotension may become critical for maintained tissue oxygenation. We suggest that O2 supplementation is important for perioperative preservation of tissue oxygenation.
This study is limited by several factors: a retrospective design often fails to extract dynamic cardiovascular variables in patients exposed to surgery. Furthermore, for the patients included in the present cohort, the recommendation to use NIRS to guide the circulation during surgery may not have been followed and a placebo-controlled randomized design is in need. A third reservation relates to the NIRS used for interpretation of changes in tissue oxygenation as the INVOS cerebral oximeter appears to be sensitive to changes in skin blood flow (Davie and Grocott, 2012).
From this retrospective evaluation of tissue oxygenation including 100 patients undergoing vascular surgical procedures, it is concluded that O2 supplementation increases the NIRS-determined oxygenation of the cerebral frontal lobe and skeletal muscles. Furthermore, the data suggest that an elevated inspired oxygen fraction is not efficient to prevent a critical reduction in cerebral oxygenation since a decrease seems to be related to a reduced cardiac output.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Peter Rasmussen, MSci PhD is thanked for statistical work and valuable discussions. Henning Bay Nielsen was funded by Rigshospitalet Research fund and the Danish Agency for Science Technology and Innovation (271-08-0857).
References
Beaussier, M., Paugam, C., Deriaz, H., Mestari, M., Chandon, M., Sautet, A., et al. (2000). Haemodynamic stability during moderate hypotensive anaesthesia for spinal surgery. A comparison between desflurane and isoflurane. Acta Anaesthesiol. Scand. 44, 1154–1159. doi: 10.1034/j.1399-6576.2000.440921.x
Belda, F. J., Aguilera, L., García de la Asunción, J., Alberti, J., Vicente, R., Ferrándiz, L., et al. (2005). Spanish Reduccion de la Tasa de Infeccion Quirurgica Group. Supplemental perioperative oxygen and the risk of surgical wound infection: a randomized controlled trial. JAMA 294, 2035–2042. doi: 10.1001/jama.294.16.2035
Bogert, L. W., and van Lieshout, J. J. (2005). Non-invasive pulsatile arterial pressure and stroke volume changes from the human finger. Exp. Physiol. 90, 437–446. doi: 10.1113/expphysiol.2005.030262
Boonmak, S., Boonmak, P., and Laopaiboon, M. (2013). Deliberate hypotension with propofol under anaesthesia for functional endoscopic sinus surgery (FESS). Cochrane Database Syst. Rev. 6, CD006623. doi: 10.1002/14651858.CD006623.pub2
Bundgaard-Nielsen, M., Holte, K., Secher, N. H., and Kehlet, H. (2007). Monitoring of peri-operative fluid administration by individualized goal-directed therapy. Acta Anaesthesiol. Scand. 51, 331–340. doi: 10.1111/j.1399-6576.2006.01221.x
Bundgaard-Nielsen, M., Jørgensen, C. C., Kehlet, H., and Secher, N. H. (2010). Normovolemia defined according to cardiac stroke volume in healthy supine humans. Clin. Physiol. Funct. Imaging 30, 318–322. doi: 10.1111/j.1475-097X.2010.00944.x
Bustamante, J., Tamayo, E., Alvarez, F. J., García-Cuenca, I., Flórez, S., Fierro, I., et al. (2011). Intraoperative PaO2 is not related to the development of surgical site infections after major cardiac surgery. J. Cardiothorac. Surg. 6, 4. doi: 10.1186/1749-8090-6-4
Casati, A., Fanelli, G., Pietropaoli, P., Proietti, R., Tufano, R., Danelli, G., et al. (2005). Continuous monitoring of cerebral oxygen saturation in elderly patients undergoing major abdominal surgery minimizes brain exposure to potential hypoxia. Anesth. Analg. 101, 740–747. doi: 10.1213/01.ane.0000166974.96219.cd
Cheng-Ching, E., Fong, J., Ontaneda, D., Hussain, M. S., Katzan, I., and Gupta, R. (2010). Intracranial atherosclerosis as a risk factor for ischemic stroke during open heart surgery. J. Stroke Cerebrovasc. Dis. 19, 257–260. doi: 10.1016/j.jstrokecerebrovasdis.2009.04.011
Davie, S. N., and Grocott, H. P. (2012). Impact of extracranial contamination on regional cerebral oxygen saturation: a comparison of three cerebral oximetry technologies. Anesthesiology 116, 834–840. doi: 10.1097/ALN.0b013e31824c00d7
Dixon, B. J., Dixon, J. B., Carden, J. R., Burn, A. J., Schachter, L. M., Playfair, J. M., et al. (2005). Preoxygenation is more effective in the 25 degrees head-up position than in the supine position in severely obese patients: a randomized controlled study. Anesthesiology 102, 1110–1115. doi: 10.1097/00000542-200506000-00009
Fries, R. B., Wallace, W. A., Roy, S., Kuppusamy, P., Bergdall, V., Gordillo, G. M., et al. (2005). Dermal excisional wound healing in pigs following treatment with topically applied pure oxygen. Mutat. Res. 579, 172–181. doi: 10.1016/j.mrfmmm.2005.02.023
García-de-la-Asunción, J., Barber, G., Rus, D., Perez-Griera, J., Belda, F. J., Martí, F., et al. (2011). Hyperoxia during colon surgery is associated with a reduction of xanthine oxidase activity and oxidative stress in colonic mucosa. Redox Rep. 16, 121–128. doi: 10.1179/174329211X13049558293632
Greif, R., Akça, O., Horn, E. P., Kurz, A., Sessler, D. I., and Outcomes Research Group. (2000). Supplemental perioperative oxygen to reduce the incidence of surgical-wound infection. N. Engl. J. Med. 342, 161–167. doi: 10.1056/NEJM200001203420303
Hedenstierna, G. (2012). Oxygen and anesthesia: what lung do we deliver to the post-operative ward? Acta Anaesthesiol. Scand. 56, 675–685. doi: 10.1111/j.1399-6576.2012.02689.x
Heringlake, M., Garbers, C., Käbler, J. H., Anderson, I., Heinze, H., Schön, J., et al. (2011). Preoperative cerebral oxygen saturation and clinical outcomes in cardiac surgery. Anesthesiology 114, 58–69. doi: 10.1097/ALN.0b013e3181fef34e
Hertzer, N. R., Beven, E. G., Young, J. R., O'Hara, P. J., Ruschhaupt, W. F. 3rd. Graor, R. A., et al. (1984). Coronary artery disease in peripheral vascular patients. A classification of 1000 coronary angiograms and results of surgical management. Ann. Surg. 199, 223–233. doi: 10.1097/00000658-198402000-00016
Hunt, T. K., and Pai, M. P. (1972). The effect of varying ambient oxygen tension on wound metabolism and collagen synthesis. Surg. Gynecol. Obstet. 135, 561–567.
Ide, K., Gulløv, A. L., Pott, F., Van Lieshout, J. J., Koefoed, B. G., Petersen, P., et al. (1999). Middle cerebral artery blood velocity during exercise in patients with atrial fibrillation. Clin. Physiol. 19, 284–289. doi: 10.1046/j.1365-2281.1999.00178.x
Madsen, P., Lyck, F., Pedersen, M., Olesen, H. L., Nielsen, H. B., and Secher, N. H. (1995). Brain and muscle oxygen saturation during head-up-tilt-induced central hypovolaemia in humans. Clin. Physiol. 15, 523–533. doi: 10.1111/j.1475-097X.1995.tb00541.x
Madsen, P. L., and Secher, N. H. (1999). Near-infrared oximetry of the brain. Prog. Neurobiol. 58, 541–560. doi: 10.1016/S0301-0082(98)00093-8
Martin, D. S., and Galliano, R. (1965). Bloodless liver resection under hypotensive hypothermia. Am. J. Surg. 109, 625–628.
Meyhoff, C. S., Wetterslev, J., Jorgensen, L. N., Henneberg, S. W., Høgdall, C., Lundvall, L., et al. (2009). PROXI Trial Group. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. JAMA 302, 1543–1550. doi: 10.1001/jama.2009.1452
Murkin, J. M. (2011). Cerebral oximetry: monitoring the brain as the index organ. Anesthesiology 114, 12–13. doi: 10.1097/ALN.0b013e3181fef5d2
Murkin, J. M., and Arango, M. (2009). Near-infrared spectroscopy as an index of brain and tissue oxygenation. Br. J. Anaesth. 103, i3–i13. doi: 10.1093/bja/aep299
Nielsen, H. B., Boushel, R., Madsen, P., and Secher, N. H. (1999). Cerebral desaturation during exercise reversed by O2 supplementation. Am. J. Physiol. 277, H1045–H1052.
Niinikoski, J. (1969). Effect of oxygen supply on wound healing and formation of experimental granulation tissue. Acta Physiol. Scand. (Suppl.) 334, 1–72.
Nissen, P., van Lieshout, J. J., Nielsen, H. B., and Secher, N. H. (2009). Frontal lobe oxygenation is maintained during hypotension following propofol-fentanyl anesthesia. AANA J. 77, 271–276.
Olsson, C., and Thelin, S. (2006). Regional cerebral saturation monitoring with near-infrared spectroscopy during selective antegrade cerebral perfusion: diagnostic performance and relationship to postoperative stroke. J. Thorac. Cardiovasc. Surg. 131, 371–379. doi: 10.1016/j.jtcvs.2005.08.068
Paulson, O. B., Strandgaard, S., and Edvinsson, L. (1990). Cerebral autoregulation. Cerebrovasc. Brain Metab. Rev. 2, 161–192.
Pedersen, P. K., Kiens, B., and Saltin, B. (1999). Hyperoxia does not increase peak muscle oxygen uptake in small muscle group exercise. Acta Physiol. Scand. 166, 309–318. doi: 10.1046/j.1365-201x.1999.00575.x
Petrozza, P. H. (1990). Induced hypotension. Int. Anesthesiol. Clin. 28, 223–229. doi: 10.1097/00004311-199002840-00008
Proctor, D. N., and Joyner, M. J. (1997). Skeletal muscle mass and the reduction of VO2max in trained older subjects. J. Appl. Physiol. 82, 1411–1415.
Pryor, K. O., Fahey, T. J. 3rd. Lien, C. A., and Goldstein, P. A. (2004). Surgical site infection and the routine use of perioperative hyperoxia in a general surgical population: a randomized controlled trial. JAMA 291, 79–87. doi: 10.1001/jama.291.1.79
Slater, J. P., Guarino, T., Stack, J., Vinod, K., Bustami, R. T., Brown, J. M. 3rd., et al. (2009). Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann. Thorac. Surg. 87, 36–44. doi: 10.1016/j.athoracsur.2008.08.070
Smith, K. J., Wong, L. E., Eves, N. D., Koelwyn, G. J., Smirl, J. D., Willie, C. K., et al. (2012). Regional cerebral blood flow distribution during exercise: influence of oxygen. Respir. Physiol. Neurobiol. 184, 97–105. doi: 10.1016/j.resp.2012.07.014
Soerensen, H., Secher, N. H., Siebenmann, C., Nielsen, H. B., Kohl-Bareis, M., Lundby, C., et al. (2012). Cutaneous vasoconstriction affects spectroscopy-determined cerebral oxygen saturation during administration of norepinephrine. Anesthesiology 117, 263–270. doi: 10.1097/ALN.0b013e3182605afe
Tubbs, R. S., Elton, S., Salter, G., Blount, J. P., Grabb, P. A., and Oakes, W. J. (2002). Superficial surgical landmarks for the frontal sinus. J. Neurosurg. 96, 320–322. doi: 10.3171/jns.2002.96.2.0320
Turtiainen, J., Saimanen, E. I., Partio, T. J., Mäkinen, K. T., Reinikainen, M. T., Virkkunen, J. J., et al. (2011). Supplemental postoperative oxygen in the prevention of surgical wound infection after lower limb vascular surgery: a randomized controlled trial. World J. Surg. 35, 1387–1395. doi: 10.1007/s00268-011-1090-y
Waggoner, J. R. 3rd. Wass, C. T., Polis, T. Z., Faust, R. J., Schroeder, D. R., Offord, K. P., et al. (2001). The effect of changing transfusion practice on rates of perioperative stroke and myocardial infarction in patients undergoing carotid endarterectomy: a retrospective analysis of 1114 Mayo Clinic patients. Mayo Perioperative Outcomes Group. Mayo Clin. Proc. 76, 376–383.
Welch, H. G., Bonde-Petersen, F., Graham, T., Klausen, K., and Secher, N. H. (1977). Effects of hyperoxia on leg blood flow and metabolism during exercise. J. Appl. Physiol. 42, 385–390.
Keywords: blood pressure, cardiac output, cerebral oxygenation, muscle oxygenation
Citation: Rokamp KZ, Secher NH, Eiberg J, Lønn L and Nielsen HB (2014) O2 supplementation to secure the near-infrared spectroscopy determined brain and muscle oxygenation in vascular surgical patients: a presentation of 100 cases. Front. Physiol. 5:66. doi: 10.3389/fphys.2014.00066
Received: 13 November 2013; Accepted: 03 February 2014;
Published online: 25 February 2014.
Edited by:
Patrice Brassard, Laval University, CanadaReviewed by:
Kurt J. Smith, Centre for Heart Lung and Vascular Health, CanadaMigue Arango, LHSC University Hospital, Canada
Copyright © 2014 Rokamp, Secher, Eiberg, Lønn and Nielsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Henning B. Nielsen, Departments of Anesthesia, Rigshospitalet, University of Copenhagen, Blegdamsvej 9, 2100 København Ø, Denmark e-mail: henning.bay@rh.regionh.dk