
- 1 Sleep Laboratory, Meyer Children’s Hospital, Rambam Medical Center and Technion – Israel Institute of Technology, Haifa, Israel
- 2 Pediatric Cardiology Department, Meyer Children’s Hospital, Rambam Medical Center and Technion – Israel Institute of Technology, Haifa, Israel
- 3 Sleep Division, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA, USA
Introduction: Up to 50% of adults with congestive heart failure (CHF) and left ventricular dysfunction demonstrate Cheyne–Stokes respiration (CSR), although the mechanisms remain controversial. Because CSR has been minimally studied in children, we sought to assess the prevalence of CSR in children with low and high output cardiac failure. We hypothesized that the existence of CSR only in children with low output CHF would support the importance of circulatory delay as a CSR mechanism. Methods: Thirty patients participated: 10 children with CHF, 10 matched children with no heart disease, and 10 adults with CHF. All participants underwent an in-laboratory polysomnographic sleep study. Results: CHF children’s average age (±SEM) was 3.6 ± 2.1 years vs. 3.7 ± 2 years in the age-matched control group. The average ejection fraction of three children with low output CHF was 22 ± 6.8%. The remaining seven had normal-high cardiac output. Compared to control children, CHF children were tachypneic and tachycardic during stable sleep (55.1 ± 6.7 vs. 26.9 ± 3 breath/min and 127.6 ± 8.7 vs. 97.6 ± 6.9 beats/min, respectively, p < 0.05 for both). They had shorter total sleep time (195 ± 49 vs. 373 ± 16 min, p < 0.05) with a low sleep efficiency of 65.6 ± 6%. None of the children had a pattern of CSR at any time during the studies while the adults with CHF had 40% prevalence of CSR. Conclusions: The complete absence of CSR in our sample of children with CHF compared to the 40% prevalence in the adults with CHF we studied, suggests that CSR may be an age-dependent phenomenon. Thus, we speculate that regardless of the exact mechanism which drives CSR, age is an over-riding factor.
Introduction
Cheyne–Stokes respiration (CSR) is a form of periodic breathing characterized by recurrent episodes of central apnea, alternating with periods of hyperpnea. Tidal volumes during these events have a typical crescendo-decrescendo appearance. CSR is associated with congestive heart failure (CHF) and has been reported to develop in approximately 40–50% of adult patients with left ventricular ejection fraction (LVEF) of less than 40%. Most of the existing data from adult patients suggest that the occurrence of CSR is a marker of increasing CHF severity. Unlike obstructive sleep apnea (OSA) which is considered to be a cause of CHF, CSR is more likely to be a consequence of CHF (Javaheri et al., 1998; Naughton and Bradley, 1998; Sin et al., 1999; Bradley and Floras, 2003). The precise pathophysiological mechanisms leading to the development of CSR are somewhat controversial. Proposed mechanisms include increased central nervous system sensitivity to changes in arterial PCO2 and PO2, a decrease in total body stores of PCO2 and PO2, with falls in the partial pressure of arterial PCO2 below the apnea threshold in response to changes in ventilation, catecholamine hypersecretion, dynamic upper airway instability, pulmonary congestion, hypoxemic events, hyper-arousability/arousals from sleep and an increased circulatory time in patients with CHF (Quaranta et al., 1997; Javaheri et al., 1998; Naughton and Bradley, 1998; Sin et al., 1999; Bradley and Floras, 2003; Ryan and Bradley, 2005). Regardless of the mechanism, aging is known to be a major risk factor for CSR occurrence among adults with CHF (Bixler et al., 1998; Javaheri et al., 1998; Sin et al., 1999).
Cheyne–Stokes respiration is associated with sleep disruption and its most immediate consequences include sleep fragmentation and impairment of neurocognitive function (Cheshire et al., 1992; Hanly and Zuber-Khokhar, 1995). In addition, there are increasing data that CSR may alter the natural history of the heart failure (Lanfranchi et al., 1999; Sin et al., 2000). Intermittent hypoxemia due to apnea, and recurrent arousal from sleep associated with hyperpnea, are related to the increased sympathetic nervous system activity which in turn is associated with increased mortality in patients with CHF (Cohn et al., 1984; Somers et al., 1989, 1993). Furthermore, it has been shown that the existence of CSR in patients with CHF has prognostic value, and specific treatment directed for the respiratory abnormality (i.e., continuous positive airway pressure – CPAP) improves cardiac function, quality of life, and perhaps prognosis (Javaheri, 2000; Bradley et al., 2005).
In contrast to systolic heart failure in adults, in children the common causes of CHF are congenital heart defects such as large ventricular septal defects. In other cases such as myocarditis and cardiomyopathies, children also demonstrate low output CHF. Interestingly, despite a relatively high prevalence of CHF in children with heart disease (27%) (Sommers et al., 2005), aside form one case report (Hoch and Barth, 2001), CSR breathing pattern has not been reported in pediatric patients with CHF to our knowledge. It is not clear whether CSR in children with CHF has not been observed because its presence has not been assessed adequately or because specific age-related mechanisms in children protect against this respiratory pattern. Thus, in the current study we sought to assess the prevalence of CSR in children with low and high output cardiac failure to provide insights into the relative importance of the above pathophysiological mechanisms. We hypothesized that the existence of CSR only in children with low output CHF would support the importance of circulatory delay as a CSR mechanism.
Materials and Methods
Subjects
We conducted a prospective observational case–control study in which we studied a population consisting of thirty patients recruited as follows: 10 consecutive children with CHF were recruited via the pediatric cardiology department clinics, Meyer Children’s Hospital (Haifa, Israel). Ten additional children without CHF were recruited as controls (matched by age and gender) from the sleep clinic. They were referred to the sleep clinic due to snoring and potential apnea, but had no known heart abnormality based on a thorough history and physical examination. Ten adults with an established diagnosis of CHF referred to the Sleep Laboratory due to suspected sleep disordered breathing were recruited as well, to serve as controls with cardiac disease. All of the children with CHF underwent a careful cardiac evaluation with a diagnosis of CHF established by a cardiologist as defined by characteristic symptoms and testing (resting tachypnea and tachycardia, pulmonary congestion etc.). Their workup included the following: medical history, physical examination, ECG, chest radiography, and two-dimensional echocardiography. Following their cardiac evaluation an in-lab polysomnographic sleep study was performed. Their medical treatment had been optimized and all their medications were continued throughout the study. There were no known electrolyte abnormalities in these children and none of them had undergone a prior corrective cardiac surgery. All participants underwent an in-lab polysomnographic sleep study.
Sleep Recordings
The patients were studied in the Technion Institute of Technology Sleep Disorders Center (Haifa, Israel) shortly following arrival to the hospital. All children were accompanied by at least one parent throughout the sleep study. During polysomnography (PSG), the following variables were continuously measured and recorded: two channels of electroencephalogram (C3-A2 and O2-A1), electrooculogram, chin and anterior tibialis electromyograms, chest and abdominal wall movement (piezoelectric electrodes), electrocardiogram, and air flow (thermistor). Arterial oxygen saturation ( ) was assessed by pulse oximetry, and end-tidal CO2 (ETCO2) levels by capnograph. All measures were digitized using a commercially available polysomnography system (EEG 4214; Nihon Kohden, Kogyo Co, Tokyo, Japan, or Embla system, Flaga hf, Iceland).
) was assessed by pulse oximetry, and end-tidal CO2 (ETCO2) levels by capnograph. All measures were digitized using a commercially available polysomnography system (EEG 4214; Nihon Kohden, Kogyo Co, Tokyo, Japan, or Embla system, Flaga hf, Iceland).
Sleep was staged according to standard criteria (American Academy of Sleep Medicine Task Force, 1999). Sleep efficiency was calculated as the percentage total sleep time vs. total recording time (time in bed). Arousals from sleep were defined as any electroencephalographic frequency change for 3 s in non-rapid eye movement (NREM) sleep and any such change associated with body movement or increase in electromyogram during rapid eye movement (REM) sleep.
Respiratory events were scored according to the common practice for measurement in children with some modifications (American Thoracic Society Task Force, 1996). Apneas were defined as the complete cessation of breathing for at least two breath cycles, and hypopneas, as any notable decrement in ventilation for at least two breath cycles, if the hypopnea was associated with a decrease of at least 3% in  , an increase in ETCO2 or arousal from sleep. In particular, obstructive apnea was defined as cessation of airflow at the nose and the mouth, as measured by the thermistor and the capnograph, with continued respiratory effort (movements of the rib cage and the abdomen) for at least two breaths. In the adults group the respiratory events were scored according to the common practice in this age group, i.e., “Chicago Criteria” (American Academy of Sleep Medicine Task Force, 1999).Central apnea was defined as the absence of airflow at both the nose and mouth as measured by the thermistor and the capnograph, associated with absence of movement of the chest and abdominal walls. Mixed apnea was defined as an apnea with both central and obstructive components in any order, with the central component lasting ≥3 s. The recurrent central events alternating with a crescendo–decrescendo pattern of tidal volume were defined as CSR, at epoch lengths of 0.5, 1, 2, and 5 min. Hypopnea was further characterized as obstructive if the reduction in airflow was associated with paradoxical chest and abdominal movement, or central if associated with an in-phase reduction in the amplitude of the chest and abdominal signals (Moser et al., 1994). The subjects were also monitored and recorded on audio/videotape using an infrared video camera. Each participant was continuously observed by a technician during the overnight recording.
, an increase in ETCO2 or arousal from sleep. In particular, obstructive apnea was defined as cessation of airflow at the nose and the mouth, as measured by the thermistor and the capnograph, with continued respiratory effort (movements of the rib cage and the abdomen) for at least two breaths. In the adults group the respiratory events were scored according to the common practice in this age group, i.e., “Chicago Criteria” (American Academy of Sleep Medicine Task Force, 1999).Central apnea was defined as the absence of airflow at both the nose and mouth as measured by the thermistor and the capnograph, associated with absence of movement of the chest and abdominal walls. Mixed apnea was defined as an apnea with both central and obstructive components in any order, with the central component lasting ≥3 s. The recurrent central events alternating with a crescendo–decrescendo pattern of tidal volume were defined as CSR, at epoch lengths of 0.5, 1, 2, and 5 min. Hypopnea was further characterized as obstructive if the reduction in airflow was associated with paradoxical chest and abdominal movement, or central if associated with an in-phase reduction in the amplitude of the chest and abdominal signals (Moser et al., 1994). The subjects were also monitored and recorded on audio/videotape using an infrared video camera. Each participant was continuously observed by a technician during the overnight recording.
Data Analysis
All records were scored by both a blinded sleep technologist and the investigators (independently) to search for CSR, in various time-scale windows. All values are shown as mean ± SEM. The three groups were compared using one way ANOVA. Children with and without CHF were compared by two tailed t-test. p < 0.05 was considered of statistical significance.
Results
Subjects Characteristics
A total of 20 children and 10 adults were studied. The children with and without CHF were matched in terms of age (3.6 ± 2.1 years vs. 3.7 ± 2 years) and gender (five males/five females vs. four males/six females). Seven of the CHF children were infants at an average age of 0.22 ± 0.04 years, with severe high output cardiac failure as a result of congenital septal defects (large VSD ± ASD) in some, along with valvular insufficiency and moderate to severe pulmonary hypertension. Six/seven children underwent surgical intervention for correction of their septal defect. Three were children at an average age of 11.5 ± 4.4 years, with severe low output cardiac failure as a result of dilated cardiomyopathy with mean left ventricle ejection fraction of 22 ± 6.8% (similar to the 26.5 ± 3.1% in the adult CHF group). Two of them underwent cardiac transplantation at a later stage. The etiology of the heart failure in the adult group was ischemic heart disease in 70%, valvular disease in 20% and other causes in 10%. All of the patients in the adult group had had a heart failure diagnosis for more than a year. The individual clinical characteristics of the CHF patients are presented in Table 1.
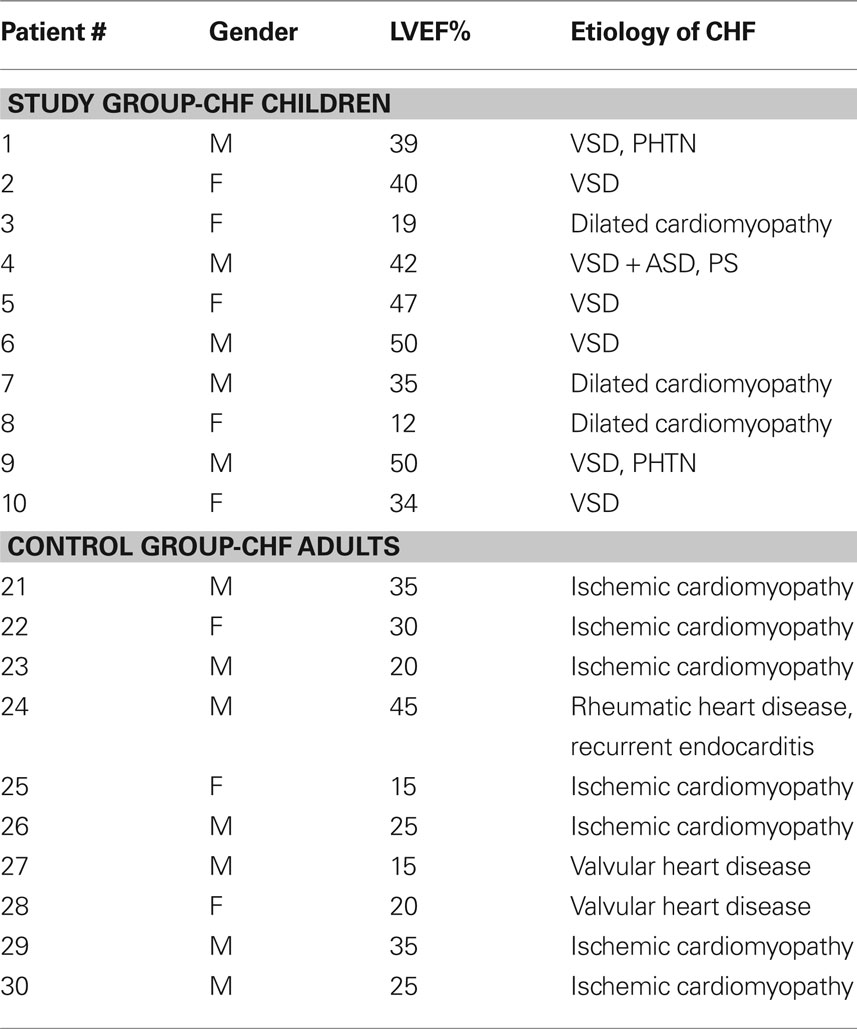
Table 1. Individual cardiac characteristics of participants with CHF.
Medical therapy for heart failure in both CHF groups, the children and adults, consisted of angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, diuretics, digoxin, and β-blockers (Table 2). When comparing children with and without CHF, subjects with CHF were tachypneic and tachycardic during stable sleep with an average respiratory rate of 55.1 ± 6.7 breath/min compared to 26.9 ± 3, and heart rate of 127.6 ± 8.7 BPM compared to 97.6 ± 6.9 (p < 0.05 for both). Sleep efficiency was low in both groups, but total sleep time was significantly lower in children with CHF than non-CHF children. None had documented arrhythmias. In the infant study group eight had normal RDI (<2) and two had and RDI of 7 and 9 (data not shown). Seven of the children in the control non-CHF group had sleep apnea, with an average RDI of 12.2 ± 3.2 events/hour and a minimal oxygen saturation ranges between 82 to 92%. All infants with CHF were irritable on admission with reduced appetite and difficulties with feedings (four/seven of the infants were fed through a nasogastric tube). All children were in the lowest 10 percentile for weight (16.4 ± 7.6 kg vs. 24.7 ± 8.8 kg in the age-matched group). Three children had an enlarged liver on their physical examination and two had pulmonary congestion and evidence of pleural effusion on chest x-ray. Data are summarized in Table 3.
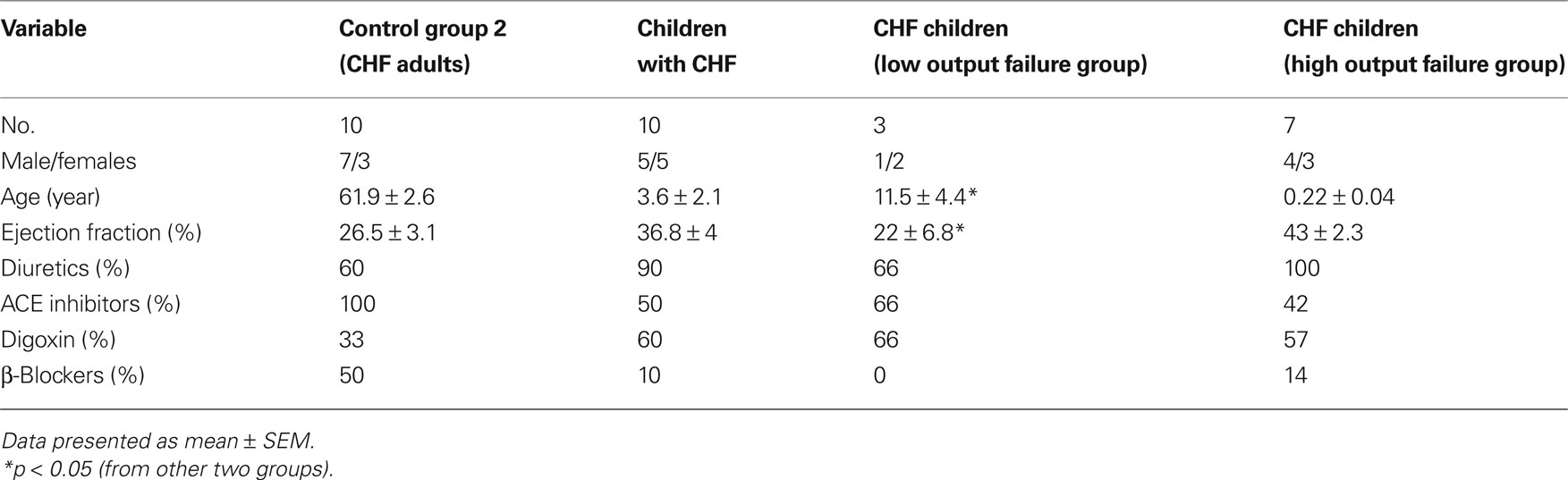
Table 2. Characteristic of the CHF patients according to their group.
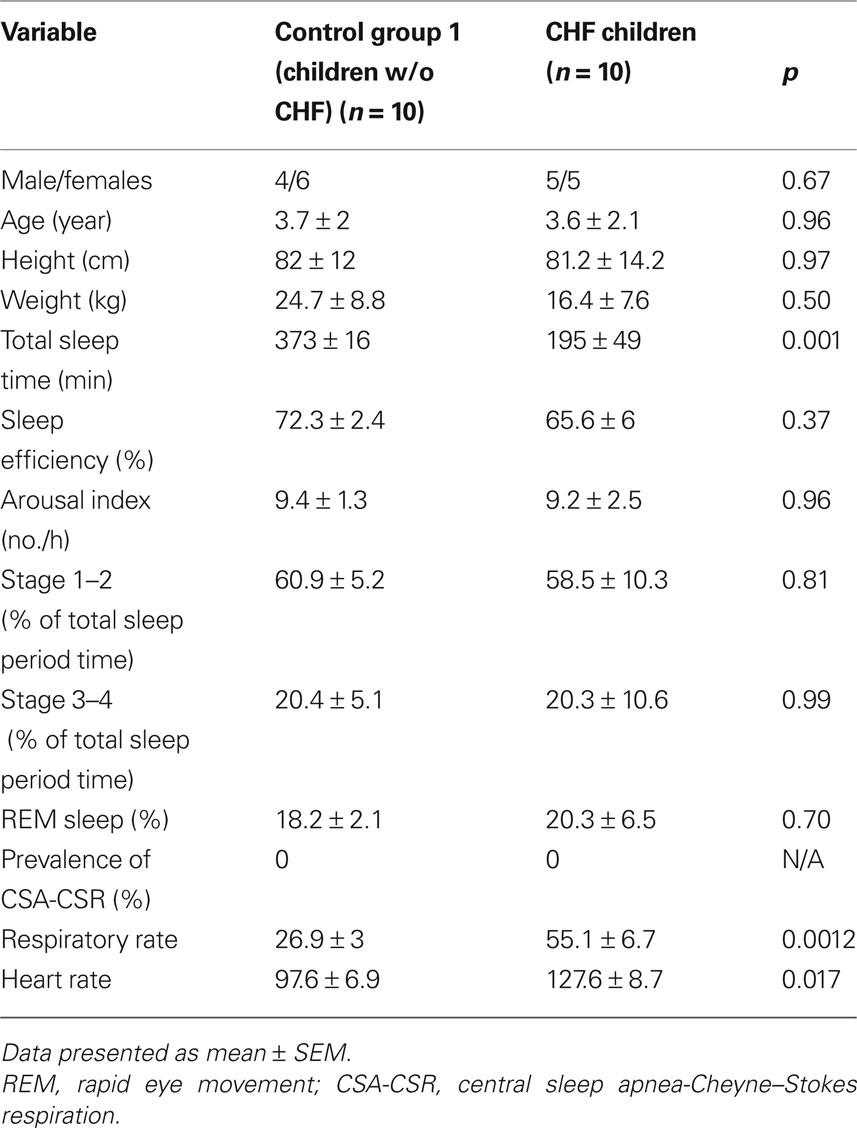
Table 3. Baseline characteristics and polysomnographic characteristics of the pediatric patients according to their group.
Table 4 demonstrates the polysomnographic characteristics of the patients, given by subgroup categorization. Sleep was fragmented in most participants, with low sleep efficiency and relatively high arousal index, which tended to be higher in the low output than high output cardiac failure, but was in both pediatric groups significantly lower than in adults with CHF. Of note, the average respiratory disturbance index of the adults with CHF was 32.8 ± 5.2/hour, with those experiencing CSR having higher RDIs than the non-CSR individuals. Among both subgroups of children with CHF, despite occasional apneas and oxygen desaturations to as low as 78% in the high output group and 92% in the low output group, as well as arousals from sleep and post arousal hyperpnea, none had a typical CSR pattern. Although total sleep time was relatively low (almost 3 h in the high output group and almost 5 h in the low output group), all patients had at least two cycles of REM–NREM sleep (active-quiet sleep in the high output group). Oxygen saturation was lowest during REM (active) sleep in all cases.
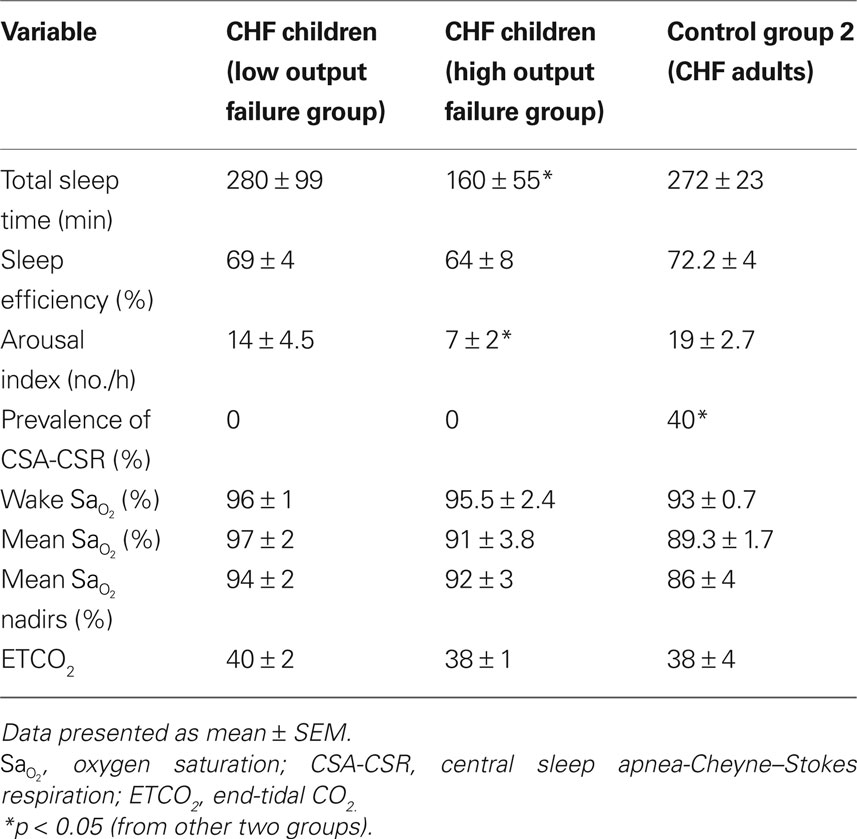
Table 4. Baseline characteristics and polysomnographic characteristics of the CHF patients according to their group.
Discussion
The major novel finding of this study is the absence of CSR among 10 children with severe heart failure. Given the high prevalence of CSR in adults with CHF (40% in our group, up to 50% in others’), we believe that the complete absence of this respiratory pattern, together with the scarcity of literature regarding CSR in children, indicates a substantial age-related effect on the development of CSR. The other notable finding of this study is the extremely poor sleep quality and reduced total sleep time of children with CHF, which was a phenomenon previously well known to practicing clinicians but lacking in objective data.
The fragmented sleep we observed in children with CHF likely results from the continuous respiratory and cardiac distress as indicated by the tachypnea and tachycardia in the study group, along with the elevated respiratory workload and pulmonary congestion. Other known factors causing airway obstruction followed by sleep fragmentation were excluded in our group of patients as RDI score was normal in the vast majority of the children. While a great deal has been written about the failure to thrive (FTT) and developmental delay of these children secondary to their respiratory distress and subsequently difficulties with feeding and low caloric intake along with high energy demand, little attention has been put on their sleep quality. From the literature regarding children with sleep apnea and other sleep disturbances (independent of cardiac pathology) we know that poor sleep quality may be associated with growth retardation, behavioral problems, and low scholastic achievements (Golan et al., 2004). In the current study, children with CHF demonstrated significantly reduced total sleep time compared to matched control children, even though many of them had sleep apnea. We believe that the very poor nocturnal sleep of children with CHF may represent a therapeutic target for future research with the potential to improve growth and developmental delay in afflicted individuals.
There are increasing data showing that in adults CSR may alter the natural history of CHF (Lanfranchi et al., 1999; Sin et al., 2000) and furthermore, recent evidence suggests that effective treatment of CSR in adults improves various aspects of cardiovascular characteristics in patients with CHF and CSR; therefore, an increased awareness of these breathing disorders may alter the therapeutic approach (Javaheri, 2000; Sin et al., 2000; Bradley et al., 2005).
When studying patients with high and low output heart failure we aimed to better learn about the impact of circulation delay, because the association between increased circulation time and CSR is not clear at this time. Stability or instability in ventilatory control is generally described using loop gain, an engineering term to describe the instability in a negative feedback control system (Younes et al., 2001). A high loop gain refers to an unstable control system (i.e., prone to periodic breathing) whereas a low loop gain describes a stable control system (i.e., not susceptible to periodic breathing) (Wellman et al., 2007). Loop gain can be considered the product of multiple different gains including central drive (i.e., chemoresponsiveness or controller gain), the efficiency of CO2 excretion (i.e., plant gain), and the delays caused by the circulation and hemoglobin binding affinity (i.e., mixing gain) (Malhotra and Jordan, 2006; Eckert et al., 2007). In humans, the relative impact of the various gains is difficult to test experimentally (Stanchina et al., 2007); therefore we thought the study of children would provide a unique opportunity to understand the importance of the various factors in control of breathing.
Initial reports observed prolonged circulation time in patients with CHF and CSR, hypothesizing that a delay in the transport of oxygenated blood to the brain or the carotid chemoreceptors is responsible for the development of CSR (Ryan and Bradley, 2005). CSR has been reported to be related to an increased circulation time from the lung to the carotid body (i.e., mixing gain) and has been shown to correlate inversely to cardiac output (Hall et al., 1996). However, trying to test this experimentally, Crowell et al. (1956) had to lengthen the heart to brain circulation time by several minutes in order to induce CSR. Furthermore, despite this extreme prolongation in circulation time, CSR was observed only in about 30% of the animals. Thus, prolonged circulation time alone is unlikely to result in CSR, and if it does so, only along with additional factors which were not addressed in out study.
Hudgel and Hamilton (1994) have demonstrated an important role of upper airway instability in CSR with much of the variability in tidal volume explainable based on fluctuations in upper airway resistance. Because the upper airway is much more stable in children than adults (Marcus et al., 2005), the absence of CSR in children with CHF may support the importance of dynamic upper airway instability in CSR pathogenesis.
A number of studies have investigated the risk factors for the presence of central sleep apnea in adult patients with CHF. Sin et al. (1999) identified the following risk factors in men and women with CHF: male gender, atrial fibrillation, age >60 years, and hypocapnia (PCO2 < 38 mmHg) during wakefulness. In our children with CHF 50% were males, no arrhythmias were recorded, and during sleep recording sporadic hypocapnic events did not result in CSR. Although our sample was small, the complete absence of CSR despite severe CHF in these children suggests that age is a strong determinant of CSR across all age groups. Several other studies have reported on the potential age-related effect on the development of CSR in patients with heart failure. Mared et al. (2004) have shown that CSR is common in elderly patients hospitalized due to decompensated chronic heart failure and that age is a stronger determinant of CSR than any of the cardiac or other clinical variables. As age is a strong predictor of CSR, this may reflect the underlying age-dependency of sleep apnea found in healthy subjects as demonstrated by Bixler et al. (1998), although the prevalence is much lower than that found in patients with heart failure.
Compared with younger CHF patients, older patients tend to have less compliant left ventricles with higher left ventricular filling pressures, as well as an increased prevalence of pulmonary venous hypertension. The idea of CSR mainly being a function of low cardiac output (as estimated by LVEF) may therefore be an oversimplification (Sin et al., 1999; Mared et al., 2004). Furthermore prevalence differences of CSR between studies could result from the age of the population studied, with 40% prevalence in our adult study group with average age of 61.9 ± 2.6 years while there are reports in the literature of prevalence of up to 70%, for example in a small group of elderly, hospitalized patients (Ancoli-Israel et al., 1994; Mared et al., 2004). Due to age restrictions or other selection criteria, the importance of age may have been underestimated in many previous studies regarding factors associated with CSR. Thus, we speculate that the absence of CSR in children and its high prevalence in adults is strongly affected by the young age of the population we studied, although the duration of CHF may also play an important role. In the pediatric population no CSR has been reported aside from one case report by Hoch and Barth (2001). who observed CSR in one boy with high output cardiac failure (a patient with Trisomy 21) most probably due to a large atrioventricular septal defect. Of note, one of our patients had Down’s syndrome, and had obstructive apneas, yet did not have CSR. Sommers et al. (2005) reported CHF in 70.6% of infants with severe heart disease during the first year of life with the condition lasting for a mean of 15 months. In 78% of patients with congenital heart disease (CHD), CHF ended after an operation as happened with our group of infants with CHD. In adults, CSR develops following a chronic prolonged course of heart failure. The relatively shorter course of the disease in children (up to corrective surgery or spontaneous improvement) may be therefore another factor accounting for the absence of CSR. Additional potential factors may include the underlying cause for the CHF and better ventricular compliance in the infant.
One could debate whether the well reported periodic breathing of the neonate is an immature form of CSR or has a similar appearance of the crescendo-decrescendo pattern of CSR. Since periodic breathing of the neonate is common in premature newborns (especially those born around gestational age of 30 weeks) but much less frequent in term infants, it may represent an immature respiratory control system, while in CSR the respiratory control sensitivity is usually increased. In term newborns, periodic breathing of the neonate has been reported in up to 3% of total sleep time at age 2 months, and less than 1% at 5 months of age (Parmelee et al., 1972). Furthermore, while periodic breathing of the neonate worsens during active (REM) sleep (Oliveira et al., 2004), this is usually not the case in CSR. In addition, while in periodic breathing, arousals from sleep may be absent, in CSR they appear during the peak hyperpneic phase of breathing (Javaheri et al., 1998; Naughton and Bradley, 1998; Sin et al., 1999; Weintraub et al., 2001; Bradley and Floras, 2003; Oliveira et al., 2004). Thus, although these two respiratory patterns may have some common features, they likely result from different mechanisms and pathophysiologies, and indeed despite considerable research regarding periodic breathing of the neonate, it has never been associated with CHF. In our cohort, all infants were born at term, and although they experienced occasional apneas they did not meet criteria to be classified as periodic breathing (at least three consecutive apneas of at least 3 s duration each, separated by intervals not longer than 20 s) (Parmelee et al., 1972). It would appear that in any case periodic breathing and CSR represent different phenomena, with periodic breathing expressing a form of immature respiratory control manifested predominantly during active sleep, and not related to heart failure, while CSR results from either heart failure or other diseases (e.g., neurological damage) via a mechanism which still needs to be better understood.
Our study has several limitations. First, our sample size is relatively small. However, since we observed zero CSR despite substantial CHF, and aside from one case, CSR has not been previously reported in children despite a relatively large number of studies on CHF, we believe that indeed CSR is an exclusively adult phenomenon as confirmed in our study. Clearly more studies are needed to prove conclusively this statement, and to identify potential protective mechanisms in children with CHF. Second, only three of our patients had low output CHF. As far as we know, even in adults, high output CHF (such as in hyperthyroidism) has not been associated with CSR. Thus, again, larger scale studies are required in order to characterize the absence of CSR in various subgroups of children with CHF. Third, we have assessed respiration with thermistors and not nasal pressure. Theoretically since this is a less sensitive method we could have missed CSR, although we believe this is unlikely. Finally, our control groups consisted of adults with CHF and children with sleep disordered breathing but not of normal healthy children. Since we aimed at investigating potential CSR in children with CHF, we believe that their sleep apnea did not impose a problem for this specific study since they did not have any heart disease.
Nevertheless, despite these limitations, we believe our study suggests that CSR is an adult phenomenon. Although our patients demonstrated the classical factors believed to drive CSR such as low output cardiac failure, pulmonary congestion, hypoxemic events, arousals from sleep and hypocapnia, none of the children had CSR while 40% of the adults did. Thus, we speculate that regardless of the exact mechanism which drives CSR, age (via CHF duration or upper airway stability) is an over-riding factor.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
American Academy of Sleep Medicine Task Force. (1999). Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The report of an American Academy of Sleep Medicine Task Force. Sleep 22, 667–689.
American Thoracic Society Task Force. (1996). Standards and indications for cardiopulmonary sleep studies in children. Am. J. Respir. Crit. Care Med. 153, 866–878.
Ancoli-Israel, S., Engler, R. L., Friedman, P. J., Klauber, M. R., Ross, P. A., and Kripke, D. F. (1994). Comparison of patients with central sleep apnea. With and without Cheyne–Stokes respiration. Chest 106, 780–786.
Bixler, E. O., Vgonzas, A. N., Ten Have, T., Tyson, K., and Kales, A. (1998). Effects of age on sleep apnea in men. 1. Prevalence and severity. Am. J. Respir. Crit. Care Med. 157, 144–148.
Bradley, T. D., and Floras, J. S. (2003). Sleep apnea and heart failure. Part II: central sleep apnea. Circulation 107, 1822–1826.
Bradley, T. D., Logan, A. G., Kimoff, R. J., Sériès, F., Morrison, D., Ferguson, K., Belenkie, I., Pfeifer, M., Fleetham, J., Hanly, P., Smilovitch, M., Tomlinson, G., and Floras, J. S., CANPAP Investigators. (2005). Continuous positive airway pressure for central sleep apnea and heart failure. N. Engl. J. Med. 353, 2025–2033.
Cheshire, K., Engleman, H., Deary, I., Shapiro, C., and Douglas, N. J. (1992). Factors impairing daytime performance in patients with sleep apnea/hypopnea syndrome. Arch. Intern. Med. 152, 538–541.
Cohn, J. N., Levine, T. B., Olivari, M. T., Garberg, V., Lura, D., Francis, G. S., Simon, A. B., and Rector, T. (1984). Plasma norepinephrine as a guide to prognosis in patients with congestive heart failure. N. Engl. J. Med. 311, 819–823.
Crowell, J. W., Guyton, A. C., and Moore, J. W. (1956). Basic oscillating mechanism of Cheyne–Stokes breathing. Am. J. Physiol. 187, 395–398.
Eckert, D. J., Jordan, A. S., Merchia, P., and Malhotra A. (2007). Central sleep apnea: pathophysiology and treatment. Chest 131, 595–607.
Golan, N., Shahar, E., Ravid, S., and Pillar, G. (2004). Sleep disorders and daytime sleepiness in children with attention-deficit/hyperactive disorder. Sleep 27, 261–266.
Hall, M. J., Xie, A., Rutherford, R., Ando, S., Floras, J. S., and Bradley, T. D. (1996). Cycle length of periodic breathing in patients with and without heart failure. Am. J. Respir. Crit. Care Med. 154, 376–381.
Hanly, P. J., and Zuber-Khokhar, N. (1995). Daytime sleepiness in patients with congestive heart failure and Cheyne–Stokes respiration. Chest 107, 952–958.
Hoch, B., and Barth, H. (2001). Cheyne–Stokes respiration as an additional risk factor for pulmonary hypertension in a boy with trisomy 21 and atrioventricular septal defect. Pediatr. Pulmonol. 31, 261–264.
Hudgel, D. W., and Hamilton, H. B. (1994). Respiratory muscle activity during sleep-induced periodic breathing in the elderly. J. Appl. Physiol. 77, 2285–2290.
Javaheri, S. (2000). Effects of continuous positive airway pressure on sleep apnea and ventricular irritability in patients with heart failure. Circulation 101, 392–397.
Javaheri, S., Parker, T. J., Liming, J. D., Corbett, W. S., Nishiyama, H., Wexler, L., and Roselle, G. (1998). Sleep apnea in 81 ambulatory male patients with stable heart failure: types and their prevalence, consequences, and presentations. Circulation 97, 2154–2159.
Lanfranchi, P. A., Braghiroli, A., Bosimini, E., Mazzuero, G., Colombo, R., Donner, C. F., and Giannuzzi, P. (1999). Prognostic value of nocturnal Cheyne–Stokes respiration in chronic heart failure. Circulation 99, 1435–1440.
Malhotra, A., and Jordan, A. S. (2006). Did fat boy Joe need hormone replacement? Sleep 29, 16–18 (Editorial).
Marcus, C. L., Katz, E. S., Lutz, J., Black, C. A., Galster, P., and Carson, K. A. (2005). Upper airway dynamic responses in children with the obstructive sleep apnea syndrome. Pediatr. Res. 57, 99–107.
Mared, L., Cline, C., Erhardt, L., Berg, S., and Midgren, B. (2004). Cheyne–Stokes respiration in patients hospitalised for heart failure. Respir. Res. 5, 14.
Moser, N. J., Phillips, B. A., Berry, D. T., and Harbison, L. (1994). What is hypopnea, anyway? Chest 105, 426–428.
Naughton, M. T., and Bradley, T. D. (1998). Sleep apnea in congestive heart failure. Clin. Chest Med. 19, 99–113.
Oliveira, A. J., Nunes, M. L., Fojo-Olmos, A., Reis, F. M., and da Costa, J. C. (2004). Clinical correlates of periodic breathing in neonatal polysomnography. Clin Neurophysiol 115, 2247–2251.
Parmelee, A. H., Stern, E., and Harris, M. A. (1972). Maturation of respiration in prematures and young infants. Neuropadiatrie 3, 294–304.
Quaranta, A. J., D’Alonzo, G. E., and Krachman, S. L. (1997). Cheyne–Stokes respiration during sleep in congestive heart failure. Chest 111, 467–473.
Ryan, C. M., and Bradley, T. D. (2005). Periodicity of obstructive sleep apnea in patients with and without heart failure. Chest 127, 536–542.
Sin, D. D., Fitzgerald, F., Parker, J. D., Newton, G., Floras, J. S., and Bradley, T. D. (1999). Risk factors for central and obstructive sleep apnea in 450 men and women with congestive heart failure. Am. J. Respir. Crit. Care Med. 160, 1101–1106.
Sin, D. D., Logan, A. G., Fitzgerald, F. S., Liu, P. P., and Bradley, T. D. (2000). Effects of continuous positive airway pressure on cardiovascular outcomes in heart failure patients with and without Cheyne–Stokes respiration. Circulation 102, 61–66.
Somers, V. K., Dyken, M. E., Mark, A. L., and Abboud, F. M. (1993). Sympathetic nerve activity during sleep in normal subjects. N. Engl. J. Med. 328, 303–307.
Somers, V. K., Mark, A. L., Zavala, D. C., and Abboud, F. M. (1989). Contrasting effects of hypoxia and hypercapnia on ventilation and sympathetic activity in humans. J. Appl. Physiol. 67, 2101–2106.
Sommers, C., Nagel, B. H., Neudorf, U., and Schmaltz, A. A. (2005). Congestive heart failure in childhood. An epidemiologic study. Herz 30, 652–662.
Stanchina, M. L., Ellison, K., Malhotra, A., Anderson, M., Kirk, M., Benser, M. E., Tosi, C., Carlisle, C., Millman, R. P., and Buxton, A. (2007). The impact of cardiac resynchronization therapy on obstructive sleep apnea in heart failure patients: a pilot study. Chest 132, 433–439.
Weintraub, Z., Cates, D., Kwiatkowski, K., Al-Hathlol, K., Hussain, A., and Rigatto, H. (2001). The morphology of periodic breathing in infants and adults. Respir. Physiol. 127, 173–184.
Wellman, A., Malhotra, A., Jordan, A. S., Schory, K., Gautam, S., and White, D. P. (2007). Chemical control stability in the elderly. J. Physiol. 581, 291–298.
Keywords: Cheyne–Stokes respiration, congestive heart failure, children, age
Citation: Peer A, Lorber A, Suraiya S, Malhotra A and Pillar G (2010) The occurrence of Cheyne–Stokes respiration in congestive heart failure: the effect of age. Front. Psychiatry 1:133. doi: 10.3389/fpsyt.2010.00133
Received: 10 April 2010;
Paper pending published: 01 May 2010;
Accepted: 17 August 2010;
Published online: 08 September 2010
Edited by:
Eliot S. Katz, Harvard Medical School, USAReviewed by:
Brian McGinley, Johns Hopkins University, USAIgnacio Tapia, The Children’s Hospital of Philadelphia, USA
Copyright: © 2010 Peer, Lorber, Suraiya, Malhotra and Pillar. This is an open-access article subject to an exclusive license agreement between the authors and the Frontiers Research Foundation, which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited.
*Correspondence: Avivit Peer, Sleep Laboratory/Oncology Division, Rambam Medical Center, Haifa 31096, Israel. e-mail: a_peer@rambam.health.gov.il