 Yi-Xing Chen1 Zhao-Chong Zeng1* Zhao-You Tang2 Jia Fan2 Jian Zhou2 Wei Jiang1 Meng-Su Zeng3 Yun-Shan Tan4
Yi-Xing Chen1 Zhao-Chong Zeng1* Zhao-You Tang2 Jia Fan2 Jian Zhou2 Wei Jiang1 Meng-Su Zeng3 Yun-Shan Tan4
- 1 Department of Radiation Oncology, Zhongshan Hospital, Fudan University, Shanghai, China
- 2 Liver Cancer Institute, Zhongshan Hospital, Fudan University, Shanghai, China
- 3 Department of Radiology, Zhongshan Hospital, Fudan University, Shanghai, China
- 4 Department of Pathology, Zhongshan Hospital, Fudan University, Shanghai, China
Purpose: This study was conducted to identify factors involved in lymph node metastasis (LNM) and evaluate their role in predicting LNM in clinically lymph node negative (clinical stage I–III) intrahepatic cholangiocarcinoma (ICC). Materials and Methods: We selected 320 patients who were diagnosed with ICC with no apparent clinical LNM (T1–3N0M0). Age, gender, tumor boundary, histological differentiation, tumor size, and carbohydrate antigen 19-9 value were the studied factors. Univariate and multivariate logistic analysis were conducted. Receiver operating characteristics curve analysis was used to test the predicting value of each factor and a test which combined the associated factors was used to predict LNM. Results: LNM was observed in 76 cases (76/320, 23.8%). Univariate and multivariate analysis showed that histological differentiation as well as tumor boundary and tumor size significantly correlated with LNM. The sensitivity and negative predictive value for LNM for the three factors when combined was 96.1 and 95% respectively. This means that 5% of the patients who did not have the risk factors mentioned above developed LNM. Conclusion: This model used the combination of three factors (low-graded histological differentiation, distinct tumor boundary, small tumor size) and they proved to be useful in predicting LNM in ICC with clinically lymph node negative cases. In patients with these criteria, lymph node dissection or lymph node irradiation may be omitted and such cases may also be good candidates for stereotactic body radiotherapy (SBRT).
Introduction
Intrahepatic cholangiocarcinoma (ICC) is a primary malignant tumor arising peripherally to the secondary bifurcation of the left or right hepatic duct. ICC is a relatively rare liver tumor when compared to hepatocellular carcinoma (HCC). ICC accounts for about 5–30% of primary liver tumors (Kaczynski et al., 1998; Yamamoto et al., 1998; Shaib and El-Serag, 2004). Surgical resection improves long-term survival in patients with ICC but the prognosis after aggressive resection remains unsatisfactory (Ohtsuka et al., 2002). Overall resectability rates were 54.6% in a study from Japan (Ikai et al., 2004) and 62% in a study from the United States (Weber et al., 2001) with the 1 and 3 year cumulative survival rates after resection being 49.4–76.6 and 17.3–52.7%, respectively (Fu et al., 2004; Shinohara et al., 2008; Choi et al., 2009; Lang et al., 2009). However, other methods such as radiotherapy have been examined in many retrospective series with promising results with respect to local control and survival benefit (Zeng et al., 2006; Chen et al., 2010; Jiang et al., 2010; Saxena et al., 2010a). Adjuvant and definitive radiotherapy may play an important role in the treatment of ICC in the future.
Lymph node metastasis (LNM) has been reported to be a significant prognostic factor in ICC (Hanazaki et al., 2002; Fu et al., 2004; Nakagawa et al., 2005; Choi et al., 2009; Guglielmi et al., 2009; Saxena et al., 2010b). It is also important to decide whether a patient with ICC should be considered for irradiation of the regional lymph nodes. If the absence of nodal metastasis is accurately detected, there would be no need for an extended irradiation field and thus the role of radiation therapy will become more significant. Therefore, identification of clinicopathologic factors that predict the status of lymph nodes in ICC could have potential clinical benefits. Till date, there are no accurate pre-operative factors that can predict LN metastasis. However, by using a combination of pre-operative factors, it might be possible to accurately categorize a subset of patients with no LNM.
In this study, 320 surgical cases with clinically negative lymph node (T1–3N0M0) ICC were analyzed and the factors associated with LNM were studied. The objectives of this study were to determine whether we could predict normal or metastatic lymph nodes using our approach and therefore avoiding unnecessary regional lymph node irradiation in selected patients with ICC.
Materials and Methods
Patients and Diagnosis
From January 2000 to January 2010, 370 patients with histologically proven ICC underwent hepatectomy at the Liver Cancer Institute, Zhongshan hospital, Fudan University. In this group, 320 patients had no metastasis to regional lymph nodes as per pre-operative images (CT/MRI). This study was approved by the ethical review board of Zhongshan Hospital, Fudan University.
Intrahepatic cholangiocarcinoma was confirmed by histopathological examination and the medical history and examination. HCC and metastasis from gastrointestinal cancers were ruled out by immunohistochemical staining for Hepa, CK7, CK19, CK20, alpha fetoprotein (AFP), MUC5AC, and MUC6. Positive staining for MUC5AC and CK7 together with negative staining for MUC6 and CK20 was suggestive of ICC. On the other hand, positive staining for MUC6 and CK20 combined with negative staining for MUC5AC and CK7 was suggestive of liver metastasis from colorectal cancer. The serum tumor markers such as carcinoembryonic antigen (CEA), carbohydrate antigen 19-9 (CA19-9), and AFP were also used as diagnostic tools to exclude HCC or mixed ICC/HCC.
Radiological images such as enhanced CT or MRI (or both) were used to assess the state of the tumor in the liver and to determine the tumor boundary, tumor size, and the presence of multiple nodules. We found that the boundary of ICC can be divided into two different forms based on radiological images: 1. During the arterial phase, ICC can have a distinct boundary, which appears as a regular border with a thin, ring-like iso-attenuated or enhanced structure relative to the liver (Figure 1A); 2. The second form has an obscure boundary that is characterized by an ill-defined border (Figure 1B). Assessment of tumor size was based on the largest dimension of the tumor. Multiple nodules were defined as the presence of two or more nodules, including intrahepatic metastases and satellite lesions. Nodal size is the current standard criteria for the defining LNM on imaging studies and lymph nodes measuring 1 cm or more in minimum diameter were regarded as metastatic. The following pre-operative demographics and clinical information were retrospectively obtained from patients’ medical records: age, gender, and CA19-9. Tumor stage was defined according to the American Joint Committee on Cancer (AJCC) seventh edition staging for ICC (Nathan and Pawlik, 2010).
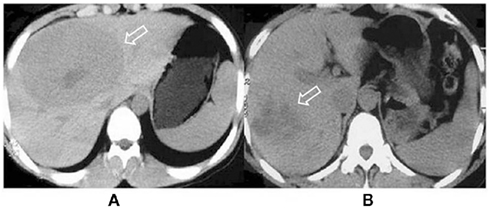
Figure 1. (A) CT scan showing an intrahepatic cholangiocarcinoma that appears as a low-density area and has a regular, distinct boundary. (B) CT scan showing an intrahepatic cholangiocarcinoma with an obscure boundary.
The locations of LNM were classified as reported by the Liver Cancer Study Group of Japan (1997). The hilum, cystic duct, pericholedochal nodes, periportal nodes, and proper hepatic nodes around and in the hepatoduodenal ligament were grouped together as the hepatic hilum nodes (N1 group). The nodes in the pancreatic head and around the common hepatic artery and celiac trunk were defined as the N2 group. The N3 group was defined as the nodes around the para-aorta, major omenta, paracolic, and paramesenteric areas.
Statistical Analysis
In order to assess the factors which predict the probability of metastasis to lymph node, we first used univariate analysis (logistic regression model) to assess the following: age (less than 65 years, 65 years or older), gender, tumor boundary (distinct, obscure), the grade of differentiation (low: well to moderately; high: poorly to undifferentiated), tumor size (5 cm or less, more than 5 cm), multiple nodules, and CA19-9 (normal range: 37 ng/ml or less; abnormal value: more than 37 ng/ml). All variables which were significant (P-value less than 0.05) in the univariate analysis were entered in the multivariate analysis in order to discriminate the significant risk factors for LN metastases.
Receiver operating characteristic (ROC) curves were used to determine the predictive value of the parameters. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and the accuracy were obtained for each of the testing method based on the binomial distribution.
All reported P-values are two sided. In both of the univariate and multivariate analyses, the relative risks (RRs) and their respective 95% confidence intervals (CIs) from the logistic regression model were reported. All statistical analyses were performed using SPSS, version 15.0 for Windows (Statistical Product and Services Solutions, SPSS Inc, Chicago, IL, USA). A value of P < 0.05 was considered statistically significant.
Results
Demographic Data
There were 136 females and 184 males in this study. The median age was 56.9 ± 11.33 years (range 18–89 years). The tumor diameter ranged from 0.8 to 15 cm, with a median diameter of 6.1 ± 2.89 cm. 236 patients (73.8%) had a low-grade lesions and 84 patients (26.2%) had a high-grade lesions. The other patients’ characteristics including tumor boundary, number of nodes, and CA19-9 are provided in Table 1.
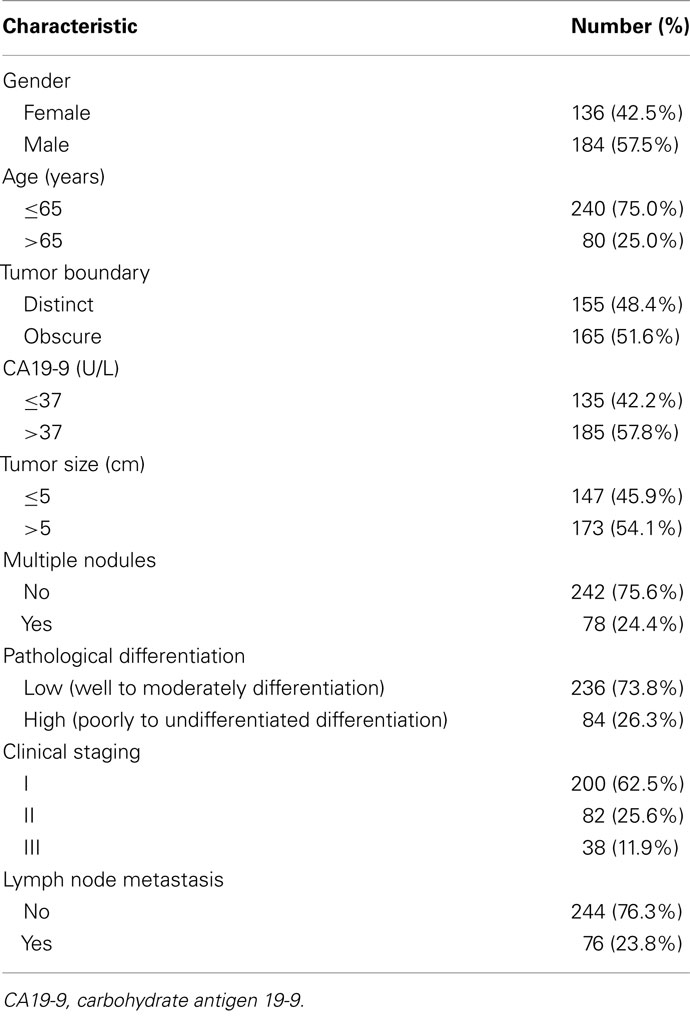
Table 1. Patient characteristics.
Two hundred (62.5%) patients had stage I cancer, 82 (25.6%) had stage II cancer and 38 (11.9%) had stage III and staging was carried out according to the seventh edition of the UICC-TNM staging system for ICC.
Among all the 320 patients, 76 (23.8%) were confirmed to have LNM by pathological examination. The most common site of LNM was the hepatic hilum (N1, n = 54, 67.8%) while other sites were the peripancreatic head (N2, n = 17, 25.9%) as well as the para-aortic area and the major omenta (N3, n = 5, 6.3%).
Analysis of the Factors Associated with LNM
In order to develop a model for predicting LNM, we first conducted a univariate analysis to test the predictive value of the following potential categorical predictors: gender, age, tumor boundary, tumor size, multiple nodules, histological differentiation, and CA19-9. As shown in the Table 2, we found that LNM was associated with elevated CA19-9 (P = 0.017, RR = 1.955), tumor boundary (P = 0.01, RR = 2.512), tumor size (P = 0.005, RR = 2.202), and the histological differentiation (P < 0.01, RR = 7.630).
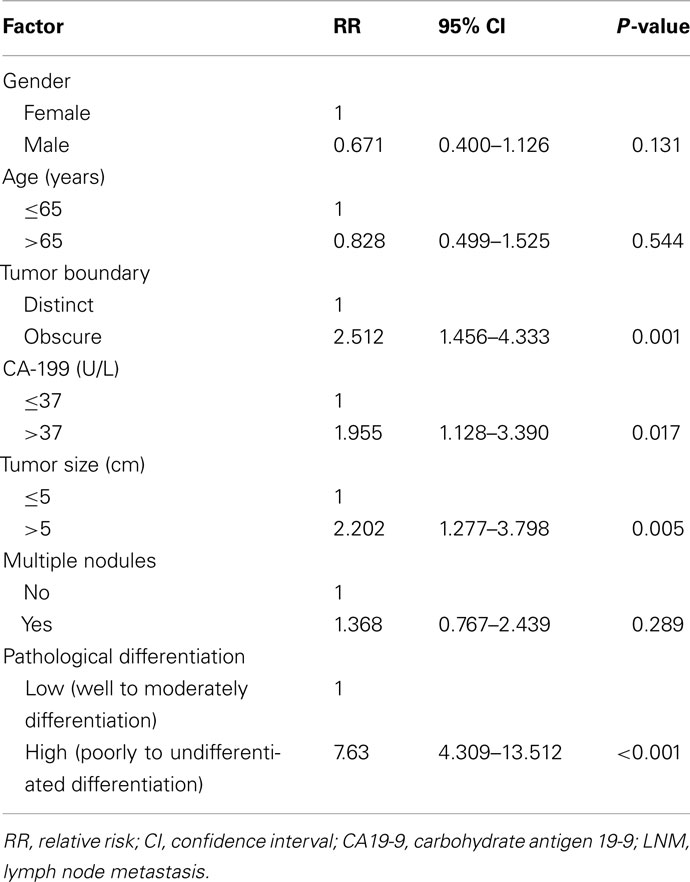
Table 2. Results of the univariate analysis of factors associated with LNM.
All variables that were significant in the univariate analysis were selected and a multivariate analysis was conducted. The variables that reached significance in the multivariate analysis were the tumor size (P = 0.006, RR = 2.371), tumor boundary (P = 0.009, RR = 2.250) and histological differentiation (P < 0.001, RR = 7.355; Table 3). However, CA19-9 was not an independent factor for predicting LNM in multivariate analysis (RR = 0.674, P = 0.105).
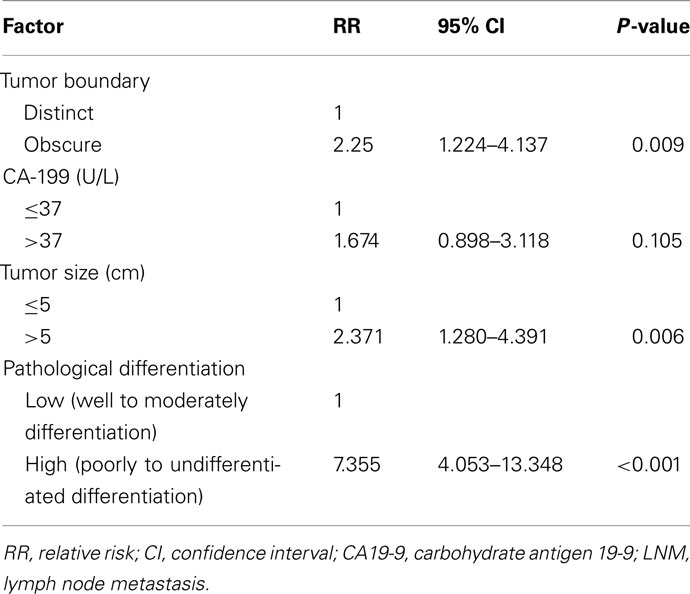
Table 3. Results of the multivariate analysis of factors associated with LNM.
Prediction Model for LNM Using Tumor Boundary, Tumor Size, and Histological Differentiation
Receiver operating characteristic curve analysis was performed for these predictive factors. The area under the curve (AUC) and the 95% CI were used to assess the power of these factors in predicting the LNM (Figure 2). ROC analysis showed that histological differentiation was accurate in predicting LNM (AUC: 0.716; 95% CI: 0.645–0.788; P < 0.001), followed by tumor boundary (AUC: 0.611; 95% CI: 0.539–0.682; P = 0.004) and tumor size (AUC: 0.594; 95% CI: 0.522–0.666; P = 0.013; Table 4).
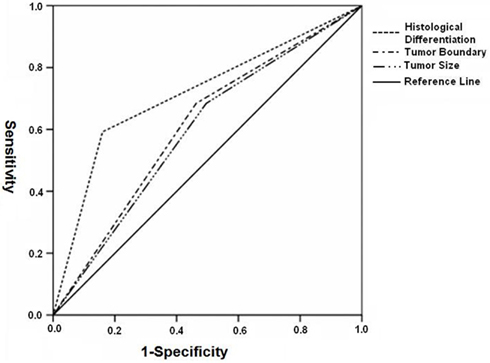
Figure 2. Receiver operating characteristic analysis: ROC analysis of histological differentiation, tumor boundary, and tumor size. The AUC of all parameters was less than 0.5, indicating that they were predictive of LNM.
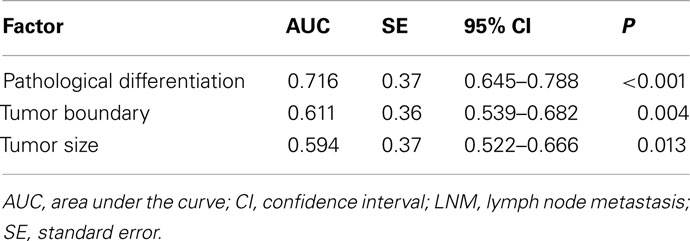
Table 4. Area under the curve demonstrating the discriminatory power of each factor for predicting LNM.
The sensitivity/specificity, PPV/NPV, and the accuracy after the combination of two or three significant factors for LNM are summarized in Table 5. Conspicuously, the sensitivity/specificity and PPV/NPV by combining the three factors (tumor boundary, tumor size, and histological differentiation) for LNM were 96.1/23.0 and 28.0/95.0%, respectively. Furthermore, the accuracy was 40.3%. This means that among the 59 patients (18.4%) who had none of these three risk factors, only three patients had LNM. For these specific patients, regional lymph node irradiation may be omitted during radiotherapy.
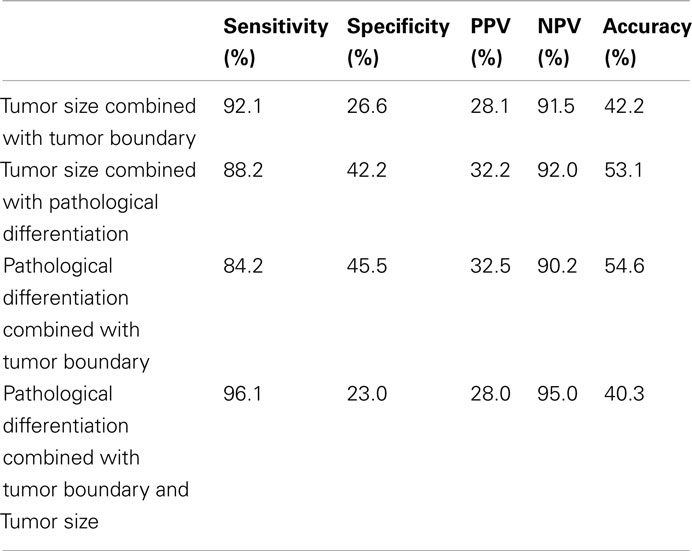
Table 5. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of factors significant on multivariate analysis.
Furthermore, we found that 73 patients (73/76, 90.1%) with LN metastasis had at least one risk factor: 18 patients had one risk factor, 34 patients had two risk factors, and 21 patients had three risk factors. 56 patients (56/244, 23.0%) without LN metastasis had no significant risk factors. In the remaining 188 patients without LN metastasis, 111 patients had one risk factor, 69 patients had two risk factors and 8 patients had three risk factors.
Discussion
Unlike HCC, ICC is commonly associated with LNM. This study, which was conducted on a relative large number of patients and showed that the incidence of LNM for those patients without pre-operative node evaluation was 23.8% (76/320); LNM has been reported to be associated with poor prognosis in patients with ICC (Hanazaki et al., 2002; Fu et al., 2004; Zeng et al., 2006; Chen et al., 2010; Jiang et al., 2010; Saxena et al., 2010a) plus it is also important in defining the target volume for the radiation oncologist.
Previous studies (Bluestein et al., 1994; Narayan et al., 1994; Fuwa et al., 2007) have developed models based on clinical or pathologic data so as to predict the risk of lymph node metastases for other cancers such as lung cancer and prostate cancer. This information is important so as to decide whether a cancer patient should undergo a staging lymphadenectomy (including laparoscopic technique) or directly considered for irradiation of the regional lymph nodes; however, limited data is available regarding ICC and LNM prediction. Since radiotherapy may play an important role in the treatment of ICC in the future, it is time to discuss how to delineate the target volume in patients with ICC. Therefore, the aim of this study was to try to determine whether we could accurately predict nodal status preoperatively in ICC and avoid unnecessary regional lymph node irradiation in selected patients. This study indicates that we can avoid unnecessary lymph node region irradiation in about 18.4% of patients with ICC who had none of the tested clinicopathologic factors.
In this study, we tried to analyze the correlation between clinicopathologic factors and LNM. Univariate analysis test showed that LNM was associated with histological differentiation, tumor boundary, tumor size, and CA19-9 serum levels. Multivariate logistic analysis revealed that only histological differentiation, tumor boundary, and tumor size, demonstrated aggressive tumor characteristics and were independent predictors for LNM. Histological differentiation and tumor size may be because of the biological behavior of ICC. Poor differentiated or undifferentiated tumors together with large tumor size points toward increased invasiveness. Even though few previous reports have described the type of tumor boundary on imaging for ICC, it was found to be a good predictor for microinvasion (Bi et al., 2010). In our study, tumor boundary is also associated with LNM. In addition, histological differentiation was a superior predictor of LNM as shown by a ROC-based approach.
Patients with elevated CA19-9 levels are more likely to develop recurrent disease and survive for a shorter time than patients with normal CA19-9 levels; higher CA19-9 levels are associated with more advanced TNM stages (Endo et al., 2008; Hatzaras et al., 2010). However, in our study, the CA19-9 value was found to be a significant factor based on the univariate analysis but not based on the multivariate analysis.
The overall accuracy for detecting metastatic lymph nodes by pre-operative imaging has been reported to be 57–82.2% (Hanazaki et al., 2002; Park et al., 2006; Kim et al., 2008). The most common error in pre-operative imaging is underestimation of the nodal involvement (Vilgrain, 2008). Therefore, combining the factors listed above may help improve pre-operative evaluation of LNM for patients with clinically negative lymph node. In our study, with the combination two of the three factors (tumor boundary, tumor size, and histological differentiation), the sensitivity and NPV were 84.2–92.1 and 90.2–92.0%, respectively. Considering the clinical significance of LN metastasis and its importance for the delineation of target volume, the tests required to predict LN metastasis should show high sensitivity and high NPV. The sensitivity and NPV of the three combined pre-operative criteria in our study reached 96.1 and 95%, respectively. This suggested that if a patient with a small tumor size (less than 5 cm), distinct tumor boundary and low-grade differentiation, the chance for LNM is very low (5%) and also indicates that regional lymph node irradiation may be omitted in these specific cases.
Technological advances in radiation planning, breathing motion reduction strategies, and image guidance have made it possible for radiation to be delivered conformally to focal liver cancers while reducing the risk of toxicity. Stereotactic body radiation therapy (SBRT), referring to an improved spatial distribution of the administered dose and delivering the potent radiation in fewer fractions, has also been used safely and efficiently for intrahepatic tumors (Mendez Romero et al., 2006; Tse et al., 2008). This is a highly attractive treatment option in a palliative situation where overall treatment time is significantly reduced. In our study, cases where the histological differentiation is low-grade, the tumor boundary is distinct, and the tumor size is less than 5 cm, the probability of LNM is low and for these patients SBRT may be a good choice.
The current study is limited because it is a small-scale retrospective hospital-based study at a single institution. Large-sized multi-center studies will be needed to confirm our results. Another important limitation of this study relates to the discrimination of tumor boundary. The classification of tumor boundary is highly subjective and therefore the inclusion of this factor could affect the accuracy of the prediction system. Consequently, a strict classification system is needed to define this parameter in the future. Finally, this large series was conducted over a long period (2000–2009); both diagnostic and therapeutic procedures for ICC have considerably changed over these years. Thus, these developments probably contributed to variance in the correlation between pre-operative characteristics and LNM.
In conclusion, it has been demonstrated that cases with low-grade differentiation, distinct tumor boundary and tumor size of no more than 5 cm, the probability of LNM is very low (5%). The tested combination of the three factors is useful for the prediction of patients without LN metastasis and we could safely omit regional lymph node irradiation in about a fifth of patients with ICC while these cases are also good candidates for SBRT.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Bi, A. H., Zeng, Z. C., Ji, Y., Zeng, H. Y., Xu, C., Tang, Z. Y., Fan, J., Zhou, J., Zeng, M. S., and Tan, Y. S. (2010). Impact factors for microinvasion in intrahepatic cholangiocarcinoma: a possible system for defining clinical target volume. Int. J. Radiat. Oncol. Biol. Phys. 78, 1427–1436.
Bluestein, D. L., Bostwick, D. G., Bergstralh, E. J., and Oesterling, J. E. (1994). Eliminating the need for bilateral pelvic lymphadenectomy in select patients with prostate cancer. J. Urol. 151, 1315–1320.
Chen, Y. X., Zeng, Z. C., Tang, Z. Y., Fan, J., Zhou, J., Jiang, W., Zeng, M. S., and Tan, Y. S. (2010). Determining the role of external beam radiotherapy in unresectable intrahepatic cholangiocarcinoma: a retrospective analysis of 84 patients. BMC Cancer 10, 492. doi:10.1186/1471-2407-10-492
Choi, S. B., Kim, K. S., Choi, J. Y., Park, S. W., Choi, J. S., Lee, W. J., and Chung, J. B. (2009). The prognosis and survival outcome of intrahepatic cholangiocarcinoma following surgical resection: association of lymph node metastasis and lymph node dissection with survival. Ann. Surg. Oncol. 16, 3048–3056.
Endo, I., Gonen, M., Yopp, A. C., Dalal, K. M., Zhou, Q., Klimstra, D., D’Angelica, M., DeMatteo, R. P., Fong, Y., Schwartz, L., Kemeny, N., O’Reilly, E., Abou-Alfa, G. K., Shimada, H., Blumgart, L. H., and Jarnagin, W. R. (2008). Intrahepatic cholangiocarcinoma: rising frequency, improved survival, and determinants of outcome after resection. Ann. Surg. 248, 84–96.
Fu, X. H., Tang, Z. H., Zong, M., Yang, G. S., Yao, X. P., and Wu, M. C. (2004). Clinicopathologic features, diagnosis and surgical treatment of intrahepatic cholangiocarcinoma in 104 patients. HBPD INT 3, 279–283.
Fuwa, N., Mitsudomi, T., Daimon, T., Yatabe, Y., Shinoda, M., Hatooka, S., Mori, S., Fukui, T., and Inaba, Y. (2007). Factors involved in lymph node metastasis in clinical stage I non-small cell lung cancer – from studies of 604 surgical cases. Lung Cancer 57, 311–316.
Guglielmi, A., Ruzzenente, A., Campagnaro, T., Pachera, S., Valdegamberi, A., Nicoli, P., Cappellani, A., Malfermoni, G., and Iacono, C. (2009). Intrahepatic cholangiocarcinoma: prognostic factors after surgical resection. World J. Surg. 33, 1247–1254.
Hanazaki, K., Kajikawa, S., Shimozawa, N., Shimada, K., Hiraguri, M., Koide, N., Adachi, W., and Amano, J. (2002). Prognostic factors of intrahepatic cholangiocarcinoma after hepatic resection: univariate and multivariate analysis. Hepatogastroenterology 49, 311–316.
Hatzaras, I., Schmidt, C., Muscarella, P., Melvin, W. S., Ellison, E. C., and Bloomston, M. (2010). Elevated CA 19-9 portends poor prognosis in patients undergoing resection of biliary malignancies. HPB (Oxford) 12, 134–138.
Ikai, I., Itai, Y. J., Okita, K., Omata, M., Kojiro, M., Kobayashi, K., Nakanuma, Y., Futagawa, S., Makuuchi, M., and Yamaoka, Y. (2004). Report of the 15th follow-up surgery of primary liver cancer. Hepatol. Res. 28, 21–29.
Jiang, W., Zeng, Z. C., Tang, Z. Y., Fan, J., Zhou, J., Zeng, M. S., Zhang, J. Y., Chen, Y. X., and Tan, Y. S. (2010). Benefit of radiotherapy for 90 patients with resected intrahepatic cholangiocarcinoma and concurrent lymph node metastases. J. Cancer Res. Clin. Oncol. 136, 1323–1331.
Kaczynski, J., Hansson, G., and Wallerstedt, S. (1998). Incidence, etiologic aspects and clinicopathologic features in intrahepatic cholangiocellular carcinoma–a study of 51 cases from a low-endemicity area. Acta Oncol. 37, 77–83.
Kim, J. Y., Kim, M. H., Lee, T. Y., Hwang, C. Y., Kim, J. S., Yun, S. C., Lee, S. S., Seo, D. W., and Lee, S. K. (2008). Clinical role of 18F-FDG PET-CT in suspected and potentially operable cholangiocarcinoma: a prospective study compared with conventional imaging. Am. J. Gastroenterol. 103, 1145–1151.
Lang, H., Sotiropoulos, G. C., Sgourakis, G., Schmitz, K. J., Paul, A., Hilgard, P., Zöpf, T., Trarbach, T., Malagó, M., Baba, H. A., and Broelsch, C. E. (2009). Operations for intrahepatic cholangiocarcinoma: single-institution experience of 158 patients. J. Am. Coll. Surg. 208, 218–228.
Liver Cancer Study Group of Japan. (1997). Classification of Primary Liver Cancer, 1st English Edn. Tokyo: Kanehara.
Mendez Romero, A., Wunderink, W., Hussain, S. M., De Pooter, J. A., Heijmen, B. J., Nowak, P. C., Nuyttens, J. J., Brandwijk, R. P., Verhoef, C., Ijzermans, J. N., and Levendag, P. C. (2006). Stereotactic body radiation therapy for primary and metastatic liver tumors: a single institution phase I-II study. Acta Oncol. 45, 831–837.
Nakagawa, T., Kamiyama, T., Kurauchi, N., Matsushita, M., Nakanishi, K., Kamachi, H., Kudo, T., and Todo, S. (2005). Number of lymph node metastases is a significant prognostic factor in intrahepatic cholangiocarcinoma. World J. Surg. 29, 728–733.
Narayan, P., Fournier, G., Gajendran, V., Leidich, R., Lo, R., Wolf, J. S. Jr., Jacob, G., Nicolaisen, G., Palmer, K., and Freiha, F. (1994). Utility of preoperative serum prostate-specific antigen concentration and biopsy Gleason score in predicting risk of pelvic lymph node metastases in prostate cancer. Urology 44, 519–524.
Nathan, H., and Pawlik, T. M. (2010). Staging of intrahepatic cholangiocarcinoma. Curr. Opin. Gastroenterol. 26, 269–273.
Ohtsuka, M., Ito, H., Kimura, F., Shimizu, H., Togawa, A., Yoshidome, H., and Miyazaki, M. (2002). Results of surgical treatment for intrahepatic cholangiocarcinoma and clinicopathological factors influencing survival. Br. J. Surg. 89, 1525–1531.
Park, M. S., Lee, D. K., Kim, M. J., Lee, W. J., Yoon, D. S., Lee, S. J., Lim, J. S., Yu, J. S., Cho, J. Y., and Kim, K. W. (2006). Preoperative staging accuracy of multidetector row computed tomography for extrahepatic bile duct carcinoma. J. Comput. Assist. Tomogr. 30, 362–367.
Saxena, A., Bester, L., Chua, T. C., Chu, F. C., and Morris, D. L. (2010a). Yttrium-90 radiotherapy for unresectable intrahepatic cholangiocarcinoma: a preliminary assessment of this novel treatment option. Ann. Surg. Oncol. 17, 484–491.
Saxena, A., Chua, T. C., Sarkar, A., Chu, F., and Morris, D. L. (2010b). Clinicopathologic and treatment-related factors influencing recurrence and survival after hepatic resection of intrahepatic cholangiocarcinoma: a 19-year experience from an established australian hepatobiliary unit. J. Gastrointest. Surg. 14, 1128–1138.
Shaib, Y., and El-Serag, H. B. (2004). The epidemiology of cholangiocarcinoma. Semin. Liver Dis. 24, 115–125.
Shinohara, E. T., Mitra, N., Guo, M., and Metz, J. M. (2008). Radiation therapy is associated with improved survival in the adjuvant and definitive treatment of intrahepatic cholangiocarcinoma. Int. J. Radiat. Oncol. Biol. Phys. 72, 1495–1501.
Tse, R. V., Hawkins, M., Lockwood G. Kim, J. J., Cummings, B., Knox, J., Sherman, M., and Dawson, L. A. (2008). Phase I study of individualized stereotactic body radiotherapy for hepatocellular carcinoma and intrahepatic cholangiocarcinoma. J. Clin. Oncol. 26, 657–664.
Weber, S. M., Jarnagin, W. R., Klimstra, D., DeMatteo, R. P., Fong, Y., and Blumgart, L. H. (2001). Intrahepatic cholangiocarcinoma: resectability, recurrence pattern, and outcomes. J. Am. Coll. Surg. 193, 384–391.
Yamamoto, M., Takasaki, K., Yoshikawa, T., Ueno, K., and Nakano, M. (1998). Does gross appearance indicate prognosis in intrahepatic cholangiocarcinoma? J. Surg. Oncol. 69, 162–167.
Zeng, Z. C., Tang, Z. Y., Fan, J., Zhou, J., Qin, L. X., Ye, S. L., Sun, H. C., Wang, B. L., Li, D., Wang, J. H., Zeng, M. S., Guo, W., and Tan, Y. S. (2006). Consideration of the role of radiotherapy for unresectable intrahepatic cholangiocarcinoma: a retrospective analysis of 75 patients. Cancer J. 12, 113–122.
Keywords: intrahepatic cholangiocarcinoma, lymph node metastasis, predictors, radiotherapy, logistic analysis
Citation: Chen Y-X, Zeng Z-C, Tang Z-Y, Fan J, Zhou J, Jiang W, Zeng M-S and Tan Y-S (2011) Prediction of the lymph node status in patients with intrahepatic cholangiocarcinoma: analysis of 320 surgical cases. Front. Oncol. 1:42. doi: 10.3389/fonc.2011.00042
Received: 31 August 2011;
Accepted: 19 October 2011;
Published online: 10 November 2011.
Edited by:
Anatoly Dritschilo, Georgetown University School of Medicine, USAReviewed by:
Sean Collins, Georgetown University Hospital, USARalph Robert Weichselbaum, University of Chicago, USA
Copyright: © 2011 Chen, Zeng, Tang, Fan, Zhou, Jiang, Zeng and Tan. This is an open-access article subject to a non-exclusive license between the authors and Frontiers Media SA, which permits use, distribution and reproduction in other forums, provided the original authors and source are credited and other Frontiers conditions are complied with.
*Correspondence: Zhao-Chong Zeng, Department of Radiation Oncology, Zhongshan Hospital, Fudan University, Shanghai 200032, China. e-mail: zeng.zhaochong@zs-hospital.sh.cn