 Victoria Fernández de Casadevante
Victoria Fernández de Casadevante Julita Gil Cuesta2,3
Julita Gil Cuesta2,3 Lourdes Cantarero-Arévalo
Lourdes Cantarero-Arévalo- 1Section for Social and Clinical Pharmacy, Department of Pharmacy, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark
- 2Infectious Disease Epidemiology, Statens Serum Institut, Copenhagen, Denmark
- 3European Program for Intervention Epidemiology Training (EPIET), European Centre for Disease Prevention and Control (ECDC), Stockholm, Sweden
Background: Cervical cancer is the fourth most common cancer affecting women worldwide. Since 2006, two human papillomavirus vaccines (HPVV) have been licensed to protect women against the virus that causes cervical cancer. However, worldwide coverage remains unequal. Studies from the USA found strong evidence for differences in HPVV uptake by ethnicity and healthcare coverage. As the profile of ethnic groups and the healthcare system in the USA differ from countries in Europe where HPVV is free in most of the countries, we conducted a systematic review in order to analyze the determinants of HPVV uptake in Europe.
Methods: We performed a systematic Pubmed, Scopus, and Science Direct search to find articles published from HPVV availability in European countries until April 2014. No age restriction was applied. We included all studies assessing factors associated with HPVV uptake. Uptake refers to either initiation and/or completion of the three dose vaccination program.
Results: Out of the 23 eligible studies, 14 were retrospective reviews of data, six were cross-sectional surveys, and three were prospective cohort studies. Higher HPVV uptake was associated with ethnic majority populations, higher socio-economic status, regular cervical screening participation by the mother, and having received previous childhood vaccinations.
Conclusion: Since the vaccine is offered for free in most of the European countries, the findings suggest that ethno-cultural and educational factors play an important role when it comes to HPVV uptake. Girls who were undervaccinated had also a lower uptake of standard childhood vaccines and mothers who were less likely to attend cervical cancer screening. This may indicate that only few parents have specific concerns with HPVV, and that preventive health care should seek ways to target these vulnerable groups.
Introduction
The latest statistics published by the International Agency for Research on Cancer (IARC), the specialized cancer agency of the World Health Organization, shows that cervical cancer occupies the fourth position in the list of the most common cancers affecting women all over the world, preceded by breast, colorectal, and lung cancers (1). More specifically, the estimated incidence of cervical cancer was of 527,624 new cases in 2012. In the same year, cervical cancer was responsible for 265,653 deaths in the world, which constituted the fourth most common cause of cancer death worldwide (1).
Cervical cancer is often defined as a disease of disparity, because it differently affects poor and wealthy countries: at least 80% of cervical cancer deaths occur in developing countries (1). However, disparities also occur within a single country, as is the case of the USA, where Hispanic and African American women have, respectively, 2 and 1.5 times more risk of developing cancer than non-Hispanic White women (2). In Europe, the incidence and mortality rates of cervical cancer vary considerably within the region (3).
Since 2006, two human papillomavirus vaccines (HPVV) have been licensed globally, aimed at preventing cervical cancer: Cervarix®, a bivalent vaccine that targets papillomavirus 16 and 18, and Gardasil®, which additionally targets papillomavirus 6 and 11. Types 16 and 18 are responsible for around 70% of all cervical cancer cases, whereas types 6 and 11 are responsible for about 90% of anogenital warts (4). Immunization as a three-dose series against the human papillomavirus (especially before sexual onset) is recommended as primary prevention method of certain HPV infections, in order to reduce the incidence of cervical cancer and other anogenital cancer (5). However, worldwide coverage remains unequal and uptake varies widely (6).
Population-based studies (7) reporting information about HPVV uptake are helpful to identify determinants associated with poor vaccination. Hence, vaccination programs or campaigns geared toward reaching populations with low HPVV uptake can be designed to improve coverage.
A systematic review and meta-analysis (8) published in February 2013 found strong evidence for differences in HPVV initiation by factors such as ethnicity and healthcare coverage. The results were based on 27 studies, of which the majority were performed in the USA (n = 22), with additional studies from Canada (n = 2), and only three were conducted in Europe. As the healthcare system and the profile of ethnic groups in the USA significantly differ from countries in Europe, we consider it relevant to focus on studies reporting data from Europe. To our knowledge, no systematic review reporting factors associated with HPV vaccine uptake has been published to date in this specific region.
The aim of this study is to conduct a systematic review of the peer-reviewed literature in order to analyze the determinants of HPVV uptake in Europe.
Method
Data Sources
The PRISMA guidelines (9) have been followed throughout the elaboration of this systematic review. A systematic Pubmed, Scopus, and Science Direct search was performed by the authors. The search terms were “HPV” or “human papillomavirus” AND “vaccine” or “immunization” AND “uptake” or “coverage” AND “inequalities,” “determinants,” “socio-economics,” “minority groups,” “ethnicity,” or “social background.” Those terms were also combined with “Europe,” “Eastern Europe,” “Russia.” Finally, the reference lists of the selected articles were reviewed in order to get additional references not identified via the database search.
Eligibility Criteria
We selected articles reporting HPVV uptake in females with no age restriction, and reporting at least one factor associated with vaccine uptake (either initiation, completion, or both). Articles could include register data or data from questionnaires/surveys, and no publication date filter was selected. All studies aimed at identifying and assessing factors associated with HPVV uptake were included. HPVV uptake by both routine and catch-up groups was considered. No European country was excluded. Only articles reported in English were selected. Interviews, reviews, and gray literature were excluded. Articles in which the main focus was knowledge, attitudes, or intentions to receive the HPV vaccine were also not eligible. Publications reporting the same cohorts were only included if the variables studied were different.
Definitions
Human Papillomavirus vaccines program initiation refers to the uptake of either the first or the second dose of the three dose program recommended to get the full benefit of the vaccine.
Human Papillomavirus vaccines program completion refers to the reception of the three vaccine doses recommended to get full protection.
The routine group refers to the primary target group to receive the HPVV, which usually aims at girls that did not start their sexual life (5). Catch-up programs refer to those programs that have been created to target slightly older girls, usually up to the age of 26. The recommended age for either routine or catch-up group is determined by each country.
Data Extraction
All the relevant data were organized and extracted into the PRISMA predefined form (9). Descriptive data such as study population, study location, study time period, study design, vaccine delivery mechanism, and sample size were extracted for each study. The overall risk of bias was assessed for each study according to the sample size, and classified to be from low to high risk (<1,000 participants). (Table 1).
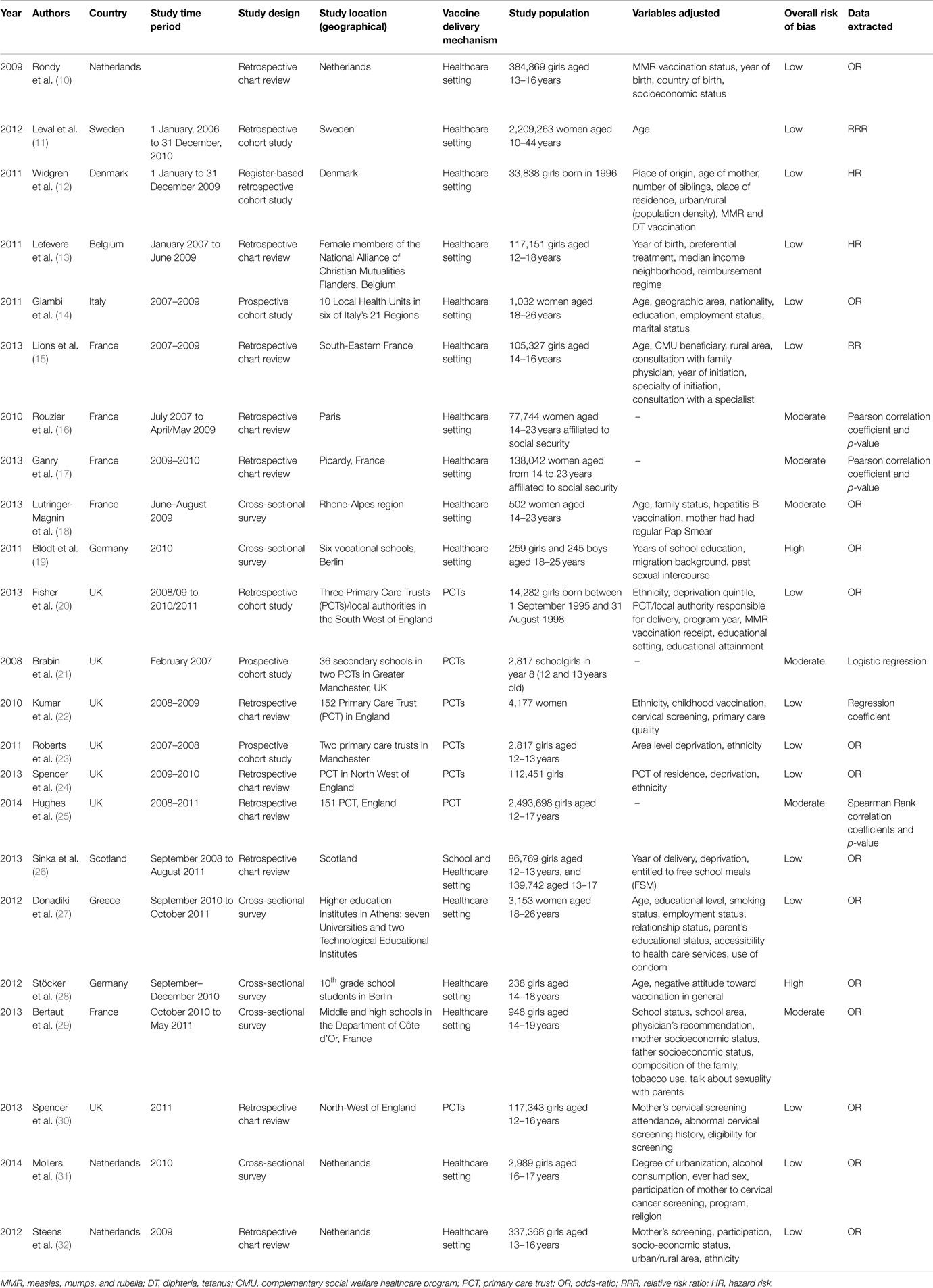
Table 1. Descriptive characteristics of studies eligible for the review.
Most of the studies reported their results based on tests for associations between variables and the following assessment of the strength of the associations. The effect measures most commonly employed were: odds-ratio (n = 14), relative risk (n = 2), and hazard ratio (n = 2). Other studies (n = 5) reported correlation coefficients and p-values to measure association, which also were included in the results section.
Data Variables and Statistical Analysis
The data analysis was performed by tabulating the data collected from the variables of interest and outcomes (HPVV uptake, either initiation, completion, or both) of the selected studies. If available, adjusted results were preferred to do the comparison among studies; however, unadjusted results were also considered in case no adjustment was performed in the study.
Results
A total of 349 articles were identified through the different databases. Of these, 221 were excluded for different reasons: having a different research question (n = 98), not being European-based studies (n = 79), being duplicates (n = 42), or not being in English (n = 2). The abstracts of the remaining 128 articles were reviewed, and 68 were excluded for not being a study based in Europe (n = 46), for being review articles (n = 6), for addressing a different research question (n = 6), for not reporting data collected through registers or surveys (n = 4), for explaining intentions and attitudes toward HPVV, not actual vaccination (n = 3), for not reporting data on factors associated to HPV vaccine uptake (n = 2), and for not reporting data on HPV vaccine uptake (n = 1). Overall, 60 full-text studies were assessed. After assessing the inclusion and exclusion criteria, 19 were identified as relevant articles for the systematic review and 41 were discarded. The reasons for exclusion were reporting about intentions, beliefs, or attitudes toward HPVV (n = 19), for not reporting data on original European studies (n = 11), for not reporting data on factors associated to HPV vaccine uptake (n = 9), and finally for not providing data regarding HPV vaccine uptake (n = 2). Additionally, four studies were found through the reference list of some of the selected articles and included in our systematic review. Overall, 23 articles reporting HPV vaccine uptake and factors associated to it were selected since they fulfilled the inclusion criteria (Figure 1).
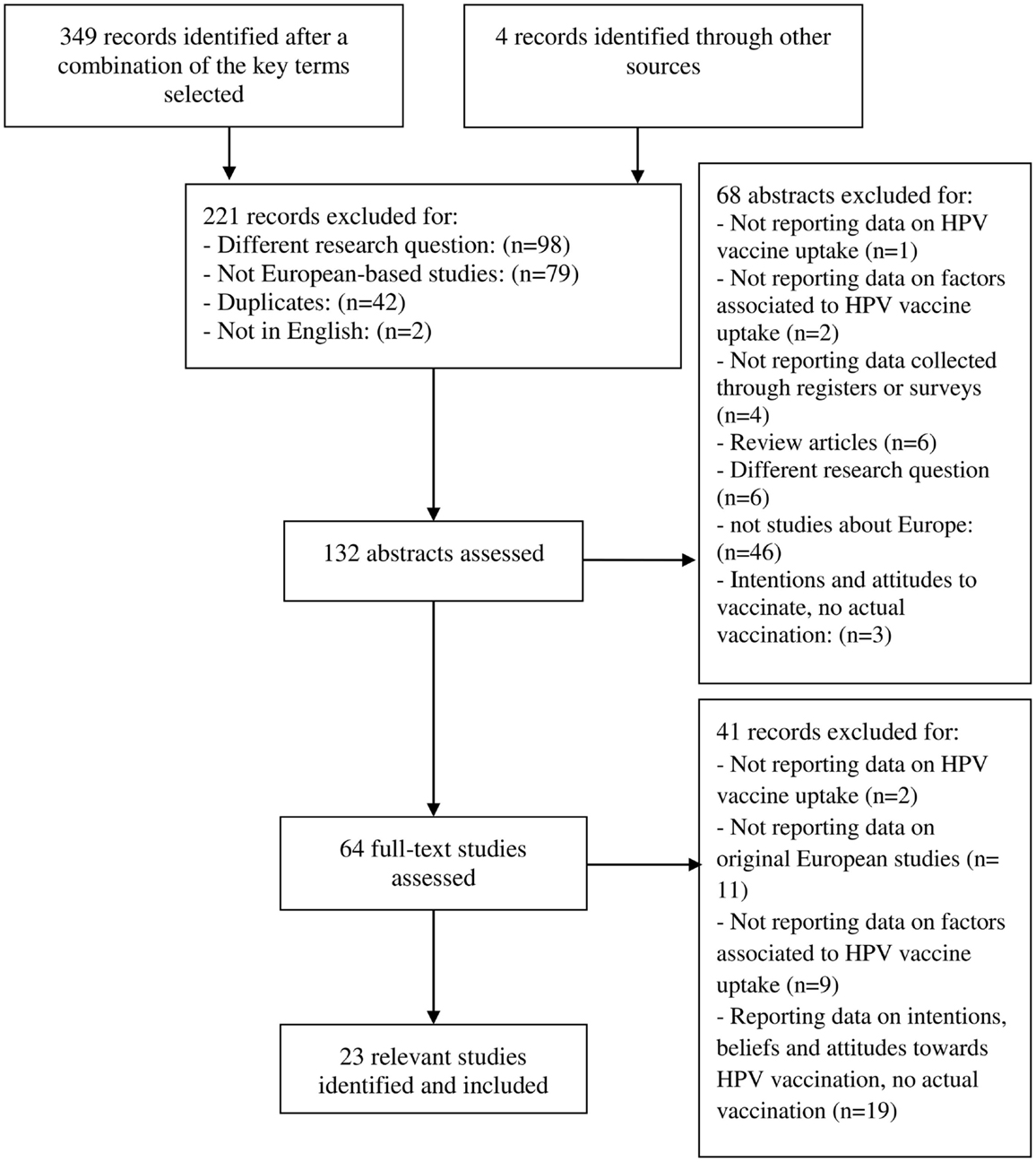
Figure 1. Flow chart of study selection procedure.
Study Characteristics
Overall, data on 6,247,077 women aged from 12 to 44 years were included in the studies presented in 23 articles, representing ten countries. Of the included studies, 11 focused on the HPVV initiation (10, 12–14, 18, 19, 21–23, 28, 31) and factors associated with it, three focused on HPVV completion (11, 25, 27), and nine focused on both initiation and completion (15–17, 20, 24, 26, 29, 30, 32), along with factors associated with it. Sample size ranged from 238 to 2,493,698 women, and 19 studies had a sample size over 1,000. The included studies were mostly retrospective chart reviews or retrospective cohort studies based on data extracted from registers or databases (n = 14). The rest were cross-sectional surveys (n = 6) and prospective cohort studies (n = 3).
Factors Associated with Vaccine Initiation
Ethnicity
Overall, 12 studies (10, 12, 17, 19–24, 28, 31, 32) compared HPVV initiation by ethnicity. Nine (10, 12, 17, 20–24, 32) found an association between ethnicity and HPVV initiation, where the uptake was substantially lower in areas with high ethnic minority populations. Out of the nine, three studies (20, 23, 24) conducted in the UK showed that the probability of Non-white girls being vaccinated was lower compared to White girls. The last study (32) conducted in the Netherlands found that having Moroccan ethnicity contributed to non-participation in the HPV immunization program compared with the ethnic majority in that country. That was confirmed by another study conducted in the Netherlands (32). On the contrary, three studies (19, 28, 31) [two of them (19, 28) with a very small sample size] found no association of HPVV initiation with ethnic background (Table 2).
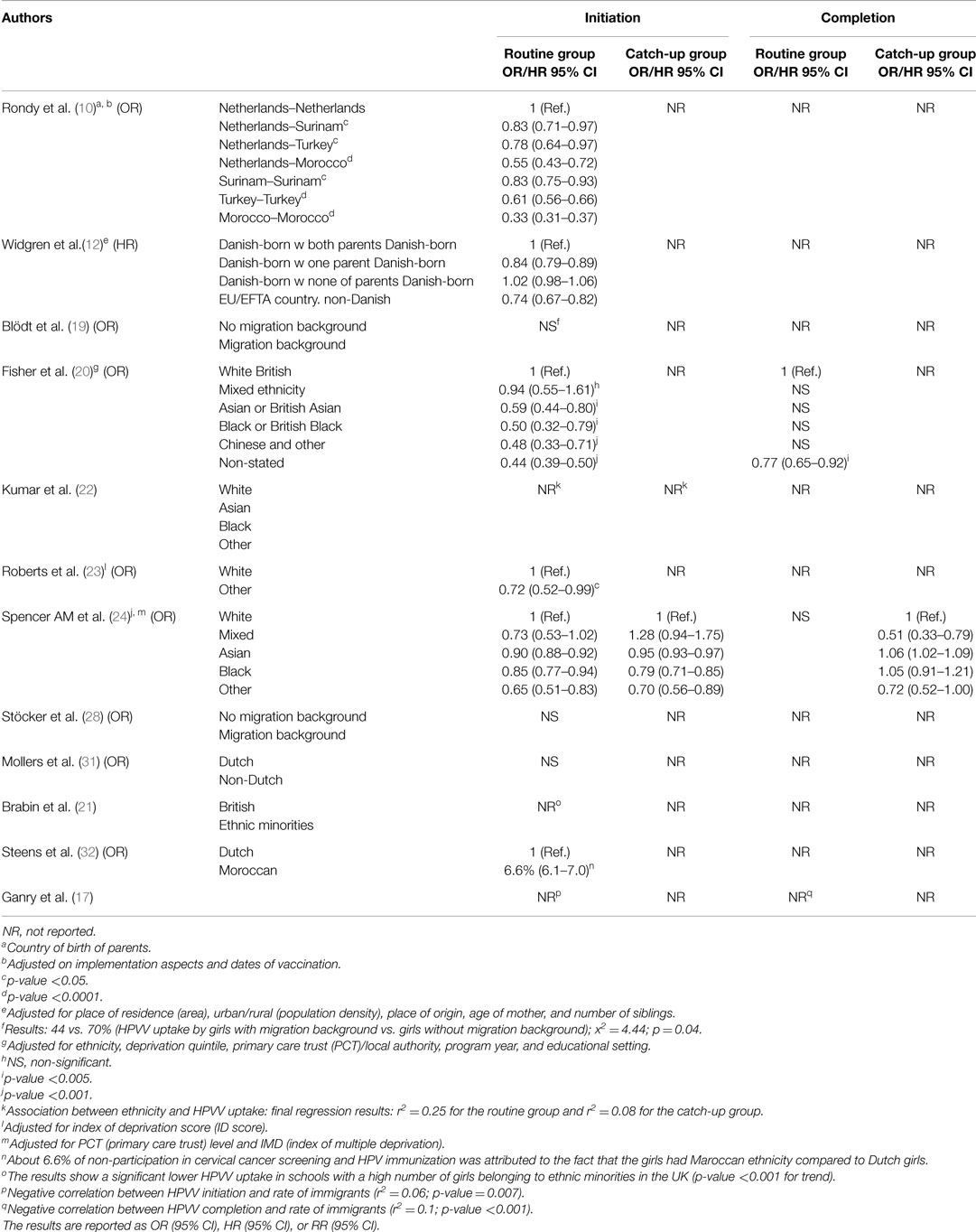
Table 2. Ethnic background as a determinant of HPVV initiation and completion.
Socio-Economic Status and Education Level
Fourteen articles (10, 13–15, 17, 20–24, 26, 29, 31, 32) reported data on socio-economic status or area-level indicators and HPV vaccine initiation. All studies (10, 13–15, 21–24, 26, 29, 32) but three (17, 20, 31) showed an association between pertaining to a disadvantaged socio-economic group and lower HPVV initiation. For two of these studies (22, 24), however, this association was only seen for those girls that belong to the catch-up group (17–18 and 14–16 years, respectively). On the contrary, three studies (17, 20, 31) found no evidence of association between HPVV initiation and socio-economic status. Regarding education level as such, a small study (19) found that girls with more than 11 years of school education had a higher HPVV initiation than those with less than 11 years of education. These results were supported by another study (14) that found that girls enrolled in a high school or higher degree had higher vaccine initiation than those with a lower degree (Table 3).
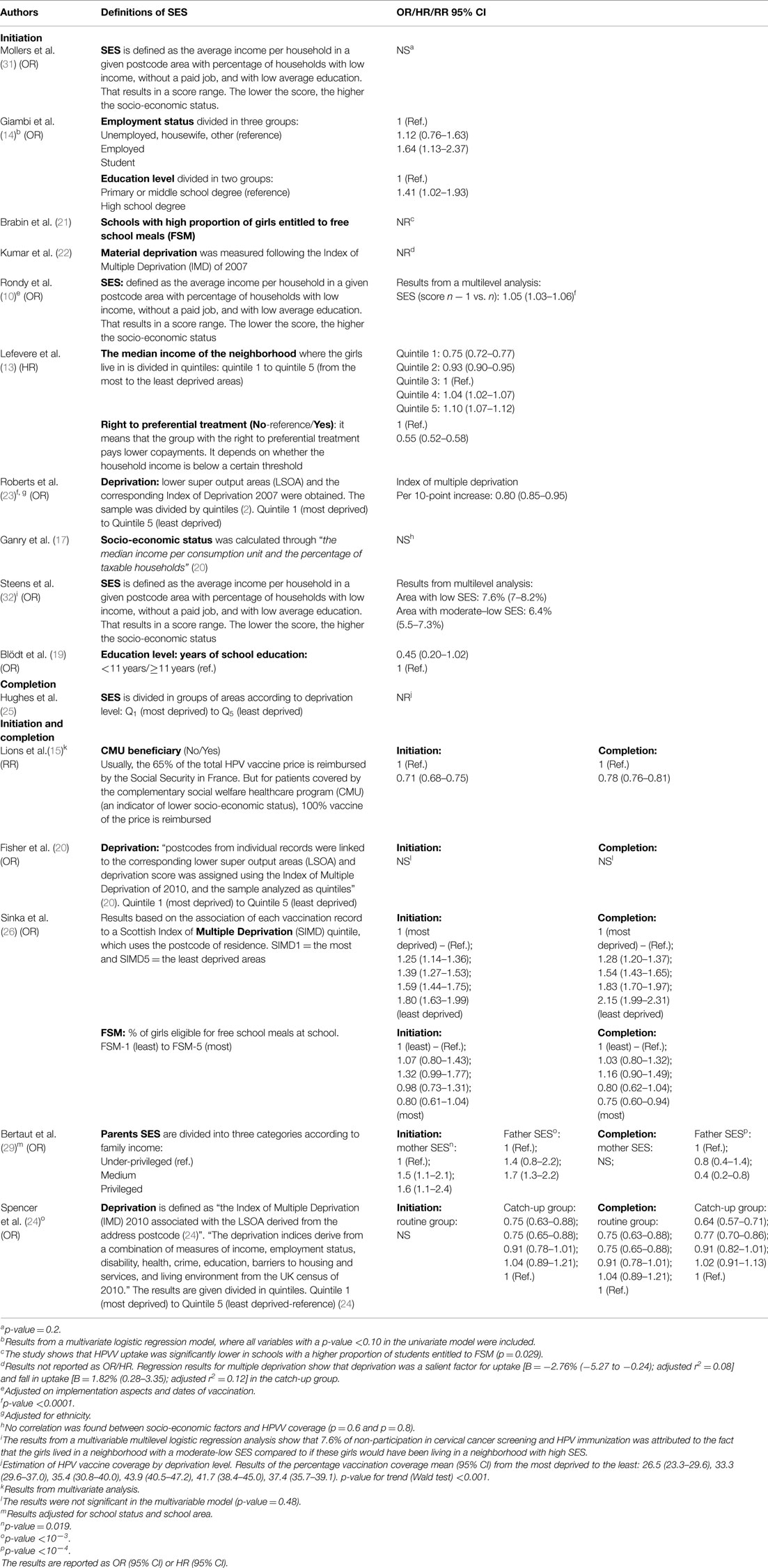
Table 3. Socio-economic status (SES) and education level as a determinant of HPVV initiation and completion.
Age
Of the seven studies including a cohort of girls aged 12–24 years (10, 13, 16–18, 26, 28), which allowed comparison of HPVV initiation between different ages, three showed the highest vaccination initiation at the age of 16–18 years (13, 16, 28), two (10, 17) at the age of 14–15 years, one (18) at the age of 14–16 years, and one (26) showed similar HPVV initiation from 12–17 years of age. Additionally, two studies including a cohort of girls aged 18–26 years (14, 19) found no significant association between age and HPVV initiation (Table 4).
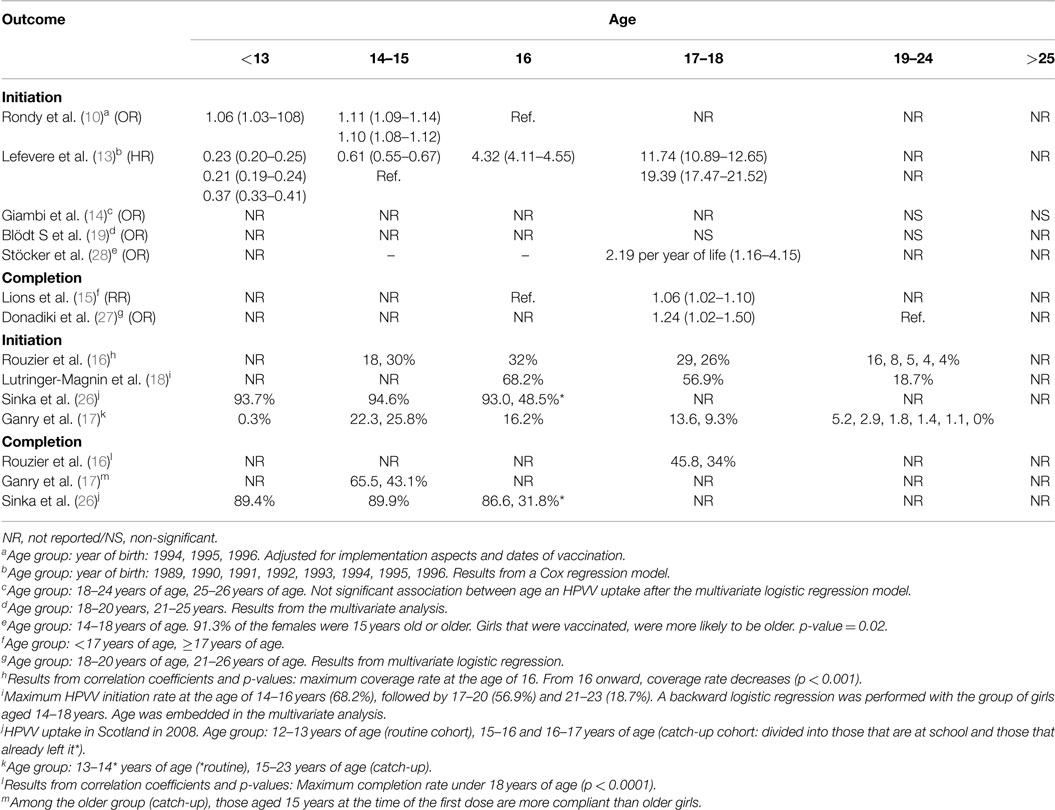
Table 4. Age as a determinant of HPVV initiation and completion.
Vaccination History
Having received, previous childhood immunization was associated with higher HPVV initiation in all studies (10, 12, 20, 23) that compared immunization initiation by childhood vaccination history, but one small study (28). Being vaccinated against Hepatitis B was found to be associated with higher HPVV initiation in one study (18) (see Table S1 in Supplementary Material).
Mother’s Cervical Screening Attendance
Regular participation of mother in cervical cancer screening programs was positively associated with HPVV initiation in four studies (18, 30–32) that compared uptake by mother’s screening attendance. In one of the studies (32), the likelihood of HPVV initiation was 40% higher if the mother regularly participated in cervical cancer screening programs compared to those whose mothers did not participate (see Table S2 in Supplementary Material).
Area of Residence
One Danish study (12) making reference to population density showed that girls living in the least urbanized areas (1–9 inhabitants/km2) had the lowest HPVV initiation (aHR = 0.87; 95% CI: 0.77–0.97) compared to the most urbanized areas (>1,000 inhabitants/km2). HPVV initiation in urban schools was twice that of rural schools (aOR = 1.9; 95% CI: 0.86–0.99) in another study (29) conducted in France. This was supported by another study also conducted in France (15), which found an association between living in a rural area and having a lower HPVV initiation (aOR = 0.96; 95% CI: 0.92–0.99). On the contrary, living in rural areas (<1,000 inhabitants/km2) remained associated with higher vaccine initiation in two other studies conducted in the Netherlands [aOR = 0.80; 95% CI: 0.70–1.00 for a high degree of urbanization (31) and 6.6%; 95% CI: 6.10–7.00 for the other study (32)]. This result means that looking at the participation in HPV immunization programs and cervical cancer screening, 6.6% of non-participation in both prevention programs was attributed to the fact that they were living in an urban area (32).
Consultation with a Specialist or Physician’s Recommendation
Having consulted with a specialist (pediatrician, family physician, gynecologist, or other) was associated with higher vaccination initiation in one study (aRR = 1.33; 95% CI: 1.30–1.36) (15) and physician’s vaccine recommendation was associated with HPVV initiation in another study (29) (aOR = 2.8; 95% CI: 1.70–4.70).
Other Factors
One study showed a lower uptake for those girls who never had sexual intercourse in the past (OR = 0.44; 95% CI: 0.17–1.11) (19), whereas the other revealed that having had sex in the past is a negative predictor of HPVV initiation (aOR = 0.80; 95% CI: 0.60–1.00) (31).
Factors Associated with Vaccine Completion
Ethnicity
Lower HPVV completion was observed among ethnic minorities in the catch-up group in a study (24) that compared vaccine completion in the routine and catch-up group by ethnicity. This was supported by another study (17) that found a negative correlation between having completed vaccination by ethnic minorities (r2 = 0.1; p < 0.001). Another study (20) also found an association between belonging to an ethnic minority group and lower HPVV completion, but in this case, only those girls belonging to the ethnic category “non-stated” showed lower vaccine program completion (aOR = 0.77; 95% CI: 0.65–0.92; p < 0.004). The study defined the “Non-stated” category as a group consisting of either children of populations that had missing ethnicity because they were born outside the participating Primary Care Trust (PCT) (e.g., immigrants), because parents did not want to reveal their ethnicity prior to the child’s birth, or because parents did not understand that specific question at the moment they were asked (Table 2).
Socio-Economic Status
Four studies (15, 24–26) out of six (15, 20, 24–26, 29) reporting information about the three-dose program completion and socio-economic status showed an association between non-completion and low socio-economic background. However, for one of these studies (25), the negative association was only observed among the oldest group of girls (aged 16 or older). In contrast, one study (20) found no association between lower HPVV completion and deprivation (p = 0.48), and one study (29) showed that after initiation of the vaccination program, girls who attended private schools [aOR = 0.50 (95% CI: 0.40–0.80), p < 0.001] or who belonged to families where the father has higher incomes were less likely to complete the three-dose program. Girls with at least one university-educated parent were more likely to be fully vaccinated than those whose parents did not finish high school [relative risk reduction (RRR) = 15.45; 95% CI: 14.65–16.30] (11). The same trend was seen in another study (27), which also compared vaccine completion between University and Technological Educational Institute students, and the results showed a higher program completion among University students (OR = 1.22; 95% CI: 1.01–1.49) (Table 3).
Age
Two studies (15, 27) reporting vaccine completion by age group showed that girls aged over 17 years were more likely to complete the vaccination program compared to other groups of age. Two other studies (16, 17), however, revealed that girls under 18 years of age were more likely to complete it. More specifically, one of these studies (17) showed higher program completion in girls aged 13–14 years. On the contrary, a study conducted in Scotland (26) found high vaccine program completion among all girls in that study, except from the group of girls aged 16–17 years that had already left school, where the uptake was lower (Table 4).
Mother’s Cervical Screening Attendance
Two studies (30, 32) found positive associations between mothers’ cervical screening attendance and girls’ program completion [aOR = 2.2; 95% CI: 1.6–2.9, and aOR = 1.54; 95% CI: 1.51–1.57, respectively] (see Table S2 in Supplementary Material).
Area of Residence
One study (15) reporting data on HPV vaccine completion by rural/urban area showed a lower vaccine completion in girls living in rural areas (RR = 0.92; 95% CI: 0.86–0.98) compared to those living in urban areas, whereas another study (29) did not find significant variation in the results by population areas (p = 0.24).
Prescriber
Two studies (15, 17) found an association between the specialization of the physician responsible for the vaccine prescription and the completion of the vaccination program. While one study (17) found that the program completion was higher if the prescriber of the first dose was a pediatrician or a gynecologist compared to a general practitioner [48.1, 44.7, and 38.3%, respectively (p < 0.001)], another found that the highest program completion was achieved if the prescriber was a family physician [(RR = 0.90; 95% CI: 0.86–0.94) for the gynecologist, and family physician was the reference group] (15). A third study (16) found no significant correlation between prescriber (general practitioner vs. gynecologist) and HPVV program completion.
Discussion
Main Findings
Belonging to ethnic minority groups and having a disadvantaged socio-economic status were associated with lower HPVV initiation and completion in the majority of the studies. The highest HPVV program initiation was observed at the age of 16–18 years in more than half of the studies. Consultation with a specialist was associated with higher HPVV initiation. Regular cervical screening participation by the mother was associated with higher HPV vaccine program initiation and completion. Having received previous childhood vaccinations was associated with higher HPVV uptake.
Findings in Relation to Other Studies
Regarding ethnicity, there is an overall association between belonging to an ethnic minority group and having a lower probability of HPVV uptake. That suggests that cultural factors concerning sexually transmitted infections could be an important issue in the HPV vaccine uptake. This result is similar to the previous systematic review mostly based on American studies that showed lower likelihood to initiate HPVV program among ethnic minority groups compared to the ethnic majority population (8). Two of the three studies that did not report a significant difference in uptake between ethnic backgrounds had a population sample inferior to 500 girls. Thus, the number of ethnic minority girls participating in the study might not be large enough to be representative.
Most of the studies showed an association between higher deprivation level and lower HPVV program initiation and completion. This is especially relevant since women and girls with low socio-economic status are at a special risk of developing cervical cancer (33, 34). Taking into account that the HPVV is offered for free in the majority of the European countries, the lower uptake among deprived people is unlikely to be a result of purely economic reasons. Studies (35–39) reporting data on social inequalities in healthcare indicate lower healthcare participation among socioeconomically deprived populations. This indicates that the lower vaccine uptake among most deprived populations might be explained by a combination of factors; parents and girls may have a different perception on the importance of HPVV as a preventive measure, parents and girls may not have received information about the immunization program, or if received, did not have the time to read it or the knowledge or language skills to understand it (39, 40). Some of the studies (22, 24, 25) measuring completion rates by socio-economic status, however, showed lower immunization program completion only for the catch-up group. In this case, the reason is likely to be the different delivery mechanism employed for older girls. The majority of girls in the routine cohort received the vaccination at school, whereas older girls are often sent to healthcare settings to receive the vaccine. This can lead to a decrease in adherence to the three-dose immunization schedule since the girls or the parents have to arrange an appointment at the clinic instead of having arranged it by the school and during normal school hours.
As referred by Koulova et al. (5) and Garnet et al. (41), it is recommended to start the vaccination program at a younger age and preferably before sexual onset in order to increase the vaccine effectiveness. However, in the light of our results, older adolescents have a higher probability to initiate and complete the program. The highest vaccination initiation rate was seen at the age of 16–18 years in four out of seven studies. These results are comparable to those published in a systematic review (4), which shows that higher vaccination rates were achieved among older adolescents. According to Dempsey et al. (42), one reason could be the fact that parents might be more likely to accept the vaccination as the age of the daughter increases.
According to the literature (43, 44), parental attitudes toward preventive measures often influence the decision-making of their daughters. This suggests that parents’ general perceptions toward vaccinations may play a role also with regard to the uptake of HPVV. Furthermore, regular mothers’ screening attendance has been found to be associated with HPVV program initiation and completion in a variety of studies in the literature (45–47). This suggests that mothers who attend preventive health services acknowledge their relevance, and may transmit these positive attitudes to their daughters or to decisions regarding their daughters, which positively contributes to a high HPVV uptake. It is a concern that non-attending cervical screening is a predictor for under-vaccination, which suggests that there may be less added value of vaccination.
Limitations
There are several potential limitations. There is a risk of selection bias, which was assessed in the different studies according to sample size and the presence or absence of adjustment for potential confounders. Studies reporting data of small samples (<1,000 participants) were considered to be at moderate-to-high risk of bias (Table 1). Studies were heterogeneous in the study design, in the independent variables included, and in the definition of reference groups, making it difficult to compare results. Additionally, vaccination coverage was reported by either caregivers, by reimbursement data, or by the people themselves, introducing a risk of misclassification bias, recall bias, or response bias. Sampling strategy also differed across studies, leading to a potential selection bias. Some studies lacked statistical significance, given the small size and given that no adjustment for potential confounders was performed. Additionally, there was little consistency in the factors controlled for in the analysis across studies, limiting potentially the comparison of the study results. Most of the studies were performed in rather wealthy countries, and no study was found from Central- or Eastern-Europe, where the majority of cervical cancer cases occur, even though the vaccine is available in most of the European countries.
Conclusion
We found an association between ethnic minority background and disadvantaged socio-economic status and lower HPVV uptake in Europe. Given that the vaccine is offered for free in most of the European countries, the findings suggest that ethno-cultural and educational factors may be important when it comes to HPVV uptake. The fact that girls who are undervaccinated with HPVV also have lower uptake of standard childhood vaccines and mothers that are less likely to attend cervical cancer screening indicate that the reasons for non-vaccination are related to a general lower compliance with preventive health rather than specific concerns about HPVV. Efforts should be put into providing vulnerable populations with a targeted information on the vaccine, and health interventions such as vaccination campaigns should specifically target them to improve HPVV uptake.
Because higher effectiveness is achieved if the vaccine is administered prior to sexual onset, communication efforts should be made to increase the HPVV acceptance among young adolescents.
Since some girls leave school early, and therefore do not take part of the school vaccination programs, a reminder program can be designed where a letter is sent to each of the girls missing any dose, aimed at reaching the maximum HPVV program initiation and completion.
Further similar studies in other European countries, especially in Eastern and Central Europe, are needed to get a representative population and to find determinants in the HPVV uptake in these countries. The creation of patterns in the HPVV uptake would allow targeting these populations in which the uptake is significantly lower, with the ultimate objective of reducing the cervical cancer burden.
Author Contributions
VFC and LC-A contributed to the conception, design, and drafting of the study. VFC was responsible for acquisition and analysis of data. VFC, LC-A, and JGC contributed to the analysis and interpretation of data. VFC, LC-A, and JGC revised it for critically important intellectual content. All authors have seen and approved the final version submitted.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We would like to acknowledge the helpful comments and critical review provided by Palle Valentiner-Branth and Kåre Mølbak at the Statens Serum Institut.
Supplementary Material
The Supplementary Material for this article can be found online at http://journal.frontiersin.org/article/10.3389/fonc.2015.00141
References
1. Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC, CancerBase No. 11 [Internet]. Lyon: International Agency for Research on Cancer (2013).
2. Watson M, Saraiya M, Benard V, Coughlin SS, Flowers L, Cokkinides V, et al. Burden of cervical cancer in the United States, 1998-2003. Cancer (2008) 113:2855–64. doi: 10.1002/cncr.23756
3. Kesic V, Poljak M, Rogovskaya S. Cervical cancer burden and prevention activities in Europe. Cancer Epidemiol Biomarkers Prev (2012) 21:1423–33. doi:10.1158/1055-9965.EPI-12-0181
4. Kessels SJ, Braunack-Mayer AJ, Reuzel R, Tooher RL. Factors associated with HPV vaccine uptake in teenage girls: a systematic review. Vaccine (2012) 30(24):3546–56. doi:10.1016/j.vaccine.2012.03.063
5. Koulova A, Tsui J, Irwin K, Van Damme P, Biellik R, Aguado MT. Country recommendations on the inclusion of HPV vaccines in national immunization programs among high-income countries, June 2006-January 2008. Vaccine (2008) 26(51):6529–41. doi:10.1016/j.vaccine.2008.08.067
6. Dorleans F, Giambi C, Dematte L, Cotter S, Stefanoff P, Mereckiene J, et al. The current state of introduction of human papillomavirus vaccination into national immunization schedules in Europe: first results of the VENICE2 2010 survey. Euro Surveill (2010) 15(47):19730.
7. Izquierdo JN, Schoenbach VJ. The potential and limitations of data from population-based state cancer registries. Am J Public Health (2000) 90(5):695–8. doi:10.2105/AJPH.90.5.695
8. Fisher H, Trotter CL, Audrey S, MacDonald-Wallis K, Hickman M. Inequalities in the uptake of human papillomavirus vaccination: a systematic review and meta-analysis. Int J Epidemiol (2013) 42(3):896–908. doi:10.1093/ije/dyt049
9. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med (2009) 6(7):e1000097. doi:10.1371/journal.pmed.1000097
10. Rondy M, van Lier A, van de Kassteele J, Rust L, de Melker H. Determinants for HPV vaccine uptake in the Netherlands: a multilevel study. Vaccine (2010) 28(9):2070–5. doi:10.1016/j.vaccine.2009.12.042
11. Leval A, Herweijer E, Ploner A, Eloranta S, Fridman Simard J, Dillner J, et al. Quadrivalent human papillomavirus vaccine effectiveness: a Swedish national cohort study. J Natl Cancer Inst (2013) 105(7):469–74. doi:10.1093/jnci/djt032
12. Widgren K, Simonsen J, Valentiner-Branth P, Mølbak K. Uptake of the human papillomavirus-vaccination within the free-of-charge childhood vaccination program in Denmark. Vaccine (2011) 29(52):9663–7. doi:10.1016/j.vaccine.2011.10.021
13. Lefevere E, Hens N, De Smet F, Van Damme P. Dynamics of HPV vaccination initiation in Flanders (Belgium) 2007-2009: a Cox regression model. BMC Public Health (2011) 11:470. doi:10.1186/1471-2458-11-470
14. Giambi C, Donati S, Declich S, Salmaso S, Ciofi Degli Atti ML, Alibrandi MP, et al. Estimated acceptance of HPV vaccination among Italian women aged 18–26 years. Vaccine (2011) 29(46):8373–80. doi:10.1016/j.vaccine.2011.08.079
15. Lions C, Pulcini C, Verger P. Papillomavirus vaccine coverage and its determinants in South-Eastern France. Med Mal Infect (2013) 43(5):195–201. doi:10.1016/j.medmal.2013.03.003
16. Rouzier R, Giordanella JP. Coverage and compliance of human papilloma virus vaccines in Paris: demonstration of low compliance with non-school-based approaches. J Adolesc Health (2010) 47(3):237–41. doi:10.1016/j.jadohealth.2010.04.006
17. Ganry O, Bernin-Mereau AS, Gignon M, Merlin-Brochard J, Schmit JL. Human papillomavirus vaccines in Picardy, France: coverage and correlation with socioeconomic factors. Rev Epidemiol Sante Publique (2013) 61(5):447–54. doi:10.1016/j.respe.2013.04.005
18. Lutringer-Magnin D, Cropet C, Barone G, Canat G, Kalecinski J, Leocmach Y, et al. HPV vaccination among French girls and women aged 14-23 years and the relationship with their mothers’ uptake of Pap smear screening: a study in general practice. Vaccine (2013) 31(45):5243–9. doi:10.1016/j.vaccine.2013.08.068
19. Blödt S, Holmberg C, Muller-Nordhorn J, Rieckmann N. Human papillomavirus awareness, knowledge and vaccine acceptance: a survey among 18-25 year old male and female vocational school students in Berlin, Germany. Eur J Public Health (2012) 22(6):808–13. doi:10.1093/eurpub/ckr188
20. Fisher H, Audrey S, Mytton JA, Hickman M, Trotter C. Examining inequalities in the uptake of the school-based HPV vaccination program in England: a retrospective cohort study. J Public Health (Oxf) (2014) 36(1):36–45. doi:10.1093/pubmed/fdt042
21. Brabin L, Roberts SA, Stretch R, Baxter D, Chambers G, Kitchener H, et al. Uptake of first two doses of human papillomavirus vaccine by adolescent schoolgirls in Manchester: prospective cohort study. BMJ (2008) 336(7652):1056–8. doi:10.1136/bmj.39541.534109.BE
22. Kumar VM, Whynes DK. Explaining variation in the uptake of HPV vaccination in England. BMC Public Health (2011) 11:172. doi:10.1186/1471-2458-11-172
23. Roberts SA, Brabin L, Stretch R, Baxter D, Elton P, Kitchener H, et al. Human papillomavirus vaccination and social inequality: results from a prospective cohort study. Epidemiol Infect (2011) 139(3):400–5. doi:10.1017/S095026881000066X
24. Spencer AM, Roberts SA, Brabin L, Patnick J, Verma A. Sociodemographic factors predicting mother’s cervical screening and daughter’s HPV vaccination uptake. J Epidemiol Community Health (2014) 68(6):571–7. doi:10.1136/jech-2013-202629
25. Hughes A, Mesher D, White J, Soldan K. Coverage of the English national human papillomavirus (HPV) immunisation program among 12 to 17 year-old females by area-level deprivation score, England, 2008 to 2011. Euro Surveill (2014) 19(2):20677.
26. Sinka K, Kavanagh K, Gordon R, Love J, Potts A, Donaghy M, et al. Achieving high and equitable coverage of adolescent HPV vaccine in Scotland. J Epidemiol Community Health (2014) 68(1):57–63. doi:10.1136/jech-2013-202620
27. Donadiki EM, Jiménez-García R, Hernández-Barrera V, Carrasco-Garrido P, López de Andrés A, Velonakis EG. Human papillomavirus vaccination coverage among Greek higher education female students and predictors of vaccine uptake. Vaccine (2012) 30(49):6967–70. doi:10.1016/j.vaccine.2012.09.028
28. Stöcker P, Dehnert M, Schuster M, Wichmann O, Delere Y. Human papillomavirus vaccine uptake, knowledge and attitude among 10th grade students in Berlin, Germany, 2010. Hum Vaccin Immunother (2013) 9(1):74–82. doi:10.4161/hv.22192
29. Bertaut A, Chavanet P, Aho S, Astruc K, Douvier S, Fournel I. HPV vaccination coverage in French girls attending middle and high schools: a declarative cross sectional study in the department of Côte d’Or. Eur J Obstet Gynecol Reprod Biol (2013) 170(2):526–32. doi:10.1016/j.ejogrb.2013.07.028
30. Spencer (nee Pilkington) AM, Brabin L, Verma A, Roberts SA. Mothers’ screening histories influence daughters’ vaccination uptake: an analysis of linked cervical screening and human papillomavirus vaccination records in the North West of England. Eur J Cancer (2013) 49(6):1264–72. doi:10.1016/j.ejca.2012.12.001
31. Mollers M, Lubbers K, Spoelstra SK, Weijmar-Schultz WC, Daemen T, Westra TA, et al. Equity in human papilloma virus vaccination uptake?: sexual behaviour, knowledge and demographics in a cross-sectional study in (un)vaccinated girls in the Netherlands. BMC Public Health (2014) 14(1):288. doi:10.1186/1471-2458-14-288
32. Steens A, Wielders CCH, Bogaards JA, Boshuizen HC, De Greeff SC, De Melker HE. Association between human papillomavirus vaccine uptake and cervical cancer screening in the Netherlands: implications for future impact on prevention. Int J Cancer (2013) 132(4):932–43. doi:10.1002/ijc.27671
33. Faggiano F, Partanen T, Kogevinas M, Boffetta P. Socioeconomic differences in cancer incidence and mortality. IARC Sci Publ (1997) (138):65–176.
34. Liu T, Wang X, Waterbor JW, Weiss HL, Soong SJ. Relationships between socioeconomic status and race-specific cervical cancer incidence in the United States, 1973–1992. J Health Care Poor Underserved (1998) 9(4):420–32. doi:10.1353/hpu.2010.0482
35. Webb R, Richardson J, Pickles A. A population-based study of primary care predictors of non-attendance for cervical screening. J Med Screen (2004) 11(3):135–40. doi:10.1258/0969141041732166
36. Wallace LA, Bramley JC, Ahmed S, Duff R, Hutchinson SJ, Carman WF, et al. Determinants of universal adolescent hepatitis B vaccine uptake. Arch Dis Child (2004) 89(11):1041–2. doi:10.1136/adc.2003.043687
37. Willoughby BJ, Faulkner K, Stamp EC, Whitaker CJ. A descriptive study of the decline in cervical screening coverage rates in the North East and Yorkshire and the Humber Regions of the UK from 1995 to 2005. J Public Health (2006) 28(4):355–60. doi:10.1093/pubmed/fdl062
38. Wilson TR, Fishbein DB, Ellis PA, Edlavitch SA. The impact of a school entry law on adolescent immunization rates. J Adolesc Health (2005) 37(6):511–6. doi:10.1016/j.jadohealth.2005.07.009
39. Goldstein ST, Cassidy WM, Hodgson W, Mahoney FJ. Factors associated with student participation in a school-based hepatitis B immunization program. J Sch Health (2001) 71(5):184–7. doi:10.1111/j.1746-1561.2001.tb07313.x
40. Tiro JA, Tsui J, Bauer HM, Yamada E, Kobrin S, Breen N. Uptake and correlatos of the human papillomavirus vaccine among adolescents girls and young adult women: an analisis of the 2007 California Health Interview Survey. J Womens Health (Larchmt) (2012) 21(6):656–65. doi:10.1089/jwh.2011.3284
41. Garnett GP, Kim JJ, French K, Goldie SJ. Chapter 21: modelling the impact of HPV vaccines on cervical cancer and screening programs. Vaccine (2006) 24(Suppl 3):178–86. doi:10.1016/j.vaccine.2006.05.116
42. Dempsey A, Zimet GD, Davis R, Koutsky L. Factors that are associated with parental acceptability of human papillomavirus vaccines: a randomized intervention study of written information about HPV. Pediatrics (2006) 117(5):1486–93. doi:10.1542/peds.2005-1381
43. Lau RR, Quadrel MJ, Hartman KA. Development and change of young adults’ preventive health beliefs and behavior: influence from parents and peers. J Health Soc Behav (1990) 31(3):240–59. doi:10.2307/2136890
44. Ogilvie G, Anderson M, Marra F, McNeil S, Pielak K, Dawar M, et al. A population-based evaluation of a publicly funded, school-based HPV vaccine program in British Columbia, Canada: parental factors associated with HPV vaccine receipt. PLoS Med (2010) 7(5):e1000270. doi:10.1371/journal.pmed.1000270
45. Chao C, Slezak JM, Coleman KJ, Jacobsen SJ. Papanicolaou screening behavior in mothers and human papillomavirus vaccine uptake in adolescent girls. Am J Public Health (2009) 99(6):1137–42. doi:10.2105/AJPH.2008.147876
46. Lefevere E, Hens N, Theeten H, Van den Bosch K, Beutels P, De Smet F, et al. Like mother, like daughter? Mother’s history of cervical cancer screening and daughter’s human papillomavirus vaccine uptake in Flanders (Belgium). Vaccine (2011) 29(46):8390–6. doi:10.1016/j.vaccine.2011.08.039
Keywords: human papillomavirus, vaccine, uptake, determinants, Europe, inequalities
Citation: Fernández de Casadevante V, Gil Cuesta J and Cantarero-Arévalo L (2015) Determinants in the uptake of the human papillomavirus vaccine: a systematic review based on European studies. Front. Oncol. 5:141. doi: 10.3389/fonc.2015.00141
Received: 01 April 2015; Accepted: 08 June 2015;
Published: 24 June 2015
Edited by:
Don S. Dizon, Warren Alpert Medical School of Brown University, USAReviewed by:
Miriam Reuschenbach, University Hospital Heidelberg, GermanyCara Mathews, Brown University, USA
Copyright: © 2015 Fernández de Casadevante, Gil Cuesta and Cantarero-Arévalo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Victoria Fernández de Casadevante, Section for Social and Clinical Pharmacy, Department of Pharmacy, Faculty of Health and Medical Sciences, University of Copenhagen, Universitetsparken 2, DK-2100 Copenhagen, Denmark, victoriacasadevante@yahoo.es