Early incident and subsyndromal delirium in older patients undergoing elective surgical procedures: a randomized clinical trial of an avoid delirium protocol
 Alisha Sachdev1 Yabtsega Moges1
Alisha Sachdev1 Yabtsega Moges1  Micah Rubin1 Amanda C. Sremac1 Zoe Arvanitakis2
Micah Rubin1 Amanda C. Sremac1 Zoe Arvanitakis2  Robert J. McCarthy1*
Robert J. McCarthy1*
- 1Department of Anesthesiology, Rush University Medical Center, Chicago, IL, United States
- 2Rush Alzheimer’s Disease Center, Rush University Medical Center, Chicago, IL, United States
Background: Pharmacological avoidance guidelines for preventing delirium have been suggested; however, there are limited pragmatic studies of these strategies. Early (<24 h) delirium can be observed in the postoperative care unit and is associated with an increased risk of subsequent delirium. We examined the effectiveness of an avoid delirium protocol (ADP) in older (>65 years) patients undergoing elective surgeries.
Methods: The randomized controlled trial assessed an ADP developed using the American Geriatric Society's Clinical Practice Guidelines for Postoperative Delirium in Older Adults, on early (<24 h) incident or subsyndromal delirium. Delirium was assessed using the confusion assessment method before surgery, in the post-anesthesia care unit, and on postoperative day 1. The primary outcome of early delirium was the combined incidence of incident or subsyndromal delirium.
Results: Early delirium was identified in 24/235 patients (10.2%) with a risk ratio of 1.27 (95% CI 0.59–2.73, P = 0.667) for patients randomized to the ADP. In cases with protocol adherence and no benzodiazepine use, early delirium was present in 10/73 (13.7%) compared to 14/148 (9.5%) in non-adherent cases [risk ratio 1.45 (95% CI 0.57–3.10, P = 0.362)]. Lower American Society of Anesthesiologists physical class [odds ratio 3.31 (95% CI 1.35–8.92, P = 0.008)] and an inpatient admission [odds ratio 2.67 (95% CI 1.55–4.87, P = 0.0002)] were associated with early delirium.
Conclusions: Our findings suggest that pharmacological avoidance protocols limiting or avoiding the use of specific classes of medications are not effective in reducing early incident or subsyndromal delirium in older patients undergoing elective surgery.
Introduction
Postoperative delirium (POD) presents acutely with confusion, disorientation, perceptual disturbances, emotional dysregulation, or sleep disturbances, manifesting within a few hours and peaking at 72 h following a surgical procedure (1). POD can be subdivided into three types, emergence, early, and late. Emergence delirium occurs during or immediately after emergence from general anesthesia, is associated with further episodes of delirium during hospitalization, and is reported to occur in up to 37.5% of older patients (2). Early delirium, within 24 h of surgery, frequently occurs in the post-anesthesia care unit (PACU) and is often associated with drugs administered intraoperatively (3). Assessments for early delirium can be successfully performed in the PACU using the confusion assessment method (CAM) after the patient reaches an Aldrete score of ≥9 (also known as the Post Anesthesia Recovery Score) (4). Early delirium in older patients has been reported to occur in up to 45% of patients receiving general anesthesia and is also associated with an increased risk for subsequent delirium during hospitalization (5). Late delirium can occur generally between postoperative days 2–5, and benzodiazepine drugs given in the postoperative period have been shown to increase the odds of its occurrence (6).
Subsyndromal delirium, defined as the presence of one or more of the core symptoms of delirium without reaching the threshold for a diagnosis of delirium, may represent a threshold state intermediate in severity between delirium and no delirium (7). Subsyndromal delirium shares similar risk factors with other forms of POD (8). The combined incidence of incident delirium and subsyndromal delirium in older patients using the CAM assessment has been reported to be between 19% and 54% following surgery in patients ≥65 years (9, 10).
Pharmacological and non-pharmacological interventions have been recommended to reduce the incidence of POD (11). Nevertheless, there are limited pragmatic effectiveness studies of these strategies (12). Non-pharmacological interventions that have been suggested include education and enriching the environment by adequately addressing needs of older adults, including vision and hearing aid availability, adequate pain control, and improved communication (13). Pharmacological classes that are recommended to be avoided include drugs with anticholinergic properties, corticosteroids, meperidine, sedative hypnotics, and polypharmacy (defined as ≥5 new medications) (14–16). Based on published guidelines from the American Geriatrics Society on avoidance of delirium in older patients, we developed an avoid delirium protocol (ADP) for use in the perioperative period (Figure 1). We hypothesized that the ADP would reduce the combined occurrence of early incident and subsyndromal delirium in older adult patients undergoing elective surgical procedures.
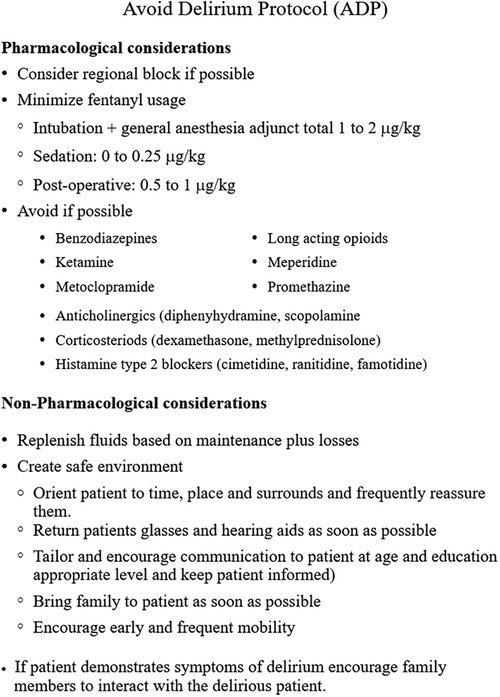
Figure 1. Avoid delirium protocol. Consort flow diagram. Based on the guidelines of the American Geriatrics Society Expert Panel on Postoperative Delirium in older adults.
Methods
This study was approved by the Institutional Review Board of Rush University (15062301-IRB01) and registered on ClinicalTrials.gov (NCT 03541408, registration date 30 May 2018). This manuscript was prepared following CONSORT guidelines. The study was a randomized, controlled clinical trial of adults (>65 years) who underwent elective surgery between 1 May 2016 and 21 August 2020. Recruitment did not occur in March and April 2020 due to COVID restrictions. The intervention was the ADP developed for the prevention of delirium in older patients (11).
Eligible patients were scheduled to undergo an elective surgical procedure, ≥65 years of age, English speaking, and willing to comply with study activities. Patients currently in the hospital, undergoing cardiac surgery with bypass, open thoracotomy, neurosurgery, or with a history of stroke, psychiatric illness, or a diagnosis of dementia were excluded. Patients were identified 1–2 weeks prior to surgery and screened for eligibility. Patients were contacted by research personnel who explained the research protocol and obtained verbal consent to meet with the patient on the day of their procedure.
At the hospital, research personnel explained the study to eligible patients, who were given the consent form, allowed to review it, and ask questions regarding the study. Willing patients provided written informed consent. Following consent, subjects were randomized into either the ADP or standard of care arm by opening a sealed envelope containing the group allocation. Randomization was performed in blocks of 10 by a statistician not involved in the study using the SAS Proc Plan procedure assuming an equal probability group assignment.
Subjects were then assessed using the confusion assessment method for the intensive care unit (CAM-ICU) to ensure a negative test (no delirium) prior to surgery. They were also evaluated for cognitive function using the Mini Mental Status Examination (MMSE) (17). The MMSE tests cognitive function by examining orientation (10 points), registration (3 points), word recall (3 points), attention and calculation (5 points) language abilities (8 points), and visuospatial activity (1 point). A cutoff value of 24 or lower, out of a maximum of 30 points, was used to identify an abnormal test performance (18). Scores of the MMSE were not revealed to the subjects. Subjects with cognitive impairment (MMSE ≤24) were excluded from follow-up evaluations and data analysis. Study personnel then contacted and revealed the study group to the patient's clinical care team. In addition, if the subject was randomized to the ADP group, a copy of the ADP protocol was sent to the care team.
The research team performing the MMSE and CAM-ICU scoring consisted of a physician (YM), and research assistants (MR and ACS) who were trained and supervised by a critical care anesthesiologist (AS) and a neurologist (ZA). Training included lectures, handouts, literature and videos, and one-to-one instruction at the bedside. The critical care anesthesiologist was contacted by research staff to discuss any cases where a clear assignment based on the scoring could not be obtained.
Subjects were also questioned regarding their work status and risk factors for delirium including: a history of delirium, functional independence, mobility devices used, history of falls, visual and/or hearing aid use, and physical trauma history. Comorbidities including renal and liver disease, history of depression, and number of current home medications were recorded. Hydration status was assessed by the clinical care team using clinical signs, capillary refill, skin turgor, and by examining the blood urea nitrogen and creatinine ratio. Research personnel recorded the status as hydrated or dehydrated in consultation with the clinical care team.
When the patient was transferred to the PACU, the research team was notified when the patient had achieved an Aldrete score of ≥9. The time from arrival to the recovery room until the first postoperative evaluation was recorded. The research evaluator determined the patient's level of sedation using the Richmond Agitation and Sedation Score (RAAS). The RAAS scores are assessed on a 10-point scale from −5 to +4. Negative scores represent sedation, where −1 is drowsy and −5 is unarousable. A score of 0 is given for a calm and alert state (good recovery), positive +1 for restlessness, +2 and +3 for increasing agitation, and +4 for combative behavior (19). Subjects were required to have an RASS of −3 through +3 prior to delirium evaluation. The researcher also assessed the patient's level of pain using the Numeric Pain Rating (NRS) scale, where 0 equals no pain and 10 equals the worst pain imaginable.
Delirium was then assessed using the CAM-ICU scoring system (20). The CAM-ICU was considered positive (delirium present) if the patient demonstrated an acute change in mental status or a fluctuation in mental status and inattention, plus either altered consciousness or disorganized thinking. Subsyndromal delirium was considered present if the subject displayed any of the CAM-ICU features but did not fulfill the diagnostic criteria for delirium. If no CAM-ICU features were present, the patient was considered to have no delirium. Patients who exhibited subsyndromal or incident delirium were assessed at least twice over the next 24 h using the RAAS scale so that the motoric subtype of delirium could be determined (21). At 24 h following surgery, subjects were again contracted either in person or via telephone by the researcher, to repeat the assessments. They also spoke with the subject's companion or care giver regarding their impression of the subject's health and mental status. They then asked the subject to rate their first night after surgery sleep on a scale of 0–10 where 0 was extremely not restful and 10 was extremely restful.
Data extracted from the medical record included age, sex, race, ethnicity, American Society of Anesthesiology Physical Status, medical history, surgical procedure, and admission status. Medications administered during and after surgery (up until discharge), duration of the surgery, total fluids administered intraoperatively, the presence, and duration of any hypotensive episodes (decrease in systolic blood pressure ≥30% of baseline). Intraoperative and recovery room opioids were converted to intravenous morphine equivalents (MME) (22).
Adherence to the ADP was assessed for all patients regardless of randomization group, by comparing medication administration in the medical record with the ADP and examining institutional enhanced recovery from anesthesia and surgery (ERAS) guidelines. Intraoperative administration of a benzodiazepine, meperidine, or morphine was considered a protocol violation, as was exceeding the recommended intubation and general anesthesia fentanyl doses. The use of corticosteroids, ketamine, anticholinergics, and histamine type 2 blockers were not considered protocol violations, when administered in accordance with ERAS guidelines for the specific surgical procedure. The subjects were classified as either protocol compliant or non-compliant.
Statistical analysis
The primary outcome of the study was the occurrence of early delirium defined as CAM-ICU-assessed incident delirium or subsyndromal delirium in the first 24 h following surgery. The proportion of subjects demonstrating early delirium was compared between the ADP and control group by an intent-to-treat analysis, using a two-sided proportions test. As a sensitivity analysis, early delirium was compared between protocol compliant and non-compliant groups using the two-sided proportions test. Risk ratios and 95% confidence intervals were calculated using maximum likelihood estimations. Imbalances in subject characteristics, risk factors for delirium, admission, and surgery type between randomized groups and between protocol compliant and non-compliant groups were assessed by determining standardized difference (Hedges G for continuous data, and Cliff's delta for ordinal and nominal data). Differences in operative and anesthesia data between groups were assessed using a chi-squared analysis for counts and the Mann–Whitney test for continuous data.
Secondary outcomes were times from PACU admission, from last drug administration of an agent ADP protocol, NRS pain score, and RAAS assessments at the time of CAM assessment. The motoric state of subjects that exhibited subsyndromal or incident delirium at 24 h was also compared. Times and pain scores were compared among groups using the Kruskal–Wallis H-test and RAAS scores using a chi-squared test.
An exploratory analysis was performed to assess risk factors for early delirium. Univariable differences in risk factors in subjects without delirium with those who had incident or subsyndromal delirium were compared using a chi-squared statistic for counts and the Mann–Whitney U-test for continuous data. Differences in binominal proportions and 95% confidence intervals were computed using the Clopper–Pearson method. Differences in medians and 95% confidence interval were determined using bootstrapping. Effect sizes of significant univariable binominal factors with early delirium are expressed as risk ratios and 95% CI determined using the Wald method. The effect size for continuous risk factors (intraoperative MME values, duration of surgery, intraoperative fluids, and postoperative pain in the first hour in the PACU) was determined for a random pair of values from a delirium subject from a no delirium subject as the Wilcoxon–Mann–Whitney odds and 95% CI.
A multi-variable adjusted estimate of the odds of early delirium was made using a logistic regression model using Firth's bias reduction method. Firth and log-F-type penalized methods have been demonstrated to perform well in data with low prevalence outcomes without overfitting (23, 24). Variables that demonstrated a P < 0.2 on univariable analysis were entered into the model. The dependent variable was the presence or absence of incident or subsyndromal delirium. Independent variables entered the model were age; ASA physical status; visual impairment; functional dependence; admission type; type of surgery; type of anesthesia; administration of an opioid, dexamethasone, ondansetron, or midazolam; total intraoperative MME; total intraoperative i.v. fluids; estimated blood loss; duration of surgery; and NRS pain in the first hour in the PACU. Multicollinearity of the independent variables was assessed by evaluating the variance inflation factor (VIF) and the condition index (25). Variables exhibiting a VIF >5 were excluded from the analysis. A backward elimination with a significance level of 0.05 to stay in the model was performed to identify a parsimonious model with minimization of the Akaike information criteria (AIC0). Odds ratios are expressed as the exponent of beta with 95% confidence intervals of the estimates determined by penalized profile likelihood method (R package logistf).
Statistical analysis was performed using RStudio version 2023.06.1 build 524 (Posix Software, PBC, Boston, MA, USA; URL: http://www.posix.com/) and R version 4.3.1, release date 16 June 2023 (The R Foundation for Statistical Computing, Vienna, Austria).
We used published data to estimate the sample size, power, and other numbers needed for this study. In a study by Sharma et al. using methods similar to those used in this study, early delirium was detected in 44% of patients in the PACU following hip fracture repair (3). In contrast, Kanno et al. detected a combined incidence of early incident and subsyndromal delirium of 19% in a study of a mixed surgical population on the surgical ward soon after surgery (10). We assumed a conservative estimate of 25% of subjects would have incident or subsyndromal delirium and since no prior study has tested a comprehensive ADP, we estimated that a clinically important reduction in early delirium would be an absolute reduction by 10%. Group sample sizes of 250 per group would achieve 80% power to detect a difference of 10% in the proportion using a two-side z-test at an alpha of 0.05. We planned to enroll 530 subjects to account for subjects lost to exclusion following randomization. At approximately the midpoint of the study (n = 263), the observed rate of combined incident and subsyndromal delirium was 10.2% and a conditional power analysis with calculation of the futility index was undertaken (26). Sample size and power calculation were made using PASS 2008, release date 27 January 2011 [Power Analysis and Sample Size Software (2008). NCSS, LLC. Kaysville, UT, USA; ncss.com/software/pass].
Results
The flow of subjects in the study is shown in Figure 2. Of the 263/876 (31%) subjects consented, 28 were excluded following informed consent, 17 subjects withdrew consent, and 11 had cancelation or rescheduling of their procedure. Two hundred thirty-five subjects had their surgical procedure as scheduled, completed follow-up, and were included in the analysis. All subjects scored above 24 on the MMSE at screening, and no subject tested positive for incident or subsyndromal delirium pre-operatively.
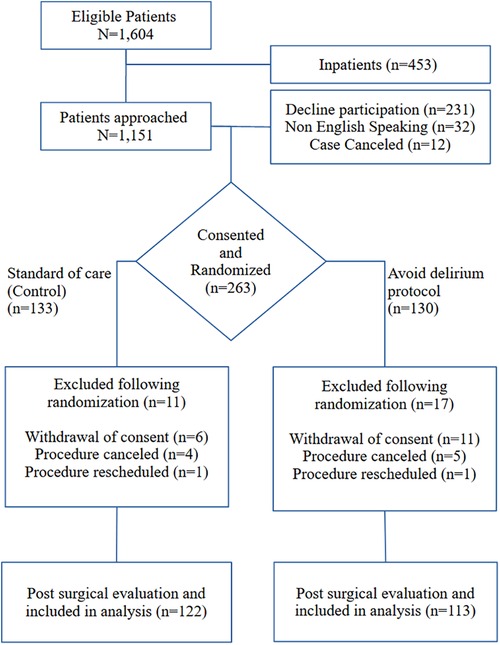
Figure 2. Consort flow diagram.
Patient characteristics, risk factors, and types of surgery between the intent-to-treat as well as the per-protocol groups are shown in Table 1. Groups were well balanced with standardized differences <0.2 for all variables except for body mass index (BMI), and <0.1 for variables except work status, MMSE, and dehydration in the ADP and control groups. In the per-protocol groups, all variables had standardized differences <0.1 except for BMI and function dependence. Operative and anesthesia data between the intent-to-treat and per protocol groups are shown in Table 2. Dexamethasone and midazolam use was greater in the control group in both the intent-to-treat and per-protocol groups. Intraoperative MME use was greater in the intent-to-treat ADP group and the dose of vasopressor equivalents per kilogram was greater in the protocol adherent group compared to the non-protocol adherent control group.
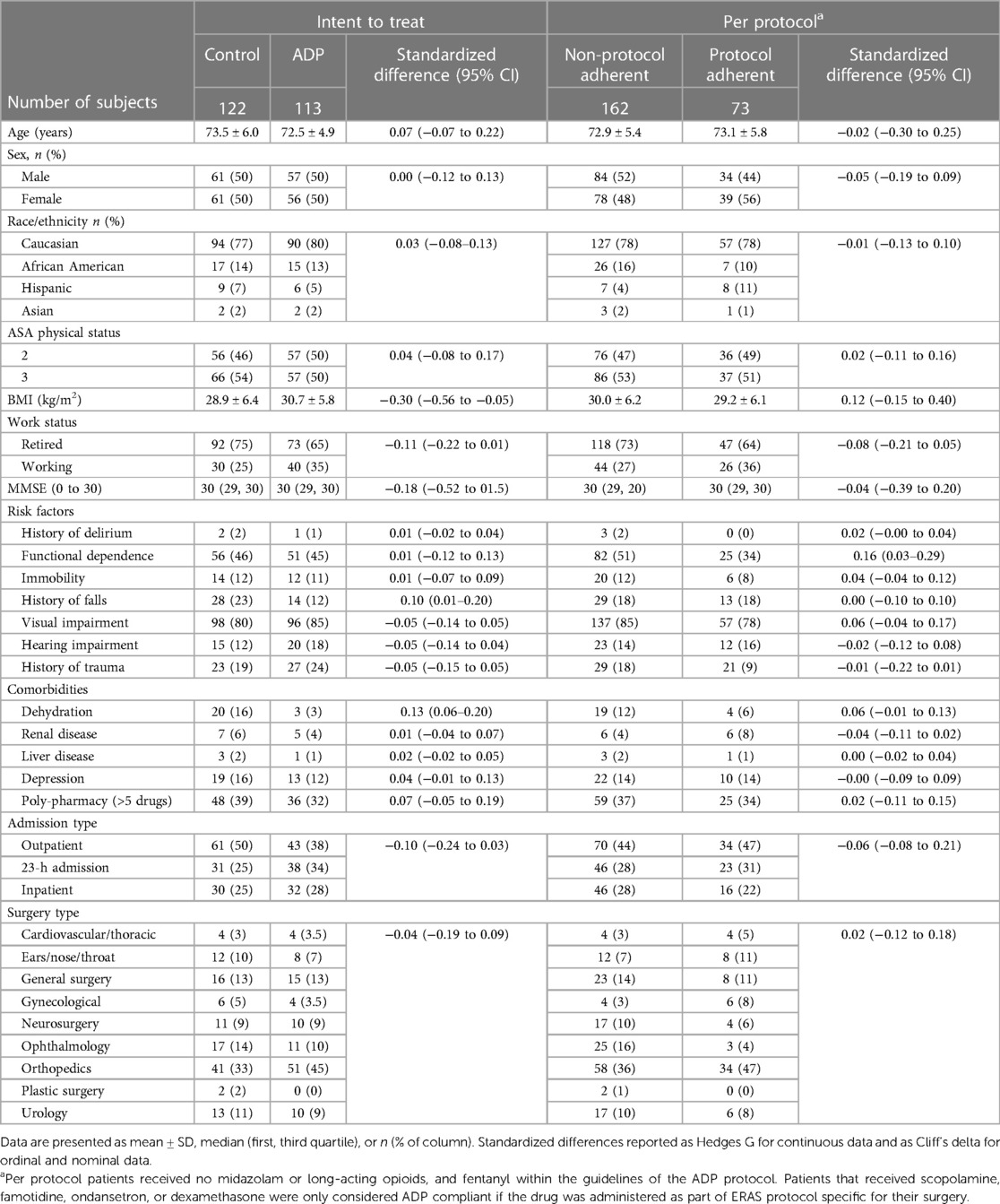
Table 1. Patient characteristics, risk factors, admission, and surgery type between patients randomized to the ADP and standard of care (control) groups, as well as the protocol compliant and non-compliant groups.
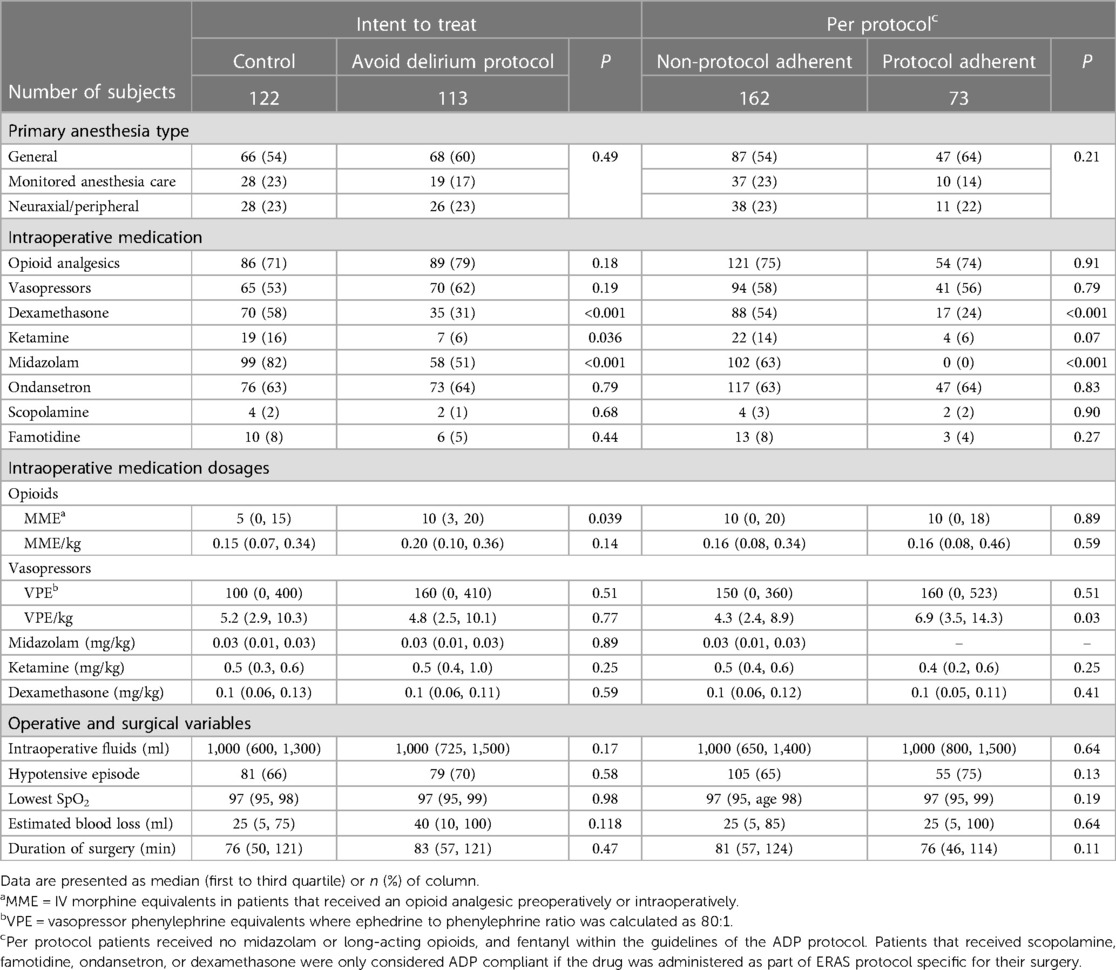
Table 2. Operative and anesthesia data comparison between randomized no-delirium protocol and standard of care control groups.
The results of the delirium assessments in the first 24 h following surgery are shown in Table 3. In the PACU, incident delirium was identified in 6/235 (2.5%), and subsyndromal delirium was in 17/235 (7.2%) subjects. Over the 24-h period, 8/235 (3.4%) had incident delirium and 16/235 (6.8%) had subsyndromal delirium for an overall incidence of early delirium of 24/235 (10.2%). The median (first, third quartile) time from PACU admission to CAM assessment in subjects without delirium was 84 (53, 129) min and was increased by 24.5 (95% CI 5–43, P = 0.002) min in patients with early delirium. Early delirium patients primarily displayed a hypoactive motoric state in the first 24 h.
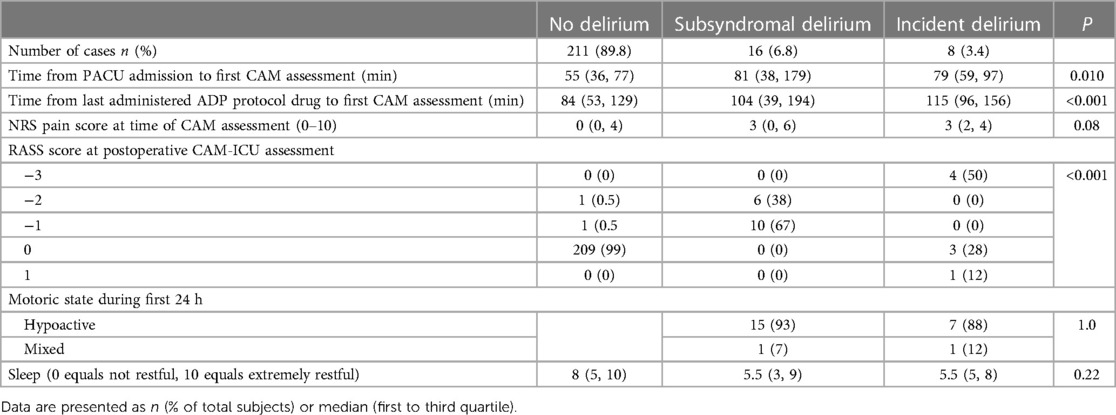
Table 3. Results of delirium assessments in first 24 h following surgery.
The incidence of early delirium was 13/113 (11.5%) in patients randomized to the ADP protocol, and 11/122 (9.0%) in those randomized to standard of care, with a risk ratio of 1.27 (95% CI 0.59–2.73, P = 0.667). In cases identified as protocol adherent, early delirium was present in 10/73 (13.7%) compared to 14/148 (9.5%) in subjects identified as not protocol adherent, with a risk ratio of 1.45 (95% CI 0.57–3.10, P = 0.362). Based on these findings the study was terminated at the 50% recruitment point, because using the estimated difference of 10% for the incidence early delirium in patient randomized to ADP, the probability of the study demonstrating a favorable outcome for the ADP with continuation to the intended sample of 500 was P < 0.0001 and the futility index was 1.0.
Univariable associations of subject characteristics, and operative and anesthesia factors with postoperative delirium, are shown in Table 4. Univariable differences in risk of early delirium were found for ASA class ≤2 compared with ASA class ≥3, general anesthesia compared with monitored anesthesia care or regional anesthesia, an inpatient admission compared with outpatient or 23-h stay, greater intraoperative MME use, greater intraoperative fluid administration; longer duration of surgery, and greater pain in the first hour in the PACU. Multivariable Firth logistic regression identified ASA class ≤2, odds ratio 3.31 (95% CI 1.35–8.92, P = 0.008) and an inpatient admission, odds ratio 2.67 (95% CI 1.55–4.87, P = 0.0002) as significant multivariable predicators of early delirium. Performance metrics of the parsimonious Firth model are likelihood ratio test = 18.76, df = 2, P < 0.001, AIC = 22.7, AUC = 0.76 (05% CI 0.68–0.84), and Brier score 0.08.
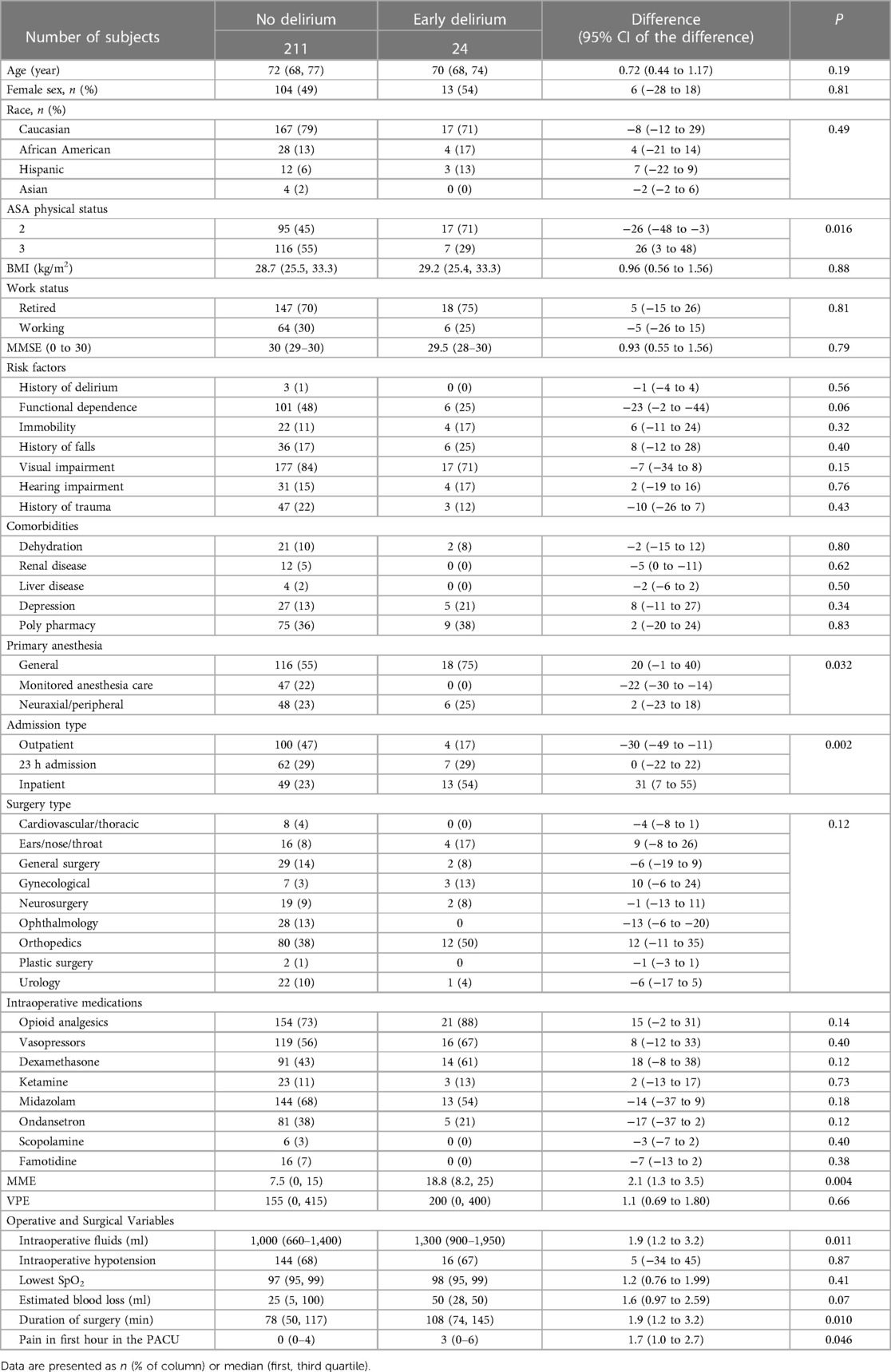
Table 4. Univariable comparisons of subject characteristic, operative, and anesthesia factors in subjects with and without early (<24 h) delirium.
Postoperative nausea and vomiting requiring treatment in the PACU occurred in 7/210 (3.3%) no delirium and 4/24 (16.7%) early delirium subjects, risk ratio 5.0 (95% CI 1.5–15.8, P = 0.017). Median (first, third quartile) MME received in the post-anesthesia care unit was 1.7 (0–6.7) MME in the no delirium subjects, and 5.8 (0–12.7) MME in the early delirium subjects, difference of 4.1 MME, 95% CI −1 MME to 8.6 MME, P = 0.048. Median (first, third quartile) duration of stay in hours was 20.8 (2.1–30.5) in the no delirium subjects, and 46.9 (23.7–64.5) in the early delirium patients, difference 26.2 h, 95% CI 4.2 to 44.9 h, P < 0.001. Median (first to third quartile) rating of sleep quality on the first postoperative night was 8 (5–10) in the no delirium subjects and 5.5 (3–9) in the early delirium subjects, difference −2.5 (95% CI −3 to 0, P = 0.081).
Discussion
The important finding of this study was the lack of efficacy of perioperative avoid delirium protocol based on minimizing or avoiding intraoperative drugs that have been associated with an increased in the risk of delirium. Despite a large body of evidence supporting various risk factors for developing postoperative delirium, no pragmatic studies exist to guide anesthetic management to attempt to prevent early delirium. Our study protocol was designed to minimize the use of agents that have been associated with postoperative delirium, including benzodiazepines, ketamine, and steroids. The protocol also incorporated non-pharmacological factors. Given that delirium can occur in patients with none of the known risk factors (27), the lack of effect of such a protocol has substantial clinical importance.
Prior studies excluding a single pharmacological class such an anticholinergic agent have not shown significant reduction in the incidence of delirium (28). Protocols involving non-pharmacological interventions including early mobilization, nutritional assistance, and cognitive exercises have demonstrated reduced delirium following gastrointestinal surgery, whereas non-pharmacological interventions coupled with a scheduled pain protocol reduced the duration of delirium but not the incidence in hip fracture patients (29, 30). Taken together, there is insufficient evidence to suggest that any single approach will benefit all patients in the intraoperative period, but rather judicious use of pharmacological agents coupled with non-pharmacological interventions is likely the best clinical approach.
We observed an incidence of early delirium (incident and subsyndromal) of (10.2%) older (≥65 years) subjects undergoing elective surgical procedures. The risk of early delirium was increased in patients with ASA score ≤2 compared with ASA score ≥3 and patients with hospital admission after surgery in our multi-variable analysis. Although univariable analysis found increased odds of receiving greater intraoperative opioid MMEs, more intravenous fluids, a longer duration of surgery, and greater pain in the first hour in the PACU compared with patient without delirium, these variables were not significant on multi-variable analysis. The lack of inclusion of these factors in the multi-variable analysis may reflect the small study sample size as well as the large number of factors that increase susceptibility to delirium. Early delirium subjects had an increased risk of nausea and vomiting in the recovery room, received more analgesia in the PACU, and had a longer duration of hospitalization. Our avoid delirium protocol, as designed, was not shown to be superior to the control arm using intent-to-treat or in our sensitivity per protocol analysis.
Prior studies have evaluated the incidence of early delirium and have reported an incidence between 11% and 45% (3, 5). Sharma et al. reported an incidence of 45% for early delirium in the recovery room following hip fracture surgery in patients aged 56–98 years, receiving general anesthesia using the CAM algorithm (3, 31). Radtke et al. reported an incidence of early delirium of 11% in adults (age >18) using the Nursing Delirium Screening Scale (Nu-DESC) in 862 subjects in the recovery room following elective general anesthesia (32). Neufeld et al. used physician raters who evaluated each patient using the Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV criteria and observed a rate of early delirium of 45% (4). When compared in recovery room patients, the CAM-ICU method demonstrated equal specificity but less sensitive than the Nu-DESC or DSM-IV methods (33, 34).
Multiple studies have explored the potential risk factors for early delirium, occurring in the first 24 h after surgery. These risk factors can be broadly separated in two categories, predisposing risk factors and triggers that initiate the event (35). In addition to age >65, predisposing factors include clinical comorbidities, frailty, depression, functional disabilities, surgical risk, and preoperative cognitive dysfunction (36). We assessed preoperative cognitive status using the MMSE, but no subjects scored less than an MMSE score of 24 and there were only 2% of subjects with a value of <27, which has been suggested to be a cutoff value for mild cognitive impairment (37).
Types of surgery, surgical approach, and anesthesia have also been evaluated as risk factors associated with early delirium. Low operative stress procedures such as cataracts have a reported incidence of early delirium around 4%, whereas following high operative stress procedures such as vascular and cardiac surgery report incidences between 45% and 50% (38). We observed the highest incidence of early delirium (30%) in women undergoing gynecological procedures; however, there were only 10 cases in our study. In a study of postoperative delirium in older (>60 years) women (n = 103) undergoing surgery for suspected gynecologic malignancies, an incidence of delirium of 17.5% was observed (39). In the study, increased opioid administration, age, and preoperative medications were also associated with an increase in postoperative delirium. Surgical approach may also be an influencing factor, however, the study concluded that choice of anesthetic, general vs. regional, was more likely responsible for early delirium (40).
General anesthesia has been demonstrated to increase the risk of postoperative delirium compared with regional anesthesia (41). Anesthesia depth also has been demonstrated to impact the incidence of delirium, with lighter depth of general anesthesia reducing the incidence of delirium by 9% (odds ratio 0.58, 95% CI 0.38–0.88) (42). The use of regional anesthesia, an opioid reducing strategy, early mobilization, and the use of ERAS protocol were credited by Chew et al. for an incidence of delirium of 0% following 462 elective total joint surgeries at a single center (43). In the current study, 23% of surgeries were performed under regional anesthesia, more than 50% of the remaining procedures involved a regional anesthetic block as part of the perioperative management, and 67% of the uses of a restricted agent involved an ERAS protocol.
Preoperative fluid status and intraoperative factors such as hypotension and low cerebral oximetry values have been evaluated. Radtke et al. demonstrated that perioperative fluid fasting and choice of intraoperative opioid use may be modifiable risk factors for early postoperative delirium (28). Intraoperative hypotension has been associated with higher odds of postoperative delirium in critically ill patients (44). There is also evidence that blood pressure fluctuation, not hypotension or hypertension alone, may also be predictive of postoperative delirium (45). A meta-analysis of cerebral oximetry monitoring during surgery demonstrated a positive impact on postoperative neurocognitive function but not on delirium or postoperative stroke (46). We did not observe an association between preoperative dehydration or intraoperative hypotension >30% of baseline with early delirium.
The results of our study should only be interpreted in the context of its limitations. Our sample size was small, the study was performed at a single institution, and we terminated the study early because we observed statistical futility in changing our finding from the null hypothesis at the 50% accrual point. The small sample size also limits the certainty of our associations of the risk factors with the occurrence of delirium. We limited the surgical procedures to elective procedures of limited complexity and short duration because we primarily wanted to evaluate patients that are discharged soon after surgery and need to be ready for discharge quickly. The addition of longer and more complex procedures may have impacted our findings with respect to the incidence and risk factors associated with early delirium. We did not use intraoperative electroencephalography monitoring, so we cannot comment on the role of anesthesia depth on the occurrence of delirium.
We used the CAM-ICU method for detection of delirium in the recovery room. The CAM-ICU was originally developed for non-verbal patients in the intensive care unit, but due to its brevity and simplicity, the CAM-ICU is increasingly being used for detecting delirium in verbal patients outside the ICU setting (47). Nevertheless, the CAM-ICU method is less sensitive than the Nu-DESC and the 3D-CAM in verbal patients, and this may have contributed to an underestimation of the incidence of early delirium (32–34, 47).
We used the MMSE to assess cognitive function prior to surgery because it is easier to administer in the preoperative area than the Montreal Cognitive Assessment (MoCA); however, the MoCA is more sensitive to mild cognitive impairment (MCI), which may have allowed us to detect an effect of MCI in our cohort. Although our groups were generally balanced with respect to risk factors for delirium, adherence to ERAS regimens created many protocol violations that substantially reduced the number of subjects that had protocol adherence (29%). Because of the multidepartment nature of ERAS, implementation of avoidance protocols such as the ADP can be challenging, especially when ERAS adherence is an institutional metric.
In conclusion, the use of avoid pharmacological agents that have been associated with delirium coupled with non-pharmacologic patient centric care did not decrease the incidence of early delirium within the first 24 h following surgery. Our findings suggest that avoidance protocols are not likely superior to judicious use of pharmacological agents coupled with non-pharmacological interventions for minimizing early delirium.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Rush University Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AS: Conceptualization, Investigation, Project administration, Supervision, Writing – original draft. YM: Investigation, Writing – review & editing. MR: Investigation, Writing – review & editing. ACS: Investigation, Supervision, Writing – review & editing. ZA: Supervision, Writing – original draft, Writing – review & editing. RM: Conceptualization, Data curation, Formal Analysis, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article.
The study was funded by Department of Anesthesiology funds. ZA was supported by NIH grants R01NS084965 and RF1AG059621.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Liu B, Huang D, Guo Y, Sun X, Chen C, Zhai Z, et al. Recent advances and perspectives of postoperative neurological disorders in the elderly surgical patients. CNS Neurosci Ther. (2022) 28:470–83. doi: 10.1111/cns.13763
2. Zhang Y, He ST, Nie B, Li XY, Wang DX. Emergence delirium is associated with increased postoperative delirium in elderly: a prospective observational study. J Anesth. (2020) 34:675–87. doi: 10.1007/s00540-020-02805-8
3. Sharma PT, Sieber FE, Zakriya KJ, Pauldine RW, Gerold KB, Hang J, et al. Recovery room delirium predicts postoperative delirium after hip-fracture repair. Anesth Analg. (2005) 101:1215–20. doi: 10.1213/01.ane.0000167383.44984.e5
4. Neufeld KJ, Leoutsakos JM, Sieber FE, Wanamaker BL, Gibson Chambers JJ, Rao V, et al. Outcomes of early delirium diagnosis after general anesthesia in the elderly. Anesth Analg. (2013) 117:471–8. doi: 10.1213/ANE.0b013e3182973650
5. Choi Y, Kim D, Kim T, Lim T, Kim S, Yoo J. Early postoperative delirium after hemiarthroplasty in elderly patients aged over 70 years with displaced femoral neck fracture. Clin Interv Aging. (2017) 12:1835–42. doi: 10.2147/CIA.S147585
6. Duprey MS, Devlin JW, Griffith JL, Travison TG, Briesacher BA, Jones R, et al. Association between perioperative medication use and postoperative delirium and cognition in older adults undergoing elective noncardiac surgery. Anesth Analg. (2022) 134:1154–63. doi: 10.1213/ANE.0000000000005959
7. Sepulveda E, Leonard M, Franco JG, Adamis D, McCarthy G, Dunne C, et al. Subsyndromal delirium compared with delirium, dementia, and subjects without delirium or dementia in elderly general hospital admissions and nursing home residents. Alzheimers Dement (Amst). (2016) 7:1–10. doi: 10.1016/j.dadm.2016.11.002
8. Denny DL, Lindseth G. Preoperative risk factors for subsyndromal delirium in older adults who undergo joint replacement surgery. Orthop Nurs. (2017) 36:402–11. doi: 10.1097/NOR.0000000000000401
9. Shim J, DePalma G, Sands LP, Leung JM. Prognostic significance of postoperative subsyndromal delirium. Psychosomatics. (2015) 56:644–51. doi: 10.1016/j.psym.2015.05.002
10. Kanno M, Doi M, Kubota K, Kanoya Y. Risk factors for postoperative delirium and subsyndromal delirium in older patients in the surgical ward: a prospective observational study. PLoS One. (2021) 16:e0255607. doi: 10.1371/journal.pone.0255607
11. American Geriatrics Society Expert Panel on Postoperative Delirium in Older Adults. American Geriatrics Society abstracted clinical practice guideline for postoperative delirium in older adults. J Am Geriatr Soc. (2015) 63:142–50. doi: 10.1111/jgs.13281
12. Swarbrick CJ, Partridge JSL. Evidence-based strategies to reduce the incidence of postoperative delirium: a narrative review. Anaesthesia. (2022) 77:92–101. doi: 10.1111/anae.15607
13. Borozdina A, Qeva E, Cinicola M, Bilotta F. Perioperative cognitive evaluation. Curr Opin Anaesthesiol. (2018) 31:756–61. doi: 10.1097/ACO.0000000000000658
14. Kassie GM, Nguyen TA, Kalisch Ellett LM, Pratt NL, Roughead EE. Preoperative medication use and postoperative delirium: a systematic review. BMC Geriatr. (2017) 17:298. doi: 10.1186/s12877-017-0695-x
15. Kurisu K, Miyabe D, Furukawa Y, Shibayama O, Yoshiuchi K. Association between polypharmacy and the persistence of delirium: a retrospective cohort study. Biopsychosoc Med. (2020) 14:25. doi: 10.1186/s13030-020-00199-3
16. Hein C, Forgues A, Piau A, Sommet A, Vellas B, Nourhashémi F. Impact of polypharmacy on occurrence of delirium in elderly emergency patients. J Am Med Dir Assoc. (2014) 15:850.e11–5. doi: 10.1016/j.jamda.2014.08.012
17. Folstein MF, Folstein SE, McHugh PR. Mini-mental state. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
18. Crum RM, Anthony JC, Bassett SS, Folstein MF. Population-based norms for the mini-mental state examination by age and educational level. JAMA. (1993) 269:2386–91. doi: 10.1001/jama.1993.03500180078038
19. Sessler CN, Gosnell MS, Grap MJ, Brophy GM, O'Neal PV, Keane KA, et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. (2002) 166:1338–44. doi: 10.1164/rccm.2107138
20. Brummel NE, Boehm LM, Girard TD, Pandharipande PP, Jackson JC, Hughes CG, et al. Subsyndromal delirium and institutionalization among patients with critical illness. Am J Crit Care. (2017) 26:447–55. doi: 10.4037/ajcc2017263
21. Peterson JF, Pun BT, Dittus RS, Thomason JW, Jackson JC, Shintani AK, et al. Delirium and its motoric subtypes: a study of 614 critically ill patients. J Am Geriatr Soc. (2006) 54:479–84. doi: 10.1111/j.1532-5415.2005.00621.x
22. Broglio K, Portenoy RK. Approximate dose conversions for commonly used opioids. Available at: https://www.uptodate.com/contents/image?imageKey=PALC%2F111216 (Accessed June 13, 2023).
23. Rahman MS, Sultana M. Performance of Firth-and logF-type penalized methods in risk prediction for small or sparse binary data. BMC Med Res Methodol. (2017) 17:33. doi: 10.1186/s12874-017-0313-9
24. Guan Y, Fu G-H. A double-penalized estimator to combat separation and multicollinearity in logistic regression. Mathematics. (2022) 10:3824. doi: 10.3390/math10203824
25. Bayman EO, Dexter F. Multicollinearity in logistic regression models. Anesth Analg. (2021) 133:362–5. doi: 10.1213/ANE.0000000000005593
26. Ware JH, Muller JE, Braunwald E. The futility index. An approach to the cost-effective termination of randomized clinical trials. Am J Med. (1985) 78:635–43. doi: 10.1016/0002-9343(85)90407-3
27. Saporito A, Sturini E. Incidence of postoperative delirium is high even in a population without known risk factors. J Anesth. (2014) 28:198–201. doi: 10.1007/s00540-013-1706-5
28. Marcantonio ER. Postoperative delirium: a 76-year-old woman with delirium following surgery. JAMA. (2012) 308:73–81. doi: 10.1001/jama.2012.6857
29. Chen CC, Lin MT, Tien YW, Yen CJ, Huang GH, Inouye SK. Modified hospital elder life program: effects on abdominal surgery patients. J Am Coll Surg. (2011) 213:245–52. doi: 10.1016/j.jamcollsurg.2011.05.004
30. Milisen K, Foreman MD, Abraham IL, De Geest S, Godderis J, Vandermeulen E, et al. A nurse-led interdisciplinary intervention program for delirium in elderly hip-fracture patients. J Am Geriatr Soc. (2001) 49:523–32. doi: 10.1046/j.1532-5415.2001.49109.x
31. Wei LA, Fearing MA, Sternberg EJ, Inouye SK. The Confusion Assessment Method: a systematic review of current usage. J Am Geriatr Soc. (2008) 56:823–30. doi: 10.1111/j.1532-5415.2008.01674.x
32. Radtke FM, Franck M, MacGuill M, Seeling M, Lütz A, Westhoff S, et al. Duration of fluid fasting and choice of analgesic are modifiable factors for early postoperative delirium. Eur J Anaesthesiol. (2010) 27:411–6. doi: 10.1097/EJA.0b013e3283335cee
33. Radtke FM, Franck M, Schneider M, Luetz A, Seeling M, Heinz A, et al. Comparison of three scores to screen for delirium in the recovery room. Br J Anaesth. (2008) 101:338–43. doi: 10.1093/bja/aen193
34. Kim S, Choi E, Jung Y, Jang I. Postoperative delirium screening tools for post-anaesthetic adult patients in non-intensive care units: a systematic review and meta-analysis. J Clin Nurs. (2023) 32:1691–704. doi: 10.1111/jocn.16157
35. Inouye SK, Charpentier PA. Precipitating factors for delirium in hospitalized elderly persons. Predictive model and interrelationship with baseline vulnerability. JAMA. (1996) 275:852–7. doi: 10.1001/jama.1996.03530350034031
36. Lindroth H, Bratzke L, Twadell S, Rowley P, Kildow J, Danner M, et al. Predicting postoperative delirium severity in older adults: the role of surgical risk and executive function. Int J Geriatr Psychiatry. (2019) 34:1018–28. doi: 10.1002/gps.5104
37. Ciesielska N, Sokołowski R, Mazur E, Podhorecka M, Polak-Szabela A, Kędziora-Kornatowska K. Is the Montreal Cognitive Assessment (MoCA) test better suited than the Mini-Mental State Examination (MMSE) in mild cognitive impairment (MCI) detection among people aged over 60? Meta-analysis. Psychiatr Pol. (2016) 50:1039–52. doi: 10.12740/PP/45368
38. Robinson TN, Eiseman B. Postoperative delirium in the elderly: diagnosis and management. Clin Interv Aging. (2008) 3:351–5. doi: 10.2147/cia.s2759
39. McAlpine JN, Hodgson EJ, Abramowitz S, Richman SM, Su Y, Kelly MG, et al. The incidence and risk factors associated with postoperative delirium in geriatric patients undergoing surgery for suspected gynecologic malignancies. Gynecol Oncol. (2008) 109:296–302. doi: 10.1016/j.ygyno.2008.02.016
40. Beck S, Hoop D, Ragab H, Rademacher C, Meßner-Schmitt A, von Breunig F, et al. Postanesthesia care unit delirium following robot-assisted vs open retropubic radical prostatectomy: a prospective observational study. Int J Med Robot. (2020) 16:e2094. doi: 10.1002/rcs.2094
41. Ehsani R, Djalali Motlagh S, Zaman B, Sehat Kashani S, Ghodraty MR. Effect of general versus spinal anesthesia on postoperative delirium and early cognitive dysfunction in elderly patients. Anesth Pain Med. (2020) 10:e101815. doi: 10.5812/aapm.101815
42. Evered LA, Chan MTV, Han R, Chu MHM, Cheng BP, Scott DA, et al. Anaesthetic depth and delirium after major surgery: a randomised clinical trial. Br J Anaesth. (2021) 127:704–12. doi: 10.1016/j.bja.2021.07.021
43. Chew D, Sethi E, Sim YE, Tan PYB, Abdullah HR, Bin Johri MN, et al. Postoperative delirium following total joint arthroplasties in a multi-ethnic population—a prospective observational study. Knee. (2021) 32:103–11. doi: 10.1016/j.knee.2021.08.009
44. Maheshwari K, Ahuja S, Khanna AK, Mao G, Perez-Protto S, Farag E, et al. Association between perioperative hypotension and delirium in postoperative critically ill patients: a retrospective cohort analysis. Anesth Analg. (2020) 130:636–43. doi: 10.1213/ANE.0000000000004517
45. Hirsch J, DePalma G, Tsai TT, Sands LP, Leung JM. Impact of intraoperative hypotension and blood pressure fluctuations on early postoperative delirium after non-cardiac surgery. Br J Anaesth. (2015) 115:418–26. doi: 10.1093/bja/aeu458
46. Wong ZZ, Chiong XH, Chaw SH, Hashim NHBM, Abidin MFBZ, Yunus SNB, et al. The use of cerebral oximetry in surgery: a systematic review and meta-analysis of randomized controlled trials. J Cardiothorac Vasc Anesth. (2022) 36:2002–11. doi: 10.1053/j.jvca.2021.09.046
Keywords: delirium, subsyndromal delirium, benzodiazepine, anesthesia, postoperative care unit
Citation: Sachdev A, Moges Y, Rubin M, Sremac AC, Arvanitakis Z and McCarthy RJ (2023) Early incident and subsyndromal delirium in older patients undergoing elective surgical procedures: a randomized clinical trial of an avoid delirium protocol. Front. Anesthesiol. 2:1268263. doi: 10.3389/fanes.2023.1268263
Received: 27 July 2023; Accepted: 10 October 2023;
Published: 2 November 2023.
Edited by:
Hossam El Beheiry, University of Toronto, CanadaReviewed by:
Matthias Bock, Hospital “F. Tappeiner,” ItalyAveek Jayant, Homi Bhabha Cancer Hospital and Research Centre, India
© 2023 Sachdev, Moges, Rubin, Sremac, Arvanitakis and McCarthy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert J. McCarthy Robert_J_McCarthy@rush.edu