Forms of professional interkinesthesia in nurses' body work: A case study of an infant's stepping
 Julia Katila1*
Julia Katila1*  Johanne S. Philipsen2
Johanne S. Philipsen2- 1Faculty of Social Sciences, Tampere University, Tampere, Finland
- 2Department of Language and Communication, University of Southern Denmark, Odense, Denmark
Moving their bodies in knowledgeable and professional ways in order to handle and connect affectively with infants entails a large part of child health care nurses' work. We deploy a phenomenological approach to videoanalysis of interaction to analyze an episode of a 1-month-old infant visiting the child health care clinic with their caregiver to have their body assessed for a neonatal stepping. Focusing on the co-movement of the baby and the nurse, we ask: how do various ways of moving as a co-embodied entity allow and corporeally prompt the baby's age-appropriate bodily ability to emerge? We develop the notion of professional interkinesthesia to indicate specific forms of body work of nurses which in this case entails moving together with the baby to make her successfully perform a specific health care task—the stepping. Building on Charles Goodwin's concept of professional vision, we uncover how the nurse moves and touches the infant's body in ways relevant to the institutional task. The study shows that accomplishing “normally” developed neonatal stepping is not work accomplished by the baby alone but requires that the bodies of the baby and the professional move in unison. While neonatal stepping is but one specific type of health care task, we propose that nurses' work entails numerous forms of professional touch and interkinesthesia that make it possible to successfully perform different types of health care operations.
Introduction
Previous interaction research has shown that embodied interaction plays a crucial role in health care encounters (Heath, 1986). Drawing on the phenomenological approach to videoanalysis of movement and kinesthesia in interaction (Wedelstaedt and Meyer, 2017; e.g., Meyer et al., 2017; Philipsen and Katila, 2021), we develop the notion of professional interkinesthesia to analyze the interkinesthetic body work of nurses. Specifically, we focus on the work of child health care nurses, who conduct health checks for infants soon after their birth. Furthermore, in our analysis, we build on Goodwin's (1994, 2018) concept of professional vision, which refers to socially organized ways of seeing, understanding, and acting to make sense of the world in occupation- or institution-specific ways. Building on Goodwin's work, scholars have shown that not only vision but also touch can be part of such institutionalized professional practices (Nishizaka, 2007; Kuroshima, 2020). Child health care nurse's hands, for instance, are knowledgeable about sensing and palpating developmentally “normal” and “abnormal” features in the baby's body and bringing them into the baby's and other co-present participants' awareness.
Building on this body of research investigating professional multimodal practices, we explore some of the embodied styles in which a nurse utilizes the interkinesthetic body to highlight and bring forth relevant features in a baby's body that are central to carrying out the institutional task. According to Behnke (2008, p. 144), interkinesthesia refers specifically to kinesthetic modes of inter-bodily relationality or intercorporeality (Merleau-Ponty, 1962, 1964, 1968). Interkinesthetic moments enable human beings to connect with each other intercorporeally through moving together (Behnke, 2008; Meyer and Wedelstaedt, 2017).
As one example of such interkinesthetic moments in child health care clinics, we selected the case of an authentic interaction between a nurse and a 4-week-old infant who is being examined for neonatal stepping. Also known as the walking reflex or response1, a baby up until 2 months of age should start stepping when held in an upright position with her or his feet touching a surface (Thelen and Fisher, 1982; e.g., Barbu-Roth et al., 2009).
As a standard procedure, babies are being examined in various ways after their birth in order to determine if they are healthy and their bodies have developed normally. The first health care examinations may thus be directly consequential for the baby and the baby's caregiver(s). Given that embodied interaction has an impact on how the health care examinations emerge, it is of great importance how the practitioner moves and interacts with the patient during these encounters.
As introduced above, we approach the baby's embodied movements, including stepping, as actions brought forth by the nurse's skilled, professional body work. Furthermore, we view the occurrence of stepping as a result of an interkinesthetic choreography in which the nurse and the baby participate together. Focusing on the co-movement of the baby and the nurse, we ask: how do these ways of moving as a co-embodied entity allow and corporeally prompt the baby's age-appropriate bodily ability to emerge? To answer this question, we utilize multimodal videoanalysis of the interaction (Streeck et al., 2011). Multimodal videoanalysis of interaction enables uncovering in detail how tasks such as testing the neonatal stepping are being achieved through moment-by-moment embodied interaction moves of the participants.
In the case study analysis, we show how the specific kinesthetic skills of the baby that are being tested become visible through the nurse's interkinesthetic highlighting and how the nurse—deploying her body, voice, eyes, and hands—provides a scaffold for the baby to move in a way that is recognizable as accomplishing the “neonatal stepping.” In doing so, we highlight how accomplishing neonatal stepping is but one example of the various institutionalized abilities of a nurse's body skilled at handling and connecting with patients in various ways.
Professional vision and professional touch
Moving their bodies, especially their hands, in knowledgeable ways is central to nurses' work. The bodies of the child health care nurses working with infants are especially shaped by different forms of body work (Twigg et al., 2011), such as touching, empathetic attunement, and moving together with the babies, in ways relevant to the institutional task at hand. Skilled in the “art of touching” (Van Dongen and Elema, 2001), the practitioners know the ways of both “instrumental” and “expressive” forms of touch (Watson, 1975; Routasalo, 1999) crucial in conducting their institutional tasks. This embodied ability enables conducting health care tasks such as palpating, diagnosing, and investigating (Nishizaka, 2007), moving or making the patient's body move (Guo et al., 2020; Raudaskoski, 2020), showing empathy (Mononen, 2019; Raia et al., 2020), and healing (Paterson, 2005). Previous studies have uncovered the health care practitioner's “professional touch” through which they palpate, investigate, and support (Nishizaka, 2007; Merlino, 2020; e.g., Kuroshima, 2020) the patient's body in ways that highlight (Goodwin, 1994, 2018) areas relevant to health care tasks, such as diagnosing illness.
Such practices are similar to other embodied, institutionalized ways of “seeing” or making visible specific aspects of the world that are important for carrying out different tasks. For example, archaeologists uncover traces of ancient human artifacts by tracing out color changes in dirt (Goodwin, 1994, 2018), food professionals touch cheese in a gourmet shop to determine qualities in them (Mondada, 2020), or auto-shop owners touch parts of a car in ways that enable diagnosis of problems (Streeck, 2013; Cuffari and Streeck, 2017). Other studies have shown how vision (Goodwin, 1994), gestural practices of pointing, tracing, and reenacting (Goodwin, 1994, 2018; Philipsen and Trasmundi, 2019; Philipsen and Katila, 2021), and touch (Nishizaka, 2007; Kuroshima, 2020; Merlino, 2020) are important for carrying out as well as teaching these different professional practices.
In this study, we show how not only touch and vision but also interkinesthetic actions of moving a patient's body and moving together with a patient can be employed in similar ways to highlight bodily (dys)functions and abilities relevant for the professional task-at-hand.
Interkinesthesia, touch, and the haptic system
Human beings are born mobile (Sheets-Johnstone, 2011), and this inborn sensemaking of the world through body movement is closely intertwined with the sense of touch and the whole haptic system. As such, early communication between infants and caregivers often unfolds as interkinesthetic. Enabled by direct intercorporeal connections between bodies, in interkinesthetically coordinated movement, single bodies connect through movement and move meaningfully together. By attuning to and anticipating the subtle body movements of the other and emerging as a co-mobile unit, bodies are able to perform movement trajectories from spontaneous co-gestures to complex and well-practiced choreographies of team sports (Behnke, 2008; Stuart, 2012; Meyer and Wedelstaedt, 2017; Philipsen and Katila, 2021).
Similarly, when infants are being tested in the health care clinic, the newborn and the nurse must attune to each other's moving bodies via the language of the body. Due to this inherently intercorporeal and interkinesthetic nature of the interaction among caregivers and babies, we do not simply analyze the nurse's touch in health care clinics. Instead, we approach the nurse's body work as an engagement of the whole “haptic system” (Gibson, 1966). Including forms of touch as well kinesthesia (Gibson, 1966; Sheets-Johnstone, 2011; Katila, 2018), the haptic system refers to “an apparatus by which the individual gets information about both the environment and his body” (Gibson, 1966, p. 97). Enabling perceiving messages both from the “inside” and “outside” of the body, the haptic system is the simultaneous sensibility of an individual toward the world and their body through bodily actions.
By focusing on the haptic system instead of mere touch, it is possible to reflect on how the bodies simultaneously feel both themselves and the world around them, including other living bodies. In their reflection on Merleau-Ponty's theory on human embodiment and affectivity, Roald et al. (2018, p. 208) describe how the perception of the world is always synonymous with a perception of one's own body, or, in authors' words, “external perception and the perception of one's own body are two facets of the same act.”. In touching, for instance, the body senses that which is being touched, as well as one's own body touching (Merleau-Ponty, 1968). Moreover, when touching other living bodies, one's body is inevitably touched by other bodies and the world. Indeed, as pointed out by Van Dongen and Elema (2001, p. 150), a nurse's body work and touch evoke feelings not only in the patients but also in the nurses themselves. The nurse connects her own feelings of being touched to those of her patient and is simultaneously affecting and affected by them (i.e., interaffectivity, Fuchs, 2017). This two-way dimension of touch (touching and being touched), combined with its both “inward” and “outward” dimension (kinesthesia/proprioception and sense of touch), indicates that the child health care nurses cannot simply unidirectionally move and touch the patients—they inevitably move with the patients and are also being touched by them. In a way, when we touch other people, our bodies and their sensorial fields spread to the world around us and the things we grasp, manipulate, and feel.
Kinesthesia also cuts across perceptual systems (Gibson, 1966, p. 111). Just as we never lack tactile experience, we also never lack kinesthetic experience of ourselves in the world, even if we do not pay attention to it most of the time. However, as Sheets-Johnstone (2002, p. 138) expresses, “Any time we care to pay attention to ourselves, there we are—kinesthetically, tactilely.” Each sensorial and perceptual action has a kinesthetic aspect in it: it is feeling the moving “I” in reaching out to the world. In terms of touching and being touched, the kinesthetic sensation is different. Feeling the “I” moving the body in touching, and feeling the “I” when being moved and touched by somebody else are distinct feelings, even if these sensations are ultimately intertwined. Due to these multi- and “inter-sensorial” (Howes 2005, p. 7) aspects of co-embodied relationality in the encounters between the nurse and the baby, we focus on uncovering forms of professional interkinesthesia. This enables us to view bodies and their multisensorial features in connection to the bodies they touch and by which they are simultaneously being touched.
Infant stepping as a context-specific action
As one example of interkinesthetic action, in this paper, we analyze how neonatal stepping is being examined in child health care clinic. Neonatal stepping refers to the tendency of a baby to start stepping when held in an upright position with her or his feet touching a surface (e.g., Forssberg, 1985). According to previous research, stepping is expected to last until about 2 months after birth (Thelen and Fisher, 1982; Barbu-Roth et al., 2009). The relationship between infant stepping and walking has been discussed to an extent. Although infant stepping disappears during the course of development, some scholars believe the response does not disappear but is only temporarily suppressed by the weight of the infant's leg (Thelen and Fisher, 1982; Cautilli and Dziewolska, 2006). It has been suggested that mature walking may evolve from infant stepping patterns (Thelen and Cooke, 1987), and that practicing infant stepping can lead to accelerated walking (Ulrich et al., 2001).
In the context of health care encounters, stepping is being evoked in the baby as part of testing if their body is developing according to age-appropriate expectations. Thus, the moments of testing can be highly meaningful and directly consequential for the baby and their caregiver, as the baby's development is being evaluated within these encounters. For the babies themselves, responding to a certain stimulus by moving their legs one after another on the ground indicates a spontaneous pre-reflective expression and body movement. However, in the institutional context of health care, through the development of the child health care occupation and developmental psychology research, it has come to mean “neonatal stepping” or “stepping reflex.”
In a sense, neonatal stepping is thus a product of the health care institution and developmental psychology research, and its occurrence is entirely context-dependent. It not only requires a nurse with a specific professional vision to conduct the task, but the special institutional environment and physical background (examination table) must be present and involved in specific ways, in order for the action to be identified as a successful occurrence of neonatal development. Moreover, the most distinctive aspect of stepping or walking is often thought of as the movement of the legs. However, walking is a body technique (Mauss, 1973) developed in humans through the evolution toward an upright posture. To state the obvious: an infant conducting the stepping reflex can move their feet, but not to hold their body upright or to walk. Thus, it is only through co-participated embodiment with the nurse that the baby momentarily becomes a walking body.
Materials and methods
Video data
The research data consist of video recordings of authentic interactions in a Finnish child health care clinic. The data collection followed the Finnish National Board of Integrity's ethical guidelines for collecting and handling data. The data include information gathered from child patients accompanied by their parents, and written informed consent was obtained from the parents (Ruusuvuori et al., 2008; Ijäs-Kallio et al., 2011; see Homanen, 2013). To illustrate our finding—the form of nurse's body work we call professional interkinesthesia—we have chosen one exemplary case of a four-week-old baby's visit to health care that we will present, analyze, and discuss in detail. We will exemplify how the professional and the baby interact with each other using their whole bodies during physical examinations in the postnatal clinic.
Methodological approach
We adopt multimodal videoanalysis of interaction as a method to analyze the health care encounter. This microanalytic approach stems from a wide field of qualitative studies focused on the intercorporeal, multimodal, multisensorial, and other semiotic aspects of naturally occurring face-to-face interactions (Streeck et al., 2011; Meyer et al., 2017; Goodwin, 2018; Goodwin and Cekaite, 2018; Katila, 2018). Our co-operative and intercorporeal perspective on microanalysis draws on embodied and experienced understandings of human action, and it is especially helpful for the study of embodied resources, such as affect, touch and interkinesthetic sociality (see Katila and Philipsen, 2019; Katila and Raudaskoski, 2020; Katila and Turja, 2021; Philipsen and Katila, 2021). With videoanalysis, it is possible to analyze embodied, communicative aspects of interaction, and to determine how these aspects are manufactured together by the participants through their mutually elaborating body movements and orientations. Moreover, by drawing on an inherently social and intercorporeal understanding of human bodies (Merleau-Ponty, 1962), we pay careful attention to how participants, in their interactions as living bodies, directly participate in and sense the social meanings implied in each other's actions. In terms of analysis, this intercorporeal starting point also requires the adoption of the researchers' own bodies to co-empathize with the communicative meanings experienced by the participants in the interactions that are revealed in the video data (Katila and Philipsen, 2019; Katila and Raudaskoski, 2020; Katila and Turja, 2021).
Results
In this section, we exemplify a nurse's interkinesthetic practices in action by showing how the nurse employs an array of multisensorial—haptic, kinesthetic, aural, and visual—body techniques embedded together to successfully accomplish an institutional task. We do this by uncovering the moment-by-moment unfolding interkinesthetic movement trajectories and multisensorial actions of “highlighting” (Goodwin, 1994), which allow aspects of the baby's bodily capabilities to “become visible” and, thus, perceptually available to co-present interlocutors. As introduced above, we analyze the details of a successful institutional action—the nurse engaging in a “walking formation” with the baby—to test the emergence of the baby's stepping response.
In the moment-by-moment interactions, it is the task of the nurse to first “make” the baby's body conduct the walking reflex. The baby by herself cannot stand upright, not to mention walk; thus, the nurse must engage with the baby in order to make the baby stand upright before they step together. Moreover, it is the nurse, through her embodied knowledge base as a health care professional, who then determines what “qualifies” as an adequate display of a stepping response. In other words, the nurse decides what kind of body movements of the baby can be treated as “stepping” and how long the baby must conduct these “symptoms” as sufficient proof of a “normally” functioning neonatal stepping. As explained by Goodwin (1994, p. 606).
“…the ability to see a meaningful event is not a transparent, psychological process but instead a socially situated activity accomplished through the deployment of a range of historically constituted discursive practices.”
Notably, the nurse cannot simply request or prompt the baby to do the walking reflex; instead, it requires specific artful types of haptic handicraft as well as co-inhabiting the walking movement with the baby. Along with applying forms of professional touch, the nurse deploys her body into a type of professional interkinesthetic action—moving with the patient to make the patient move in the desired manner.
Making off an interkinesthetic formation of a “walking body”
In what follows, we illustrate how the nurse and the baby emerge through careful embodied coordination in an interkinesthetic formation. In Extract 1 Part 1, we show how the nurse arranges the baby in an upright posture to allow the occurrence of the stepping and the “making of a walking body.” We will analyze how the nurse accomplishes this by lifting and twisting the baby's body in an upright position while verbalizing the action. The nurse's gentle touch invites this asymmetric but reciprocal interkinesthetic body movement of lifting and being lifted. Embedded in the same haptic and tactile actions are caressing the baby's skin. Thus, different forms of tactile and haptic actions—lifting, stroking, and palpating—unite into a single interkinesthetically coordinated trajectory. In the extract, a 4-week-old baby (BA) arrives at the children's health care clinic with her mother (MO). Beside the main nurse (N1), a nurse trainee (N2) is present in the encounter (see Image 1, Participant map).

Extract, Part 1.
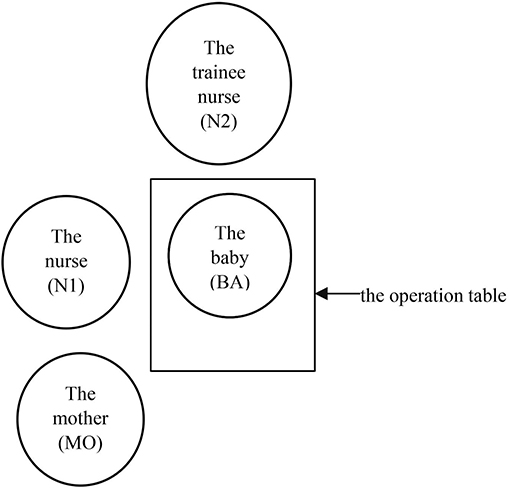
Image 1. Participant map.
We will analyze the interactional organization of making a stepping or “walking body”. The verbal transcription conventions are presented in Appendix 1. The conventions are modified for our purpose from the work of conversation analyst Jefferson (2004). In addition to more conventional transcription signs, A before utterances is used to indicate adult-targeted voice, whereas I indicates infant-targeted, high-pitched “baby talk” or “motherese” voice (see Fernald, 1985), often addressed at babies by caregivers.
before utterances is used to indicate adult-targeted voice, whereas I indicates infant-targeted, high-pitched “baby talk” or “motherese” voice (see Fernald, 1985), often addressed at babies by caregivers.
In Figures 1, 2, N1 starts to lift the baby while twisting and lifting her to an upright position. Here, the baby's body is entirely lifted and moved by the nurse, and the trajectory of the movement is authored by her. However, the baby takes part in the movement by aligning with the nurse's corporeal language and allowing herself to be lifted. The bodies move together in a trajectory designed by the nurse in an interkinesthetic formation, with asymmetric but complementary kinesthetic roles. The baby is feeling her body being lifted and the nurse is simultaneously feeling the baby's body through touch as well as the baby's weight in her hands and arms. Thus, this intercorporeally coordinated action engages different but complementary aspects in the haptic system (Gibson, 1966) for both: the nurse engages in forms of active touch and moves the other to conduct the professional practice; the baby feels the sensation of being touched, lifted, and manipulated by the nurse. Essentially, these complementary aspects of touching and being touched only make sense together, and the sentient body of the nurse is also constantly being affected by the moving and sensible body of the baby. Moreover, verbal and embodied cues work together to create this tactilely coordinated interkinesthetic formation. N1 laminates the ongoing action by saying [A shall we see a little bit now if we take good↑STEPS (line 01). Through this utterance, N1 discursively unites herself and the baby—using the plural first-person form “we”—to create a shared agency (see Parry, 2017) with the baby. Through this grammatical form, N1 unites the baby into a co-embodied gestalt about to take steps. Importantly, uttered in an adult-targeted voice, N1 also informs the other co-present participants of what happens next.
N1 then supports the baby's body gently in an upright position and gently strokes the baby's back with her right hand (Figure 3). She then reaches the baby's bottom (Figure 4), and changes the position of her hands (Figure 5) so that both the baby and N1 face the same direction (Figure 6). The hands of the nurse move in various ways on the baby's body, manipulating the baby's body through “haptic communication” (Schindler, 2017). In concert with each other, these haptic communicative movements display skilled, professional handcraft. At the same time, the nurse's hands (1) move the baby's body and simultaneously corporeally request that the baby move her own body in a desired direction, acting as implicit embodied requests, (2) palpate the baby's body, and (3) gently soothe the baby's body. In this haptic movement, various types of professional touch in nursing—“instrumental” and “expressive” (Watson, 1975; Routasalo, 1999; Van Dongen and Elema, 2001; Paterson, 2005)—intersect.
To summarize, in Extract 1 Part 1, we see how the nurse connects her body to that of the baby through touch, and then moves the baby's body in various ways relevant to the institutional task-at-hand. Her hands, moving together with the baby through the haptic actions of lifting, twisting, and escorting the baby's body, include creative and institutionalized forms of professional touch and interkinesthesia that enable the baby's body to emerge in an upright body posture required for the forthcoming stepping. The success of the action not only includes manipulative touch, but it also includes more affective forms of touch as well as accompanying verbal actions that manage the “participation framework” (see Goodwin and Goodwin, 2004) with other co-present participants, especially the baby's mother. However, in Extract 1 Part 1, the nurse primarily moves, touches, and manipulates the baby's body to present the baby's body in a desired fashion. Although the co-embodied, interkinesthetic movement is present here in the form of the complementary roles of moving and being moved, in Extract 1 Part 2, the moment continues into more equally distributed labor concerning the movement of the baby's body—the co-embodied interkinesthetic formation of the baby's “walking body”.
Extract, Part 2.
Highlighting certain parts of the body to initiate specific types of movement
In Extract 1 Part 2, which immediately follows Extract 1 Part 1, we illustrate how the nurse moves the baby's body in a certain way to encourage the emergence of the neonatal stepping to occur. The emergence of the baby's stepping is enabled by the nurse's table, which acts as a medium for the forthcoming stepping. The nurse moves the baby's body against the table in a manner that makes stepping and the desired movement trajectory relevant. This emerges as a professional interkinesthetic action of “highlighting” (Goodwin, 1994), as it enables the specific movement capabilities of the baby to “become visible” and thus perceptually available to all co-present participants.
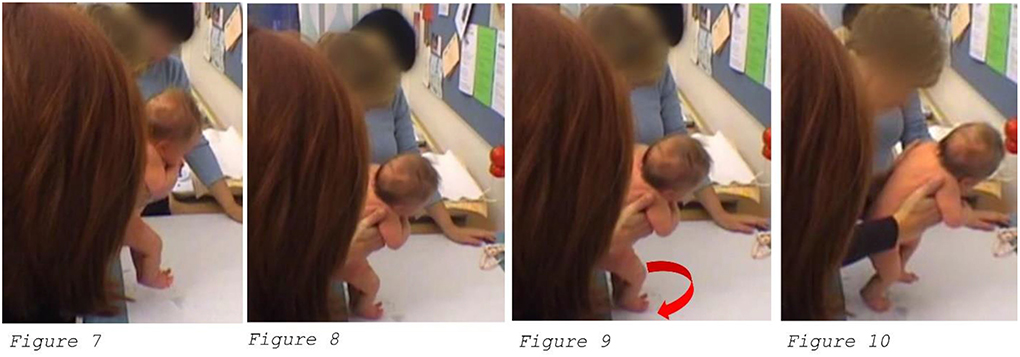
After accomplishing an upright posture, N1 first lifts the baby's body slightly (Figure 7), and then lands her feet back to the table (Figure 8). After providing this momentum for the baby's body to start stepping by touching the table with the baby's feet, the nurse then circles the baby's feet lightly against the table clockwise (Figure 9). By moving the baby's body up and against the table in this specific manner, the nurse creates a scaffold, a narrow field of potential next body movements for the baby to act upon next. This body technique not only communicates to the baby about the relevance of the feet, but also about the relevance of moving the leg forward. The circle illustrated in Figure 9 initiates movement of the feet, and as the movement of the circle flows clockwise, it is embodiedly relevant for the baby's left leg to continue the movement. As N1 then slightly tilts the baby toward the left, this embedded haptic directive results in the baby “taking her first step” with her left foot (Figure 10). This circling choreography of the bodies is only visually available for the analyst, but it is directly felt (inter)kinesthetically and haptically by the participants. We—the analysts—can only imagine through our own embodied knowledge the body-to-body sensed details of the finetuned haptic movements of the nurse, resulting in the baby moving in a desired manner. However, it is exactly these pre-reflexive and pre-discursive ways of the body that make the dance-like circling motion initiated by the nurse understandable as a request for the baby to move in a particular manner. Such interkinesthetically accomplished ways of the nurse's body are professional practices that enable bringing forth relevant “symptoms”—stepping—in the baby's body and thus highlight aspects of the baby's body essential for successfully accomplishing the institutional task.
Thus far, we have described how the nurse accomplishes with the baby the corporeal “pre-requirement” for the stepping reflex to occur—upright posture (Extract 1 Part 2)—and the way in which the nurse palpates the baby's body to bring about certain next body movements in the baby's body, namely stepping. Next, we illustrate how the bodies of the baby and the nurse “walk together” in the form of an interkinesthetic stepping formation.
Infant stepping as a result of professional interkinesthesia
In Extract 1 Part 3, we will describe how, after the stepping has been initiated (Part 2), the nurse and baby together inhabit a stepping or walking body. Enabled by the interkinesthetic connection between the bodies, the movement trajectory entails a careful reciprocity of steering and being steered, leading the movement and being moved—somewhat similar to a couple dance. The tactile arrangement and the emerging asymmetric but reciprocal movements of the bodies resemble “shepherding” actions conducted by parents with their children in a “control formation,” with the adult positioned behind the child (Cekaite, 2010, p. 2, 7). However, unlike in shepherding, the body of the baby here is being fully carried by the nurse, and the baby's stepping movements are corporeal responses to the continuous interkinesthetically orchestrated palpation moves.
Extract, Part 3.
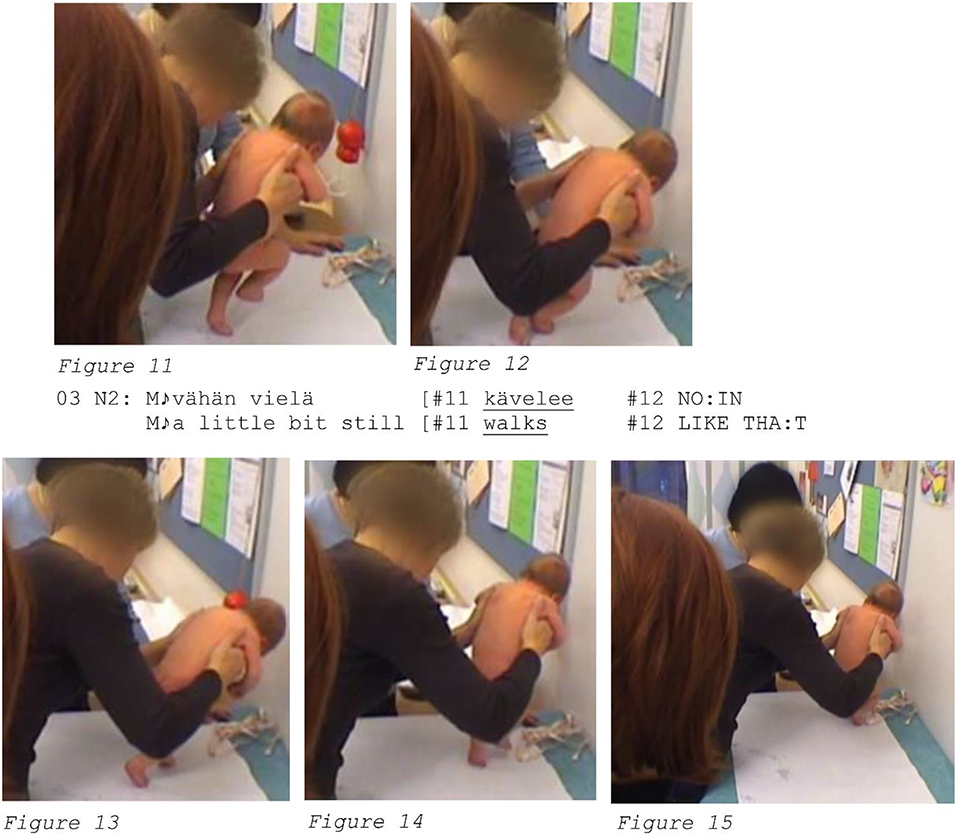
After the baby has taken her first step (see Extract 1 Part 2, Figure 10), the embodied movements of the baby and the nurse unfold in a careful and rhythmic reciprocity involving their co-participation. It is only after the baby herself moves her own leg that N1 lightly steers the baby's body again toward the right, and this steering, accompanied by carrying the baby's body and moving it slightly forward, provides another scaffold for the baby's right leg to move forward and create another “step” (Figures 11, 12). During these first two steps, the nurse laminates the baby's steps with verbal evaluation, “a little bit still [walks LIKE THA:T” (line 03), through which she makes official to the baby and the other participants that how the baby has moved her body so far qualifies as an occurrence of neonatal stepping. In other words, the step is treated as successfully fulfilling the requirements of the institutional task and as qualifying as a “normal” movement and development of the body. By using the third-person singular verb form, “walks,” N1 highlights the baby's agency in the walking activity and downplays her own contribution in making the stepping possible. Further, N1 uses a baby-targeted or motherese tone of voice. The vocal quality she uses is very affective in nature, resonating an empathetic engagement with the baby. This affective aural action rhythmically co-occurs with the interkinesthetic one: the co-embodied steps occur with the same tempo as the health care practitioner's words, the two inhabiting a multi-sensorial—kinesthetic, haptic, and aural—intercorporeality.
Even though the category of stepping has now been officially accomplished, the co-embodied movement of the nurse and the baby continues. By carefully attuning to the timing of the baby's locomotion, N1 again steers the baby's body slightly from left to right once more (Figures 13, 14), using the rhythm of the baby's steps while holding and moving the baby forward at the speed initiated by the baby with her walking tempo. Showing an active agency in stopping the movement, the baby then “collapses” at the table and lets her body be held entirely by the nurse (Figure 15).
In summary, Extract 1 Part 3 shows us how the baby—in spite of the fact that as a one-month-old, she obviously cannot walk—is made to inhabit a walking body. The emerging stepping activity is an entirely co-embodied and interkinesthetic accomplishment, requiring the intercorporeal collaboration of the nurse and baby: while the nurse is holding and moving the baby's body forward, the baby is the one who actually provides the steps and therefore also actively participates in the tempo and unfolding of the movement. Furthermore, the type of action is not just any type of stepping but an institution-specific category of stepping reflex that resembles the recognizable body technique of walking. For it to be recognizable as a stepping reflex, the co-embodied stepping action of the baby and the nurse must be “environmentally coupled” (Goodwin, 2007) with the operation table and, more broadly, the specific institutional context.
As for the forms of professional touch, we observe that they are entirely intertwined with forms of professional interkinesthesia. Engaging the haptic system and sensations of moving and being moved, the distribution of the corporeal body control between the nurse and the baby constantly “fluctuates” (see Guo et al., 2020). Furthermore, these interkinesthetic activities are here orchestrated not only through touch but also through co-occurring vocal expressions, which together create a shared affective space that all co-present participants embody. Kinesthetic sensation is not only embedded in touch; it is included in all body movements (Gibson, 1966, p. 111), including vocal action. Therefore, interkinesthesia, even if closely related to touching and being touched, entails more generally the idea of moving comprehensively in ways that make sense together.
In Extract 1 Parts 1–3, we have demonstrated how the interkinesthetic ability of human beings is harnessed as an institutional action for the nurse's “professional vision” (Goodwin, 1994). Importantly, it brings forth how the stepping reflex is an entirely intercorporeal accomplishment wherein biological, neural, and motor development is enmeshed within the professional skill of the nurse and the moment-by-moment unfolding of the body-to-body communication between the nurse and the baby.
Indeed, the fluent and unattended way in which the nurse moves with the baby's body exemplifies well the embeddedness of the skilled and professionalized aspect of her interkinesthetic abilities. The specific body movements of making the baby step are certainly learned and habitualized as a result of countless times of repetition of similar movements with babies but are still actualized in a novel moment, with a new participant—a baby who has no previous experience on moving with the nurse in this specific manner. Elsewhere, in the context of analyzing breathing together with the patient in a therapist's office, we (Philipsen and Katila, 2021, p. 11) suggested that:
In order to grasp such opportunities for interkinesthetic co-participation, the therapist cannot simply act as a distanced or professionalized body, but must lend their body to the intercorporeal momentum, and as a consequence also be open to be influenced by the body of the patient.
Arguably, an intercorporeal momentum of a similar kind also takes place in the current context, when the nurse is witnessed lending her body for the purpose of making the baby's body move—first to be in an upright posture and then step—in certain ways.
Discussion: The professionalized ways of the nurse's body
In this study, we have exemplified what we called professional interkinesthesia at the child health care nurse's office. We showed how, deploying an array of professional kinesthetic and haptic movements, such as lifting, twisting, moving with and moving from one side to another, the nurse was able to make the baby move in an institutionally relevant manner—to conduct the “neonatal stepping.” Especially when deploying a specific circling movement while touching the table with the baby's feet, the nurse was able to provide a scaffold for the baby's neonatal stepping response to occur. This professional interkinesthetic “highlighting” (Goodwin, 1994) made it possible for the baby's task-relevant capabilities to “become visible” and publicly observable.
These body techniques are a combination of both the embodied and professional skills of the nurse. They are habitualized to the extent that they are rarely explicitly attended to but still always conducted in a slightly new and creative way with a new patient. Indeed, as the bodies and embodied affordances of each nurse are all different, so are the bodies and embodied affordances of each baby who comes to the clinic. Thus, the examinations involve elements of historically learned and habitualized practices as well as spontaneous coordination and attunement in each new encounter. For instance, not all babies are able to respond to the embodied movements of the nurse and conduct the stepping, even if the nurse makes all relevant body trajectories to bring about these movements in the baby. Needless to say, the neonatal stepping is not only a result of the intercorporeal communication between the nurse and the baby, but the baby must have actually developed this embodied tendency so that the interactional and kinesthetic emergence of the stepping is possible.
Our detailed video analysis exemplified how making of a normally moving body required the nurse initiating an interkinesthetic formation with the baby, and their bodies to move in unison by attuning to each other's movements through tactile, aural, visual, and affective resonance. During these moments of interkinesthetic togetherness, the baby and nurse are in the process of “making” (Behnke, 1997) the baby's body move and react normally. As expressed by Behnke (1997, p. 198):
[…] even if my body is something I do, I do not do it alone: the micromovements through which I am continually making a body are situated within a more encompassing interkinesthetic field, including not only the movements and micromovements of those around me, but also the sedimented traces of such movements and micromovements in the artifacts around me.
Extensively growing and developing during the first months and years of their lives, newborn human bodies are in a constant process of making. Moving together in health care examinations provides a vivid culmination point of not only the making of a moving body, but the making of a “normally” moving body: that is, a body that fulfills the criteria of the normal movement of a body at a certain age discovered by developmental psychology.
Moreover, these visits to health care clinics—among the first ones, if not the first one in the newborn's life—also provide some of the baby's first exposures to modes of behavior when presenting one's body as an “object for medical investigation” (Heath, 2006). These first moments of the socialization of children into the role of a patient in health care require embodied guidance and controlling touch from the professionals, as well as acts of empathy and soothing through touch and, for instance, the motherese tone of voice. By including controlling and soothing tactile and aural actions, the health care practitioner is able to prompt the baby toward specific types of behavior expected in a health care meeting.
Finally, although in this study we have only addressed one very specific example, forms of professional interkinesthesia are everywhere in different types of health care encounters involving body work. In the future, more studies exploring forms of skilled body work and professional interkinesthesia are needed to uncover the multitude of ways in which health care practitioners use their bodies in interaction with the patients to accomplish institutional tasks. Embodied interaction influences the success of the health care operations and, thus, unveiling its detailed dynamics are of interest not only to researchers of health and embodied interaction but also to health care practitioners.
As conductors of hands-on body work, the hands of health care practitioners are especially skilled at moving and moving with the bodies of the patients. Although neonatal stepping is a good example of co-embodied agency, health care professionals constantly “lend” their bodies for the sake of institutional actions to various extents and in various ways. These ways of moving together are professionalized, institutionalized, and habitualized versions of the human bodies' basic ability and tendency to coordinate movement with other people, that is, the interkinesthetic co-embodiment.
Data availability statement
The dataset is not available for sharing because of confidentiality reasons. Requests to access these datasets should be directed to julia.katila@tuni.fi.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Tampere Region. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author contributions
JK wrote most of the data-analysis, theoretical part, introduction methods and materials, and conclusions. JP wrote some parts and commented on the data-analysis, helped with theoretical part, and conclusions. All authors contributed to the article and approved the submitted version.
Funding
Funding from the Finnish academy project Touch and Affect in Health Care Interaction and from the Tampere University Library for the publication fees is gratefully acknowledged.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^The researchers are not in agreement if the stepping response can be called a reflex or not (see e.g. Barbu-Roth et al., 2009).
References
Barbu-Roth, M., Anderson, D. I., Desprès, A., Provasi, J., Cabrol, D., and Campos, J. J. (2009). Neonatal stepping in relation to terrestrial optic flow. Child Dev. 80, 8–14. doi: 10.1111/j.1467-8624.2008.01241.x
Behnke, E. A. (1997). Ghost gestures: phenomenological investigations of bodily micromovements and their intercorporeal implications. Hum. Studies. 20, 181–201. doi: 10.1023/A:1005372501258
Behnke, E. A. (2008). Interkinaesthetic affectivity: a phenomenological approach. Cont. Philos. Rev. 41, 143–161. doi: 10.1007/s11007-008-9074-9
Cautilli, J. D., and Dziewolska, H. (2006). Brief report: the use of opportunity to respond and practice to increase efficiency of the stepping reflex in a five-month-old infant. Behav. Anal. Today. 7, 538–547. doi: 10.1037/h0100088
Cekaite, A. (2010). Shepherding the child: embodied directive sequences in parent-child interactions. Text and Talk. 30, 1–25. doi: 10.1515/text.2010.001
Cuffari, E., and Streeck, J. (2017). “Taking the world by hand,” in Intercorporeality: Beyond the Body, Meyer, C., Streeck, J., and Scott Jordan, J. (eds). (Oxford: Oxford University Press) p. 173–201. doi: 10.1093/acprof:oso/9780190210465.003.0007
Fernald, A. (1985). Four- month-old infants prefer to listen to motherese. Infant Behav. Dev. 8, 181–195. doi: 10.1016/S0163-6383(85)80005-9
Forssberg, H. (1985). Ontogeny of human locomotor control I. Infant stepping, supported locomotion and transition to independent locomotion. Experimental Brain Research. 57, 480–495.
Fuchs, T. (2017). “Intercorporeality and Interaffectivity,” in Intercorporeality: Emerging Socialities in Interaction, Meyer, C., Streeck, J., and Scott Jordan, J. (eds). (Oxford: Oxford University Press) p. 3–23. doi: 10.1093/acprof:oso/9780190210465.003.0001
Goodwin, C. (1994). Professional vision. Am. Anthropol. 96, 606–633. doi: 10.1525/aa.1994.96.3.02a00100
Goodwin, C. (2007). “Environmentally coupled gestures,” in Gesture and the Dynamic Dimensions of Language, Duncan, S., Cassell, J., and Levy, E. (eds). (Amsterdam and Philadelphia: John Benjamins) p. 195–212. doi: 10.1075/gs.1.18goo
Goodwin, C. (2018). Co-operative Action. Cambridge: Cambridge University Press. doi: 10.1017/9781139016735
Goodwin, C., and Goodwin, M. H. (2004). “Participation,” in Companion to Linguistic Anthropology, Duranti, A. (ed). (Oxford: Basil Blackwell) p. 222–244. doi: 10.1002/9780470996522.ch10
Goodwin, M. H., and Cekaite, A. (2018). Embodied Family Choreography: Practices of Control, Care, and Mundane Creativity. Oxford and New York: Routledge. doi: 10.4324/9781315207773
Guo, E., Katila, J., and Streeck, J. (2020). Touch and the fluctuation of agency and motor control in pediatric dentistry. Social interact. 3. doi: 10.7146/si.v3i1.120249
Heath, C. (1986). Body Movement and Speech in Medical Interaction. Cambridge: Cambridge University Press. doi: 10.1017/CBO9780511628221
Heath, C. (2006). “Body work: the collaborative production of the clinical object,” in Communication in medical care: Interaction between primary care physicians and patients, Heritage, J., and Maynard, D. W. (eds). (Cambridge: Cambridge University Press). p. 185–213. doi: 10.1017/CBO9780511607172.009
Homanen, R. (2013). Doing pregnancy, the unborn, and the maternity healthcare institution. [Dissertation]. Tampere: Tampere University Press
Howes, D. (2005). “Introduction: Empires of the Senses,” in Empire of the Senses: The Sensual Culture Reader, Howes, D.(ed). Oxford: Berg. p. 1–20. doi: 10.4324/9781003230700-1
Ijäs-Kallio, T., Ruusuvuori, J., and Peräkyl,ä, A. (2011). Unilateral decision making and patient participation in primary care. Commun. Med. 8,145–155. doi: 10.1558/cam.v8i2.145
Jefferson, G. (2004). “A sketch of some orderly aspects of overlap in conversation,” in Conversation Analysis: Studies from the First Generation, Lerner, G. (ed). (Amsterdam: Benjamins) p. 43–59. doi: 10.1075/pbns.125.05jef
Katila, J. (2018). Tactile intercorporeality in a group of mothers and their children: a micro study of practices for intimacy and participation. [Dissertation]. Tampere: Tampere University Press.
Katila, J., and Philipsen, J. S. (2019). The intercorporeality of closing a curtain: sharing similar past experiences in interaction. Pragmatics Cognit. 26, 167–196. doi: 10.1075/pc.19030.kat
Katila, J., and Raudaskoski, S. (2020). Interaction analysis as an embodied and interactive process: multimodal, co-operative, and intercorporeal ways of seeing video data as complementary professional visions. Hum. Stud. 43, 445–470. doi: 10.1007/s10746-020-09553-4
Katila, J., and Turja, T. (2021). Capturing the nurse's kinesthetic experience of wearing an exoskeleton: The benefits of using intercorporeal perspective to video analysis. Social Interact. 4(3). doi: 10.7146/si.v4i3.128149
Kuroshima, S. (2020). Therapist and patient accountability through tactility and sensation in medical massage sessions. Social Interact. 3. doi: 10.7146/si.v3i1.120251
Merleau-Ponty, M. (1968). The Visible and the Invisible (A. Lingis, Trans.). Evanston: Northwestern University Press.
Merlino, S. (2020). “Professional touch in speech and language therapy for the treatment of post-stroke aphasia,” in Touch in Social Interaction Touch, Language, and Body, Cekaite, A., and Lorenza, M. (eds) (Milton: Taylor and Francis) p. 197–223. doi: 10.4324/9781003026631-9
Meyer, C., Streeck, J., and Jordan, S. J. (2017). “Introduction,” in Intercorporeality: Emerging Socialities in Interaction, Meyer, C., Streeck, J., and Scott Jordan, J. (eeds). (Oxford: Oxford University Press). doi: 10.1093/acprof:oso/9780190210465.001.0001
Meyer, C., and Wedelstaedt, U. V. (2017). “Intercorporeality, interkinesthesia, and enaction: new perspectives on moving bodies in interaction,” in Moving Bodies in Interaction - Interacting Bodies in Motion: Intercorporeality, Interkinaesthesia, and Enaction in Sports, Meyer C. Wedelstaedt U. V.(eds). (Amsterdam: John Benjamins Publishing Company). 1–45. doi: 10.1075/ais.8
Mondada, L. (2020). Sensorial Practices of food: how professionals and amateurs touch cheese in gourmet shops,” in Touch in Social Interaction Touch, Language, and Body, Cekaite, A., and Lorenza, M. (eds) (Milton: Taylor and Francis) p. 288–310. doi: 10.4324/9781003026631-13
Mononen, K. (2019). Embodied care: affective touch as a facilitating resource for interaction between caregivers and residents in a care home for older adults. Linguistics Vanguard. 5. doi: 10.1515/lingvan-2018-0036
Nishizaka, A. (2007). Hand touching hand: referential practice at a Japanese midwife house. Hum. Stud. 30, 199–217. doi: 10.1007/s10746-007-9059-4
Parry, R. (2017). “Distribution of agency across body and self,” in Distributed Agency, Enfield, N., and Kockelman, P. (eds). (Oxford: Oxford University Press) p. 119–129. doi: 10.1093/acprof:oso/9780190457204.003.0013
Paterson, M. (2005). “Affecting touch: towards a felt phenomenology of therapeutic touch,” in Emotional Geographies, Davidson, J., Bondi, L., Smith, M. (eds) (Aldershot: Ashgate) p. 161–176.
Philipsen, J. S., and Katila, J. (2021). Interkinesthesia in psychotherapy: a resource for exploring body memories and learning new ways of making-a-body. Body Mov. Dance Psychother. 16, 302–317 doi: 10.1080/17432979.2021.1914731
Philipsen, J. S., and Trasmundi, S. B. (2019). Gesture reuse as distributed embodied cognition. Gesture. 18, 1–30. doi: 10.1075/gest.00031.phi
Raia, F., Goodwin, M. H., and Deng, M. (2020). Forms of touch during medical encounters with an advanced heart failure (AdHF) doctor who practices relational medicine. Social Interact. 3. doi: 10.7146/si.v3i1.120259
Raudaskoski, P. (2020). Participant status through touch-in-interaction in a residential home for people with acquired brain injury. Social Interact. 3. doi: 10.7146/si.v3i1.120269
Roald, T., Kasper, L., and Køppe, S. (2018). Affective incarnations: Maurice Merleau-Ponty's challenge to bodily theories of emotion. J. Theoretical Philosophical Psychol. 38, 205–218. doi: 10.1037/teo0000101
Routasalo, P. (1999). Physical touch in nursing studies: a literature review. J. Adv. Nurs. 30, 843–850. doi: 10.1046/j.1365-2648.1999.01156.x
Ruusuvuori, J., Lindfors, P., Homanen, R., Haverinen, S., Lehtonen, H., and Keskinen, K. (2008). Ennaltaehkäisevä terveystyö neuvolassa: Muuttuva asiakassuhde, tiimityö ja 81 hyvinvointineuvolamalli. Hyvinvointipalvelujen julkaisuja 7/2008. Tampere: Tampereen kaupunki, Tietotuotanto ja laadunarviointi.
Schindler, L. (2017). “Teaching Bodies: Visual and Haptic Communication in Martial Arts,” in Moving Bodies in Interaction - Interacting Bodies in Motion: Intercorporeality, Interkinaesthesia, and Enaction in Sports, Meyer, C., and Wedelstaedt, U. V. (eds) (Amsterdam: John Benjamins Publishing Company) p. 424–462.
Sheets-Johnstone, M. (2002). Relationality and caring: an ontogenetic and phylogenetic perspective. J. Philosophy Sport. 29, 136–148. doi: 10.1080/00948705.2002.9714630
Sheets-Johnstone, M. (2011). Primacy of Movement, 2nd ed. Amsterdam: John Benjamins. doi: 10.1075/aicr.82
Streeck, J. (2013). ‘Interaction and the living body'. J. Pragmat. 46, 69–90. doi: 10.1016/j.pragma.2012.10.010
Streeck, J., Goodwin, C., and LeBaron, C. (2011). “Embodied interaction in the material world: an introduction,” in Embodied Interaction: Language and Body in the Material World, Streeck J. Goodwin C. LeBaron C.(Cambridge: Cambridge University Press) p. 1–26.
Stuart, S. A. J. (2012). “Enkinaesthesia: the essential sensuous background for co-agency,” in Z. Knowing Without Thinking: Mind, Action, Cognition and the Phenomenon of the Background, Radman, H., and Basingstoke, H. (eds) (Palgrave Macmillan) p. 167–186. doi: 10.1057/9780230368064_9
Thelen, E., and Cooke, D. W. (1987). Relationship between newborn stepping and later walking: a new interpretation. Dev. Med. Child Neurol. 29, 380–393. doi: 10.1111/j.1469-8749.1987.tb02492.x
Thelen, E., and Fisher, D. M. (1982). Newborn stepping: an explanation for a “disappearing” reflex. Dev. Psychol. 18, 760–775. doi: 10.1037/0012-1649.18.5.760
Twigg, J., Wolkowitz, C., Cohen, R. L., and Nettleton, S. (2011). Conceptualising body work in health and social care. Sociol. Health Illn. 33, 171–188. doi: 10.1111/j.1467-9566.2010.01323.x
Ulrich, D. A., Beverly, D. U., Rosa, M. A.-K., and Joonkoo, Y. (2001). Treadmill training of infants with down syndrome: evidence-based developmental outcomes. Pediatrics. 108, 1–7. doi: 10.1542/peds.108.5.e84
Van Dongen, E., and Elema, R. (2001). The art of touching: The culture of ‘body work' in nursing. Anthropol. Med. 8, 149–162. doi: 10.1080/13648470120101345
Watson, W. H. (1975). The meanings of touch: geriatric nursing. J. Communicat. 25, 104–112. doi: 10.1111/j.1460-2466.1975.tb00611.x
Wedelstaedt, U. V., and Meyer, C. (2017). “Intercorporeality and Interkinesthetic Gestalts in Handball,” in Moving Bodies in Interaction - Interacting Bodies in Motion: Intercorporeality, Interkinaesthesia, and Enaction in Sports, Meyer, C., and Wedelstaedt, U. V. (eds) (Amsterdam: John Benjamins Publishing Company) p. 98–159. doi: 10.1075/ais.8.03vwe
Appendix
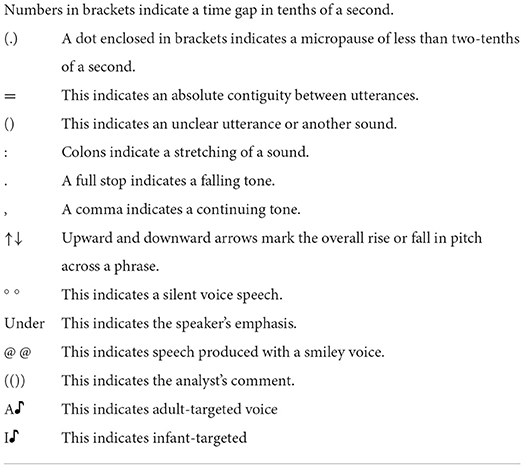
Table A1. The transcription conventions used in the conversations.
Keywords: interkinesthesia, touch, professional vision, intercorporeality, infant reflexes, nurse's bodywork, video analysis, embodied interaction
Citation: Katila J and Philipsen JS (2022) Forms of professional interkinesthesia in nurses' body work: A case study of an infant's stepping. Front. Commun. 7:954483. doi: 10.3389/fcomm.2022.954483
Received: 27 May 2022; Accepted: 08 August 2022;
Published: 30 August 2022.
Edited by:
Arianna Maiorani, Loughborough University, United KingdomReviewed by:
Asta Cekaite, Linköping University, SwedenRebekah Wegener, University of Salzburg, Austria
Copyright © 2022 Katila and Philipsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia Katila, julia.katila@tuni.fi