“A hard-won capability”: the experiences of parents managing their babies' medicines after discharge from a neonatal unit
 Louise Bracken1*†
Louise Bracken1*†  Janet Clark1†
Janet Clark1†  Andrea Gill1†
Andrea Gill1†  Fiona O'Brien2†
Fiona O'Brien2†  Rachael Dewey1
Rachael Dewey1  Catrin Barker1
Catrin Barker1  Bernie Carter1,3
Bernie Carter1,3- 1Paediatric Medicines Research Unit, Alder Hey Children's NHS Foundation Trust, Liverpool, United Kingdom
- 2Royal College of Surgeons in Ireland, Dublin, Ireland
- 3Faculty of Health, Social Care and Medicine, Edge Hill University, Ormskirk, United Kingdom
Introduction: Parents of babies who required neonatal care are responsible for managing their medicines after they are discharged home. There is wide variation in the information and amount of preparation given to parents prior to assuming this challenging task. The aim of the Parent co-Designed Drug Information for parents and Guardians Taking Neonates home (PADDINGToN) study was to explore parents' experiences of managing their babies' medicines post discharge from a neonatal unit and to use this information to develop suitable resources for future families.
Methods: A qualitative participatory interpretative approach using a mixture of remote and face-to-face small group interviews or one-to-one interviews was used. Parents were recruited using social media advertisements and convenience sampling from five study sites (four neonatal units in England and one in Ireland). Parents from other neonatal units were invited to take part through social media advertisement. The interviews were audio-recorded and inductive reflexive thematic analysis was used to analyze the data.
Results: 17 parents (14 mothers, 3 fathers) participated. One over-arching theme, 'A hard won capability', and four major interpretive themes were generated from the analysis of the data: Being in NICU and the prospect of going home: emotional and practical challenges; Living the reality of being at home: the uncertainty associated with giving medicines; Being at home: battling the system and a lack of support/knowledge; and Suggesting ways forward: parents' lived insights into improving information and resources.
Conclusion: Despite the challenges they faced, parents developed strategies for safely and reliably managing medicines administration and they assimilated knowledge, built their confidence and achieved a capability in medicines administration. Their experiences have been used to build a suite of medicines administration resources to support future parents.
1. Introduction
Over 90,000 babies are cared for in neonatal units in the UK and Ireland annually (BLISS, 2022). This means that approximately one in seven babies will require neonatal care because they are born too early, have too low a birth weight, or have a medical condition that needs specialist treatment (HQIP Ra, 2022). This specialist treatment often involves complex medication regimens and is associated with the risk of medication errors. The medication-use process within the Neonatal Intensive Care Unit (NICU) is complex including the use of off-label and licensed medications (Costa et al., 2018; Reis et al., 2021). As medication administration has the potential for considerable consequences if errors occur (Krzyzaniak and Bajorek, 2016), this has been described as being particularly worrisome (Krzyzaniak and Bajorek, 2016; Henry Basil et al., 2022). Medication error rates in NICU are reported as ranging from 4 to 35.1 per 1000 patient days (Alghamdi et al., 2019).
At discharge home, 28% of babies born prematurely are prescribed more than three medicines with the median number of medicines per patient at discharge being 2.5 (range 2–7) (Morris and Johnson, 2019). Family Integrated Care (FICare) encourages parents to give medicines in the hospital, thus preparing them for discharge home. However, even in NICUs with established FICare programs, there is variability in approach. As the establishment of FICare programs is not a widespread practice, most medicines are still given by nurses (Griffin and Abraham, 2006; Berman et al., 2019; Murray et al., 2022). Murray et al. (2022) explored the views of parents and healthcare professionals (HCPs) around parent-led administration in the NICU. HCPs acknowledged the need for parents to take an active role but had some concerns about the practicalities and accountability of parents administering doses in the NICU. The study identified the need for clear guidance to facilitate parent participation while ensuring patient safety. Morris and Johnson (2019) reported similar findings with nursing staff wanting clear documentation to ensure accountability for who was responsible for administering medicines and the need for a communication process with parents around any prescription changes. Once at home, the responsibility for medicine administration falls on parents (BLISS, 2022), and findings show that the frequency that parents administer medicines at home is increasing (Team PaM, 2017). There are many factors contributing to this trend including improving survival from serious health problems, the increasing use of medicines to treat health problems, and the desire to move the delivery of care closer to home. A systematic review of carers for all ages has estimated the median rate of medication errors and unintentional medication discrepancies for adults following discharge was 53% (Alqenae et al., 2020). The frequency of pediatric medication errors by parents or carers at home varies from 30 to 80% with risks depending on caregiver characteristics and whether the prescription contains ≥3 drugs (Lopez-Pineda et al., 2022). In cases where a parent was responsible for the administration of medicines to infants born prematurely, the overall administration error rate was 66.3%, with the most common error (54%) being the measurement of a dose that differed from the prescription (54%) (Solanki et al., 2017).
Research has shown that about a quarter of all families who start a new medicine experience a problem when administering their medicine within the first month (Conroy and McIntyre, 2005). This is perhaps unsurprising as there is variation in both the information supplied before discharge and the support given to parents in the administration of medications. There is a deficit in studies focusing on the support and preparation needed by parents of premature babies, so they can effectively, safely, and confidently undertake medicine management at home.
This study reports on findings from focus groups with parents that were part of a larger mixed-methods study Parent co-Designed Drug Information for parents and Guardians Taking Neonates home (PADDINGToN) that focused on co-designing drug information for parents taking neonates home from neonatal units.
The broad aim of this sub-study was to explore parents' experiences of medicine management of their baby post-discharge from neonatal units. The particular focus was the information and preparation they received about medicines before discharge and whether there were any gaps in the information or preparation provided. How they addressed such challenges and their suggestions for improving practice were also explored.
2. Methods
This study used a qualitative participatory interpretative approach using face-to-face and remote small group or one-to-one interviews. It was conducted in accordance with Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Tong et al., 2007). A participatory approach was core to the study. Parent participation was evident through the engagement with two very active parent representatives in the study management group. These parents provided sustained and invaluable insight and guidance to the design of the overall study. They contributed to the structure, content, and wording of the questionnaires, interviews, focus groups, and information sheets and were directly involved in the co-design workshops which formed the final stage of the study (not reported in this study) (Davies et al., 2019). These co-design workshops involved a larger group of parents and developed the medical information resources. A group of 22 HCPs and a new group of parents (n = 26) who were not involved in the initial co-design reviewed the resources to refine factors such as content, layout, and appearance of the resources.
Ethics approval was gained via the London—Bloomsbury Research Ethics Committee (IRAS ID: 21/LO/0351) and the Rotunda Hospital Ethics Committee (REC-2021-O13).
2.1. Recruitment and consent
Parents were identified via social media advertisements and the five participating study sites: three in the north-west of England, one in the north of England, and one in Ireland. Inclusion criteria were parents (aged ≥ 16 years) of babies receiving care or discharged within the last 5 years from a neonatal unit who will/did require medication to be continued after discharge from the hospital. Exclusion criteria included parents/carers who do not speak English. Researchers confirmed appropriateness and eligibility with clinical teams before approaching potential participants. For parents of babies recruited via the study sites, researchers did not approach parents whose baby was considered unlikely to survive. Convenience sampling was used to recruit up to 25 participants who met the eligibility criteria. The window for recruitment was 4 months and this, along with COVID-19 pandemic restrictions, meant that the planned target of 25 participants was not achieved. However, the data were sufficiently rich to ensure the team was confident of the quality, breadth, and depth of the dataset. Written informed consent or e-consent for participation was taken by RD, JC, and AG and was undertaken either face-to-face or remotely by telephone or via a secure video platform (Zoom or Teams).
2.2. Small group and one-to-one semi-structured interview methods
Initially, the research plan had been to undertake focus groups as they are an ideal method of generating concentrated data on a topic through interaction between the participants and researcher to explore the differences and similarities between their experiences and contexts (Barbour, 2018; Morgan, 2019). However, the constraints imposed by the COVID-19 pandemic meant that it proved impossible for sufficient participants (around 5–8 parents) to be available to attend a remote (Zoom or Teams) or in-person group at the same time. Therefore, the method had to shift, and parents were invited to participate in remote or in-person small group or individual interviews. Some of the principles of focus groups remained in place (e.g., two researchers were involved in each interview; one taking the lead for asking questions and the other taking notes, providing additional support, and being alert to identifying any potential participant distress) (Liamputtong, 2011; Morgan, 2019). The emphasis in the interviews was on encouraging interaction, sharing experiences and ideas, and active listening.
The interviews were semi-structured. Short personal introductions by participants and researchers were followed by a discussion of the topic areas identified from the PADDINGToN e-survey to parents and HCPs. The small group and individual interviews were undertaken between December 2021 and March 2022 by RD, CB, LB, AG, and JC. The interviews were composed of five main sections: Section 1 focused on welcome, explanation, and then an opportunity for each parent to tell an outline story of their experience; Sections 2–4 focused on information about medicines (what information, when it had been given, and who gave the information); and Section 5 focused on recapping what had been discussed, checking-in to ensure parents were not upset and reminding parents about what to do if they were upset (see Supplementary material: Overview of interview structure).
Two researchers (LB and JC) have previous experience of undertaking qualitative interviews and three (RD, AG, and FO'B) had minimal experience. However, in preparation for undertaking the interviews, a qualitative researcher (BC) with extensive experience in undertaking small group and one-to-one interviews provided guidance and support via remote preparation and feedback sessions.
The interviews were digitally audio-recorded, and field notes were made to support the analysis of the data. The audio-recording notes from the chat rooms in Zoom or Teams and field notes were transcribed verbatim and analyzed using reflexive thematic analysis (Braun and Clarke, 2019). This analysis followed the five stages of inductive reflexive thematic analysis (familiarization, generating initial codes, searching for themes, reviewing themes, and producing reports), allowing the shift from descriptive to interpretative analysis (Braun and Clarke, 2021). Analysis was conducted by AG (female, academic, and clinical pediatric pharmacist), JC (female, children's research nurse), LB (female, PhD, academic pediatric pharmacist), FO'B (female, PhD, academic), and BC (female, PhD, academic children's nurse). Pseudonyms were applied alphabetically to parents.
3. Results
Seventeen parents (14 mothers and 3 fathers) participated; all had the experience of medicine management of their baby post-discharge from the NICU (see Table 1). Eleven parents were interviewed one-on-one, eight remotely, and three in cubicles on the ward. Six parents took part in small group interviews with two in each group; two group interviews were done remotely and one in a cubicle on the ward. Table 1 provides an overview of the characteristics of the parents and their babies. Five parents were recruited via social media and 12 (out of 27 parents approached) by research staff at the hospital sites.
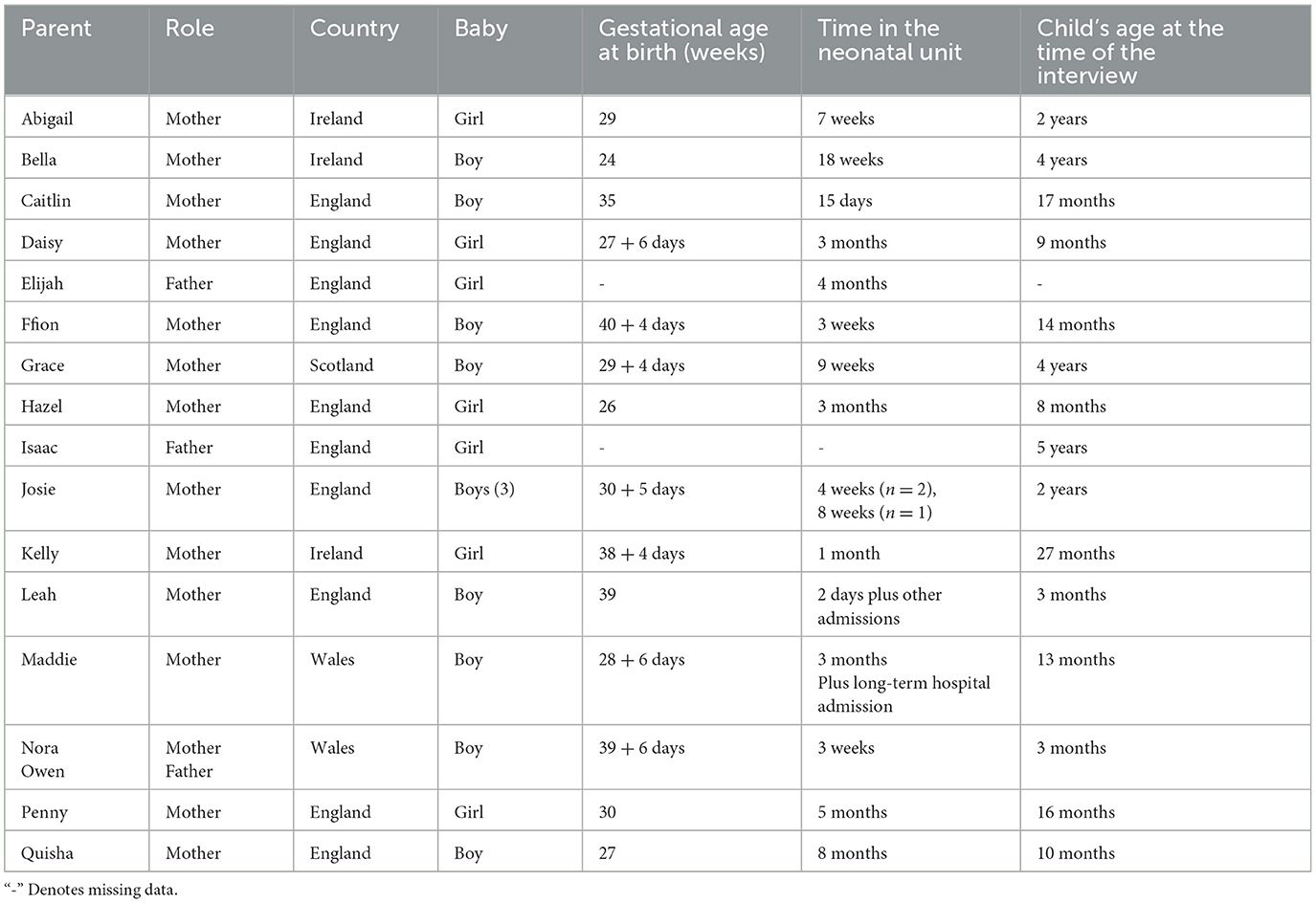
Table 1. Characteristics of parents and babies.
The interviews (one-to-one or small group) lasted 18 to 93 min (an average of 35 min). Illustrative quotations are used throughout to support the findings.
One overarching interpretive theme, “A hard won capability,” and four major themes were generated from the analysis of the data (see Figure 1). While each of these major themes is distinct, they each inform and relate to each other. The themes are:
• Being in NICU and the prospect of going home: emotional and practical challenges
• Living the reality of being at home: the uncertainty associated with giving medicines
• Being at home: battling the system and a lack of support/knowledge
• Suggesting ways forward: parents' lived insights into improving information and resources.
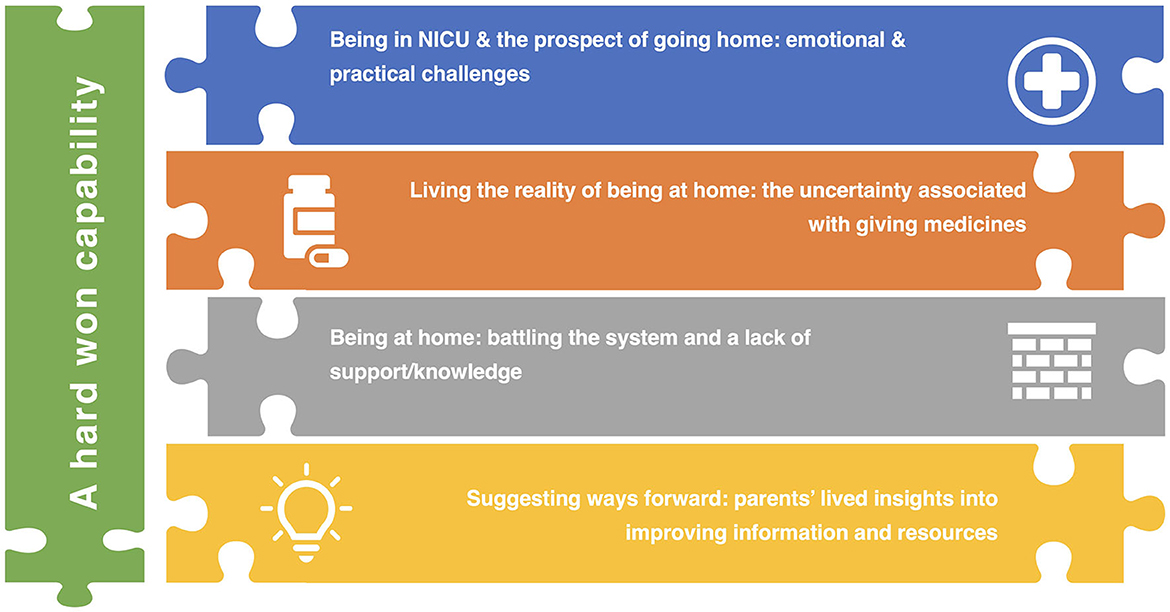
Figure 1. Overview of overarching and major themes.
The overarching theme, “A hard won capability,” reflects the challenges faced, the skills and knowledge, and the strategies used and proposed in relation to parents' experiences of medicine management of their baby post-discharge from the NICU. Additional illustrative quotes are presented in Table 2.

Table 2. Additional illustrative quotations.
3.1. Theme 1: being in NICU and the prospect of going home: emotional and practical challenges
Within this theme, parents' responses to and the emotions evoked by their baby's admission to NICU and subsequent discharge home are explored. The initial experiences of being in the NICU provide the context for their experiences of taking their baby home. The NICU was described as “a shell shocking…. [and] terrifying environment be in” (Abigail). Quisha described herself as being “really scared” and noted that this was heightened because her “English is not so good.” Typically, parents described their baby's trajectory through NICU as being a “very up and down journey” (Bella) with a sense of fear of what would happen next. Parents often were torn between feeling they needed to be in the NICU and also pulled by their responsibilities at home; this was particularly challenging for parents with other children. Abigail explained, “really my mind was everywhere you know.” The pull to go home was strong and for some parents, this superseded any other considerations:
“I didn't care what they gave me to come home…. …. If I was giving her medication for every half an hour, I wouldn't have cared. Just get me home!” (Kelly).
Although some parents were given information about and opportunity to practice giving their baby medication, this was not the case for all. Grace said she thought that there was “an assumption that we kind of knew what we were doing.” Many parents had not been involved in learning about or giving their baby medications while they were in the hospital or where they had been, as the timing varied. This was seen as a missed opportunity, and Abigail explained that she “wasn't really hands-[on] involved in helping administer medication.” However, some parents were proactive about finding out about the medication their baby was prescribed. Bella explained she would regularly ask:
“What's this medicine for…what does it do… is that medicine stopped now?.... I just was afraid that something would be missed and ….I got very used to being very involved in the day-to-day” (Bella).
Parents were aware that giving medication required the acquisition of skill and confidence and that some medicine-related tasks could challenge health professionals. Josie reflected that when she saw a nurse “struggling,” she thought “if she doesn't know, how on earth am I gonna manage this at home?” (Josie). Hazel talked of the importance of practicing giving medicines before her baby was discharged home:
“It gives you that confidence… even it though it was sort of simple putting it in the bottle…. it is such a big scary thing with her being so small” (Hazel).
Parents experienced various levels of advice pre-discharge ranging from “nothing…. they literally put them into a bag handed them to me and off we went” (Abigail) through to being given “a piece of paper and it was like ‘there's dosage, off you go”' (Bella), to a schedule (timetable) of medicines. Elijah was positive as he explained “we were given time to practice.” Some parents were exposed to more detailed information supported by videos, demonstrations by the nurse, support from a specialist, and links to websites. However, typically this is related to the management of equipment (e.g., PEG tubes) rather than medication. Bella said that “the hospital should be more aware of the holistic needs that a family has instead of just focusing on maybe just the baby's needs.”
3.2. Theme 2: living the reality of being at home: the uncertainty associated with giving medicines
For many parents, the joy of being at home was muted by the sudden realization that giving their baby medication was complicated, and many talked of being terrified by the responsibility of the role and the potential for error. Daisy explained, “trust me…. I didn't think it would be this hard.” Josie summed up her terror, explaining:
“When your babies are premature, you're terrified of everything, so you do exactly what you're told … I remember thinking ‘I'm really daunted by this, I do not know what I'm doing” (Josie).
Another mother talked of initially “being confused… [having to do] everything yourself ” (Quisha). Caitlin talked of the pressure to ensure her baby “had exactly the right amount of milk and medicine.” However, parents instigated strategies to help them cope with the stress and challenge and support their proficiency and capability. Ffion explained, “we worked out what worked for us.” Typically, this involved creating a schedule or a list to keep things on track as one of the mothers explained:
“I just did my own [list]…I'll have morning meds in one section and then like the afternoon's and then at night. So I did just write everyday morning, afternoon, night and then every day when I've given it I just cross it off so I know I've done it” (Penny).
Some parents talked of the role of giving medication made them feel initially more like “a nurse… [although acknowledged that] over time I turned into a parent” (Bella). Most responsibility fell on the mothers as any information shared had usually been shared solely with the mothers.
Most parents second-guessed themselves and at times, worried about “have I done this right”? (Josie). The fear of over dosage was visceral, Bella explained, “I was terrified of giving the wrong amount,” and parents were concerned about the consequences of under dosing or omitting doses:
“We were never given the, I suppose the comfort, that if he doesn't have it, what it could do, what to look out for. For those 4 days we were on tenterhooks” (Nora).
Some parents put checking processes in place to reduce the risk similar to those they had witnessed in the hospital. Quisha explained, “I tell my husband come check it … check if I am right… I don't wanna give him more or less.”
Parents were vigilant about giving medicines, and some were concerned about not knowing about potential “side effects” (Bella) and “I didn't know it wasn't licensed for children” (Kelly). Information about potential adverse effects did not appear to be routinely shared with parents:
“We were given the prescription, and it was literally on a notepad paper the nurse wrote it down from obviously her own file. And it was like… there you go… so nothing about side effects” (Abigail).
Other concerns related to whether medicines could or should be prioritized or what to do if a dose was missed and that this could create a sense of “panic” (Josie).
3.3. Theme 3: being at home: battling the system and a lack of support/knowledge
For some parents, battles with the system started before their baby was discharged. This was most obvious in the families living in Ireland where financial aspects of the health system added complexity. Abigail recalled “fighting for everything… [and being] the only one in the battle.”
All parents talked of the challenges of managing medicines at home; this was especially complicated with the interplay of different medications. For some babies, this could be compounded by parents having to consider their babies' oxygen therapy requirements. Bella sums this dilemma up:
“I was constantly over analyzing… Was that a side effect of the medication? Is that normal? Is he lacking oxygen? Do I need to increase the oxygen? I didn't know, I wasn't confident” (Bella).
Changes to medication or the form in which the medication was dispensed could create additional challenges and make parents doubt themselves. Quisha's capability was diminished when the sildenafil she had ordered as a repeat prescription was sent to her in powder form, as she was used to it being made up for her as a liquid and she did not know “how to mix this or what do I need to put in there.” Quisha eventually gained the advice she needed from the hospital pharmacist. Some parents were disconcerted when the brand of medication they were used to and trusted was changed without explanation. Another aspect of medicine administration that created challenges was when the route was changed meaning parents felt unsure about how to translate prior learning to a new situation:
“I only ever saw them put it in through that [nasogastric tube]. And of course, putting it into his mouth is totally different. So I used to mix it in with milk but again I was like ‘Does it matter if it's warm or does that affect the medicine?' I wasn't sure” (Josie).
Sustaining supplies of medications was often complex. One mother recalled how “we were never given information on how to get [ongoing supplies] ourselves” (Nora). Another parent talked of how the medications were “a pain to get hold of ” (Penny), especially when it was not clear who had responsibility for prescribing, the delays this could create, and the number of calls she had to make. Abigail recalled the stress associated with getting medication dispensed:
“I remember having nearly a meltdown in the chemist. Like how hard is it to order this brand? And they were like ‘Well that one costs 350 euro, to order you need to ring the DPS scheme'. And I was like ‘None of that was relayed to me” (Abigail).
This stress needs to be considered in the context of the parents already having to deal with so many factors caring for their premature baby at home; typically, parents talk of being “so busy with him, there's so much work” (Quisha). Nora summed up many parents' experiences saying:
“When you're going home with the baby that's poorly you don't need to be chasing other professionals” (Nora).
The challenges of medicine management were compounded by a sense of isolation from people who could provide clear advice, support, and reassurance and explain “don't worry about it, it's absolutely fine” (Josie).
For some parents, the professionals such as General Practitioners (GPs) and other community health professionals to whom they turned for help and had little knowledge of the medications or the needs of their baby. Caitlin talked about the problems this created:
“We've been sent home a few times from hospital… with medicines for the GP to continue [and] the GP's been a bit unsure about what they've told us to do... It's hard when it's just a piece of paper to show them” (Caitlin).
Hazel echoed these concerns. Parents were sometimes positioned as the person apparently expected to, and capable of, being the conduit between the hospital and community; this taxed their own understanding and was stressful. Isaac suggested “a linked up IT system” was needed to support communication. Being at home and being expected to know what to do was at odds with the relatively sheltered experience of being in the hospital, where skilled and knowledgeable help was readily available. Without access to knowledgeable HCPs, some parents turned to the internet, although this had limited value and was not trusted. As Kelly explained, “every website seems to have health written in it, but you don't actually know whether it's factual or not.” Grace wanted real information rather than “just kind of Googling …or TikTok.” Other parents also talked of the responsibility placed on them to ensure their GP was informed of the medications their baby was prescribed; this was deemed to be unreasonable. Reasons for this included the GP letter being lost requiring the parent to fill in the gap by going to see their GP. Penny explained that “if you haven't got all of them bottles, you don't know [what to tell the GP].” Owen made his feelings clear:
“I think it's the reliance on the parents … to make sure that all the information, the finding of the GPs, the online patient's script, whatever, the initial one done, that the responsibility is put on the parents and it's not possible” (Owen).
For some parents, their sense of responsibility also included checking whether the medication should be stopped or continued. Kelly recalled her actions:
“So I just kind of stopped them [spironolactone and furosemide] naturally myself, but nobody had told me to stop them bar the nurse kind of mentioning it in passing” (Kelly).
3.4. Theme 4: suggesting ways forward: parents' lived insights into improving information and resources
Although there were examples of good practices relating to informing parents and promoting skills and confidence relating to medicine management, many parents felt ill-prepared and ill-equipped to be capable, confident, skillful, and informed. One mother reflected on the lack of priority given to medicine management, recalling:
“We did have a CPR class… so I don't see why they can't do medication administration class and support” (Abigail).
Based on their experiences and their reflections, parents were able to provide clear ideas about ways in which HCPs in the neonatal unit could better help them prepare to manage their babies' medicines at home.
At a minimum, processes need to improve on the experiences many parents described as just being “given your medicines and basically off you pop get on with it” (Penny) or information “done to tick a box as opposed to meaningful engagement to support the parent” (Bella). Daisy suggested a system to help remind parents about when to give medicines as she sometimes “forgot” to give a dose.
Three key aspects were identified: more consistent, better-timed, and more clearly presented and useful information shared with both parents, who should provide the information and opportunity to practice.
Even parents who felt that “on the whole [preparation] was fine” (Caitlin) still talked of having some questions they would have liked to ask pre-discharge:
“We were giving [multivitamins] to him in his milk. I wasn't 100% [sure]… when I got home whether it was okay to put the other [medicines] in his milk” (Caitlin).
Other parents recalled feeling overwhelmed by input and information on the neonatal unit but not being able to take it in or recall it accurately. The timing of information was also important as information given at the start of the neonatal unit journey might not seem important until they were discharged. Abigail had forgotten about the booklet they had been given soon after admission and only came across it under her bed (where her husband had put it) when she was tidying things up at home. Grace said that for her the right time was “the days leading up to the discharge.”
Caitlin emphasized the importance of information being shared and returned to during their stay in the neonatal unit as “the more you see and hear something, the more it kind of sinks in.” Caitlin also thought that HCPs should include her husband noting that it would have been “helpful… when my husband had come to pick us up, they'd [HCPs] done a run with us there together.” Quisha talked of how she sometimes missed out on being able to talk to the doctors “because I couldn't go early morning” when they did the ward round. Elijah talked about sharing information was important since he and his wife “shared responsibilities [for medicine administration].”
Verbal information was valued as it engendered confidence and the HCP could provide additional explanation and reassurance and tell you:
“Don't forget or don't mind about this one... Like this is the big one or the serious one and just make sure administer it in the morning” (Bella).
Structured, planned written information (either in a group or one-to-one) was perceived as being valuable as it provided a backup or reminder; suggestions included “some sort of written plan” (Nora) or a “logbook” (Abigail). Parents suggested that this structured information should contain information including the timing of medication, dosage, administration, adverse effects, and which medications were the most important. This could be done one-on-one or in a group. This would both inform parents and would be useful when parents were engaging with community-based HCPs to improve communication and reduce the need for having “to check with the hospital” (Penny). However, parents warned against too much detail. Kelly explained she “probably wouldn't have wanted to know everything,” whereas another mother explained:
“I'm not gonna sit through and read through all this about where it was manufactured and who did x y and z. But a really simple sheet without too much written on it [would be helpful]” (Caitlin).
This mother further explained that the sheet could also contain contact information as this could reduce worry about who to contact and whether this contact was legitimate. Another benefit of written information was that it allowed parents to go through the information at their own pace with the chance to “get your head [round it]” (Josie).
Parents also wanted information and skills acquisition to be offered and available to their partners, noting it “would be nice to know that [partner] had a resource” (Kelly). Some parents talked of storing up questions to ask their consultant at the next clinic visit as they were unconvinced they would get clear or informed replies from community-based HCPs. However, as Bella explained, the consultant indicated that these were questions the GP should be answering. Bella's response was “I know, but you're the one who knows [baby's name] the best, so that's what we were doing.”
While parents thought that the consultants and doctors were knowledgeable, it was suggested that they “might not necessarily have the personal touch….. they're very textbook.. they can sometimes be a little bit cold [whereas] the nurses are extremely warm” (Bella). Caitlin agreed that information would be best shared “by the nurses and the healthcare assistants…..the ones that were caring for [baby's name] day-to-day.” Although hospital pharmacists were perceived to be experts and “good at their jobs,” they were thought of as being “more removed” (Bella), so less likely to be involved in giving medicine management advice pre-discharge.
Many parents wanted to have been able to practice giving medications before discharge as they recognized that this task was a “massive responsibility” (Nora). This was not routinely done on the neonatal unit and typically, parents had minimal or no opportunity to practice before discharge. Isaac suggested that it would help if they had “been witnessed when [they] were administering medication.”
4. Discussion
The study aimed to explore parents' experiences of medicine management of their baby post-discharge from the NICU. The findings clearly show that parents acquired the skills and knowledge they needed to become capable of the challenging task of administering medicines to their babies. The term capable infers the “ability or power to do something,” and to a greater or lesser extent, parents' power or ability to manage medicines was constrained due to various factors including stress, lack of preparation and information about medicine management, uncertainty related to medicine management, communication problems, and lack of support within the community. Despite these challenges, parents developed strategies for safely and reliably managing medicine administration and they assimilated knowledge, built their confidence, and achieved a capability in medicine administration, albeit that this was “a hard-won capability.”
Parents talked of the stress they experienced while their baby was in the neonatal unit and their experiences aligned with the experiences of other parents as evidenced in studies and systematic reviews (Cheng et al., 2019; Ding et al., 2019; Caporali et al., 2020; Adams et al., 2022). The alteration of parental role has been identified within the global literature as a source of stress for mothers and fathers in neonatal units (Caporali et al., 2020). Lack of parental involvement and engagement in caregiving while in neonatal units and during the discharge process impedes parents' preparedness to care for their infant at home (Caporali et al., 2020; Hebballi et al., 2021). Despite longing to go home, parents must accommodate the transition from the high initial stress of the neonatal environment to a similarly stressful environment of being at home and responsible for administering medicines. This is compounded by their awareness that their baby is small and fragile (Lakshmanan et al., 2019).
Typically, parents' knowledge and skills were acquired in an ad hoc manner, with little formal education and preparation from HCPs before discharge from the neonatal unit. The need for planned support, information, and preparation for transition is identified in other studies as being important (Lakshmanan et al., 2019; HQIP Ra, 2022). There is good evidence that family-centered care and education within the NICU can empower parents and improve their skills and knowledge (Ding et al., 2019). Family-integrated care can also reduce maternal stress (Cheng et al., 2019). However, there is little evidence that such programs and approaches are addressing medication administration. Most medication administration in the NICU remains nurse-led (Murray et al., 2022). Where education on medicine administration does not occur, parents must rely on other ways of acquiring knowledge and skills. As seen in other studies, a strong thread of experiential and reflective learning (Yardley et al., 2012; Carter et al., 2017) was evident in the way that parents talked about developing their ability to manage medicines. Their learning mostly occurred within the home, without support from HCPs, and was triggered by the requirement to develop their capacity to manage medicines safely.
The uncertainty associated with giving medicines and the fear of making a medication error was compounded by communication problems and a lack of support within the community. Parents in this study and other studies felt unsupported within the community and found the lack of expert advice compounded a sense of isolation and heightened their sense of responsibility to manage on their own or rely on asking hospital-based professionals for advice (Berman et al., 2019). Other studies have identified parents' role and the stress inherent in being expected to act as the go-between for information sharing and communication between professionals (Page et al., 2020).
Based on the insights from the parents in this study, and supported by literature specific to neonatal medication administration, the way forward would seem to be the implementation of a parent-led, participatory framework to support and educate parents about safely, capably, and confidently administering medicine (Murray et al., 2022). Robust written and verbal information for parents about medications can reduce the likelihood of errors (Ojha and Choonara, 2017).
Such an approach would build on the more in-depth evidence of the benefits provided by family-centered interventions to support parents in neonatal units (e.g., enhancing knowledge and skills) (Cheng et al., 2019; Ding et al., 2019). Although there is less evidence available on the impact of post-NICU discharge support and education interventions, multiple benefits for parents (e.g., increased competency and confidence) have been demonstrated (Griffith et al., 2022). As with parents in other studies, parents proposed improved engagement with community-based providers and services (Page et al., 2020; Lakshmanan et al., 2022). The strategies the parents proposed to improve their preparedness, confidence, and capability were based on their experiences and are ones that are relatively simple to implement. They are also evident in guidance on preventing home medication errors (Yin et al., 2014). They included better education and opportunity to practice, written information, and review of medication. Parents developed their own schedules for guiding their medicine administration. Other studies have shown aide-memories can be useful, although some concerns are raised about accuracy (Barber et al., 2014; O'Donovan et al., 2022).
The strengths of the study include the study design which encouraged the engagement and interaction of parents who were supported to share their experiences. The study also had some limitations. Parents who participated were predominantly mothers (only three fathers participated). Data were not collected on socioeconomic status, ethnic group, national identity, religion, and sexual or gender identity. The sample was not representative of the population as a whole; as such, the findings may not reflect parents from more vulnerable groups or in more marginal circumstances. The shift to small group or one-to-one interviews rather than using focus groups and the impact of COVID restrictions on face-to-face interactions reduced the opportunities for parents to interact with each other and share ideas; this may have limited the findings generated. While the majority of participants were recruited within 2 years from their neonatal discharge, a small number of participants (n = 4) were interviewed between 3 and 5 years post-discharge and therefore may not have had the same level of recall about their experience. Another limitation relates to the limited demographic data (e.g., birth weight, medical acuity, duration of admission, ethnicity, and socioeconomic status) routinely collected in this sub-study; this means that the influence of such factors on parent responses could not be considered.
5. Conclusion
Confidence and competence in medicine administration were “a hard-won capability” for the parents in this study. HCPs are well-positioned to support parents in preparation for discharge home. Preparation should include practice giving medicines, an overview of the practical issues they may face following discharge, and standardized written information, including how to obtain further supplies of medicines. Improved communication between hospital-based HCPs and those in the community would also help reduce difficulties for parents at this particularly vulnerable time.
Parents described both the weight of responsibility of giving medicines to their baby and their fear of making a mistake and the unknown consequences should this occur. Provision of simple medicine information, co-designed with parents, as early as possible before discharge, could provide reassurance and have the potential to make a huge difference. Standardizing this information across all neonatal units in the UK and Ireland, and in the community, could ensure a consistent message was provided to parents, no matter who provided this information.
A set of PADDINGToN resources have been co-designed with some of the parents involved in this study and will be made available.
Data availability statement
The datasets presented in this article are not readily available because of Ethics Committee restrictions. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the London—Bloomsbury Research Ethics Committee (IRAS ID: 21/LO/0351), the HRA and Health and Care Research Wales (HCRW), and the Rotunda Hospital Ethics Committee (REC-2021-O13). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AG, LB, FO'B, JC, and BC: idea for the article and data analysis. AG, LB, FO'B, JC, RD, and CB: design, implementation, and conducting the project. AG, LB, FO'B, JC, BC, RD, and CB: writing. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Neonatal and Paediatric Pharmacists Groups (NPPG).
Acknowledgments
The authors are grateful for the input and kind help of Rachel Corry, Julie Lalor, members of the PADDINGToN Study Management Group (Neil Caldwell, Cara Sutton, Kathryn Johnson, Brian Cleary, Fiona Gaffney, Naomi McCallion, Elaine Neary, Mark Turner), and Bliss (UK Charity) who circulated adverts. The authors are also grateful for the support provided by the clinical and research teams at the Rotunda Hospital-Dublin, Leeds General Infirmary, Alder Hey Children's NHSFT, Wirral Hospital, and Liverpool Women's Hospital.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomm.2023.1204599/full#supplementary-material
References
Adams, W. A., Malcolm, W., Goldstein, R., Lemmon, M. E., Mago-Shah, D., Cotten, M., et al. (2022). Longitudinal medical needs for periviable NICU survivors. Early Hum. Dev. 169, 105580. doi: 10.1016/j.earlhumdev.2022.105580
Alghamdi, A., Keers, A. R, N., Sutherland, A., and Ashcroft, D. M. (2019). Prevalence and nature of medication errors and preventable adverse drug events in paediatric and neonatal intensive care settings: a systematic review. Drug Safety 14, 1–14. doi: 10.1007/s40264-019-00856-9
Alqenae, F. A., Steinke, D., and Keers, R. N. (2020). Prevalence and nature of medication errors and medication-related harm following discharge from hospital to community settings: a systematic review. Drug Safety Off. J. ISoP 43, 517–577. doi: 10.1007/s40264-020-00918-3
Barber, S., Thakkar, K., Marvin, V., Franklin, B. D., and Bell, D. (2014). Evaluation of My Medication Passport: a patient-completed ‘aide-memoire' designed by patients, for patients, to help towards medicines optimisation. BMJ Open 4, e005608. doi: 10.1136/bmjopen-2014-005608
Berman, L., Raval, M. V., Ottosen, M., Mackow, A. K., and Goldin, A. B. (2019). Parent perspectives on readiness for discharge home after neonatal intensive care unit admission. J. Pediatr. 205, 98–104. doi: 10.1016/j.jpeds.2018.08.086
BLISS (2022). Statistics About Neonatal Care. Available online at: https://www.bliss.org.uk/research-campaigns/neonatal-care-statistics/statistics-about-neonatal-care (accessed August 24, 2023).
Braun, V., and Clarke, V. (2019). Reflecting on reflexive thematic analysis. Q. Res. Sport Exer. Health 11, 589–597. doi: 10.4135/9781071814307
Caporali, C., Orcesi, S., Provenzi, L., Pisoni, C., Zecca, M., Gasparini, L., et al. (2020). A global perspective on parental stress in the neonatal intensive care unit: a meta-analytic study. J. Perinatol. 40, 1739–1752. doi: 10.1038/s41372-020-00798-6
Carter, B., Arnott, J., Simons, J., and Bray, L. (2017). Developing a sense of knowing and acquiring the skills to manage pain in children with profound cognitive impairments: mothers' perspectives. Pain Res. Manage. 2017, 2514920. doi: 10.1155/2017/2514920
Cheng, C., Franck, L. S., Ye, X. Y., Hutchinson, S. A., Lee, S. K., O'Brien, K., et al. (2019). Evaluating the effect of Family Integrated Care on maternal stress and anxiety in neonatal intensive care units. J. Rep. Inf. Psychol. 39, 166–176. doi: 10.1080/02646838.2019.1659940
Conroy, S., and McIntyre, J. (2005). The use of unlicensed and off-label medicines in the neonate. Semin. Fetal. Neonatal. Med. 10, 115–122. doi: 10.1016/j.siny.2004.11.003
Costa, H., Costa, T. X., Martins, R. R., and Oliveira, A. G. (2018). Use of off-label and unlicensed medicines in neonatal intensive care. PLoS ONE 13, e0204427. doi: 10.1371/journal.pone.0204427
Davies, H. T., Phillips, B., Preston, J., and Stones, S. R. (2019). Making research central to good paediatric practice. Arch. Dis. Childhood 104, 385–388. doi: 10.1136/archdischild-2018-315117
Ding, X. R. N., Zhu, L. R. N. M., Zhang, R. M. D. M., Wang, L. R. N. M., Wang, T. T. M., Latour, J. M. R. N. P., et al. (2019). Effects of family-centred care interventions on preterm infants and parents in neonatal intensive care units: a systematic review and meta-analysis of randomised controlled trials. Austr. Critic. Care 32, 63–75. doi: 10.1016/j.aucc.2018.10.007
Griffin, T., and Abraham, M. (2006). Transition to home from the newborn intensive care unit: applying the principles of family-centered care to the discharge process. J. Perinat. Neonatal. Nurs. 20, 243–249. doi: 10.1097/00005237-200607000-00012
Griffith, T., Singh, A., Naber, M., Hummel, P., Bartholomew, C., Amin, S., et al. (2022). Scoping review of interventions to support families with preterm infants post-NICU discharge. J. Pediatr. Nurs. 67, e135–e149. doi: 10.1016/j.pedn.2022.08.014
Hebballi, N. B., Kerl, C. G., Garcia, E. I., Ottosen, M. J., Kelly, K. C., Bartz-Kurycki, M. A., et al. (2021). Barriers to transition to home from the neonatal intensive care unit: a qualitative perspectives of parents and healthcare providers. J. Perinat. Neonatal. Nurs. 35, 340–349. doi: 10.1097/JPN.0000000000000570
Henry Basil, J., Premakumar, C. M., Mhd Ali, A., Mohd Tahir, N. A., and Mohamed Shah, N. (2022). Prevalence, causes and severity of medication administration errors in the neonatal intensive care unit: a systematic review and meta-analysis. Drug Safety J. ISoP 45, 1457–1476. doi: 10.1007/s40264-022-01236-6
HQIP Ra (2022). National Neonatal Audit Programme (NNAP) Annual Report on 2020 Data. London: Royal College of Paediatrics and Child Health.
Krzyzaniak, N., and Bajorek, B. (2016). Medication safety in neonatal care: a review of medication errors among neonates. Ther. Adv. Drug Safety 7, 102–119. doi: 10.1177/2042098616642231
Lakshmanan, A., Kubicek, K., Williams, R., Robles, M., Vanderbilt, D. L., Mirzaian, C. B., et al. (2019). Viewpoints from families for improving transition from NICU-to-home for infants with medical complexity at a safety net hospital: a qualitative study. BMC Pediatr. 19, 223. doi: 10.1186/s12887-019-1604-6
Lakshmanan, A., Sunshine, I., Calvetti, S., Espinoza, J., Santoro, S., Butala, S., et al. (2022). Designing a mobile health solution to facilitate the transition from nicu to home: a qualitative study. Children 9, 260. doi: 10.3390/children9020260
Lopez-Pineda, A., Gonzalez de Dios, J., Guilabert Mora, M., Mira-Perceval Juan, G., and Mira Solves, J. J. (2022). A systematic review on pediatric medication errors by parents or caregivers at home. Expert Opin. Drug Safety 21, 95–105. doi: 10.1080/14740338.2021.1950138
Morris, S., and Johnson, K. (2019). “Polypharmacy in premature neonates: what are we prescribing for families when they go home?” in British Association of Perinatal Medicine Annual Conference Newcastle, UK.
Murray, S., Paize, F., Mullen, R., and Morecroft, C. (2022). SP5 Parent-led administration of medicine on the neonatal unit. Arch. Dis. Childhood 107, e25. doi: 10.1136/archdischild-2022-NPPG.5
O'Donovan, B., Kirke, C., Pate, M., Hugh, S. M. M., Bennett, K. E., Cahir, C., et al. (2022). ‘Everyone should know what they're on': a qualitative study of attitudes towards and use of patient held lists of medicines among patients, carers and healthcare professionals in primary and secondary care settings in Ireland. BMJ Open 12, e064484. doi: 10.1136/bmjopen-2022-064484
Ojha, S., and Choonara, I. (2017). Medication errors in infants at home. Arch. Dis. Childhood 102, 947. doi: 10.1136/archdischild-2017-313007
Page, B. F., Hinton, L., Harrop, E., and Vincent, C. (2020). The challenges of caring for children who require complex medical care at home: ‘the go between for everyone is the parent and as the parent that's an awful lot of responsibility'. Health Exp. 23, 1144–1154. doi: 10.1111/hex.13092
Reis, F., Pissarra, R., Soares, H., Soares, P., and Guimarães, H. (2021). Off-label and unlicensed drug treatments in neonatal intensive care units: a systematic review. JPNIM 10, e100213. doi: 10.7363/100213
Solanki, R., Mondal, N., Bhat, V., and Mahalakshmy, T. (2017). Medication errors by caregivers at home in neonates discharged from the neonatal intensive care unit. Arch. Dis. Childhood 102, 651–654. doi: 10.1136/archdischild-2016-311877
Team PaM (2017). Prescriptions Dispensed in the Community. England: NHS Digital: Health and Social Care Information Centre.
Tong, A., Sainsbury, P., and Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 19, 349–357. doi: 10.1093/intqhc/mzm042
Yardley, S., Teunissen, P. W., and Dornan, T. (2012). Experiential learning: AMEE guide no. 63. Med. Teach. 34, e102–e115. doi: 10.3109/0142159X.2012.650741
Keywords: neonate, medicines administration, parent, neonatal unit, home
Citation: Bracken L, Clark J, Gill A, O'Brien F, Dewey R, Barker C and Carter B (2023) “A hard-won capability”: the experiences of parents managing their babies' medicines after discharge from a neonatal unit. Front. Commun. 8:1204599. doi: 10.3389/fcomm.2023.1204599
Received: 12 April 2023; Accepted: 20 September 2023;
Published: 27 October 2023.
Edited by:
Victoria Team, Monash University, AustraliaReviewed by:
Alice McCloskey, Liverpool John Moores University, United KingdomRosa Mendizabal, University College London, United Kingdom
Corri Stuyvenberg, University of Minnesota Medical Center, United States
Copyright © 2023 Bracken, Clark, Gill, O'Brien, Dewey, Barker and Carter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Louise Bracken, Louise.Bracken@alderhey.nhs.uk
†These authors have contributed equally to this work and share first authorship