 Salvatore Crisafulli1
Salvatore Crisafulli1 Elisabetta Poluzzi2
Elisabetta Poluzzi2 Carlotta Lunghi2,3
Carlotta Lunghi2,3 Vincenzo Di Francesco4Luca Pellizzari4
Vincenzo Di Francesco4Luca Pellizzari4 Luca Pasina5Chiara Elli5
Luca Pasina5Chiara Elli5 Francesco Trotta6
Francesco Trotta6 Agnese Cangini6
Agnese Cangini6 Caterina Trevisan7,8
Caterina Trevisan7,8 Maria Beatrice Zazzara9
Maria Beatrice Zazzara9 Graziano Onder10
Graziano Onder10 Gianluca Trifirò11*
Gianluca Trifirò11*- 1Department of Medicine, University of Verona, Verona, Italy
- 2Department of Medical and Surgical Sciences, Alma Mater Studiorum, University of Bologna, Bologna, Italy
- 3Department of Health Sciences, Université du Québec à Rimouski, Lévis, QC, Canada
- 4Geriatric Unit A, Azienda Ospedaliera Universitaria Integrata, Verona, Italy
- 5Laboratory of Clinical Pharmacology and Appropriateness of Drug Prescription, Department of Health Policy, Istituto di Ricerche Farmacologiche Mario Negri IRCCS, Milan, Italy
- 6HTA & Pharmaceutical Economy Division, Italian Medicines Agency (AIFA), Rome, Italy
- 7Department of Medicine, University of Padua, Padua, Italy
- 8Department of Medical Sciences, University of Ferrara, Ferrara, Italy
- 9Fondazione Policlinico Universitario “Agostino Gemelli” IRCCS, Rome, Italy
- 10Department of Cardiovascular, Endocrine-Metabolic Diseases and Aging, Istituto Superiore di Sanità (ISS), Rome, Italy
- 11Department of Diagnostics and Public Health, University of Verona, Verona, Italy
The ageing process is associated with an increased probability of accumulating health deficits, chronic conditions and geriatric syndromes, leading to a growing prevalence of multimorbidity, defined as the co-occurrence of two or more chronic conditions (of which, at least one physical condition). One of the most frequent and direct consequences of multimorbidity, especially amongst older adults, is polypharmacy, a condition characterized by the concomitant use of five or more drugs per day. Polypharmacy is one of the main risk factors for adverse clinical outcomes, including drug-drug interactions and adverse drug reactions, also resulting in increased hospitalizations, morbidity, and increased use of healthcare resources, with considerable implications for healthcare costs. Deprescribing is one of potential approaches to reduce inappropriate prescribing and it is defined as the stopping or dose reduction of medications that are either inappropriate or unnecessary, especially among patients with polypharmacy. In this review, the major issues associated with polypharmacy among older people, the current guidelines for the management of polypharmacy and the strategies to implement deprescribing in different settings (i.e., hospital setting, nursing homes and general practice) are discussed.
Polypharmacy and deprescribing: A picture from the national report on medicines use in older adults
The number of older adults has been steadily growing worldwide and this results in an increasing multimorbidity and related polypharmacy. Polypharmacy is defined as the use of multiple medicines at the same time, and it is a consequence of the coexistence, in the same person, of multiple chronic diseases requiring numerous pharmacological treatments (Masnoon et al., 2017; Pazan and Wehling, 2021). In the scientific literature, the definition commonly used for polypharmacy is the regular use of at least five medications (Rankin et al., 2018), while the use of ≥10 medications is often defined as “major” or “excessive” polypharmacy (Guthrie et al., 2015). Polypharmacy is associated with an increased risk of interactions between medicines, but also between medicines and diseases or between medicines and food.
The Italian National Report on Medicine Use in Italy and the Italian National Report on Medicine Use in older adults, being published within Medicines Utilization Monitoring Centre (The Medicines Utilisation Monitoring Centre of the Italian Medicines Agency, 2022; The Medicines Utilisation Monitoring Centre of the Italian Medicines Agency, 2020), assessed different aspects of medicines use in this population, including polypharmacy, providing new interpretative keys, and suggesting possible interventions aimed at improving the use of drugs in this population. Data were extracted from the administrative database “Pharmaceutical Prescriptions database” (also known as the Italian Health Insurance Card database) that includes anonymized patient-level data on medications prescribed and dispensed by community pharmacies and reimbursed by Italian National Health System. Data were collected per each drug package, identified via package unique identifier codes, and then grouped according to the fifth level World Health Organization (WHO) Anatomical Therapeutic Chemical (ATC) classification. Data were analysed in terms of prevalence, amount of use, expressed as defined daily dose per 1,000 users (DDD/1,000 users per day), expenditure per user and number of substances received by each patient. In 2021, the prevalence of medicines’ use in Italy (i.e., subjects which received at least one pharmaceutical prescription) among the elderly was 97%, meaning that almost the whole elderly population has received at least one dose during the year. Every user aged ≥65 years has received about 3.5 doses every day, with a greater consumption in men than women (3,568.8 vs. 3438.8 DDD/1,000 users per day) (The Medicines Utilisation Monitoring Centre of the Italian Medicines Agency, 2022). The number of doses rose with the age, ranging between 2710.3 DDD/1,000 user per day in subjects aged between 65 and 69 years and 3853.8 DDD/1,000 user per day in subjects aged ≥85 years. Similarly, the expenditure per use ranged between 4304 € and 620.9 €. In 2021 each user took on average 7.4 different substances, with the lowest value (a mean of 5.8 substances per user) in the age group 65–69 years and the highest value (a mean 8.4 substances per user) recorded in the subjects aged ≥85. For both genders, it was observed a progressive increase in the number of different active ingredients taken with increasing age, increasing from a mean of 5.8 substances in men aged between 65 and 69 years to a mean of 8.6 in men aged ≥85 years. A similar trend was observed in women, with a mean of 5.9 different substances taken in the age group 65–69 years and a mean of 8.3 different active ingredients taken by women aged ≥85 years (Table 1).
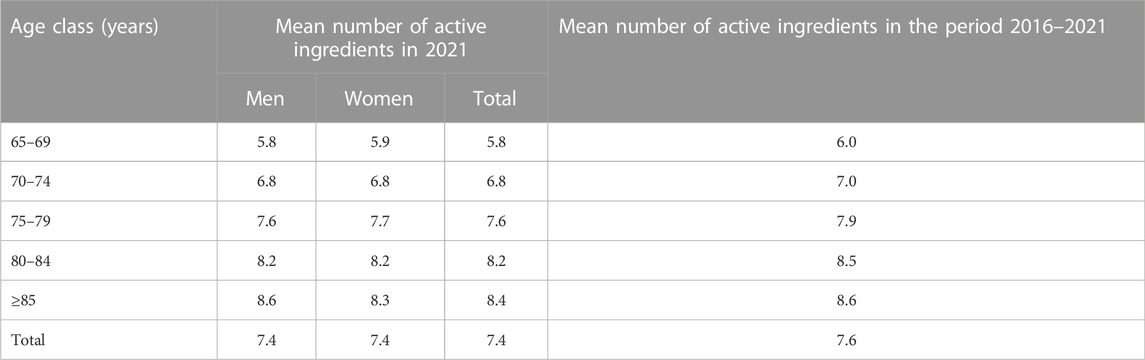
Table 1. Mean number of active ingredients by age and gender in 2021.
About 66.6% of elderly users received prescriptions for at least 5 different medications during the year and 26.8% of subjects aged ≥65 took at least 10 different active ingredients. These data confirm a frequent use of polypharmacy in patients aged over 65 years and, consequently, a greater risk of drug interactions (Figure 1).
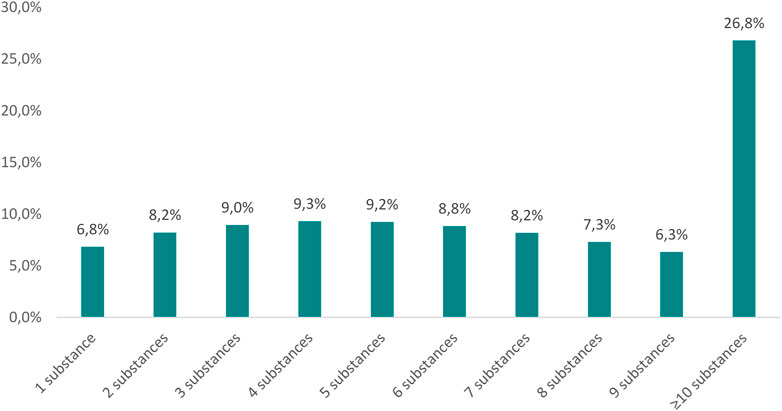
Figure 1. Percentage distribution of elderly users by number of active ingredients in 2021.
It was also assessed the concomitant intake of at least two medicines increasing the risk of gastrointestinal bleeding, including non-steroidal anti-inflammatory drugs (NSAIDs), anticoagulants and antiplatelet agents. Concomitant use of 2 or more medicines increasing the risk of gastrointestinal bleeding was common in the elderly population (6.6% of the elderly population) and it increased with age (4.7% in the population between 65 and 74 years, 8.1% between 75 and 84 years and 9.5% between 85 years or older) (The Medicines Utilisation Monitoring Centre of the Italian Medicines Agency, 2020). Moreover, the concomitant use of two or more medicines that increase the risk of renal failure, including NSAIDs, spironolactone, angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers was evaluated. It is known that renal function progressively decreases with increasing age. In elderly patients, the reduction of the renal function can be accentuated by the use of the above-mentioned medicines, especially if taken in combination. This concomitant use failure is common in the elderly population, and it was observed in 9.5% of the elderly population.
Although the use in individuals aged ≥90 years is lower than in the younger age groups, a significant use of medicines, including lipid-lowering medicines and anti-osteoporotics, not supported by a real therapeutic need was found (The Medicines Utilisation Monitoring Centre of the Italian Medicines Agency, 2020; Zazzara et al., 2022). Medicines prescription in this population raises several issues. Individuals aged ≥90 years represent a poorly studied population, usually excluded from clinical trials that lead to medicines’ approval. If some people aged 90 years or over, on the one hand, is affected by a smaller number of pathologies due to a selection effect (only the healthiest elderly survives in the most advanced ages, according to a phenomenon defined as the “healthy survivor effect”), on the other hand this population presents some issues related to pharmaceutical treatment (Evert et al., 2003; Hadley and Rossi, 2005; Hagberg and Samuelsson, 2008). For example, in this population, with limited life expectancy, the prescription of “preventive” drugs, whose function is to reduce the risk of acute events, could be of little advantage. Achieving the effect of some of these medicines (e.g., antihypertensive, lipid-lowering, antiplatelet drugs, drugs for the treatment of osteoporosis) in fact requires long periods and a person aged ≥90 years may not have a sufficient life expectancy to receive the benefits of these treatments. The reduction of prescribed medicines could be explained by a different attitude of physicians towards the prescribing process, with increased attention to avoiding the prescription of potentially inappropriate medications (PIMs). Nevertheless, the high number of prescribed medicines, in particular medicines prescribed for the treatment and primary and secondary prevention of cardiovascular events highlights the need of evidence to improve medication use in the oldest old and to guide physicians when prescribing medicines in older adults and in the deprescribing. Deprescribing is the planned and supervised process of reducing or discontinuing pharmaceutical treatment that may be no longer effective or cause harm, with the aim of reducing the burden or harm of medicines by improving the quality of life (Reeve et al., 2015; Halli-Tierney et al., 2019). Studies evaluating the impact of deprescribing suggest that it could be achievable, well-tolerated and can lead to improved outcomes (Ibrahim et al., 2021). Therefore, it could be more implemented in the future promoting the collaboration among the different healthcare professionals.
The clinical and economic impact of polypharmacy
Polypharmacy may often be based on inappropriate prescriptions of drugs that are not medically necessary or no longer needed (Masnoon et al., 2017; Sirois et al., 2019). According to this definition, the prescription of medicines for which there is no evidence-based indication, are not effective or constitute a risk for adverse drug reactions should be considered as inappropriate polypharmacy (Mair et al., 2020).
Especially in frail elderly patients, polypharmacy is one of the main risks for potentially inappropriate prescribing, leading to adverse clinical outcomes, including drug-drug interactions (DDIs) and adverse drug reactions (e.g., falls and cognitive impairment), also resulting in increased morbidity, hospitalizations, increased length of hospital stay and mortality (Calderón-Larrañaga et al., 2016; Wastesson et al., 2018; Zazzara et al., 2021). This, in turn, leads to an increased use of healthcare resources, with considerable implications for healthcare costs (G. Kojima et al., 2012).
Regarding DDIs, polypharmacy is one of the most relevant risk factors (Johnell and Klarin, 2007; Wolff et al., 2021). The prevalence of clinically relevant DDIs among home-dwelling older adults reported in the scientific literature widely ranges from 35% to 77% (Novaes et al., 2017; Santos et al., 2017; Hermann et al., 2021; Sheikh-Taha and Asmar, 2021), and the most commonly reported are myopathy due to the increased levels of statins when used with calcium channel blockers and postural hypotension caused by the interaction between thiazide diuretics and ACE inhibitors (Sheikh-Taha and Asmar, 2021).
A considerable number of studies demonstrated that polypharmacy increases the risk of falls among both community-dwelling and institutionalized older adults (Damián et al., 2013; T. Kojima et al., 2011; Kua et al., 2019). Evidence from the English Longitudinal Study of Ageing (ELSA) Study showed that the prevalence of hospital admission due to falls among patients aged more than 50 years increased with polypharmacy (Zaninotto et al., 2020). In particular, the prevalence of fall-related hospital admissions increased from 1.5% in patients reporting no medication use to 8% among those with polypharmacy (i.e., use of 5–9 different drugs) and 15% among those receiving more than 10 different drugs (Zaninotto et al., 2020). Polypharmacy has also been associated with cognitive impairment and dementia (Oyarzun-Gonzalez et al., 2015; Park et al., 2017; Rawle et al., 2018). More specifically, as observed for falls, the risk for negative cognitive outcomes increases with an increasing number of prescribed drugs (Oyarzun-Gonzalez et al., 2015; Park et al., 2017; Rawle et al., 2018). A systematic review and meta-analysis of observational studies showed that the average percentage of hospital admissions due to adverse drug reactions in older adults with polypharmacy was 8.7% [95% confidence interval (CI), 7.6%–9.8%], with NSAIDs, beta-blockers, antibiotics, oral anticoagulants, digoxin, ACE inhibitors, calcium channel blockers, antineoplastic drugs, opioids, and oral antidiabetics being the most frequently involved drug classes (Oscanoa et al., 2017).
Another adverse consequence of polypharmacy includes decreased medication adherence resulting in worsening of underlying medical conditions. Low adherence to medications has been reported to increase with the number of prescribed drugs among older adults (Pasina et al., 2014), leading to therapeutic failure and disease progression (Marcum & Gellad, 2012).
Such adverse clinical outcomes are in turn associated with an increased risk of unplanned and recurrent hospitalization and mortality, especially among elderly patients (Payne et al., 2014; Davies et al., 2020).
A meta-analysis of both randomized controlled trials and observational studies assessing the association between polypharmacy and death found that mortality risk increases as the number of taken drugs increases, with a pooled odds ratio ranging from 1.2 (95% CI: 1.1–1.4) among patients taking 1–4 medications to 2.0 (95% CI: 1.4–2.7) among patients taking ≥10 different medications (Leelakanok et al., 2017). However, the authors of this study reported that the estimates of many of the included studies were likely affected by residual confounding (Leelakanok et al., 2017).
The negative clinical outcomes associated with polypharmacy ultimately have a negative impact also from an economic perspective. A recently published article assessing the economic impact of polypharmacy in elderly patients with cardiovascular diseases showed that, as compared to the absence of polypharmacy (i.e., <5 medications), polypharmacy (i.e., ≥5 medications) was associated with an increased healthcare expenditure (incidence rate ratio for the increase of healthcare expenditure: 2.0; 95% CI, 1.4–2.7), including both pharmacy-related and non-pharmacy-related expenditures (Kwak et al., 2022).
Adverse drug reactions are one of the main reasons for hospital admissions as well as increased length of hospital stay, most of which are caused by polypharmacy and, as such, are avoidable (Formica et al., 2018). In this regard, Hoonhout et al. reported that, as compared to patients aged less than 65 years (2,851€), the additional cost associated with preventable adverse drugs events increased by 8.6% among the subgroup of patients aged more than 65 years (3,097 €) (Hoonhout et al., 2010).
Guidelines for the management of polypharmacy
The phenomenon of the ageing population across the world has led to a growing interest in formulating guidelines and health policies in response to the needs of such a complex population requiring high clinical and social care demands. The ageing process is associated with an increased probability of accumulating health deficits, chronic conditions, and geriatric syndromes (such as frailty), that lead to a growing prevalence of multimorbidity, defined as the co-occurrence of two or more chronic conditions (of which, at least one physical condition) (Rockwood and Mitnitski, 2007; Calderón-Larrañaga et al., 2016; Johnston et al., 2019; Vetrano et al., 2019). More than 75% of adults aged 60 years and older already suffer from more than two chronic conditions, and this proportion reaches almost 100% among adults older than 80 years (Calderón-Larrañaga et al., 2016). One of the most glaring, and probably the most frequent and direct, consequences of multimorbidity is represented by polypharmacy.
Therefore, a changeover in the administration of the healthcare systems is essential to sustain the care of persons with multimorbidity and polypharmacy. The main goal of this change is to redirect the focus of care from a single disease-centered approach to a holistic approach, outlining all individual needs and guaranteeing multidisciplinary assistance in all settings of care (Palmer et al., 2018). In the last decade, several guidelines have been formulated worldwide to summarize recommendations for evaluating, managing, and optimizing the care of persons affected by multimorbidity and/or polypharmacy. These recommendations may guide healthcare professionals in their daily practice and upgrade the healthcare systems according to the real care necessities (Table 2).

Table 2. Recommendations for evaluating, managing, and optimizing the care of persons affected by multimorbidity and/or polypharmacy.
Italy is one of the countries with the oldest population, with more than 7 million people aged ≥75 years and 765 thousand aged over 90 in 2019 (Istituto Nazionale di Statistica, 2020). The Italian National Statical Institute estimates that by 2045 more than one-third of the Italian population will be 65 years and older, with a high proportion of people living with multimorbidity and polypharmacy. Moreover, according to the Osservatorio Nazionale sull’Impiego dei Medicinali “OsMed” (Medicines Utilization Monitoring Centre) database, adults aged 70–79 years consume a median number of drugs equal to 7, increasing to 8 among adults aged 80 and older (Zazzara et al., 2022).
In light of this evidence, recognizing that multimorbidity and polypharmacy are health priorities for the Italian welfare and National Health System, the Italian Society of Gerontology and Geriatrics (SIGG) promoted the development of Italian guidelines on the management of persons with multimorbidity and polypharmacy, published in 2022 (Onder et al., 2022). This initiative involved the main national scientific societies operating in the fields of geriatrics, general and internal medicine and pharmacology including: the Italian College of General Practice (Società Italiana di Medicina Generale e delle Cure Primarie), the Italian Society of Internal Medicine (Società Italiana di Medicina Interna), the Italian Society of Hospital and Community Geriatrics (Società Italiana di Geriatria Ospedale e Territorio), the Italian Society of Pharmacology (Società Italiana di Farmacologia) and the Italian Scientific Society of Hospital Internal Medicine (Federazione delle Associazioni dei Dirigenti Ospedalieri Internisti Medicina Interna).
The rationale of the guidelines was to develop recommendations for the clinical management of individuals with multimorbidity and/or polypharmacy and to provide evidence-based guidance to improve the quality of the offered care. These recommendations are addressed to healthcare professionals, healthcare system policymakers, stakeholders, and patients, whose point of view has been considered to underline health priorities, goals, and expectations. Through the identification of such care priorities and the prompt recognition of subjects at higher risk of health decompensations and adverse events, the guidelines aim to improve the allocation of healthcare resources and reduce related costs. The panel of experts included epidemiologists, geriatricians, internal medicine physicians, general practitioners (GPs), pharmacists, pharmacologists, nurses, and patient representatives. A total of 13 review questions were formulated for the present guidelines by the panel. Special attention was paid to the optimization of polypharmacy management and the implementation of efficient interventions to reduce the burden of treatments and their related costs. Moreover, the panel emphasized the need of recognizing PIMs and evaluated the safety and cost-effectiveness of the deprescribing process of specific drugs. Finally, great importance was given to issues concerning goal-oriented care, self-management, and patients’ education and empowerment.
After performing appropriate systematic reviews, the panel developed 13 recommendations, whose main principles are summarized below.
First, the guidelines on management of persons with multimorbidity and polypharmacy underlined the importance of identifying health trajectories, patients’ care needs and health priorities to agree upon an individualized care plan, comprising advanced care directives. This plan should reflect patients’ preferences and expectations, define realistic objectives, and be coordinated by a recognized figure in charge. Continuous communication of the care plan between the patients, their caregivers, and healthcare professionals is strongly encouraged as essential to reduce unplanned hospital admissions and regulate emergency care accesses.
Second, most of the questions and the final recommendations discuss deprescribing. In this regard, recommendations recognized the importance of educating the patients and their caregivers about the benefit/risk profile of polypharmacy and the deprescribing process and empowering self-management. These actions can be facilitated by a regular follow-up with a scheduled revision of pharmacological regimes considering interactions between diseases and treatments and the efficacy and safety of each treatment before deciding on drug continuation, withdrawal, or introduction. Among the instruments that could be useful for these purposes are Beers Criteria (American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults,” 2019) or Screening Tool of Older People’s Prescriptions (STOPP) and Screening Tool to Alert to Right Treatment (START) criteria, and the INTERCheck tool (Istituto Farmacologico e di Ricerca Mario Negri, 2022), developed by the “Istituto di Ricerche Farmacologiche Mario Negri”, which may facilitate the process of drugs reconciliation and identify the prescriptions of PIMs (Rochon and Gurwitz, 2017).
For instance, the guidelines recommended deprescribe proton pump inhibitors (PPIs) in patients without a clear indication for continuous treatment and stopping the treatment after a maximum of 6 weeks, independently of the indication. The potential renewal of the treatment, preferably on-demand, should be evaluated in case of remerging symptoms.
Concerning statins, the panel recommended deprescription in patients with life expectantly inferior to 1 year and to assess the risk/benefits of this treatment in people aged 80 and older, considering cardiovascular risk factors, life expectancy, frailty, and possible drug interactions.
Finally, the panel narrowed the indications for vitamin D supplementation in individuals with multimorbidity, independently of the vitamin D serum levels, to prevent fractures in patients with osteoporosis and to prevent falls in institutionalized patients.
Instead, the panel did not find strong and consistent evidence to formulate recommendations for deprescribing anti-hypertensive and antiplatelet drugs. Further studies are needed to clarify this issue better.
Overall, the Italian guidelines on the management of persons with multimorbidity and polypharmacy highlight the importance of health professionals’ training in terms of multimorbidity, polytherapy and deprescribing, and stress the need to improve the collaborations between health workers in different care settings to guarantee a continuum in the care. In this context, educating the patients and their caregivers is essential, as well as increasing their awareness of processes such as deprescribing and promoting goal-oriented care with a multidisciplinary and comprehensive approach.
Lastly, the panel underlined the importance of developing new technologies to share health information and facilitate the management of persons with multimorbidity and/or polypharmacy and emphasizes the need to improve national research plan strategies in these fields.
Deprescribing in hospital setting
In up to 20% of cases, hospital admission is caused by symptoms of drug adverse reaction (Lazarou et al., 1998). In both adults and elderly patients, the mean number of drugs taken at hospitalization is 5, so potential inappropriate therapy is high even in the absence of symptoms (Veronese et al., 2021). Thus, drug discontinuation during hospital stay is sometimes immediate and compulsory, due to adverse reactions clearly caused by a drug. On the other hand, stopping drugs may follow a more complex evaluation focused on the patient’s clinical and functional state. For instance, anemia may be observed in a patient treated with oral anticoagulants, whose renal function has been declining. Dose, drug choice or even indication for anticoagulation should be revised, according to the level of renal function stabilization. The balance between the risks of bleeding and thrombosis prevention may be not easy to establish during the short period of hospitalization.
In any case, hospital admission suggests a comprehensive re-evaluation of therapy. Life expectancy could be modified by a new clinical event causing admission and a new treatment with drugs potentially interfering with previous chronic therapy could be necessary. Overall, an accurate therapy review allows to withdraw at least one drug. Any reduction of the number of drugs has a clinical advantage in terms of safety and reduction of adverse drug reactions. This process can be conducted in hospital after careful evaluation of the risk of discontinuation by an expert physician and cannot be delegated to an informatic tool which evaluates only drug interactions. Very often drugs prescribed for cardiovascular primary prevention many years before should be reconsidered in older patients and eventually deprescribed.
Deprescribing is the process of evaluating if present and potential harms of a drug outweigh benefits, by considering the actual patient function, life expectancy and his/her preferences (Scott et al., 2015). This is an active, positive professional intervention that needs a multidimensional evaluation, particularly in older patients. In fact, not only comorbidities and functional status should be taken into account but also cognitive status, disability, social and emotive conditions and nutritional balance. Ceasing drugs requires the same steps that are necessary for starting a new drug: deprescribing specularly follows prescribing. A therapeutic goal needs to be identified, an informed consent should be obtained, and a close monitoring of the effects should be planned.
Hospital stay can be too short to reach stable functional and clinical conditions and the effects of therapy modifications may be seen on a longer period. Furthermore, it is reasonable to stop one drug at a time, in order to better detect potential harms and benefits of withdrawal, so a longer period could be needed. For these reasons, it is recommendable to share the program of deprescribing with the GP for a continuous care between hospital and home, and to instruct patients as well to identify and report possible future withdrawal reactions or symptoms returning after drug discontinuation.
In particular, deprescribing should be considered in older patients when: 1) presenting with a new symptom or clinical syndrome suggestive of adverse drug reaction; 2) manifesting advanced or end-stage disease, terminal illness, severe dementia, extreme frailty, full dependence for daily living activities; 3) receiving high-risk drugs or combinations; 4) receiving preventive drugs with no clear short to mid-term benefit.
There are several successful experiences of deprescribing in terms of mortality and hospital readmission, and, in both cases, results were obtained only when the process included patients’ involvement and education and close post discharge monitoring.
Specific deprescribing protocols have been developed focusing on a specific goal. One of the most studied is focused on reducing the risk of falls in the elderly. A list of fourteen drugs (mostly psychotropic medications) was selected by a panel of experts to be included in the Screening Tool of Older Persons Prescriptions in older adults with high fall risk (STOPPFall) (Seppala et al., 2021), and benzodiazepines were unanimously considered the drugs at higher risk for falling (Christensen and Lundh, 2016).
More general criteria for inappropriate prescribing were developed for the screening of the PIMs. Again, benzodiazepines were identified as drugs that should be more frequently discontinued in elderly patients. PPIs are largely used at older age for gastrointestinal diseases and symptoms, but sometimes they are used to prevent bleeding in asymptomatic patients assuming other drugs causing gastrointestinal (e.g., NSAIDs, new oral anticoagulants, etc.). In many cases, PPIs should be discontinued in mid-to-long term whenever possible, because chronic use of such drugs may cause pulmonary infections, dysmicrobism, maldigestion and malnutrition. Unfortunately, since chronic treatment with PPIs causes hypergastrinemia, the withdrawal of such drugs frequently causes gastrointestinal symptoms even in patients without prior reflux or gastric pain because of acid hypersecretion stimulated by gastrin for a variable period. This transitory problem should be discussed with the patients at the moment of deprescribing, otherwise they would start PPIs again.
By using STOPP criteria in a large sample of hospitalized geriatric patients, it has been recently found that the absolute number of drugs taken was correlated with a higher risk of inappropriate prescriptions, but in the multivariate analysis the risk factors for inappropriate prescription did not include the number of drugs (Seppala et al., 2021). Risk factors were: 1) living in a nursing residence; 2) having a physical mobility deficit; 3) suffering from one geriatric syndrome; 4) reporting one prior hospitalization during the past 12 months. Again, the evaluation of patients’ characteristics, as well as the number of prescribed drugs and pharmacokinetics evaluation play a crucial role to avoid PIM prescription. Therefore, a comprehensive evaluation of the patients, supported by a pharmacological careful review, is needed.
Deprescribing in nursing homes
Older nursing home residents often have a number of diseases that frequently require multiple medications (Avorn and Gurwitz, 1995; Dwyer et al., 2010), which expose them to an increased risk of inappropriate prescribing, adverse drug events and potentially severe DDIs (Teramura-Grönblad et al., 2016; Halvorsen et al., 2017; Herr et al., 2017). Nursing home residents are complex and vulnerable, with a higher burden of cognitive deficits than non-institutionalized elderly (Avorn and Gurwitz, 1995).
The quality of drug prescribing to nursing home residents has worsened during the last two decades and this should be of concern for clinicians and policymakers, especially considering the high and chronic use of multiple psychotropic medications (Selbaek et al., 2007; MacRae et al., 2021). Most nursing home residents do suffer from dementia, with psychiatric and behavioral symptoms, so higher prescription of psychotropic drugs is likely (Eggermont et al., 2009; Nijk et al., 2009; Wetzels et al., 2011). However, long-term use of psychotropic drugs in older people raise important safety concerns (Billioti de Gage et al., 2014; Weich et al., 2014) and prescription for only short periods is generally recommended (Gareri et al., 2014). Despite these recommendations, long-term use is still commonFare clic o toccare qui per immettere il testo. (Ruggiero et al., 2010), even if successful discontinuation may result in improvements in cognitive and psychomotor function and also working memory, reaction times, balance and fewer falls (van der Cammen et al., 2014). Many reasons have been proposed why psychotropic drugs are so commonly used in this setting, and behavioral symptoms are those most commonly cited (Sloane et al., 1991). However, psychotropic treatment of behavioral disturbances is often not effective in patients with dementia and in fact there has been some success in reducing these drugs by training staff to use behavioral interventions instead of drugs (Ray et al., 1993).
Some studies suggest that, in addition to psychotropic drugs, other medications with high prevalence of use, such as antiulcer agents, laxatives and antiplatelets need an appropriate medication review (Pasina, et al., 2020). For example, PPIs are among the most commonly used drugs in nursing homes (Pasina, et al., 2020a), but their overuse is widespread. The high prevalence and inappropriate use have been found to be related to the general health vulnerability of nursing home residents, who present poly-pathology and polypharmacy and to the mean number of concomitant drugs used, independently of the prescription of gastro-toxic drugs. However, their regular use has been associated with diarrhea and other adverse events, with heavy implications for drug costs (Teramura-Grönblad et al., 2010; Benmassaoud et al., 2016). So, optimization of their prescriptions is recommended.
Similarly, antiplatelets, and mainly acetylsalicylic acid, are among the most prescribed cardiovascular drugs in nursing homes (van Dijk et al., 2000; Pasina, et al., 2020), but most nursing home residents are inappropriately treated for primary prevention of cardio-or cerebrovascular disease (Pasina, et al., 2020b). This widespread prophylactic use of antiplatelets in nursing homes is inappropriate, because the benefit–risk ratio for primary prevention in current practice is extremely small and the benefits of antiplatelets to prevent cardio- and cerebrovascular disease are recognized and appropriate only for secondary prevention. In addition, nursing home residents without an evidence-based indication for antiplatelets received PPIs in an unnecessary ‘prescribing cascade’ that should be assessed for deprescribing.
The regular use of PPIs is also related with an increased probability of receiving drugs to treat anemia, such as iron supplement, folate or cyanocobalamin and erythropoietin in nursing home residents, as the effect of a prescribing cascade. So, there is a real need to avoid the increasing use of PPIs in nursing homes and to optimize their prescription (Elli et al., 2022).
Again, laxatives are among commonly used in nursing homes, but their use is closely related to the use of medications that can cause constipation, especially psychotropic drugs, such as antidepressants, anti-Parkinson dopaminergic agents and benzodiazepines (Elli et al., 2021). Optimizing the prescription of psychotropic drugs could probably be effective in decreasing the “prescribing cascade” with laxatives.
These examples of prescribing cascade in nursing homes suggest that prescribers need to pay more attention to the benefit–risk ratio for each drug used, because drugs with a very small expectation of benefit raise the number of administered drugs with the related risk of adverse reactions and costs.
Deprescribing is often difficult involving identifying a problem (use of an inappropriate drug) and a therapeutic decision (withdrawing it with close follow-up) (Scott et al., 2015), but discontinuation of potentially inappropriate medications is feasible (Pasina et al., 2016; Wouters et al., 2017). For example, the combination of educational interventions (“ex cathedra” presentations) and the use of computerized prescription support systems was found to significantly reduce the prescription of potentially inappropriate psychotropic drugs, psychotropic duplicates, and of drugs associated with potentially severe DDIs (Pasina et al., 2016).
Different types of interventions to optimize medications in nursing homes have been identified (Spinewine et al., 2021): micro-level interventions, such as medication review or patient-centered care, and macro-level interventions, such as guidelines and legislation (defined as change in reimbursement, initiation of public reporting of antipsychotic use). Some examples of micro-level interventions are reported in five recent multicenter trials in Europe, which involved multidisciplinary interventions consisting of education of healthcare providers and medication reviews (Fog et al., 2017; Wouters et al., 2017; Cool et al., 2018; Husebø et al., 2019; Strauven et al., 2019); these interventions showed positive effects on reduction of the number of drugs by 9% and PIMs by 65%. Interventions to optimize medications with high prevalence of use in nursing homes, like psychotropic drugs, anticholinergic drugs and anti-infective drugs were also considered: interdisciplinary interventions using START/STOPP criteria can lead to a significant reduction in psychotropic drug use ranging from 11.9% for antidepressants to 39.5% for anxiolytics (Weeks et al., 2019). The anticholinergic burden can be reduced with micro-level interventions, but there is no consensus for the most useful tool, owing to the heterogeneity of scales used to measure it. Antibiotic use can also be reduced by stewardship program activities, including local multidisciplinary networks (micro-level) and guidelines publication (macro-level): a reduction of 22% in the prevalence of antibacterial use over a 6 year period was observed in Switzerland, although effects on health outcomes are still lacking in nursing homes (Plüss-Suard et al., 2020).
A systematic review evaluating the impact of deprescribing interventions (defined as either medication discontinuation, substitution, or reduction) by healthcare professionals on clinical outcomes like mortality, falls, PIMs, and hospitalization found that deprescribing was effective in reducing the number of nursing home residents with PIMs by 59% and therefore reducing the risk of adverse effects and reasonably improving clinical health outcomes (Kua et al., 2019). Among the 41 studies included, the medication review was led by physicians, pharmacists or by a multidisciplinary team using Beers or START/STOPP criteria and medication review-directed deprescribing interventions could also reduce the risk of death by 26% and the number of fallers by 24%. Another systematic review evaluated the economic impact of interventions aimed at optimizing drug utilization in the elderly (Laberge et al., 2021). Despite the still limited evidence, such interventions seem to provide benefits that outweigh the costs of their implementation.
Some barriers for deprescribing interventions have been found to be healthcare providers’ concerns about deprescribing and perceived reluctance of nursing home residents to change, but patient-centered interventions are recognized to be of crucial importance and the nursing homes are an ideal setting for comprehensive drug regimen review and deprescribing, which is all too often neglected in elderly patients in all clinical settings.
Deprescribing in general practice
GPs represent the main contact with healthcare for most patients in many healthcare systems, including the Italian. Indeed, in most healthcare organizations, patient visits the GP for periodic monitoring, for additional mild-medium new symptoms and for refilling prescriptions. In healthcare systems like the Italian one, GPs have good continuity of care with their patients, especially older patients, because they need to manage multimorbid conditions and polypharmacy. GPs are, therefore, in the best position to implement deprescribing as they know and regularly see their patients, they know their actual and past medical history and all the medication they are taking. Moreover, patients often have an established relationship of trust with their GP. The general practice could thus seem to be the best opportunity for reviewing and defining the patient priorities and feasibility of complex polypharmacy deprescribing.
Nevertheless, the evidence of deprescribing intervention benefits in general practice implementation is still lacking. A few trials aimed at estimating the feasibility and the impact of GP-led medication review and deprescribing in primary care (Mahlknecht et al., 2021; McCarthy et al., 2022), but the results are still unclear, with small to moderate effects in terms of reduction in the number of medications or PIMs and inconclusive results in terms of health outcomes (i.e., reduction in of hospitalisation or mortality). The Supporting Prescribing in Older Adults with Multimorbidity in Irish Primary Care (SPPiRE) trial was conducted in recent years to estimate the effect of a GP-led medication review in older patients living in the community (McCarthy et al., 2022). The trial was conducted among GP practices (51 with 404 patients), and the outcome was a reduction in PIM use and polypharmacy. Even though the reduction in PIMs and polypharmacy was statistically significant in that trial, the effect was small, and the potential improvement of the prescription quality was unclear (McCarthy et al., 2022). Similar results were reported in a cluster-randomized controlled trial conducted in Northern Italy (Mahlknecht et al., 2021). The trial was conducted among 22 GPs (and 307 patients 75 years and above) for 24 months, and the intervention consisted of a medication review (based on Beers criteria and potential for DDIs). In this study, apart from the reduction in the number of medications achieved in the intervention group, all-cause mortality, and unplanned hospitalisations (the primary composite outcome) did not differ from the experimental and control groups.
Several barriers have already been identified both from the patient’s and the GP’s points of view (Reeve et al., 2013; Duncan et al., 2017). Common patient barriers are, among others, the fear of stopping medications (for possible side effects or withdrawal symptoms, i.e., in the case of benzodiazepines or antidepressants), the influence of family and the belief in the need for medications for their wellbeing (Reeve et al., 2013). Among barriers reported by prescribers, lack of time for each visit (needed for empowerment and engagement of each patient) and scarce awareness of the reasons for specialist prescriptions, together with the relevant risk of legal responsibility (or clinical inertia), are the major ones (Anderson et al., 2014; Luymes et al., 2018; Doherty et al., 2020; Mahlknecht et al., 2021).
Implementing deprescribing initiatives in primary care requires the enhancement of GPs’ awareness of the tools and instruments to identify PIMs and apply a deprescribing process. These tools can comprise validated lists, criteria, apps, and other web resources. GPs do not only need to be aware of the inappropriateness of medications in the elderly and the risk of polypharmacy, especially in the oldest or frail patients, but they also need to strengthen their relationship with their patients, enabling shared decision-making with them and their caregivers (Carrier et al., 2019; Rieckert et al., 2020). Nonetheless, studies aimed at estimating the effectiveness of electronic decision support tools in deprescribing showed a reduction in the number of medications consumed by older patients but failed to show a decrease in unplanned hospitalisations (Rieckert et al., 2020).
The collaboration between GPs and other healthcare professionals seems to be an enabling factor for the effective implementation of deprescribing in general practice. Even when a GP applies deprescribing, it is not uncommon that deprescribed medications are restarted due to the reoccurrence of the condition treated or symptoms. In the Italian trial by Mahlknecht et al., the medication review was performed by a clinical pharmacologist, an internist, and an evidence-based medicine expert and modifications of the therapy were proposed to the GP (Mahlknecht et al., 2021). Of the suggested drug regimen changes, 24% were accepted by GPs. Still, a third of these medications (i.e., benzodiazepines, antidepressants, PPIs, and NSAIDs) was restarted over the study period. A possible reason could be the lack of communication and shared decisions between the specialists performing the medication review and the GP.
Clinical pharmacists may support GPs in the medication review process and provide valuable suggestions on possible deprescribing in a specific patient by analysing their overall drug therapy in the light of preliminarily shared inappropriate medication criteria and DDIs. Moreover, nurses in the GP’s staff may check for adherence and possible symptoms suggesting adverse effects or inefficacy and again provide physicians with key information for eventual deprescribing decisions. The opportunity to involve staff in the medication review and deprescribing processes requires adapting the general principles of this process. If a 5-step process is generally suggested according to Woodward’s principles, seven steps are necessary for general practice (Reeve et al., 2014). The additional steps are represented by principle zero, which means engaging practice staff in education and appropriate identification of patients, and principle six, which is providing feedback to staff about deprescribing occurrences within the practice.
However, when we consider other healthcare professionals involved in the management of the single patient treatments, we cannot ignore other prescribers (i.e., clinicians at the hospital and secondary care specialists) who directly add or stop medicines to the patient. This complex scenario strongly requires sharing initiatives of medication review and deprescribing within local healthcare organisations.
In both interprofessional collaborations (GP’s staff and multiprescriber scenario), a priori sharing of steps, roles, and main criteria to be considered in deprescribing is needed. This sharing approach can allow the involvement of other professionals, such as the community pharmacists, who may further check for adherence, and possible inappropriate uses when dispensing medical products (both prescribed and self-medication) to the patient (Bryant et al., 2011).
Future perspectives
There are still many knowledge gaps on deprescribing the most frequently prescribed chronic medicines in elderly people. Future research, including randomized controlled trials and, whenever applicable, observational studies, should generate further evidence to properly guide clinicians in implementing deprescribing in routine clinical practice in specific high-risk patient populations (Thompson et al., 2019).
Effective polypharmacy management requires a regular and systematic re-evaluation of the benefit-risk profile of different drugs prescribed by specialists and GPs or taken as self-medication by the patients, especially to minimize risks. Rigorously scientific strategies to optimize pharmacological treatments, especially among elderly patients, are crucial to reducing the burden of polypharmacy regimens on both patients’ outcomes and healthcare systems.
Multidisciplinary teams including specialists, GPs, clinical pharmacologists, pharmacists and nurses, play a key role in structurally reviewing medication regimens and promoting therapeutic reconciliation and adherence to treatment and are particularly suited to meet the multiple needs of older patients, including polypharmacy management (Topinková et al., 2012).
The implementation of computerized decision-making support systems (i.e., multiple integrated systems using information technologies to improve healthcare delivery by enhancing clinical decision-making through targeted clinical knowledge, patient information, and other health information) could help reduce PIMs prescription, detecting adverse drug reactions, improve medication adherence and facilitate patients’ pharmacological management (Osheroff, 2012). Such systems may also help clinicians personalize therapies to meet the needs of their individual patients and avoid some of the polypharmacy-related risks. In this regard, it is important that physicians actively engage patients and/or their caregivers in decision-making processes to improve patients’ knowledge of their medication regimens and increase prescribing appropriateness.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of interest
GTò has served in the last three years on advisory boards/seminars funded by SANOFI, Eli Lilly, AstraZeneca, Abbvie, Servier, Mylan, Gilead, Amgen; he was the scientific director of a Master program on pharmacovigilance, pharmacoepidemiology and real-world evidence which has received non-conditional grant from various pharmaceutical companies; he coordinated a pharmacoepidemiology team at the University of Messina until October 2020, which has received funding for conducting observational studies from various pharmaceutical companies (Boehringer Ingelheim, Daichii Sankyo, PTC Pharmaceuticals). He is also scientific coordinator of the academic spin-off “INSPIRE srl” which has received funding for conducting observational studies from contract research organizations (RTI Health Solutions, Pharmo Institute NV). None of these listed activities are related to the topic of the manuscript.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
All Wales Medicines Strategy Group (2014). Polypharmacy: Guidance for prescribing. Available at: https://awttc.nhs.wales/files/guidelines-and-pils/polypharmacy-guidance-for-prescribing-pdf/.
American Geriatrics Society (2019). American geriatrics society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatrics Soc. 67 (4), 674–694. doi:10.1111/jgs.15767
Anderson, K., Stowasser, D., Freeman, C., and Scott, I. (2014). Prescriber barriers and enablers to minimising potentially inappropriate medications in adults: A systematic review and thematic synthesis. BMJ Open 4 (12), e006544. doi:10.1136/bmjopen-2014-006544
Australian and New Zealand Society for Geriatric Medicine (2018). Position statement 29: Prescribing in older people. Available at: https://anzsgm.org/wp-content/uploads/2019/02/PositionStatementNo29PrescribinginOlder People26March2018.pdf.
Australian Health Ministers’ Advisory Council (2017). National strategic framework for chronic conditions. Available at: https://www.health.gov.au/sites/default/files/documents/2019/09/national-strategic-framework-for-chronic-conditions.pdf.
Avorn, J., and Gurwitz, J. H. (1995). Drug use in the nursing home. Ann. Intern. Med. 123 (3), 195–204. doi:10.7326/0003-4819-123-3-199508010-00007
Benmassaoud, A., McDonald, E. G., and Lee, T. C. (2016). Potential harms of proton pump inhibitor therapy: Rare adverse effects of commonly used drugs. CMAJ Can. Med. Assoc. J. = J. de l’Association Medicale Can. 188 (9), 657–662. doi:10.1503/cmaj.150570
Bergert, F. W., Braun, M., Ehrenthal, K., Feßler, J., Gross, J., Hüttner, U., et al. (2014). Recommendations for treating adult and geriatric patients on multimedication. Int. J. Clin. Pharmacol. Ther. 52 (1), 1–64. doi:10.5414/cpp52s001
Billioti de Gage, S., Moride, Y., Ducruet, T., Kurth, T., Verdoux, H., Tournier, M., et al. (2014). Benzodiazepine use and risk of alzheimer’s disease: Case-control study. BMJ Clin. Res. Ed.) 349, g5205. doi:10.1136/bmj.g5205
Boyd, C., Smith, C. D., Masoudi, F. A., Blaum, C. S., Dodson, J. A., Green, A. R., et al. (2019). Decision making for older adults with multiple chronic conditions: Executive summary for the American geriatrics society guiding principles on the care of older adults with multimorbidity. J. Am. Geriatrics Soc. 67 (4), 665–673. doi:10.1111/jgs.15809
Bryant, L. J. M., Coster, G., Gamble, G. D., and McCormick, R. N. (2011). The general practitioner-pharmacist collaboration (GPPC) study: A randomised controlled trial of clinical medication reviews in community pharmacy. Int. J. Pharm. Pract. 19 (2), 94–105. doi:10.1111/j.2042-7174.2010.00079.x
Calderón-Larrañaga, A., Vetrano, D. L., Onder, G., Gimeno-Feliu, L. A., Coscollar-Santaliestra, C., Carfí, A., et al. (2016). Assessing and measuring chronic multimorbidity in the older population: A proposal for its operationalization. Journals Gerontology Ser. A Biol. Sci. Med. Sci. 72 (10), 1417–1423. doi:10.1093/gerona/glw233
Carrier, H., Zaytseva, A., Bocquier, A., Villani, P., Verdoux, H., Fortin, M., et al. (2019). GPs’ management of polypharmacy and therapeutic dilemma in patients with multimorbidity: A cross-sectional survey of GPs in France. Br. J. General Pract. 69 (681), e270–e278. doi:10.3399/bjgp19X701801
Christensen, M., and Lundh, A. (2016). Medication review in hospitalised patients to reduce morbidity and mortality. Cochrane Database Syst. Rev. 2, CD008986. doi:10.1002/14651858.CD008986.pub3
Cool, C., Cestac, P., McCambridge, C., Rouch, L., de Souto, B. P., Rolland, Y., et al. (2018). Reducing potentially inappropriate drug prescribing in nursing home residents: Effectiveness of a geriatric intervention. Br. J. Clin. Pharmacol. 84 (7), 1598–1610. doi:10.1111/bcp.13598
Damián, J., Pastor-Barriuso, R., Valderrama-Gama, E., and de Pedro-Cuesta, J. (2013). Factors associated with falls among older adults living in institutions. BMC Geriatr. 13, 6. doi:10.1186/1471-2318-13-6
Davies, L. E., Spiers, G., Kingston, A., Todd, A., Adamson, J., and Hanratty, B. (2020). Adverse outcomes of polypharmacy in older people: Systematic review of reviews. J. Am. Med. Dir. Assoc. 21 (2), 181–187. doi:10.1016/j.jamda.2019.10.022
Doherty, A. J., Boland, P., Reed, J., Clegg, A. J., Stephani, A.-M., Williams, N. H., et al. (2020). Barriers and facilitators to deprescribing in primary care: A systematic review. BJGP Open 4 (3), bjgpopen20X101096. doi:10.3399/bjgpopen20X101096
Duncan, P., Duerden, M., and Payne, R. A. (2017). Deprescribing: A primary care perspective. Eur. J. Hosp. Pharm. 24 (1), 37–42. doi:10.1136/ejhpharm-2016-000967
Dwyer, L. L., Han, B., Woodwell, D. A., and Rechtsteiner, E. A. (2010). Polypharmacy in nursing home residents in the United States: Results of the 2004 national nursing home survey. Am. J. Geriatric Pharmacother. 8 (1), 63–72. doi:10.1016/j.amjopharm.2010.01.001
Eggermont, L. H. P., de Vries, K., and Scherder, E. J. A. (2009). Psychotropic medication use and cognition in institutionalized older adults with mild to moderate dementia. Int. Psychogeriatrics 21 (2), 286–294. doi:10.1017/S1041610209008552
Elli, C., Novella, A., Nobili, A., Ianes, A., and Pasina, L. (2022). Anemia in nursing homes, proton pump inhibitors and prescribing cascade of antianemic drugs. Eur. Geriatr. Med. 13 (3), 553–558. doi:10.1007/s41999-022-00636-2
Elli, C., Novella, A., Nobili, A., Ianes, A., and Pasina, L. (2021). Laxative agents in nursing homes: An example of prescribing cascade. J. Am. Med. Dir. Assoc. 22 (12), 2559–2564. doi:10.1016/j.jamda.2021.04.021
Evert, J., Lawler, E., Bogan, H., and Perls, T. (2003). Morbidity profiles of centenarians: Survivors, delayers, and escapers. Journals Gerontology Ser. A Biol. Sci. Med. Sci. 58 (3), M232–M237. doi:10.1093/gerona/58.3.M232
Fog, A. F., Kvalvaag, G., Engedal, K., and Straand, J. (2017). Drug-related problems and changes in drug utilization after medication reviews in nursing homes in Oslo, Norway. Scand. J. Prim. Health Care 35 (4), 329–335. doi:10.1080/02813432.2017.1397246
Formica, D., Sultana, J., Cutroneo, P., Lucchesi, S., Angelica, R., Crisafulli, S., et al. (2018). The economic burden of preventable adverse drug reactions: A systematic review of observational studies. Expert Opin. Drug Saf. 17 (7), 681–695. doi:10.1080/14740338.2018.1491547
Gareri, P., de Fazio, P., Manfredi, V. G. L., and De Sarro, G. (2014). Use and safety of antipsychotics in behavioral disorders in elderly people with dementia. J. Clin. Psychopharmacol. 34 (1), 109–123. doi:10.1097/JCP.0b013e3182a6096e
Guthrie, B., Makubate, B., Hernandez-Santiago, V., and Dreischulte, T. (2015). The rising tide of polypharmacy and drug-drug interactions: Population database analysis 1995-2010. BMC Med. 13, 74. doi:10.1186/s12916-015-0322-7
Hadley, E. C., and Rossi, W. K. (2005). Exceptional survival in human populations: National Institute on Aging perspectives and programs. Mech. Ageing Dev. 126 (2), 231–234. doi:10.1016/j.mad.2004.08.014
Hagberg, B., and Samuelsson, G. (2008). Survival after 100 years of age: A multivariate model of exceptional survival in Swedish centenarians. Journals Gerontology. Ser. A, Biol. Sci. Med. Sci. 63 (11), 1219–1226. doi:10.1093/gerona/63.11.1219
Halli-Tierney, A. D., Scarbrough, C., and Carroll, D. (2019). Polypharmacy: Evaluating risks and deprescribing. Am. Fam. Physician 100 (1), 32–38.
Halvorsen, K. H., Selbaek, G., and Ruths, S. (2017). Trends in potentially inappropriate medication prescribing to nursing home patients: Comparison of three cross-sectional studies. Pharmacoepidemiol. Drug Saf. 26 (2), 192–200. doi:10.1002/pds.4142
Hermann, M., Carstens, N., Kvinge, L., Fjell, A., Wennersberg, M., Folleso, K., et al. (2021). Polypharmacy and potential drug–drug interactions in home-dwelling older people – a cross-sectional study. J. Multidiscip. Healthc. 14, 589–597. doi:10.2147/JMDH.S297423
Herr, M., Grondin, H., Sanchez, S., Armaingaud, D., Blochet, C., Vial, A., et al. (2017). Polypharmacy and potentially inappropriate medications: A cross-sectional analysis among 451 nursing homes in France. Eur. J. Clin. Pharmacol. 73 (5), 601–608. doi:10.1007/s00228-016-2193-z
Hoonhout, L. H. F., de Bruijne, M. C., Wagner, C., Asscheman, H., van der Wal, G., and van Tulder, M. W. (2010). Nature, occurrence and consequences of medication-related adverse events during hospitalization: A retrospective chart review in The Netherlands. Drug Saf. 33 (10), 853–864. doi:10.2165/11536800-000000000-00000
Husebø, B. S., Ballard, C., Aarsland, D., Selbaek, G., Slettebo, D. D., Gulla, C., et al. (2019). The effect of a multicomponent intervention on quality of life in residents of nursing homes: A randomized controlled trial (COSMOS). J. Am. Med. Dir. Assoc. 20 (3), 330–339. doi:10.1016/j.jamda.2018.11.006
Ibrahim, K., Cox, N. J., Stevenson, J. M., Lim, S., Fraser, S. D. S., and Roberts, H. C. (2021). A systematic review of the evidence for deprescribing interventions among older people living with frailty. BMC Geriatr. 21 (1), 258. doi:10.1186/s12877-021-02208-8
Istituto Farmacologico e di Ricerca Mario Negri (2022). INTERCheck web. Available at: https://intercheckweb.marionegri.it/.
Istituto Nazionale di Statistica (Istat) (2020). Aspetti di vita degli over 75. Available at: https://www.istat.it/it/archivio/241894.
Johnell, K., and Klarin, I. (2007). The relationship between number of drugs and potential drug-drug interactions in the elderly: A study of over 600, 000 elderly patients from the Swedish prescribed drug register. Drug Saf. 30 (10), 911–918. doi:10.2165/00002018-200730100-00009
Johnston, M. C., Crilly, M., Black, C., Prescott, G. J., and Mercer, S. W. (2019). Defining and measuring multimorbidity: A systematic review of systematic reviews. Eur. J. Public Health 29 (1), 182–189. doi:10.1093/eurpub/cky098
Kojima, G., Bell, C., Tamura, B., Inaba, M., Lubimir, K., Blanchette, P. L., et al. (2012). Reducing cost by reducing polypharmacy: The polypharmacy outcomes project. J. Am. Med. Dir. Assoc. 13 (9), e11–e15. doi:10.1016/j.jamda.2012.07.019
Kojima, T., Akishita, M., Nakamura, T., Nomura, K., Ogawa, S., Iijima, K., et al. (2011). Association of polypharmacy with fall risk among geriatric outpatients. Geriatrics Gerontology Int. 11 (4), 438–444. doi:10.1111/j.1447-0594.2011.00703.x
Kua, C.-H., Mak, V. S. L., and Huey Lee, S. W. (2019). Health outcomes of deprescribing interventions among older residents in nursing homes: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 20 (3), 362–372. e11. doi:10.1016/j.jamda.2018.10.026
Kwak, M. J., Chang, M., Chiadika, S., Aguilar, D., Avritscher, E., Deshmukh, A., et al. (2022). Healthcare expenditure associated with polypharmacy in older adults with cardiovascular diseases. Am. J. Cardiol. 169, 156–158. doi:10.1016/j.amjcard.2022.01.012
Laberge, M., Sirois, C., Lunghi, C., Gaudreault, M., Nakamura, Y., Bolduc, C., et al. (2021). Economic evaluations of interventions to optimize medication use in older adults with polypharmacy and multimorbidity: A systematic review. Clin. Interventions Aging 16, 767–779. doi:10.2147/CIA.S304074
Lazarou, J., Pomeranz, B. H., and Corey, P. N. (1998). Incidence of adverse drug reactions in hospitalized patients. A meta-analysis of prospective studies. JAMA 279 (15), 1200–1205. doi:10.1001/jama.279.15.1200
Leelakanok, N., Holcombe, A. L., Lund, B. C., Gu, X., and Schweizer, M. L. (2017). Association between polypharmacy and death: A systematic review and meta-analysis. J. Am. Pharm. Assoc. 57 (6), 729–738. e10. doi:10.1016/j.japh.2017.06.002
Luymes, C. H., Poortvliet, R. K. E., van Geloven, N., de Waal, M. W. M., Drewes, Y. M., Blom, J. W., et al. (2018). Deprescribing preventive cardiovascular medication in patients with predicted low cardiovascular disease risk in general practice - the ECSTATIC study: A cluster randomised non-inferiority trial. BMC Med. 16 (1), 5. doi:10.1186/s12916-017-0988-0
MacRae, C., Henderson, D. A., Mercer, S. W., Burton, J., De Souza, N., Grill, P., et al. (2021). Excessive polypharmacy and potentially inappropriate prescribing in 147 care homes: A cross-sectional study. BJGP Open 5 (6), BJGPO.2021.0167. doi:10.3399/BJGPO.2021.0167
Mahlknecht, A., Wiedermann, C. J., Sandri, M., Engl, A., Valentini, M., Vögele, A., et al. (2021). Expert-based medication reviews to reduce polypharmacy in older patients in primary care: A northern-Italian cluster-randomised controlled trial. BMC Geriatr. 21 (1), 659. doi:10.1186/s12877-021-02612-0
Mair, A., Wilson, M., and Dreischulte, T. (2020). Addressing the challenge of polypharmacy. Annu. Rev. Pharmacol. Toxicol. 60, 661–681. doi:10.1146/annurev-pharmtox-010919-023508
Mangin, D., Bahat, G., Golomb, B. A., Mallery, L. H., Moorhouse, P., Onder, G., et al. (2018). International group for reducing inappropriate medication use & polypharmacy (IGRIMUP): Position statement and 10 recommendations for action. Drugs & Aging 35 (7), 575–587. doi:10.1007/s40266-018-0554-2
Marcum, Z. A., and Gellad, W. F. (2012). Medication adherence to multidrug regimens. Clin. Geriatric Med. 28 (2), 287–300. doi:10.1016/j.cger.2012.01.008
Masnoon, N., Shakib, S., Kalisch-Ellett, L., and Caughey, G. E. (2017). What is polypharmacy? A systematic review of definitions. BMC Geriatr. 17 (1), 230. doi:10.1186/s12877-017-0621-2
McCarthy, C., Clyne, B., Boland, F., Moriarty, F., Flood, M., Wallace, E., et al. (2022). GP-delivered medication review of polypharmacy, deprescribing, and patient priorities in older people with multimorbidity in Irish primary care (SPPiRE study): A cluster randomised controlled trial. PLoS Med. 19 (1), e1003862. doi:10.1371/journal.pmed.1003862
Muth, C., Blom, J. W., Smith, S. M., Johnell, K., Gonzalez-Gonzalez, A. I., Nguyen, T. S., et al. (2019). Evidence supporting the best clinical management of patients with multimorbidity and polypharmacy: A systematic guideline review and expert consensus. J. Intern. Med. 285 (3), 272–288. doi:10.1111/joim.12842
National Institute for Health and Care Excellence (NICE) (2016). Multimorbidity: Clinical assessment and management. Available at: https://www.nice.org.uk/guidance/ng56/evidence/full-guideline-pdf-2615543103.
National Institute for Health and Care Excellence (NICE) (2015). Older people with social care needs and multiple long-term conditions. Available at: https://www.nice.org.uk/guidance/ng22/resources/older-people-with-social-care-needs-and-multiple-longterm-conditions-pdf-1837328537797.
Nederlands Huisartsen Genootschap (NHG) (2012). Multidisciplinaire richtlijn polyfarmacie bij ouderen. Available at: Https://Richtlijnendatabase.Nl/Richtlijn/Polyfarmacie_bij_ouderen/Polyfarmacie_bij_ouderen_-_korte_beschrijving.Html#:∼:Text=Deze%20richtlijn%20richt%20zich%20op,De%20uitvoering%20van%20de%20medicatiebeoordeling.
NHMRC Cognitive Decline Partnership Centre (2018). Quality use of medicines to optimise ageing in older Australians: Recommendations for a national strategic action plan to reduce inappropriate polypharmacy. Available at: https://cdpc.sydney.edu.au/wp-content/uploads/2019/06/quality-use-of-medicines.pdf.
Nijk, R. M., Zuidema, S. U., and Koopmans, R. T. C. M. (2009). Prevalence and correlates of psychotropic drug use in Dutch nursing-home patients with dementia. Int. Psychogeriatrics 21 (3), 485–493. doi:10.1017/S1041610209008916
Novaes, P. H., Da Cruz, D. T., Lucchetti, A. L. G., Leite, I. C. G., and Lucchetti, G. (2017). The “iatrogenic triad”: Polypharmacy, drug–drug interactions, and potentially inappropriate medications in older adults. Int. J. Clin. Pharm. 39 (4), 818–825. doi:10.1007/s11096-017-0470-2
Onder, G., Vetrano, D. L., Palmer, K., Trevisan, C., Amato, L., Berti, F., et al. (2022). Italian guidelines on management of persons with multimorbidity and polypharmacy. Aging Clin. Exp. Res. 34 (5), 989–996. doi:10.1007/s40520-022-02094-z
Oscanoa, T. J., Lizaraso, F., and Carvajal, A. (2017). Hospital admissions due to adverse drug reactions in the elderly. A meta-analysis. Eur. J. Clin. Pharmacol. 73 (6), 759–770. doi:10.1007/s00228-017-2225-3
Osheroff, J. (2012). Improving outcomes with clinical decision support. Chicago: HIMSS Publishing. doi:10.4324/9781498757461
Oyarzun-Gonzalez, X. A., Taylor, K. C., Myers, S. R., Muldoon, S. B., and Baumgartner, R. N. (2015). Cognitive decline and polypharmacy in an elderly population. J. Am. Geriatrics Soc. 63 (2), 397–399. doi:10.1111/jgs.13283
Palmer, K., Marengoni, A., Forjaz, M. J., Jureviciene, E., Laatikainen, T., Mammarella, F., et al. (2018). Multimorbidity care model: Recommendations from the consensus meeting of the joint action on chronic diseases and promoting healthy ageing across the life cycle (JA-CHRODIS). Health Policy 122 (1), 4–11. doi:10.1016/j.healthpol.2017.09.006
Park, H.-Y., Park, J.-W., Song, H. J., Sohn, H. S., and Kwon, J.-W. (2017). The association between polypharmacy and dementia: A nested case-control study based on a 12-year longitudinal cohort database in South Korea. PLOS ONE 12 (1), e0169463. doi:10.1371/journal.pone.0169463
Pasina, L., Brucato, A. L., Falcone, C., Cucchi, E., Bresciani, A., Sottocorno, M., et al. (2014). Medication non-adherence among elderly patients newly discharged and receiving polypharmacy. Drugs & Aging 31 (4), 283–289. doi:10.1007/s40266-014-0163-7
Pasina, L., Marengoni, A., Ghibelli, S., Suardi, F., Djade, C. D., Nobili, A., et al. (2016). A multicomponent intervention to optimize psychotropic drug prescription in elderly nursing home residents: An Italian multicenter, prospective, pilot study. Drugs & Aging 33 (2), 143–149. doi:10.1007/s40266-015-0336-z
Pasina, L., Novella, A., Cortesi, L., Nobili, A., Tettamanti, M., Ianes, A., et al. (2020). Drug prescriptions in nursing home residents: An Italian multicenter observational study. Eur. J. Clin. Pharmacol. 76 (7), 1011–1019. doi:10.1007/s00228-020-02871-7
Pasina, L., Novella, A., Elli, C., Nobili, A., and Ianes, A. (2020b). Inappropriate use of antiplatelet agents for primary prevention in nursing homes: An Italian multicenter observational study. Geriatrics Gerontology Int. 20 (9), 828–832. doi:10.1111/ggi.13984
Pasina, L., Novella, A., Elli, C., Nobili, A., and Ianes, A. (2020a). Overuse of proton pump inhibitors in nursing homes: An Italian multicenter observational study. Pharmacoepidemiol. Drug Saf. 29 (4), 461–466. doi:10.1002/pds.4963
Payne, R. A., Abel, G. A., Avery, A. J., Mercer, S. W., and Roland, M. O. (2014). Is polypharmacy always hazardous? A retrospective cohort analysis using linked electronic health records from primary and secondary care. Br. J. Clin. Pharmacol. 77 (6), 1073–1082. doi:10.1111/bcp.12292
Pazan, F., and Wehling, M. (2021). Polypharmacy in older adults: A narrative review of definitions, epidemiology and consequences. Eur. Geriatr. Med. 12 (3), 443–452. doi:10.1007/s41999-021-00479-3
Peralta-Pedrero, M. L., Valdivia-Ibarra, F. J., Hernández-Manzano, M., Medina-Beltrán, G. R., Cordero-Guillén, M. A., Baca-Zúñiga, J., et al. (2013). Clinical practice guideline. Drug prescription in elderly. Rev. Medica Del Inst. Mex. Del Seguro Soc. 51 (2), 228–239.
Plüss-Suard, C., Niquille, A., Héquet, D., Krähenbühl, S., Pichon, R., Zanetti, G., et al. (2020). Decrease in antibacterial use and facilitylevel variability after the introduction of guidelines and implementation of physician-pharmacist-nurse quality circles in Swiss long-term care facilities. J. Am. Med. Dir. Assoc. 21 (1), 78–83. doi:10.1016/j.jamda.2019.05.016
Rankin, A., Cadogan, C. A., Patterson, S. M., Kerse, N., Cardwell, C. R., Bradley, M. C., et al. (2018). Interventions to improve the appropriate use of polypharmacy for older people. Cochrane Database Syst. Rev. 9, CD008165. doi:10.1002/14651858.CD008165.pub4
Rawle, M. J., Cooper, R., Kuh, D., and Richards, M. (2018). Associations between polypharmacy and cognitive and physical capability: A British birth cohort study. J. Am. Geriatrics Soc. 66 (5), 916–923. doi:10.1111/jgs.15317
Ray, W. A., Taylor, J. A., Meador, K. G., Lichtenstein, M. J., Griffin, M. R., Fought, R., et al. (1993). Reducing antipsychotic drug use in nursing homes. A controlled trial of provider education. Archives Intern. Med. 153 (6), 713–721. doi:10.1001/archinte.153.6.713
Reeve, E., Gnjidic, D., Long, J., and Hilmer, S. (2015). A systematic review of the emerging definition of 'deprescribing' with network analysis: Implications for future research and clinical practice. Br. J. Clin. Pharmacol. 80 (6), 1254–1268. doi:10.1111/bcp.12732
Reeve, E., Shakib, S., Hendrix, I., Roberts, M. S., and Wiese, M. D. (2014). Review of deprescribing processes and development of an evidence-based, patient-centred deprescribing process. Br. J. Clin. Pharmacol. 78 (4), 738–747. doi:10.1111/bcp.12386
Reeve, E., To, J., Hendrix, I., Shakib, S., Roberts, M. S., and Wiese, M. D. (2013). Patient barriers to and enablers of deprescribing: A systematic review. Drugs & Aging 30 (10), 793–807. doi:10.1007/s40266-013-0106-8
Rieckert, A., Reeves, D., Altiner, A., Drewelow, E., Esmail, A., Flamm, M., et al. (2020m1822). Use of an electronic decision support tool to reduce polypharmacy in elderly people with chronic diseases: Cluster randomised controlled trial. BMJ Clin. Res. Ed.) 369, m1822. doi:10.1136/bmj.m1822
Rochon, P. A., and Gurwitz, J. H. (2017). The prescribing cascade revisited. Lancet 389 (10081), 1778–1780. doi:10.1016/S0140-6736(17)31188-1
Rockwood, K., and Mitnitski, A. (2007). Frailty in relation to the accumulation of deficits. Journals Gerontology Ser. A Biol. Sci. Med. Sci. 62 (7), 722–727. doi:10.1093/gerona/62.7.722
Ruggiero, C., Dell’Aquila, G., Gasperini, B., Onder, G., Lattanzio, F., Volpato, S., et al. (2010). Potentially inappropriate drug prescriptions and risk of hospitalization among older, Italian, nursing home residents: The ULISSE project. Drugs & Aging 27 (9), 747–758. doi:10.2165/11538240-000000000-00000
Santos, T. R. A., Silveira, E. A., Pereira, L. V., Provin, M. P., Lima, D. M., and Amaral, R. G. (2017). Potential drug-drug interactions in older adults: A population-based study. Geriatrics Gerontology Int. 17 (12), 2336–2346. doi:10.1111/ggi.13070
Scherer, M., Wagner, H. O., Lühmann, D., Muche-Borowski, C., Schäfer, I., Dubben, H. H., et al. (2017). Multimorbidität. Available at: https://www.degam.de/files/Inhalte/Leitlinien-Inhalte/Dokumente/DEGAM-S3-Leitlinien/053-047_Multimorbiditaet/053-047l_%20Multimorbiditaet_redakt_24-1-18.pdf.
Scott, I. A., Hilmer, S. N., Reeve, E., Potter, K., le Couteur, D., Rigby, D., et al. (2015). Reducing inappropriate polypharmacy: The process of deprescribing. JAMA Intern. Med. 175 (5), 827–834. doi:10.1001/jamainternmed.2015.0324
Scottish Government Polypharmacy Model of Care Group (2018). Polypharmacy guidance, realistic prescribing 3 rd edition. Available at: https://www.therapeutics.scot.nhs.uk/wp-content/uploads/2018/09/Polypharmacy-Guidance-2018.pdf.
Selbaek, G., Kirkevold, Ø., and Engedal, K. (2007). The prevalence of psychiatric symptoms and behavioural disturbances and the use of psychotropic drugs in Norwegian nursing homes. Int. J. Geriatric Psychiatry 22 (9), 843–849. doi:10.1002/gps.1749
Seppala, L. J., Petrovic, M., Ryg, J., Bahat, G., Topinkova, E., Szczerbińska, K., et al. (2021). STOPPFall (screening tool of older persons prescriptions in older adults with high fall risk): A delphi study by the EuGMS task and finish group on fall-risk-increasing drugs. Age Ageing 50 (4), 1189–1199. doi:10.1093/ageing/afaa249
Sheikh-Taha, M., and Asmar, M. (2021). Polypharmacy and severe potential drug-drug interactions among older adults with cardiovascular disease in the United States. BMC Geriatr. 21 (1), 233. doi:10.1186/s12877-021-02183-0
Sirois, C., Domingues, N. S., Laroche, M.-L., Zongo, A., Lunghi, C., Guénette, L., et al. (2019). Polypharmacy definitions for multimorbid older adults need stronger foundations to guide research, clinical practice and public health. Pharmacy 7 (3), 126. doi:10.3390/pharmacy7030126
Sloane, P. D., Mathew, L. J., Scarborough, M., Desai, J. R., Koch, G. G., and Tangen, C. (1991). Physical and pharmacologic restraint of nursing home patients with dementia. Impact of specialized units. JAMA 265 (10), 1278–1282. doi:10.1001/jama.1991.03460100080028
Spinewine, A., Evrard, P., and Hughes, C. (2021). Interventions to optimize medication use in nursing homes: A narrative review. Eur. Geriatr. Med. 12 (3), 551–567. doi:10.1007/s41999-021-00477-5
Strauven, G., Anrys, P., Vandael, E., Henrard, S., De Lepeleire, J., Spinewine, A., et al. (2019). Cluster-controlled trial of an intervention to improve prescribing in nursing homes study. J. Am. Med. Dir. Assoc. 20 (11), 1404–1411. doi:10.1016/j.jamda.2019.06.006
Teramura-Grönblad, M., Hosia-Randell, H., Muurinen, S., and Pitkala, K. (2010). Use of proton-pump inhibitors and their associated risks among frail elderly nursing home residents. Scand. J. Prim. Health Care 28 (3), 154–159. doi:10.3109/02813432.2010.493315
Teramura-Grönblad, M., Raivio, M., Savikko, N., Muurinen, S., Soini, H., Suominen, M., et al. (2016). Potentially severe drug-drug interactions among older people and associations in assisted living facilities in Finland: A cross-sectional study. Scand. J. Prim. Health Care 34 (3), 250–257. doi:10.1080/02813432.2016.1207142
The Medicines Utilisation Monitoring Centre of the Italian Medicines Agency (2020). National Report on Medicines use in older adults in Italy. Year 2019. Available at: https://www.aifa.gov.it/documents/20142/241052/OsMed_2019_Eng.pdf.
The Medicines Utilisation Monitoring Centre of the Italian Medicines Agency (2022). National report on medicines use in Italy. Year 2021. Available at: https://www.aifa.gov.it/documents/20142/1740782/Rapporto-OsMed-2021.pdf.
Thompson, W., Reeve, E., Moriarty, F., Maclure, M., Turner, J., Steinman, M. A., et al. (2019). Deprescribing: Future directions for research. Res. Soc. Adm. Pharm. 15 (6), 801–805. doi:10.1016/j.sapharm.2018.08.013
Topinková, E., Baeyens, J. P., Michel, J.-P., and Lang, P.-O. (2012). Evidence-based strategies for the optimization of pharmacotherapy in older people. Drugs & Aging 29 (6), 477–494. doi:10.2165/11632400-000000000-00000
van der Cammen, T. J. M., Rajkumar, C., Onder, G., Sterke, C. S., and Petrovic, M. (2014). Drug cessation in complex older adults: Time for action. Age Ageing 43 (1), 20–25. doi:10.1093/ageing/aft166
van Dijk, K. N., de Vries, C. S., van den Berg, P. B., Brouwers, J. R., and De Jong-van den Berg, L. T. (2000). Drug utilisation in Dutch nursing homes. Eur. J. Clin. Pharmacol. 55 (10), 765–771. doi:10.1007/s002280050012
Veronese, N., Custodero, C., Cella, A., Demurtas, J., Zora, S., Maggi, S., et al. (2021). Prevalence of multidimensional frailty and pre-frailty in older people in different settings: A systematic review and meta-analysis. Ageing Res. Rev. 72, 101498. doi:10.1016/j.arr.2021.101498
Vetrano, D. L., Palmer, K., Marengoni, A., Marzetti, E., Lattanzio, F., Roller-Wirnsberger, R., et al. (2019). Frailty and multimorbidity: A systematic review and meta-analysis. Journals Gerontology Ser. A 74 (5), 659–666. doi:10.1093/gerona/gly110
Wastesson, J. W., Morin, L., Tan, E. C. K., and Johnell, K. (2018). An update on the clinical consequences of polypharmacy in older adults: A narrative review. Expert Opin. Drug Saf. 17 (12), 1185–1196. doi:10.1080/14740338.2018.1546841
Weeks, W. B., Mishra, M. K., Curto, D., Petersen, C. L., Cano, P., Hswen, Y., et al. (2019). Comparing three methods for reducing psychotropic use in older demented Spanish care home residents. J. Am. Geriatr. Soc. 67 (7), 1444–1453. doi:10.1111/jgs.15855
Weich, S., Pearce, H. L., Croft, P., Singh, S., Crome, I., Bashford, J., et al. (2014). Effect of anxiolytic and hypnotic drug prescriptions on mortality hazards: Retrospective cohort study. BMJ Clin. Res. Ed.) 348, g1996. doi:10.1136/bmj.g1996
Wetzels, R. B., Zuidema, S. U., de Jonghe, J. F. M., Verhey, F. R. J., and Koopmans, R. T. C. M. (2011). Prescribing pattern of psychotropic drugs in nursing home residents with dementia. Int. Psychogeriatrics 23 (8), 1249–1259. doi:10.1017/S1041610211000755
Wolff, J., Hefner, G., Normann, C., Kaier, K., Binder, H., Hiemke, C., et al. (2021). Polypharmacy and the risk of drug–drug interactions and potentially inappropriate medications in hospital psychiatry. Pharmacoepidemiol. Drug Saf. 30 (9), 1258–1268. doi:10.1002/pds.5310
Wouters, H., Scheper, J., Koning, H., Brouwer, C., Twisk, J. W., van der Meer, H., et al. (2017). Discontinuing inappropriate medication use in nursing home residents: A cluster randomized controlled trial. Ann. Intern. Med. 167 (9), 609–617. doi:10.7326/M16-2729
Zaninotto, P., Huang, Y. T., Di Gessa, G., Abell, J., Lassale, C., and Steptoe, A. (2020). Polypharmacy is a risk factor for hospital admission due to a fall: Evidence from the English longitudinal study of ageing. BMC Public Health 20 (1), 1804. doi:10.1186/s12889-020-09920-x
Zazzara, M. B., Cangini, A., Da Cas, R., Ippoliti, I., Marengoni, A., Pierantozzi, A., et al. (2022). Medication use and costs among older adults aged 90 Years and older in Italy. Front. Pharmacol. 13, 818875. doi:10.3389/fphar.2022.818875
Keywords: deprescribing, multimorbidity, polypharmacy, elderly, geriatrics
Citation: Crisafulli S, Poluzzi E, Lunghi C, Di Francesco V, Pellizzari L, Pasina L, Elli C, Trotta F, Cangini A, Trevisan C, Zazzara MB, Onder G and Trifirò G (2022) Deprescribing as a strategy for improving safety of medicines in older people: Clinical and regulatory perspective. Front. Drug Saf. Regul. 2:1011701. doi: 10.3389/fdsfr.2022.1011701
Received: 04 August 2022; Accepted: 12 December 2022;
Published: 23 December 2022.
Edited by:
Hai-Yan Qian, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaReviewed by:
Daniel Morales, University of Dundee, United KingdomMarios Kyriazis, National Gerontology Centre, Cyprus
Copyright © 2022 Crisafulli, Poluzzi, Lunghi, Di Francesco, Pellizzari, Pasina, Elli, Trotta, Cangini, Trevisan, Zazzara, Onder and Trifirò. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gianluca Trifirò, Z2lhbmx1Y2EudHJpZmlyb0B1bml2ci5pdA==