Factors associated with anxiety about handling contaminated patients during a nuclear disaster among disaster medical assistant teams in Japan: a cross-sectional study
 Hisami Shibata1
Hisami Shibata1  Takumi Yamaguchi2,3,4* Yumiko Yamada5 Tetsuko Shinkawa6 Hideko Urata6 Yuko Matsunari4
Takumi Yamaguchi2,3,4* Yumiko Yamada5 Tetsuko Shinkawa6 Hideko Urata6 Yuko Matsunari4- 1Department of Nursing, Nagasaki University Hospital, Nagasaki, Japan
- 2Research Administration Center, Saitama Medical University, Saitama, Japan
- 3Nuclear Safety Research Association, Tokyo, Japan
- 4School of Health Sciences, Kagoshima University, Kagoshima, Japan
- 5School of Nursing, Kwassui Women's University, Nagasaki, Japan
- 6Atomic Bomb Disease Institute, Nagasaki University, Nagasaki, Japan
Introduction: Japanese Disaster Medical Assistance Teams (DMATs) are pivotal in disaster response, especially during nuclear crises. The objective of this study was to identify factors associated with anxiety among Japanese DMAT personnel when handling contaminated patients during nuclear disasters.
Materials and methods: In this cross-sectional study, 609 Japanese DMAT members from Kyushu and Okinawa, Japan, were surveyed. Multivariate binomial logistic regression was used to determine anxiety predictors.
Results: Of the 276 respondents, 77.2% expressed anxiety about managing contaminated patients. Women and younger team members expressed the highest level of anxiety associated with handling contaminated patients during nuclear disasters.
Conclusion: This study revealed heightened anxiety among female and younger Japanese DMAT personnel regarding the handling of contaminated patients during nuclear disasters. Targeted training addressing these concerns is essential for effective disaster response.
1 Introduction
The Great Hanshin-Awaji Earthquake disaster of 1995 resulted in numerous preventable deaths, with many injured and sick individuals succumbing because of a lack of adequate medical care in the affected regions (1, 2). This tragic event underscored the urgent need for an improved disaster medical response. Consequently, in 2005, the Ministry of Health, Labor and Welfare established the Japanese Disaster Medical Assistance Team (DMAT) scheme (3). This initiative is in line with the Basic Plan for Disaster Management (4), which aims to provide prompt and effective medical care during major human-made or natural disasters. In countries frequently impacted by various calamities, Japanese DMATs are indispensable for providing an emergency response. Given the critical nature of their responsibilities, Japanese DMAT members often encounter unique psychological challenges. Ensuring their mental wellbeing is crucial for an effective disaster response (5, 6).
The devastating Great East Japan Earthquake and Tsunami in March 2011 led to significant casualties from both the earthquake and the subsequent tsunamis. This disaster was further compounded by the nuclear accident at the Fukushima Daiichi Nuclear Power Station (7). Recognizing the potential risks, it became imperative to establish personal radiation exposure doses for Japanese DMAT members to guarantee their safety and efficiency during nuclear disaster interventions (8).
While there is ample documentation on general anxiety and stress factors affecting emergency responders, there is limited research on the specific causes of anxiety experienced by Japanese DMAT personnel in nuclear disaster situations (9). It is essential to consider the unique cultural, training, and experiential aspects that might distinguish Japanese DMAT members from their international peers.
This study aims to identify the primary factors contributing to anxiety among Japanese DMAT personnel during nuclear disaster response missions. By examining a distinct population (Japanese DMAT members) in a specialized context (nuclear disaster response), this study endeavors to bridge an existing knowledge gap.
2 Materials and methods
2.1 Study design
This study employed a cross-sectional, observational study design.
2.2 Setting
A request for study collaboration was mailed to the directors of 138 Japanese DMAT-designated medical institutions in Kyushu and Okinawa, Japan. Out of these, 55 institutions granted their consent, and a total of 609 Japanese DMAT team members affiliated with these institutions were surveyed. The study was conducted from December 2018 to February 2019.
2.3 Participants
Questionnaires, along with return envelopes, were dispatched to the 55 consenting Japanese DMAT-designated medical institutions in Kyushu and Okinawa. These institutions were requested to distribute the questionnaires to the study participants. The questionnaire detailed the study's objectives and ethical considerations. The participants were instructed to return the questionnaires after completion using the provided return envelopes.
Out of the 609 subjects, 332 (54.5%) responded. After the exclusion of 56 questionnaires with incomplete answers, 276 were considered for the analysis.
2.4 Variables
Survey items were derived from a prior study (10). Demographic variables included “job title,” “gender,” “age,” “years of Japanese DMAT experience,” “marital status,” “having children,” “emergency medical experience,” “radiology experience,” “nuclear disaster dispatch experience,” “nuclear disaster training experience,” “participation in prefecture-hosted training,” “dispatch team affiliation,” “nuclear power plant located in prefecture,” “residence within the UPZ (Urgent Protection action planning Zone),” “affiliation to nuclear disaster medicine facilities,” and “holds training experience.” Additionally, participants were queried with respect to their “understanding of nuclear disaster medicine,” “interest in nuclear disaster medicine,” “willingness to participate in nuclear disaster medicine,” and “anxiety about treating contaminated patients during nuclear disasters.”
2.5 Statistical methods
Both univariate and multivariate binomial logistic regression analyses were performed, with “anxiety about treating contaminated patients during nuclear disasters” as the dependent variable. Variables with a P < 0.1 in the univariate analysis were included in the multivariate model (11). Given the potential for the “job title” variable to act as a confounder, it was incorporated into the model as an adjustment variable, irrespective of the univariate analysis results. The forced entry method was employed for model selection, and coefficients, odds ratios (ORs), 95% confidence intervals (CIs), and P values were computed. The Hosmer-Lemeshow test yielded a value of 0.687, indicating adequate model fit. Furthermore, in the model of multiple logistic regression analysis in this study, 13 variables were entered as explanatory and adjustment variables; according to Peduzzi et al., an EPV value of 10 or greater does not cause major problems in bias, precision, and significance testing. The EPV value in this study was approximately 19.7, which was an appropriate model selection (12). All variance inflation factors in the multivariate analysis were ≤ 2.357, indicating no multicollinearity concerns (values < 2.5 are considered acceptable). Statistical analyses were executed using R version 4.3.1, with a significance level set at P < 0.05.
2.6 Ethical consideration
Participants were informed about the study's details and provided their informed consent before completing the questionnaire. This research adhered to the principles of the Declaration of Helsinki and received approval from the Ethics Committee of Nagasaki University Graduate School of Biomedical Sciences (approval number: 18113001).
3 Results
3.1 Descriptive statistics
Table 1 presents the descriptive statistics of the participants. Of the 276 respondents, 81 (29.3%) were medical doctors, 104 (37.7%) were nurses, and 91 (33.0%) were operations coordinators. A majority, 187 (67.8%), had experience in emergency medicine, while 52 (18.8%) had radiology experience. Among the participants, 166 (60.1%) had children, and 158 (57.2%) had previously been dispatched for disaster relief. Only six participants (2.2%) had experience in nuclear disaster relief. Other notable statistics include 69 (25.0%) participants with nuclear disaster training experience, 39 (14.1%) who had participated in prefecture-sponsored training, and 70 (25.4%) residing in a nuclear power plant's vicinity. The median number of years of participants' overall experience, Japanese DMAT experience, and age were 16.0, 4.0, and 41.0 years, respectively, with interquartile ranges of 12.0, 5.0, and 13.0 years, respectively.
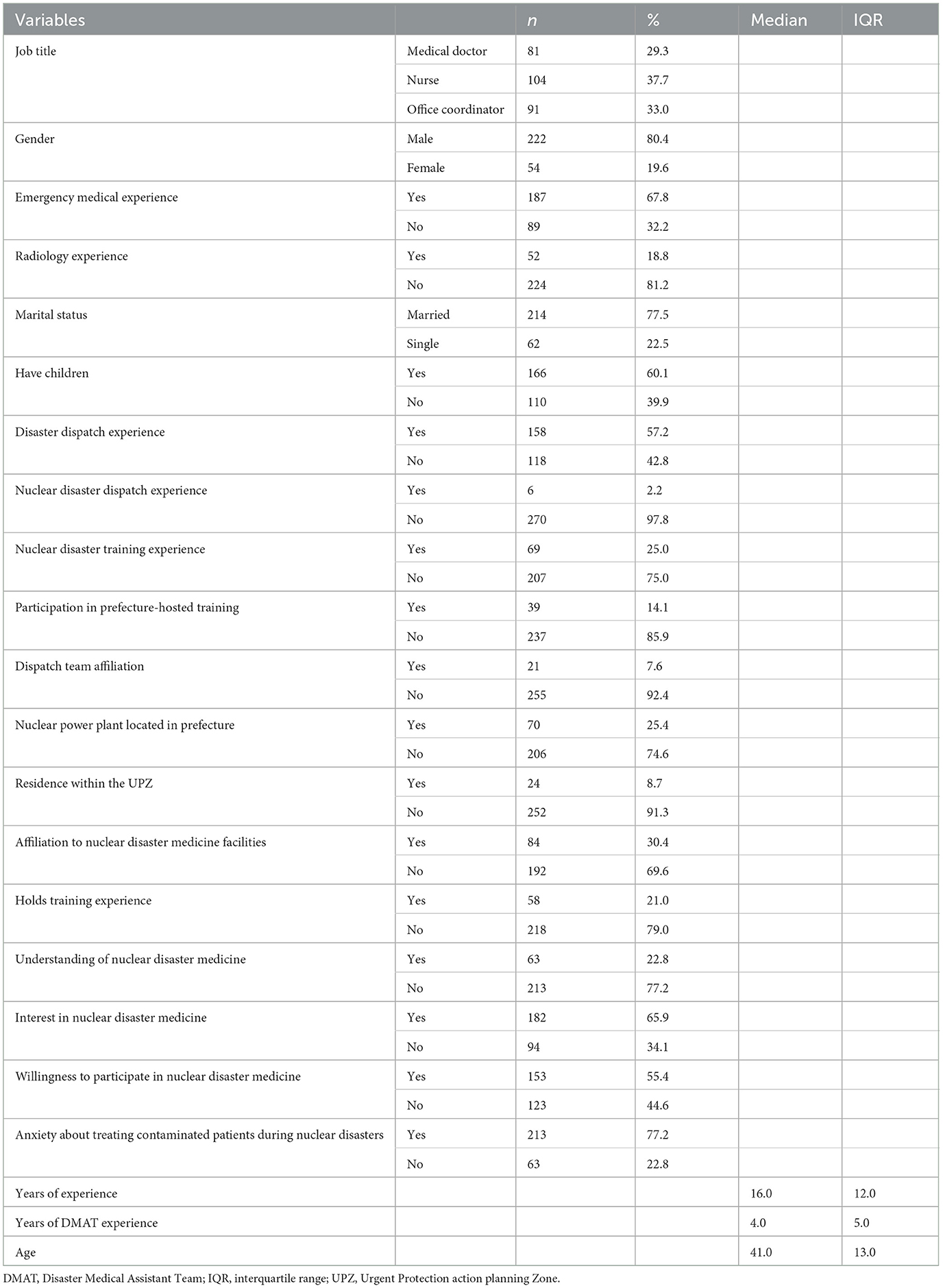
Table 1. Descriptive statistics of the study participants.
Additionally, 77.2% of the study subjects had concerns about how to deal with contaminated and injured people in the event of a nuclear disaster (Figure 1).
Figure 1. The proportion of anxiety about treating contaminated patients during nuclear disasters.
3.2 Results of multiple binominal logistic regression analysis
The univariate binomial logistic regression analysis (where B indicates the binomial regression coefficient) yielded the following significant variables with P < 0.1: “gender” (B = 0.82, OR = 2.27, 95%CI = 0.97–5.30, P = 0.06), “radiology experience” (B = 0.86, OR = 2.36, 95%CI = 1.23–4.53, P = 0.01), “nuclear disaster dispatch experience” (B = 2.91, OR = 18.28, 95%CI = 2.09–159.52, P = 0.01), “nuclear disaster training experience” (B = 0.93, OR = 2.53, 95%CI = 1.38–4.62, P < 0.001), “participation in prefecture–hosted training” (B = 0.90, OR = 2.46, 95%CI = 1.20–5.05, P = 0.01), “dispatch team affiliation” (B = 0.81, OR = 2.24, 95%CI = 0.88–5.67, P = 0.09), “affiliation to nuclear disaster medicine facilities” (B = 0.63, OR = 1.88, 95%CI = 1.05–3.37, P = 0.03), “holds training experience” (B = 0.87, OR = 2.38, 95%CI = 1.26–4.48, P = 0.01),” “understanding of nuclear disaster medicine” (B = 1.30, OR = 3.69–1.99, 95%CI = 6.82, P < 0.001), “willingness to participate in nuclear disaster medicine” (B = 0.70, OR = 2.01, 95%CI = 1.11–3.65, P = 0.02), “years of experience (B = −0.04, OR = 0.97, 95%CI = 0.93–1.00, P = 0.05),” “age” (B = −0.04, OR = 0.96, 95%CI = 0.93–0.99, P = 0.01), and “years of Japanese DMAT experience” (B = −0.10, OR = 0.91, 95%CI = 0.83–0.99, P = 0.03).
In addition to the aforementioned analyses, a post-hoc power analysis was conducted to confirm the adequacy of the sample size and the statistical detection power of gender effects within our study. This analysis utilized the adjusted odds ratio (aOR = 2.826) associated with gender (female) along with the total sample size (n = 276) and a significance level (α = 0.05). Utilizing the g*Power software for this calculation, the power (1-β error probability) was determined to be 0.977. This result indicates that the sample size of our study was sufficiently robust for statistically detecting the effects of gender, affirming the statistical validity of our analysis. Owing to potential multicollinearity, a multivariate binomial logistic regression analysis excluding the variable “years of Japanese DMAT experience” was also conducted. After adjusting for the variable “job title,” the variables “female gender” (B = 1.039, aOR = 2.826, 95%CI = 1.179–7.775, P = 0.029), and “younger age” (B = −0.044, aOR = 0.956, 95%CI = 0.915–1.000, P = 0.049)” were independently and significantly associated (Table 2).
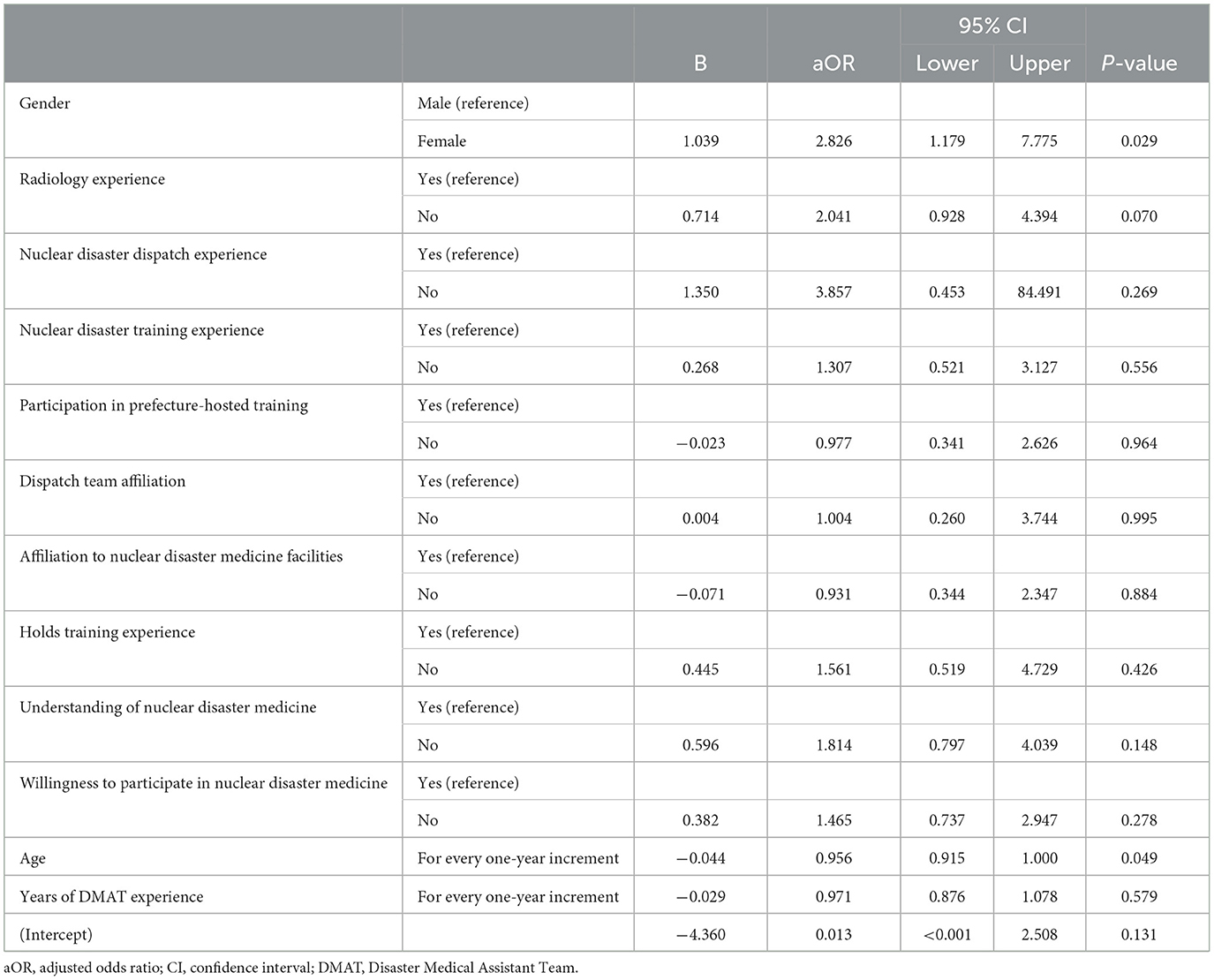
Table 2. Results of multiple binominal logistic regression analysis of factors associated with anxiety about handling contaminated patients during a nuclear disaster.
4 Discussion
This cross-sectional observational study sought to discern factors contributing to anxiety among Japanese DMAT personnel during nuclear disaster responses. A significant 77.2% of the 276 participants conveyed apprehension about managing contaminated patients in nuclear disaster scenarios.
Our multivariate binomial logistic regression analysis pinpointed gender and age as significant predictors of anxiety about managing contaminated patients during a nuclear disaster, irrespective of job title. Prior research has indicated that women often perceive risks more acutely and experience heightened anxiety and distress compared with men (13–15). This study's findings align with past research where Japanese female DMAT members were less inclined than their male counterparts to operate above public radiation dose limits in nuclear disaster contexts (16). Given that the majority of nurses are female, it is plausible that they harbor heightened concerns about interacting with radioactively contaminated patients. A past study on risk perception has shown that increased knowledge correlates with decreased risk perception (17). Therefore, to mitigate such anxieties, it is imperative to offer training on the facts about radiation health effects. Interestingly, although the general perception in Japan suggests that the elderly are more wary of radiation risks (18), our study found that younger Japanese DMAT members were more anxious in this regard. This could be attributed to their limited experience in handling radioactive contamination, leading to uncertainties about protective measures. The potential long-term ramifications of radioactive exposure, coupled with the existing knowledge gaps, can exacerbate these anxieties. Young women, in particular, might be apprehensive because of potential pregnancy concerns and the hereditary effects of radiation. After the Fukushima Daiichi Nuclear Power Station incident, the Fukushima Prefectural government initiated the Fukushima Health Management Survey, which revealed that over 60% of residents in 2011 were concerned about radiation's hereditary effects. However, this percentage has been declining annually (19), likely because of extensive information dissemination through various media (20–23). For Japanese DMAT members, accurate information about radiation health effects could significantly alleviate their anxieties. Hence, a tailor-made training program addressing nuclear disaster medicine scenarios would be indispensable for Japanese DMAT personnel.
4.1 Strengths and limitations
This study offers crucial insights but has its limitations. The cross-sectional design means that causal relationships cannot be inferred. The focus on Japanese DMAT personnel from Kyushu and Okinawa might not encapsulate the broader Japanese DMAT community's sentiments. The 54.5% response rate also raises concerns about potential response bias. Nonetheless, this research pioneers in identifying specific anxiety triggers for Japanese DMAT personnel in nuclear disaster contexts. By concentrating on a distinct population and setting, we have discovered the profound influence of gender and age on anxiety levels in Japanese DMAT personnel during nuclear disaster interventions. Such revelations are pivotal for crafting specialized training and support for Japanese DMAT personnel.
5 Conclusions
Our findings spotlight the pronounced anxiety among Japanese DMAT personnel, especially women and younger team members, when navigating nuclear disasters. These insights emphasize the urgency for targeted training and support tailored to the distinct challenges encountered by different Japanese DMAT demographic groups. As Japan remains vulnerable to both natural and human-made catastrophes, ensuring the mental wellbeing of frontline responders such as Japanese DMAT personnel is crucial for an effective nuclear disaster response.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of Nagasaki University Graduate School of Biomedical Sciences. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HS: Conceptualization, Investigation, Methodology, Writing – original draft. TY: Data curation, Formal analysis, Validation, Writing – original draft, Writing – review & editing. YY: Software, Validation, Writing – review & editing. TS: Supervision, Validation, Visualization, Writing – review & editing. HU: Project administration, Resources, Supervision, Writing – review & editing. YM: Funding acquisition, Project administration, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study obtained funding from the Research and Education Center for Natural Hazards, Kagoshima University.
Acknowledgments
We thank all study participants and Lorraine Law, BSc, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Japan International Cooperation Agency. 25 Years Since the Great Hanshin-Awaji Earthquake: The Birth of the DMAT and How Disaster Medical Assistance Know-How was Handed Down to it (Part I). Available online at: https://www.jica.go.jp/Resource/english/news/field/2019/20200117_01.html (accessed August 8, 2023).
2. World Health Organization. Available online at: https://extranet.who.int/kobe_centre/sites/default/files/WHO%20Guidance_Research%20Methods_Health%20EDRM_2021_Chapter-1.pdf (Accessed August 8, 2023).
3. Ministry of Health Labour and Welfare. Japan DMAT Action Guidelines. Available online at: https://www.mhlw.go.jp/stf/shingi/2r9852000001khc1-att/2r9852000001khl1.pdf (accessed August 8, 2023).
4. Cabinet Office, Goverment Goverment of Japan. Disaster Management in Japan. Available online at: https://www.bousai.go.jp/1info/pdf/saigaipanf_e.pdf (accessed August 8, 2023).
5. Iyama K, Kakamu T, Yamashita K, Shimada J, Tasaki O, Hasegawa A. Current situation survey for establishing personally acceptable radiation dose limits for nuclear disaster responders. J Radiat Res. (2022) 63:615–9. doi: 10.1093/jrr/rrac026
6. Koido Y, Kubo T, Toyokuni Y, Matsuzawa Y, Yano Y, Katsube T. Investigation of the receiving united states national disaster medical system (NDMS) disaster medical assistant team (DMAT) in Japan: development of standard operation procedures for receiving international medical teams. Prehosp Disaster Med. (2022) 37:s63–s63. doi: 10.1017/S1049023X22001625
7. United Nation Scientific Committee on the Effects of Atomic Radiation (UNSCEAR). UNSCEAR 2013 report - Vol. I. Available online at: https://www.unscear.org/unscear/en/publications/2013_1.html (accessed August 4, 2023).
8. Iwasa H, Nakayama C, Moriyama N, Orui M, Yasumura S. Posttraumatic growth after the fukushima nuclear disaster: examination of free descriptions among fukushima residents who lived in the evacuation area. Int J Environ Res Public Health. (2021) 19:192. doi: 10.3390/ijerph19010192
9. Moon S, Kim JH. Evaluating the effect of brief disaster education on emergency department staff: can short, low-cost education improve disaster readiness of non-DMAT healthcare personnel? Prehosp Disaster Med. (2023) 38:s140–1. doi: 10.1017/S1049023X23003692
10. Yamada Y, Orita M, Shinkawa T, Urata H, Kondo H, Takamura N. Nurses' interest in nuclear disaster medicine: future capacity building. J Radiat Res. (2019) 60:333–4. doi: 10.1093/jrr/rrz008
11. Shao J. Bootstrap model selection. J Am Stat Assoc. (1996) 91:655–65. doi: 10.1080/01621459.1996.10476934
12. Peduzzi P, Concato J, Feinstein AR, Holford TR. Importance of events per independent variable in proportional hazards regression analysis II. ACCURACY and precision of regression estimates. J Clin Epidemiol. (1995) 48:1503–10. doi: 10.1016/0895-4356(95)00048-8
13. Susanto N, Susatyo Nugroho WP, Rizkiyah E. Evaluating risk perception based on gender differences for mountaineering activity. E3S Web of Conf. (2018) 31:09028. doi: 10.1051/e3sconf/20183109028
14. Alsharawy A, Spoon R, Smith A, Ball S. Gender differences in fear and risk perception during the COVID-19 pandemic. Front Psychol. (2021) 12:689467. doi: 10.3389/fpsyg.2021.689467
15. Brown GD, Largey A, McMullan C. The impact of gender on risk perception: Implications for EU member states' national risk assessment processes. Int J Disaster Risk Reduct. (2021) 63:102452. doi: 10.1016/J.IJDRR.2021.102452
16. Ochi G, Hasegawa A, Hirohashi N, Yamamoto N, Morizane T, Hiratsuka Y, Ohkura T. Estimating the proportion of DMAT members able to act during a radiation disaster through a questionnaire survey in Chugoku-Shikoku District and Fukushima Prefecture. J J Disast Med. (2022) 27:65–74. doi: 10.51028/jjdisatmed.27.1_65
17. Sjöberg L, Drottz-Sjöberg B-M. Knowledge and risk perception among nuclear power plant employees. Risk Anal. (1991) 11:607–18. doi: 10.1111/J.1539-6924.1991.TB00650.X
18. Yamaguchi T, Horiguchi I, Kunugita N. Factors associated with refraining from purchasing foods produced in affected areas after the fukushima Daiichi nuclear power station accident. Int J Environ Res Public Health. (2022) 19:3378. doi: 10.3390/ijerph19063378
19. Ministry of the Environment, Japan. Health Effects of Radiation: 5 Themes - (v) Changes in Perception of Radiation Risks. Available online at: https://www.env.go.jp/en/chemi/rhm/portal/digest/nextgeneration/detail_005.html
20. Tsubokura M, Onoue Y, Torii HA, Suda S, Mori K, Nishikawa Y, et al. Twitter use in scientific communication revealed by visualization of information spreading by influencers within half a year after the Fukushima Daiichi nuclear power plant accident. PLoS ONE. (2018) 13:e0203594. doi: 10.1371/journal.pone.0203594
21. Thomson R, Ito N, Suda H, Lin F, Liu Y, Hayasaka R, Isochi R, Wang Z. Trusting tweets: the fukushima disaster and information source credibility on twitter. In: Proceedings of the 9th International ISCRAM Conference. (2012). Available online at: https://www.emknowledge.org.au/ISCRAM2012/proceedings/112.pdf (accessed August 10, 2023).
22. Nakayama C, Sato O, Sugita M, Nakayama T, Kuroda Y, Orui M, et al. Lingering health-related anxiety about radiation among Fukushima residents as correlated with media information following the accident at Fukushima Daiichi Nuclear Power Plant. PLoS ONE. (2019) 14:e0217285. doi: 10.1371/journal.pone.0217285
Keywords: DMAT, disaster medical assistance team, nuclear disaster, radioactive contaminated patients, anxiety
Citation: Shibata H, Yamaguchi T, Yamada Y, Shinkawa T, Urata H and Matsunari Y (2024) Factors associated with anxiety about handling contaminated patients during a nuclear disaster among disaster medical assistant teams in Japan: a cross-sectional study. Front. Disaster Emerg. Med. 2:1361236. doi: 10.3389/femer.2024.1361236
Received: 25 December 2023; Accepted: 29 March 2024;
Published: 17 April 2024.
Edited by:
Ives Hubloue, Vrije University Brussels, BelgiumCopyright © 2024 Shibata, Yamaguchi, Yamada, Shinkawa, Urata and Matsunari. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Takumi Yamaguchi, takumi@saitama-med.ac.jp