Awareness and access to mass media sources of information about modern family planning methods among women with disabilities in Nigeria: An analysis of 2018 demographic and health survey
 Hussaini Zandam
Hussaini Zandam Monika Mitra1
Monika Mitra1 - 1The Lurie Institute for Disability Policy, The Heller School for Social Policy and Management, Brandeis University, Waltham, MA, United States
- 2Economics Department and Research Consortium on Disability, Fordham University, Bronx, NY, United States
Background: Family planning is the foundation of sexual and reproductive health, and necessary for achieving the Sustainable Development Goals. Yet, the needs of women with disabilities and their access to these services have been neglected for decades, especially in Low and Middle-income Countries. To improve utilization of these services among women with disabilities, they have to be aware and informed about the services. This study was conducted to examine awareness and mass media sources of information on family planning between women with and without disabilities.
Methods: This study used data from the 2018 Nigeria Demographic and Health Surveys (NDHS). Our analytic sample included 26,585 women between 15 and 49 years of age who answered the disability module. We compared demographics and socioeconomic characteristics of women with and without disabilities using the chi-square test for categorical variables. In addition, we conducted logistic regressions to estimate the unadjusted and adjusted odds ratio (with 95% confidence intervals) for level of awareness and mass media sources of information on modern contraceptive methods, using women without a disability as the reference group.
Results: Finding showed that women with disabilities have poor awareness about family planning compared to women without disabilities even after adjusting for all covariates (AOR = 0.42, 95% CI: 0.23–0.76, P < 0.05). We also found that women with disabilities are less likely to receive information about family planning from any of the available mass media channels even after adjusting for covariates (AOR = 0.46, 95% CI: 0.22–0.98, P < 0.05).
Conclusions: The study revealed that women with disabilities Nigeria have poor awareness about modern family planning methods compared to non-disabled women. They are also less likely to receive information about modern family planning methods compared to non-disabled women. To effectively reach women with disabilities, information barriers must be eliminated, coupled with increased opportunities to access family planning information. Donors, government, and other relevant stakeholders should consider funding inclusive campaigns and explore other mechanisms for disseminating family planning information to women with disabilities.
Background
Family planning is the foundation of sexual and reproductive health and necessary for achieving the Sustainable Development Goals (1). Sexual and reproductive health allows individuals to achieve desired birth spacing, family size and improve health outcomes for infants, children, women, and families. Specifically, access to contraceptives prevents unsafe sex, abortions, HIV (human immunodeficiency virus), and other sexually transmitted infections, which constitute significant risk health challenges among women (2, 3). Yet, women with disabilities and their access to these services have been neglected for decades because of many reasons including the widespread assumption that people with disabilities are not sexual or sexually active (4–6). There has been a growing recognition of the rights of people with disabilities since the World Report on Disability was published (7) and the United Nations Convention on the Rights of People with Disabilities, which has ratified by several countries (8). The World Report on Disability, for the first time, brought global recognition to the rights of people with disabilities, who are often described as the world's largest minority group. The report officially recognizes, among others, the need for sexual and reproductive health policies and programs to be inclusive of women with disabilities (7).
Nigeria is an important country especially in light of the global contraceptive goal referred to as 120 by 20, which aims to increase access to modern contraceptives for 120 million more women by 2020 (9). With national modern contraceptive prevalence rates staggering at 12.5%, Nigeria has struggled to achieve its country goal of increasing contraceptive uptake by more than 1.5% per year in order to reach Sustainable Development Goal target (10–12). Low uptake of contraceptives in the country has been associated with myriad of factors including cultural and religious factors (13, 14) and lack of adequate knowledge and poor attitudes (15–17). Several initiatives have been implemented to improve contraceptive uptake including awareness campaigns through mass media channels. Studies have shown that improving awareness through mass media can influence people into adopting family planning methods (18–20). For instance, the impact evaluation of the Nigerian Urban Reproductive Health Initiative showed that between 2015 and 2020, awareness campaign through radio, television, and community events significantly increased the use of modern contraceptives from 21.1% to 30.1% in the states the program was implemented (21). Despite the potential of the education and awareness interventions, program deficiencies have also been observed especially in targeting harder-to-reach groups of women (12). A review of program and policy documents on contraception found that women with disabilities were not included in the family planning program design and planning in Nigeria (22–24).
Monitoring disability-inclusive policy and programming require a nationally representative and internationally comparable data to measure and close any existing gaps. The available literature on family planning in sub-Saharan Africa does not account for the disability-related disparities in knowledge and access to modern contraceptives. To address this gap, we analyzed nationally representative data from the Nigeria Demographic and Health Surveys (NDHS) to compare contraceptive knowledge and information sources between women with and without disabilities. We hypothesized that women with disabilities are more likely to report poor knowledge of modern contraceptives and limited access to information on modern contraceptives than non-disabled women. A study on the knowledge and access to information about family planning using an internationally comparable definition of disability and a nationally representative sample will not only contribute to close the gap in research on modern contraceptives among women with disabilities, it may also form the basis for developing inclusive interventions to improve contraceptive knowledge and demand among women with disabilities.
Methods
We conducted a secondary analysis of the publicly available 2018 Nigeria Demographic and Health Surveys (NDHS) (25). The NDHS is supported by the United States Agency for International Aid (USAID) and provides up-to-date estimates of key demographic, socioeconomic and health indicators in Nigeria including sexual and reproductive health in adults, infant and maternal mortality, child mortality, nutritional status, malaria, and disability status. The NDHS employed a stratified two-stage sample survey design. In the first stage, primary sampling units (PSUs) or enumeration areas (EAs) in urban and rural areas were selected. In the second stage, a random sample of residential dwelling units (DUs) from each PSU was selected for the survey.
The Disability Module is part of the Household Questionnaire offered to all identified household members. Detailed information about survey design, sampling methods, and response rates is available in the NDHS final survey reports (25). The NDHS data are nationally representative of women 15–49 years of age. A total of 41,821 women were interviewed in 2018. Of these, only 26,585 were offered the disability module and formed our analytic sample.
Measurements
Our dependent variables were as follows: (i) awareness of modern family planning methods; and (ii) access to information about modern family planning methods from mass media sources. The first dependent variable was generated from a questions asking knowledge of contraceptive methods including, lack of knowledge of any method, knowledge of traditional method, folkloric method, and modern methods. Responses were categorized as yes/no question where yes indicates familiarity with any modern contraceptive method (e.g., contraceptive pill, male condom, intrauterine contraceptive device etc.). The second dependent variable was generated from four yes/no questions asking whether the respondent heard or read information about modern family planning methods in the last few 12 months (1) on radio; (2) on TV; (3) in newspaper or magazine, leaflets or brochure; and (4) from mobile public announcement.
Disability
The primary explanatory variable was disability and was assessed from responses to the Washington Group Short Set of Questions on Disability (WGSS) (26). It is the standard approach to measuring disability in censuses and large surveys producing valid data that is internationally comparable (27). Disability status assessment was based on experience of difficulties by an individual related to: (1) seeing; (2) hearing; (3) walking; (4) remembering; (5); communicating and (6) washing or taking care of self. Possible responses to the questions were as follows: no difficultly; some difficulty; a lot of difficulty; and cannot do at all. We employed the recommendation from the Washington Group on Disability Statistics' analytical guidelines in creating a dichotomous disability categorization (26). Women who reported “a lot of difficulty” or “cannot function at all” to any of the six functional domains were classified as having a disability; women who reported “none” or “some difficulty” were classified as not having a disability (26). Despite the validity of the WGSS, it also has limitations, especially not capturing some types of disabilities such as mental health-related disabilities (28).
Covariates
Covariates for this study included age (<25 years, 25–34, or 35+ years), education (no education or having at least primary level education), union status (married or single), religion affiliation (Christian or Muslim/traditionalists), employment status (working or not working) and parity (0, 1–2, 3–4, and 5+). Household characteristics included household wealth (poorest or others) and place of residence (urban or rural).
Statistical methods
We compared demographics and socioeconomic characteristics of women with and without disabilities using the chi-square test for categorical variables. Both dependent variables were analyzed as binary (yes/no) variables. We calculated the proportions for each outcome indicator and compare between women with and without disabilities. Then we conducted logistic regressions to estimate the unadjusted and adjusted ratios (with 95% confidence intervals) for awareness and access of information, using women without a disability as the reference group. We used Stata version 16 for all analyses, applying svy commands to account for the complex sampling design of the NDHS, and we used a P-value <.05 as the highest level of acceptable significance.
Results
Women's characteristics
Table 1 describes the sample and provides bivariate contrasts in sociodemographic and household characteristics between Nigerian women with and without disabilities. In comparison to women without disabilities, women with disabilities are more likely to be older and, have no education, and be from poorer households. Similarly, women with disabilities are less likely to be married and to live in urban areas. However, there was no statistically significant difference in employment status between the two groups of women.
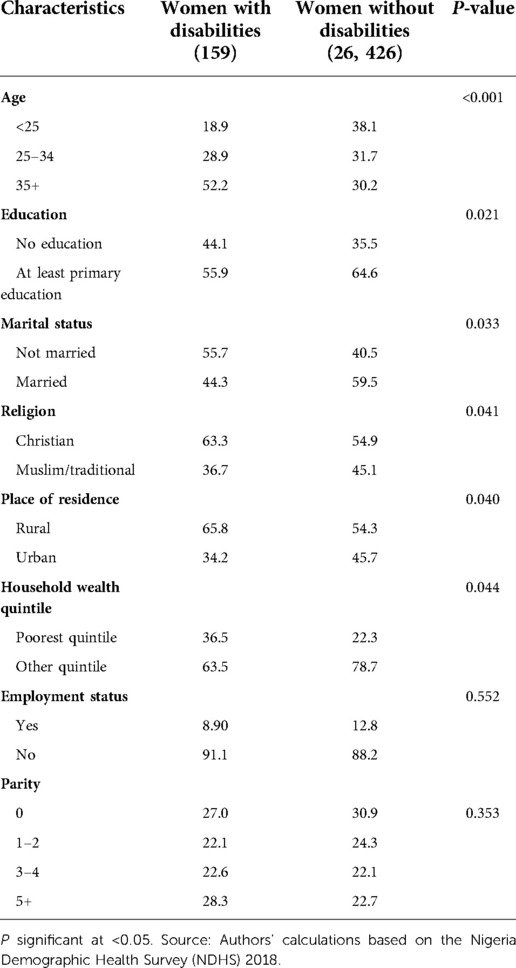
Table 1. Demographic characteristics by disability status.
Awareness and mass media sources of information about modern family planning methods by disability status
Results from comparison of level of awareness and acces to information on modern methods are presented in Table 2. A significantly higher proportion of women without disabilities (91.3%) reported to have awareness of modern methods compared to women with disabilities (77.8%). Similarly, fewer women with disabilities (19.5%) reported receiving information on modern methods from mass media channels (radio, TV, print media and mobile text message) compared to non-disabled women (32.8%).
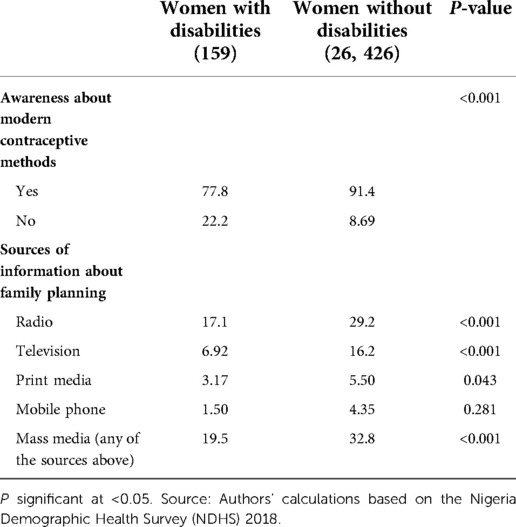
Table 2. Awareness of modern family planning methods and mass media sources of information about modern family planning methods by disability status.
Association between awareness and mass media sources of information about modern family planning methods by disability status
Table 3 present results of unadjusted and adjusted odds ratios from bivariate and multivariate analyses for awareness and access to information on modern methods by disability status. Women with disabilities significantly reported poor awareness of modern methods compared to non-disabled women in the unadjusted analyses (OR = 0.39, 95% CI: 0.26–0.57, P < 0.05). The difference in level of awareness remained significant even after accounting for other factors (AOR = 0.40, 95% CI: 0.22–0.72, P < 0.05).
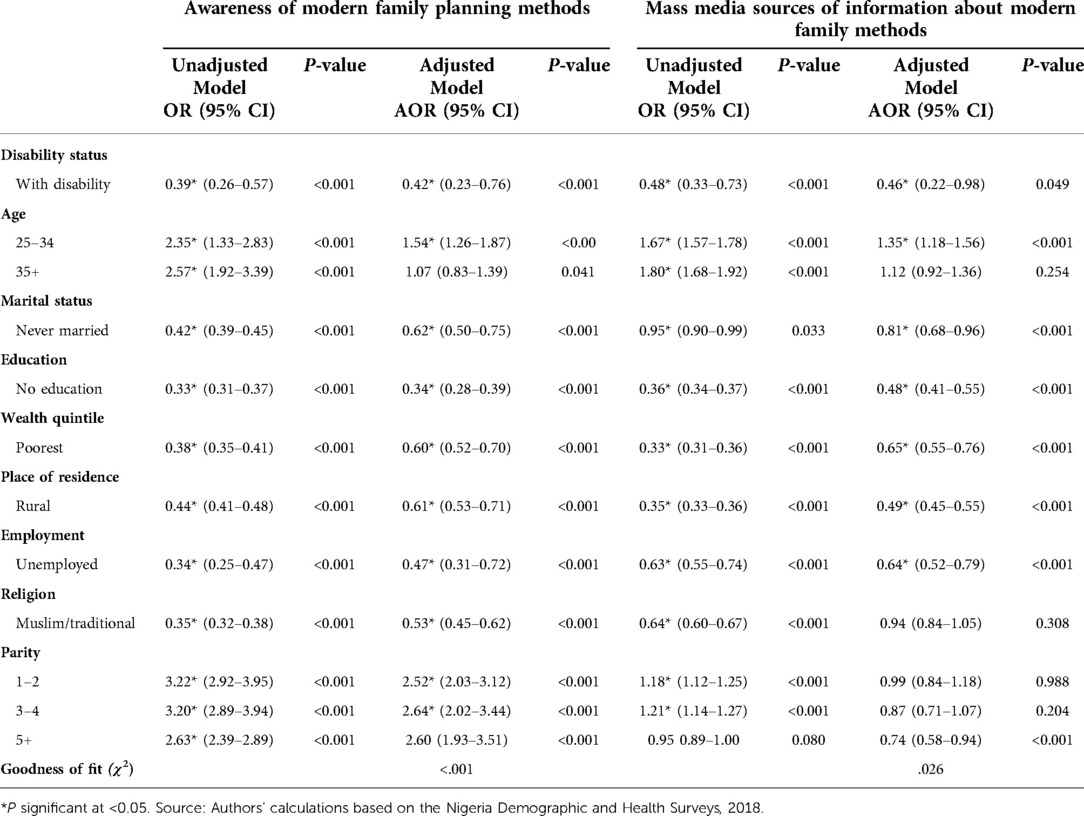
Table 3. Association between disability status and awareness of modern family planning method and receiving information about modern family planning methods.
Similarly, women with disabilities were less likely to receive information about modern family planning methods via any mass media channels compared to women without disabilities (OR = 0.48, 95% CI: 0.33–0.73, P < 0.05). The difference remained even after adjusting for all covariates (AOR = 0.46, 95% CI: 0.22–0.98, P < 0.05). Other sociodemographic variables including age, marital status, education, wealth, location of residence, parity and religion were independently associated with awareness and mass media access to information.
Discussion
In this secondary analysis of 2018 NDHS data, we found substantial disparities in awareness and access to information on modern family planning methods between disabled and non-disabled women in Nigeria. Approximately one-fourth of Nigerian women with disabilities had no awareness of any modern family planning method compared to only about one-fifth of women without disabilities. Similarly, only about one-fourth of women with disabilities were reported to have received information from mass media sources about modern family planning methods compared to about one-third of non-disabled women.
Though most women in our study had awareness of modern methods, we found relatively low awareness among women with disabilities and among women who were unmarried, younger, uneducated, Muslim/traditionalists, unemployed, and those from rural and poor households. These sociodemographic differences suggest deficiencies in Nigerian information sharing programs reaching women from low socioeconomic backgrounds (12, 29, 30). Our study also finds that more than half of women in our sample, irrespective of disability status, were not exposed to information about family planning from any mass media channel. This is supported by a previous study using the 2013 NDHS data, which found that 63 percent of women were not exposed to family planning information from the media (31). Our study strengthened the limited reach of family planning messaging in the country.
Women with disabilities in our sample were more likely to be older and unmarried which may also influence their perception and demand for family planning information. Women with disabilities often experience multiple concurrent intersections related to gender and disability. These intersections are often complex and multilayered resulting in women with disabilities experiencing a wide range of attitudinal, communication, and physical barriers when accessing and using sexual and reproductive services (32, 33). The widespread perception that people with disabilities are asexual creates barriers for them to access sexual and reproductive health services (34). This means that they don't know as much about sexual and reproductive services including information as their non-disabled peers. Parents, educators, and health professionals are often uncomfortable or unprepared to discuss sexuality and reproduction issues with disabled people, which could be attributed to normative definitions of sexuality, as well as widespread societal devaluation of disability and cultural portrayals of disabled people as asexual beings (32, 33).
This study has shown some of the challenges of family planning among women with Disabilities in Nigeria, which undermines its effort to achieve its family planning Sustainable Development Goal (1). Disabled women's access to contraceptive information and services is underpinned by internationally recognized human rights, including the right to attain the highest level of health and their right to information that will enable them to make responsible and informed choices about their sexual and reproductive health (35). Nigeria having ratified the United Nations Convention on the Rights of People with Disabilities has a legal obligation to rectify this disparity (36). Women and girls with disabilities are the most vulnerable of the largest minority group of people with disabilities (7). They face a greater risk of neglect, exploitation, and violence both within and outside the home (37). Ensuring equitable access to family planning and its proper utilization can help them reap its socioeconomic and health benefits such as empowerment to determine reproduction and autonomy within their households and enhance their earning power (2, 3). The findings of this study highlight the need for an aggressive, accessible, inclusive family planning campaign such as incorporating screen readers, audio transcriptions for video, and sign language interpretation to increase disabled women's knowledge of modern contraceptives and echo decades' old neglect that people with disabilities have been experiencing regarding their sexual and reproductive health (4–6).
This study has several limitations. The NDHS has no information about the onset, cause, severity, and length of disability. Lack of these information may have limited the scope of the data to capture an individual's experience and access to family planning information. The limited sample size of participants who responded to the disability questions clearly under-represented women with disabilities, which may also influence our finding. The limited sample also made it difficult to disaggregate findings by type of disability, which could provide valuable information on the unique challenges faced by women with different type of disabilities. Another limitation is that of accuracy of disability estimates because disability questions are responded by the head of household or a household representative instead of the individuals. The 2018 NDHS data is the first wave to include disability; limiting our ability to infer causality in our findings. Finally, the DHS is a self-reported survey; hence the data is subjected to potential recall bias, and some questions may be affected by social and cultural sensitivity issues. Despite these limitations, the DHS has been used extensively, and findings have been highly relevant to researchers, policymakers, and non-governmental organizations working across various sectors for the sexual and reproductive health of women with disabilities.
Conclusion
The study revealed that Nigerian women with disabilities have poor awareness and access to information on modern contraceptives. In order to effectively reach women with disabilities, informational barriers must be eliminated coupled with increased opportunities to access family planning information. Donors, government, and other relevant stakeholders should consider funding inclusive campaigns and explore other mechanisms for disseminating family planning information to women with disabilities.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://www.dhsprogram.com/data/available-datasets.cfm.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
All authors provided input into drafts and approved the final draft of the manuscript. In addition, HZ contributed to the design of the study, data acquisition/analyses and data interpretation; MM contributed to the design of the study, data analyses and interpretation; SM contributed to the design of the study, data analyses and interpretation. All authors contributed to the article and approved the submitted version
Funding
This research is funded from a grant from the United States' National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) grant number: 90AR5024.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Starrs AM, Ezeh AC, Barker G, Basu A, Bertrand JT, Blum R, et al. Accelerate progress—sexual and reproductive health and rights for all: report of the guttmacher–lancet commission. Lancet. (2018) 391(10140):2642–92. doi: 10.1016/S0140-6736(18)30293-9. Available at: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(18)30293-9/fulltext (cited May 25, 2020).29753597
2. Glasier A, Gülmezoglu AM, Schmid GP, Moreno CG, Van Look PF. Sexual and reproductive health: a matter of life and death. Lancet. (2006) 368:1595–607. doi: 10.1016/S0140-6736(06)69478-6
3. Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJL. Selected major risk factors and global and regional burden of disease. Lancet. (2002) 360(9343):1347–60. doi: 10.1016/S0140-6736(02)11403-6
4. Milligan MS, Neufeldt AH. The myth of asexuality: a survey of social and empirical evidence. Sex Disabil. (2001) 19:91–109. doi: 10.1023/A:1010621705591
5. Vilchinsky N, Werner S, Findler L. Gender and attitudes toward people using wheelchairs: a multidimensional perspective. Rehabil Couns Bull. (2010) 53(3):163–74. doi: 10.1177/0034355209361207. Available at: https://wwws.sagepub.com/doi/10.1177/0034355209361207 (cited May 25, 2020).
6. Seidel A, Wienholz S, Michel M, Luppa M, Riedel-Heller SG. Sexual knowledge among adolescents with physical handicaps: a systematic review. Sex Disabil. (2014) 32:429–41. doi: 10.1007/s11195-013-9326-4
7. World Health Organization. WORLD REPORT ON DISABILITY WHO Library Cataloguing-in-Publication Data. (2011). Available at: www.who.int/about/licensing/copyright_form/en/index.html (cited May 25, 2020).
8. Convention on the Rights of Persons with Disabilities and Optional Protocol UNITED NATIONS. (2008). Available at: https://www.un.org/disabilities/documents/convention/convoptprot-e.pdf (cited May 25, 2020).
9. Brown W, Druce N, Bunting J, Radloff S, Koroma D, Gupta S, et al. Developing the “120 by 20” goal for the global FP2020 initiative. Stud Fam Plann. (2014) 45(1):73–84. doi: 10.1111/j.1728-4465.2014.00377.x. Available at: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1728-4465.2014.00377.x (cited May 26, 2020).24615576
10. Hounton S, Barros AJD, Amouzou A, Shiferaw S, Maïga A, Akinyemi A, et al. Patterns and trends of contraceptive use among sexually active adolescents in Burkina Faso, Ethiopia, and Nigeria: evidence from cross-sectional studies. Glob Health Action. (2015) 8(1). doi: 10.3402/gha.v8.29737
11. Fagbamigbe AF, Afolabi RF, Idemudia ES. Demand and unmet needs of contraception among sexually active in-union women in Nigeria: distribution, associated characteristics, barriers, and program implications. Sage Open. (2018) 8(1):215824401775402. Available at: https://wwws.sagepub.com/doi/10.1177/2158244017754023 (cited May 25, 2020). doi: 10.1177/2158244017754023
12. Mercer LD, Lu F, Proctor JL. Sub-national levels and trends in contraceptive prevalence, unmet need, and demand for family planning in Nigeria with survey uncertainty. BMC Public Health. (2019) 19(1):1–9. doi: 10.1186/s12889-019-8043-z
13. Akamike IC, Madubueze UC, Okedo-Alex IN, Anyigor CJ, Azuogu BN, Umeokonkwo CD, et al. Perception, pattern of use, partner support and determinants of uptake of family planning methods among women in rural communities in Southeast Nigeria. Contracept Reprod Med. (2020) 5(1):14. doi: 10.1186/s40834-020-00120-x. Available at: https://contraceptionmedicine.biomedcentral.com/articles/10.1186/s40834-020-00120-x (cited February 21, 2021).32884833
14. Austin A. Unmet contraceptive need among married Nigerian women: an examination of trends and drivers. Contraception. (2015) 91(1):31–8. doi: 10.1016/j.contraception.2014.10.002. Available at: https://linkinghub.elsevier.com/retrieve/pii/S0010782414006969 (cited May 25, 2020).25453583
15. Bolarinwa OA, Olagunju OS. Knowledge and factors influencing long-acting reversible contraceptives use among women of reproductive age in Nigeria. Gates Open Res. (2020) 3, Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7447856/ (cited February 21, 2021). doi: 10.12688/gatesopenres.12902.3
16. Ajayi AI, Adeniyi OV, Akpan W. Use of traditional and modern contraceptives among childbearing women: findings from a mixed methods study in two southwestern Nigerian states. BMC Public Health. (2018) 18(1):604. doi: 10.1186/s12889-018-5522-6. Available at: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-018-5522-6 (cited February 21, 2021).29739372
17. Solanke BL. Factors influencing contraceptive use and non-use among women of advanced reproductive age in Nigeria. J Heal Popul Nutr. (2017) 36(1):1. doi: 10.1186/s41043-016-0077-6. Available at: http://jhpn.biomedcentral.com/articles/10.1186/s41043-016-0077-6 (cited February 21, 2021).
18. Speizer IS, Guilkey DK, Escamilla V, Lance PM, Calhoun LM, Ojogun OT, et al. On the sustainability of a family planning program in Nigeria when funding ends. Anglewicz P, editor. PLoS One. (2019) 14(9):e0222790. doi: 10.1371/journal.pone.0222790. Available at: https://dx.plos.org/10.1371/journal.pone.0222790 (cited July 29, 2020).31557217
19. Rutaremwa G, Kabagenyi A, Wandera SO, Jhamba T, Akiror E, Nviiri HL. Predictors of modern contraceptive use during the postpartum period among women in Uganda: a population-based cross sectional study health behavior, health promotion and society. BMC Public Health. (2015) 15(1). doi: 10.1186/s12889-015-1611-y. Available at: https://pubmed.ncbi.nlm.nih.gov/25885372/ (cited July 29, 2020).25885372
20. Jato MN, Simbakalia C, Tarasevich JM, Awasum DN, Kihinga CNB, Ngirwamungu E. The impact of multimedia family planning promotion on the contraceptive behavior of women in Tanzania. Int Fam Plan Perspect. (1999) 25(2):60–7. doi: 10.2307/2991943. Available at: https://www.jstor.org/stable/2991943 (cited July 29, 2020).
21. Atagame KL, Benson A, Calhoun L, Corroon M, Guilkey D, Iyiwose P, et al. Evaluation of the Nigerian urban reproductive health initiative (NURHI) program. Stud Fam Plann. (2017) 48(3):253–68. doi: 10.1111/sifp.12027. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5896011/?report=abstract (cited July 29, 2020).28620974
22. Nigeria Family Planning Blueprint (Scale-Up Plan) Federal Government of Nigeria Federal Ministry of Health. (2014).
23. Nigeria. Family Planning (2020). Available at: http://www.familyplanning2020.org/nigeria (cited May 25, 2020).
24. Policy in Brief National Reproductive Health Policy (2010). Available at: www.championingchange.org (cited May 25, 2020).
25. NPC. The Federal Republic of Nigeria Nigeria Demographic and Health Survey 2018. (2019). Available at: www.DHSprogram.com (cited May 26, 2020).
26. Group W, Documents I, Implementation A, Tools WG. Analytic guidelines: Creating disability identifiers using the Washington Group Short Set (WG-SS) SPSS Syntax. (2017). p. 1–11. Available at: http://www.washingtongroup-disability.com/ (cited May 26, 2020).
27. Loeb M. International census/survey data and the short set of disability questions developed by the Washington group on disability statistics. In: Altman BM, editor. International measurement of disability. Cham: Springer (2016). p. 255–304. Available at: https://link.springer.com/chapter/10.1007/978-3-319-28498-9_15 (cited September 4, 2020).
28. Groce NE, Mont D. Counting disability: emerging consensus on the Washington Group questionnaire. (2017). Available at: https://www.un.org/development/desa/disabilities/convention-on-the- (cited September 4, 2020).
29. Saleh F, Raji MO, Oche M, Tunau K, Kaoje AU. Socio-demographic factors associated with knowledge and uptake of family planning among women of reproductive age in a rural community of Abuja, Nigeria. J Sains Kesihat Malaysia. (2018) 16(01):71–9. doi: 10.17576/jskm-2018-1601-09
30. Adefalu AA, Ladipo OA, Akinyemi OO, Popoola OA, Latunji OO, Iyanda OF. Awareness and opinions regarding contraception by women of reproductive age in North-West Nigeria. Pan Afr Med J. (2018) 30. doi: 10.11604/pamj.2018.30.65.12975. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6192713/?report=abstract (cited September 4, 2020).30344849
31. Ladi C, Dahiru ET, Aliyu AA. Contextual factors influencing modern contraceptive use in Nigeria. United States Agency for International Development (2015) Rockville, Maryland, USA.
32. Mac-Seing M, Zinszer K, Eryong B, Ajok E, Ferlatte O, Zarowsky C. The intersectional jeopardy of disability, gender and sexual and reproductive health: experiences and recommendations of women and men with disabilities in Northern Uganda. Sex Reprod Heal Matters. (2020) 28(2):1772654. doi: 10.1080/26410397.2020.1772654. Available at: https://www.tandfonline.com/doi/full/10.1080/26410397.2020.1772654 (cited September 4, 2020).
33. Carew MT, Braathen SH, Swartz L, Hunt X, Rohleder P. The sexual lives of people with disabilities within low- and middle-income countries: a scoping study of studies published in English. Glob Health Action. (2017) 10(1):1337342. doi: 10.1080/16549716.2017.1337342. Available at: http://www.ncbi.nlm.nih.gov/pubmed/28678682 (cited September 17, 2017).28678682
34. Schenk KD, Tun W, Sheehy M, Okal J, Kuffour E, Moono G, et al. “Even the fowl has feelings”: access to HIV information and services among persons with disabilities in Ghana, Uganda, and Zambia. Disabil Rehabil. (2020) 42(3):335–48. doi: 10.1080/09638288.2018.1498138. Available at: https://pubmed.ncbi.nlm.nih.gov/30282493/ (cited February 11, 2021).30282493
35. Jaramillo Ruiz F. The committee on the rights of persons with disabilities and its take on sexuality. Reprod Health Matters. (2017) 25(50):92–103. doi: 10.1080/09688080.2017.1332449. Available at: https://www.tandfonline.com/doi/full/10.1080/09688080.2017.1332449 (cited July 30, 2020).28784074
36. Arimoro AE. Are they not Nigerians? The obligation of the state to end discriminatory practices against persons with disabilities. Int J Discrim Law. (2019) 19(2):89–109. doi: 10.1177/1358229119846764. Available at: https://wwws.sagepub.com/doi/10.1177/1358229119846764 (cited September 4, 2020).
37. United Nations Enable. Women and girls with disabilities. Available at: https://www.un.org/development/desa/disabilities/issues/women-and-girls-with-disabilities.html (cited September 4, 2020).
Keywords: modern contraceptives, disability, knowledge, information, disparity
Citation: Zandam H, Mitra M and Mitra S (2022) Awareness and access to mass media sources of information about modern family planning methods among women with disabilities in Nigeria: An analysis of 2018 demographic and health survey. Front. Glob. Womens Health 3:746569. doi: 10.3389/fgwh.2022.746569
Received: 24 July 2021; Accepted: 31 October 2022;
Published: 2 December 2022.
Edited by:
Sunday A. Adedini, Federal University Oye-Ekiti, NigeriaReviewed by:
Alida Gertz, WellStar Health System, United StatesAna Luiza Vilela Borges, University of São Paulo, Brazil
© 2022 Zandam, Mitra and Mitra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hussaini Zandam huzandam@brandeis.edu
Specialty Section: This article was submitted to Contraception and Family Planning, a section of the journal Frontiers in Global Women's Health