Utilization of social franchising in family planning services: a Pakistan perspective
 Nayab1
Nayab1  Taimoor Ahmad1
Taimoor Ahmad1  Areesh Fatmee1 Ibtisam Sajjad1 Zona Usmani1
Areesh Fatmee1 Ibtisam Sajjad1 Zona Usmani1  Ayesha Khan2 Sara Shahzad3
Ayesha Khan2 Sara Shahzad3  Adnan Ahmad Khan1,4*
Adnan Ahmad Khan1,4*
- 1Program, Research and Development Solutions (RADS), Islamabad, Pakistan
- 2Urban Impact Lab, Akhter Hameed Khan Foundation, Islamabad, Pakistan
- 3University of Cambridge, Cambridge, United Kingdom
- 4Ministry of National Health Services, Regulations and Coordination (MoNHSRC), Islamabad, Pakistan
Introduction: Pakistan's private sector caters to around 65% of family planning users. Private sector family planning was promoted in the Delivering Accelerated Family Planning in Pakistan (DAFPAK) program by UK's Foreign, Commonwealth & Development Office (FCDO) in 2019. We use data from DAFPAK to analyze the clientele and products distributed by two major NGOs, Marie Stopes Society (MSS) and DKT Pakistan, that support private providers in Pakistan. We also examined the effect of COVID-19 on client visits and contraceptives uptake at private facilities in Pakistan.
Methods: DAFPAK used field validation surveys to analyze the volume of clients and products of 639 private facilities across three provinces (Punjab, KPK and Balochistan) of Pakistan. The data was collected in two phases (February 2020 and 2021) using multi-stage cluster sampling at 95% confidence level. Using a generalized negative binomial regression, facility-level characteristics and impact of COVID-19 was analyzed with the volume of clients and products given out at 95% confidence interval alongside descriptive analysis.
Results: DKT facilities covered 53% of the sample while MSS covered 47%, with 72% facilities in the rural areas. Average facility existence duration is 87 months (7.25 years). While the average experience of the facility staff is 52 months (4.33 years). MSS is serving more clients as compared to DKT during both phase 1 (IRR: 3.15; 95% CI: 2.74, 3.61) and phase 2 (IRR: 2.11; 95% CI: 1.79, 2.49). Similarly, MSS had a greater volume of products given out in both phases 1 (IRR: 1.89; 95% CI: 1.51, 2.38) and phase 2 (IRR: 2.57; 95% CI: 2.09, 3.14). In both phases, client visits and product distribution decreased when client privacy is invaded (IRR: 0.74; 95% CI: 0.67, 0.82 – phase 1) and (IRR: 0.83; 95% CI: 0.72, 0.97 – phase 2). Lastly, during COVID-19, products distribution decreased by a factor of 0.84 (IRR: 0.84; 95% CI: 0.72, 0.97) but client visits remain unaffected.
Conclusion: Overall, clientele is low for all facilities. At a facility, privacy is a determinant of client visits and products given out per visit. Transiently, during COVID-19, client volumes decreased, with a shift from oral pills to condoms and emergency contraceptive pills.
Introduction
Pakistan is the world's fifth most populous country of 241 million people. It had committed at the London Family Planning summit 2012 to raise its Contraceptive Prevalence Rate (CPR) to 55% by 2020 (1). This was later modified to 50% by 2025% and 60% by 2030 and the commitment was institutionalized nationally as “Recommendations of the Council of Common Interests” (CCI) and Pakistan's FP2030 pledge (2, 3). Despite political commitment, allocated budgets, and large-scale family planning (FP) programs, the national contraceptive prevalence rate (CPR) has remained in the 30%–35% range since 2007 (3–6), and Pakistan's population growth rate increased from 2.4% (Census 2017) to 2.55% (Census 2023) (7, 8).
Approximately 36%–65% of family planning services in low and middle-income countries (LMIC) are offered by private sector providers through social franchising initiatives (9). In Pakistan, the private sector plays a dominant role, albeit, mainly through social marketing outlets such as pharmacies, markets, shops, etc., that serve 54% of users that avail FP each year, and is expanding relatively slowly (3–6). On the other hand, socially franchised private clinics serve another 11% (3, 10, 11). Government services, including lady health workers and clinics, serve around 35% of users in a year. Among these, the outreach of LHW may have maximized and is not expanding (12, 13). Both private or public health facilities remain underutilized and therefore potentially have the most room for expansion (14).
Nearly all private FP facilities are supported by NGOs through the social franchising approach where private healthcare providers are included into networks where they are shared in a brand that gives them credibility in the communities they operate. In return, this branding allows the supporting NGO to assure quality of services and products that engenders trust among clients. The approach allows flexibility in services and method choices, and adaptability to the local context and needs in order to promote sustainability, albeit often with grant supported subsidies for providers (15, 16). The concept is well established, with demonstrated success. For example, programs from Pakistan showed an 11% increase in IUDs use (17), while 22% rise in Long Acting Reversible Contraception (LARC) utilization was observed in Kenya through social franchising programs (18).
Given the potential importance of private clinics in scaling up FP services, factors that affect facility utilization must be studied. Facility-level factors that impact client satisfaction include the lack of privacy (19), limited autonomy (20), inadequate communication (21), and poor sanitation (22). Inadequate quality of care may result in clients not returning for future services and premature discontinuation of contraceptives (23). Secular events such as large lockdowns that happened during COVID-19 pandemic, can reduce clinic attendance (24).
COVID-19 caused major disruptions from the illness itself, as well as from lockdowns instituted to curb infections. Pakistan saw five waves during the COVID-19 pandemic over two years (Khan et al, under review). Health services, including family planning, were disrupted, due to lockdowns when either clinics or outreach closed or when supplies could not be delivered, or because people opted to stay home. The United Nations Population Fund (UNFPA) estimated that access to FP services would be constrained due to COVID-19 for 12 million women in lower and middle income countries (LMIC), resulting in 1.4 million unintended pregnancies (25). In Pakistan, the health ministry records suggest that services resumed very quickly after the first quarter. A study of FP services in recent years must account for the impact of COVID-19 on these services.
The current study is the first exploration of volume of clients and the factors that influence such utilization, including the impact of COVID-19 disruptions, from two of Pakistan's largest private-sector clinic providers to understand healthcare utilization in the private sector. We used data from the Delivering Accelerated Family Planning in Pakistan (DAFPAK) program (2019–2025) by UK's Foreign, Commonwealth & Development Office (FCDO). DAFPAK was designed to increase access and quality of FP services through the public and private sectors, and is the largest donor funded FP program in Pakistan. The program funded social franchising implementing partners Marie Stopes Society (MSS) and DKT International to support private sector clinic based services (26).
Data and methodology
The study aims to evaluate the volume of clientele utilizing family planning services and examine the influence of facility-level characteristics, as well as the disruptions caused by COVID-19, on the utilization of these services. To attain this, we conducted a generalized negative binomial regression analysis.
Sample size data
Third-party validation and monitoring (TPV&M) of DAFPAK provided FCDO with insights, regular updates and assurance on the delivery, progress, and impact of the project. TPV&M collated quarterly reports and validated the results through six monthly field validation of implementing partners' (IPs) performance through provider assessments, product verification, facility/outlet verification, and training verification for private service providers through field surveys.
This study uses survey data collected during DAFPAK's six-monthly field validations survey. The analysis includes only those facilities that were active and serving clients at the time of the survey. Facilities not serving clients were excluded the data was collected in two phases. In the first phase, independent six-monthly field validation took place during February 2020 and validated the IPs results reported for the period July to December 2019. While in the second phase, independent six-monthly field validation was carried out during February 2021. The second phase reflects data collected for services rendered while the COVID-19 epidemic was extant.
We used a multi-stage cluster random sampling methodology, ensuring representation of all IPs service delivery modalities across DAFPAK implementation districts (which were treated as clusters for sampling). Using a UNICEF MICS 3 sample size calculator, and assuming a design effect of 1.5 with a marginal error of 95% confidence interval at 0.12 and allowing for up to 10% refusals. Data collection was done through electronic tablets using SurveyCTO.
The six-monthly data collection covered 324 and 355 facilities in the first and second phase of the program respectively. Facilities which did not serve any client were dropped from the analysis. In phase one and two, 23 and 17 facilities were dropped. Therefore, the final data included 301 and 338 facilities in phase one and two.
In phase 1, a total of 301 facilities (DKT = 163 and MSS = 138) were covered from 20 districts in 3 provinces. Eleven districts were from Khyber Pakhtunkhwa (KPK), 8 from Punjab, and 1 from Balochistan. In phase 2, 338 facilities (DKT = 178 and MSS = 160) were selected from a total of 15 districts; 9 from KPK, 5 from Punjab, and 1 from Balochistan. In total 639 facilities were spread across two time periods.
Variables
We have used count data representing the number of clients and products dispatched by each facility along with their characteristic variables.
Dependent variables
The number of clients visiting a facility for each family planning method was summed up for all facilities to generate the variable for volume of clients at the facility level for the last month. A similar variable for volume of products given out was obtained by adding the products given out by each facility in the sample for the last month. The volume of clients and products are used as the dependent variables in the regression analysis.
Independent variables
Facility type is a binary variable representing the type of family planning facility. The variable is given a value of 0 if the facility is operated by DKT and a value of 1 for MSS. Duration of facility is a continuous variable showing the duration in months since the facility has started its operation.
The variable region is a binary variable depicting if the facility is operating in an urban or rural area. A value of 1 is assigned if the facility is located in the urban settlement and 0 otherwise. Work experience is a continuous variable measured in terms of months where the minimum number of months a worker has worked with a facility is 2 months and the highest is 240 months. Work experience of service-providing staff can influence FP method uptake (26).
Moreover, variables presenting other infrastructural characteristics like availability of logo, washroom, and information, education, and communication (IEC) material like booklets, brochures, and charts may affect client satisfaction and visits to a facility. These are used as binary variables (No = 0 and Yes = 1) for this analysis. Since family planning is presumed to be dealt with privacy and maintaining privacy at facility center influences client's satisfaction and uptake of contraceptive (27, 28). A binary variable (overhearing conversation in the counseling area) is used as a proxy for privacy invasion. The variable takes on a value of 1 if people in the waiting room can overhear the conversation happening in the counselling area and 0 otherwise.
Lastly, COVID-19 is a binary variable taking on a value of 1 if the data collection was carried out during the COVID-19 time period and 0 otherwise. The second phase (second six monthly) of data collection took place during the COVID-19.
Statistical analysis
Preliminary cross-tabulations were performed to observe the empirical differences in the volume of clients and products between MSS and DKT. Based on these results, we further analyzed the association between the facility level characteristics and COVID-19 on the volume of clients and products.
Both datasets consist of count data collected at the facility level. The data was over-dispersed for outcome variables (Table 1). Hence, instead of an ordinary least square (OLS) or Poisson regression, a generalized negative binomial regression is used for this analysis. A negative binomial regression is a special type of regression that is used to determine the association between confounding variables on a count outcome variable that has over-dispersed data (13).
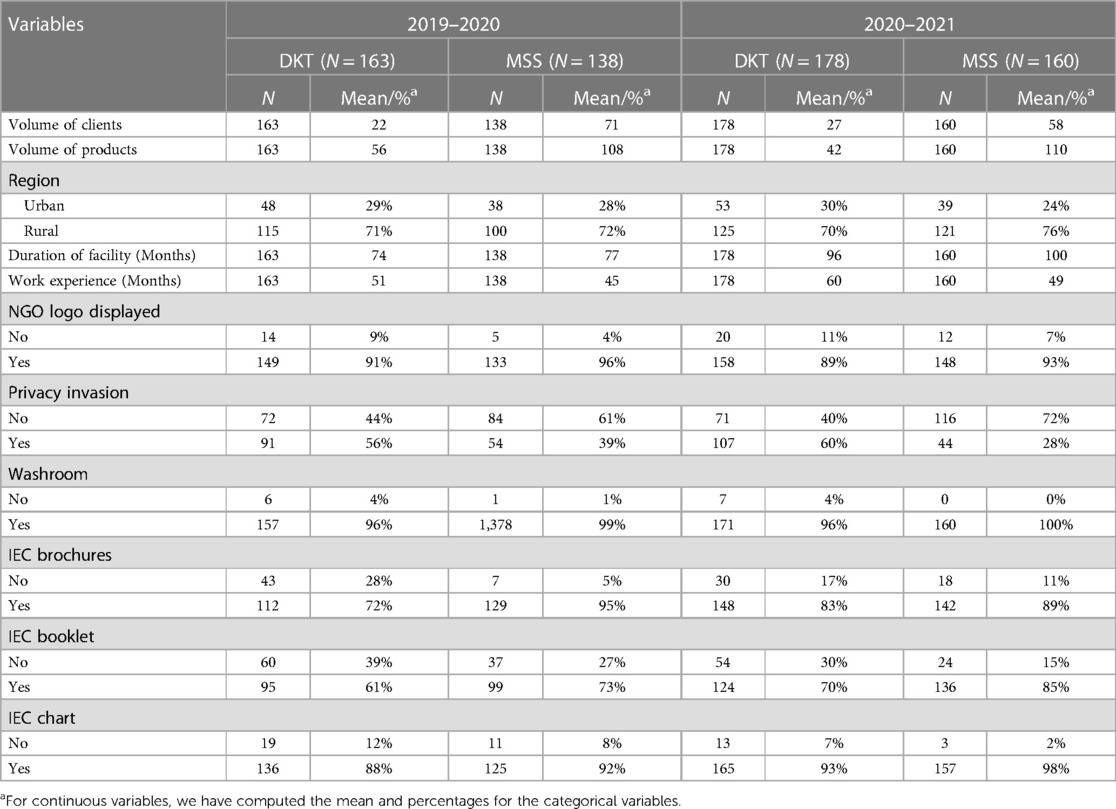
Table 1. Summary statistics of variables (February 2020 and February 2021).
The negative binomial regression equation used is as follows:
Generalized negative binomial regression is used to identify association between the type of facility (DKT/MSS) and region with volume of clients/products for the first and second phase separately. We have also included other facility-level characteristics like duration of facility, work experience of staff, availability of logo, washroom, IEC material and privacy that may affect the volume of clients and products.
Generalized negative binomial regression was also used to assess the impact of COVID-19 on volume of clients and products. Since first phase covers the pre COVID-19 time period and the second phase was initiated during the COVID-19. The datasets for both periods were appended and a binary variable for COVID-19 was generated (pre-COVID-19 = 0 and COVID-19 = 1) to incorporate the COVID-19 effect. Each regression was run separately for volume of clients and products.
Lastly, in order to analyze the impact of COVID-19 on client visits and product uptake of each method, generalized negative binomial regressions were run for each method type. The analysis was performed using the statistical software STATA 17.
Results
In the preliminary analysis, histograms of the total volume of clients and products were generated to assess the distribution of the data (Figure 1). Both distributions showed a right-skewed pattern. The skewness and kurtosis tests indicate that both volume of clients (p-value 0.000) and products (p-value 0.000) significantly deviate from normal distribution. The study included 163 DKT and 138 MSS facilities in phase one, and 178 DKT and 160 MSS facilities in phase two (Table 1). Most facilities (72%) were situated in the rural areas. On average each facility had been in existence for 87 months (7.25 years) and the average experience of the facility staff was around 52 months (4.33 years).
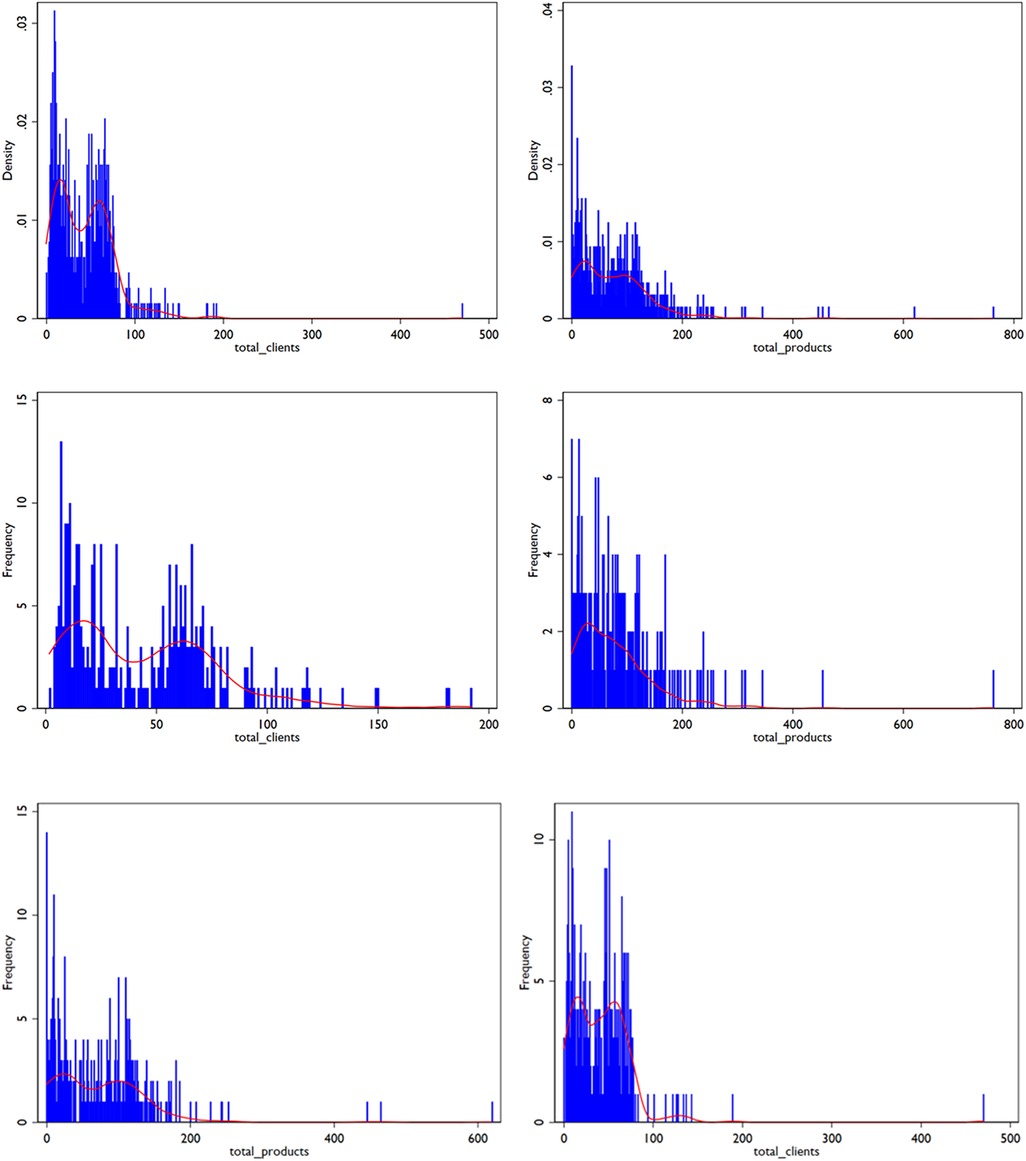
Figure 1. Density distribution of Volume of Clients and Products (Both Phases).
MSS served 9,784 and 9,267 clients per facility in phases 1 and 2 (Table 2). In phase 1, MSS facilities served an average of 71 clients per month, compared to 22 by DKT. During the second phase, MSS served an average of 58 clients per month, compared to 27 by DKT. MSS facilities served more clients with condoms and intra-uterine contraceptive device (IUCD) services, while DKT served more clients for the combined oral contraceptive (CoC), emergency contraceptive (EC) pills and injections. Notably, the average clientele per month for MSS dropped by 13 per month during the second phase, while it increased for DKT by 5.
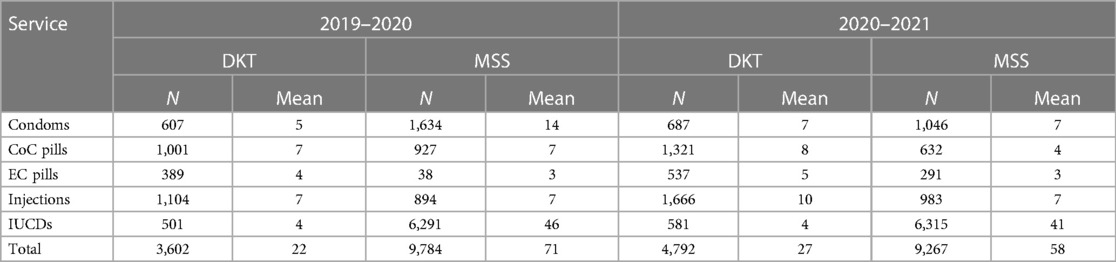
Table 2. Volume of clients served by facility type and products in the last month.
The pattern of products distributed was similar for the volume of clients (Table 3). MSS gave out more commodities per facility than DKT. The most common methods given by MSS were condoms and IUCD, while pills and injections were the main method for DKT. In the second period, DKT distributed fewer products per facility on average, while MSS increased its distribution.
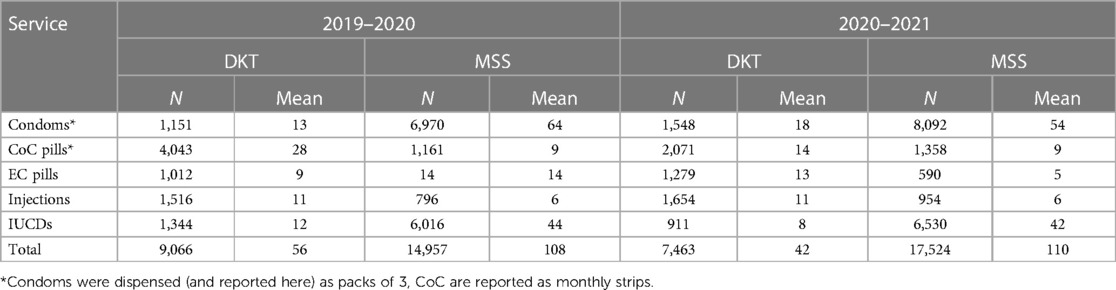
Table 3. Volume of product given out on average to each client by facility type in the last month.
Since each facility did not serve and distribute each type of client and product in both phases, the denominator was different for each method (Tables 7, 8 in Appendix). For the total, we used the total number of facilities in each phase (Table 1).
We estimated the average amount of products received by a client during their visit (Table 4). DKT clients received 2 packs of condoms, while MSS clients received 4 packs. DKT providers reported giving 1 injection and 3 IUCDs per visit to their clients (phase 1). During the COVID-19 period (phase 2), MSS providers reported giving twice as many condoms and pills as compared to phase one. In contrast, DKT providers gave out the same or slightly fewer commodities per visit during phase two. It is unclear why there are 2 or 3 IUCD listed per client visit by DKT providers.
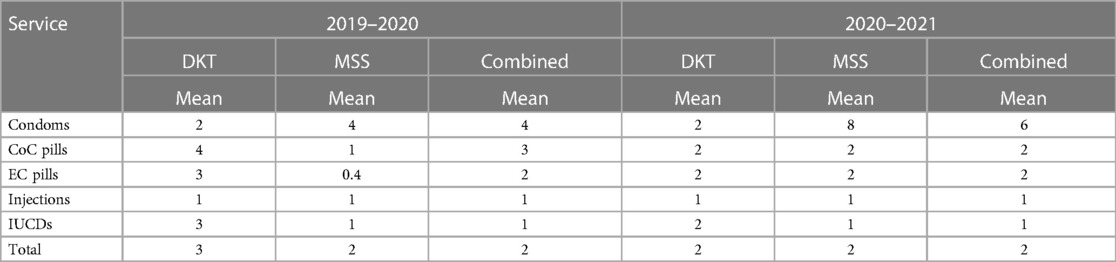
Table 4. Product per client by facility type in the last month.
Table 5 presents the results of a regression analysis for predictors of the volume of clients at facilities. After controlling for all other factors in the model, MSS had 3.15 times more clients than DKT facilities during phase 1 (IRR: 3.15; 95% CI: 2.74, 3.61) and 2.11 times more during phase 2 (IRR: 2.11; 95% CI: 1.79, 2.49). Absence of private space to talk about FP during a clinic visit was a key detractor of client visits that decreased client volume by 26% (IRR: 0.74; 95% CI: 0.67, 0.82). Factors that had no significant impact on client volumes were rural vs. urban location, the presence of an NGO logo on clinic board, work experience or duration of operation of the clinic, availability of IEC material or a washroom in the clinic. There was no difference observed in client volume during the COVID-19 period (2020–2021).
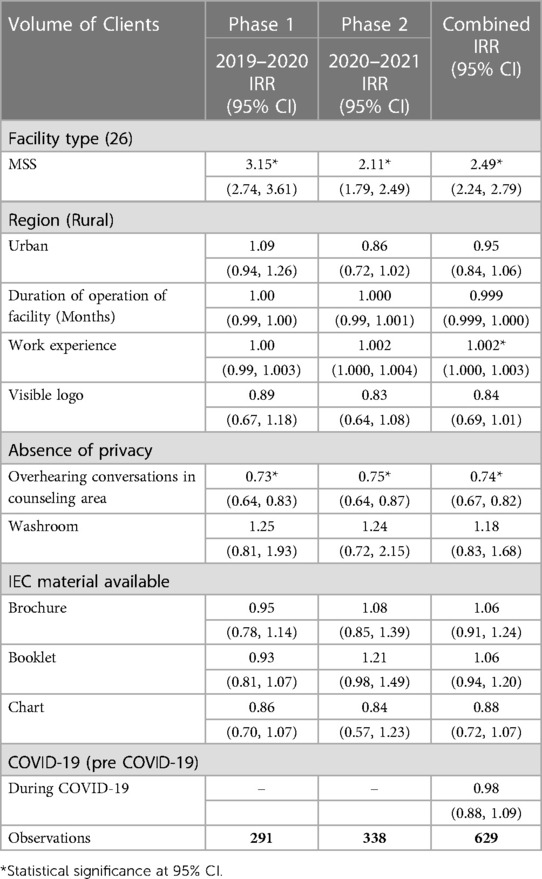
Table 5. Negative binomial regression for volume of clients visiting facilities.
A regression for product distribution shows comparable results (Table 6). On average, MSS facilities gave out 2.3 times more products than DKT facilities (IRR: 2.26; 95% CI: 1.94, 2.63). As with volume of clients, there was no significant impact of rural vs. urban location, duration of operation or work experience, availability of IEC material or a washroom. However, visibility of the NGO logo increased product volumes by 69% only during phase 1 but had no impact in phase 2. Conversely, absence of privacy did not impact product volumes in phase 1 but reduced them by 22% in phase 2. There was 16% less product distributed during phase 2, while COVID-19 was in sway.
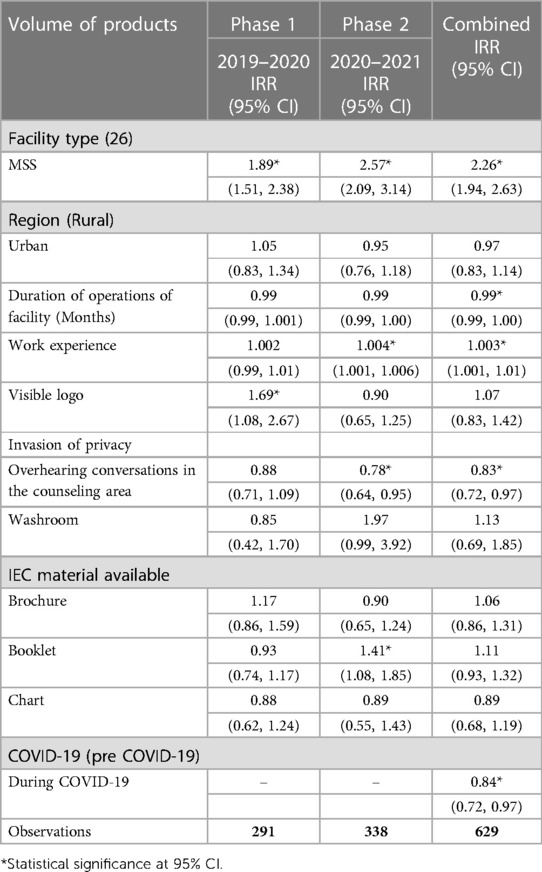
Table 6. Negative regression for volume of product.
Discussion
This is the first study to describe clinic volumes of major private providers of FP i.e., DKT and MSS in Pakistan. We found that MSS facilities consistently outperformed DKT facilities in both client volumes and product distribution across two phases. However, overall daily clientele is low for both NGOs. Common methods given out by MSS were condoms and IUCDs, while DKT served more clients with pills and injections. During COVID-19, MSS reported distributing short-term methods such as condoms and pills, whereas DKT's distribution remained static. Regression analysis revealed that MSS facilities had significantly more clients and distributed more products than DKT facilities. Absence of privacy was a major detractor for client volumes. Having an NGO logo, duration of practice, presence of a washroom or IEC materials did not affect client volumes. The COVID-19 pandemic led to a 16% reduction in product distribution during phase 2.
In Pakistan there is substantial underutilization of both private and public FP health facilities, underscoring significant room for scaling up client volumes at DKT and MSS supported clinics, other NGOs, and public sector clinics (29). DKT and MSS compare favorably with the public sector population welfare department facilities, which serve an average of two clients every three days, based on 725,000 clients served annually from its 3,300+ facilities nationwide (3). To address these gaps in FP services, it is crucial to enhance the capacity of existing clinics, such as the 300+ MSS clinics nationwide serving around 200,000–250,000 clients annually and 1,200+ DKT clinics nationwide serving around 250,000–300,000 clients annually. A previous analysis suggested that acquiring Pakistan's FP2030 targets requires a substantial increase in users, with an estimated additional 9 million users to achieve national targets (14). Mere tripling of these low volumes (to 5–9 clients a day) can add one million clients from these clinics alone, and more so if one includes the 7,000+ clinics supported by Greenstar Social Marketing and 125 by Rahnuma-Family Planning Association of Pakistan. Since a greater volume of clients increase efficiency and lowers costs per client, expanding the clientele would increase operating costs only marginally or not at all (30–32). In turn, these savings may eventually be used to open new efficient clinics and increase the total clientele of these NGOs (or of government facilities) in previously underserved areas (33).
Service and product outreach of DKT and MSS
Both MSS and DKT offer a wide array of method choices, reflecting the mandate of the DAFPAK project, and is consistent with the concept that availability of multiple methods increases overall uptake of FP (34). However, the specific method-mix also depends on the core model of the organization. IUCD and condoms for MSS, along with sterilization surgeries that are not part of the DAFPAK package and middle and high-end contraceptive pills and condoms for DKT. During COVID-19, as client volumes shrank, MSS clients received more condoms per visit, presumably to minimize contact, while the overall pattern remained unchanged for DKT. The high number of IUCD (2–3 per client) dispensed by DKT providers is unexplained.
Factors that affect clientele
Client satisfaction is considered as an indicator of quality service provision (35). Several factors affect client volumes including branding (particularly for socially franchised facilities), training and experience of providers, more spacious clinics, availability of washrooms, IEC material and appropriate privacy (19, 26). We found that a major factor associated with high client volumes is a facility's reputation for providing privacy. Prioritizing privacy and confidentiality are shown to be protective in reducing the discontinuation of family planning methods (35). Many health and family planning facilities are small establishments with 1–2 rooms, where patients are sometimes examined and counseled in the same room where other clients are also waiting, or in other instances, a mere curtain separates the two. It is therefore a major concern, particularly in communities where FP is not discussed publicly (35, 36).
Beyond privacy, studies have shown that providers' work experience, availability of equipment, and counseling material are significantly associated with client satisfaction and visits to FP facilities (26, 37). The fact that our analysis showed no association of these factors with client visits or products dispensed raises interesting questions about the role perceived quality plays in driving foot traffic at health facilities, and may be studied in future work. The presence of a banner displaying the name of the supporting organization was complex. While displaying such a banner did not affect client volumes, it increased the amount of product taken by clients per visit, suggesting that presence of a banner may increase trust, which in turn leads to higher quantities of contraceptives being purchased.
COVID-19 and family planning through social franchising
Many low and middle-income countries experienced a decline in method uptake, higher discontinuation of methods and fewer facilities visits during COVID-19 (38). A World Health Organization survey revealed that almost 70% of 105 countries experienced disruptions in family planning services due to the pandemic (39). These were driven by demand factors such as fear of acquiring infection at clinic visits, lack of knowledge about contraceptive availability during COVID-19 times, preferences for methods requiring with no or fewer trips to health facilities, restricted access to family planning facilities (24). Demand factors that further limited FP uptake were fewer clinics open, reduced outreach or referrals, limited counselling regarding side effects of contraceptives, and stock-outs related local or global supply chain disruption due to COVID-19 (32, 33). Specific changes in method mix varied across countries. A shift to condoms seen in our study is consistent with United Kingdom (40) and Ghana (41) where clients switched to short-term methods rather than long-term methods and may have been related to greater mobility of men, which may have been accentuated during COVID-19 (42). Moreover, condoms do not require medical personal assistance or counselling, hence, increasing its uptake (43). However, around 10% of women in Kenya and Burkina Faso shifted to more effective methods like injections and IUCDs that also minimized contact between clients and providers (44).
Providers in DAFPAK adapted by implementing social distancing and personal protection guidelines. Our results show that both the number of client visits and product uptake decreased during COVID-19. The average client visit per facility decreased for each method except EC pills and injections, as did the average product given out per facility, with the highest decreases for CoC pills and the least for emergency contraception pills and injections. Between the two-time periods, the product mix shifted from CoC pills (22%–14%) to mainly condoms (34%–39%) followed by EC pills (4%–7%) during the COVID-19, while injections (10%) and IUCDs (31%) remained unchanged. In essence, there was a slight shift from more reliable methods to condoms and presumably some dropouts.
Limitations
Our study is limited by the fact that it depicts data from only two private sector providers, DKT and MSS. Although they are among the largest of such NGOs, the absence of Greenstar Social Marketing (GSM), the Family Planning Association of Pakistan (FPAP) and outreach NGOs is a gap. While utilization patterns of those NGOs is likely similar (Dr. Aziz Rab, CEO GSM, personal communications), it would have been useful to formally document their patterns. Secondly, since private providers don't often keep service records, data were collected using supply lists plus some element of recall which could have added errors.
Recommendations
To enhance family planning services, prioritize enhancing the serving capacity of existing DKT and MSS clinics over opening new clinics, reducing costs per user and improving clinic efficiency. The cost savings can then be used to open new, efficient clinics in previously underserved areas, expanding the clientele. Improve the physical infrastructure of health and family planning facilities, particularly in low-resource settings, ensuring better privacy and confidentiality for clients by providing more spacious clinics, and separate rooms for counseling/examinations and waiting. Additionally, investing in providing training on privacy and confidentiality could enhance client satisfaction, increasing family planning method uptake and continuation. Additionally, enhance access to family planning services during pandemics by promoting telemedicine and home delivery services for contraceptives, mitigating disruptions caused by factors such as fear of infection, reduced clinic visits, and supply chain disruptions, ensuring continuous access to contraceptives and supporting method continuation.
Conclusion
This study provides insight into the effectiveness of private-sector providers. The private sector has better utilization but a smaller footprint than the public sector. However, both public and private sector health and FP facilities are significantly underutilized and can improve substantially. In particular, private (mostly urban) and public (more often rural) clinics are complementary in where they are located and the clientele they serve. Thus, such contributions from the private sector are vital if Pakistan were to achieve its FP2030 goals. Moreover, while FP services are enhanced, COVID-19 highlighted the importance of emergency preparedness to avoid crucial service outages in emergencies. This would include both the means to offer services and to maintain supply chains to ensure appropriate commodity security is assured.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
N: Writing – original draft, Methodology, Formal Analysis, Data curation, Conceptualization. TA: Writing – original draft, Methodology, Formal Analysis, Supervision. AF: Writing – review & editing, Validation. IS: Writing – review & editing, Data curation, Conceptualization. ZU: Methodology, Formal Analysis, Writing – review & editing. AyK: Writing – review & editing, Validation. SS: Writing – review & editing, Validation. AdK: Methodology, Writing – review & editing, Validation, Supervision, Conceptualization.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported, in whole or in part, by the Bill & Melinda Gates Foundation [grant number: INV-025171]. Under the grant conditions of the Foundation, a Creative Commons Attribution 4.0 Generic License has already been assigned to the Author Accepted Manuscript version that might arise from this submission.
Acknowledgments
This research study was supported through the British High Commission (BHC)-funded Delivering Accelerated Family Planning in Pakistan (DAFPAK) program (£90 million, October 2017–June 2025). DAFPAK aims to increase demand for family planning, expand the availability of quality family planning services in both private and public sectors, provide technical assistance and support a more conducive, coherent, and supportive policy framework for family planning. The data used in this study was collected as part of the third-party validation monitoring and research component of DAFPAK, led by Integrity. Field data collection was led by Research and Development Solutions (RADS). Additionally, we thank Mr. Muhammad Ibrahim for his assistance in understanding the data issues and cleaning, reviewing, and suggesting the methodology along with deeper insights on the analysis, and reviewing the final version before publication.
Nayab Nayab, Taimoor Ahmad, Areesh Fatmee, Ibstisam Sajjad, Zona Usmani, Ayesha Khan, Sara Shahzad and Adnan Ahmad Khan.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. GOV.UK. Family planning summit: summary of UK commitments. Available online at: https://www.gov.uk/government/publications/family-planning-summit-summary-of-uk-commitments (Cited March 26, 2024).
2. UNFPA Pakistan. (2019). National symposium on alarming population growth in Pakistan. Available online at: https://pakistan.unfpa.org/en/publications/national-symposium-alarming-population-growth-pakistan (Cited March 26, 2024).
3. Khan AA. Family planning trends and programming in Pakistan. J Pak Med Assoc. (2021) 71(Suppl 7)(11):S3–11.
4. NIPS/Pakistan NI of PS, International ICF. Pakistan demographic and health survey 2012–2013 (2013). Available online at: https://dhsprogram.com/publications/publication-fr290-dhs-final-reports.cfm (Cited March 26, 2024).
5. NIPS/Pakistan NI of PS, International M. Pakistan demographic and health survey 2006–2007 (2008). Available online at: https://dhsprogram.com/publications/publication-fr200-dhs-final-reports.cfm (Cited March 26, 2024).
6. National Institute of Population Studies (NIPS) I. Pakistan demographic and health survey 2017–2018. Available online at: https://dhsprogram.com/pubs/pdf/FR354/FR354.pdf (Accessed March 16, 2024).
7. Final Results (Census-2017) Pakistan Bureau of Statistics. Available online at: https://www.pbs.gov.pk/content/final-results-census-2017 (Cited March 30, 2024).
8. World Population Prospects 2019: Highlights. 10 Key findings—It’s over 9000!. Available online at: https://www.medbox.org/document/world-population-prospects-2019-highlights-10-key-findings (Cited March 26, 2024).
9. Campbell OMR, Benova L, Macleod D, Goodman C, Footman K, Pereira AL, et al. Who, what, where: an analysis of private sector family planning provision in 57 low- and middle-income countries. Trop Med Int Health. (2015) 20(12):1639–56. doi: 10.1111/tmi.12597
10. Khan AA, Khan A, Javed W, Hamza HB, Orakzai M, Ansari A, et al. Family planning in Pakistan: applying what we have learned. J Pak Med Assoc. (2013) 63(4 Suppl. 3):S3–10.24386723
11. UNFPA Pakistan. (2019). Improving access to family planning services through the private sector in Pakistan a stakeholder analysis. Available online at: https://pakistan.unfpa.org/en/publications/improving-access-family-planning-services-through-private-sector-pakistan-stakeholder (Cited March 26, 2024).
12. Hafeez A, Mohamud BK, Shiekh MR, Shah SAI, Jooma R. Lady health workers programme in Pakistan: challenges, achievements and the way forward. J Pak Med Assoc. (2011) 61(3):210–5.21465929
13. Hunt S, Wood P, Zulfiqar T, Cheema I, Malanag I, Arif M. Lady health worker programme: third party evaluation of performance (2009).
14. Abdullah M, Bilal F, Khan R, Ahmed A, Khawaja AA, Sultan F, et al. Raising the contraceptive prevalence rate to 50% by 2025 in Pakistan: an analysis of number of users and service delivery channels. Health Res Policy Syst. (2023) 21(1):4. doi: 10.1186/s12961-022-00950-y
15. Social franchising: a blockbuster to address unmet need for family planning and to advance toward the FP2020 goal. Glob Health Sci Pract. (2015) 3(2):147–8. doi: 10.9745/GHSP-D-15-00155
16. Munroe E, Hayes B, Taft J. Private-sector social franchising to accelerate family planning access, choice, and quality: results from marie stopes international. Glob Health Sci Pract. (2015) 3(2):195–208. doi: 10.9745/GHSP-D-15-00056
17. Azmat SK, Shaikh BT, Hameed W, Mustafa G, Hussain W, Asghar J, et al. Impact of social franchising on contraceptive use when complemented by vouchers: a quasi-experimental study in rural Pakistan. PLoS One. (2013) 8(9):e74260. doi: 10.1371/journal.pone.0074260
18. Beyeler N, York De La Cruz A, Montagu D. The impact of clinical social franchising on health services in low- and middle-income countries: a systematic review. PLoS One (2013) 8(4):e60669. doi: 10.1371/journal.pone.0060669
19. Brittain AW, Williams JR, Zapata LB, Moskosky SB, Weik TS. Confidentiality in family planning services for young people. Am J Prev Med. (2015) 49(2 0 1):S85–92. doi: 10.1016/j.amepre.2015.04.001
20. Saleem S, Bobak M. Women’s autonomy, education and contraception use in Pakistan: a national study. Reprod Health. (2005) 2(1):8. doi: 10.1186/1742-4755-2-8
21. Bossyns P, Miyé H, VLerberghe W. Supply-level measures to increase uptake of family planning services in Niger: the effectiveness of improving responsiveness. Trop Med Int Health. (2002) 7(4):383–90. doi: 10.1046/j.1365-3156.2002.00865.x
22. Naseer M. Determinants of patient’s satisfaction with health care system in Pakistan: a critical review (2012).
23. Shahidzadeh-Mahani A, Omidvari S, Baradaran HR, Azin SA. Factors affecting quality of care in family planning clinics: a study from Iran. Int J Qual Health Care. (2008) 20(4):284–90. doi: 10.1093/intqhc/mzn016
24. UNFPA. Impact of COVID-19 on family planning: what we know one year into the pandemic. Available online at: https://www.unfpa.org/resources/impact-covid-19-family-planning-what-we-know-one-year-pandemic (Cited March 26, 2024).
25. Pakistan. DKT international. Available online at: https://www.dktinternational.org/country-programs/pakistan/ (Cited March 26, 2024).
26. Hamid S, Stephenson R. Provider and health facility influences on contraceptive adoption in urban Pakistan. Int Fam Plan Perspect. (2006) 32(2):71–8. doi: 10.1363/3207106
27. Wogu D, Lolaso T, Meskele M. Client satisfaction with family planning services and associated factors in Tembaro District, Southern Ethiopia. Open Access J Contracept. (2020) 11:69–76. doi: 10.2147/OAJC.S258831
28. Agha S, Do M. The quality of family planning services and client satisfaction in the public and private sectors in Kenya. Int J Qual Health Care. (2009) 21(2):87–96. doi: 10.1093/intqhc/mzp002
29. Abbas K, Khan A, Khan A. Costs and utilization of public sector family planning services in Pakistan. J Pak Med Assoc. (2013) 63:S33–9.24386728
30. World Bank Blogs. Investing in sexual and reproductive health paves the way for healthier families and stronger economies. Available online at: https://blogs.worldbank.org/en/health/investing-sexual-and-reproductive-health-paves-way-healthier-families-and-stronger-economies (Cited March 31, 2024).
31. Silumbwe A, Nkole T, Munakampe MN, Milford C, Cordero JP, Kriel Y, et al. Community and health systems barriers and enablers to family planning and contraceptive services provision and use in Kabwe District, Zambia. BMC Health Serv Res. (2018) 18(1):390. doi: 10.1186/s12913-018-3136-4
32. Patil SR, Gopalakrishnan L, Sai VS, Matikanya R, Rajpal P. Markets, incentives, and health promotion can improve family planning and maternal health practices: a quasi-experimental evaluation of a tech-enabled social franchising and social marketing platform in India. BMC Public Health. (2024) 24(1):264. doi: 10.1186/s12889-023-17413-w
33. Goldberg D, Sahgal B, Beeson T, Wood S, Mead H, Abdul-Wakil A, et al. Patient perspectives on quality family planning services in underserved areas. Patient Exp J. (2017) 4(1):54–65. doi: 10.35680/2372-0247.1194
34. Ross J, Stover J. Use of modern contraception increases when more methods become available: analysis of evidence from 1982 to 2009. Glob Health Sci Pract. (2013) 1(2):203–12. doi: 10.9745/GHSP-D-13-00010
35. Corley AG, Sprockett A, Montagu D, Chakraborty NM. Exploring and monitoring privacy, confidentiality, and provider bias in sexual and reproductive health service provision to young people: a narrative review. Int J Environ Res Public Health. (2022) 19(11):6576. doi: 10.3390/ijerph19116576
36. Nour T. The magnitude and factors associated with unmet need for family planning among married women in Jigjiga City administration, Somali Region, Eastern Ethiopia (2019).
37. Tessema GA, Streak Gomersall J, Mahmood MA, Laurence CO. Factors determining quality of care in family planning services in Africa: a systematic review of mixed evidence. PLoS ONE. (2016) 11(11):e0165627. doi: 10.1371/journal.pone.0165627
38. Malkin M, Mickler AK, Ajibade TO, Coppola A, Demise E, Derera E, et al. Adapting high impact practices in family planning during the COVID-19 pandemic: experiences from Kenya, Nigeria, and Zimbabwe. Glob Health Sci Pract. (2022) 10(4):e2200064. doi: 10.9745/GHSP-D-22-00064
39. Roberton T, Carter ED, Chou VB, Stegmuller AR, Jackson BD, Tam Y, et al. Early estimates of the indirect effects of the COVID-19 pandemic on maternal and child mortality in low-income and middle-income countries: a modelling study. Lancet Glob Health. (2020) 8(7):e901–8. doi: 10.1016/S2214-109X(20)30229-1
40. Walker SH. Effect of the COVID-19 pandemic on contraceptive prescribing in general practice: a retrospective analysis of English prescribing data between 2019 and 2020. Contracept Reprod Med. (2022) 7(1):3. doi: 10.1186/s40834-022-00169-w
41. Fuseini K, Jarvis L, Hindin MJ, Issah K, Ankomah A. Impact of COVID-19 on the use of emergency contraceptives in Ghana: an interrupted time series analysis. Front Reprod Health. (2022) 4:811429. doi: 10.3389/frph.2022.811429
42. Caselli F, Grigoli F, Sandri D, Spilimbergo A. Mobility under the COVID-19 pandemic: asymmetric effects across gender and age. IMF Econ Rev. (2022) 70(1):105–38. doi: 10.1057/s41308-021-00149-1
43. Aslam S, Farooq N, Qurrat-Ul-Ain , Bano T, Kanwal T, Akhter Z, et al. Frequency and trend of contraception services during the COVID 19 pandemic; A two-year retrospective analysis at a tertiary care hospital. J Soc Obstetricians Gynaecologists Pak. (2022) 12(3):235–40.
44. Karp C, Wood SN, Guiella G, Gichangi P, Bell SO, Anglewicz P, et al. Contraceptive dynamics during COVID-19 in sub-Saharan Africa: longitudinal evidence from Burkina Faso and Kenya. BMJ Sex Reprod Health. (2021) 47(4):252–60. doi: 10.1136/bmjsrh-2020-200944
Appendix

Table 7. Facilities providing services (clients) across both phase.
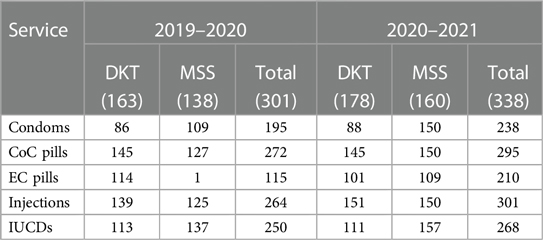
Table 8. Facilities providing products across both phase.
Keywords: family planning, social franchising, COVID-19, volume of clients, volume of products, privacy of clients, clients of family planning
Citation: Nayab, Ahmad T, Fatmee A, Sajjad I, Usmani Z, Khan A, Shahzad S and Khan AA (2024) Utilization of social franchising in family planning services: a Pakistan perspective. Front. Glob. Womens Health 5:1376374. doi: 10.3389/fgwh.2024.1376374
Received: 25 January 2024; Accepted: 3 May 2024;
Published: 17 May 2024.
Reviewed by:
Eleonora Hristova-Atanasova, Medical University of Plovdiv, BulgariaSarosh Iqbal, University of Management and Technology, Pakistan
© 2024 Nayab, Ahmad, Fatmee, Sajjad, Usmani, Khan, Shahzad and Khan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Adnan Ahmad Khan, adnan@resdev.org