 Joana Vitte1,2*
Joana Vitte1,2* Stéphane Ranque3,4
Stéphane Ranque3,4 Ania Carsin2,5
Ania Carsin2,5 Carine Gomez4,6Thomas Romain1Carole Cassagne3,4Marion Gouitaa7Mélisande Baravalle-Einaudi5Nathalie Stremler-Le Bel5Martine Reynaud-Gaubert4,6Jean-Christophe Dubus4,5
Carine Gomez4,6Thomas Romain1Carole Cassagne3,4Marion Gouitaa7Mélisande Baravalle-Einaudi5Nathalie Stremler-Le Bel5Martine Reynaud-Gaubert4,6Jean-Christophe Dubus4,5 Jean-Louis Mège1,4
Jean-Louis Mège1,4 Jean Gaudart8
Jean Gaudart8
- 1Aix-Marseille Univ, APHM Assistance Publique Hôpitaux de Marseille, Hôpital de La Conception, Laboratoire d’Immunologie, Marseille, France
- 2Aix-Marseille Univ, UMR INSERM 1067 CNRS 7333, Marseille, France
- 3Aix-Marseille Univ, APHM Assistance Publique Hôpitaux de Marseille, Hôpital Timone, Laboratoire de Parasitologie, Marseille, France
- 4Aix-Marseille Univ, URMITE, UMR 63, CNRS 7278, INSERM U1095, IRD 198, Marseille, France
- 5Aix-Marseille Univ, APHM Assistance Publique Hôpitaux de Marseille, Hôpital Timone Enfants, Pneumo-pédiatrie, Centre de Ressources et de Compétences en Mucoviscidose, Marseille, France
- 6Aix-Marseille Univ, APHM Assistance Publique Hôpitaux de Marseille, Hôpital Nord, Centre de Ressources et de Compétences en Mucoviscidose, Marseille, France
- 7Aix-Marseille Univ, APHM Assistance Publique Hôpitaux de Marseille, Hôpital Nord, Service de Pneumologie, Marseille, France
- 8Aix Marseille Univ, IRD, INSERM, SESSTIM UMR 912, Faculté de Médecine campus Timone, Marseille, France
Molecular-based allergy diagnosis yields multiple biomarker datasets. The classical diagnostic score for allergic bronchopulmonary aspergillosis (ABPA), a severe disease usually occurring in asthmatic patients and people with cystic fibrosis, comprises succinct immunological criteria formulated in 1977: total IgE, anti-Aspergillus fumigatus (Af) IgE, anti-Af “precipitins,” and anti-Af IgG. Progress achieved over the last four decades led to multiple IgE and IgG(4) Af biomarkers available with quantitative, standardized, molecular-level reports. These newly available biomarkers have not been included in the current diagnostic criteria, either individually or in algorithms, despite persistent underdiagnosis of ABPA. Large numbers of individual biomarkers may hinder their use in clinical practice. Conversely, multivariate analysis using new tools may bring about a better chance of less diagnostic mistakes. We report here a proof-of-concept work consisting of a three-step multivariate analysis of Af IgE, IgG, and IgG4 biomarkers through a combination of principal component analysis, hierarchical ascendant classification, and classification and regression tree multivariate analysis. The resulting diagnostic algorithms might show the way for novel criteria and improved diagnostic efficiency in Af-sensitized patients at risk for ABPA.
Introduction
Aspergillus fumigatus (Af) is a ubiquitous airborne fungus clinically relevant in asthmatic, cystic fibrosis (CF), and immunosuppressed patients. Af–human host interaction spans asymptomatic immunization with detectable immunoglobulin G to Af, sensitization with detectable IgE to Af, through severe pulmonary or systemic diseases such as allergic bronchopulmonary aspergillosis (ABPA), chronic pulmonary aspergillosis, invasive aspergillosis, and chronic lung allograft disease (1).
Diagnosis of Af-related disease relies on a body of clinical, radiological, immunological and mycological evidence. Among Af-related diseases in humans, ABPA or Hinson and Pepys’ disease (2, 3) is the most frequent, preferentially targeting CF and asthmatic patients. The estimated prevalence of ABPA is 8–10% (range 1–25%) among CF patients and 1–2% among asthmatic ones (4–6). Lung transplantation does not completely prevent ABPA (7). ABPA diagnosis is particularly arduous in CF patients, as they may experience cough, bronchospasm, intercurrent infections, radiological abnormalities, Af colonization, and/or sensitization without true ABPA (4). In addition, mere colonization or sensitization by Af has been shown to contribute to the deterioration of respiratory function, in pediatric and adult CF patients (6, 8–11). A chronic disease made up of a succession of flare up and remission, ABPA has a major social burden impact, threatening people with asthma, 334 million people worldwide (12) and CF, around 70,000 people (13).
The diagnostic score for ABPA, established in 1977 and updated in 2013, includes succinct immunological criteria: total IgE, anti-Af IgE, anti-Af “precipitins,” and anti-Af IgG (14). Progress achieved over the last four decades in the understanding and workup of Af—immune response cross talk led to the identification of multiple IgE and IgG biomarkers, with quantitative, standardized, molecular-level reports (15–17). Yet, the newly available biomarkers are not included in ABPA diagnostic criteria, either individually or in algorithms, despite favorable reports (1) and persisting underdiagnosis of ABPA (4). This prompted us to apply multivariate statistical analysis to Af-related immune biomarkers in search for a discriminant yet doctor-friendly diagnostic tool. We present here a proof-of-concept work on the potential benefit of multivariate algorithms for the diagnosis of ABPA.
Materials and Methods
The statistical analysis was performed retrospectively using flowcharts and laboratory data from 39 ABPA-free CF patients with detectable sIgE to Af extract (Af-CF group) and 10 ABPA patients (7 asthmatics, 3 CF; 2 children) from the Adult and Pediatric Regional Centers for Cystic Fibrosis (RCCF) and the Pulmonology Departments of Marseille, Southern France. Patient demography and detailed sIgE and sIgG4 data were previously described (17). Data from one ABPA patient (CF background, 12-year-old male) diagnosed with ABPA in July 2016 were included.
sIgE, sIgG, and sIgG4 for Af extract and recombinant allergens Asp f 1, Asp f 2, Asp f 3, Asp f 4, and Asp f 6 were measured with Thermo Fisher ImmunoCAP (Uppsala, Sweden). The detection thresholds were 0.01 mgA/L for sIgG and sIgG4 and 0.11 kUA/L for sIgE. In 44 of these 49 patients, determination of IgG to Af was also performed with an ELISA kit (Orgentec, Trappes, France), and Af precipitins were evaluated by immunoelectrophoresis (Sebia, Evry, France). ABPA patients were assayed at the initial diagnosis of ABPA or during a subsequent flare. The diagnosis of ABPA relied on (i) acute or subacute pulmonary function deterioration in patients with asthma or CF; (ii) total IgE levels of 500 kIU/L or higher; (iii) elevated levels of specific IgE and either sIgG or precipitins to Af; and (iv) chest or computed tomographic pulmonary infiltrates, with pathognomonic high attenuation mucous plugging. Therapeutic unresponsiveness to antibiotics, followed by resolution under corticosteroid treatment, was an additional criterion. Skin prick test reactivity for Af was not assessed because of discontinued availability of fungal Af extracts.
Ethics Statement
Recombinant Af allergen sIgE and sIgG (4) determination was part of the regular medical care since their commercial release. Patients received written laboratory workup reports. The study was based on a retrospective, non-interventional review of medical charts and laboratory results. According to the French law (18, 19), ethical approval and patient consent were not necessary for this type of study, while patients were informed and retained the right to oppose the use of their anonymized medical data for research purposes.
Statistical Analysis
First, we performed a hierarchical classification on principal components, as previously described (20, 21). All the variables (biomarker measures) were included in this analysis and were equally weighted. A principal component analysis (PCA) was the first preprocessing step to explore the biomarker on the mixed data set, which takes into consideration relationships between biomarkers. Then, the coordinates of each variable in the first 20 principal components, which summarize 95% of the information, were used to perform a hierarchical ascendant classification (HAC). This method provides classes according to the immunological profile using an objective non-supervised classification technique that allows classifying independently from diagnosis. Furthermore, using the first 20 principal components is a way of denoising the data, thus yielding a more robust classification (21).
Next, we performed a classification and regression tree (CART) multivariate analysis. CART is a supervised, non-parametric and non-linear regressive approach (22), which classified the patients according to the outcome binary variable ABPA or Af-CF. Among all covariates, CART analyzed each possible threshold to split the sample in two opposite homogeneous groups. This process was recursively repeated until an optimal criterion was reached. The process enabled a tree to be built in which the terminal classes were groups with common biomarker findings. Statistical analysis was performed using R2.13.0 (R Foundation for Statistical Computing; http://cran.r-project.org/).
Results
The PCA-HAC approach identified three clusters within the population, with a homogenous cluster 1 comprising 34/39 Af-CF patients, cluster 2 comprising 6/10 ABPA patients, and cluster 3 including both ABPA and Af-CF patients (Figure 1).
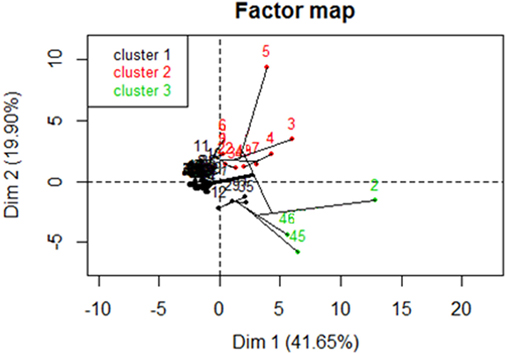
Figure 1. Hierarchical ascendant classification on principal component analysis (PCA) of the study sample. X- and Y-axes are the two first dimensions issued from the PCA. Patients are denoted 1–10 for the allergic bronchopulmonary aspergillosis (ABPA) group and 11–49 for the Aspergillus fumigatus (Af)-cystic fibrosis (CF) group. Af-sensitized patients without ABPA (Af-CF) are mostly found in the homogenous cluster 1 (34/39), while ABPA patients are mostly found in cluster 2 (6/10).
Classification and regression tree multivariate analysis method applied to current biomarkers of ABPA (total IgE, sIgE to Af, ELISA IgG to Af, and Af precipitins) resulted in a classification based on three parameters only: total IgE, ELISA IgG, and sIgE. Together, these three results allowed correct classification of 38/39 Af-CF patients and 3/10 ABPA patients. The remaining seven ABPA patients were correctly classified with a probability of 88% (Figure S1 in Supplementary Material).
Classification and regression tree was sequentially performed on datasets of either sIgE, IgG or IgG4 responses to Af molecules Asp f 1, Asp f 2, Asp f 3, Asp f 4, and Asp f 6. The molecular sIgE dataset allowed proper classification of 35/39 Af-CF patients and 8/10 ABPA, the latter with an 89% probability (Figure S2 in Supplementary Material).
Datasets of either IgG or IgG4 responses to molecules Asp f 1, Asp f 2, Asp f 3, Asp f 4, and Asp f 6 resulted in 70–80% of incorrect classification of ABPA patients (not shown), in line with previous IgG4 results (17).
Finally, the classification tree built using the three molecular datasets together (sIgE, sIgG, and sIgG4) performed better, and adequately classified 35/39 Af-CF and 7/10 ABPA patients. The number of equivocally classified Af-CF or ABPA patients was reduced to 4 and 3, respectively (Figure 2).
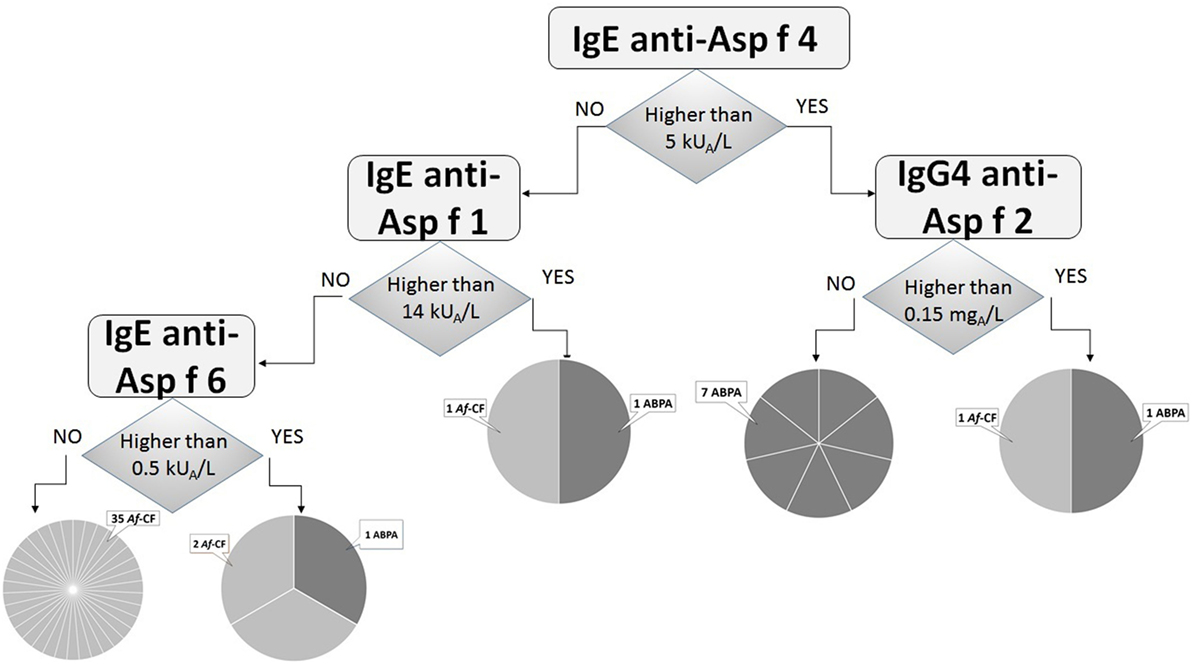
Figure 2. Classification tree using analysis of sIgE, sIgG, and sIgG4 responses to Asp f 1, Asp f 2, Asp f 3, Asp f 4, and Asp f 6 molecules. The diagnostic algorithm retains IgE to Asp f 4, Asp f 1, Asp f 6, and IgG4 to Asp f 2, yielding 1 Aspergillus fumigatus (Af)-cystic fibrosis (CF)-only groups counting 35/39 patients, 1 allergic bronchopulmonary aspergillosis (ABPA)-only group of 7 patients, and 3 mixed groups of undetermined clinical significance where other criteria are needed. Overall, 7/10 ABPA patients and 35/39 Af-CF patients are clearly identified.
Discussion
The present study shows that multivariate analysis approaches can be applied to the analysis of complex Af-induced immune response patterns and hold promise for improving diagnostic discrimination between ABPA and ABPA-free patients.
While the multivariate analysis of the current diagnostic criteria (total IgE, sIgE to Af, ELISA IgG to Af, and Af precipitins) correctly classified 38/39 of Af-CF patients, only 3/10 ABPA patients were correctly classified (Figure S1 in Supplementary Material). This result suggests that current criteria perform well at identifying ABPA-free patients and excluding ABPA diagnosis but are not optimally efficient for ABPA diagnosis. Shifting from sIgE against Af extracts to their molecular counterparts improved ABPA identification. Indeed, the best performance for identifying ABPA cases (8/10 correctly classified patients, Figure S2 in Supplementary Material) was obtained with multivariate analysis of molecular sIgE responses alone, a finding that supports the prominent pathophysiological and diagnostic significance of sIgE responses in ABPA.
The best compromise for identifying both Af-CF and ABPA patients was obtained with multivariate analysis of sIgE, IgG, and IgG4 against molecular Asp f 1, Asp f 2, Asp f 3, Asp f 4, and Asp f 6. The algorithm retained only four parameters (sIgE to Asp f 4, Asp f 1, and Asp f 6; IgG4 to Asp f 2) and correctly classified 35/39 Af-CF and 7/10 ABPA patients (Figure 2). This result is in line with previous reports on Asp f 4, Asp f 6, and Asp f 1 as ABPA biomarkers [reviewed in Ref. (1)].
In terms of overall diagnostic performance, multivariate analysis still needs improvement. One clue may come from the PCA results, which show that most Af-CF cases cluster together (34/39, cluster 1), but ABPA cases only partially do so (6/10, cluster 2, Figure 1). Biological heterogeneity resulting in a mixed Af-CF and ABPA cluster 3 needs further work. Differences might be underlain by sIgE or IgG (4) responses to further Af molecules currently not available. Conversely, it is likely that genetic, clinical, or radiological features not considered in our study may contribute to Af-CF and ABPA heterogeneity. Finally, increasing the size of the study population should improve the power of statistical analysis and yield more performant diagnostic flowcharts.
Taken together, our results add a diagnostic perspective to recent reports of multivariate analysis in allergic patients as a basis for personalized medicine (23). Further confirmation on large-scale populations and detailed analysis of variables are necessary. However, we believe that multivariate analysis of the complex Af-induced immune responses will pave the way for the discovery of clinically efficient diagnostic biomarkers and novel ABPA diagnostic algorithms.
Ethics Statement
Recombinant Af allergen sIgE and sIgG (4) determination was part of the regular medical care since their commercial release. Patients received written laboratory workup reports. The study was based on a retrospective, non-interventional review of medical charts and laboratory results. According to the French law (18, 19), ethical approval and patient consent were not necessary for this type of study, while patients were informed and retained the right to oppose the use of their anonymized medical data for research purposes.
Author Contributions
JV, SR, and JG designed the research. AC, CG, MG, NB, MB-E, MR-G, and J-CD reviewed and collected clinical data. SR and CC interpreted and collected mycological data. TR and JV interpreted and collected immunological data. JG performed statistical analysis. JV, SR, J-CD, MR-G, J-LM, and JG wrote the manuscript. All the authors read and approved the final version of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at http://journal.frontiersin.org/article/10.3389/fimmu.2017.01019/full#supplementary-material.
Figure S1. Classification tree using the classical laboratory measures comprised in the current diagnostic score of allergic bronchopulmonary aspergillosis (ABPA) (redrawn). The diagnostic algorithm retains total IgE, ELISA IgG, and specific IgE, yielding 2 Aspergillus fumigatus (Af)-cystic fibrosis (CF)-only groups counting 38/39 patients, 1 ABPA-only group of 3 patients, and 1 mixed group of 8 patients with an 88% probability of having ABPA. Overall, 38/39 Af-CF patients, but only 3/10 ABPA patients are clearly identified.
Figure S2. Classification tree analyzing sIgE responses to Asp f 1, Asp f 2, Asp f 3, Asp f 4, and Asp f 6 molecules. The resulting diagnostic algorithm retains IgE to Asp f 4, Asp f 1, and Asp f 6, yielding 1 Aspergillus fumigatus (Af)-cystic fibrosis (CF)-only group counting 35/39 patients, 1 mixed group of 9 patients with an 89% probability of having allergic bronchopulmonary aspergillosis (ABPA), and 2 mixed groups of undetermined clinical significance where other criteria are needed. Overall, 35/39 Af-CF patients, but no ABPA patients are clearly identified.
Abbreviations
ABPA, allergic bronchopulmonary aspergillosis; Af, Aspergillus fumigatus; CART, classification and regression tree; CF, cystic fibrosis; HAC, hierarchical ascendant classification; Ig, immunoglobulin; PCA, principal component analysis; s, specific.
References
1. Carsin A, Romain T, Ranque S, Reynaud-Gaubert M, Dubus JC, Mège JL, et al. Aspergillus fumigatus in cystic fibrosis: an update on immune interactions and molecular diagnostics in allergic bronchopulmonary aspergillosis. Allergy (2017). doi:10.1111/all.13204
2. Hinson KF, Moon AJ, Plummer NS. Broncho-pulmonary aspergillosis: a review and report of eight cases. Thorax (1952) 7:317–33. doi:10.1136/thx.7.4.317
3. Pepys J, Riddell RW, Citron KM, Clayton YM, Short EI. Clinical and immunologic significance of Aspergillus fumigatus in the sputum. Am Rev Respir Dis (1959) 80:167–80.
4. Maturu VN, Agarwal R. Prevalence of Aspergillus sensitization and ABPA in cystic fibrosis: systematic review and meta-analysis. Clin Exp Allergy (2015) 45:1765–78. doi:10.1111/cea.12595
5. Kousha M, Tadi R, Soubani AO. Pulmonary aspergillosis: a clinical review. Eur Respir Rev (2011) 20:156–74. doi:10.1183/09059180.00001011
6. Jubin V, Ranque S, Stremler Le Bel N, Sarles J, Dubus JC. Risk factors for Aspergillus colonization and allergic bronchopulmonary aspergillosis in children with cystic fibrosis. Pediatr Pulmonol (2010) 45:764–71. doi:10.1002/ppul.21240
7. Verleden GM, Dupont LJ, Van Raemdonck DE. ABPA: does it really exist after lung transplantation? J Heart Lung Transplant (2009) 28:1239. doi:10.1016/j.healun.2009.07.006
8. Fillaux J, Brémont F, Murris M, Cassaing S, Tétu L, Segonds C, et al. Aspergillus sensitization or carriage in cystic fibrosis patients. Pediatr Infect Dis J (2014) 33:680–6. doi:10.1097/INF.0000000000000231
9. Schønheyder H, Jensen T, Høiby N, Andersen P, Koch C. Frequency of Aspergillus fumigatus isolates and antibodies to Aspergillus antigens in cystic fibrosis. Acta Pathol Microbiol Immunol Scand B (1985) 93:105–12.
10. Woolnough KF, Richardson M, Newby C, Craner M, Bourne M, Monteiro W, et al. The relationship between biomarkers of fungal allergy and lung damage in asthma. Clin Exp Allergy (2017) 47:48–56. doi:10.1111/cea.12848
11. Felton TW, Roberts SA, Isalska B, Brennan S, Philips A, Whiteside S, et al. Isolation of Aspergillus species from the airway of lung transplant recipients is associated with excess mortality. J Infect (2012) 65:350–6. doi:10.1016/j.jinf.2012.07.008
12. Global Asthma Report 2014. (2014). Available from: http://www.globalasthmareport.org/ (accessed July 29, 2017).
13. Cutting GR. Cystic fibrosis genetics: from molecular understanding to clinical application. Nat Rev Genet (2015) 16:45–56. doi:10.1038/nrg3849
14. Agarwal R, Chakrabarti A, Shah A, Gupta D, Meis JF, Guleria R, et al. Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria. ABPA complicating asthma ISHAM working group. Clin Exp Allergy (2013) 43:850–73. doi:10.1111/cea.12141
15. Matricardi PM, Kleine-Tebbe J, Hoffmann HJ, Valenta R, Hilger C, Hofmaier S, et al. EAACI molecular allergology user’s guide. Pediatr Allergy Immunol (2016) (27S23):81–3. doi:10.1111/pai.12563
16. Teutschbein J, Simon S, Lother J, Springer J, Hortschansky P, Morton CO, et al. Proteomic profiling of serological responses to Aspergillus fumigatus antigens in patients with invasive aspergillosis. J Proteome Res (2016) 15:1580–91. doi:10.1021/acs.jproteome.6b00042
17. Vitte J, Romain T, Carsin A, Gouitaa M, Stremler-Le Bel N, Baravalle-Einaudi M, et al. Aspergillus fumigatus components distinguish IgE but not IgG4 profiles between fungal sensitization and allergic broncho-pulmonary aspergillosis. Allergy (2016) 71:1640–3. doi:10.1111/all.13031
20. Lê S, Josse J, Husson F. FactoMineR: an R package for multivariate analysis. J Stat Softw (2008) 25:1–18. doi:10.18637/jss.v025.i01
21. Husson F, Josse J, Pagès J. Principal Component Methods – Hierarchical Clustering – Partitional Clustering: Why Would We Need to Choose for Visualizing Data? Technical Report – Agrocampus 2010. Agro Campus Ouest, Applied Mathematics Department (2016). Available from: http://factominer.free.fr/docs/HCPC_husson_josse.pdf
22. Breiman L, Friedman JH, Olshen RA, Stone CJ. Classification and Regression Trees. Belmont, CA: Wadsworth (1984).
Keywords: allergic bronchopulmonary aspergillosis, Aspergillus fumigatus, immunoglobulin, molecular allergens, multivariate analysis
Citation: Vitte J, Ranque S, Carsin A, Gomez C, Romain T, Cassagne C, Gouitaa M, Baravalle-Einaudi M, Bel NS-L, Reynaud-Gaubert M, Dubus J-C, Mège J-L and Gaudart J (2017) Multivariate Analysis As a Support for Diagnostic Flowcharts in Allergic Bronchopulmonary Aspergillosis: A Proof-of-Concept Study. Front. Immunol. 8:1019. doi: 10.3389/fimmu.2017.01019
Received: 14 May 2017; Accepted: 08 August 2017;
Published: 22 August 2017
Edited by:
Marina I. Arleevskaya, Kazan State Medical Academy, RussiaReviewed by:
Fernanda Ferreira Cruz, Federal University of Rio de Janeiro, BrazilAnita Hilda Straus, Federal University of São Paulo, Brazil
Ashok K. Chaturvedi, University of Texas at San Antonio, United States
Copyright: © 2017 Vitte, Ranque, Carsin, Gomez, Romain, Cassagne, Gouitaa, Baravalle-Einaudi, Bel, Reynaud-Gaubert, Dubus, Mège and Gaudart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joana Vitte, jvitte@ap-hm.fr