 Ma. Natividad Flores-Castro1
Ma. Natividad Flores-Castro1 Ramcés Falfán-Valencia2
Ramcés Falfán-Valencia2 Olivia Briceño3
Olivia Briceño3 Ilse Adriana Gutiérrez-Pérez1
Ilse Adriana Gutiérrez-Pérez1 Oscar Zaragoza-García1
Oscar Zaragoza-García1 Gloria Pérez-Rubio2
Gloria Pérez-Rubio2 Cristina Morales-Martínez4
Cristina Morales-Martínez4 Iris Paola Guzmán-Guzmán1*
Iris Paola Guzmán-Guzmán1*- 1Laboratory of Multidisciplinary Research and Biomedical Innovation, Faculty of Chemical-Biological Sciences, Autonomous University of Guerrero, Chilpancingo, Mexico
- 2Pneumogenomics Laboratory, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City, Mexico
- 3Infectious Diseases Research Center, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City, Mexico
- 4Hospital IMSS-Bienestar Dr. José G. Parres, Cuernavaca, Mexico
Introduction: Interleukin-6 (IL-6) plays an important role in the pathogenesis, progression, and severity of rheumatoid arthritis (RA). High levels of IL-6 are involved in the maintenance of inflammation in the synovium and the development of new blood vessels in the inflamed synovium, contributing to pannus formation. In the present study, we aimed to investigate the relationship of IL-6 polymorphisms/ haplotypes with RA in Mexican patients and on circulating levels of IL-6 and the clinical features of the disease.
Methods: A total of 225 patients with RA and 362 healthy controls were recruited. Patients’ clinical features were collected, and inflammatory and serological parameters [anti-cyclic citrullinated peptides (anti-CCPs) and rheumatoid factor (RF)] were assessed. All subjects were genotyped for IL-6 polymorphisms (rs1800797, rs1800796, and rs1818879) using real-time polymerase chain reaction (PCR) with TaqMan probes. Circulating levels of IL-6 were measured by commercial ELISA (enzyme-linked immunosorbent assay) kits.
Results and discussion: Our results show that the GGG haplotype of the IL-6 gene is associated with a serological status of double-positive autoantibodies [odds ratio (OR) = 2.09, p = 0.009], as well as with a double-positive high autoantibodies status (OR = 2.08, p = 0.04), although a marginal association was shown to RA susceptibility (OR = 1.34, p = 0.050). Polymorphisms and haplotypes were not associated with serum levels of IL-6. However, serum levels of IL-6 ≥27.6 pg/mL were associated with clinical features of RA severity, such as morning stiffness ≥30 min (OR = 1.83, p = 0.001), HAQ-DI ≥1 (OR = 2.73, p=0.009), DAS28-ESR ≥3.2 (OR = 3.63, p = 0.002), and hsCRP ≥10 mg/L (OR = 6.35, p < 0.001). This study provides evidence of the relationship between IL-6 haplotypes, circulating levels of IL-6, and clinical features and serological status to autoantibodies in patients with RA from Mexico.
1 Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disease characterized by inflammation of synovial joints, cartilage loss, and subcondral bone erosions. During RA, the persistence of the inflammatory process, the uncontrolled immune response, synovial proliferation, disease progression, and damage to both cartilage and bone are orchestrated by proinflammatory cytokines, including interleukin-6 (IL-6) (1–3).
Some cells, such as T lymphocytes, B lymphocytes, monocytes, fibroblasts, endothelial cells, and synoviocytes, can produce and secrete IL-6 (4), and binding with its receptor (IL-6/IL-6R) activates the JAK-STAT pathway. When IL-6 binds to the soluble receptor (IL-6/sIL-6R), cell recruitment is promoted, whereas when IL-6 binds to the membrane receptor (IL-6/IL-6R), systemic inflammation is promoted by increasing the synthesis of acute phase proteins such as C-reactive protein, serum amyloid A, fibrinogen, alpha-1-antitrypsin, alpha-1-antichymotrypsin, and haptoglobin (2, 4, 5). IL-6 is also known to be a cytokine required for immunoglobulin class switching and plays an important role in acquired immune response by stimulating effector T-cell development (5–7).
Higher serum IL-6 levels have been found in patients with RA with high clinical activity and higher radiological grades and in those with functional disability (8, 9). Moreover, it has been shown that IL-6 expression might be, in part, genetically modulated by single-nucleotide polymorphisms (SNPs) in RA (1, 10). Several SNPs have been described in the IL-6 gene, which are mainly located on regulatory regions, which have been associated with the transcription of the gene with possible effects on the severity and susceptibility to develop RA (11, 12). Several SNPs have been reported on the promoter region of IL-6 located at position −597G/C (rs1800797) (13), −572G/C (rs1800796) (13–16), and −174G/C (rs1800795) (13, 15, 17, 18) in the promoter region of IL-6 and have been associated with susceptibility to RA. Interestingly, another SNP, rs1818879, located in the 3′ untranslated region (UTR), has been associated with chronic inflammatory and autoimmune diseases, such as multiple sclerosis (19), but it has not been studied in RA.
Recent research focused on IL-6 SNPs has shown that specific haplotypes are associated with susceptibility to RA. On a Turkish cohort of patients with RA, the GG haplotype (rs1800795 and rs2069837) (20) and the haplotype GCCGCT (rs1800797, rs1800796, rs1800795, rs1524107, rs2069840, and rs1474347) in a Chinese RA cohort have been reported to be associated with RA susceptibility (13), but not another clinical characteristic in RA; however, these susceptibility results differed between populations. The present study analyzed the role of IL-6 SNPs rs1800797, rs1800796, and rs1818879 and haplotypes with the susceptibility to RA, as well as the relationship of circulating levels of IL-6 with serological and inflammatory markers in a Mexican population with RA.
2 Materials and methods
2.1 Study population
A case–control study was conducted among patients with RA (n = 225, including both women and men). The diagnosis of patients with RA was based on the ACR/EULAR criteria 2010 (21). Participants were recruited from December 2017 to December 2020 at the Department of Internal Medicine from Hospital IMSS-Bienestar Dr. Raymundo Abarca Alarcón in Guerrero, Mexico. A general population group of 362 participants was considered, consisting of healthy controls from samples taken from the open population with no history of RA, autoimmune, musculoskeletal, or infectious diseases to determine the association with RA. The study was approved by the Research Committee Ethics of the Autonomous University of Guerrero, Mexico (approval code CB-004/2017). All participants signed a written informed consent.
2.2 Sociodemographic and clinical data
Demographic, clinical information, and antirheumatic treatment data were gathered from all patients during consultations and from their medical records. Clinical characteristics, such as morning stiffness, and tender and swollen joint count, were assessed. Furthermore, functional disability was evaluated using HAQ-DI (Health Assessment Questionnaire); a HAQ-DI score ≥1 denoted disability presence.
The Disease Activity Score in 28 joints with erythrocyte sedimentation rate (DAS28-ESR) were assessed. The scores for DAS28-ESR were categorized as follows: >5.1, ≥3.2 to ≤5.1, ≥2.6 to <3.2, and <2.6, representing high, moderate, low disease activity, and remission, respectively. Also, the joint damage was assessed using radiographs from hands, classifying the Sharp–van der Heijde (SvH) score into five categories: 0 = normal; 1 = asymmetrical or minimal narrowing up to a maximum of 25%; 2 = definite narrowing with loss of up to 50% of the normal space; 3 = definite narrowing with loss of 50%–99% of the normal space or subluxation; and, 4 = absence of joint space, presumptive evidence of ankylosis, or complete luxation.
The standard treatments were mainly methotrexate, received orally, in combination with chloroquine and corticosteroids (Cs) such as prednisone and non-steroidal anti-inflammatory drugs (NSAIDs); this study does not include patients treated with biological agents.
2.3 Serological status and inflammatory markers
Blood samples were collected after 8 h of overnight fasting via venipuncture and transferred to tubes with and without a clot activator. An erythrocyte sediment rate (ESR) test was performed using the Wintrobe method. The quantification of high-sensitivity C-reactive protein (hsCRP) and rheumatoid factor (RF) was evaluated by the immunoturbidimetry method, according to the manufacturer’s instructions (COBAS C311, Roche Diagnostics GmbH, Germany). IgG isotype antibodies against citrullinated peptides (anti-CCPs) were determined using an ELISA (enzyme-linked immunosorbent assay) commercial kit (DIASTAT anti-CCP Axis-Shield, Dundee, United Kingdom) following the manufacturer’s specifications and the Multiskan FC Microplaque Photometer automated plate reader (Thermo Scientific, Shanghai). Elevated levels of hsCRP were considered ≥10 mg/L; RF positive when >20 IU/mL; anti-CCPs positive when >5 U/mL; RF high when >60 IU/L; anti-CCPs high when >30 U/mL; double-positive autoantibodies when RF levels exceeded 20 IU/mL and anti-CCPs exceeded 5 U/mL; and double-positive high autoantibodies when RF levels exceeded 60 IU/mL and anti-CCPs exceeded 30 U/mL.
2.4 DNA extraction and TaqMan genotyping
Genomic DNA was extracted from peripheral blood, and SNPs were genotyped by allele discrimination using commercial TaqMan probes (Applied Biosystems, San Francisco, CA, USA). The analyzed SNPs included rs1800797/promoter, −597G/A (C_1839695_20), rs1800796/promoter, −572G/C (C_11326893_10), and rs1818879/3′UTR G/A (C_26518729_10), all of which are listed under the catalog number 4351379. These were evaluated with quantitative polymerase chain reaction (qPCR) on a 7300 Real-Time PCR System (Applied Biosystems/Thermo Fisher Scientific Inc., Singapore), following the manufacturer’s instructions. Amplifications were conducted under the following cycling conditions: one cycle at 60°C for 30 s, 95°C for 10 min; 40 cycles at 95°C for 15 s and 60°C for 1 min; and, finally, 60°C for 30 s. Genotype analysis was conducted using the sequence detection software in StepOne™ version 2.3 software (Applied Biosystems, CA, USA).
2.5 Determination of circulating levels of IL-6
Circulating levels of IL-6 were measured using a specific sandwich ELISA method (BioLegend Max™, Inc. San Diego, CA, USA, cat. 430507), following the manufacturer’s instructions on an automatized equipment Multiskan Go (Thermo Scientific, Finland). The absorbance was read at 450 nm using a standard curve, and IL-6 levels were quantified. The detection sensitivity for IL-6 was 1.6 pg/mL. In this study, IL-6 values were categorized as follows: low (<10.6 pg/mL), middle (10.6 to 27.29 pg/mL), and high (≥27.3 pg/mL), based on cutoff tertiles from the data of our cohort.
2.6 Statistical analysis
The categorical variables were expressed as proportions and compared using the chi-squared test. Nonparametric quantitative variables were presented with medians and 5th–95th percentiles. IL-6 SNP-allele frequencies were calculated, and the Hardy–Weinberg equilibrium (HWE) exact test (estimation of P value) was performed for each group of participants (cases and controls) using STATA version 16 software. Differences in genotypes and allele frequencies between populations were measured using the chi-square test.
Genotype, allele, and haplotype frequencies for IL-6 SNPs (rs1800797, rs1800796, and rs1818879) were estimated using the SHEsis online software (22). To analyze linkage disequilibrium (LD) between SNPs, we calculated Lewontin’s D′ value using the SHEsis program, as well as the association between the haplotypes, RA susceptibility, clinical, and serological parameters.
The association between high levels of IL-6 with clinical and serological parameters was assessed with a logistic regression model adjusted for age, sex, and therapy scheme combined, providing odds ratios (ORs) and 95% confidence intervals (95% CI). Data analysis was performed using STATA version 16 (StataCorp, College Station, TX, USA) and GraphPad Prism v.8.4 (GraphPad Software, San Diego, CA, USA). In this study, values of p < 0.05 were considered statistically significant.
3 Results
3.1 Participant characteristics
The median age of the participants was 46 years for the RA group and 50 years for the control group. Ninety-two percent of our cohort was composed of women on the RA arm and 94% on the control group (Table 1). When analyzing the patients with RA, the median time since RA diagnosis was 6 years, with a morning stiffness median of 10 min, an HAQ-DI score of 0.21, a DAS28-ESR of 3.12, and an SvH score of 2. The levels of RF, anti-CCPs, and ESR were high on average. The median levels of hsCRP were 6.34 mg/L, and the median circulating levels of IL-6 were 15.90 pg/mL. All patients present an antirheumatic scheme with disease-modifying antirheumatic drugs (DMARDs) in monotherapy or combination (Table 1).
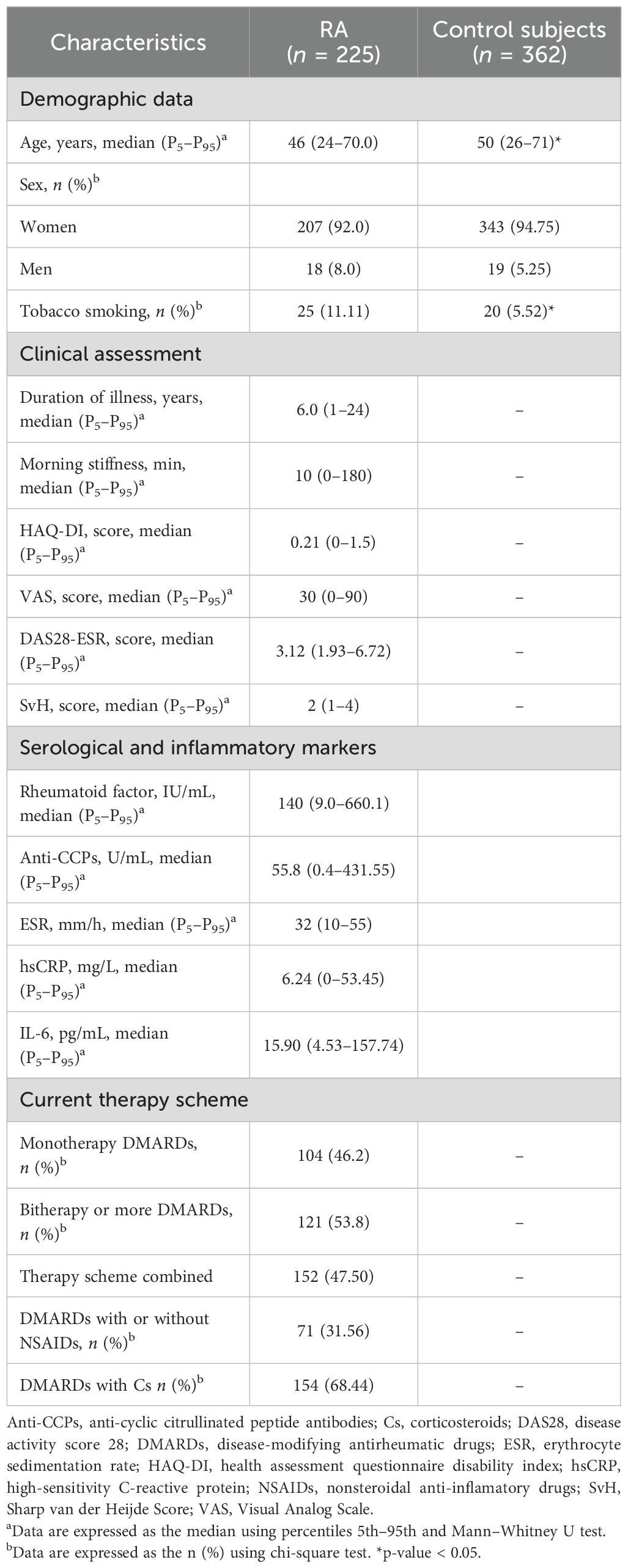
Table 1. Demographic, clinical, and treatment characteristics in patients with RA.
3.2 IL-6 polymorphisms and haplotype and their contribution to RA susceptibility
The distribution of genotypic and allelic frequencies of the three investigated SNPs is presented in Table 2. The genotypes and alleles of the SNPs were not associated with an increased risk of developing the disease in our cohort. However, the GG haplotype (rs1800797/rs1818879) was associated with the susceptibility to RA (OR = 1.34, 95% CI, 1.01–1.79, p = 0.03), while the GGG haplotype showed a trend toward RA susceptibility without reaching significance (OR = 1.34, 95% CI, 0.99–1.80, p = 0.05) (Table 3).
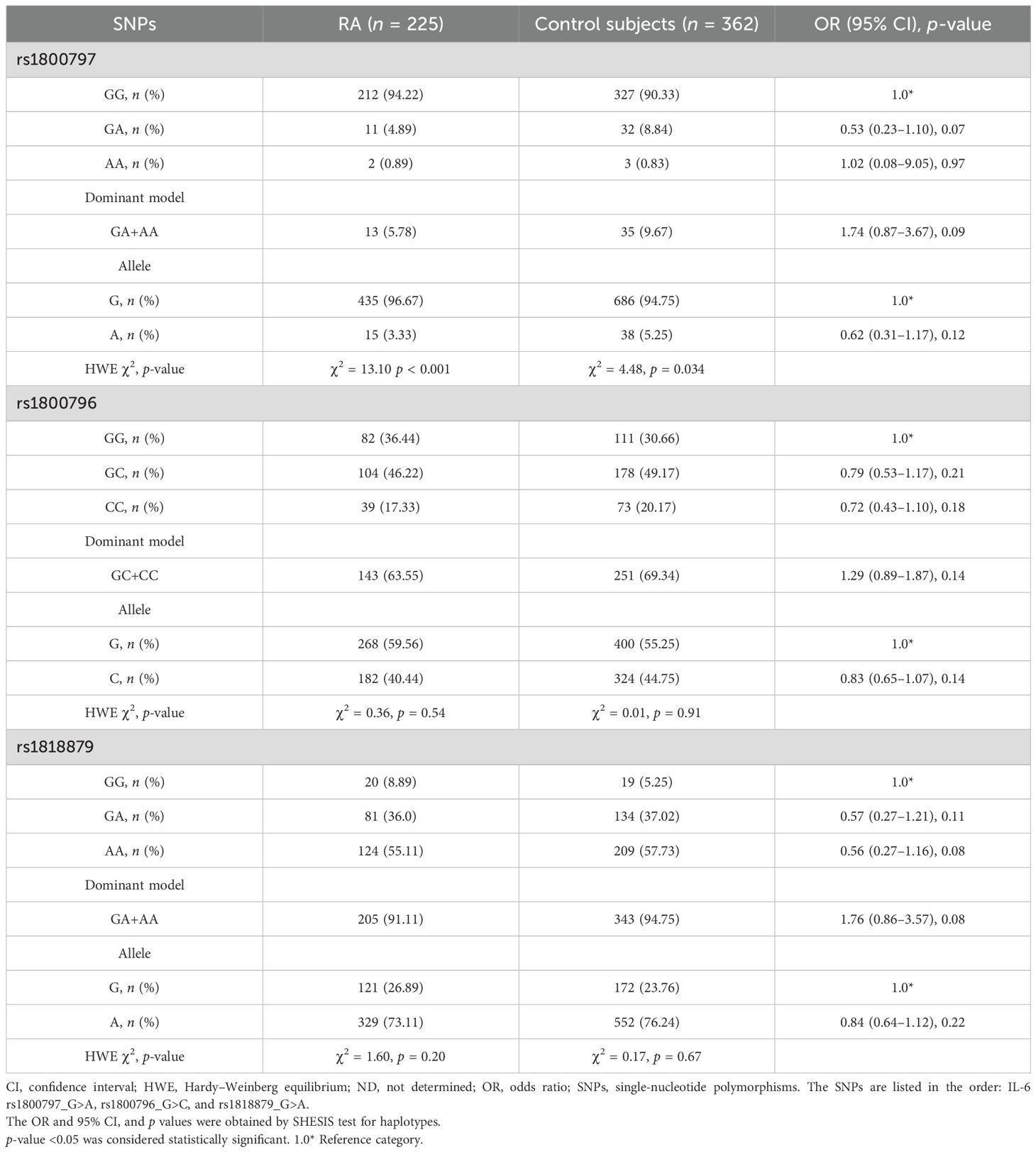
Table 2. Genotype and allele frequencies of polymorphisms in IL-6 gene.
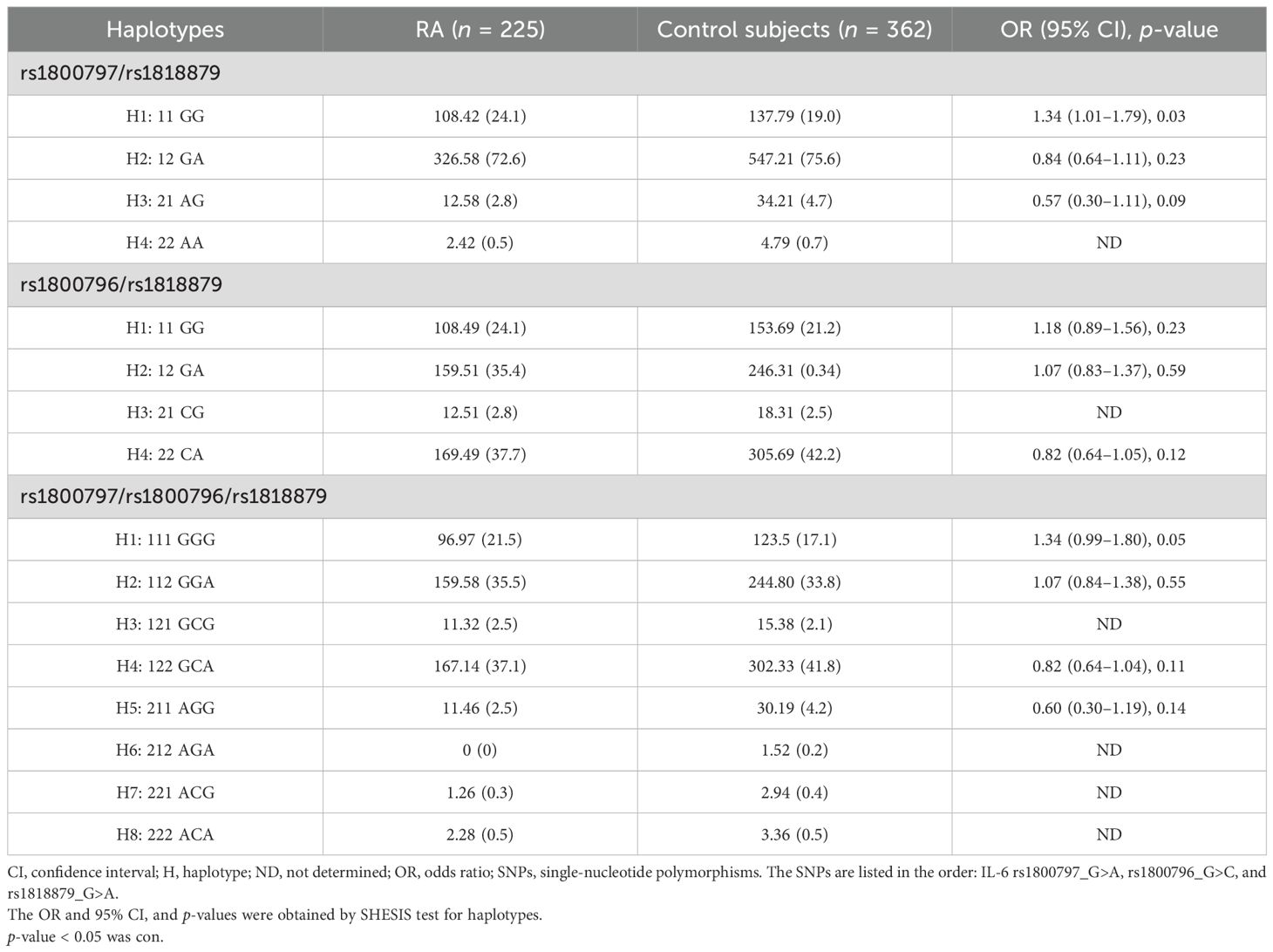
Table 3. Haplotype frequencies of polymorphisms in IL-6 gene.
LD analysis revealed a high level of linkage in patients with RA (Supplementary Figure S1A) between the rs1800797-rs1818879 and rs1800796-rs1818879 polymorphisms, while these SNPs were not linked in control subjects (Supplementary Figure S1B); this suggests a potential disease-causing allele linked to a specific haplotype in the patients with RA from our population. Individually, the SNPs did not correlate with increased serum IL-6 levels (Supplementary Figures S2A–C).
3.3 Association between circulating levels of IL-6 and clinical parameters in RA
In order to explore the relationship of IL-6 concentrations on the clinical and serological parameters of patients with RA, we reclassify the cohort on individual with low, middle, or high levels of IL-6 according to the IL-6 tertiles found in our cohort. The patients with RA with high levels of IL-6 (≥27.3 pg/mL) showed a longer morning stiffness time (p = 0.003), a higher functional disability score (p = 0.009), greater clinical activity (p < 0.001), and an increased number of tender and swelling joints (all p < 0.001); furthermore, they had higher levels of ESR (p = 0.006), hsCRP (p < 0.001), and RF (p = 0.033) (Table 4).
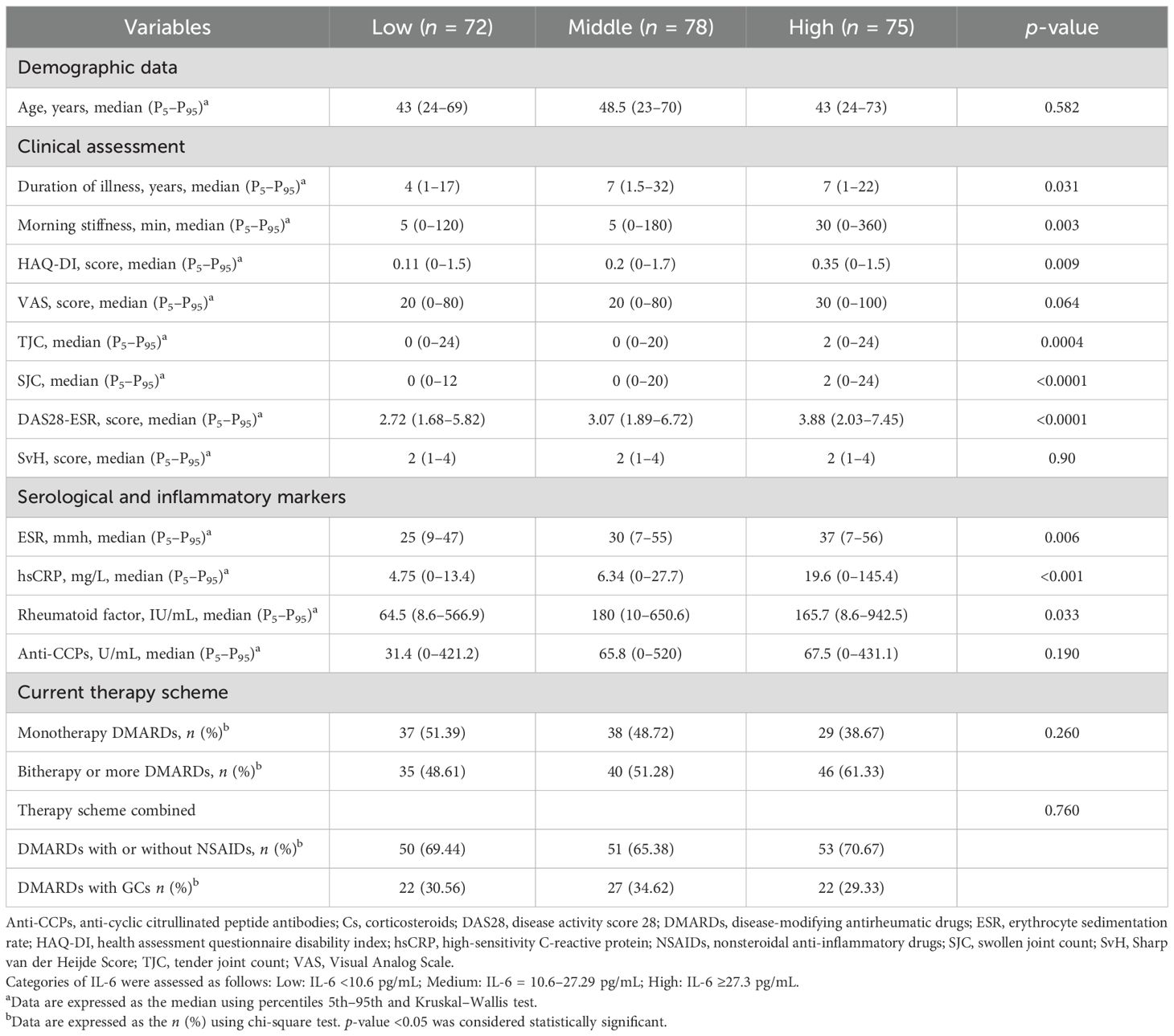
Table 4. Clinical, serological, and therapy characteristics according to IL-6 tertile.
In addition, we analyzed the proportion of patients with RA with clinical and serological parameters predictive of severity of the disease, in relation to IL-6 tertile values, finding a significantly higher proportion of patients in the high tertile of IL-6 with morning stiffness >30 min (p < 0.01), functional disability defined by HAQ-DI ≥1 (p < 0.05), moderate–high clinical activity (p < 0.01), hsCRP ≥10 mg/L (p < 0.05), and double-positive (RF+/Anti-CCPs+) high autoantibodies (p < 0.05) (Figure 1).
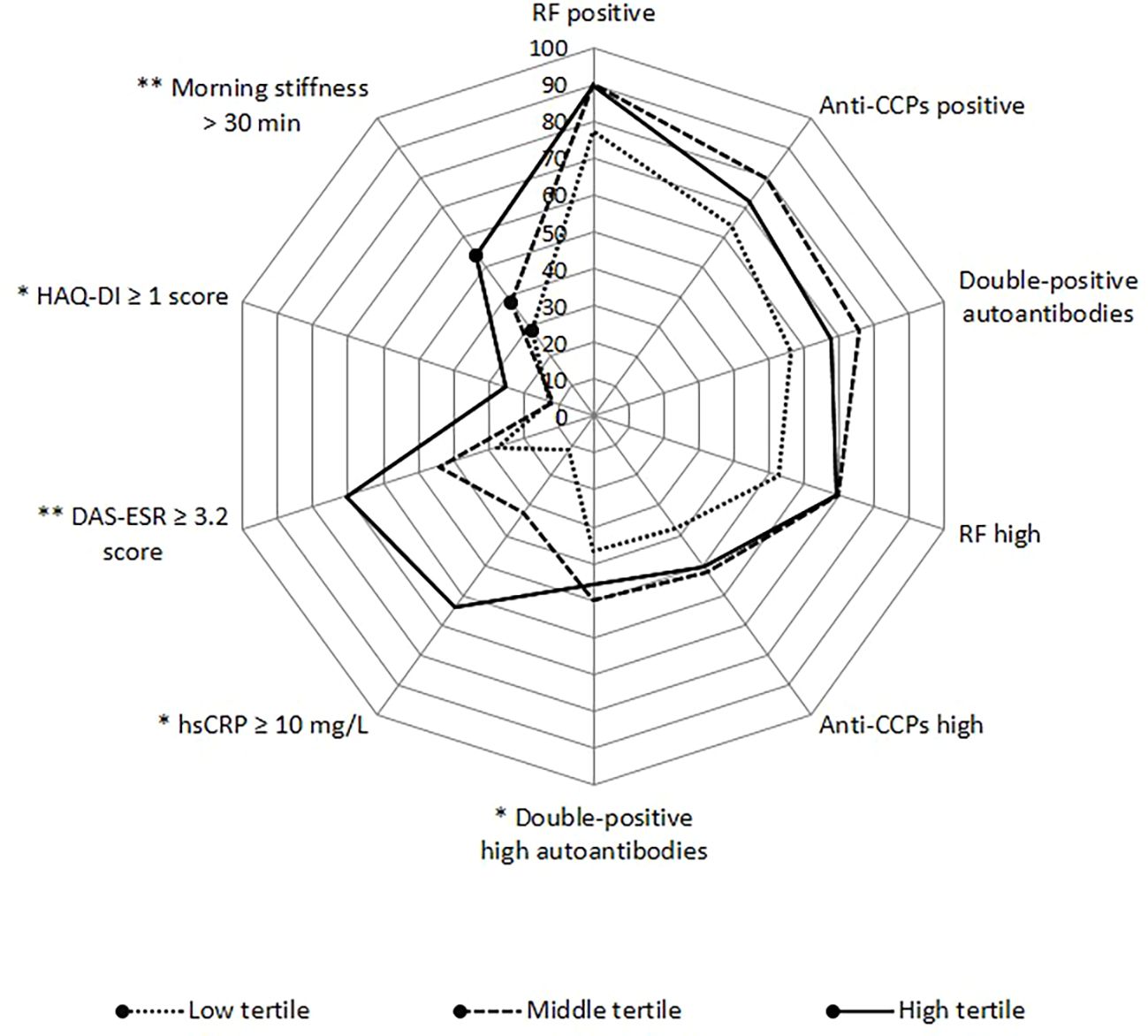
Figure 1. Proportion of serological and clinical alterations according to IL-6 tertiles. Anti-CCPs, anti-cyclic citrullinated peptide antibodies; DAS28, disease activity score 28; ESR, erythrocyte sedimentation rate; HAQ-DI, health assessment questionnaire disability index; hsCRP, high-sensitivity C-reactive protein; RF, rheumatoid factor. Categories: RF positive >20 IU/mL; Anti-CCPs positive >5 IU/mL; RF high >60 IU/mL; Anti-CCPs high >30 IU/mL; double-positive autoantibodies when levels were RF >20 IU/mL and anti-CCPs >5 IU/mL; double-positive high autoantibodies when levels were RF >60 IU/mL and anti-CCPs >30 IU/mL. Low tertile: IL-6 <10.6 pg/mL; medium tertile: IL-6 = 10.6–27.29 pg/mL; high tertile: IL-6 ≥27.3 pg/mL. *p-value < 0.05, **p-value < 0.01.
3.4 IL-6 haplotype and circulating levels of IL-6 in relation to severity parameters in RA
We explore the ORs associated with the severity parameters or poor prognosis of RA in individuals with the GG and GGG haplotypes with the highest circulating levels. The GG haplotype (rs1800797/rs1818879) was not associated with severity parameters or poor prognosis of RA and serum levels of IL-6. However, the GGG haplotype of the IL-6 gene shows significant association with serologic status for double-positive autoantibodies, including RF+/anti-CCPs+ (OR = 2.09, 95% CI, 1.18–3.68, p = 0.009). It is also associated with high anti-CCPs+ levels (OR = 1.61, 95% CI, 1.02–2.54, p = 0.03) and with the double-positive high autoantibodies’ serologic status (OR = 2.08, 95% CI, 0.99–4.36, p = 0.04) (Figure 2A).
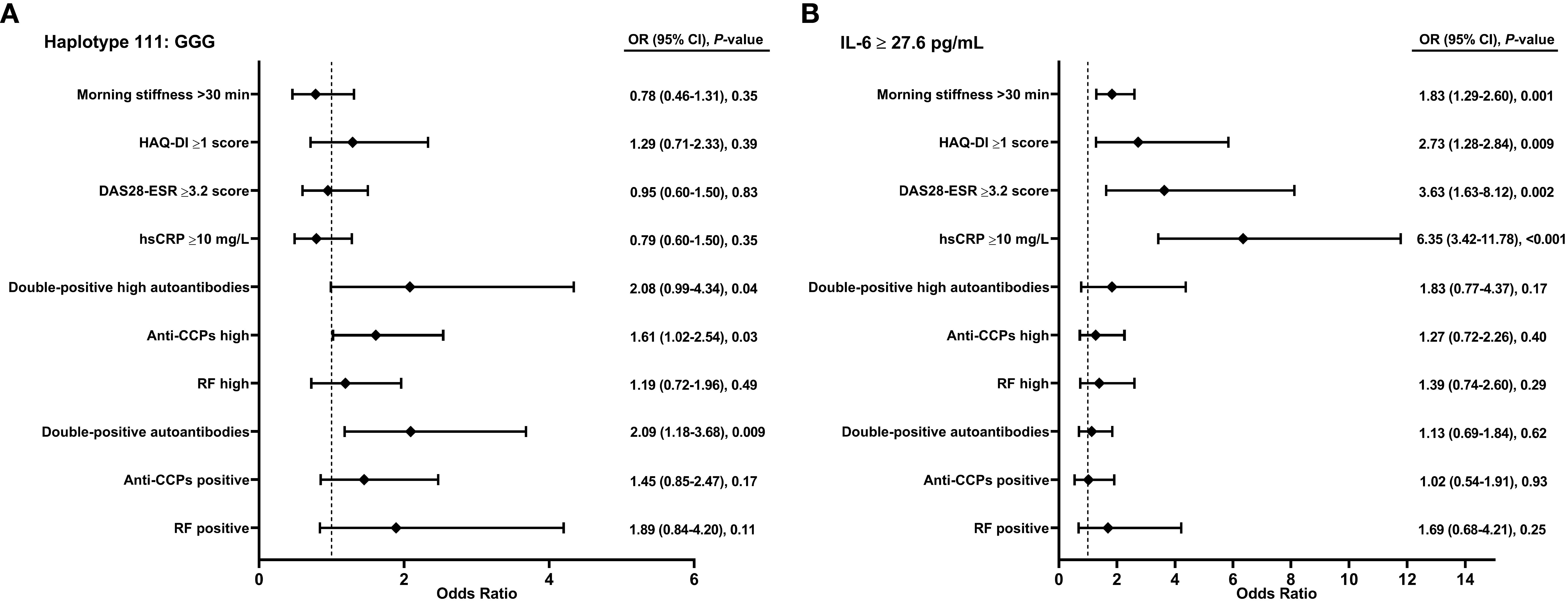
Figure 2. Association of haplotype and circulating levels of IL-6 on severity in patients with RA. (A) Haplotype. (B) Circulating levels of IL-6. Anti-CCPs, anti-cyclic citrullinated peptide antibodies; DAS28, disease activity score 28; ESR, erythrocyte sedimentation rate; HAQ-DI, health assessment questionnaire disability index; hsCRP, high-sensitivity C-reactive protein; RA, rheumatoid arthritis; RF, rheumatoid factor. Categories: RF positive >20 IU/mL; Anti-CCPs positive >5 U/mL; RF high >60 IU/mL; Anti-CCPs high >30 U/mL; double-positive autoantibodies when levels were RF >20 IU/mL and anti-CCPs >5 U/mL; double-positive high autoantibodies when levels were RF >60 IU/mL and anti-CCPs >30 U/mL. Figure (A) Odds ratio of univariate model. Figure (B) Odds ratio of multivariate model adjusted by age, sex, and therapy scheme combined. p-value < 0.05 was considered significant.
In an adjusted multivariate analysis accounting for age, sex, and therapy scheme, high circulating levels of IL-6 (≥27.3 pg/mL) are associated with increased susceptibility to morning stiffness ≥30 min (OR = 1.83, 95% CI, 1.29–2.60, p = 0.001), HAQ-DI ≥1 (OR = 2.73, 95% CI, 1.28–2.84, p = 0.009), DAS28-ESR ≥3.2 (OR = 3.63, 95% CI, 1.63–8.12, p = 0.002), and hsCRP ≥10 mg/L (OR = 6.36, 95% CI, 3.42–11.78, p < 0.001) (Figure 2B).
4 Discussion
We analyzed the role of three IL-6 SNPs and haplotypes on the susceptibility to develop RA and on the main clinical features on individuals diagnosed with RA. We found that haplotype GGG is associated with serological status to autoantibodies; furthermore, it suggests a role in susceptibility to RA, while the circulating levels of IL-6 are linked to features related to severity and poor prognosis in patients with RA.
Previous studies have reported that the SNPs rs1800797 (13) and rs1800796 (13–16) in the promoter region of the IL-6 gene are associated with susceptibility to RA. However, the association of rs1800796 SNP with RA has not been established in populations from Turkey (23), Egypt (24), and Mexico (Mexican mestizo population) (25).
In a meta-analysis involving populations from Asia, the Middle East, Eastern Europe, Western Europe, and Latin America (15), the rs1800797 SNP was not linked to increased risk of developing RA. Similarly, in this study, individual SNPs did not show association with RA susceptibility, but the rs1800797 and rs1818879 SNPs, as well as the rs1800796 and rs1818879 SNPs, were found to be in strong LD. Likewise, other populations have reported high association between the SNPs rs1800797 and rs1818879 (26). The connection between these SNPs, despite their distant locations, could be explained by the formation of a loop that facilitates interaction between the promoter region (loci of the SNPs rs1800797 and rs1800796) and the 3′UTR region (rs1818879) of the IL-6 gene (27, 28).
In Turkish patients with RA, the GG haplotype (rs1800795 and rs2069837) (20) and the haplotype GCCGCT (rs1800797, rs1800796, rs1800795, rs1524107, rs2069840, and rs1474347) in Chinese patients with RA have been reported to be strongly associated with RA susceptibility (13). In the present study, the GG haplotype (rs1800797 and rs1818879) was associated, while the GGG haplotype (rs1800797, rs1800796, and rs1818879) showed a marginal association. It is important to consider that the Mexican population has a mestizo background; thus, ethnicity could potentially be a factor related to the variability in RA development. Some studies suggest that the Amerindian component in the Mexican population may play a role in susceptibility to RA (29).
The GGG haplotype was significantly associated with double-positive autoantibodies’ status (RF+/Anti-CCPs+) and double-positive high autoantibodies’ serologic status. A possible explanation of these findings is that SNPs could influence the expression of IL-6 (1, 10). IL-6 plays a key role as a regulator of both T-cell migration and activation, as well as B lymphocytes’ maturation into long-lived plasma cells, which is crucial in producing autoantibodies such as RF and anti-CCP (30). Furthermore, it has been shown that fibroblast-like synoviocytes (FLS) express CD40L and IL-6, while other studies suggest that the mechanism of FLS-dependent B-cell activation is subject to the involvement of both CD40L and IL-6, indicating that this cytokine participates in autoantibody production in RA (31, 32). Previous studies have demonstrated that patients with RA who are double-positive for autoantibodies (RF and anti-CCPs) have significantly higher IL-6 levels compared to seronegative patients or those positive for only a single autoantibody (33).
In the present study, circulating levels of IL-6 were not associated with individual SNPs or haplotypes, possibly because SNP rs1818879 does not participate directly in IL-6 synthesis although it has an indirect influence on IL-6 levels by binding to other SNPs located in the gene promoter region. Furthermore, it is important to consider that there are post-transcriptional and post-translational mechanisms that could be regulating the levels of the cytokine. For example, in the complementary chain of the IL-6 gene, the IL-6-AS1 gene is transcribed, the product of which is a long non-coding RNA that acts as an endogenous competitor to regulate IL-6 expression (28). On the other hand, soluble glycoprotein 130 (sgp130) acts as an antagonist of the trans-signaling mechanism by binding to the IL-6:sIL6R complex (34). Additionally, given that all patients in this study received anti-rheumatic therapy, we raise the possibility that treatment could mask the relationship between SNPs and circulating levels of IL-6.
Patients with RA treated with sulfasalazine experience a significant decrease in IL-6 levels, and this reduction in IL-6 is linked to improvements in clinical and laboratory measures of disease activity. This suggests that sulfasalazine may partly exert its disease-modifying effect by suppressing cytokine production (35). Additionally, in patients with RA with newly diagnosed disease and after 3 months of methotrexate treatment, radiological damage progression was correlated with IL-6 levels (36). In RA treatment, IL-6 blockade has become a first-line option, showing significantly greater clinical efficacy in patients who do not respond to conventional antirheumatic therapy or even to less conventional treatments. This indicated that IL-6-targeted drugs may reduce the burden of immune-inflammatory disease in a larger proportion of patients (37). However, in this study, monotherapy or combination therapies of antirheumatic drugs were not associated with circulating levels of IL-6.
According to circulating levels of IL-6 in this study, the median reported was similar to that reported in other studies on RA populations (38, 39), while others reported higher levels of circulating levels of IL-6 in patients with RA (8, 9, 40, 41). Several studies have found an association between IL-6 levels with clinical, serological, inflammatory, and biochemical markers in patients with RA (8, 9, 38–40). In the same way, we found a relationship between circulating levels of IL-6 and severity-related characteristics in patients with RA, such as morning stiffness, functional disability, moderate clinical activity, and higher levels of hsCRP. Symptoms like morning stiffness, pain, and functional disability could be linked to a peak in serum cortisol during the early morning hours in patients with RA who maintain elevated IL-6 levels (42). IL-6 acts on FLS, promoting their growth, increasing their survival, and modulating the synthesis of chemokines and matrix metalloproteinases (MMPs) (43); it also described that IL-6 can influence the differentiation and survival of osteoclasts, which express matrix metalloproteinase 3 (MMP-3); thus, osteoclasts induced by IL-6 may be involved in the joint destruction of RA (44). This partially explains the observed relationship with morning stiffness >30 min and HAQ-DI scores of 1 or higher, which may be linked to joint damage. IL-6 levels have been proposed as a marker of progression in bone and joint destruction during early RA stages (45). It has also been shown that progressive joint destruction tissue damage and persistent synovial inflammation lead to functional disability (46). IL-6 is involved not only in bone metabolism but also in immune response, hematopoiesis, and inflammation, and has been correlated with RA’s clinical activity and severity (47). As seen in our study, a DAS28-ESR score of 3.2 or higher was associated with high circulating levels of IL-6, similar to findings in other studies within the RA population (8, 9, 38–40).
Finally, in this study, elevated hsCRP levels ≥10 mg/L were associated with a high tertile of IL-6. Similarly, Boyapati et al. (48) reported that US patients with RA in the high tertile of IL-6 (64.7 pg/mL) had elevated CRP levels, moderately higher clinical disease activity at baseline, and greater joint damage. Furthermore, Zeb et al. (9) reported that, in Pakistani patients with RA, higher IL-6 levels correlated with CRP and disease severity. IL-6 directly promotes CRP synthesis through the binding of IL-6 to its receptor (IL-6R) on the hepatocyte membrane, activating the JAK-STAT pathway (2, 5). Furthermore, the exacerbated production of CRP in synovial tissue by FLS could be through the mechanism associated with CD32/64-p38 activation and NF-kB signaling (49), which further aggravates the inflammatory process in RA.
Other mechanisms related to IL-6 regulation could be related to the trans-presentation process, where circulating IL-6 binds to the membrane receptor of dendritic cells (IL-6Rα) and subsequently the IL-6/IL-6Rα complex binds to gp130 expressed on CD4+ T cells and forms a gp130 homodimer, activating signaling JAK. This interaction is necessary for the generation of Th17 cells (2). Furthermore, a computational model revealed that IL-6 and IL-17 (interleukin-17) signaling promotes the formation of the STAT3–NF-kB complex, followed by its binding to the promoter regions of NF-kB target genes to accelerate inflammatory responses, including IL-6 production (50).
4.1 Strengths and limitations
This study demonstrates the association of a new haplotype with serological status in RA. However, the results found should be interpreted with caution, as this study only included patients from southern Mexico. Furthermore, using other methods such as eQLT identification from different tissues and cell types, as well as implementing an in silico analysis, would allow us to better understand how the IL-6 gene and genetic variants influence susceptibility to RA or circulating levels of IL-6, as well as the molecular mechanisms of IL-6 related to inflammation and immune regulation.
5 Conclusion
In conclusion, the GGG haplotype of the IL-6 gene is linked to double-positive high autoantibodies, while elevated circulating levels of IL-6 are connected to clinical severity features in Mexican patients with RA. Additional studies are necessary to clarify the mechanism behind the SNPs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was approved by Research Committe Ethics of the Autonomous University of Guerrero Mexico (approval code CB-004/2017). The study were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MF-C: Formal Analysis, Investigation, Methodology, Writing – original draft. RF-V: Methodology, Writing – review & editing. OB: Methodology, Writing – review & editing. IG-P: Investigation, Methodology, Writing – original draft. OZ-G: Investigation, Methodology, Writing – original draft. GP-R: Writing – review & editing. CM-M: Methodology, Writing – review & editing. IG-G: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We thank the patients for their generosity in taking part in the study. Special thanks to the rheumatologist. José Eduardo Navarro-Zarza, who contributed to the management and approach to of these patients.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2025.1679644/full#supplementary-material
References
1. Krishna Priya EK, Srinivas L, Rajesh S, Sasikala K, and Banerjee M. Pro-inflammatory cytokine response pre-dominates inmuno-genetic pathway in development of rheumatoid arthritis. Mol Biol Rep. (2020) 47:8669–77. doi: 10.007/s11033-020-05909-2
2. Kondo N, Kuroda T, and Kobayashi D. Cytokine networks in the pathogenesis of rheumatoid arthritis. Int J Mol Sci. (2021) 22:10922. doi: 10.3390/ijms222010922
3. Mueller AL, Payandeh Z, Mohammadkhani N, Mubarak SMH, Zakeri A, Alagheband Bahrami A, et al. Recent advances in understanding the pathogenesis of rheumatoid arthritis: new treatment strategies. Cells. (2021) 10:3017. doi: 10.3390/cells10113017
4. Kishimoto T. Interleukin-6: from basic science to medicine–40 years in immunology. Annu Rev Immunol. (2005) 23:1–21. doi: 10.1146/annurev.immunol.23.021704.115806
5. Castell JV, Gomez-Lechon MJ, David M, Hirano T, Kishimoto T, and Heinrich PC. Recombinant human interleukin-6 (IL-6/BSF-2/HSF) regulates the synthesis of acute phase proteins in human hepatocytes. FEBS Lett. (1988) 232:347–50. doi: 10.1016/5793(88)80766-x
6. Srirangan S and Choy EH. The role of interleukin 6 in the pathophysiology of rheumatoid arthritis. Ther Adv Musculoskelet Dis. (2010) 2:247–56. doi: 10.1177/1759720X10378372
7. Tanaka T, Narazaki M, and Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. (2014) 6:a016295. doi: 10.1101/cshperspect.a016295
8. Roghani SA, Shamsi A, Jalili C, Jalili F, Lotfi R, Garman N, et al. Interleukin-6 positively correlates with cardiovascular disease predictor algorithms and biomarker in rheumatoid arthritis patients. J Cell Mol Med. (2024) 28:e70028. doi: 10.1111/jcmm.70028
9. Zeb S, Khan Z, Ashraf, Javaid M, Rumman, Swati MAA, et al. Relationship between serum interleukin-6 levels, systemic immune-inflammation index, and other biomarkers across different rheumatoid arthritis severity levels. Cureus. (2024) 16:e72334. doi: 10.7759/cureus.72334
10. You CG, Li XJ, Li YM, Wang LP, Li FF, Guo XL, et al. Association analysis of single nucleotide polymorphisms of proinflammatory cytokine and their receptors genes with rheumatoid arthritis in northwest Chinese Han population. Cytokine. (2013) 61:133–8. doi: 10.1016/j.cyto.2012.09.007
11. Rego PI, Fernández M, and Blanco FJ. Gene polymorphisms and pharmacogenetics in rheumatoid arthritis. Curr Genomics. (2008) 9:381–93. doi: 10.2174/138920208785699553
12. Padyukov L. Genetics of rheumatoid arthritis. Semin Immunopathol. (2022) 44:47–62. doi: 10.1007/s00281-022-00912-0
13. Li F, Xu J, Zheng J, Sokolove J, Zhu K, Zhang Y, et al. Association between interleukin-6 gene polymorphisms and rheumatoid arthritis in Chinese Han population: a case-control study and a meta-analysis. Sci Rep. (2014) 4:5714. doi: 10.1038/srep05714
14. Zhang C, Jiao S, Li T, Zhao L, and Chen H. Relationship between polymorphisms in -572G/C interleukin 6 promoter gene polymorphisms (rs1800796) and risk of rheumatoid arthritis: A meta-analysis. Int J Rheum Dis. (2020) 23:47–54. doi: 10.1111/1756-185X.13729
15. Pacheco-Soto BT, Porchia LM, Lara-Vazquez WC, Torres-Rasgado E, Perez-Fuentes R, and Gonzalez-Mejia ME. The association between interleukin-6 promoter polymorphisms and rheumatoid arthritis by ethnicity: A meta-analysis of 33 studies. Rheumatol Clin (Engl Ed). (2021) 17:447–55. doi: 10.1016/j.reumae.2020.03.003
16. Chen J, Zhang A, Yang Y, Si Y, and Hao D. Assessment of interleukin 6 gene polymorphisms with rheumatoid arthritis. Gene. (2021) 10:765. doi: 10.1016/j.gene.2020.145070
17. Harun-Or-Roshid M, Mollah MNH, and Jesmin. A comprehensive meta-analysis comprising 149 case-control studies to investigate the association between IL-6 gene rs1800795 polymorphism and multiple disease risk. Gene. (2023) 861:147234. doi: 10.1016/j.gene.2023.147234
18. Hao X, Zhao H, Zhu L, Li Z, Yang J, and Bai Q. Inflammatory factor Interleukin-6 and its correlation with rheumatoid arthritis: A meta-analysis. Heliyon. (2024) 10:e39472. doi: 10.1016/j.heliyon.2024.e39472
19. Bruno A, Dolcetti E, Azzolini F, Moscatelli A, Gambardella S, Ferese R, et al. Interleukin 6 SNP rs1818879 regulates radiological and inflammatory activity in multiple sclerosis. Genes (Basel). (2022) 13:897. doi: 10.3390/genes13050897
20. Yucel B, Sumer C, Gok I, Karkucak M, Alemdaroglu E, and Ucar F. Associations between cytokine gene polymorphisms and rheumatoid arthritis in Turkish population. North Clin Istanb. (2020) 7:563–71. doi: 10.14744/nci.2020.70845
21. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumatol. (2010) 62:2569–81. doi: 10.1002/art.27584
22. Shi YY and He L. SHEsis, a powerful software platform for analyses of linkage disequilibrium, haplotype construction, and genetic association at polymorphism loci. Cell Res. (2005) 15:97–8. doi: 10.1038/sj.cr.729027
23. Arman A, Coker A, Sarioz O, Inanc N, and Direskeneli H. Lack of association between IL-6 gene polymorphisms and rheumatoid arthritis in Turkish population. Rheumatol Int. (2012) 32:2199–201. doi: 10.1007/s00296-011-2057-x
24. Amr K, El-Awady R, and Raslan H. Assessment of the -174G/C (rs1800795) and -572G/C (rs1800796) interleukin 6 gene polymorphisms in Egyptian patients with rheumatoid arthritis. Open Access Maced J Med Sci. (2016) 4:574–7. doi: 10.3889/oamjms.2016.110
25. Zavaleta-Muñiz SA, Martín-Márquez BT, Gonzalez-López L, Gonzalez-Montoya NG, Díaz-Toscano ML, Ponce-Guarneros JM, et al. The -174G/C and -572G/C interleukin 6 promoter gene polymorphisms in mexican patients with rheumatoid arthritis: a case-control study. Clin Dev Immunol. (2013) 2013:959084. doi: 10.1155/2013/959084
26. Qi L, van Dam RM, Meigs JB, Manson JE, Hunter D, and Hu FB. Genetic variation in IL6 gene and type 2 diabetes: tagging-SNP haplotype analysis in large-scale case-control study and meta-analysis. Hum Mol Genet. (2006) 15:1914–20. doi: 10.1093/hmg/ddl113
27. Kämäräinen OP, Solovieva S, Vehmas T, Luoma K, Riihimäki H, Ala-Kokko L, et al. Common interleukin-6 promoter variants associate with the more severe forms of distal interphalangeal osteoarthritis. Arthritis Res Ther. (2008) 10:R21. doi: 10.1186/ar2374
28. Yi E, Zhang J, Zheng M, Zhang Y, Liang C, Hao B, et al. Long noncoding RNA IL6-AS1 is highly expressed in chronic obstructive pulmonary disease and is associated with interleukin 6 by targeting miR-149-5p and early B-cell factor 1. Clin Transl Med. (2021) 11:e479. doi: 10.1002/ctm2.479
29. Díaz-Peña R, Quiñones LA, Castro-Santos P, Durán J, and Lucia A. Latin american genes: the great forgotten in rheumatoid arthritis. J Pers Med. (2020) 10:196. doi: 10.3390/jpm10040196
30. Hernández-Flores D and Valor L. IL-6: su papel en la patogenia de la artritis reumatoide. Consecuencias clínicas. Reumatol Clínica. (2018) 14:7–10.
31. Cerutti A, Zan H, Schaffer A, Bergsagel L, Harindranath N, Max EE, et al. CD40 ligand and appropriate cytokines induce switching to IgG, IgA, and IgE and coordinated germinal center and plasmacytoid phenotypic differentiation in a human monoclonal IgM+IgD+ B cell line. J Immunol. (1998) 160:2145–57. doi: 10.4049/jimmunol.160.5.2145
32. Bleck D, Loacker-Schöch K, Classen T, Jose J, Schneider M, and Pongratz G. Fibroblast-like synoviocytes preferentially induce terminal differentiation of IgD+ memory B cells instead of naïve B cells. Immunology. (2024) 173:520–35. doi: 10.1111/imm.13840
33. Sokolove J, Johnson DS, Lahey LJ, Wagner CA, Cheng D, Thiele GM, et al. Rheumatoid factor as a potentiator of anti-citrullinated protein antibody-mediated inflammation in rheumatoid arthritis. Arthritis Rheumatol. (2014) 66:813–21. doi: 10.1002/art.38307
34. Bonomi A, Veglia F, Baldassarre D, Strawbridge RJ, Golabkesh Z, Sennblad B, et al. Analysis of the genetic variants associated with circulating levels of sgp130. Results from the IMPROVE study. Genes Immun. (2020) 21:100–8. doi: 10.1038/s41435-019-0090-z
35. Danis VA, Franic GM, Rathjen DA, Laurent RM, and Brooks PM. Circulating cytokine levels in patients with rheumatoid arthritis: results of a double blind trial with sulphasalazine. Ann Rheum Dis. (1992) 51:946–50. doi: 10.1136/ard.51.8.946
36. Nishina N, Kaneko Y, Kameda H, Kuwana M, and Takeuchi T. Reduction of plasma IL-6 but not TNF-α by methotrexate in patients with early rheumatoid arthritis: a potential biomarker for radiographic progression. Clin Rheumatol. (2013) 32:1661–6. doi: 10.1007/s10067-013-2309-0
37. Kim GW, Lee NR, Pi RH, Lim YS, Lee YM, Lee JM, et al. IL-6 inhibitors for treatment of rheumatoid arthritis: past, present, and future. Arch Pharm Res. (2015) 38:575–84. doi: 10.1007/s12272-015-0569-8
38. Abel Meguid MH, Hamad YH, Swilam RS, and Barakat MS. Relation of interleukin-6 in rheumatoid arthritis patients to systemic bone loss and structural bone damage. Rheumatol Int. (2013) 33:697–703. doi: 10.1007/s00296-012-2375-7
39. Tekeoğlu İ, Harman H, Sağ S, Altındiş M, Kamanlı A, and Nas K. Levels of serum pentraxin 3, IL-6, fetuin A and insulin in patients with rheumatoid arthritis. Cytokine. (2016) 83:171–5. doi: 10.1016/j.cyto.2016.04.009
40. Warjukar PR, Mohabey AV, Jain PB, and Bandre GR. Decoding the correlation between inflammatory response marker interleukin-6 (IL-6) and C-reactive protein (CRP) with disease activity in rheumatoid arthritis. Cureus. (2024) 16:e62954. doi: 10.7759/cureus.62954
41. Xue M, Lin H, Lynch T, Bereza-Malcom L, Sinnathurai P, Thomas R, et al. Exploring the association between circulating endothelial protein C receptor and disease activity of rheumatoid arthritis in a pilot study. Rheumatol Adv Pract. (2024) 8:rkae096. doi: 10.1093/rap/rkae096
42. Straub RH and Cutolo M. Circadian rhythms in rheumatoid arthritis: implications for pathophysiology and therapeutic management. Arthritis Rheum. (2007) 56:399–408. doi: 10.1002/art.22368
43. Pablos Álvarez JL. Interleukin 6 in the physiopathology of rheumatoid arthritis. Reumatol Clin. (2009) 5:34–9. doi: 10.1016/S1699-258X(09)70203-7
44. Yokota K. Osteoclast differentiation in rheumatoid arthritis. Immunol Med. (2024) 47:6–11. doi: 10.1080/25785826.2023.2220931
45. Saeki Y, Kudo-Tanaka E, Ohshima S, Matsushita M, Tsuji S, Maeda Y, et al. Baseline anti-citrullinated peptide antibody (ACPA) titers and serum interleukin-6 (IL-6) levels possibly predict progression of bone destruction in early stages of rheumatoid arthritis (ERA). Rheumatol Int. (2013) 33:451–6. doi: 10.1007/s00296-012-2397-1
46. Figueroa Pedrosa MM. Evaluación del daño radiográfico en la artritis reumatoide. Rev Española Reumatol. (2002) 1:22–6.
47. Pandolfi F, Franza L, Carusi V, Altamura S, Andriollo G, and Nucera E. Interleukin-6 in rheumatoid arthritis. Int J Mol Sci. (2020) 21:5238. doi: 10.3390/ijms21155238
48. Boyapati A, Schwartzman S, Msihid J, Choy E, Genovese MC, Burmester GR, et al. Association of high serum interleukin-6 levels with severe progression of rheumatoid arthritis and increased treatment response differentiating sarilumab from adalimumab or methotrexate in a post hoc analysis. Arthritis Rheumatol. (2020) 72:1456–66. doi: 10.1002/art.41299
49. Fang Z, Lv J, Wang J, Qin Q, He J, Wang M, et al. C-reactive protein promotes the activation of fibroblast-like synoviocytes from patients with rheumatoid arthritis. Front Immunol. (2020) 11:958. doi: 10.3389/fimmu.2020.00958
Keywords: IL-6, haplotype, clinical activity, serological status, rheumatoid arthritis
Citation: Flores-Castro MN, Falfán-Valencia R, Briceño O, Gutiérrez-Pérez IA, Zaragoza-García O, Pérez-Rubio G, Morales-Martínez C and Guzmán-Guzmán IP (2025) Interleukin-6 levels and their haplotypes are associated with serological autoantibodies status and clinical activity in rheumatoid arthritis. Front. Immunol. 16:1679644. doi: 10.3389/fimmu.2025.1679644
Received: 04 August 2025; Accepted: 21 October 2025;
Published: 06 November 2025.
Edited by:
Giorgio Biasiotto, University of Brescia, ItalyReviewed by:
Ryan Dos Costa, Federal University of Bahia (UFBA), BrazilJ. Jesmin, University of Dhaka, Bangladesh
Copyright © 2025 Flores-Castro, Falfán-Valencia, Briceño, Gutiérrez-Pérez, Zaragoza-García, Pérez-Rubio, Morales-Martínez and Guzmán-Guzmán. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Iris Paola Guzmán-Guzmán, cGFvX25raWxsZXJAeWFob28uY29tLm14