Severe Influenza With Invasive Pulmonary Aspergillosis in Immunocompetent Hosts: A Retrospective Cohort Study
 Yishan Duan
Yishan Duan Xinyan Ou2
Xinyan Ou2 - 1Department of Respiratory Medicine, Sichuan University West China Hospital, Chengdu, China
- 2College of Computer Science, Chongqing University, Chongqing, China
Background: Influenza was an independent risk factor for invasive pulmonary aspergillosis (IPA). In light of increasing incidence and mortality of influenza associated aspergillosis, our study summarized risk factors, clinical characteristics, and prognostic factors of developing aspergillosis in immunocompetent hosts with influenza to further screen high-risk population and improve outcome.
Methods: We reviewed the patient characteristics, laboratory examinations, radiological imaging, and microbiology data of 72 influenza patients with IPA and 84 influenza patients without IPA admitted to West China Hospital.
Result: Our study shown that aspergillosis co-infection increased overall mortality of severe influenza from 22.6 to 52.8%, along with higher white blood count (WBC) (10.9 ± 5.0 vs. 8.4 ± 3.3, P = 0.016), Neutrophiles (9.5 ± 5.0 vs. 7.0 ± 3.8, P = 0.023), procalcitonin (PCT) (8.6 ± 15.9 vs. 1.2 ± 2.1, P = 0.009), and a lower CD4+ T cell count (189.2 ± 135.3 vs. 367.1 ± 280.0, P = 0.022) in death group. No impact of age, gender, underlying diseases, immunosuppressive agents and steroids use, CD4+ T cell count on incidence of influenza associated aspergillosis was observed. But influenza associated aspergillosis cases mostly accompanied with more H1N1 subtype (91.7 vs. 79.8%, P = 0.037) and higher level of C-reactive protein (CRP) (117.6 ± 88.1 vs. 78.5 ± 75.2, P = 0.017) and interleukin 6 (IL-6) (133.5 ± 149.2 vs. 69.9 ± 100.0, P = 0.021) than those without aspergillosis.
Conclusion: Aspergillosis co-infection in severe influenza patients can lead to a significant increased mortality, which was associated with severe respiratory failure due to mixed infection and immunosuppression. Pulmonary excessive inflammatory response was related with IPA co-infection.
Introduction
Increasing aspergillosis co-infection have been reported as a common complication of severe influenza and became an important cause of increased mortality among severe influenza patients in recent years (1–7). A sharp increase in reported cases occurred after the 2009 H1N1 influenza pandemic and 128 influenza associated aspergillosis cases have been published up to June 2018 in literature review of cases and case series (6), and the incidence rate of invasive pulmonary aspergillosis (IPA) reached up to 19% in the setting of severe influenza (3). With a deeper understanding of invasive fungal diseases (IFDs), the updated and revised definitions of IFDs expanded host factors for probable IFDs and new criteria for proven IFDs is applicable to patients even without host factors (8). Significant increased aspergillosis co-infection in the setting of severe influenza suggested that severe influenza was probably one of host factors. The bigger point is that the occurrence of IPA among severe influenza patients usually entails a poorer prognosis. The overall mortality of influenza associated aspergillosis reported in systematic reviews fluctuated between 40 and 60%, which was generally thought to be much higher than mortality of severe influenza patients with other co-infections or without co-infections (1, 3, 5, 6).
IPA typically occurs in immunocompromised hosts. But majority of reported influenza associated aspergillosis cases did not have classic host factors for IPA and influenza was observed to be independently associated with IPA in various studies (5, 6, 9, 10). Glucocorticoids was generally considered to be an important cause of aspergillus co-infection in patients with severe influenza, as glucocorticoids was frequently used in severe influenza patients with septic shock or acute respiratory distress syndrome (ARDS) (11, 12). Moreover, male sex, age, and comorbidities (including cancer, chronic obstructive pulmonary disease (COPD), severe hepatic insufficiency, and renal failure) have also been reported as risk factors for aspergillosis co-infection and were likely associated with increased mortality of aspergillosis group in some studies with small sample sizes (1, 2, 4, 6, 13). However, many young patients without underlying disease and glucocorticoid use were observed to develop IPA in the setting of severe influenza. There are still controversies in potential risk factors of developing IPA in the setting of severe influenza because the sample sizes of researches on these issues were too small. Moreover, there was still lack of detailed studies on target clinical manifestations, imaging features, and poor prognosis of influenza associated aspergillosis.
Our study enrolled a total of 156 severe influenza patients, systematically and comprehensively analyzed differences in patient characteristics, clinical features, and outcome parameters between severe influenza patients with and without aspergillosis. Besides, we also attempt to conduct risk evaluation of poor prognosis among influenza associated aspergillosis cases and explore the impact of clinical diagnosis and treatment on outcomes of influenza associated aspergillosis to identify the better diagnostic and management strategy.
Methods
Study Population
Our study consisted of 72 patients diagnosed with severe influenza with IPA in West China Hospital of Sichuan University from December 2018 to March 2019, and 84 severe influenza patients in the same period matched by age and gender. Among them, 75 patients were admitted to Intensive Care Unit (ICU), 81 patients were admitted to respiratory department or infectious diseases department. Patients < 18 years were excluded.
Definition of Severe Influenza
Diagnostic criteria for influenza include clinical symptoms of influenza and at least one positive assay for the following pathogens detection: real time polymerase chain reaction; viral isolation; viral antigen detection (1).
Severe influenza refers to patients with symptoms of lower respiratory tract infection or severe complications (pneumonia, septic shock, multiple organ dysfunction, and so on) (14, 15).
Diagnosis of IPA
The IPA diagnostic criteria consists of host factors, clinical features, and mycological evidence on the basis of EORTC/MSG criteria (16). Consensus that influenza was independently associated with IPA has been reached in previous studies and autopsy series of severe influenza indicated that strict interpretation of the host factors for IPA contributed to missed diagnosis of IPA (17, 18), so we used a modified EORTC/MSG criteria in which no specific host factor was required (1). Clinical features included new infiltrates on the chest X-ray or computed tomography (CT) scan, as well as clinical symptoms including fever or dyspnea, hemoptysis, and/or wheezing. Mycological evidence included positive aspergillus cultivation, galactomannan (GM) antigen detected in serum (i.e., ≥0.5) or bronchoalveolar lavage fluid (BAL, optical density ≥ 1.0) (3, 16). According to EORTC/MSG criteria, patients were classified into three types of IPA (proven IPA, probable IPA, and possible IPA) (16). In order to fully exclude aspergillus colonization, both clinical symptoms and new infiltrates in pulmonary imaging are required for patients with only positive culture for aspergillus (19). All the IPA diagnosis was ultimately made by two senior respiratory physicians on basis of comprehensive consideration of clinical symptoms, imaging findings, and microbial evidence.
Data Collection
Data were recorded from medical records among all cases, including demographics, underlying diseases, immunosuppressive agents and steroids use, cumulative doses of steroids. Besides, the initial clinical symptoms and outcome parameters (oxygenation index, respiratory support method, ICU admission, and mortality) were also included into our study. Moreover, we reviewed laboratory examinations, radiological imaging (pulmonary X-ray/CT), microbiology data (bacterial, fungus, and viral examinations) during hospitalization. The lung imaging findings were divided into four patterns: consolidation, ground-glass opacity (GGO), nodular, and cavity sign (20, 21). (If there were more than two types abnormal imaging patterns in pulmonary X-ray/CT, the major one should be selected as the main imaging characteristic).
Statistical Analysis
The analysis was performed with SPSS 24.0 (SPSS Inc., Chicago, IL, USA). Qualitative variables were expressed as counts and frequencies and quantitative variables were expressed as means and standard deviations. For qualitative variables, we chose to use Fisher's exact test or χ2 test depending on data. Quantitative variables were compared by t-test and ranked data was analyzed by Wilcoxon rank-sum tests or Spearman correlation test. In this study, P ≤ 0.05 was considered as statistically significant.
Results
From December 2018 to March 2019, 156 patients were diagnosed with severe influenza infection in West China Hospital of Sichuan University, of which 72 patients matched our IPA definition. Biopsies is necessary for Proven IPA. All patients in our study lacked biopsy examination due to severe illness, so all IPA cases in our study belonged to probable IPA or possible IPA. All the data of severe influenza patients with and without aspergillosis co-infection are summarized in Table 1.
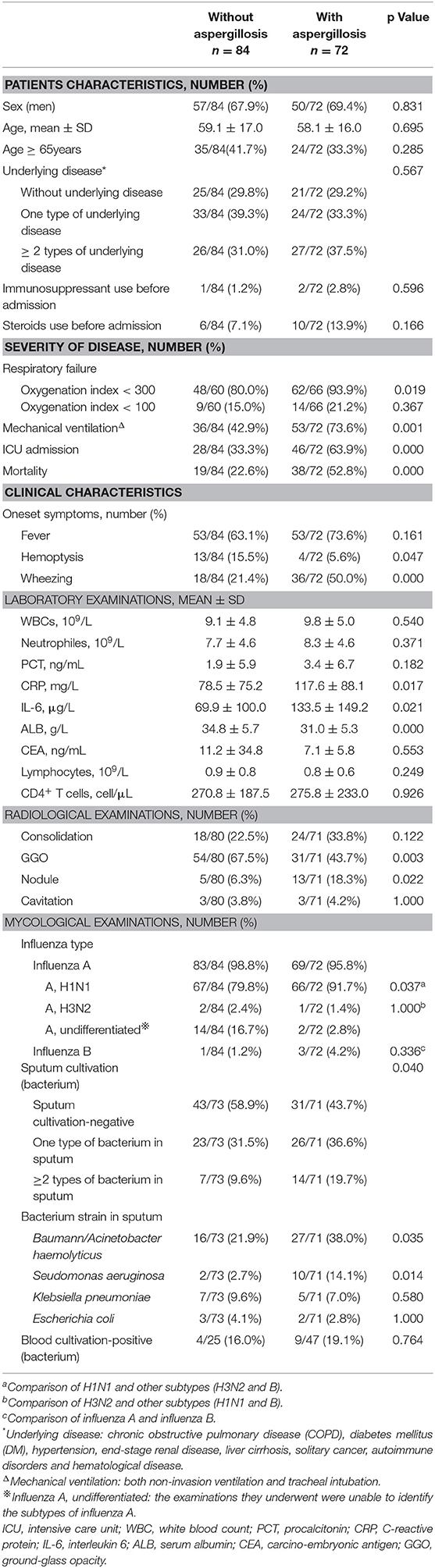
Table 1. Comparisons between severe influenza patients with and without aspergillosis.
Clinical Characteristics of Severe Influenza Patients With and Without Aspergillosis
No significant differences were observed in terms of age, male sex, underlying diseases, immunosuppressive agents, and steroids use prior to hospitalization between severe influenza patients with and without aspergillosis (P > 0.05).
Fever was the main symptom of severe influenza, but no difference was observed in patients with and without aspergillosis in term of fever (63.1 vs. 73.6%, P = 0.161). More wheezing was detected in patients with aspergillosis than those without it (50.0 vs. 21.4%, P = 0.000). More patients with hemoptysis were found in patients with influenza alone (15.5 vs. 5.6%, P = 0.047).
Both serum CRP level (117.6 ± 88.1 vs. 78.5 ± 75.2, P = 0.017) and IL-6 level (133.5 ± 149.2 vs. 69.9 ± 100.0, P = 0.021) of severe influenza patients with aspergillosis were greatly higher than those without aspergillosis. However, serum PCT level, WBC, and Neutrophile count were not found to be different between two groups. Moreover, the aspergillosis group had a significant lower ALB level (34.8 ± 5.7 vs. 31.0 ± 5.3, P = 0.000) than patients with influenza alone.
GGO pattern was the most common abnormal pulmonary imaging characteristic and patients with influenza alone presented with GGO pattern (67.5 vs. 43.7%, P = 0.003) more often than those with aspergillosis. Compared to pulmonary imaging characteristics of patients with influenza alone, more nodule pattern (18.3 vs. 6.3%, P = 0.022) were observed in patients with aspergillosis.
Influenza A was the most common influenza subtype identified in both patients with and without aspergillosis. More H1N1 was shown in severe influenza patients with aspergillosis than those without aspergillosis (91.7 vs. 79.8%, P = 0.037).
The overall distribution of bacterium in sputum was different between the two groups (P = 0.040). Among severe influenza patients with aspergillosis, Baumann/Acinetobacter haemolyticus (38.0%) was the bacterium most frequent identified in sputum, followed by Pseudomonas aeruginosa (14.1%) and Klebsiella pneumoniae (7.0%). As for severe influenza patients without aspergillosis, Baumann/Acinetobacter haemolyticus (21.9%), Klebsiella pneumoniae (9.6%), and Esecherichia coli (4.1%) were the three most common bacteria identified in sputum. The result of bacteria species distribution in sputum showed that more Baumann/Acinetobacter haemolyticus (38.0 vs. 21.9%, P = 0.035) and Seudomonas aeruginosa (14.1 vs. 2.7%, P = 0.014) were shown in patients with aspergillosis. The result of blood bacterial cultivation showed that Baumann/Acinetobacter haemolyticus was the most common bacteria species identified in both patients with aspergillosis (8.7%) and patients with influenza alone (8.0%) (Supplementary Materials).
Comparison of Outcome Parameters in Severe Influenza Patients With and Without Aspergillosis
Compared with patients without aspergillosis, more patients with type I respiratory failure (oxygenation index < 300) were observed in severe influenza with aspergillosis (80.0 vs. 93.9%, P = 0.019). Severe influenza patient with aspergillosis required mechanical ventilation (both non-invasion ventilation and tracheal intubation) (73.6 vs. 42.9%, P = 0.001) and ICU admission (63.9 vs. 33.3%, P = 0.000) more often than did patients without it. Moreover, patients with aspergillosis following influenza had a significantly higher mortality than those without it (52.8 vs. 22.6%, P = 0.000).
Prognostic Factors of Severe Influenza Patients With Aspergillosis
Thirty-four patients (47.2%) were alive and 38 patients (52.8%) had died among influenza associated aspergillosis cases. In order to find out factors related with poor prognosis of influenza associated aspergillosis cases, we further divided aspergillosis group into death group and survive group. Result showed more patients with oxygenation index < 100 were observed in death group than survive group (31.6 vs. 7.1%, P = 0.016). The rates of mechanical ventilation (92.1 vs. 52.9%, P = 0.000) and ICU admission (89.5 vs. 35.3%, P = 0.000) in death group were significantly higher than survive group.
No difference in terms of age, gender, underlying diseases, immunosuppressive agents and steroids use was observed between death group and survive group (Table 2). A significantly reduction of CD4+ T cells count were observed in death group (189.2 ± 135.3 vs. 367.1 ± 280.0, P = 0.022). Further subgroup analysis revealed a significantly higher mortality in aspergillosis group with CD4+ T cells count < 200 cell/μL (60.7 vs. 30.6%, P = 0.023) (Supplementary Materials). A higher serum WBCs (10.9 ± 5.0 vs. 8.4 ± 3.3, P = 0.016), Neutrophiles (9.5 ± 5.0 vs. 7.0 ± 3.8, P = 0.023) and PCT (8.6 ± 15.9 vs. 1.2 ± 2.1, P = 0.009) level were observed in death group than survive group. Moreover, patients in dead group had a lower ALB level (29.7 ± 5.3 vs. 32.4 ± 4.9, P = 0.025) and higher CEA level (10.7 ± 6.8 vs. 4.3 ± 2.7, P = 0.008) than those alive.
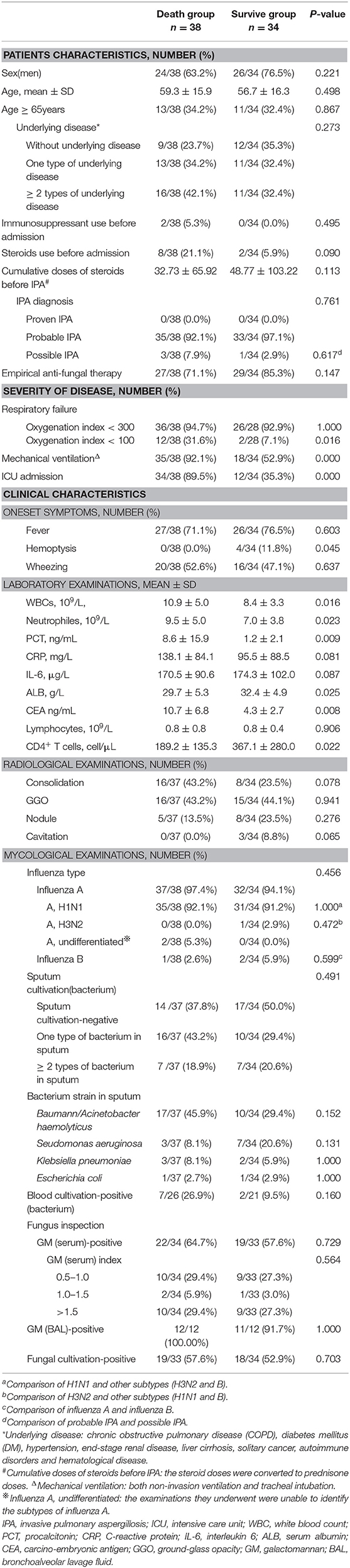
Table 2. Comparison between death group and survive group in severe influenza with aspergillosis.
Pulmonary radiological examinations showed no significant difference between death group and survive group (Table 2). Bowman/Acinetobacter haemolyticus was the most frequent bacterium isolated in both sputum (17/37, 45.9%) and blood (3/26, 11.5%) in death group. No differences in the positive detection rate of GM test (serum and BAL) and fungal cultivation were observed between the death and survive group. Our data did not show obvious correlation between serum GM index and mortality in severe influenza patients with aspergillosis (Table 2).
Discussion
Analysis of clinical data of severe influenza patients showed that there were no significant correlation between patient characteristics (including age, gender, underlying diseases, immunosuppressive agents, and steroids use) and the incidence and mortality of influenza associated aspergillosis. H1N1 was the major influenza subtype of severe influenza patients with aspergillosis, and patients with more serious inflammatory response and respiratory failure were observed in influenza associated aspergillosis. Aspergillosis co-infection following severe influenza could lead to a significant increase in mortality, which was associated with more severe bacterial infection, respiratory failure, as well as poorer immunity and nutritional status.
Contrary to previous researches (1, 3–5), we did not find the poor baseline characteristic of patients and decreased CD4+ T cells count followed by influenza had any impact on the occurrence of aspergillosis co-infection. But severe influenza patients with aspergillosis mostly belonged to the H1N1 category and accompanied with higher inflammatory level represented by CRP and IL-6. These data suggested an association between aspergillus invasion and influenza virus infection. Although the pathogenesis of aspergillosis in the setting of severe influenza have not to be defined yet, it is generally recognized that influenza may promote IPA via breakdown of bronchial mucosa and disruption of mucociliary clearance (22), which was related with increased risk of aspergillosis. In comparison with seasonal influenza virus, H1N1 virus causes more damage to the airway epithelial cells (21). But much more importantly, the pulmonary severe inflammatory response induced by influenza invasion played a more crucial role in pathogenesis of aspergillosis co-infection and also was the major cause of ARDS in severe influenza patients. A biphasic immunological response to severe infection (an early hyper-inflammatory phase followed by an anti-inflammatory response, leading to a hypo-inflammatory state, which is called compensatory anti-inflammatory response syndrome) was reported to make immunocompetent hosts vulnerable to bacteria and fungi co-infection (23). IL-6 and CRP were the synthesis of pro-inflammatory cytokines released from the epithelial cells invaded by influenza and resulted in further alveolar damage according to enhance phagocytosis of immune cells and activate a series of innate immunoresponses (24, 25). The significant up-regulated IL-6 and CRP level were observed in severe influenza (especially H1N1category) and were linked to severe tissue and organ damage and to the likelihood of developing more severe clinical manifestations, respiratory failure and complications, as well as poorer outcome (26). Our data also showed rapidly increased secretion of IL-6 and CRP in severe influenza patients with aspergillosis than those with influenza alone. These suggested that the occurrence of aspergillosis co-infection was related with influenza virus attacks and resulting pulmonary excessive inflammatory response in immunocompetent hosts.
Bacterial superinfection was generally considered to be related to a higher incidence and mortality of influenza associated aspergillosis (27). Our result also revealed increased bacterial infection indicators (e.g., WBC, Neutrophiles counts, and PCT) in both severe influenza patients with and without aspergillosis. Further analysis indicated no impact of bacterial infection on the incidence of influenza associated aspergillosis. But a higher level of bacterial infection (represented by WBC, Neutrophiles counts, and PCT level on admission) accompanied by a lower oxygenation index was observed to be associated with higher mortality of these severe influenza patients with aspergillosis. As we known, viral infection can result in a decreased CD4+ T cells, which actually plays an essential role in the defense against fungal infections (5). All the patients in our study had no history of immunodeficiency before admission, so decreased CD4+ T cells count was regarded as a subsequent change of viral infection. Although decreased CD4+ T cells in severe influenza patients was thought to be associated with aspergillus infection in a study with small sample (28), our data do not support the association between decreased CD4+ T cells and the occurrence of influenza associated aspergillosis. But reduction of CD4+ T cells was proved to be associated with higher mortality of severe influenza patients with aspergillosis, especially in patients with CD4+ T cells count < 200 cell/μL. In our study, IPA co-infection increased overall mortality of severe influenza patients from 22.64 to 52.78%. Based on previous studies and our data, we considered that the high mortality of severe influenza associated aspergillosis was mainly related with severe respiratory failure secondary to mixed infection (including viral, bacteria, and aspergillosis) and failure to recovery of immunologic dissonance induced by viral invasion.
In our study, 77.27% diagnosis of IPA co-infection was confirmed within 3 days after influenza diagnosis. Therefore, it is essential to emphasize positive searching for evidence of fungal co-infections in early stage. Severe influenza with IPA in immunocompetent hosts did not have classical radiographic findings (e.g., cavitary lesions, halo, or crescent) (1, 9, 20), the most important clinical diagnosis method of IPA still depends on fungal screening, including GM tests and fungal cultivation. Compared with serum GM test sensitivity of 33% among IPA patients in ICU without classical host risk factors (29), our data suggested that serum GM tests of influenza associated aspergillus cases revealed superior performance with positive rate of 61.2%. So serum GM test can be recommended as an active monitoring method for severe influenza patients at high risk of fungal co-infection, especially for patients unable to obtain BAL GM test due to serious illness or primary hospitals without condition to conduct bronchoalveolar lavage examination. Serum GM test would be particularly important to provide proof for early diagnosis.
Conclusion
Aspergillosis co-infection in severe influenza patients can lead to a significant increased mortality, and the high mortality was associated severe respiratory failure secondary to mixed infection (including viral, bacteria, and aspergillosis). Active and effective controlling infection, improving immunity, and nutrition status were the key to lowering the morality of influenza associated aspergillosis. Aspergillus co-infection in severe influenza patients was related with influenza subtype and excessive pulmonary inflammatory response, but had no relation with age, gender, underlying diseases, CD4+ T cells count, immunosuppressive agents, and steroids use. Therefore, for all severe influenza patients with suspicious fungal signs and symptoms, clinicians should take initiative to search for microbiological evidence to avoid delayed and missed diagnosis of aspergillosis co-infection.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author/s.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements. Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
YSD made substantial contributions to the study design, data acquisition, analysis, or interpretation and drafting the final manuscript. XMO designed the study. YSC, XYO, and BML contributed to the data collection and completed the statistical analysis. All authors read and approved the final manuscript.
Funding
This work was supported by the National Science Foundation of China (Grants No. 31671189) and the Sichuan Science and Technology Agency (Grants No. 2018SZ0109).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2020.602732/full#supplementary-material
References
1. Ku YH, Chan KS, Yang CC, Tan CK, Chuang YC, Yu WL. Higher mortality of severe influenza patients with probable aspergillosis than those with and without other coinfections. J Formos Med Assoc. (2017) 116:660–70. doi: 10.1016/j.jfma.2017.06002
2. van de Veerdonk FL, Kolwijck E, Lestrade PP, Hodiamont CJ, Rijnders BJ, van Paassen J, et al. Influenza-Associated Aspergillosis in Critically Ill Patients. Am J Respir Crit Care Med. (2017) 196:524–7. doi: 10.1164/rccm201612-2540LE
3. Schauwvlieghe A, Rijnders BJA, Philips N, Verwijs R, Vanderbeke L, Van Tienen C, et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med. (2018) 6:782–92. doi: 10.1016/s2213-2600(18)30274-1
4. Crum-Cianflone NF. Invasive aspergillosis associated with severe influenza infections. Open Forum Infect Dis. (2016) 3:ofw171. doi: 10.1093/ofid/ofw171
5. Huang L, Zhang N, Huang X, Xiong S, Feng Y, Zhang Y, et al. Invasive pulmonary aspergillosis in patients with influenza infection: a retrospective study and review of the literature. Clin Respir J. (2019) 13:202–11. doi: 10.1111/crj12995
6. Vanderbeke L, Spriet I, Breynaert C, Rijnders BJA, Verweij PE, Wauters J. Invasive pulmonary aspergillosis complicating severe influenza: epidemiology, diagnosis and treatment. Curr Opin Infect Dis. (2018) 31:471–80. doi: 10.1097/qco0000000000000504
7. Lamoth F, Calandra T. Let's add invasive aspergillosis to the list of influenza complications. Lancet Respir Med. (2018) 6:733–5. doi: 10.1016/s2213-2600(18)30332-1
8. Donnelly JP, Chen SC, Kauffman CA, Steinbach WJ, Baddley JW, Verweij PE, et al. Revision and update of the consensus definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin Infect Dis. (2020) 71:1367–76. doi: 10.1093/cid/ciz1008
9. Shah MM, Hsiao EI, Kirsch CM, Gohil A, Narasimhan S, Stevens DA. Invasive pulmonary aspergillosis and influenza co-infection in immunocompetent hosts: case reports and review of the literature. Diagn Microbiol Infect Dis. (2018) 91:147–52. doi: 10.1016/j.diagmicrobio.2018.01.014
10. Kwon OK, Lee MG, Kim HS, Park MS, Kwak KM, Park SY. Invasive pulmonary aspergillosis after influenza A infection in an immunocompetent patient. Tuberc Respir Dis (Seoul). (2013) 75:260–3. doi: 10.4046/trd.2013.75.6.260
11. Venkatesh B, Finfer S, Cohen J, Rajbhandari D, Arabi Y, Bellomo R, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. (2018) 378:797–808. doi: 10.1056/NEJMoa1705835
12. Thompson BT, Chambers RC, Liu KD. Acute respiratory distress syndrome. N Engl J Med. (2017) 377:562–72. doi: 10.1056/NEJMra1608077
13. Alshabani K, Haq A, Miyakawa R, Palla M, Soubani AO. Invasive pulmonary aspergillosis in patients with influenza infection: report of two cases and systematic review of the literature. Expert Rev Respir Med. (2015) 9:89–96. doi: 10.1586/17476348.2015996132
14. Bautista E, Chotpitayasunondh T, Gao Z, Harper SA, Shaw M, Uyeki TM, et al. Clinical aspects of pandemic 2009 influenza A (H1N1) virus infection. N Engl J Med. (2010) 362:1708–19. doi: 10.1056/NEJMra1000449
15. Hagau N, Slavcovici A, Gonganau DN, Oltean S, Dirzu DS, Brezoszki ES, et al. Clinical aspects and cytokine response in severe H1N1 influenza A virus infection. Crit Care. (2010) 14:R203. doi: 10.1186/cc9324
16. De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, Calandra T, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis. (2008) 46:1813–21. doi: 10.1086/588660
17. Meersseman W, Lagrou K, Maertens J, Van Wijngaerden E. Invasive aspergillosis in the intensive care unit. Clin Infect Dis. (2007) 45:205–16. doi: 10.1086/518852
18. Roosen J, Frans E, Wilmer A, Knockaert DC, Bobbaers H. Comparison of premortem clinical diagnoses in critically III patients and subsequent autopsy findings. Mayo Clin Proc. (2000) 75:562–7. doi: 10.4065/75.6562
19. Uffredi ML, Mangiapan G, Cadranel J, Kac G. Significance of Aspergillus fumigatus isolation from respiratory specimens of nongranulocytopenic patients. Eur J Clin Microbiol Infect Dis. (2003) 22:457–62. doi: 10.1007/s10096-003-0970-y
20. Park SY, Lim C, Lee SO, Choi SH, Kim YS, Woo JH, et al. Computed tomography findings in invasive pulmonary aspergillosis in non-neutropenic transplant recipients and neutropenic patients, and their prognostic value. J Infect. (2011) 63:447–56. doi: 10.1016/j.jinf.2011.08007
21. Kang H, Lee KS, Jeong YJ, Lee HY, Kim KI, Nam KJ. Computed tomography findings of influenza A (H1N1) pneumonia in adults: pattern analysis and prognostic comparisons. J Comput Assist Tomogr. (2012) 36:285–90. doi: 10.1097/RCT0b013e31825588e6
22. Shieh WJ, Blau DM, Denison AM, Deleon-Carnes M, Adem P, Bhatnagar J, et al. 2009 pandemic influenza A (H1N1): pathology and pathogenesis of 100 fatal cases in the United States. Am J Pathol. (2010) 177:166–75. doi: 10.2353/ajpath.2010.100115
23. Hartemink KJ, Paul MA, Spijkstra JJ, Girbes AR, Polderman KH. Immunoparalysis as a cause for invasive aspergillosis? Intensive Care Med. (2003) 29:2068–71. doi: 10.1007/s00134-003-1778-z
24. Guo XJ, Thomas PG. New fronts emerge in the influenza cytokine storm. Semin Immunopathol. (2017) 39:541–50. doi: 10.1007/s00281-017-0636-y
25. Gershov D, Kim S, Brot N, Elkon KB. C-Reactive protein binds to apoptotic cells, protects the cells from assembly of the terminal complement components, and sustains an antiinflammatory innate immune response: implications for systemic autoimmunity. J Exp Med. (2000) 192:1353–64. doi: 10.1084/jem.192.9.1353
26. Zuniga J, Torres M, Romo J, Torres D, Jimenez L, Ramirez G, et al. Inflammatory profiles in severe pneumonia associated with the pandemic influenza A/H1N1 virus isolated in Mexico City. Autoimmunity. (2011) 44:562–70. doi: 10.3109/08916934.2011592885
27. Jia L, Xie J, Zhao J, Cao D, Liang Y, Hou X, et al. Mechanisms of severe mortality-associated bacterial co-infections following influenza virus infection. Front Cell Infect Microbiol. (2017) 7:338. doi: 10.3389/fcimb.2017.00338
28. Fox A, Le NM, Horby P, van Doorn HR, Nguyen VT, Nguyen HH, et al. Severe pandemic H1N1 2009 infection is associated with transient NK and T deficiency and aberrant CD8 responses. PLoS ONE. (2012) 7:e31535. doi: 10.1371/journal.pone.0031535
29. Boch T, Reinwald M, Spiess B, Liebregts T, Schellongowski P, Meybohm P, et al. Detection of invasive pulmonary aspergillosis in critically ill patients by combined use of conventional culture, galactomannan, 1-3-beta-D-glucan and Aspergillus specific nested polymerase chain reaction in a prospective pilot study. J Crit Care. (2018) 47:198–203. doi: 10.1016/j.jcrc.2018.07001
Keywords: severe influenza, aspergillosis, prognostic factors, immunocompetent hosts, excessive inflammatory response
Citation: Duan Y, Ou X, Chen Y, Liang B and Ou X (2021) Severe Influenza With Invasive Pulmonary Aspergillosis in Immunocompetent Hosts: A Retrospective Cohort Study. Front. Med. 7:602732. doi: 10.3389/fmed.2020.602732
Received: 04 September 2020; Accepted: 21 December 2020;
Published: 18 January 2021.
Edited by:
Rogerio Souza, University of São Paulo, BrazilReviewed by:
George Dimopoulos, University General Hospital Attikon, GreeceMarcello Magri, Universidade de São Paulo, Brazil
Copyright © 2021 Duan, Ou, Chen, Liang and Ou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xuemei Ou, ouxuemei@163.com