The impact on the scientific community of the 2018 addendum to the CHCC
 Marzia Caproni1
Marzia Caproni1  Valentina Ruffo di Calabria2
Valentina Ruffo di Calabria2  Elena Biancamaria Mariotti2*
Elena Biancamaria Mariotti2*  Alice Verdelli3 Cristina Aimo2 Alberto Corrà2 Lavinia Quintarelli1 Walter Volpi3
Alice Verdelli3 Cristina Aimo2 Alberto Corrà2 Lavinia Quintarelli1 Walter Volpi3  Erkan Alpsoy4 Cord Sunderkötter5
Erkan Alpsoy4 Cord Sunderkötter5- 1Immunopathology and Rare Skin Disease Unit, P.O. Piero Palagi, Azienda USL Toscana Centro, ERN-SKIN Member, University of Florence, Florence, Italy
- 2Section of Dermatology and Venereology, Department of Health Sciences, University of Florence, Florence, Italy
- 3Section of Dermatology and Venereology, Azienda USL Toscana Centro, Florence, Italy
- 4Section of Dermatology and Venereology, Akdeniz University School of Medicine, Antalya, Turkey
- 5Department of Dermatology and Venereology, University Hospital Halle (Saale), Martin-Luther-University Halle-Wittenberg, Wittemberg, Germany
Introduction
The term vasculitis encompasses a wide and heterogeneous group of disorders with shared histopathological findings, namely inflammation and necrosis of the blood vessel wall with variable hemorrhagic and ischemic features. Vasculitis may range in severity from a self-limited disorder in one single organ to a life-threatening disease as vessels of any size can be affected (1).
The 1994 Chapel Hill Consensus Conference Nomenclature of Vasculitides (CHCC1994) managed to provide a consensus on definitions of such conditions instead of a classification system or shared diagnostic criteras. At first, vasculitides were distinguished according to the size of the affected vessels and the involved immunopathogenic process. Because of the scientific advances in the understanding of the underlying mechanisms, the classification was further expanded and updated with the 2012 revised International CHCC (CHCC2012), which resulted in the introduction of new categories namely Variable vessel vasculitis, Vasculitis associated with systemic disease and Vasculitis associated with probable etiology (2).
However, even though vasculitides frequently involves the skin, it was only in 2018 that a standardized specific nomenclature was proposed on the basis of the CHCC nomenclatures to highlight the special features of cutaneous vasculitides (CV). These acquirements were included in the Dermatologic Addendum to CHCC2012 (D-CHCC). Accordingly, CV were divided into three groups: (1) CV as part of a systemic vasculitis; (2) skin-limited or skin-dominant vasculitis as a variant of a systemic vasculitis which is restricted to the skin without clinically visible or manifested systemic vasculitis and (3) single organ vasculitis of the skin (SOV). The SOVs group has no equivalent in other organs and they differ from the skin-dominant forms since they do not fulfill sufficient clinical, laboratory, and/or pathologic features of a known systemic vasculitis. They encompass Nodular vasculitis (erythema induratum of Bazin), Erythema elevatum et diutinum, Recurrent macular vasculitis in hypergammaglobulinemia (hypergammaglobulinemic purpura of Waldenstrom) and Normocomplementemic urticarial vasculitis (3). However, other forms, e.g., IgM/IgG immune complex vasculitis, may be also included in this group in the future if supported by research. A good example of systemic vs. skin-limited vasculitis would be IgA vasculitis (IgAV), since many patients with vasculitis which present at dermatology offices have skin-limited IgA: the latter is confirmed by leukocytoclastic vasculitis on histopathology and perivascular IgA deposition on immunofluorescence. While these patients do not show pathological urine, i.e., no erythrocytes urine and no abdominal pain as well as absence of signs of nephritis (non-pathological urine analysis, no dysmorphic erythrocytes, no rise in blood pressure), of gastrointestinal vasculitis (no postprandial abdominal pain, negative hemoccult) and of arthritis, though one cannot exclude that they would show microscopic alterations such as IgA deposition in kidneys since one would not subject these patients to renal biopsies. Systemic but also skin limited IgAV present with perivascular deposition of hypogalactosidated IgA (GdIgA), so this modified IgA1 is not the reason for the difference (4), but patients with systemic IgAV appear to have higher serum levels of GdIgA during active disease (5, 6). None of these Consensus conferences was ever meant to provide diagnostic criteria, but rather to standardize an expanding terminology of different nosologic entities. In more recent years the Diagnostic and Classification Criteria in Vasculitis (DCVAS) represented an interdisciplinary attempt to implement the classification criteria of systemic vasculitides by recruiting 6,991 participants from 136 sites in 32 countries starting from January 2011 to December 2017 (7). The extensive data set collected internationally thanks to the DCVAS study has been subsequently analyzed and resulted in the 2022 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification for Microscopic polyangiitis (MPA), Granulomatosis with Polyangiitis (GPA) and Eosinophilic Granulomatosis with Polyangiitis (EGPA) (8, 9) These new formal criteria are based on weighted items, including also ANCA testing and modern imaging techniques. Because of their excellent sensitivity and high specificity, they represent a useful tool for the clinician, in the setting of clinical research, in differentiating cases of MPA/GPA/EGPA from similar types of vasculitides, when a diagnosis of small- or medium-vessel vasculitis has already been made and other conditions that potentially mimic vasculitides have already been excluded. It is important to note once more that even though these criteria are not meant for diagnostic purpose in the everyday clinical practice, they have been validated to replace the European Medicines Agency (EMA) algorithm published in 2007, previously used to harmonize and rationalize the use of the ACR and CHCC classification systems for epidemiologic purposes (10).
Finally, Diagnostic and Classification criteria in VASculitis (DCVAS) also developed diagnostic criteria for ANCA Associated Vasculitis (AAV) in a large study recruiting patients into an international cohort from 2010 until December 2017 with AAV and comparator diseases (11–13).
The impact of dermatological addendum in scientific community
We performed a review of the literature to evaluate the actual impact that the D-CHCC has had during the last 4 years in the scientific community. From 2018 until September 2018, the Addendum has been cited in 115 publications on Pubmed and the number of citations per year showed an increasing pattern with a maximum peak reached in 2021 (n = 36) (Figure 1). Of these publications, 107 (1, 2, 4, 6, 14–115) were written in English and published by Journals specialized in Dermatology (n = 41), Rheumatology (n = 20) and Immunology (n = 13) and their Countries of publication were mainly represented by the United States of America (n = 37), Germany (n = 21), United Kingdom (n = 16).
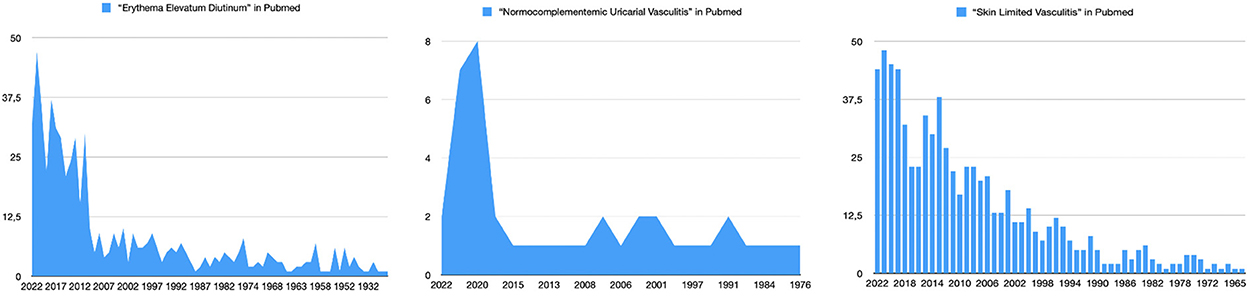
Figure 1. Count of the articles that used the terms “Normocomplementemic Urticarial Vasculitis”, “Erythema Elevatum Diutinum” and “Skin Limited Vasculitis” over the years in Pubmed.
Limiting the research to the new described CV, we only found one study in the English literature that was aimed to further investigate the clinical and immunopathologic features of cutaneous IgM/IgG immune complex vasculitis (8) Its main goal was to elucidate the clinical differences between IgM/IgG vasculitis and the more common skin-limited IgA vasculitis (sI-IgAV), thus proposing practical advice for the everyday medical practice. Hemorrhagic blisters and targetoid lesions seemed to be more frequent in the sI-IgAV group, suggesting that these two features could represent a valuable clinical tool that may help differentiating the two forms when immunological tests are unavailable or unaffordable. A group of researchers tried to link special clinical characteristics to the “Recurrent macular vasculitis in hypergammaglobulinemia” category in 2019, while this term was hardly used before 2018 and the clinical symptoms or very similar diseases were referred to with many different names (golfer's vasculitis, Waldenströn purpura, exercise-induced vasculitis, Saturday night vasculitis). Concerning “Normocomplementemic urticarial vasculitis,” a slight increase in its usage was appreciable after the introduction of the D-CHCC. In fact, before 2018, eight articles only reported this term over 27 years (1991–2018), while after 2018, nine cases could be counted until now (Figure 1). The “Erythema elevatum et diutinum” category, although largely adopted throughout the years, reached its peak of use the biennium 2019–2020 (Figure 1).
Extending our search to other forms of vasculitis, such as IgA vasculitis, we found many discrepancies. In fact, the term “Henoch-Schonlein purpura” has been used 962 times, mainly by Pediatrics journals, instead or together with the updated and more accurate terminology of “IgA vasculitis.” These data show that there is still confusion in the use of terminology, often based on old classifications and highlight the need for a synergistic work to reach a real widespread consensus on the nomenclature of vasculitis. Moreover, only a few articles (48 in 2021) use the term “skin limited vasculitis” to distinguish these forms from the ones with systemic involvement, although its number has risen since publication of D-CHCC (Figure 1). Thus, although this phenomenon has been known for a long time by dermatologists, it is still not reflected by a punctual use of the specific terms.
Discussion
The D-CHCC has been adopted internationally by several experts of the field. According to our data, many authors have cited the D-CHCC in their work in the last years as it has been quoted almost 200 times so far, thus recognizing its clarifying role in the nomenclature of CV. Many are becoming more familiar with the new terminology, mainly dermatologists and rheumatologist and especially experts in the field of vasculitis or dermatopathology have explicitly welcome its appearance and supported its use. However, it is not yet mentioned in all articles on CV and several recent publications on vasculitis do not use the terminology as it was consented on. In this regard, it is not of secondary importance the still widespread use of eponymous terminology. This issue is linked to that of the provisional definitions or unsolved problems in the actual nomenclature. For example, while the term IgG/IgM vasculitis will likely continue to be used, further data must be provided for the existence of an isolated form of IgG/IgM vasculitis (no IgA involvement; no other, IgG-IC generating autoimmune disorders associated) (56). The establishment of a standardized and universally accepted nomenclature will also provide a fundamental base for multicentric studies, which would allow us to collect and compare a more significant set of data that is nowadays lacking for a deeper understanding of CV. As modifications to the actual nomenclature are possible, dermatologists and rheumatologists, among others, are invited to contribute with suggestions for improvement. In fact, the D-CHCC represent a basis for interdisciplinary discussion on CV offering written statements which can be either falsified or verified by clinical observation on patients. One of the aims of the D_CHCC group was the chance to test the practicability of the D-CHCC definitions in the clinical setting. In particular it would be useful to know, if each dermatosis with histopathologically proven vasculitis, can be assigned to the various defined forms of vasculitides. Another aim of the D-CHCC was to encourage the acquisition of new data to help clarify e.g., the existence of lymphocytic or eosinophilic vasculitis according to the consented, but provisional definitions.
To conclude, CV encompass a wide and heterogeneous group of rare conditions, probably often underdiagnosed and under investigated by clinicians with no specialized dermatologic competences, especially in the cases where clinical manifestations are minor and self-limiting. Even though some clinical entities are now known to have specific clinical features, much more needs to be done to further implement our knowledge in the underlying pathogenetic mechanisms, which remain partially unknown and is of fundamental importance for a better diagnostic and therapeutic management of patients suffering from CV.
Author contributions
MC, EA, and CS conceptualized the work. VC and EM wrote the text. AV and CA collected the data. AC, LQ, and WV revised the drafts. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Morita TCAB, Trés GFS, Criado RFJ, Sotto MN, Criado PR. Update on vasculitis: an overview and dermatological clues for clinical and histopathological diagnosis - part I. An Bras Dermatol. (2020) 95:355–71. doi: 10.1016/j.abd.2020.01.003
2. Caproni M, Verdelli A. An update on the nomenclature for cutaneous vasculitis. Curr Opin Rheumatol. (2019) 31:46–52. doi: 10.1097/BOR.0000000000000563
3. Sunderkötter CH, Zelger B, Chen KR, Requena L, Piette W, Carlson JA, et al. Nomenclature of cutaneous vasculitis: dermatologic addendum to the 2012 revised international chapel hill consensus conference nomenclature of vasculitides. Arthritis Rheumatol. (2018) 70:171–84. doi: 10.1002/art.40375
4. Neufeld M, Molyneux K, Pappelbaum KI, Mayer-Hain S, von Hodenberg C, Ehrchen J, et al. Galactose-deficient IgA1 in skin and serum from patients with skin-limited and systemic IgA vasculitis. J Am Acad Dermatol. (2019) 81:1078–85. doi: 10.1016/j.jaad.2019.03.029
5. Mayer-Hain S, Gebhardt K, Neufeld M, Ehrchen JM, Molyneux K, Barratt J, et al. Systemic activation of neutrophils by immune complexes is critical to IgA vasculitis. J Immunol. (2022) 209:1048–58. doi: 10.4049/jimmunol.2100924
6. Pillebout E, Sunderkötter C. IgA vasculitis. Semin Immunopathol. (2021) 43:729–38. doi: 10.1007/s00281-021-00874-9
7. Caplan A, Micheletti RG. Advances in cutaneous vasculitis research and clinical care. Ann Transl Med. (2021) 9:439. doi: 10.21037/atm-20-6395
8. Pyo JY, Ahn SS, Song JJ, Park YB, Lee SW. Reclassification of previously diagnosed GPA patients using the 2022 ACR/EULAR classification criteria. Rheumatology (Oxford). (2022) 4:keac267. doi: 10.1093/rheumatology/keac267
9. Jain V, Tiwari V. Microscopic Polyangiitis. In: StatPearls. Treasure Island (FL): StatPearls Publishing. (2022).
10. Abdulkader R, Lane SE, Scott DG, Watts RA. Classification of vasculitis: EMA classification using CHCC 2012 definitions. Ann Rheum Dis. (2013) 72:1888. doi: 10.1136/annrheumdis-2013-203511
11. Grayson PC, Ponte C, Suppiah R, Robson JC, Craven A, Judge A, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis. Ann Rheum Dis. (2022) 81:309–14. doi: 10.1136/annrheumdis-2021-221794
12. Robson JC, Grayson PC, Ponte C, Suppiah R, Craven A, Judge A, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for granulomatosis with polyangiitis. Ann Rheum Dis. (2022) 81:315–20. doi: 10.1136/annrheumdis-2021-221795
13. Suppiah R, Robson JC, Grayson PC, Ponte C, Craven A, Khalid S, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for microscopic polyangiitis. Ann Rheum Dis. (2022) 81:321–6. doi: 10.1136/annrheumdis-2021-221796
14. Takeuchi S, Kawakami T, Okano T, Shida H, Nakazawa D, Tomaru U, et al. Elevated myeloperoxidase-DNA complex levels in sera of patients with IgA vasculitis. Pathobiology. (2022) 89:23–8. doi: 10.1159/000519869
15. Mutlu MY, Içaçan OC, Çelik S, Bes C. ANCA Associated Vasculitis and Related Pulmonary Alveolar Hemorrhage in a Patient with Pulmonary Alveolar Proteinosis. Clin Ter. (2021) 172:389–91. doi: 10.7417/CT.2021.2344
16. Dissemond J, Romanelli M. Inflammatory skin diseases and wounds. Br J Dermatol. (2022) 187:167–77. doi: 10.1111/bjd.21619
17. Robert M, Miossec P, Hot A. The Th17 pathway in vascular inflammation: culprit or consort? Front Immunol. (2022) 13:888763. doi: 10.3389/fimmu.2022.888763
18. Marzano AV, Maronese CA, Genovese G, Ferrucci S, Moltrasio C, Asero R, et al. Urticarial vasculitis: clinical and laboratory findings with a particular emphasis on differential diagnosis. J Allergy Clin Immunol. (2022) 149:1137–49. doi: 10.1016/j.jaci.2022.02.007
19. Kato K, Mizuno T, Koseki T, Ito Y, Takahashi K, Tsuboi N, et al. Frequency of immune checkpoint inhibitor-induced vasculitides: an observational study using data from the japanese adverse drug event report database. Front Pharmacol. (2022) 13:803706. doi: 10.3389/fphar.2022.803706
20. Assan F, Bottin L, Francès C, Moguelet P, Tavolaro S, Barbaud A, et al. Antiphospholipid-negative Sneddon's syndrome: a comprehensive overview of a rare entity. Ann Dermatol Venereol. (2022) 149:3–13. doi: 10.1016/j.annder.2021.08.007
21. Sunderkötter C. Suspected allergy to Beta-Lactam antibiotics: an infectiological perspective. Allergol Select. (2022) 6:27–32. doi: 10.5414/ALX02314E
22. Dastoli S, Nisticò SP, Morrone P, Patruno C, Leo A, Citraro R, et al. Colchicine in managing skin conditions: a systematic review. Pharmaceutics. (2022) 14:294. doi: 10.3390/pharmaceutics14020294
23. Zhang N, Sun J, Ji C, Bao X, Yuan C. Predicting bacterial infection risk in patients with ANCA-associated vasculitis in southwest China: development of a new nomogram. Clin Rheumatol. (2022) 41:3451–60. doi: 10.1007/s10067-022-06314-9
24. Stewart M, Lo A, Shojania K, Au S, Seidman MA, Dutz JP, et al. Cutaneous polyarteritis nodosa diagnosis and treatment: A retrospective case series. J Am Acad Dermatol. (2022) doi: 10.1016/j.jaad.2022.06.009. [Epub ahead of print].
25. Karadag AS, Parish LC, Wang JV. Roxburgh's Common Skin Diseases. (19th ed.). Boca Raton: CRC Press. (2022).
26. Karassa FB, Pelechas E, Zouzos G. The immunogenetics of vasculitis. Adv Exp Med Biol. (2022) 1367:299–334. doi: 10.1007/978-3-030-92616-8_11
27. Shionoya A, Hida T, Ikeda H, Sugita S, Segawa K, Hasegawa T, et al. Case of immunoglobulin (Ig)M/IgG immune complex vasculitis associated with multicentric Castleman's disease. J Dermatol. (2021) 48:e614–5. doi: 10.1111/1346-8138.16180
28. Liao Z, Tang J, Luo L, Deng S, Luo L, Wang F, et al. Altered circulating CCR6+and CXCR3+ T cell subsets are associated with poor renal prognosis in MPO-ANCA-associated vasculitis. Arthritis Res Ther. (2021) 23:194. doi: 10.1186/s13075-021-02576-x
29. Schiffmann ML, Dissemond J, Erfurt-Berge C, Hafner J, Itzlinger-Monshi BA, Jungkunz HW, et al. German S1 guideline: diagnosis and treatment of livedovasculopathy. J Dtsch Dermatol Ges. (2021) 19:1668–78. doi: 10.1111/ddg.14520
30. Su T, Wang H, Wang S, Yang L. Clinicopathological Patterns and Predictors of the Functional Restoration of Immunoglobulin G4-Related Kidney Disease: A Chinese Single-Center Cohort Study. Front Med (Lausanne). (2021) 8:736098. doi: 10.3389/fmed.2021.736098
31. Domínguez-Quintana M, Alba MA, Hinojosa-Azaola A. Classification of ANCA-associated vasculitis: differences based on ANCA specificity and clinicopathologic phenotype. Rheumatol Int. (2021) 41:1717–28. doi: 10.1007/s00296-021-04966-5
32. Kimura K, Miyabe C, Nakamura S, Tochihara M, Ishiguro N. Case of hypergammaglobulinemic purpura successfully treated with colchicine. J Dermatol. (2021) 48:E524–5. doi: 10.1111/1346-8138.16078
33. Frumholtz L, Laurent-Roussel S, Lipsker D, Terrier B. Cutaneous vasculitis: review on diagnosis and clinicopathologic correlations. Clin Rev Allergy Immunol. (2021) 61:181–93. doi: 10.1007/s12016-020-08788-4
34. Nieto-Benito LM, Balaguer-Franch I, Barchino-Ortiz L. Pearl necklace-like bullous and purpuric lesions. Intern Med J. (2021) 51:1551–2. doi: 10.1111/imj.15482
35. Yamaki Y, Hayashi D, Honda K, Imai H, Takada H. A.case of omalizumab-associated eosinophilic granulomatosis with polyangiitis. Pediatr Int. (2021) 63:1119–21. doi: 10.1111/ped.14540
36. Sunderkötter C, Golle L. Dermatological differential diagnoses of idiopathic inflammatory muscle disease. Aktuelle Rheumatol. (2021) 46:382–7 doi: 10.1055/a-1551-5556
37. Batista M, Calado R, Gil F, Cardoso JC, Tellechea O, Gonçalo M. Histopathology of chronic spontaneous urticaria with occasional bruising lesions is not significantly different from urticaria with typical wheals. J Cutan Pathol. (2021) 48:1020–6. doi: 10.1111/cup.13985
38. Pan L, Wang J, Liu J, Guo L, Yang S. Deficiency in the frequency and function of Tr1 cells in IgAV and the possible role of IL-27. Rheumatology (Oxford). (2021) 60:3432–42. doi: 10.1093/rheumatology/keaa752
39. Liu M, Yu Y, Hu S. A review on applications of abatacept in systemic rheumatic diseases. Int Immunopharmacol. (2021) 96:107612. doi: 10.1016/j.intimp.2021.107612
40. Matsuda KM, Yoshizaki A, Kotani H, Kuzumi A, Fukayama M, Ebata S, et al. Development of a prediction model of treatment response in patients with cutaneous arteritis: Insights from a cohort of 33 patients. J Dermatol. (2021) 48:1021–6. doi: 10.1111/1346-8138.15868
41. Ko CJ, Gehlhausen JR, McNiff JM. Leukocytoclastic Vasculitis and Microvascular Occlusion: Key Concepts for the Working Pathologist. Surg Pathol Clin. (2021) 14:309–25. doi: 10.1016/j.path.2021.01.006
42. Fraticelli P, Benfaremo D, Gabrielli A. Diagnosis and management of leukocytoclastic vasculitis. Intern Emerg Med. (2021) 16:831–41. doi: 10.1007/s11739-021-02688-x
43. Yoshida S, Muto J, Utsunomiya R, Kitazawa R, Matsumoto T, Sayama K. Cutaneous arteritis with compartment syndrome: Case report and review of published works. J Cutan Immunol Allergy. (2021) 4:57–61. doi: 10.1002/cia2.12165
44. Puhl V, Bonnekoh H, Scheffel J, Hawro T, Weller K, von den Driesch P, et al. A novel histopathological scoring system to distinguish urticarial vasculitis from chronic spontaneous urticarial. Clin Transl Allergy. (2021) 11:e12031. doi: 10.1002/clt2.12031
45. Cappel MA, Cappel JA, Wetter DA. Pernio (Chilblains), SARS-CoV-2, and COVID toes unified through cutaneous and systemic mechanisms. Mayo Clin Proc. (2021) 96:989–1005. doi: 10.1016/j.mayocp.2021.01.009
46. Walls AC, Din RS, Okhovat JP, Chansky PB, Micheletti RG, Mostaghimi A. Low utility of radiologic imaging in evaluating cutaneous small-vessel vasculitis: a multi-institutional retrospective study. J Am Acad Dermatol. (2021) 84:1197–9. doi: 10.1016/j.jaad.2020.09.051
47. Kawamura M, Mizutani Y, Mizutani Y, Matsuyama K, Miyazaki T, Seishima M. Clinical and pathological differences between skin-limited IgM/IgG vasculitis and skin-limited IgA vasculitis. J Cutan Immunol Allerg. (2021) 4:28–33. doi: 10.1002/cia2.12156
48. Chen RY, Wu SF, Yu WS, Ma LL, Jiang LD. A ten-year monocenter epidemiological analysis of the subtypes of hospitalized patients with vasculitis [???????????????????????]. Fudan Univ J Med Sci. (2021) 48:162–8, 228. doi: 10.3969/j.issn.1672-8467.2021.02.003
49. Hočevar A, Tomšič M, Perdan Pirkmajer K. Clinical approach to diagnosis and therapy of polyarteritis nodosa. Curr Rheumatol Rep. (2021) 23:14. doi: 10.1007/s11926-021-00983-2
50. Dang T, Chavez LO, Leon M, Gandhi K, Taweesedt P, Surani S. Gastrointestinal complications of vasculitis. In: Brown RM, editor. Vasculitis: From Diagnosis to Treatment. El Paso: Department of Internal Medicine, Texas Tech University Health Science Center (2021). p. 179–98.
51. Isoherranen K, Kluger N, Hannula-Jouppi K, Väkevä L. The role of negative pressure wound therapy (npwt) in the management of vasculitic wounds: Case series of eight patients. Int J Low Extrem Wounds. (2021). doi: 10.1177/15347346211063700. [Epub ahead of print].
52. Prieto-Peña D, Pina T, González-Gay MA. Cutaneous vasculitis. In: Salvarani C, Boiardi L, Muratore F, editors. Large and Medium Size Vessel and Single Organ Vasculitis. Rare Diseases of the Immune System. Cham: Springer (2021). doi: 10.1007/978-3-030-67175-4_18
53. Kodet O. Vasculitis from the perspective of a dermatologist. Cesko-Slov Dermatol. (2021) 96:99–122.
54. Endo M, Yamamoto T, Chen KR. Sarcoid vasculitis presenting with erythema nodosum-like lesions. Sarcoidosis Vasc Diffuse Lung Dis. (2021) 38:e2021013. doi: 10.36141/SVDLD.V38I1.11277
55. Betti C, Camozzi P, Gennaro V, Bianchetti MG, Scoglio M, Simonetti GD, et al. Atypical Bacterial Pathogens and Small-Vessel Leukocytoclastic Vasculitis of the Skin in Children: Systematic Literature Review. Pathogens. (2021) 10:31. doi: 10.3390/pathogens10010031
56. Marzano AV, Genovese G, Tavecchio S, Germiniasi F, Fanoni D, Caproni M, et al. Clinical and immunopathologic features of idiopathic cutaneous immunoglobulin M/G vasculitis versus idiopathic skin-limited immunoglobulin A vasculitis. J Am Acad Dermatol. (2021) 84:175–8. Erratum in: J Am Acad Dermatol. (2021) 84:1506. doi: 10.1016/j.jaad.2020.04.060
57. Llamas-Velasco M, Fernández-Figueras MT. A practical approach to the clinico-pathological diagnosis of panniculitis. Diagn Histopathol. (2021) 27:34–41 doi: 10.1016/j.mpdhp.2020.10.012
58. Ratzinger G, Zelger B, Frischhut N, Zelger B. Cutaneous vasculitis. Diagn Histopathology. 2021;27:6–12 doi: 10.1016/j.mpdhp.2020.10.009
59. San Martin-Leal A, Gonzalez-Cuevas R, Lucchini-Wortzman V, Affeld-Carmona C. Disseminated nodular vasculitis. Piel. (2021) 36:67–70 doi: 10.1016/j.piel.2020.02.006
60. Gao N, Pan L. Multiple gastrointestinal ulcers in a patient with microscopic polyangiitis: a clinical image. J Clin Rheumatol. (2020) 26:e319–20. doi: 10.1097/RHU.0000000000001175
61. Ismayilov R, Haziyev T, Ozdemir DA, Saglam A, Buyukasik Y. Leukocytoclastic vasculitis as a previously unreported paraneoplastic manifestation of acute lymphoblastic leukemia in adults. J Hematopathology. (2020) 13:265–8. doi: 10.1007/s12308-020-00416-6
62. Maglie R, Genovese G, Solimani F, Guglielmo A, Pileri A, Portelli F, et al. Immune-mediated dermatoses in patients with haematological malignancies: a comprehensive review. Am J Clin Dermatol. (2020) 21:833–54. doi: 10.1007/s40257-020-00553-9
63. García-García B, Aubán-Pariente J, Munguía-Calzada P, Vivanco B, Argenziano G, Vázquez-López F. Development of a clinical-dermoscopic model for the diagnosis of urticarial vasculitis. Sci Rep. (2020) 10:6092. doi: 10.1038/s41598-020-63146-w
64. Yan Y, Zheng B, Wang X. Tuberculosis-associated panniculitis. Chin J Dermatol. (2020) 53:944–7. doi: 10.35541/cjd.20190499
65. Munera-Campos M, Bielsa I, Martínez-Morillo M, Aparicio G, Olivé A, Ferrándiz C. Manifestations, clinical course and prognostic markers in cutaneous polyarteritis nodosa. J Dtsch Dermatol Ges. (2020) 18:1250–9. doi: 10.1111/ddg.14271
66. Mitschang C, Görge T. Diagnostik und Behandlung vaskulitischer Ulzerationen [Diagnosis and treatment of vasculitic ulcerations]. Hautarzt. (2020) 71:870–9. doi: 10.1007/s00105-020-04694-0
67. Guzman AK, Balagula Y. Drug-induced cutaneous vasculitis and anticoagulant-related cutaneous adverse reactions: insights in pathogenesis, clinical presentation, and treatment. Clin Dermatol. (2020) 38:613–28. doi: 10.1016/j.clindermatol.2020.06.015
68. Calle-Botero E, Abril A. Lupus Vasculitis. Curr Rheumatol Rep. (2020) 22:71. doi: 10.1007/s11926-020-00937-0
69. Micheletti RG, Pagnoux C. Management of cutaneous vasculitis. Presse Med. (2020) 49:104033. doi: 10.1016/j.lpm.2020.104033
70. Kullberg SA, Krug H, Gaddis K, Goldfarb N. Programmed cell death protein 1 inhibitor-induced recalcitrant mixed small and medium vessel vasculitis. Dermatol Online J. (2020) 26:13030. doi: 10.5070/D3269050167
71. Paule R, Vignon M, Régent A, London J, Cohen P, Le Jeunne C, et al. IgA monoclonal gammopathy associated with refractory IgA vasculitis successfully treated with clone-targeted therapy. Autoimmun Rev. (2020) 19:102611. doi: 10.1016/j.autrev.2020.102611
72. Yamamoto T, Chen KR. Cutaneous arteriolitis: a novel cutaneous small vessel vasculitis disorder clinicopathologically different from cutaneous polyarteritis nodosa and cutaneous venulitis. J Cutan Pathol. (2020) 47:854–9. doi: 10.1111/cup.13726
73. Al Kamzari A, Al Musalhi B, Al Abrawi S, Al-Zakwani I, Abdwani R. Urticarial vasculitis in pediatric systemic lupus erythematosus. Pediatr Dermatol. (2020) 37:651–5. doi: 10.1111/pde.14184
74. Holl-Ulrich K, Rose C. Kutane Vaskulitis und Vaskulopathie : Differenzialdiagnosen an der unteren Extremität [Cutaneous vasculitis and vasculopathy : Differential diagnosis in biopsies of the lower extremities]. Pathologe. (2020) 41:355–63. doi: 10.1007/s00292-020-00786-9
75. Ragab G, Hegazy MT, Ali M, Abdel-Halim MRE, Puéchal X. Three patterns of cutaneous involvement in granulomatosis with polyangiitis. J Adv Res. (2020) 24:311–5. doi: 10.1016/j.jare.2020.05.009
76. Miyazawa R, Tanei R, Tsuchida M, Sugihara T. A case of MPO-ANCA-positive cutaneous polyarteritis nodosa with livedo racemosa arising from immune-deposit-positive necrotizing vasculitis. G Ital Dermatol Venereol. (2020) 155:357–8. doi: 10.23736/S0392-0488.18.05956-4
77. Montero-Vilchez T, Martinez-Lopez A, Salvador-Rodriguez L, Del Carmen Ramírez-Barberena M, Tercedor-Sanchez J, Molina-Leyva A, et al. Cutaneous manifestations of granulomatosis with polyangiitis: a case series study. Acta Derm Venereol. (2020) 100:adv00150. doi: 10.2340/00015555-3506
78. George EA, Kornik R, Robinson-Bostom L. Providencia stuartii septic vasculitis. JAAD Case Rep. (2020) 6:422–5. doi: 10.1016/j.jdcr.2020.02.043
79. Zhou S, Li Q, Wu H, Lu Q. The pathogenic role of innate lymphoid cells in autoimmune-related and inflammatory skin diseases. Cell Mol Immunol. (2020) 17:335–46. doi: 10.1038/s41423-020-0399-6
80. Lefèvre G, Leurs A, Gibier JB, Copin MC, Staumont-Sallé D, Dezoteux F, et al. CEREO—French National Reference Center for Hypereosinophilic Syndromes. “Idiopathic Eosinophilic Vasculitis”: Another Side of Hypereosinophilic Syndrome? A Comprehensive Analysis of 117 Cases in Asthma-Free Patients. J Allergy Clin Immunol Pract. (2020) 8:1329–40.e3. doi: 10.1016/j.jaip.2019.12.011
81. Koch M, Khan Z, Karle EM, Patel TP. Immune complex vasculitis: a rash that cannot be missed. BMJ Case Rep. (2020) 13:e233545. doi: 10.1136/bcr-2019-233545
82. Mooyaart AL, Seelen MAJ, van Doorn MBA. Dermal C4d deposition and neutrophil alignment along the dermal-epidermal junction as a diagnostic adjunct for hypocomplementemic urticarial vasculitis (Anti-C1q Vasculitis) and underlying systemic disease. Am J Dermatopathol. (2020) 42:399–406. doi: 10.1097/DAD.0000000000001501
83. Wilk M, Zelger BG, Hayani K, Zelger B. Erythema nodosum, early stage-A subcutaneous variant of leukocytoclastic vasculitis? Clinicopathological correlation in a series of 13 patients. Am J Dermatopathol. (2020) 42:329–36. doi: 10.1097/DAD.0000000000001469
84. Hočevar A, Šuput Skvarča D, Tomšič M, Perdan Pirkmajer K. Multifocal thrombophlebitis and orbital cellulitis. Am J Case Rep. (2020) 21:e919715. doi: 10.12659/AJCR.919715
85. Pellanda G, Lava SAG, Milani GP, Bianchetti MG, Ferrarini A, Vanoni F. Immune deposits in skin vessels of patients with acute hemorrhagic edema of young children: a systematic literature review. Pediatr Dermatol. (2020) 37:120–3. doi: 10.1111/pde.14041
86. Jung JH, Seok H, Choi SJ, Song GG, Han Y. Association between rs1800795 polymorphisms in the interleukin-6 gene and vasculitis: a meta-analysis. Sarcoidosis Vasc Diffuse Lung Dis. (2019) 36:302–10. doi: 10.36141/svdld.v36i4.8653
87. Misra D, Patro P, Sharma A. Drug-induced vasculitis. Indian J Rheumatol. (2019) 14:S3–9. doi: 10.4103/0973-3698.272156
88. Ludwin A, Ludwin I, Szczeklik W, Martins WP. Cutaneous small-vessel vasculitis following hysterosalpingo-foam sonography (HyFoSy). Ultrasound Obstet Gynecol. (2019) 54:831–4. doi: 10.1002/uog.20372
89. Gonzalez CD, Florell SR, Bowen AR, Presson AP, Petersen MJ. Histopathologic vasculitis from the periulcer edge: a retrospective cohort study. J Am Acad Dermatol. (2019) 81:1353–7. doi: 10.1016/j.jaad.2019.04.011
90. Erden A, Bolek EC, Yardimci KG, Kilic L, Bilgen SA, Karadag O. Do ANCA-associated vasculitides and IgG4-related disease really overlap or not? Int J Rheum Dis. (2019) 22:1926–32. doi: 10.1111/1756-185X.13693
91. Steuer AB, Cohen JM. The color of skin: purple diseases of the skin, nails, and mucosa. Clin Dermatol. (2019) 37:528–47. doi: 10.1016/j.clindermatol.2019.07.016
92. Ratzinger G, Zelger BG, Zelger BW. Bar code reader - an algorithmic approach to cutaneous occluding vasculopathies? Part I: small vessel vasculopathies. J Dtsch Dermatol Ges. (2019) 17:895–904. doi: 10.1111/ddg.13930
93. Wenzel J. Cutaneous lupus erythematosus: new insights into pathogenesis and therapeutic strategies. Nat Rev Rheumatol. (2019) 15:519–32. doi: 10.1038/s41584-019-0272-0
94. Sunderkötter C, Michl C. Hautveränderungen bei Vaskulitiden : Teil 2: Spezielle Aspekte der Krankheitsbilder großer, mittelgroßer und kleiner Gefäße [Cutaneous alterations in vasculitides : Part 2: Special aspects of diseases of large, medium and small vessels]. Internist (Berl). (2019) 60:805–13. doi: 10.1007/s00108-019-0642-3
95. Sunderkötter C, Michl C. Hautveränderungen bei Vaskulitiden : Teil 1: Nomenklatur, Einteilung und klinisch-histologische Korrelationen [Cutaneous alterations in vasculitides : Part 1: Nomenclature, classification and correlation between clinical signs and histological features]. Internist (Berl). (2019) 60:799–804. doi: 10.1007/s00108-019-0641-4
96. Shirai T, Shirota Y, Fujii H, Ishii T, Harigae H. Four distinct clinical phenotypes of vasculitis affecting medium-sized arteries. Scand J Rheumatol. (2019) 48:308–14. doi: 10.1080/03009742.2018.1551965
97. Mohammad AJ, Jones RB, Smith R, Jayne D. Efficacy and safety of rituximab in the treatment of eosinophilic granulomatosis with polyangiitis. RMD Open. (2019) 5:e000905. doi: 10.1136/rmdopen-2019-000905
98. Carmona FD, López-Mejías R, Márquez A, Martín J, González-Gay MA. Genetic Basis of Vasculitides with Neurologic Involvement. Neurol Clin. (2019) 37:219–34. doi: 10.1016/j.ncl.2019.01.006
99. Brandy-García AM, Coto-Hernández R, Caminal-Montero L. Saturday night vasculitis. Med Clin (Barc). (2019) 152:e37–e38. doi: 10.1016/j.medcle.2018.06.016
100. Drerup C, Metze D, Ehrchen J, Mitschang C, Neufeld M, Sunderkötter C. Evidence for immunoglobulin-mediated vasculitis caused by monoclonal gammopathy in monoclonal gammopathy of unclear significance prompting oncologic treatment. JAAD Case Rep. (2019) 5:288–91. doi: 10.1016/j.jdcr.2019.01.013
101. Pagnoux C. Microscopic polyangiitis and granulomatosis with polyangiitis. ERS Monogr. (2019) 2019:153–72. doi: 10.1183/2312508X.10014619
102. Bănicioiu-Covei S, Vreju AF, Ciurea PL, Roşu A. Behçet's disease with rapidly progressive bilateral optic neuropathy and avascular femoral neck necrosis. Literature review and management update. Rom J Morphol Embryol. (2019) 60:955–61.
103. Yazici H, Yazici Y. Editorial: a review of vasculitis 2019: an introduction. Curr Opin Rheumatol. (2019) 31:1–2. doi: 10.1097/BOR.0000000000000565
104. Lipke A, Gethöffer K, Sindrilaru A, Scharffetter-Kochanek K. Progredientes Ulcus cruris mit Nekrose [Progressive lower leg ulceration with necrosis]. Hautarzt. (2019) 70:68–71. doi: 10.1007/s00105-018-4298-z
105. Fernandez AP. Connective tissue disease: current concepts. Dermatol Clin. (2019) 37:37–48. doi: 10.1016/j.det.2018.07.006
106. Watts RA. Evolving concepts in classification of systemic vasculitis: where are we and what is the way forward? Int J Rheum Dis. (2019) 22 Suppl 1:21–7. doi: 10.1111/1756-185X.13304
107. Human A, Pagnoux C. Diagnosis and management of ADA2 deficient polyarteritis nodosa. Int J Rheum Dis. (2019) 22 Suppl 1:69–77. doi: 10.1111/1756-185X.13283
108. Funai N, Kobori G, Machida S, Tokura Y. Polyarteritis nodosa with ureteric stenosis. J Cutan Immunol Allergy. (2018) 1:170–3. doi: 10.1002/cia2.12035
109. Doutre MS. Quoi de neuf en médecine interne? [What's new in internal medicine?]. Ann Dermatol Venereol. (2018) 145 (Suppl 7):VIIS24–VIIS31. doi: 10.1016/S0151-9638(18)31286-9
110. Sunderkötter C, Lamprecht P, Mahr A, Metze D, Zelger B. Nomenclature of cutaneous vasculitides - German translation of the dermatologic addendum to the 2012 Revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. J Dtsch Dermatol Ges. (2018) 16:1425–32. doi: 10.1111/ddg.13703
111. Lamprecht P, Klapa S, Holl-Ulrich K. 70/m mit palpabler Purpura, Sugillationen und trockener Endgliednekrose : Vorbereitung auf die Facharztprüfung: Folge 15 [70-year-old male with palpable purpura, suggillations and necrosis of the distal phalanges : Preparation for the medical specialist examination: Part 15]. Hautarzt. (2018) 69(Suppl 2):145–8. doi: 10.1007/s00105-018-4276-5
112. Anderson M, Chu T, Mauskar MM. Urticaria, urticarial vasculitis, angioedema, and related diseases. Curr Derm Rep. (2018) 7:190–7. doi: 10.1007/s13671-018-0223-z
113. Dissemond J, Erfurt-Berge C, Goerge T, Kröger K, Funke-Lorenz C, Reich-Schupke S. Systemic therapies for leg ulcers. J Dtsch Dermatol Ges. (2018) 16:87390. doi: 10.1111/ddg.13586
114. Loricera J, Blanco R. Vasculitis syndromes: a closer look at skin involvement in vasculitis. Nat Rev Rheumatol. (2018) 14:186–7. doi: 10.1038/nrrheum.2018.26
Keywords: vasculitides, nomenclature, Chapel Hill Consensus Conference, addendum to Chapel Hill Consensus, provisional definitions of vasculitides
Citation: Caproni M, Calabria VRd, Mariotti EB, Verdelli A, Aimo C, Corrà A, Quintarelli L, Volpi W, Alpsoy E and Sunderkötter C (2022) The impact on the scientific community of the 2018 addendum to the CHCC. Front. Med. 9:1081063. doi: 10.3389/fmed.2022.1081063
Received: 26 October 2022; Accepted: 02 November 2022;
Published: 01 December 2022.
Edited by:
Laura Atzori, University of Cagliari, ItalyReviewed by:
Filosa Giorgio, Employer, ItalyCopyright © 2022 Caproni, Calabria, Mariotti, Verdelli, Aimo, Corrà, Quintarelli, Volpi, Alpsoy and Sunderkötter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elena Biancamaria Mariotti, elenabiancamaria.mariotti@unifi.it