 Dinah B. Aziz
Dinah B. Aziz Jeanette W. P. Teo
Jeanette W. P. Teo Véronique Dartois
Véronique Dartois Thomas Dick
Thomas Dick- 1Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore
- 2Department of Pharmacy, Faculty of Science, National University of Singapore, Singapore, Singapore
- 3Department of Laboratory Medicine, National University Hospital, Singapore, Singapore
- 4The Public Health Research Institute, Rutgers, New Jersey Medical School, The State University of New Jersey, Newark, NJ, United States
- 5Department of Microbiology and Immunology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, Singapore
Lung disease caused by non-tuberculous mycobacteria (NTM), relatives of Mycobacterium tuberculosis, is increasing. M. abscessus is the most prevalent rapid growing NTM. This environmental pathogen is intrinsically resistant to most commonly used antibiotics, including anti-tuberculosis drugs. Current therapies take years to achieve cure, if cure if achieved. Thus, there is an urgent medical need to identify new, more efficacious treatments. Here, we explore the possibility of repurposing antibiotics developed for other indications. We asked whether novel two-drug combinations of clinically used antibiotics can be identified that show synergistic activity against this mycobacterium. An in vitro checkerboard titration assay was employed to test 180 dual combinations of 41 drugs against the clinical isolate M. abscessus Bamboo. The most attractive novel combination was further profiled against reference strains representing three sub-species (M. abscessus subsp. abscessus, massiliense and bolletii) and a collection of clinical isolates. This resulted in the identification of a novel synergistic antibiotic pair active against the M. abscessus complex: the glycopeptide teicoplanin with the glycylcycline tigecycline showed inhibitory activity at 2–3 μM (teicoplanin) and 1–2 μM (tigecycline). This novel combination can now be tested in M. abscessus animal models of infection and/or patients.
Introduction
Among the rapid growing non-tuberculous mycobacteria (NTM), M. abscessus is the most common cause of lung disease (Griffith et al., 2007; Medjahed et al., 2010; Hoefsloot et al., 2013). A poor rate of successful chemotherapeutic treatment makes M. abscessus disease a chronic incurable infection (Griffith et al., 2007). The bacterium is intrinsically drug resistant to most antibiotics (Brown-Elliott et al., 2012; Nessar et al., 2012). Currently, M. abscessus infections are treated by a multi-drug regimen consisting of a macrolide (clarithromycin), amikacin and either cefoxitin or imipenem (Benwill and Wallace, 2014; Ryu et al., 2016). Different clinics may choose to add on additional antibiotics and recently, tigecycline has been used (Wallace et al., 2014; Floto et al., 2016). The treatment issues are further complicated by the ability of two out of three sub-species of M. abscessus to develop macrolide resistance upon exposure to sub-inhibitory concentrations of the drug (Nash et al., 2009; Bastian et al., 2011; Maurer et al., 2014). Indeed, a recent study conducted in a hollow fiber model showed that the standard regimen of clarithromycin, amikacin, and cefoxitin exerted low sterilizing activity within the first 14 days of treatment, and re-growth of the bacteria was seen after this period due to inducible macrolide resistance (Ferro et al., 2016). Demonstrated transmission of M. abscessus between cystic fibrosis patients (Bryant et al., 2016) has increased the urgency to identify novel treatments for this NTM pathogen.
Screening for synergy interactions of approved drugs is an approach to new medicines that allows rapid bench-to-bedside translation (Hill and Cowen, 2015). A series of synergy studies have been conducted for M. abscessus and among the combinations that have been identified so far are imipenem + clarithromycin, imipenem + levofloxacin, clarithromycin + linezolid, clarithromycin + vancomycin, clofazimine + amikacin, tigecycline + clarithromycin, tigecycline + clofazimine, tigecycline + linezolid, clavulanate + meropenem, doripenem + rifampicin, biapenem + rifampicin, avibactam + ertapenem, avibactam + tebipenem, and avibactam + panipenem (Miyasaka et al., 2007; Cremades et al., 2009; Shen et al., 2010; van Ingen et al., 2012; Huang et al., 2013; Oh et al., 2014; Singh et al., 2014; Kaushik et al., 2015, 2017; Mukherjee et al., 2017).
To identify novel synergistic combinations, we carried out a large scale study using the checkerboard assay employing two different strategies. The first strategy was to screen combinations of β-lactams with β-lactamase inhibitors (Livermore, 1995; Bebrone et al., 2010). M. abscessus harbors the blamab gene encoding an Ambler class A β-lactamase (Soroka et al., 2014) and an inhibitor might restore activity of β-lactams against M. abscessus. The second strategy was to screen combinations of cell wall-targeting antibiotics with antibiotics that engage intracellular targets. This approach is based on our previous findings that vancomycin displayed (moderate) activity against M. abscessus (Aziz et al., 2017) and showed synergy with clarithromycin (Mukherjee et al., 2017). We screened a total of 180 dual drug combinations against a clinical isolate of M. abscessus and found that the combination of teicoplanin and tigecycline displayed synergistic activity. We characterized the in vitro activity of this novel combination against M. abscessus reference strains and diverse clinical isolates.
Materials and Methods
Compounds
The 36 antibiotics and 5 β-lactamase inhibitors used in this study were obtained from commercial sources and dissolved according to the manufacturer’s recommendations. Teicoplanin was obtained from Sigma-Aldrich, while tigecycline was obtained from Adooq BioScience. Both antibiotics were dissolved in 90% dimethyl sulfoxide (DMSO).
Bacterial Strains and Culture Media
Mycobacterium abscessus Bamboo (Yee et al., 2017) was used for screening of combinations and the subsequent confirmation of synergy hit combinations. For the checkerboard titration assay determination of the activity of the teicoplanin + tigecycline hit against the various M. abscessus subspecies within the M. abscessus complex, M. abscessus subsp. abscessus (ATCC 19977), M. abscessus subsp. bolletii (CCUG 50184-T) and M. abscessus subsp. massiliense (CCUG 48898-T) were used. Reference strains were obtained from the American Type Culture Collection (ATCC) and the Culture Collection University of Goteborg (CCUG), respectively. For further characterization of the teicoplanin + tigecycline combination in the macrolide resistance induction assay, M. abscessus subsp. abscessus (ATCC 19977) harboring the T28 sequevar of erm41 gene, conferring inducible resistance upon exposure to sub-inhibitory concentrations of macrolides (Nash et al., 2009; Bastian et al., 2011) was used. For determination of synergy of teicoplanin + tigecycline against a variety of clinical isolates, strains were obtained from the strain collection of the clinical microbiology laboratory at the National University Hospital, Singapore. The strains were characterized by the lab as previously described (Aziz et al., 2017). For the evaluation of the bactericidal activity of the synergy combination M. abscessus subsp. abscessus (ATCC 19977) was used.
Liquid cultures were grown in standard mycobacterium medium, Middlebrook 7H9 broth (BD Difco) supplemented with 0.5% albumin, 0.2% glucose, 0.085% sodium chloride, 0.0003% catalase, 0.2% glycerol and 0.05% Tween 80. Solid cultures were grown on Middlebrook 7H10 agar (BD Difco) supplemented with 0.5% albumin, 0.2% glucose, 0.085% sodium chloride, 0.5% glycerol, 0.0003% catalase and 0.006% oleic acid.
Mycobacterium abscessus bacterial work was carried out under BSL-2 conditions according to approved biosafety protocols.
Checkerboard Titration Assay
This assay was carried out in 96-well microtiter plates as previously described (Hsieh et al., 1993; Kaushik et al., 2015), with some modifications. Drugs were tested within the range of concentrations of either 0–25 μM or 0–50 μM, at twofold serial dilutions. For each combination, 8 concentrations of a drug were tested for synergy against 11 concentrations of another drug. Hence, for each two-drug combination screened for synergy, 88 different combination concentrations are tested. A total of 180 different two-drug combinations were tested in this study. For the screening of combinations, this assay was carried out using the Tecan D300e Digital Dispenser for dispensing of drugs. For confirmation of the teicoplanin + tigecycline hit, as well as its subsequent characterization against sub-species, clinical isolates and induced cultures, drugs were dispensed manually. Results were reproducible between the two methods of dispensing drugs for this assay. Briefly, this assay was carried out in 96-well flat bottom plates, with two different compounds, with a starting inoculum of an optical density at 600 nm (OD600) of 0.05 (107 colony forming units or cfu/mL) in a final volume of 200 μL. The culture for the starting inoculum was diluted from a pre-culture at mid-log phase (OD600 = 0.4 to 0.6). The plates were sealed using parafilm, put in an airtight container with moist tissue and incubated for 3 days at 37°C on an orbital shaker at 110 rpm. Each plate had a media-only control, a drug free control as well as a positive control of clarithromycin at 20 μM. After 3 days of incubation, the cultures in the wells were manually re-suspended before OD600 was read in the plate reader (Tecan Infinite 200 Pro) and used to calculate growth inhibition percentage of each well. The Fractional Inhibitory Concentration Index (FICI) was used to analyze the results from the checkerboard assay. FICI was calculated by using the concentrations at which at least 90% inhibition of the culture in the well as compared to the drug free culture was observed. It was computed as FICI = [(concentration of drug A in combination/concentration of drug A when used alone) + (concentration of drug B in combination/concentration of drug B when used alone)] (Hsieh et al., 1993). Synergy is defined as FICI ≤ 0.5, indifference is defined as 0.5 < FICI ≤ 4, and antagonism is defined as FICI > 4 (Hsieh et al., 1993).
Macrolide Resistance Induction Assay
M. abscessus subsp. abscessus (ATCC 19977) mid-log phase culture was diluted to OD600 = 0.05 and treated with clarithromycin at a sub-inhibitory concentration of 0.075 μM (fourfold lower than clarithromycin MIC50 (concentration that causes 50% growth inhibition). An untreated culture was set up as a control. Cultures were grown to mid-log phase overnight and then subjected to the checkerboard titration assay as described above.
Bactericidal Assay
Bactericidal activity determinations were carried out in 14 mL round bottom tubes with the compounds added at set concentrations, with a starting inoculum of OD600 0.05 (107 cfu/mL) in a final volume of 1 mL. The culture for the starting inoculum was diluted from a pre-culture at mid-log phase (OD600 = 0.4 to 0.6). Tubes were incubated for 3 days at 37°C with shaking at 160 rpm. After 3 days of drug exposure, 10 μL of the cultures were plated at different dilutions in 12 well plates containing 2 mL of 7H10 agar in each well. The plates were sealed with parafilm and incubated at 37°C for 4 days and then colonies were counted. We report fold-kill, which is the reduction in cfu/mL of the treated culture compared to the time zero untreated control.
Results
Screening of 180 Two-Drug Combinations for Synergy Against M. abscessus Identifies 11 Hits
We screened a total of 180 two-drug combinations of approved antibiotics for their growth inhibition potency against the clinical isolate M. abscessus Bamboo using the checkerboard assay. Hits were defined as combinations that showed at least a fourfold decrease in concentration of each drug that was needed to achieve 90% inhibition as compared to the concentration needed to achieve that same level of inhibition when either drug was used alone. Screening of β-lactam – β-lactamase inhibitor combinations, identified 6 hits out of 110 combinations (Table 1). Screening of combinations of cell envelope targeting drugs with antibiotics that inhibit intracellular targets, identified 5 hits out of 70 combinations (Table 2). Taken together, the screen identified 11 primary hits (6.1% hit rate) which were re-confirmed with fresh solids (Table 3).
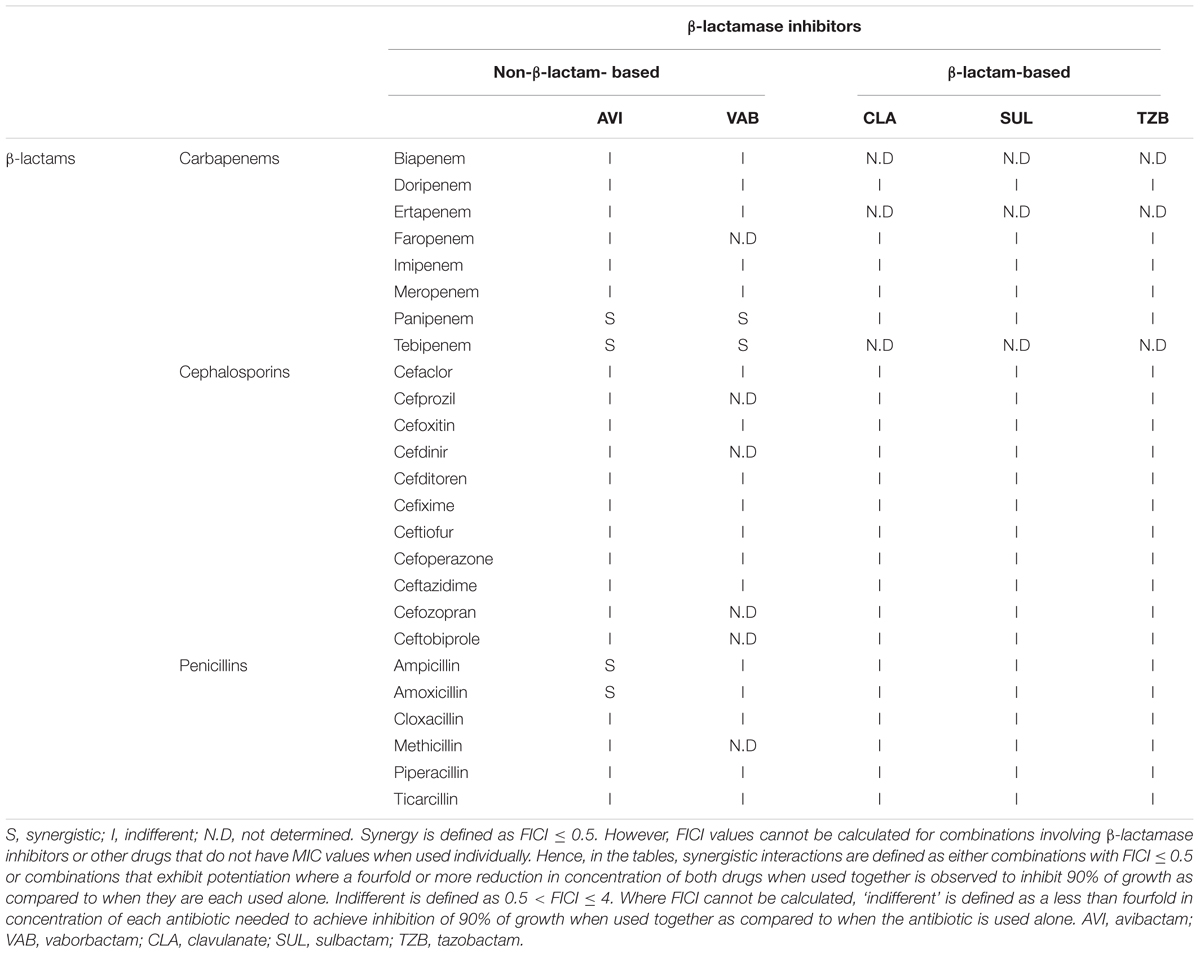
TABLE 1. Outcome of screening 110 combinations of β-lactams and β-lactamase inhibitors against Mycobacterium abscessus Bamboo: 6 two-drug hits.
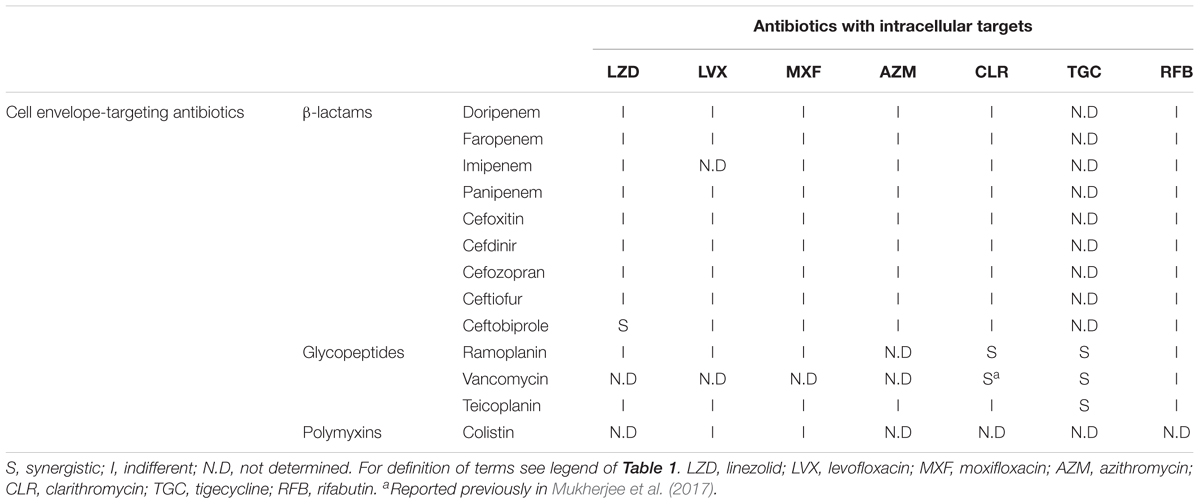
TABLE 2. Outcome of screening 70 combinations of cell envelope-targeting antibiotics with antibiotics targeting intracellular targets against M. abscessus Bamboo: 5 synergistic two-drug hits.
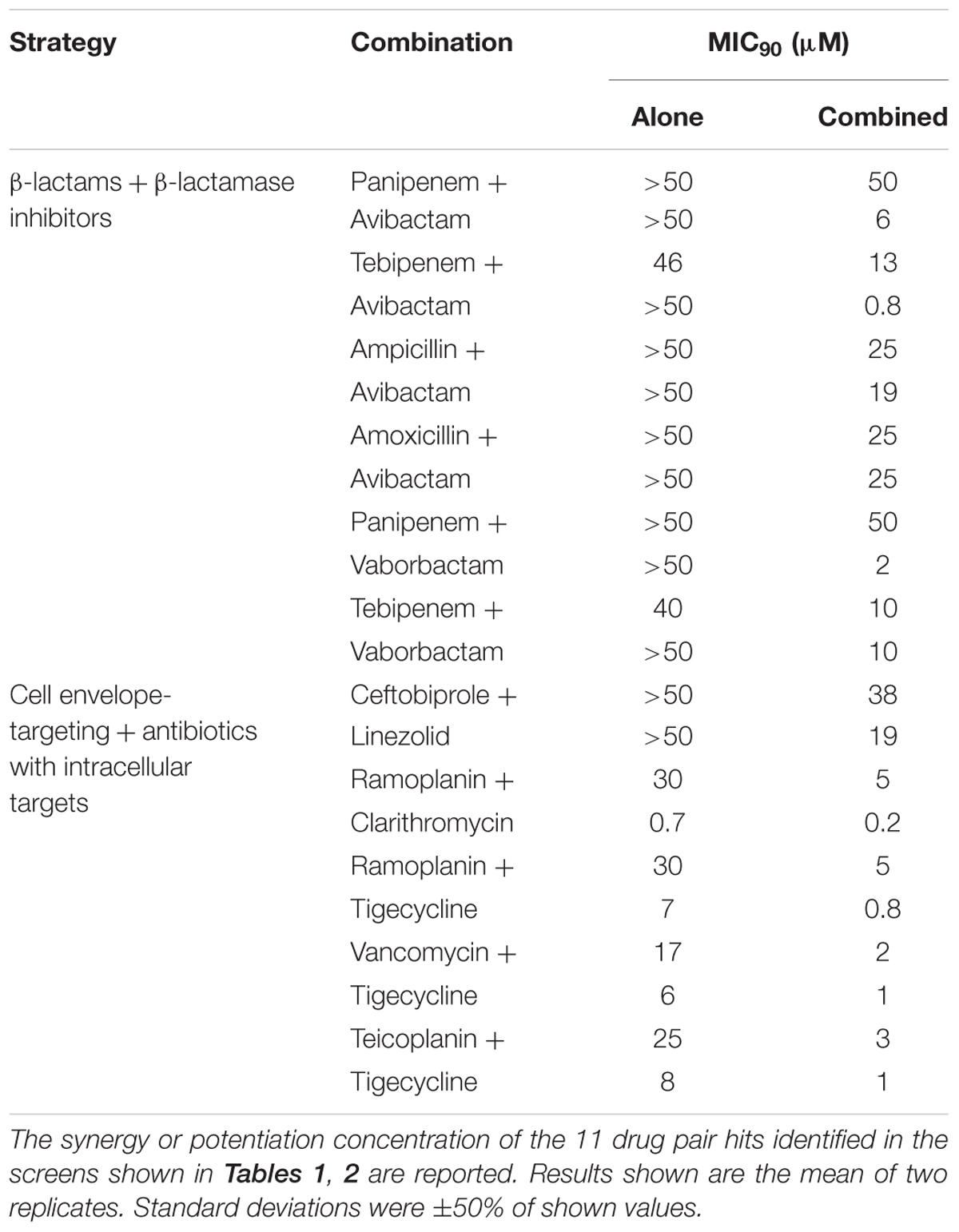
TABLE 3. Reconfirmation of 11 two-drug hits identified from screening of 180 combinations against M. abscessus Bamboo.
Three of our combination hits, panipenem + avibactam, tebipenem + avibactam, and amoxicillin + avibactam were reported previously (Dubee et al., 2015a; Kaushik et al., 2017).
Out of our eight novel hits, the potencies of ampicillin + avibactam, panipenem + vaborbactam, tebipenem + vaborbactam, and ceftobiprole + linezolid were only modest, with MIC90 (concentrations that inhibit 90% of growth) of 25 + 19 μM, 50 + 2 μM, 10 + 10 μM, and 38 + 19 μM (Table 3).
One of our novel hits involved the glycopeptide ramoplanin in combination with clarithromycin, however, this is not unexpected since we had previously reported synergy between the glycopeptide vancomycin with clarithromycin (Mukherjee et al., 2017).
Three novel hits showed encouraging synergy effects: Ramoplanin + tigecycline, vancomycin + tigecycline and teicoplanin + tigecycline inhibited growth at 5 + 0.8 μM, 2 + 1 μM and 3 + 1 μM, respectively (Table 3). Ramoplanin, vancomycin, and teicoplanin are all glycopeptides. Ramoplanin is not well absorbed and unstable in the bloodstream due to hydrolysis of the lactone bond (Farver et al., 2005). This makes ramoplanin unsuitable to repurpose for use in treatment of M. abscessus lung infections. As teicoplanin shows systemic exposure upon intravenous or intramuscular administration and has been reported to have a better safety and efficacy profile compared to vancomycin (Svetitsky et al., 2009), we characterized the activity of teicoplanin in combination with the glycylcycline tigecycline in more detail.
Teicoplanin + Tigecycline Displays Activity Against Reference Strains Representing the Three Subspecies of the M. abscessus Complex
To determine whether the teicoplanin + tigecycline combination shows similar attractive potency across the three subspecies of the M. abscessus complex, we carried out the checkerboard titration assay to determine the FICI value of the combination against the reference strains M. abscessus subsp. abscessus ATCC 19977, M. abscessus subsp. bolletii CCUG 50184-T and M. abscessus subsp. massiliense CCUG 48898-T. The teicoplanin + tigecycline combination was synergistic against all three subspecies (Table 4). These results suggest that this novel combination is active across the phylogenetically divergent M. abscessus complex.
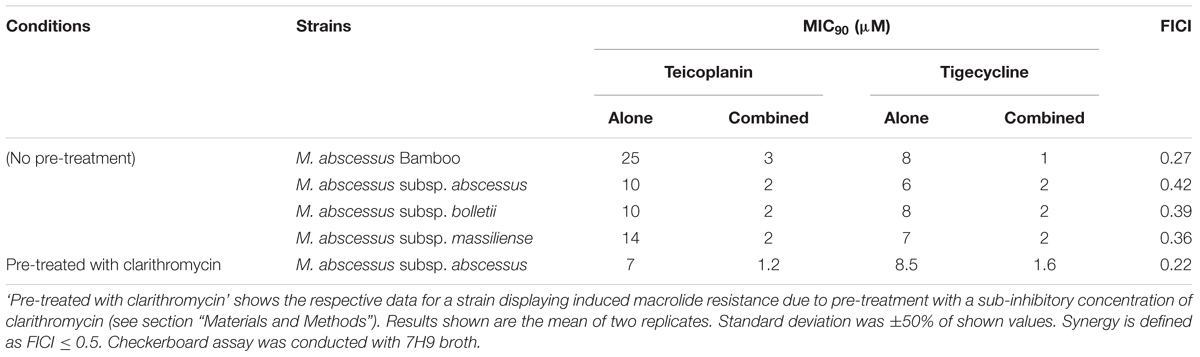
TABLE 4. Synergy concentrations and FICI values of teicoplanin + tigecycline combination against M. abscessus screening strain and three reference strains of the M. abscessus sub-species.
Teicoplanin + Tigecycline Retains Its Activity Against M. abscessus subsp. abscessus ATCC 19977 Cultures Displaying Induced Macrolide Resistance
The checkerboard titration assay was performed using M. abscessus subsp. abscessus ATCC 19977 cultures that had been exposed to a sub-inhibitory concentration of clarithromycin to induce macrolide resistance to determine whether the teicoplanin + tigecycline combination retains its activity under these conditions. The combination still exhibited synergy against the culture with induced macrolide resistance as seen by its FICI value of 0.22 (Table 4).
Teicoplanin + Tigecycline Shows Potent Activity Against M. abscessus Clinical Isolates
The teicoplanin + tigecycline combination showed potent growth inhibition activity against the screening strain as well as the reference strains representing the three subspecies of M. abscessus. This suggests that most clinical M. abscessus strains may be susceptible to this combination. To provide evidence for a widespread susceptibility of M. abscessus to the teicoplanin + tigecycline combination, we tested its activity against a collection of clinical isolates covering various subspecies of M. abscessus, including clarithromycin resistant as well as clarithromycin sensitive strains. The combination displayed synergy against 70.4% of the isolates with FICI values ranging from 0.32 to 0.48 (Table 5). This result indicates that this combination is active against a large number of M. abscessus isolates.
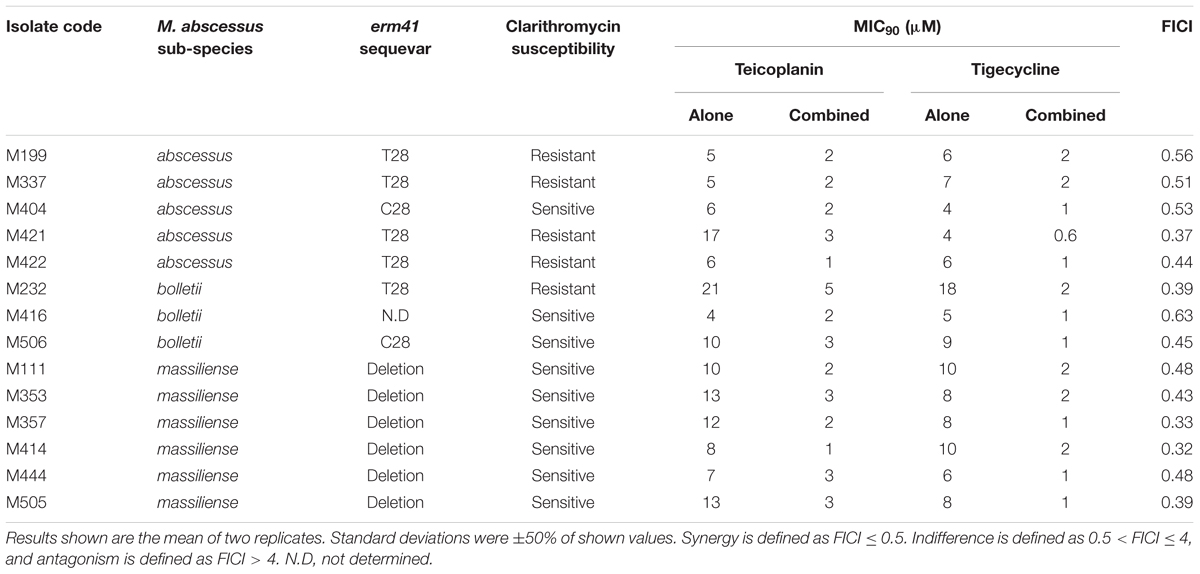
TABLE 5. Synergy concentrations and FICI values of the teicoplanin + tigecycline combination against 14 clinical M. abscessus isolates.
Teicoplanin + Tigecycline Is Not Bactericidal Against M. abscessus subsp. abscessus ATCC 19977
To determine whether the teicoplanin + tigecycline combination shows bactericidal activity against M. abscessus, cultures were treated with the drug combination and the effect on viability was determined by cfu enumeration as described in Section “Materials and Methods.” The teicoplanin + tigecycline combination showed no bactericidal activity.
Discussion
A synergy screen of 180 dual antibiotic combinations against M. abscessus yielded a total of 11 hits. Six hits were obtained from combinations of β-lactams with β-lactamase inhibitors, and five hits from combinations of cell wall-targeting antibiotics with antibiotics that have intracellular targets.
From the analyses of combinations of β-lactams with β-lactamase inhibitors, the most striking observation is that all six hits involved a non-β-lactam-based β-lactamase inhibitor. 4 out of the 6 hits involved avibactam. This is consistent with previous reports showing that this inhibitor is effective against M. abscessusβ-lactamases (Ehmann et al., 2012; Soroka et al., 2014; Dubee et al., 2015a; Kaushik et al., 2017). The remaining 2 hits involved the novel non-β-lactam-based β-lactamase inhibitor vaborbactam, which has not been previously studied for activity against M. abscessus β-lactamases. Activity of avibactam and now vaborbactam suggests that it may be worthwhile to characterize other types of non-β-lactam β-lactamase inhibitors like phosphonates, hydroxamates, or vanadate-catechol complexes, in combination with β-lactams for any potentiation effect of the combinations against M. abscessus (Bebrone et al., 2010).
It is to note that out of the three sub-classes of β-lactams we tested, avibactam appears not to improve the activity of cephalosporins, in contrast to a previous report describing potentiation between ceftaroline and avibactam against M. abscessus (Dubee et al., 2015b). A recent study by Kaushik et al. (2017) which focused on combinations of avibactam, sulbactam and tazobactam with carbapenems against M. abscessus reported 3 hits, with potentiation observed for combinations of avibactam with ertapenem, tebipenem, or panipenem (Kaushik et al., 2017). In this study, we could confirm potentiation for combinations of avibactam with tebipenem or panipenem, however, we did not observe any potentiation between avibactam and ertapenem. Another study found potentiation between clavulanate and meropenem, which we also did not observe (Kaushik et al., 2015). The reasons for these discrepancies remain to be determined (Fisher et al., 2005). One possible explanation may be the use of different M. abscessus strains. This study used the clinical isolate M. abscessus Bamboo in the initial screening, while other studies used other strains including M. abscessus subsp. abscessus ATCC19977. In comparison to avibactam, vaborbactam improved the activity of selected compounds only from the carbapenems but not from the penicillins.
Vaborbactam is a new β-lactamase inhibitor and is the first one to contain a cyclic boronic acid structure (Lomovskaya et al., 2017). Despite its difference in structure from avibactam, both β-lactamase inhibitors were able to potentiate the activity of the same two carbapenems, panipenem and tebipenem. Panipenem is an earlier carbapenem and the drug needs to be administered together with betamipron to block its deactivation by dehydropeptidase I (Papp-Wallace et al., 2011). Tebipenem is a more recently discovered carbapenem and is the first oral drug of this class (Papp-Wallace et al., 2011).
From the analyses of combinations of cell wall-targeting antibiotics with drugs that have intracellular targets, we obtained five novel hits, with the teicoplanin + tigecycline combination being most attractive. Teicoplanin + tigecycline combination displayed synergy at a similar range across reference strains representing the three subspecies of M. abscessus with growth inhibitory combination concentrations of 2–3 μM teicoplanin + 1–2 μM tigecycline. The combination also retained activity against most clinical isolates. A limitation of the combinations tested in this category is, that we only tested combinations of tigecycline with glycopeptides and not with other classes of cell wall-targeting antibiotics such as β-lactams, and this should be explored in future studies.
Teicoplanin is a glycopeptide and acts by interacting with the D-ala-D-ala terminal of the muramyl-pentapeptide which results in inhibition of the cell wall peptidoglycan synthesis (Parenti, 1986). The drug is reported to have good tissue and cellular penetration (Parenti, 1986). Teicoplanin was found to have lower adverse event rates compared to the glycopeptide vancomycin (Svetitsky et al., 2009). Tigecycline is a glycylcycline acting via inhibiting protein synthesis (Olson et al., 2006). Both teicoplanin and tigecycline are administered intravenously, which may limit their application. However, it is noteworthy that despite this limitation tigecycline is used to treat M. abscessus infections (Wallace et al., 2014). The exact molecular mechanism by which the synergistic combination of teicoplanin + tigecycline exerts its activity remains to be determined. Tigecycline may have limited ability to penetrate the bacterium to gain access to its intracellular target. One may speculate that with the administration of teicoplanin together with tigecycline, teicoplanin is able to ‘weaken’ the bacterial cell wall and allow greater penetration of tigecycline into the bacterium.
Conclusion
This study has identified teicoplanin + tigecycline as a novel synergistic combination against M. abscessus in vitro. The drug pair can now be tested in M. abscessus animal models of infection and/or in patients.
Author Contributions
DA, VD, and TD conceived the idea, developed the strategy, and wrote the manuscript. DA carried out the experiments. JT provided and characterized the clinical isolates.
Funding
Research reported in this publication was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under Award Number R01AI132374 and by the Cystic Fibrosis Foundation under Award Number DICK17XX00 to TD. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Cystic Fibrosis Foundation. This research was also supported by the Singapore Ministry of Health National Medical Research Council under its TCR Flagship grant NMRC/TCR/011-NUHS/2014 as part of the Singapore Programme of Research Investigating New Approaches to Treatment of Tuberculosis (SPRINT-TB; www.sprinttb.org). TD holds a Toh Chin Chye Visiting Professorship at the Department of Microbiology and Immunology, Yong Loo Lin School of Medicine, National University of Singapore.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Wei Chang Huang, Taichung Veterans General Hospital, Taichung, Taiwan for the M. abscessus Bamboo strain.
References
Aziz, D. B., Low, J. L., Wu, M. L., Gengenbacher, M., Teo, J. W. P., Dartois, V., et al. (2017). Rifabutin is active against Mycobacterium abscessus complex. Antimicrob. Agents Chemother. 61:e00155-17. doi: 10.1128/AAC.00155-17
Bastian, S., Veziris, N., Roux, A. L., Brossier, F., Gaillard, J. L., Jarlier, V., et al. (2011). Assessment of clarithromycin susceptibility in strains belonging to the Mycobacterium abscessus group by erm(41) and rrl sequencing. Antimicrob. Agents Chemother. 55, 775–781. doi: 10.1128/AAC.00861-10
Bebrone, C., Lassaux, P., Vercheval, L., Sohier, J. S., Jehaes, A., Sauvage, E., et al. (2010). Current challenges in antimicrobial chemotherapy: focus on ss-lactamase inhibition. Drugs 70, 651–679. doi: 10.2165/11318430-000000000-00000
Benwill, J. L., and Wallace, R. J. Jr. (2014). Mycobacterium abscessus: challenges in diagnosis and treatment. Curr. Opin. Infect. Dis. 27, 506–510. doi: 10.1097/QCO.0000000000000104
Brown-Elliott, B. A., Nash, K. A., and Wallace, R. J. Jr. (2012). Antimicrobial susceptibility testing, drug resistance mechanisms, and therapy of infections with nontuberculous mycobacteria. Clin. Microbiol. Rev. 25, 545–582. doi: 10.1128/CMR.05030-11
Bryant, J. M., Grogono, D. M., Rodriguez-Rincon, D., Everall, I., Brown, K. P., Moreno, P., et al. (2016). Emergence and spread of a human-transmissible multidrug-resistant nontuberculous mycobacterium. Science 354, 751–757. doi: 10.1126/science.aaf8156
Cremades, R., Santos, A., Rodriguez, J. C., Garcia-Pachon, E., Ruiz, M., and Royo, G. (2009). Mycobacterium abscessus from respiratory isolates: activities of drug combinations. J. Infect. Chemother. 15, 46–48. doi: 10.1007/s10156-008-0651-y
Dubee, V., Bernut, A., Cortes, M., Lesne, T., Dorchene, D., Lefebvre, A. L., et al. (2015a). beta-Lactamase inhibition by avibactam in Mycobacterium abscessus. J. Antimicrob. Chemother. 70, 1051–1058. doi: 10.1093/jac/dku510
Dubee, V., Soroka, D., Cortes, M., Lefebvre, A. L., Gutmann, L., Hugonnet, J. E., et al. (2015b). Impact of beta-lactamase inhibition on the activity of ceftaroline against Mycobacterium tuberculosis and Mycobacterium abscessus. Antimicrob. Agents Chemother. 59, 2938–2941. doi: 10.1128/AAC.05080-14
Ehmann, D. E., Jahic, H., Ross, P. L., Gu, R. F., Hu, J., Kern, G., et al. (2012). Avibactam is a covalent, reversible, non-beta-lactam beta-lactamase inhibitor. Proc. Natl. Acad. Sci. U.S.A. 109, 11663–11668. doi: 10.1073/pnas.1205073109
Farver, D. K., Hedge, D. D., and Lee, S. C. (2005). Ramoplanin: a lipoglycodepsipeptide antibiotic. Ann. Pharmacother. 39, 863–868. doi: 10.1345/aph.1E397
Ferro, B. E., Srivastava, S., Deshpande, D., Pasipanodya, J. G., van Soolingen, D., Mouton, J. W., et al. (2016). Failure of the amikacin, cefoxitin, and clarithromycin combination regimen for treating pulmonary Mycobacterium abscessus infection. Antimicrob. Agents Chemother. 60, 6374–6376. doi: 10.1128/AAC.00990-16
Fisher, J. F., Meroueh, S. O., and Mobashery, S. (2005). Bacterial resistance to beta-lactam antibiotics: compelling opportunism, compelling opportunity. Chem. Rev. 105, 395–424. doi: 10.1021/cr030102i
Floto, R. A., Olivier, K. N., Saiman, L., Daley, C. L., Herrmann, J. L., Nick, J. A., et al. (2016). US cystic fibrosis foundation and European cystic fibrosis society consensus recommendations for the management of non-tuberculous mycobacteria in individuals with cystic fibrosis. Thorax 71(Suppl. 1), i1–i22. doi: 10.1136/thoraxjnl-2015-207360
Griffith, D. E., Aksamit, T., Brown-Elliott, B. A., Catanzaro, A., Daley, C., Gordin, F., et al. (2007). An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 175, 367–416. doi: 10.1164/rccm.200604-571ST
Hill, J. A., and Cowen, L. E. (2015). Using combination therapy to thwart drug resistance. Future Microbiol. 10, 1719–1726. doi: 10.2217/fmb.15.68
Hoefsloot, W., van Ingen, J., Andrejak, C., Angeby, K., Bauriaud, R., Bemer, P., et al. (2013). The geographic diversity of nontuberculous mycobacteria isolated from pulmonary samples: an NTM-NET collaborative study. Eur. Respir. J. 42, 1604–1613. doi: 10.1183/09031936.00149212
Hsieh, M. H., Yu, C. M., Yu, V. L., and Chow, J. W. (1993). Synergy assessed by checkerboard. A critical analysis. Diagn. Microbiol. Infect. Dis. 16, 343–349.
Huang, C. W., Chen, J. H., Hu, S. T., Huang, W. C., Lee, Y. C., Huang, C. C., et al. (2013). Synergistic activities of tigecycline with clarithromycin or amikacin against rapidly growing mycobacteria in Taiwan. Int. J. Antimicrob. Agents 41, 218–223. doi: 10.1016/j.ijantimicag.2012.10.021
Kaushik, A., Gupta, C., Fisher, S., Story-Roller, E., Galanis, C., Parrish, N., et al. (2017). Combinations of avibactam and carbapenems exhibit enhanced potencies against drug-resistant Mycobacterium abscessus. Future Microbiol. 12, 473–480. doi: 10.2217/fmb-2016-0234
Kaushik, A., Makkar, N., Pandey, P., Parrish, N., Singh, U., and Lamichhane, G. (2015). Carbapenems and rifampin exhibit synergy against Mycobacterium tuberculosis and Mycobacterium abscessus. Antimicrob. Agents Chemother. 59, 6561–6567. doi: 10.1128/AAC.01158-15
Livermore, D. M. (1995). beta-Lactamases in laboratory and clinical resistance. Clin. Microbiol. Rev. 8, 557–584.
Lomovskaya, O., Sun, D., Rubio-Aparicio, D., Nelson, K., Tsivkovski, R., Griffith, D. C., et al. (2017). Vaborbactam: spectrum of beta-lactamase inhibition and impact of resistance mechanisms on activity in Enterobacteriaceae. Antimicrob. Agents Chemother. 61:e01443-17. doi: 10.1128/AAC.01443-17
Maurer, F. P., Castelberg, C., Quiblier, C., Bottger, E. C., and Somoskovi, A. (2014). Erm(41)-dependent inducible resistance to azithromycin and clarithromycin in clinical isolates of Mycobacterium abscessus. J. Antimicrob. Chemother. 69, 1559–1563. doi: 10.1093/jac/dku007
Medjahed, H., Gaillard, J. L., and Reyrat, J. M. (2010). Mycobacterium abscessus: a new player in the mycobacterial field. Trends Microbiol. 18, 117–123. doi: 10.1016/j.tim.2009.12.007
Miyasaka, T., Kunishima, H., Komatsu, M., Tamai, K., Mitsutake, K., Kanemitsu, K., et al. (2007). In vitro efficacy of imipenem in combination with six antimicrobial agents against Mycobacterium abscessus. Int. J. Antimicrob. Agents 30, 255–258. doi: 10.1016/j.ijantimicag.2007.05.003
Mukherjee, D., Wu, M. L., Teo, J. W. P., and Dick, T. (2017). Vancomycin and clarithromycin show synergy against Mycobacterium abscessus in vitro. Antimicrob. Agents Chemother. 61:e01298-17. doi: 10.1128/AAC.01298-17
Nash, K. A., Brown-Elliott, B. A., and Wallace, R. J. Jr. (2009). A novel gene, erm(41), confers inducible macrolide resistance to clinical isolates of Mycobacterium abscessus but is absent from Mycobacterium chelonae. Antimicrob. Agents Chemother. 53, 1367–1376. doi: 10.1128/AAC.01275-08
Nessar, R., Cambau, E., Reyrat, J. M., Murray, A., and Gicquel, B. (2012). Mycobacterium abscessus: a new antibiotic nightmare. J. Antimicrob. Chemother. 67, 810–818. doi: 10.1093/jac/dkr578
Oh, C. T., Moon, C., Park, O. K., Kwon, S. H., and Jang, J. (2014). Novel drug combination for Mycobacterium abscessus disease therapy identified in a Drosophila infection model. J. Antimicrob. Chemother. 69, 1599–1607. doi: 10.1093/jac/dku024
Olson, M. W., Ruzin, A., Feyfant, E., Rush, T. S., O’Connell, J., and Bradford, P. A. (2006). Functional, biophysical, and structural bases for antibacterial activity of tigecycline. Antimicrob. Agents Chemother. 50, 2156–2166. doi: 10.1128/AAC.01499-05
Papp-Wallace, K. M., Endimiani, A., Taracila, M. A., and Bonomo, R. A. (2011). Carbapenems: past, present, and future. Antimicrob. Agents Chemother. 55, 4943–4960. doi: 10.1128/AAC.00296-11
Parenti, F. (1986). Structure and mechanism of action of teicoplanin. J. Hosp. Infect. 7(Suppl. A), 79–83.
Ryu, Y. J., Koh, W. J., and Daley, C. L. (2016). Diagnosis and treatment of nontuberculous mycobacterial lung disease: clinicians’ perspectives. Tuberc. Respir. Dis. 79, 74–84. doi: 10.4046/trd.2016.79.2.74
Shen, G. H., Wu, B. D., Hu, S. T., Lin, C. F., Wu, K. M., and Chen, J. H. (2010). High efficacy of clofazimine and its synergistic effect with amikacin against rapidly growing mycobacteria. Int. J. Antimicrob. Agents 35, 400–404. doi: 10.1016/j.ijantimicag.2009.12.008
Singh, S., Bouzinbi, N., Chaturvedi, V., Godreuil, S., and Kremer, L. (2014). In vitro evaluation of a new drug combination against clinical isolates belonging to the Mycobacterium abscessus complex. Clin. Microbiol. Infect. 20, O1124–O1127. doi: 10.1111/1469-0691.12780
Soroka, D., Dubee, V., Soulier-Escrihuela, O., Cuinet, G., Hugonnet, J. E., Gutmann, L., et al. (2014). Characterization of broad-spectrum Mycobacterium abscessus class A beta-lactamase. J. Antimicrob. Chemother. 69, 691–696. doi: 10.1093/jac/dkt410
Svetitsky, S., Leibovici, L., and Paul, M. (2009). Comparative efficacy and safety of vancomycin versus teicoplanin: systematic review and meta-analysis. Antimicrob. Agents Chemother. 53, 4069–4079. doi: 10.1128/AAC.00341-09
van Ingen, J., Totten, S. E., Helstrom, N. K., Heifets, L. B., Boeree, M. J., and Daley, C. L. (2012). In vitro synergy between clofazimine and amikacin in treatment of nontuberculous mycobacterial disease. Antimicrob. Agents Chemother. 56, 6324–6327. doi: 10.1128/AAC.01505-12
Wallace, R. J. Jr., Dukart, G., Brown-Elliott, B. A., Griffith, D. E., Scerpella, E. G., and Marshall, B. (2014). Clinical experience in 52 patients with tigecycline-containing regimens for salvage treatment of Mycobacterium abscessus and Mycobacterium chelonae infections. J. Antimicrob. Chemother. 69, 1945–1953. doi: 10.1093/jac/dku062
Keywords: Mycobacterium abscessus, teicoplanin, tigecycline, synergy, repurposing
Citation: Aziz DB, Teo JWP, Dartois V and Dick T (2018) Teicoplanin – Tigecycline Combination Shows Synergy Against Mycobacterium abscessus. Front. Microbiol. 9:932. doi: 10.3389/fmicb.2018.00932
Received: 27 February 2018; Accepted: 23 April 2018;
Published: 11 May 2018.
Edited by:
Farhat Afrin, Taibah University, Saudi ArabiaReviewed by:
Yusuf Akhter, Babasaheb Bhimrao Ambedkar University, IndiaAnna D. Tischler, University of Minnesota, United States
Gyanu Lamichhane, Johns Hopkins Medicine, United States
Copyright © 2018 Aziz, Teo, Dartois and Dick. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thomas Dick, td367@njms.rutgers.edu