Cerebellar Continuous Theta Burst Stimulation for Aphasia Rehabilitation: Study Protocol for a Randomized Controlled Trial
 Kai Zheng1,2,3†
Kai Zheng1,2,3†  Mingyun Chen1† Ying Shen4† Xinlei Xu2,3 Fanglan Gao2,3
Mingyun Chen1† Ying Shen4† Xinlei Xu2,3 Fanglan Gao2,3  Guilan Huang2,3
Guilan Huang2,3  Yingying Ji2,3 Bin Su2,3 Da Song2,3 Hui Fang2,3 Peng Liu1*
Yingying Ji2,3 Bin Su2,3 Da Song2,3 Hui Fang2,3 Peng Liu1*  Caili Ren2,3*
Caili Ren2,3*- 1Department of Rehabilitation Medicine, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China
- 2Department of Neurorehabilitation, Wuxi Tongren Rehabilitation Hospital, Wuxi, China
- 3The Affiliated Wuxi Mental Health Center of Nanjing Medical University, Wuxi, China
- 4Rehabilitation Medicine Center, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China
Background: Language recovery is limited in moderate to severe post-stroke aphasia patients. Repetitive transcranial magnetic stimulation (rTMS) has emerged as a promising tool in improving language dysfunctions caused by post-stroke aphasia, but the treatment outcome is as yet mixed. Considerable evidence has demonstrated the essential involvement of the cerebellum in a variety of language functions, suggesting that it may be a potential stimulation target of TMS for the treatment of post-stroke aphasia. Theta burst stimulation (TBS) is a specific pattern of rTMS with shorter stimulation times and better therapeutic effects. The effect of continuous TBS (cTBS) on the cerebellum in patients with aphasia with chronic stroke needs further exploration.
Methods: In this randomized, sham-controlled clinical trial, patients (n = 40) with chronic post-stroke aphasia received 10 sessions of real cTBS (n = 20) or sham cTBS (n = 20) over the right cerebellar Crus I+ a 30-min speech-language therapy. The Western Aphasia Battery (WAB) serves as the primary measure of the treatment outcome. The secondary outcome measures include the Boston Diagnostic Aphasia Examination, Boston Naming Test and speech acoustic parameters. Resting-state fMRI data were also obtained to examine treatment-induced changes in functional connectivity of the cerebro-cerebellar network. These outcome measures are assessed before, immediately after, and 12 weeks after cerebellar cTBS intervention.
Discussion: This protocol holds promise that cerebellar cTBS is a potential strategy to improve language functions in chronic post-stroke aphasia. The resting-state fMRI may explore the neural mechanism underlying the aphasia rehabilitation with cerebellar cTBS.
Introduction
Aphasia is an acquired language disorder caused by ischemic or hemorrhagic stroke (Engelter et al., 2006), characterized by impairments in verbal fluency, language comprehension, word repetition, and picture naming as well as reading/writing skills. Approximately, one-third of post-stroke patients develops aphasia (Engelter et al., 2006), which persists in approximate 20% of long-term stroke survivors (Berthier, 2005). Patients with post-stroke aphasia suffer from decreased quality of life, limited independence, and substantial long-term disability (Cruice et al., 2011; Ellis et al., 2012). To date, speech-language therapy (SLT) is considered as the standard protocol for the treatment of post-stroke aphasia and produce beneficial effects on language functions, but the effect size is somewhat small that results in modest improvements (Brady et al., 2012). Therefore, it is important to develop other therapeutic approaches to improve the effectiveness of SLT for aphasia treatment.
In recent years, repetitive transcranial magnetic stimulation (rTMS) has emerged as a promising non-invasive neuromodulation method to augment the treatment of post-stroke non-fluent aphasia (Hartwigsen and Saur, 2017; Fisicaro et al., 2019; Ren et al., 2019). Generally, low-frequency rTMS (≤1 Hz) is considered to decrease cortical excitability, while high-frequency rTMS (≥5 Hz) produces the opposite effect (Chen and Seitz, 2001). The majority of recent studies have shown naming improvements in post-stroke non-fluent aphasia by delivering inhibitory low-frequency rTMS over the intact right inferior frontal gyrus (IFG) (the right hemisphere homolog of Broca’s area) (Hara et al., 2015; Harvey et al., 2017; Ren et al., 2019; Kim et al., 2020). Similar beneficial effects on post-stroke aphasia were also observed when excitatory high-frequency rTMS was applied over the left perilesional cortex (Broca’s area) or right intact IFG (Hara et al., 2017; Hu et al., 2018). Alternatively, applying rTMS over other cortical regions is also beneficial for post-stroke aphasia, as evidenced by improvement in speech perception and auditory comprehension following low-frequency rTMS over the right posterior superior temporal gyrus (pSTG) (Kawamura et al., 2019; Ren et al., 2019). Nevertheless, it is noteworthy that the evidence for beneficial effects of rTMS on post-stroke aphasia is not unequivocal (Breining and Sebastian, 2020). Some studies reported null results when low-frequency rTMS was applied over the right hemisphere, showing that rTMS did not add to the effect of SLT on post-stroke aphasia (Santos et al., 2017; Heikkinen et al., 2018). Among many possible resources of the inconsistencies across the studies investigating the efficacy of rTMS for post-stroke aphasia are type of stimulation modality (inhibitory or excitatory), laterality of brain hemisphere (left or right), and choice of stimulation target (Broca’s area, STG, etc.) (Breining and Sebastian, 2020). Particularly, the optimal protocol of rTMS over the right hemisphere remains controversial for aphasia rehabilitation (Anglade et al., 2014), which is due to the limited knowledge about the causal links between cortical brain regions and language functions. Accordingly, developing a novel stimulation protocol with other potential targets that are significantly involved in language processing is important for improving effectiveness of TMS in augmenting the treatment of post-stroke aphasia.
The present study protocol proposes a research protocol that stimulates the right cerebellum with TMS to augment SLT for patients with post-stroke aphasia. Multiple lines of evidence have demonstrated significant contributions of the right cerebellum to a variety of language functions, including word retrieval and generation, verbal working memory, language learning, and semantic processing (Gordon, 1996; Desmond and Fiez, 1998; Murdoch, 2010; Stoodley, 2012; Mariën and Borgatti, 2018). Clinical evidence has shown deficits in a variety of language tasks as a result of damage to the right cerebellum (Marien et al., 1996, 2001; Silveri et al., 1998). Moreover, a growing body of empirical and clinical studies using transcranial direct current stimulation (tDCS) has established a causal link between the right cerebellum and language functions. For example, applying tDCS over the right cerebellum in healthy individuals exerts modulatory effects on various speech/language tasks, such as verbal generation (Pope and Miall, 2012), verbal fluency (Turkeltaub et al., 2016), semantic prediction (D’Mello et al., 2017), and speech motor learning (Lametti et al., 2018). Clinically, several recent studies showed augmentation of SLT in post-stroke aphasia with tDCS over the right cerebellum (Sebastian et al., 2016, 2020; Marangolo et al., 2018). For example, one randomized, double-blind, sham-controlled study found significant improvement in verbal generation in patients with post-stroke aphasia following 4-week cathodal tDCS over the right cerebellum coupled with SLT (Marangolo et al., 2018). In another randomized, double-blind, sham-controlled study (Sebastian et al., 2020), both cathodal and anodal tDCS over the right cerebellum led to improved picture naming in chronic post-stroke aphasia, while greater gains were noted for patients receiving cathodal cerebellar tDCS. Taken together, these studies provide evidence suggesting that the cerebellum may be an optimal site of neuromodulation for the treatment of post-stroke aphasia.
On the other hand, continuous theta burst stimulation (cTBS) is applied over the right cerebellum in the present study protocol. As a specific form of rTMS, cTBS produces an inhibitory effect on cortical excitability for up to 60 min after less than 1-min of stimulation (Huang et al., 2005). In addition to modulating cerebellar activity (Koch, 2010), cTBS over the right cerebellum exerts modulatory effects on speech/language production (Arasanz et al., 2012; Sheu et al., 2019). Cerebellar TBS is safe and tolerable and has reported no serious adverse effects (Hurtado-Puerto et al., 2020). The previous studies have shown that the cerebellar cTBS modulates motor cortical excitability and improves motor symptoms (e.g., gait ataxia and dyskinesia) in a variety of neurodegenerative diseases, such as Parkinson’s disease (PD) and spinocerebellar ataxia (SCA) (Koch et al., 2009, 2014; Benussi et al., 2020; Maas et al., 2020). Moreover, one recent study on patients with SCA showed that single-session c-TBS over the right cerebellum produces facilitatory effects on their abnormalities in auditory-motor integration for vocal pitch regulation (Lin et al., 2022). Therefore, it is plausible to assume that stimulating the right cerebellum with inhibitory cTBS coupled with SLT leads to beneficial effects on chronic post-stroke aphasia, which is yet to be answered.
To this end, the purpose of the present study is to investigate the short- and long-term effectiveness of cTBS over the right cerebellum in augmenting language recovery in chronic post-stroke aphasia in a randomized, sham-controlled design. In addition to aphasia test batteries and speech acoustic analyses for evaluation of treatment outcome, the resting-state functional magnetic resonance (RS-fMRI) is also used to explore the neural mechanisms underlying aphasia rehabilitation. The previous studies have shown associations between improved spelling or phonemic fluency and increased resting-state functional connectivity between the cerebellum and language-related cortical regions for patients with chronic post-stroke aphasia or healthy individuals following tDCS over the right cerebellum (Sebastian et al., 2016; Turkeltaub et al., 2016). Accordingly, we hypothesize that, following cTBS over the right cerebellum, patients with chronic post-stroke aphasia will exhibit improved language functions and increased functional connectivity within the cerebro-cerebellar language network. This randomized, sham-controlled study provides significant new insights into the therapeutic efficacy of cTBS over the right cerebellum to augment SLT for post-stroke aphasia and the underlying neuroplastic mechanisms.
Methods
Study Design
This is a prospective, randomized, sham-controlled, single-center study (Registration number: ChiCTR210049828) that will be conducted in the Department of Neurorehabilitation, Wuxi Tongren Rehabilitation Hospital, China. Hospitalized patients with chronic post-stroke aphasia are recruited to participate in the study. They are randomly assigned with a ratio of 1:1 to a real or sham stimulation group. Details about the study design and data collection are shown in Figure 1 and Table 1. On the day of enrollment (T0), after the end of cerebellar cTBS intervention (T1), and 12 weeks post-treatment completion (T2), aphasia test batteries and speech acoustic analyses are performed to evaluate language functions in post-stroke aphasia. Also, RS-fMRI data are collected before and after the end of the intervention. This study has been approved by the Ethics Committee of Wuxi Mental Health Center and Wuxi Tongren Rehabilitation Hospital (WXMHCIRB2021LLky078).
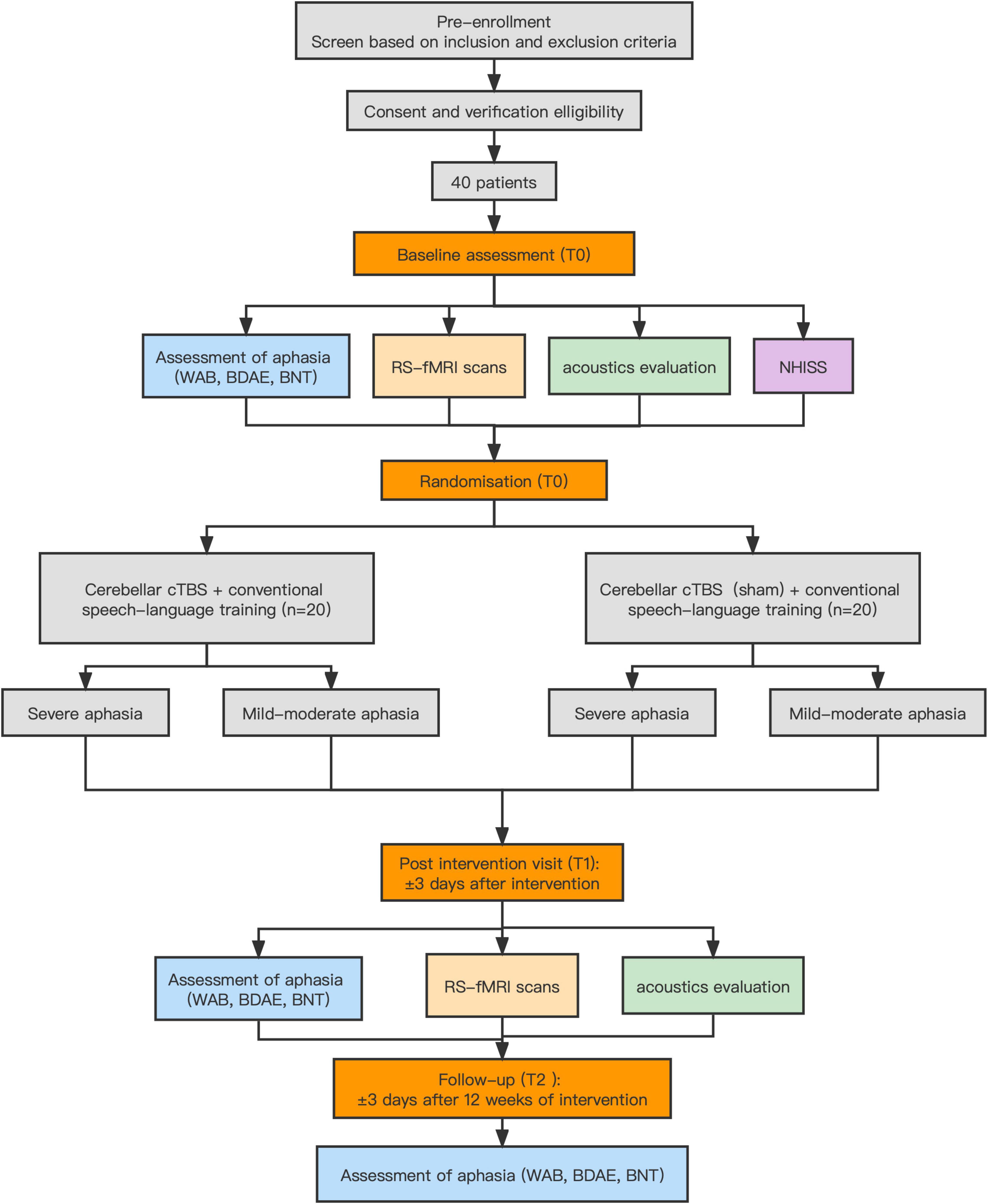
Figure 1. Flow chart of study procedure. cTBS, continuous theta burst stimulation.
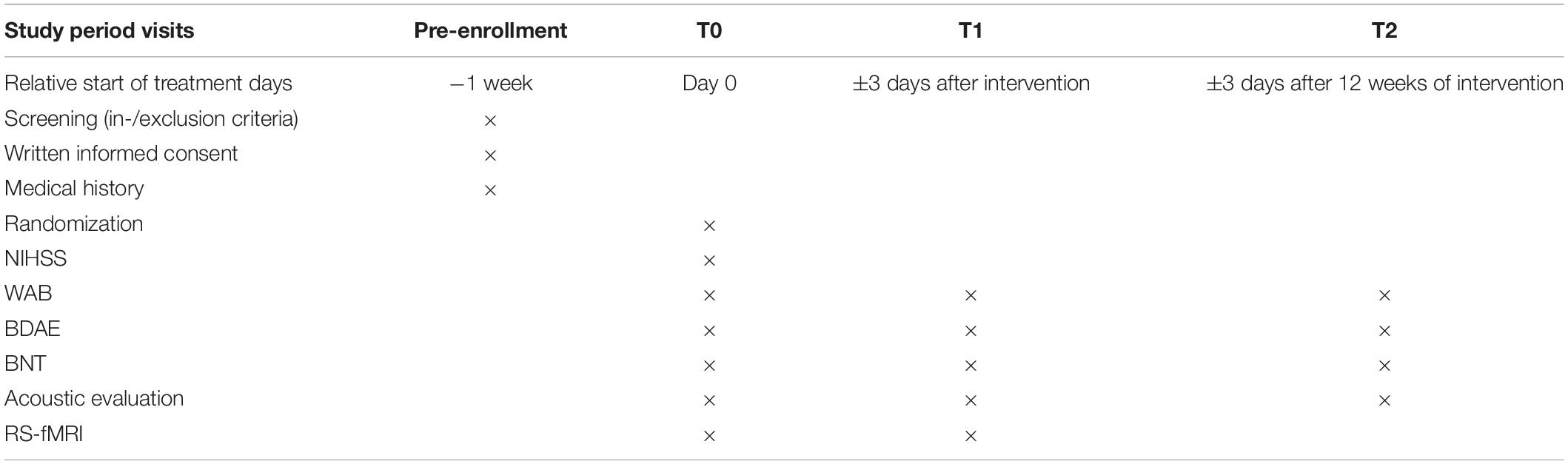
Table 1. Overview of data collection and study timings.
Participants
The inclusion and exclusion criteria of the present study correspond to the guidelines for using rTMS in clinics and research (Wassermann, 1998; Rossi et al., 2009; Rossini et al., 2015). Participant inclusion criteria are: (1) patients aged 40–80 years; (2) first-ever unilateral ischemic stroke on the left hemisphere; (3) longer than 6 months post-stroke; (4) non-fluent aphasia as confirmed by the Western Aphasia Battery (WAB); (5) right-handed, native-Chinese speakers without experience of professional vocal or instrumental training; (6) Boston Diagnostic Aphasia Examination (BDAE) Grades I–III; and (7) elementary education level and above, with normal or corrected to normal vision. Participant exclusion criteria are: (1) history of substance or alcohol abuse, premorbid seizures, or neuropsychiatric diseases; (2) contraindications involving TMS and fMRI (e.g., skull defect or skin damage at the stimulation site, intracranial implant, cardiac pacemaker, and implanted drug pumps); (3) history of neurosurgical treatment; (4) unable to cooperate with assessment and treatment due to severe cognitive impairment; and (5) other neurological disease. All participants provide written informed consent prior to participating in the study.
Sample Size
The sample size was calculated using PASS software (v.15.0) on the basis of previous studies. With an effect size of 0.5 based on the WAB-AQ (Hu et al., 2018), we expect that the target effect size had 80% of power with a type I error of 5% (α = 0.05). Thus, the sample size of each group is at least 16. With an assumption of 20% dropout rate, a sample size of 20 participants will be targeted for each group.
Randomization and Blinding
Once the inclusion criteria are satisfied, the participant is allocated to one real or sham cTBS group using the network-based random sequence generator to receive real or sham cTBS over the right cerebellum coupled with SLT. Based on the previous studies, patients will receive a 10-day cerebellar cTBS within 2 weeks (Thiel et al., 2013; Wang et al., 2014; Hara and Abo, 2021). The concealment of allocation is performed using sealed envelopes with numbers. The participants and physicians performing the SLT or the data collection/processing are blinded to the grouping. Note that physicians conducting the cTBS intervention cannot be blinded due to the nature of the cTBS intervention and are thus not involved in the research process. The designer and the staff responsible for allocation concealment will not participate in the whole intervention.
Interventions
The application of cerebellar cTBS is administered using Magneuro 100 (Vishee Medical Technology Co., Ltd., Nanjing, China) equipped with a figure 8-shaped coil (7 cm out diameter). Before intervention, a single-pulse TMS will be applied over the right primary motor cortex to determine active motor threshold (AMT). The AMT is defined as the lowest stimulus intensity that produces a motor evoked potential (MEP) of >200 μV in at least 5–10 consecutive trials with 10% maximal voluntary contraction of the first dorsal interosseous muscle of the non-paretic hand (Koch et al., 2020). Each participant receives real or sham cTBS over the Crus I of the right lateral cerebellum (3 cm right and 1 cm inferior to the inion) at 80% of AMT (Lin et al., 2022). A standard cTBS protocol consists of bursts of 3 pulses at 50 Hz that are repeatedly presented at 5 Hz, resulting in a total of 600 pulses in 40 s. The coil is oriented vertically to the target with the handle pointing superiorly during real stimulation; while the stimulation face of the coil is turned 90°, so that the side of the coil is placed on the target during sham stimulation (Rastogi et al., 2017). Immediately following real or sham cerebellar cTBS, all participants receive a 30-min SLT that includes training on comprehension, expression of spoken language, semantic, and phonological processing. The content of SLT will be modified based evaluation of language function on an individual level. Totally, each participant receives 10 sessions of cerebellar cTBS coupled with SLT (5 sessions per week) within 2 weeks.
Outcome Measures
The primary outcome measure is the WAB assessment that is divided into four subitems including spontaneous speech, auditory verbal comprehension, repetition, and naming. The original scores of the four items are 20, 200, 100, and 100, respectively. An aphasia quotient (AQ) is calculated using the following formula: AQ = (spontaneous speech + auditory verbal comprehension/20 + repetition/10 + naming/10) × 2. The AQ indicates the severity of aphasia and can be used as an index for evaluating the improvement and deterioration of aphasia. The highest AQ score is 100, and the normal range is 98.4–99.6. AQ <93.8 is considered as aphasia.
In addition to the WAB scores, there are several secondary measures of treatment outcome including BDAE, Boston Naming Test (BNT), speech acoustic parameters, and RS-fMRI. BDAE is used to measure the severity of impaired language function that can be divided into five grades from severe to mild. The BNT is an assessment tool to measure the confrontational word naming of 30 object pictures. The speech acoustic parameters include fundamental frequency, intensity, speaking rate, maximum phonation time, range of voice features, and speech intelligibility. Speech signals are recorded using a laptop at sampling frequency 44.1 K Hz and Praat software is used to extract acoustic parameters.
RS-fMRI data are acquired using a 3.0 T MAGNETOM Skyra scanner (Siemens, Germany). The participants are instructed to lie still with their eyes closed and think of nothing. Functional images are obtained using echo-planar imaging (EPI) pulse sequence with the following parameters: repetition time (TR) = 2,000 ms; echo time (TE) = 30 ms; 35 slices, field of view (FOV) = 224 mm × 224 mm; slice thickness = 3.5 mm; layer spacing 0.7 mm; flip angle (FA) = 90°; acquisition matrix 64 × 64; voxel size = 3.5 mm × 3.5 mm × 3.5 mm. For registration purposes, a set of high-resolution structural images are acquired through a T1-weighted sequence: 192 sagittal slices; slice thickness = 1 mm; TR = 6.6 ms; TE = 3.1 ms; FA = 12°; FOV = 256 mm × 256 mm. The scanning lasted for 8 min and produced 240 brain volumes.
Data Analysis
Repeated-measures analysis of variances (RM-ANOVAs) are performed to examine differences in the WAB, BDAE, and BNT scores as well as speech parameters across the conditions, with a within-subject factor of phase (pre- vs. post-treatment) and a between-subject factor of group (real vs. sham cTBS). In the post hoc analysis, multiple comparisons are corrected with Bonferroni adjustment. Prior to entering the data into the RM-ANOVAs, Kolmogorov–Smirnov test is used to verify whether they are normally distributed. For non-normally distributed measures, the Wilcoxon Signed Rank Test is used for comparison across the conditions. The intention-to-treat (ITT) analysis is used when there are missing data.
The preprocessing of RS-fMRI data is conducted using DPABI software (v. 6.1) on the MATLAB platform (Mathworks, Natick, MA, United States) (Yan et al., 2016). The main steps are as follows: (1) use MRIConvert software (v. 2.1.0, Lewis Center, Eugene, OR, United States) to convert raw data in DICOM format to NIFI format; (2) remove the first 10 slices and correct the remaining 230 slices for slice timing; (3) correct head motion exceeding 3 mm in any direction or head rotation exceeding 3°; (4) spatially normalize the functional images to a standard Montreal Neurological Institute (MNI) space and resample them to a voxel size of 3 mm × 3 mm × 3 mm; (5) apply a band-pass filter (0.01–0.08) for each voxel to reduce the influence of low frequency fluctuation and high-frequency noise (Lv et al., 2018); and (6) smooth the functional data with a 6-mm full width at half maximum (FWHM) Gaussian kernel.
After the preprocessing, regional homogeneity (ReHo), degree centrality (DC), and seed-to-voxel analyses are conducted to measure the local and global functional connectivity within the language networks. ReHo is calculated based on the Kendall’s coefficient of concordance (KCC), which measures the consistency of the time signal between a voxel and surrounding voxels. Higher ReHo values represent better consistency between the local voxel and the regional brain activities. DC values reflect the network connection intensity between a certain voxel and all of the brain, indicating the importance of this voxel as the network node (Zang et al., 2004). One-way ANOVAs are conducted on the ReHo and DC values to explore differences across the conditions within the predefined gray matter mask. The ANOVA F maps are corrected using Gaussian random field (GRF) correction (single voxel p < 0.001, cluster level p < 0.05). The ReHo and DC values of the peak voxels in the surviving clusters are extracted and entered into SPSS (v. 22) for further analysis. Seed-to-voxel analyses are conducted with a priori regions of interest (ROI). The ROIs consist of language-related regions in cerebellar Crus I; IFG pars opercularis; IFG pars triangularis; primary motor cortex (M1); anterior and posterior STG; angular gyrus; anterior and posterior supramarginal gyrus (SMG), which are selected from the AAL atlas (Tzourio-Mazoyer et al., 2002). These ROI-based functional connectivity maps are statistically compared between pre- and post-treatment and between real cTBS and sham stimulation group. Differences across the conditions are considered significant when p < 0.05 at the voxel level, with a false discovery rate (FDR) cluster corrected p < 0.05.
Safety
Adverse effects are defined as any negative experiences that occur to the patients who underwent the cerebellar cTBS or MRI scanning. All adverse effects will be reported by the investigator during the treatment and within 1 week after the end of treatment. Particularly, seizures that are the most severe TMS-related adverse effects with a risk of approximately 0.02%, are only expected to occur during or immediately after cerebellar cTBS. In addition, adverse effects that occur during the MRI scanning will be reported within 24 h. Earplugs will be provided to patients to protect their hearing against noise. Any serious incident will be immediately reported to the Medical Research Ethics Committee of Wuxi Tongren Rehabilitation Hospital.
Discussion
This randomized, sham-controlled clinical trial investigates the neural and behavioral effects of cTBS over the right cerebellum on chronic post-stroke aphasia. We hypothesize that stimulating the right cerebellum with inhibitory cTBS can produce beneficial effects in augmenting SLT for language recovery in post-stroke aphasia by regulating functional connectivity between the right cerebellum and the cerebral cortical regions involved in language processing. These results can provide supportive evidence that the right cerebellum may be a potential optimal stimulation target for the treatment of chronic post-stroke aphasia.
Variability in lesion location and size in brain reorganization for post-stroke aphasia complicate efforts to determine the optimal stimulation strategy at the cortical level (Breining and Sebastian, 2020). Right cerebellar stimulation, in contrast, can potentially serve as a single target site that can be used across patients with post-stroke aphasia with varying site and size of lesion in the left hemisphere (Turkeltaub et al., 2016). The present study proposes a new stimulation protocol for language recovery in chronic post-stroke aphasia by applying inhibitory cTBS over the right cerebellum, since this region has been demonstrated to be essentially involved in a variety of language functions (Gordon, 1996; Desmond and Fiez, 1998; Murdoch, 2010; Stoodley, 2012; Mariën and Borgatti, 2018) and damage to this region leads to impaired language performance (Marien et al., 1996, 2001; Silveri et al., 1998). More importantly, several clinical studies reported improvement in verbal generation or naming functions in the patients with chronic post-stroke aphasia following anodal or cathodal tDCS over the right cerebellum (Sebastian et al., 2016, 2020; Marangolo et al., 2018), providing further evidence in support of the right cerebellum as an optimal stimulation site for neuromodulation in aphasia. On the other hand, Sebastian et al. (2020) found greater beneficial effects on naming functions (relative to sham) when chronic post-stroke patients received cathodal tDCS over the right cerebellum than when they received anodal cerebellar tDCS. And applying inhibitory cTBS over the right cerebellum led to facilitatory effects on impaired vocal motor control in patients with SCA (Lin et al., 2022). As compared to rTMS, cTBS induces robust, long-lasting changes in activation in much shorter periods. Therefore, cTBS over the right cerebellum proposed in the present study protocol may be a promising technique to augment SLT for language recovery in chronic post-stroke aphasia.
The present study protocol also investigates the neural effects of cTBS over the right cerebellum on chronic post-stroke aphasia with RS-fMRI. The majority of previous studies reported behavioral performance assessed by aphasia test batteries following stimulation with rTMS or tDCS (Sebastian et al., 2020), but little is known about the underlying neural mechanisms (Sebastian et al., 2016). In a case report study that combined tDCS and RS-fMRI, Sebastian et al. (2016) found that improvement in spelling induced by anodal tDCS over the right cerebellum was accompanied by increased functional connectivity of the cerebro-cerebellar network. In another study on healthy individuals (Turkeltaub et al., 2016), in addition to improved phonemic fluency, increased resting-state functional connectivity between the cerebellum and speech-motor areas and within the left-lateralized network involved in cognitive aspects of language and motor aspect of speech production were found following tDCS over the right posterolateral cerebellum. Moreover, cerebellar cTBS can modulate activity in the neural pathway that reciprocally links the cerebellum and prefrontal and parietal regions involved in language production (O’Reilly et al., 2010; Stoodley, 2012) by altering short- and long-intracortical inhibition (Koch et al., 2008). Therefore, it is possible that c-TBS over the right cerebellum is effective in an augmenting chronic post-stroke aphasia by altering functional connectivity of the cerebro-cerebellar network.
The present study applies a figure-of-8 coil to the cerebellum. This coil has been shown to be a flat coil model with increased trial tolerances (Hardwick et al., 2014) that can stimulate the superficial layers of the cerebellar cortex (Li et al., 2019). The reported average depth of the lateral cerebellar gray matter is approximately 14.6–14.7 mm from the scalp surface, which is within a range of ∼30 mm at 100% peak output of the figure-of-8 coil (Hardwick et al., 2014). Several studies have successfully applied rTMS or TBS over the cerebellum with a figure-of-8 coil to change motor or speech performance (Theoret et al., 2001; Koch et al., 2008; Popa et al., 2010; Demirtas-Tatlidede et al., 2011; Lin et al., 2022). On the other hand, the present study protocol performs acoustic signal analysis to extract speech parameters for the evaluation of language function with the WAB, BDAE, and BNT scores. The previous research has shown impaired abilities of speech production and motor control in patients with non-fluent aphasia (e.g., Broca’s aphasia) (Hillis, 2007; Behroozmand et al., 2018). Therefore, performing speech acoustic analysis has the potential to comprehensively elucidate the mechanisms underlying the treatment of post-stroke aphasia with cTBS over the right cerebellum coupled with SLT.
Conclusion
In conclusion, the present study protocol proposes a randomized, sham-controlled clinical trial to investigate the efficacy of cTBS over the right cerebellum in augmenting language recovery in chronic post-stroke aphasia and the neural mechanisms underlying the treatment outcome. If this intervention study produces a significant positive effect as expected, the findings will provide valuable evidence for establishing a novel and feasible stimulation protocol to promote language recovery from chronic post-stroke aphasia.
Ethics Statement
The studies involving human participants were reviewed and approved by the Medical Research Ethics Committee of Wuxi Mental Health Center (Wuxi Tongren Rehabilitation Hospital). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CR and PL designed the study. CR, MC, YS, PL, and KZ drafted the protocol. MC coordinated the trial. FG, HF, YJ, and DS performed data acquisition and clinical evaluation. GH and BS conducted the interventions. CR, YS, and MC revised the manuscript. All authors read and approved the final manuscript.
Funding
This work was supported by the National Natural Science Foundation of China (No. 81772439), Natural Science Foundation of Jiangsu Province (No. BK20201138), Wuxi Taihu Talent Project (No. WXTTP2020008), and Top Talent Support Program for Young and Middle-Aged People of Wuxi Health Committee and General Project from Wuxi Health Commission (No. MS201911).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnagi.2022.909733/full#supplementary-material
References
Anglade, C., Thiel, A., and Ansaldo, A. I. (2014). The complementary role of the cerebral hemispheres in recovery from aphasia after stroke: a critical review of literature. Brain Inj. 28, 138–145. doi: 10.3109/02699052.2013.859734
Arasanz, C. P., Staines, W. R., and Schweizer, T. A. (2012). Isolating a cerebellar contribution to rapid visual attention using transcranial magnetic stimulation. Front. Behav. Neurosci. 6:55. doi: 10.3389/fnbeh.2012.00055
Behroozmand, R., Phillip, L., Johari, K., Bonilha, L., Rorden, C., Hickok, G., et al. (2018). Sensorimotor impairment of speech auditory feedback processing in aphasia. Neuroimage 165, 102–111. doi: 10.1016/j.neuroimage.2017.10.014
Benussi, A., Pascual-Leone, A., and Borroni, B. (2020). Non-invasive cerebellar stimulation in neurodegenerative ataxia: a literature review. Int. J. Mol. Sci. 21:1948. doi: 10.3390/ijms21061948
Berthier, M. L. (2005). Poststroke aphasia : epidemiology, pathophysiology and treatment. Drugs Aging 22, 163–182. doi: 10.2165/00002512-200522020-00006
Brady, M. C., Kelly, H., Godwin, J., and Enderby, P. (2012). Speech and language therapy for aphasia following stroke. Cochrane Database Syst. Rev. 2016:Cd000425.
Breining, B. L., and Sebastian, R. (2020). Neuromodulation in post-stroke aphasia treatment. Curr. Phys. Med. Rehabil. Rep. 8, 44–56. doi: 10.1007/s40141-020-00257-5
Chen, R., and Seitz, R. J. (2001). Changing cortical excitability with low-frequency magnetic stimulation. Neurology 57, 379–380.
Cruice, M., Worrall, L., and Hickson, L. (2011). Reporting on psychological well-being of older adults with chronic aphasia in the context of unaffected peers. Disabil. Rehabil. 33, 219–228. doi: 10.3109/09638288.2010.503835
Demirtas-Tatlidede, A., Freitas, C., Pascual-Leone, A., and Schmahmann, J. D. (2011). Modulatory effects of theta burst stimulation on cerebellar nonsomatic functions. Cerebellum 10, 495–503. doi: 10.1007/s12311-010-0230-5
Desmond, J. E., and Fiez, J. A. (1998). Neuroimaging studies of the cerebellum: language, learning and memory. Trends Cogn. Sci. 2, 355–362. doi: 10.1016/s1364-6613(98)01211-x
D’Mello, A. M., Turkeltaub, P. E., and Stoodley, C. J. (2017). Cerebellar tDCS modulates neural circuits during semantic prediction: a combined tDCS-fMRI study. J. Neurosci. 37, 1604–1613. doi: 10.1523/JNEUROSCI.2818-16.2017
Ellis, C., Simpson, A. N., Bonilha, H., Mauldin, P. D., and Simpson, K. N. (2012). The one-year attributable cost of poststroke aphasia. Stroke 43, 1429–1431. doi: 10.1161/STROKEAHA.111.647339
Engelter, S. T., Gostynski, M., Papa, S., Frei, M., Born, C., Ajdacic-Gross, V., et al. (2006). Epidemiology of aphasia attributable to first ischemic stroke: incidence, severity, fluency, etiology, and thrombolysis. Stroke 37, 1379–1384.
Fisicaro, F., Lanza, G., Grasso, A. A., Pennisi, G., and Pennisi, M. (2019). Repetitive transcranial magnetic stimulation in stroke rehabilitation: review of the current evidence and pitfalls. Ther. Adv. Neurol. Disord. 12:175628641987831. doi: 10.1177/1756286419878317
Hara, T., and Abo, M. (2021). New treatment strategy using repetitive transcranial magnetic stimulation for post-stroke aphasia. Diagnostics 11:1853. doi: 10.3390/diagnostics11101853
Hara, T., Abo, M., Kakita, K., Mori, Y., Yoshida, M., and Sasaki, N. (2017). The effect of selective transcranial magnetic stimulation with functional near-infrared spectroscopy and intensive speech therapy on individuals with post-stroke aphasia. Eur. Neurol. 77, 186–194. doi: 10.1159/000457901
Hara, T., Abo, M., Kobayashi, K., Watanabe, M., Kakuda, W., and Senoo, A. (2015). Effects of low-frequency repetitive transcranial magnetic stimulation combined with intensive speech therapy on cerebral blood flow in post-stroke aphasia. Transl. Stroke Res. 6, 365–374. doi: 10.1007/s12975-015-0417-7
Hardwick, R. M., Lesage, E., and Miall, R. C. (2014). Cerebellar transcranial magnetic stimulation: the role of coil geometry and tissue depth. Brain Stimul. 7, 643–649. doi: 10.1016/j.brs.2014.04.009
Hartwigsen, G., and Saur, D. (2017). Neuroimaging of stroke recovery from aphasia – Insights into plasticity of the human language network. Neuroimage 190, 14–31. doi: 10.1016/j.neuroimage.2017.11.056
Harvey, D. Y., Podell, J., Turkeltaub, P. E., Faseyitan, O., Coslett, H. B., and Hamilton, R. H. (2017). Functional reorganization of right prefrontal cortex underlies sustained naming improvements in chronic aphasia via repetitive transcranial magnetic stimulation. Cogn. Behav. Neurol. 30, 133–144. doi: 10.1097/WNN.0000000000000141
Heikkinen, P. H., Pulvermuller, F., Makela, J. P., Ilmoniemi, R. J., Lioumis, P., Kujala, T., et al. (2018). Combining rTMS with intensive language-action therapy in chronic aphasia: a randomized controlled trial. Front. Neurosci. 12:1036. doi: 10.3389/fnins.2018.01036
Hillis, A. E. (2007). Aphasia: progress in the last quarter of a century. Neurology 69, 200–213. doi: 10.1212/01.wnl.0000265600.69385.6f
Hu, X. Y., Zhang, T., Rajah, G. B., Stone, C., Liu, L. X., He, J. J., et al. (2018). Effects of different frequencies of repetitive transcranial magnetic stimulation in stroke patients with non-fluent aphasia: a randomized, sham-controlled study. Neurol. Res. 40, 459–465. doi: 10.1080/01616412.2018.1453980
Huang, Y. Z., Edwards, M. J., Rounis, E., Bhatia, K. P., and Rothwell, J. C. (2005). Theta burst stimulation of the human motor cortex. Neuron 45, 201–206.
Hurtado-Puerto, A. M., Nestor, K., Eldaief, M., and Camprodon, J. A. (2020). Safety considerations for cerebellar theta burst stimulation. Clin. Ther. 42, 1169–1190.e1. doi: 10.1016/j.clinthera.2020.06.001
Kawamura, M., Takahashi, N., and Kobayashi, Y. (2019). Effect of repetitive transcranial magnetic stimulation on the right superior temporal gyrus for severe aphasia caused by damage to the left inferior frontal gyrus. Case Rep. Neurol. 11, 189–198. doi: 10.1159/000500669
Kim, W. J., Rosselin, C., Amatya, B., Hafezi, P., and Khan, F. (2020). Repetitive transcranial magnetic stimulation for management of post-stroke impairments: an overview of systematic reviews. J. Rehabil. Med. 52:jrm00015. doi: 10.2340/16501977-2637
Koch, G. (2010). Repetitive transcranial magnetic stimulation: a tool for human cerebellar plasticity. Funct. Neurol. 25, 159–163.
Koch, G., Brusa, L., Carrillo, F., Lo Gerfo, E., Torriero, S., Oliveri, M., et al. (2009). Cerebellar magnetic stimulation decreases levodopa-induced dyskinesias in Parkinson disease. Neurology 73, 113–119. doi: 10.1212/WNL.0b013e3181ad5387
Koch, G., Esposito, R., Motta, C., Casula, E. P., Di Lorenzo, F., Bonni, S., et al. (2020). Improving visuo-motor learning with cerebellar theta burst stimulation: behavioral and neurophysiological evidence. Neuroimage 208:116424. doi: 10.1016/j.neuroimage.2019.116424
Koch, G., Mori, F., Marconi, B., Codeca, C., Pecchioli, C., Salerno, S., et al. (2008). Changes in intracortical circuits of the human motor cortex following theta burst stimulation of the lateral cerebellum. Clin. Neurophysiol. 119, 2559–2569. doi: 10.1016/j.clinph.2008.08.008
Koch, G., Porcacchia, P., Ponzo, V., Carrillo, F., Cáceres-Redondo, M. T., Brusa, L., et al. (2014). Effects of two weeks of cerebellar theta burst stimulation in cervical dystonia patients. Brain Stimul. 7, 564–572. doi: 10.1016/j.brs.2014.05.002
Lametti, D. R., Smith, H. J., Freidin, P. F., and Watkins, K. E. (2018). Cortico-cerebellar networks drive sensorimotor learning in speech. J. Cogn. Neurosci. 30, 540–551. doi: 10.1162/jocn_a_01216
Li, W., Zhuang, J., Guo, Z., Jones, J. A., Xu, Z., and Liu, H. (2019). Cerebellar contribution to auditory feedback control of speech production: evidence from patients with spinocerebellar ataxia. Hum. Brain Mapp. 40, 4748–4758. doi: 10.1002/hbm.24734
Lin, Q., Chang, Y., Liu, P., Jones, J. A., Chen, X., Peng, D., et al. (2022). Cerebellar continuous theta burst stimulation facilitates auditory-vocal integration in spinocerebellar ataxia. Cereb. Cortex 32, 455–466. doi: 10.1093/cercor/bhab222
Lv, H., Wang, Z., Tong, E., Williams, L. M., Zaharchuk, G., Zeineh, M., et al. (2018). Resting-state functional MRI: everything that nonexperts have always wanted to know. AJNR Am. J. Neuroradiol. 39, 1390–1399. doi: 10.3174/ajnr.A5527
Maas, R., Helmich, R. C. G., and van de Warrenburg, B. P. C. (2020). The role of the cerebellum in degenerative ataxias and essential tremor: insights from noninvasive modulation of cerebellar activity. Mov. Disord. 35, 215–227. doi: 10.1002/mds.27919
Marangolo, P., Fiori, V., Caltagirone, C., Pisano, F., and Priori, A. (2018). Transcranial cerebellar direct current stimulation enhances verb generation but not verb naming in poststroke aphasia. J. Cogn. Neurosci. 30, 188–199. doi: 10.1162/jocn_a_01201
Mariën, P., and Borgatti, R. (2018). Language and the cerebellum. Handb. Clin. Neurol. 154, 181–202.
Marien, P., Engelborghs, S., Fabbro, F., and De Deyn, P. P. (2001). The lateralized linguistic cerebellum: a review and a new hypothesis. Brain Lang. 79, 580–600. doi: 10.1006/brln.2001.2569
Marien, P., Saerens, J., Nanhoe, R., Moens, E., Nagels, G., Pickut, B. A., et al. (1996). Cerebellar induced aphasia: case report of cerebellar induced prefrontal aphasic language phenomena supported by SPECT findings. J. Neurol. Sci. 144, 34–43. doi: 10.1016/s0022-510x(96)00059-7
Murdoch, B. E. (2010). The cerebellum and language: historical perspective and review. Cortex 46, 858–868. doi: 10.1016/j.cortex.2009.07.018
O’Reilly, J. X., Beckmann, C. F., Tomassini, V., Ramnani, N., and Johansen-Berg, H. (2010). Distinct and overlapping functional zones in the cerebellum defined by resting state functional connectivity. Cereb. Cortex 20, 953–965. doi: 10.1093/cercor/bhp157
Popa, T., Russo, M., and Meunier, S. (2010). Long-lasting inhibition of cerebellar output. Brain Stimul. 3, 161–169. doi: 10.1016/j.brs.2009.10.001
Pope, P. A., and Miall, R. C. (2012). Task-specific facilitation of cognition by cathodal transcranial direct current stimulation of the cerebellum. Brain Stimul. 5, 84–94. doi: 10.1016/j.brs.2012.03.006
Rastogi, A., Cash, R., Dunlop, K., Vesia, M., Kucyi, A., Ghahremani, A., et al. (2017). Modulation of cognitive cerebello-cerebral functional connectivity by lateral cerebellar continuous theta burst stimulation. Neuroimage 158, 48–57. doi: 10.1016/j.neuroimage.2017.06.048
Ren, C., Zhang, G., Xu, X., Hao, J., Fang, H., Chen, P., et al. (2019). The effect of rTMS over the different targets on language recovery in stroke patients with global aphasia: a randomized sham-controlled study. Biomed. Res. Int. 2019:4589056. doi: 10.1155/2019/4589056
Rossi, S., Hallett, M., Rossini, P. M., and Pascual-Leone, A. (2009). Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin. Neurophysiol. 120, 2008–2039.
Rossini, P. M., Burke, D., Chen, R., Cohen, L. G., Daskalakis, Z., Di Iorio, R., et al. (2015). Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin. Neurophysiol. 126, 1071–1107. doi: 10.1016/j.clinph.2015.02.001
Santos, M. D. D., Cavenaghi, V. B., Mac-Kay, A., Serafim, V., Venturi, A., Truong, D. Q., et al. (2017). Non-invasive brain stimulation and computational models in post-stroke aphasic patients: single session of transcranial magnetic stimulation and transcranial direct current stimulation. A randomized clinical trial. Sao Paulo Med. J. 135, 475–480. doi: 10.1590/1516-3180.2016.0194060617
Sebastian, R., Kim, J. H., Brenowitz, R., Tippett, D. C., Desmond, J. E., Celnik, P. A., et al. (2020). Cerebellar neuromodulation improves naming in post-stroke aphasia. Brain Commun. 2:fcaa179. doi: 10.1093/braincomms/fcaa179
Sebastian, R., Saxena, S., Tsapkini, K., Faria, A. V., Long, C., Wright, A., et al. (2016). Cerebellar tDCS: a novel approach to augment language treatment post-stroke. Front. Hum. Neurosci. 10:695. doi: 10.3389/fnhum.2016.00695
Sheu, Y. S., Liang, Y., and Desmond, J. E. (2019). Disruption of cerebellar prediction in verbal working memory. Front. Hum. Neurosci. 13:61. doi: 10.3389/fnhum.2019.00061
Silveri, M. C., Di Betta, A. M., Filippini, V., Leggio, M. G., and Molinari, M. (1998). Verbal short-term store-rehearsal system and the cerebellum. Evidence from a patient with a right cerebellar lesion. Brain 121(Pt 11), 2175–2187. doi: 10.1093/brain/121.11.2175
Stoodley, C. J. (2012). The cerebellum and cognition: evidence from functional imaging studies. Cerebellum 11, 352–365. doi: 10.1007/s12311-011-0260-7
Theoret, H., Haque, J., and Pascual-Leone, A. (2001). Increased variability of paced finger tapping accuracy following repetitive magnetic stimulation of the cerebellum in humans. Neurosci. Lett. 306, 29–32. doi: 10.1016/s0304-3940(01)01860-2
Thiel, A., Hartmann, A., Rubi-Fessen, I., Anglade, C., Kracht, L., Weiduschat, N., et al. (2013). Effects of noninvasive brain stimulation on language networks and recovery in early poststroke aphasia. Stroke 44, 2240–2246. doi: 10.1161/STROKEAHA.111.000574
Turkeltaub, P. E., Swears, M. K., D’Mello, A. M., and Stoodley, C. J. (2016). Cerebellar tDCS as a novel treatment for aphasia? Evidence from behavioral and resting-state functional connectivity data in healthy adults. Restor. Neurol. Neurosci. 34, 491–505. doi: 10.3233/RNN-150633
Tzourio-Mazoyer, N., Landeau, B., Papathanassiou, D., Crivello, F., Etard, O., Delcroix, N., et al. (2002). Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 15, 273–289.
Wang, C. P., Hsieh, C. Y., Tsai, P. Y., Wang, C. T., Lin, F. G., and Chan, R. C. (2014). Efficacy of synchronous verbal training during repetitive transcranial magnetic stimulation in patients with chronic aphasia. Stroke 45, 3656–3662. doi: 10.1161/STROKEAHA.114.007058
Wassermann, E. M. (1998). Risk and safety of repetitive transcranial magnetic stimulation: report and suggested guidelines from the International Workshop on the Safety of Repetitive Transcranial Magnetic Stimulation, June 5-7, 1996. Electroencephalogr. Clin. Neurophysiol. 108, 1–16. doi: 10.1016/s0168-5597(97)00096-8
Yan, C. G., Wang, X. D., Zuo, X. N., and Zang, Y. F. (2016). DPABI: data processing & analysis for (resting-state) brain imaging. Neuroinformatics 14, 339–351.
Keywords: study protocol, aphasia, continuous theta burst stimulation, cerebellum, randomized controlled trial (RCT)
Citation: Zheng K, Chen M, Shen Y, Xu X, Gao F, Huang G, Ji Y, Su B, Song D, Fang H, Liu P and Ren C (2022) Cerebellar Continuous Theta Burst Stimulation for Aphasia Rehabilitation: Study Protocol for a Randomized Controlled Trial. Front. Aging Neurosci. 14:909733. doi: 10.3389/fnagi.2022.909733
Received: 31 March 2022; Accepted: 03 May 2022;
Published: 02 June 2022.
Edited by:
Wenxin Niu, Tongji University, ChinaReviewed by:
Jack Jiaqi Zhang, The Hong Kong Polytechnic University, Hong Kong SAR, ChinaIsabel Catarina Duarte, Coimbra Institute for Biomedical Imaging and Translational Research (CIBIT), Portugal
Copyright © 2022 Zheng, Chen, Shen, Xu, Gao, Huang, Ji, Su, Song, Fang, Liu and Ren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Caili Ren, rencaili@njmu.edu.cn; Peng Liu, liupeng2@mail.sysu.edu.cn
†These authors have contributed equally to this work