 Hui Lu
Hui Lu Peng-Fei Wu2,3†
Peng-Fei Wu2,3† Wan Zhang
Wan Zhang- 1Department of Neurology, Xuanwu Hospital, Capital Medical University, Beijing, China
- 2Center for Medical Genetics & Hunan Provincial Key Laboratory for Medical Genetics, School of Life Sciences, Central South University, Changsha, China
- 3Department of Neurology, Beth Israel Deaconess Medical Center & Harvard Medical School, Boston, MA, United States
- 4School of Medicine, South China University of Technology, Guangzhou, China
- 5Biology Department, College of Arts & Sciences, Boston University, Boston, MA, United States
- 6Department of Neurology, Affiliated Hospital of Nantong University, Nantong, China
Study Objectives: To clarify the effects of sleep duration on stroke and stroke subtypes, we adopted a Mendelian randomization (MR) approach to evaluate their causal relationship.
Methods: A genome-wide association study including 446,118 participants from UK biobank was used to identify instruments for short sleep, long sleep and sleep duration. Summary-level data for all stroke, ischemic stroke, intracerebral hemorrhage, and their subtypes were obtained from meta-analyses conducted by the MEGASTROKE consortium. MR analyses were performed using the inverse-variance-weighted method, weighted median estimator, MR pleiotropy residual sum and outlier (MR-PRESSO) test, and MR-Egger regression. Sensitivity analyses were further performed using leave-one-out analysis, MR-PRESSO global test and Cochran's Q test to verify the robustness of our findings.
Results: By two-sample MR, we didn't find causal associations between sleep duration and risk of stroke. However, in the subgroup analysis, we found weak evidence for short sleep in increasing risk of cardio-embolic stroke (odds ratio [OR], 1.33; 95% confidence interval [CI], 1.11–1.60; P = 0.02) and long sleep in increasing risk of large artery stroke [OR, 1.41; 95% CI, 1.02–1.95; P = 0.04]. But the associations were not significant after Bonferroni correction for multiple comparisons.
Conclusions: Our study suggests that sleep duration is not causally associated with risk of stroke and its subtypes.
Introduction
Stroke is the second leading cause of death worldwide, with an age-standardized mortality rate of 86.5 per 100,000 population per year (1). Although stroke incidence, prevalence, mortality and disability-adjusted life-years rates have declined from 1990 to 2017, the absolute number of people who developed new stroke, died, survived or remained disabled from stroke has almost doubled (2). Globally in 2017, ischemic stroke constituted 65%, primary intracranial hemorrhage (ICH)-26% and subarachnoid hemorrhage-9% of all incidents of stroke (2). Given the global burden of stroke, it is imperative to identify other modifiable lifestyle factors to prevent stroke.
Sleep is gaining recognition as an important lifestyle factor relevant to the prevention of stroke. A large proportion of people sleep less or more than the recommended 7–8 h of sleep (3). Recent reports have suggested an association between both short (<6 h) and long (>9 h) sleep duration and risk of stroke (4, 5). However, the evidence supporting this association is not consistent. Some studies have found a link between long or short sleep duration and an increased risk of stroke (6–9), whereas other studies have claimed no significant association (10, 11). These conflicting findings from observational epidemiological studies may be due to differences in the study population, sample size, sleep duration assessment methods, or covariates adjusted in the statistical models. Also, observational studies are prone to biases, particularly from confounders such as disturbed sleep conditions and poor health. It is also difficult to distinguish if abnormal sleep duration causes stroke, or risk factors like poor health result in both abnormal sleep duration and stroke. In addition, whether sleep duration has different influences on different stroke subtypes is unknown.
These limitations may be overcome by use of genetic proxies of lifetime exposure in Mendelian randomization (MR) (12). While observational studies investigate the association between an exposure and outcome, MR investigates the link between genetic variants relating to the exposure and outcome (13). By studying the genetic variants rather than the exposure directly, MR overcomes the potential impact of confounding factors on the exposure (13). Therefore, MR has advantages in its ability to draw conclusions about the causal relationship between exposure and outcome.
Sleep duration is a heritable trait. Twin- and family- based studies have suggested that 9 ~ 45% of variability in self-reported sleep duration is influenced by genetic factors (14, 15). Recent genome-wide association studies (GWAS) in up to 446,118 participants from the UK Biobank identified 78 single nucleotide polymorphism (SNP) for habitual self-reported sleep duration (15). In this study, we utilized a two-sample MR approach to investigate whether there existed causal effects of lifetime sleep duration on stroke or stroke subtypes.
Methods
This study was based on MR design, which utilized publicly shared databases; no additional participant consent is required.
GWAS Data Sources
Summary statistics for sleep traits were obtained from the Sleep Disorder Knowledge Portal (http://sleepdisordergenetics.org/). Dashti et al. has performed the most up-to-data GWAS meta-analysis of self-reported habitual short sleep (<7 h/days; 106,192 individuals), long sleep (≥9 h/day; 34,184 individuals), and sleep duration in 446,118 European-ancestry adults from the UK Biobank (15). Seventy-eight loci genome-wide significantly associated with sleep duration (P < 5 × 10−8), 27 and eight loci for short and long sleep in terms of 7–8 h sleep duration (305,742 controls), respectively, were identified.
Stroke datasets were released by the MEGASTROKE consortium (http://www.megastroke.org/). The results for GWAS meta-analysis restricted to European participants (40,585 cases and 406,111 controls) were available. Stroke were categorized into any ischemic stroke (AIS; 34,217 cases), large artery stroke (LAS; 4,373 cases), cardioembolic stroke (CES; 7,193 cases), and small vessel stroke (SVS; 5,386 cases) (16). Summary statistics for ICH were obtained from another meta-analysis by the International Stroke Genetics Consortium. 1,545 cases defined by neurological deficits with compatible brain imaging and 1,481 controls of European ancestry were incorporated (17). ICH was subtyped into lobar (the lesion originating at the cerebral cortex or cortical-subcortical junction; 686 cases), and non-lobar (thalamus, internal capsule, basal ganglia, deep periventricular white matter, cerebellum, or brain stem; 909 cases). All ethical approval had been obtained in these original researches.
Selection of Instrumental SNPs
MR analyses were based on genetic instrumental variables, a set of independent SNPs (r2 < 0.1 in European populations, 1000 Genomes Project Phase 3) significantly associated with the exposure, for which either their own or their proxy SNPs (r2 > 0.8) outcome association statistics should be available concurrently. For sleep-stroke MR analyses, among SNPs associated with short sleep, long sleep and sleep duration, rs142180737, rs549961083, and rs2139261, respectively, was removed owing to no available proxies. For sleep-ICH analyses, 18 short sleep-related SNPs were retained, among which 3 proxies (rs12705966, rs7549825, rs11955683; r2 ≥ 0.86, D′ ≥ 0.97) were adopted; 5 long sleep-related SNPs were retained, and rs17688916 was proxied by rs113871181 (r2 = 0.90, D′ = 0.99); 61 sleep duration-related SNPs were retained, among which 8 proxies (rs4470910, rs62535668, rs1517564, rs77493530, rs7549825, rs3786694, rs67008484, rs180767; r2 ≥ 0.82, D′ ≥ 0.96) were utilized.
Mendelian Randomization Analysis
We performed a two-sample MR using R (version 3.5.3) and TwoSampleMR and MR-PRESSO packages (18, 19). Firstly, an MR estimate for each instrumental SNP was generated using the Wald method (20, 21). To compute the overall estimate, the inverse-variance weighted (IVW) model was used for the primary MR analysis. Three additional methods, the MR pleiotropy residual sum and outlier (MR-PRESSO), weighted median estimator (WM) and MR-Egger regression, based on different MR assumptions were conducted. IVW generally gave a consistent estimate of the causality, which was based on a fixed-effect meta-analysis. The inverse-variance weighted estimate may be biased, however, in the presence of invalid instrumental variables with horizontal pleiotropy (20). MR-PRESSO has the advantage of detecting horizontal pleiotropy and yielding a corrected estimate via outlier removal if necessary (18). WM and MR-Egger were less statistically well-powered, yet more robust to horizontal pleiotropy. The weighted median estimator pooled effects of individual variants efficiently under the prerequisite that more than 50% of the weight came from valid instrumental variables (22). MR-Egger regression assumed that the pleiotropic associations are independent and conducted a weighted linear regression of the outcome coefficient on the exposure coefficient. The intercept and slope of MR-Egger regression provided an exploration of pleiotropy and the causality estimate adjusted for pleiotropy (18). Accordingly, the comprehensive evaluation of MR results was rendered possible through 4 MR approaches based on different assumptions.
Furthermore, 3 sensitivity analyses were implemented. To explore whether the MR estimates were disproportionately influenced by certain SNP alone, we performed a leave-one-out analysis by omitting instrumental SNPs one by one (23). MR-PRESSO global and distortion test was conducted likewise, detecting the significant distortion in the causal estimates before and after outlier removal. We also examined the heterogeneity across all instrumental SNPs quantified by Cochran's Q statistics.
Results
Table 1 summarized the main results of the MR analyses exploring the causality between 3 self-reported sleep traits and stroke, ICH and their subtypes. Overall, genetically determined short sleep was not causally associated with stroke (odds ratio [OR], 0.91; 95% confidence interval [CI], 0.78–1.07) and ICH (OR, 0.55; 95% CI, 0.23–1.29). In subtype analyses, there was weak evidence showing that per unit increment in log-odds for short sleep would increase risk for CES by 33% (OR, 1.33; 95% CI, 1.11–1.60; P = 0.02).
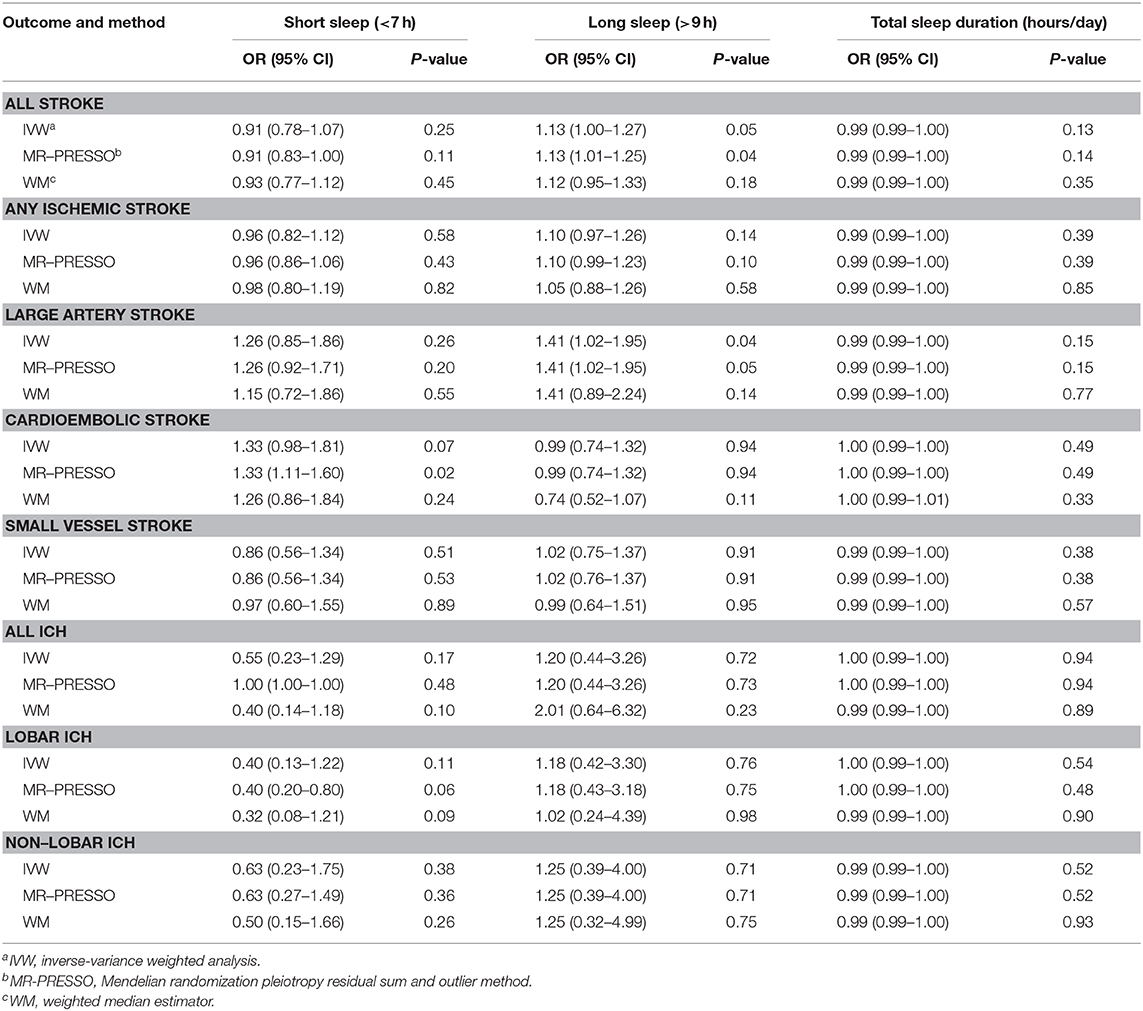
Table 1. Mendelian randomization estimates for causal effect of sleep on ischemic stroke.
MR results did not support the causal association between long sleep and stroke (OR, 1.13; 95% CI, 1.00–1.27) or ICH (OR, 1.20; 95% CI, 0.44–3.26), either. But there was suggestive evidence supporting long sleep as a possible risk factor for LAS. The OR of LAS per unit increase in log-odds for long sleep was 1.41 (95% CI, 1.02–1.95; P = 0.04). The causality between short or long sleep and the other subtypes of stroke was not statistically significant. Besides, no causal effects of sleep duration on stroke, ICH, or their subtypes were identified.
The MR-Egger regression and MR-PRESSO global tests demonstrated no presence of horizontal pleiotropy among all instrumental SNPs (Supplementary Tables 1–3). The leave-one-out analyses and Cochran's Q tests indicated no heterogeneity (Supplementary Figures 1–3). Notably, the results from different MR methods were consistent on the whole, yet we had inadequate power to detect weak associations, that is, an estimated statistical power below 80% to detect the true effect size between 0.8 and 1.2 (Supplementary Table 4).
Discussion
In this study, we have not found any evidence that sleep traits (short sleep, long sleep, or total sleep duration) were causally associated with the risk of stroke or stroke subtypes (AIS, SVS, or ICH). However, we found weak evidence that short sleep can increase the risk of CES and long sleep can increase the risk of LAS, albeit the associations did not reach statistical significance after correction for multiple comparisons. To our knowledge, no previous MR study had assessed the causal association of sleep duration and risk of stroke subtypes (24).
Lots of population-based cohort studies have been performed examining the association of sleep duration and stroke. However, results of meta-analyses based on these cohort studies are conflicting. One meta-analysis including 19 studies (31 cohorts) with a total of 816,995 individuals shows both short (risk ratio [RR], 1.32; 95% CI, 1.18–1.47) and long (RR, 1.48; 95% CI, 1.31–1.68) sleep can increase the risk of stroke (9). However, another meta-analysis including 153 studies with 5,172,710 participants found no sufficient evidence on the association between short sleep and risk of stroke (RR, 1.08; 95% CI, 0.98–1.19) (11). To clarify their relationship, we leveraged pre-existing databases from the UKB and MEGASTROKE projects in this study and concluded no significant association between sleep duration and stroke.
Different subtypes of stroke have different pathological processes, so we went further to investigate the effects of sleep duration upon subtypes of stroke. In the subgroup analysis of our MR study, we found weak evidence for long sleep in increasing risk of LAS. This result seemed consistent with earlier MR study on myocardial infarction (25). A potential explanation is that long sleep might be associated with an increased risk of atherosclerosis (26). Spending excessive time in bed can elicit daytime lethargy and exacerbate sleep fragmentation (27), which was considered to be associated with more severe arteriolosclerosis and subcortical macroscopic infarcts (4). In addition, long sleep duration may be linked to low levels of physical activity, type 2 diabetes, poor sleep quality, poor physical/mental health, low socioeconomic status, and vary by ethnicity (28–32). All of these factors might increase the risk of LAS. We also found weak evidence for short sleep in increasing risk of CES. The possible hypothesis is that short sleep duration is independently associated with prevalent and incident atrial fibrillation (AF) (33). Each 1-h reduction in sleep duration was associated with 17% greater risk of prevalent AF and 9% greater risk of incident AF (33). Sleep deprivation increases atrial electromechanical delay, increases sympathetic nervous system activity and activates pro-inflammatory systems, which are pathways predisposing to AF (34–36). AF has been well-acknowledged as the leading cause for CES, which may explain the weak association of short sleep with increased risk of CES in our study. Lastly, sleep duration is merely one of the commonly reported sleep traits. We did not investigate the causal effect of other sleep characteristics on risk of stroke, such as sleep apnea and REM percentage. Long sleep duration is reported to be associated with an increased risk of stroke in obstructive sleep apnea patients with existing cardiovascular disease (37). Meanwhile, a recent study has showed that less REM sleep was associated with greater risk of cardiovascular mortality in middle-aged and older adults (38). Future MR studies are warranted to explore the role of more detailed sleep characteristics.
There were several limitations for our study. Firstly, we could not detect a non-linear relationship between sleep duration and stroke using these MR methods and summary-level statistics. Secondly, intrinsic pleiotropy of instrumental SNPs could hinder the reliability of MR results (39); nevertheless, we failed to detect any horizontal pleiotropy when employing several efficient tools to scrutinize it in this study. Thirdly, SNPs identified by GWAS are acknowledged to explain a small proportion of variance, including the sleep traits-associated SNPs; hence, this study had restricted power to detect a weak effect, especially the association of sleep traits with ICH, considering the much smaller sample size as opposed to other subtypes of stroke. Fourthly, data on sleep duration are self-reported by the participants which might be less accurate than objective methods, such as polysomnography. Concerns about self-reported sleep duration were raised, and acceptable correlations between self-reported sleep duration and that measured by actigraphy have been reported (40). More detailed characteristics for sleep duration were not collected, such as chronotype, napping, dozing and snoring, which may undermine this study's clinical implications. Fifthly, our database originated from European-ancestry studies, whereas it is well-known that stroke burden varies among ethnicities worldwide, such as in the Chinese Han population, in which stroke seems more prevalent than in Europeans (41); therefore, we should be cautious when generalizing the conclusion to other ethnicities worldwide.
In summary, our study found little evidence on causal relationship between genetically predicted sleep duration with risk of stroke and its subtypes.
Data Availability Statement
All datasets generated for this study are included in the article/Supplementary Material.
Author Contributions
HL: conceptualization, methodology, writing-original draft preparation, writing-reviewing and editing, and supervision. P-FW: conceptualization, data curation, software, formal analysis, writing-original draft preparation, and data visualization. R-ZL: data curation, software, and formal analysis. WZ: writing-reviewing and editing, data visualization, and validation. GH: validation, resources, writing-reviewing, editing, and supervision. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We extend sincere thanks to Dr. Dashti, Dr. Malik, Dr. Woo, et al., ISGEC, MEGASTROKE, International Stroke Genetics Consortium and all concerned investigators and consortia for sharing GWAS summary statistics on sleep and stroke. We thank all individuals for participating in the original GWAS studies. P-FW has received a visiting PhD stipend from the China Scholarship Council.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2020.00976/full#supplementary-material
References
1. GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet. (2017) 390:1151–210. doi: 10.1016/S0140-6736(17)32152-9
2. Krishnamurthi RV, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the global burden of disease study 2017. Neuroepidemiology. (2020) 54:171–9. doi: 10.1159/000506396
3. Liu Y, Wheaton AG, Chapman DP, Cunningham TJ, Lu H, Croft JB. Prevalence of healthy sleep duration among adults–United States, 2014. Morb Mortal Wkly Rep. (2016) 65:137–41. doi: 10.15585/mmwr.mm6506a1
4. Yin J, Jin X, Shan Z, Li S, Huang H, Li P, et al. Relationship of sleep duration with all-cause mortality and cardiovascular events: a systematic review and dose-response meta-analysis of prospective cohort studies. J Am Heart Assoc. (2017) 6:e005947. doi: 10.1161/JAHA.117.005947
5. Akinseye OA, Ojike NI, Akinseye LI, Dhandapany PS, Pandi-Perumal SR. Association of sleep duration with stroke in diabetic patients: analysis of the national health interview survey. J Stroke Cerebrovasc Dis. (2016) 25:650–5. doi: 10.1016/j.jstrokecerebrovasdis.2015.11.023
6. Leng Y, Cappuccio FP, Wainwright NW, Surtees PG, Luben R, Brayne C, et al. Sleep duration and risk of fatal and nonfatal stroke: a prospective study and meta-analysis. Neurology. (2015) 84:1072–9. doi: 10.1212/WNL.0000000000001371
7. Jike M, Itani O, Watanabe N, Buysse DJ, Kaneita Y. Long sleep duration and health outcomes: a systematic review, meta-analysis and meta-regression. Sleep Med Rev. (2018) 39:25–36. doi: 10.1016/j.smrv.2017.06.011
8. Kawachi T, Wada K, Nakamura K, Tsuji M, Tamura T, Konishi K, et al. Sleep duration and the risk of mortality from stroke in japan: the takayama cohort study. J Epidemiol. (2016) 26:123–30. doi: 10.2188/jea.JE20140272
9. Krittanawong C, Tunhasiriwet A, Wang Z, Zhang H, Farrell AM, Chirapongsathorn S, et al. Association between short and long sleep durations and cardiovascular outcomes: a systematic review and meta-analysis. Eur Heart J Acute Cardiovasc Care. (2019) 8:762–70. doi: 10.1177/2048872617741733
10. Ford ES. Habitual sleep duration and predicted 10-year cardiovascular risk using the pooled cohort risk equations among US adults. J Am Heart Assoc. (2014) 3:e001454. doi: 10.1161/JAHA.114.001454
11. Itani O, Jike M, Watanabe N, Kaneita Y. Short sleep duration and health outcomes: a systematic review, meta-analysis, and meta-regression. Sleep Med. (2017) 32:246–56. doi: 10.1016/j.sleep.2016.08.006
12. Gage SH, Jones HJ, Taylor AE, Burgess S, Zammit S, Munafò MR. Investigating causality in associations between smoking initiation and schizophrenia using mendelian randomization. Sci Rep. (2017) 7:40653. doi: 10.1038/srep40653
13. Davey SG, Ebrahim S. What can mendelian randomisation tell us about modifiable behavioural and environmental exposures. BMJ. (2005) 330:1076–9. doi: 10.1136/bmj.330.7499.1076
14. de Castro JM. The influence of heredity on self-reported sleep patterns in free-living humans. Physiol Behav. (2002) 76:479–86. doi: 10.1016/S0031-9384(02)00699-6
15. Dashti HS, Jones SE, Wood AR, Lane JM, van Hees VT, Wang H, et al. Genome-wide association study identifies genetic loci for self-reported habitual sleep duration supported by accelerometer-derived estimates. Nat Commun. (2019) 10:1100. doi: 10.1038/s41467-019-08917-4
16. Malik R, Chauhan G, Traylor M, Sargurupremraj M, Okada Y, Mishra A, et al. Multiancestry genome-wide association study of 520,000 subjects identifies 32 loci associated with stroke and stroke subtypes. Nat Genet. (2018) 50:524–37. doi: 10.1038/s41588-018-0058-3
17. Woo D, Falcone GJ, Devan WJ, Brown WM, Biffi A, Howard TD, et al. Meta-analysis of genome-wide association studies identifies 1q22 as a susceptibility locus for intracerebral hemorrhage. Am J Hum Genet. (2014) 94:511–21. doi: 10.1016/j.ajhg.2014.02.012
18. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from mendelian randomization between complex traits and diseases. Nat Genet. (2018) 50:693–8. doi: 10.1038/s41588-018-0099-7
19. Hemani G, Zheng J, Elsworth B, Wade KH, Haberland V, Baird D, et al. The MR-Base platform supports systematic causal inference across the human phenome. Elife. (2018) 7:e34408. doi: 10.7554/eLife.34408
20. Baiocchi M, Cheng J, Small DS. Instrumental variable methods for causal inference. Stat Med. (2014) 33:2297–340. doi: 10.1002/sim.6128
21. Meng XH, Tan LJ, Xiao HM, Tang BS, Deng HW. Examining the causal role of leptin in bone mineral density: a mendelian randomization study. Bone. (2019) 125:25–9. doi: 10.1016/j.bone.2019.05.006
22. Bowden J, Davey SG, Haycock PC, Burgess S. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. (2016) 40:304–14. doi: 10.1002/gepi.21965
23. Hemani G, Bowden J, Davey SG. Evaluating the potential role of pleiotropy in mendelian randomization studies. Hum Mol Genet. (2018) 27:R195–208. doi: 10.1093/hmg/ddy163
24. Dashti HS, Redline S, Saxena R. Polygenic risk score identifies associations between sleep duration and diseases determined from an electronic medical record biobank. Sleep. (2019) 42:zsy247. doi: 10.1093/sleep/zsy247
25. Daghlas I, Dashti HS, Lane J, Aragam KG, Rutter MK, Saxena R, et al. Sleep duration and myocardial infarction. J Am Coll Cardiol. (2019) 74:1304–14. doi: 10.1016/j.jacc.2019.07.022
26. Blasco-Colmenares E, Moreno-Franco B, Latre ML, Mur-Vispe E, Pocovi M, Jarauta E, et al. Sleep duration and subclinical atherosclerosis: the aragon workers' health study. Atherosclerosis. (2018) 274:35–40. doi: 10.1016/j.atherosclerosis.2018.05.003
27. Youngstedt SD, Kripke DF. Long sleep and mortality: rationale for sleep restriction. Sleep Med Rev. (2004) 8:159–74. doi: 10.1016/j.smrv.2003.10.002
28. Amagai Y, Ishikawa S, Gotoh T, Kayaba K, Nakamura Y, Kajii E. Sleep duration and incidence of cardiovascular events in a japanese population: the jichi medical school cohort study. J Epidemiol. (2010) 20:106–10. doi: 10.2188/jea.JE20090053
29. Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, Verschuren WM. Sufficient sleep duration contributes to lower cardiovascular disease risk in addition to four traditional lifestyle factors: the MORGEN study. Eur J Prev Cardiol. (2014) 21:1367–75. doi: 10.1177/2047487313493057
30. Suzuki E, Yorifuji T, Ueshima K, Takao S, Sugiyama M, Ohta T, et al. Sleep duration, sleep quality and cardiovascular disease mortality among the elderly: a population-based cohort study. Prev Med. (2009) 49:135–41. doi: 10.1016/j.ypmed.2009.06.016
31. Whinnery J, Jackson N, Rattanaumpawan P, Grandner MA. Short and long sleep duration associated with race/ethnicity, sociodemographics, and socioeconomic position. Sleep. (2014) 37:601–11. doi: 10.5665/sleep.3508
32. Smagula SF, Koh WP, Wang R, Yuan JM. Chronic disease and lifestyle factors associated with change in sleep duration among older adults in the Singapore Chinese health study. J Sleep Res. (2016) 25:57–61. doi: 10.1111/jsr.12342
33. Genuardi MV, Ogilvie RP, Saand AR, DeSensi RS, Saul MI, Magnani JW, et al. Association of short sleep duration and atrial fibrillation. Chest. (2019) 156:544–52. doi: 10.1016/j.chest.2019.01.033
34. Esen Ö, Akçakoyun M, Açar G, Bulut M, Alizade E, Kargin R, et al. Acute sleep deprivation is associated with increased atrial electromechanical delay in healthy young adults. Pacing Clin Electrophysiol. (2011) 34:1645–51. doi: 10.1111/j.1540-8159.2011.03186.x
35. Castro-Diehl C, Diez RAV, Redline S, Seeman T, McKinley P, Sloan R, et al. Sleep duration and quality in relation to autonomic nervous system measures: the multi-ethnic study of atherosclerosis (MESA). Sleep. (2016) 39:1927–40. doi: 10.5665/sleep.6218
36. Kanagasabai T, Ardern CI. Contribution of inflammation, oxidative stress, and antioxidants to the relationship between sleep duration and cardiometabolic health. Sleep. (2015) 38:1905–12. doi: 10.5665/sleep.5238
37. Li J, Zheng D, Loffler KA, Wang X, McEvoy RD, Woodman RJ, et al. Sleep duration and risk of cardiovascular events: the save study. Int J Stroke. (2020). doi: 10.1177/1747493020904913. [Epub ahead of print].
38. Leary EB, Watson KT, Ancoli-Israel S, Redline S, Yaffe K, Ravelo LA, et al. Association of rapid eye movement sleep with mortality in middle-aged and older adults. JAMA Neurol. (2020). doi: 10.1001/jamaneurol.2020.2108. [Epub ahead of print].
39. Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey SG. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. (2008) 27:1133–63. doi: 10.1002/sim.3034
40. Cespedes EM, Hu FB, Redline S, Rosner B, Alcantara C, Cai J, et al. Comparison of self-reported sleep duration with actigraphy: results from the hispanic community health study/study of latinos sueño ancillary study. Am J Epidemiol. (2016) 183:561–73. doi: 10.1093/aje/kwv251
Keywords: stroke, sleep duration, mendelian randomization, genome-wide association study, single nucleotide polymorphism
Citation: Lu H, Wu P-F, Li R-Z, Zhang W and Huang G-x (2020) Sleep Duration and Stroke: A Mendelian Randomization Study. Front. Neurol. 11:976. doi: 10.3389/fneur.2020.00976
Received: 28 June 2020; Accepted: 27 July 2020;
Published: 07 October 2020.
Edited by:
Vincent Thijs, University of Melbourne, AustraliaReviewed by:
Gad Abraham, Baker Heart and Diabetes Institute, AustraliaMaurice Giroud, Centre Hospitalier Regional Universitaire De Dijon, France
Copyright © 2020 Lu, Wu, Li, Zhang and Huang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hui Lu, erjihuixin@163.com; Guo-xiang Huang, hgxcsu@163.com
†These authors have contributed equally to this work