 Martin Paredes-Cruz1,2
Martin Paredes-Cruz1,2 Israel Grijalva3*
Israel Grijalva3* Yoscelina Estrella Martínez-López2
Yoscelina Estrella Martínez-López2 Gabriel Guizar-Sahagún3
Gabriel Guizar-Sahagún3 Eloisa Colín-Ramírez4David Rojano-Mejía5*
Eloisa Colín-Ramírez4David Rojano-Mejía5*- 1Epidemiology and Health Services Research Unit, Siglo XXI National Medical Center, Mexican Social Security Institute (IMSS), Mexico City, Mexico
- 2Doctoral Program in Medical, Dental and Health Sciences, National Autonomous University of Mexico (UNAM), Mexico City, Mexico
- 3Neurological Diseases Research Unit, Siglo XXI National Medical Center, Specialty Hospital of the Highly Specialized Medical Units (UMAE), Mexican Social Security Institute (IMSS), Mexico City, Mexico
- 4School of Sport Sciences, Universidad Anahuac Mexico, Huixquilucan, Mexico
- 5Health Research Coordination Department, Siglo XXI National Medical Center, Mexico City, Mexico
Study design: Systematic review.
Objective: To provide current evidence on the efficacy of 4-aminopyridine (4-AP) to bring about functional improvement in individuals with chronic traumatic spinal cord injury (SCI).
Methods: The Medline (PubMed), Web of Science and SCOPUS databases were systematically searched for relevant articles on the efficacy of 4-AP to treat SCI, from the dates such articles were first published until May 2022. Full-text versions of all the articles selected were examined independently by two reviewers. Methodological quality was rated using the Modified Jadad Scale, and risk of bias was assessed with the RoB-2 test. Data extracted included human models/types, PRISMA assessment protocols, and the results of each study. Descriptive syntheses are provided.
Results: In total, 28 articles were initially identified, 10 of which were included after screening. Most of the studies reviewed reported some degree of patient improvement in one or more of the following parameters: motor, sensitivity and sexual function, sphincter control, spasticity, ability to function independently, quality of life, central motor conduction, pain, and pulmonary function.
Conclusions: This review confirms the efficacy of 4-AP in improving several conditions resulting from SCI but further research on this topic is warranted. Additional randomized clinical trials with 4-AP involving larger sample sizes are needed, as are consistent outcome measures in order to obtain adequate data for analysis with a view to enhance treatment benefits.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=334835, PROSPERO CRD42022334835.
Introduction
Four-Aminopyridine (4-AP) is a potassium-channel blocker with the ability to promote action potentials along demyelinated axons (1, 2). The 4-AP compound also aids synaptic transmission by enhancing the flow of presynaptic calcium currents, a function secondary to blocking the potassium channel (2, 3).
This drug was approved in 2012 as a treatment to help improve ambulatory functions in adults with multiple sclerosis (2). Because of its mechanism of action, 4-AP may also be useful to treat alterations resulting from other neurological conditions such as spinal cord injuries (SCIs) (4, 5).
Less than half of traumatic SCIs involve a completely transected spinal cord, even when neurological loss results in a clinically complete injury (6–8). Similarly, magnetic resonance imaging of people with complete injuries has yielded evidence of spinal cord continuity (8). The extent of SCIs depends on the severity of the primary mechanical traumatic event, as well as on the cascade of subsequent secondary events (7). Nonetheless, nerve fibers crossing the epicenter of the lesion often remain intact (9). Accordingly, pharmacological compounds (such as 4-AP) that enhance electrical conduction in surviving axons have been used to improve the condition of the neural pathways that underly locomotor control. This has led to functional benefits for individuals after injury (9, 10).
Various authors have identified functional improvement in patients with spinal cord injuries, although methodologies and outcomes vary and point to benefits in different areas—mainly motor function, sensitivity, sexual function, sphincter control, spasticity and functional independence—depending on the specific purpose of each study.
In light of the above, we carried out a systematic review to assess the efficacy of 4-AP to improve functionality in traumatic SCI patients.
Methods
Literature search strategy
This systematic review followed the guidelines in Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (11), while the study protocol was registered with PROSPERO (CRD42022334835). We used the following databases to identify studies relevant for an electronic search in current literature: PubMed (MEDLINE), Web of Science and Scopus, until May 26, 2022. In this paper we have used various combinations of the following terms: spinal cord injuries (SCI), 4-aminopyridine (4-AP), patients, and humans. Our search was limited to the following kinds of documents: articles, human clinical trials and literature in English. Our investigation included original research studies investigating the efficacy of 4-AP for treating individuals with traumatic SCI (Figure 1).

Figure 1. PRISMA flow diagram describing the screening and review process (11).
Selection criteria
Our study defined eligibility criteria according to PICOS variables: Population (P), Intervention (I), Comparator (C), Outcome (O) and Study Design (S).
Population. Individuals diagnosed with SCI (either complete or incomplete) who had been given 4-AP in a clinical trial as an intervention to manage or treat their condition.
Intervention. Studies using 4-AP administered both orally and intravenously were included, and all dosage levels were considered.
Comparator. Individuals received either 4-AP or a placebo as comparator.
Results. Included are studies that reported the effect of 4-AP in humans in the context of any long-term quantitative or qualitative clinical outcome. Results included scores for motor and sensory functions, functional independence, sphincter control, sexual function, quality of life, pain, spasticity and central motor conduction. Also included are data on secondary outcomes, like adverse reactions, as indicators of safety.
Study design. Includes primary research studies and randomized clinical trials (RCTs) only, and excludes reviews, pilot studies, prospective studies, retrospective studies and case series, single-case studies, editorial reports, and protocols.
Studies selected and data extracted
We identified articles using the search strategy described above. Based on titles and abstracts, we then eliminated duplicate results and included or excluded articles according to the PICOS criteria indicated. We reexamined the articles, scrutinized their full text and assessed their methodological quality before including them in our systematic review. Next, we rated the quality of the clinical trials according to the Modified Jadad Scale (12). Descriptive syntheses of the findings of all studies are provided in the text and tables below (Tables 1, 2).
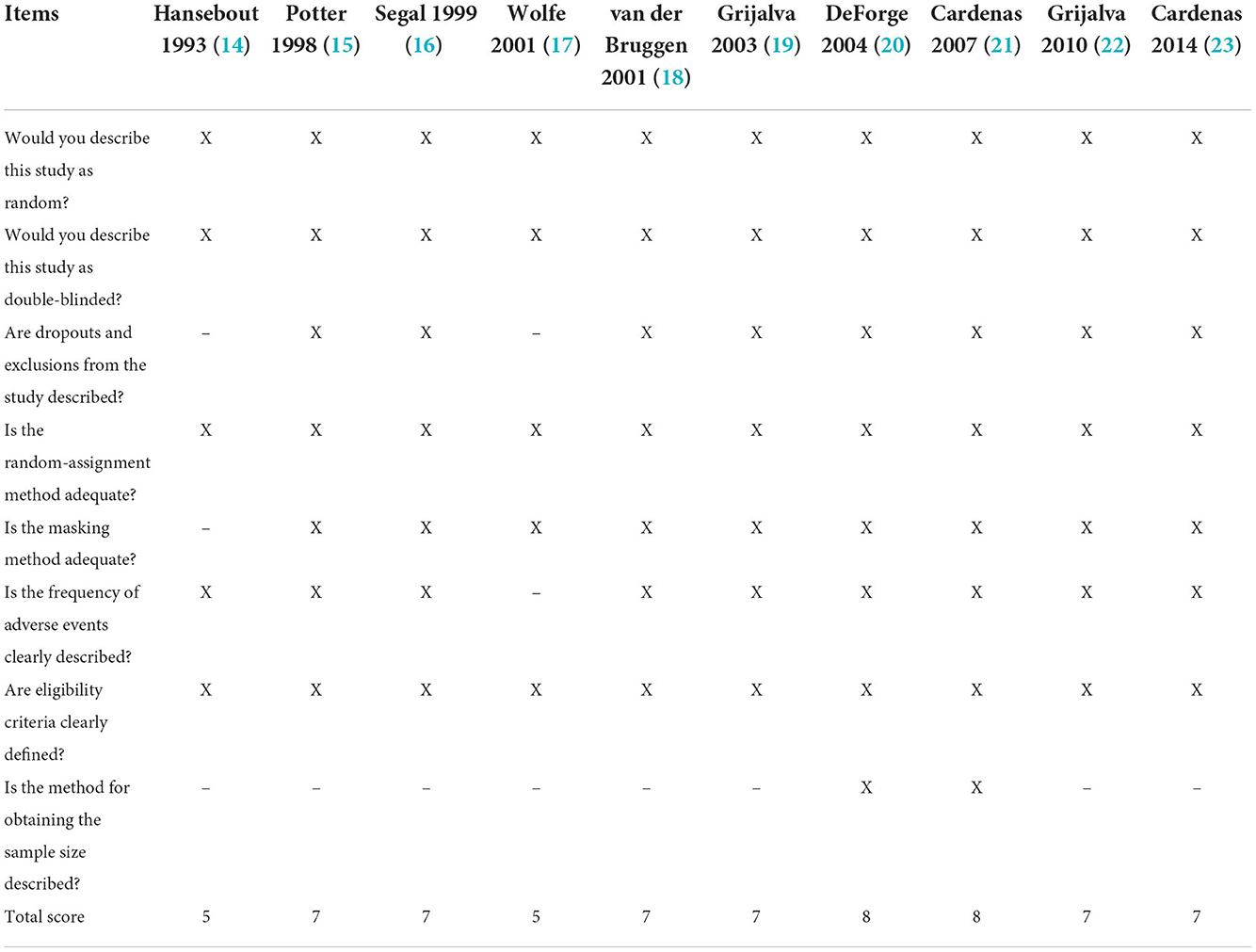
Table 1. Clinical trial quality evaluation using the Modified Jadad Scale.

Table 2. Main characteristics of randomized control trials assessing the effects of 4-aminopyridine on the treatment of spinal cord injury.
After critically evaluating the articles, two reviewers (MPC, YEML) screened the abstracts and full texts, extracted data and utilized a spreadsheet to record the information. Data extraction focused on: author, country, year, inclusion criteria, sample size, intervention, number of participants (at baseline and at the end of the study), duration of treatment, study objectives, as well as significant differences between groups. The team resolved any discrepancies regarding data extraction through discussion.
Assessment of risk of bias in selected trials
In order to assess risk of bias (RoB), the reports were reviewed independently by two reviewers (MPC, YEML) using RoB-2 (Risk of Bias in Randomized Studies to Assess Human-Centered Studies) (13). Through discussion, the team resolved any disagreements over the RoB assessment.
Results
Study selection
This study identified a total of 28 abstracts. After eliminating duplicates and selecting abstracts, 19 articles were considered eligible for full-text evaluation. Of these, 10 were included in the final synthesis as shown in Figure 1 (14–23). Tables 1, 2 provide general descriptions.
Location and study design
The studies took place in Canada (14, 15, 17, 20), the United States (16, 21, 23), Mexico (19, 22) and the Netherlands (18). Median sample size was 23 participants. All studies involved RCTs.
Risk of bias in the selected studies
The results of our bias risk assessment for each trial are shown in Figures 2, 3. All trials were rated low risk of bias for random sequence generation. Nine were classified as low risk of bias for allocation concealment, participant and personnel blinding, as well as for outcome and incomplete results assessment blinding. Two trials were rated as high risk for other biases, primarily because their sample size was small.
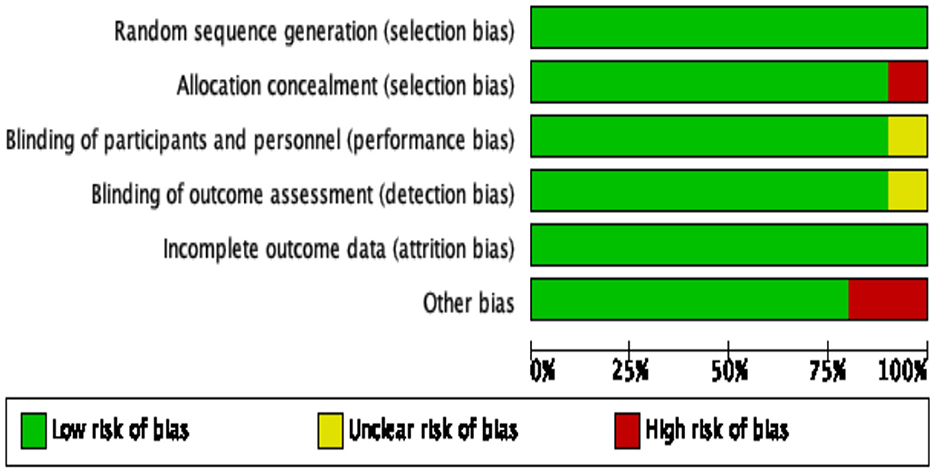
Figure 2. Graphic representation of risk of bias in randomized control trials assessing the effects of 4-aminopyridine on the management of spinal cord injury.

Figure 3. Risk-of-bias summary for randomized control trials assessing the effects of 4-aminopyridine on the management of spinal cord injury.
Efficacy of 4-aminopyridine in individuals with traumatic spinal cord injury
Five of the 10 studies selected used the ASIA Impairment Scale (AIS) and focused on neurological status (motor and sensory control). Improvement was found in four of these variables (14–16, 19) among individuals taking 4-AP as opposed to a placebo. Five studies used the Modified Ashworth Scale to assess spasticity; three of them (14–16) reported improvement. Five studies assessed sexual function; three used the International Index of Erectile Function (IIEF) and two, a clinical interview questionnaire. Four of these five studies indicated improvement (20–23). Three of the four studies that assessed sphincter control found improvement (21–23). Two of the four studies evaluated functional independence using the Spinal Cord Independence Measure (SCIM), while one used the Functional Independence Scale (FIM), and another, the WONCA/COOP Functional Health Assessment Scale. Three of the four studies evaluating functional independence demonstrated improvement (15, 18, 19). Two studies assessed pain with the McGill Pain Questionnaire but only one reported improvement (14). None of the studies that focused on gait speed and vibration perception showed any improvement (18, 20). Each of the following functions was evaluated using a single test for each. All of them identified benefits: central motor conduction was assessed with the Motor Evoked Potentials (MEP) test; quality of life with the 7-point Terrible-Enchanted Scale; and pulmonary function, with an appropriate lung capacity test (Table 2).
Safety
Of the 10 articles included in this review, eight secondarily evaluated 4-AP safety and identified mild-to-moderate adverse events; few articles reported serious events (Table 2).
Discussion
This systematic review examined existing literature on the efficacy of 4-aminopyridine (4-AP) as a treatment for spinal cord injury (SCI). Ten studies were included of which three yielded insufficient results to pool with the findings of other research. The remaining seven studies provided evidence that in various respects 4-AP improved functionality in individuals with traumatic SCI.
In the evidence supported by our systematic review, we observed that efficacy of 4-AP to improve function mainly depends on two circumstances: first, that the tract is preserved and the extent to which it is myelinated (24–30); and second, the main objective of each study. Therefore, it is to be expected that patients will not improve in every way. Significant improvements in neurological status–specifically in motor and sensory functions, functional independence, sphincter control and sexual function–were observed in both men and women, along with improvements in quality of life, pain, spasticity and central motor conduction. Drug intake ranged from a maximum dose of 10 mg per day to 1.45 mg per kilogram of body weight per day. The greatest benefits resulted from higher doses. Administration periods ranged from 2 weeks to 1 year in open-label clinical trials. The greatest changes were identified in individuals with incomplete SCI compared to patients with complete SCI.
There are no RCTs on medium or long-term treatment of spinal cord injury patients with 4-AP. Nevertheless, two Phase III clinical trials of multiple sclerosis evaluated open long-term doses of 10 mg of 4-AP twice a day (20 mg/day) for a maximum period of 5 years. These trials proved that improvements were maintained during long term use and adverse events were similar to those previously reported in prior studies (31, 32). On the other hand, in the experience of our team (still unpublished data) treatment was given to openly enrolled patients for a long-term ranging from 3 months to 3 years during which 4-AP was safe. It appears, and the team considers, that the presence or absence of adverse events depends on personal susceptibility because some patients presented mild adverse events at low doses, while others at high doses presented none. Now, in terms of severe adverse events, convulsions are the events of greatest concern, but in this case it was determined that doses<40 mg/day were safe and no severe adverse events occurred, whereas at doses greater that 40 mg/day the risk of convulsions increased (22, 23). Most of these studies assessed 4-AP safety and identified mild-to-moderate adverse events that would not impede treatment continuity, as well as few serious events, such that 4-AP was considered safe even at high doses (1.45 mg/kg/day) (22). As mentioned before, one of the alleged mechanisms of action of 4-AP is that it increases action potential conduction in demyelinated fibers, thus improving their strength. It is likewise believed that 4-AP increases neuronal excitability and potentiates synaptic transmission (24–29). For all of this, the action and toxicity of this drug could be due to either one of these two mechanisms, however optimal dose to maximize the risk-benefit ratio appears to depend on the amount of axons preserved after the injury, as well as their degree of demyelination.
Unfortunately, not all of the articles included in our review assessed the same outcomes, although 9 of the 10 articles included in this study proved the efficacy of 4-aminopyridine to improve function, particularly motor and sensitivity function (14–16, 19), sexual function (20–23), sphincter control (21–23), functional independence (15, 18, 19), and spasticity (14–16). Although these published articles did not express patient preferences regarding their expectations for improvement, our group's experience indicates that patients assign the greatest importance to functional independence mainly because it involves sphincter control and mobility. Therefore, it will be important to evaluate these two results variables in experimental studies. In terms of these considerations, 7 of the 10 articles included in our own study proved 4-AP efficacy in these variables: 3 showed efficacy in sphincter control (21–23), and 4 in motor function (14–16, 19).
Although the main result of this study demonstrated the efficacy of 4-AP, study variables are heterogeneous and therefore made it difficult to perform a meta-analysis. We recommend that future studies conduct uniform and comprehensive assessments employing the same outcome variables. While some of the studies analyzed demonstrated no statistically significant differences, substantive clinical benefits were achieved. These included walking with the help of devices, enhanced sensation, improved bladder and anal sphincter control, psychogenic erections in men, and improvements in daily living, which provided individuals greater functional independence.
The results were more encouraging when specific functions–bladder and anal sphincter control, quality of life and functional Independence– were comprehensively evaluated along with sensory and motor functions. As noted by Cardenas et al. (21), even minimal improvements in bladder control and sexual function were enormously significant in the daily lives of individuals with chronic SCI.
Despite improvements in gait brought about by administering 4-AP to individuals with multiple sclerosis, clinically significant, long-lasting effects appeared soon after initiation of treatment, yet disappeared shortly after drug withdrawal (31–34). In the case of individuals with SCI, however, such benefits appeared to last even after treatment had ended (14, 16, 19, 22).
Other studies indicated that the effects of 4-AP seemed to differ depending on the selection of “responsive participants,” where different variables were in play: (a) the severity of the injury, as individuals with cervical injury apparently showed greater improvement than those with thoracic or lumbar injury; (b) the type of injury (complete or incomplete AIS classification), SCIs were not uniform and affected ascending and descending tracts in a variety of ways—the recovery of a function depended on the tract affected, so improvement varied in each individual; and (c) the phase of the injury: in the acute phase, preserved axons were demyelinated or insufficiently myelinated and therefore, long-term myelination in the chronic phase could support response to treatment. All of the above factors make it difficult to evaluate the efficacy of any pharmacological intervention among this population (14, 16, 19, 35, 36).
Clinical efficacy of 4-AP is currently still under evaluation via randomized controlled clinical trials in pathologies such as multiple sclerosis (NCT01576354), spinal cord injury (NCT03899584, NCT05447676, NCT01621113), Guillain-Barré syndrome (NCT00056810), among others.
Limitations
Limiting this systematic review to literature in English entailed the risk of language bias in our selection of studies, while the inclusion of studies with heterogeneous results did not allow us to perform a meta-analysis, only a qualitative synthesis.
Varied outcome measures were used in the studies reviewed, which made it difficult to compare results. We found considerable variation among studies in terms of route, dose, and/or duration of treatment with 4-AP. All these factors were also considered limitations when evaluating the efficacy of this drug.
Conclusion
There is a dearth of literature on the efficacy and safety of 4-AP in treating individuals with traumatic SCI. Although this systematic review provides information showing that 4-AP is an effective treatment for improving some functions after chronic SCI, further randomized clinical trials with 4-AP involving larger sample sizes are needed. Future research should use uniform outcome measures to allow adequate data acquisition and analysis.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Author contributions
DR-M and IG supervised the findings. MP-C and YM-L contributed to data collection, extraction, and analysis and developed the theory. IG, EC-R, GG-S, and DR-M made critical contributions and final approval of the manuscript. All authors discussed the results and contributed to the final manuscript.
Acknowledgments
MP-C is a doctoral student. This work is part of the requirements to earn a Doctor of Sciences degree from the Medical, Dental and Health Sciences program at the National Autonomous University of Mexico (UNAM). The National Council of Science and Technology (CONACYT) granted MP-C a postgraduate scholarship (CVU 630343).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Smith KJ, Felts PA, John GR. Effects of 4-aminopyridine on demyelinated axons, synapses and muscle tension. Brain. (2000) 123:171–84. doi: 10.1093/brain/123.1.171
2. Wiener J, Hsieh J, McIntyre A, Teasell R. Effectiveness of 4-aminopyridine for the management of spasticity in spinal cord injury: a systematic review. Top Spinal Cord Inj Rehabil. (2018) 24:353–62. doi: 10.1310/sci17-00048
3. Donovan WH, Halter JA, Graves DE, Blight AR, Calvillo O, McCann MT, et al. Intravenous infusion of 4-AP in chronic spinal cord injured subjects. Spinal Cord. (2000) 38:7–15. doi: 10.1038/sj.sc.3100931
4. Shi R, Sun W. Potassium channel blockers as an effective treatment to restore impulse conduction in injured axons. Neurosci Bull. (2011) 27:36–44. doi: 10.1007/s12264-011-1048-y
5. Yan R, Page JC, Shi R. Acrolein-mediated conduction loss is partially restored by K? channel blockers. J Neurophysiol. (2016) 15:701–10. doi: 10.1152/jn.00467.2015
6. Kakulas BA, Kaelan C. The neuropathological foundations for the restorative neurology of spinal cord injury. Clin Neurol Neurosurg. (2015) 129(Suppl. 1):S1–7. doi: 10.1016/j.clineuro.2015.01.012
7. Bunge RP, Puckett WR, Hiester ED. Observations on the pathology of several types of human spinal cord injury, with emphasis on the astrocyte response to penetrating injuries. Adv Neurol. (1997) 72:305–15.
8. Bunge RP, Puckett WR, Becerra JL, Marcillo A, Quencer RM. Observations on the pathology of human spinal cord injury. A review and classification of 22 new cases with details from a case of chronic cord compression with extensive focal demyelination. Adv Neurol. (1993) 59:75–89.
9. Baptiste DC, Fehlings MG. Emerging drugs for spinal cord injury. Expert Opin Emerg Drugs. (2008) 13:63–80. doi: 10.1517/14728214.13.1.63
10. Domingo A, Al-Yahya AA, Asiri Y, Eng JJ, Lam T. Spinal cord injury rehabilitation evidence research team. A systematic review of the effects of pharmacological agents on walking function in people with spinal cord injury. J Neurotrauma. (2012) 29:865–79. doi: 10.1089/neu.2011.2052
11. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. (2010) 8:336–41. doi: 10.1016/j.ijsu.2010.02.007
12. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. (1996) 17:1–12. doi: 10.1016/0197-2456(95)00134-4
13. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomized trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
14. Hansebout RR, Blight AR, Fawcett S, Reddy K. 4-Aminopyridine in chronic spinal cord injury: a controlled, double-blind, crossover study in eight patients. J Neurotrauma. (1993) 10:1–18. doi: 10.1089/neu.1993.10.1
15. Potter PJ, Hayes KC, Segal JL, Hsieh JT, Brunnemann SR, Delaney GA, et al. Randomized double-blind crossover trial of fampridine-SR (sustained release 4-aminopyridine) in patients with incomplete spinal cord injury. J Neurotrauma. (1998) 15:837–49. doi: 10.1089/neu.1998.15.837
16. Segal JL, Pathak MS, Hernandez JP, Himber PL, Brunnemann SR, Charter RS. Safety and efficacy of 4-aminopyridine in humans with spinal cord injury: a long-term, controlled trial. Pharmacotherapy. (1999) 19:713–23. doi: 10.1592/phco.19.9.713.31540
17. Wolfe DL, Hayes KC, Hsieh JT, Potter PJ. Effects of 4-aminopyridine on motor evoked potentials in patients with spinal cord injury: a double-blinded, placebo-controlled crossover trial. J Neurotrauma. (2001) 18:757–71. doi: 10.1089/089771501316919120
18. Van der Bruggen MA, Huisman HB, Beckerman H, Bertelsmann FW, Polman CH, Lankhorst GJ. Randomized trial of 4-aminopyridine in patients with chronic incomplete spinal cord injury. J Neurol. (2001) 248:665–71. doi: 10.1007/s004150170111
19. Grijalva I, Guízar-Sahagún G, Castañeda-Hernández G, Mino D, Maldonado-Julián H, Vidal-Cantú G, et al. Efficacy and safety of 4-aminopyridine in patients with long-term spinal cord injury: a randomized, double-blind, placebo-controlled trial. Pharmacotherapy. (2003) 23:823–34. doi: 10.1592/phco.23.7.823.32731
20. DeForge D, Nymark J, Lemaire E, Gardner S, Hunt M, Martel L, et al. Effect of 4-aminopyridine on gait in ambulatory spinal cord injuries: a double-blind, placebo-controlled, crossover trial. Spinal Cord. (2004) 42:674–85. doi: 10.1038/sj.sc.3101653
21. Cardenas DD, Ditunno J, Graziani V, Jackson AB, Lammertse D, Potter P, et al. Phase 2 trial of sustained-release fampridine in chronic spinal cord injury. Spinal Cord. (2007) 45:158–68. doi: 10.1038/sj.sc.3101947
22. Grijalva I, García-Pérez A, Díaz J, Aguilar S, Mino D, Santiago-Rodríguez E, et al. High doses of 4-aminopyridine improve functionality in chronic complete spinal cord injury patients with MRI evidence of cord continuity. Arch Med Res. (2010) 41:567–75. doi: 10.1016/j.arcmed.2010.10.001
23. Cardenas DD, Ditunno JF, Graziani V, McLain AB, Lammertse DP, Potter PJ, et al. Two phase 3, multicenter, randomized, placebo-controlled clinical trials of fampridine-SR for treatment of spasticity in chronic spinal cord injury. Spinal Cord. (2014) 52:70–6. doi: 10.1038/sc.2013.137
24. Lewis MJ, Howard JF Jr, Olby NJ. The relationship between trans-lesional conduction, motor neuron pool excitability, and motor function in dogs with incomplete recovery from severe spinal cord injury. J Neurotrauma. (2017) 34:2994–3002. doi: 10.1089/neu.2017.5012
25. Lewis MJ, Laber E, Olby NJ. Predictors of response to 4-amynopiridine in chronic canine spinal cord injury. J Neurotrauma. (2019) 36:1428–34. doi: 10.1089/neu.2018.5975
26. Blight AR. Effect of 4-aminopyridine on axonal conduction-block in chronic spinal cord injury. Brain Res Bull. (1989) 22:47–52. doi: 10.1016/0361-9230(89)90126-3
27. Sherratt RM, Bostock H, Sears TA. Effects of 4-aminopyridine on normal and demyelinated mammalian nerve fibres. Nature. (1980) 283:570–2. doi: 10.1038/283570a0
28. Hayes KC. 4-aminopyridine and spinal cord injury: a review. Restor Neurol Neurosci. (1994) 6:259–70. doi: 10.3233/RNN-1994-6401
29. Sedehizadeh S, Keogh M, Maddison P. The use of aminopyridines in neurological disorders. Clin Neuropharmacol. (2012) 35:191–200. doi: 10.1097/WNF.0b013e31825a68c5
30. Hayes KC. Fampridine-SR for multiple sclerosis and spinal cord injury. Expert Rev Neurother. (2007) 7:453–61. doi: 10.1586/14737175.7.5.453
31. Goodman AD, Bethoux F, Brown TR, Schapiro RT, Cohen R, Marinucci LN, et al. Long-term safety and efficacy of dalfampridine for walking impairment in patients with multiple sclerosis: results of open-label extensions of two Phase 3 clinical trials. Mult Scler. (2015) 21:1322–31. doi: 10.1177/1352458514563591
32. Goodman AD, Cohen JA, Cross A, Vollmer T, Rizzo M, Cohen R, et al. Fampridine-SR in multiple sclerosis: a randomized, double-blind, placebo-controlled, dose-ranging study. Mult Scler. (2007) 13:357–68. doi: 10.1177/1352458506069538
33. Castelnovo G, Gerlach O, Freedman MS, Bergmann A, Sinay V, Castillo-Triviño T, et al. Safety, patient-reported well-being, and physician-reported assessment of walking ability in patients with multiple sclerosis for prolonged-release fampridine treatment in routine clinical practice: results of the LIBERATE study. CNS Drugs. (2021) 35:1009–22. doi: 10.1007/s40263-021-00840-x
34. Goodman AD, Brown TR, Edwards KR, Krupp LB, Schapiro RT, Cohen R, et al. A phase 3 trial of extended release oral dalfampridine in multiple sclerosis. Ann Neurol. (2010) 68:494–502. doi: 10.1002/ana.22240
35. Hayes KC, Blight AR, Potter PJ, Allatt RD, Hsieh JT, Wolfe DL, et al. Preclinical trial of 4-aminopyridine in patients with chronic spinal cord injury. Paraplegia. (1993) 31:216–24. doi: 10.1038/sc.1993.40
Keywords: 4-aminopyridine, spinal cord injury, functional improvement, efficacy, motor function, sensitive functions, sphincter control, clinical trials
Citation: Paredes-Cruz M, Grijalva I, Martínez-López YE, Guizar-Sahagún G, Colín-Ramírez E and Rojano-Mejía D (2022) Functional improvement in individuals with chronic spinal cord injury treated with 4-aminopyridine: A systematic review. Front. Neurol. 13:1034730. doi: 10.3389/fneur.2022.1034730
Received: 01 September 2022; Accepted: 11 November 2022;
Published: 29 November 2022.
Edited by:
Ulises Gomez-Pinedo, Health Research Institute of Hospital Clínico San Carlos, SpainReviewed by:
Marco Rovaris, Santa Maria Nascente, Fondazione Don Carlo Gnocchi Onlus (IRCCS), ItalyAlejandro A. Canales-Aguirre, CONACYT Centro de Investigación y Asistencia en Tecnología y Diseño del Estado de Jalisco (CIATEJ), Mexico
Copyright © 2022 Paredes-Cruz, Grijalva, Martínez-López, Guizar-Sahagún, Colín-Ramírez and Rojano-Mejía. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Rojano-Mejía, rojanodavid@gmail.com; Israel Grijalva, igrijalvao@yahoo.com