 Marion Mortamais1*
Marion Mortamais1* Meriem Abdennour1
Meriem Abdennour1 Valérie Bergua2
Valérie Bergua2 Christophe Tzourio2
Christophe Tzourio2 Claudine Berr1
Claudine Berr1 Audrey Gabelle1,3
Audrey Gabelle1,3 Tasnime N. Akbaraly4,5,6
Tasnime N. Akbaraly4,5,6- 1Institut National de la Santé et de la Recherche Médicale, Université de Montpellier, Neuropsychiatry: Epidemiological and Clinical Research, Montpellier, France
- 2University of Bordeaux, Institut National de la Santé et de la Recherche Médicale, Bordeaux Population Health Research Center, UMR 1219, CHU Bordeaux, Bordeaux, France
- 3Memory Resources and Research Center, Department of Neurology, Gui de Chauliac Hospital, Montpellier, France
- 4MMDN, Université de Montpellier, EPHE, Institut National de la Santé et de la Recherche Médicale, U1198, Montpellier, France
- 5Department of Epidemiology and Public Health, University College London, London, United Kingdom
- 6Autism Resources Centre of Languedoc-Roussillon, University Hospital of Montpellier, CHRU de Montpellier, Montpellier, France
Background: Anxiety is common in patients with cognitive impairment and dementia. However, whether anxiety is a risk factor for dementia is still not known. We aimed to examine the association between trait anxiety at baseline and the 10-year risk of incident dementia to determine to which extent depressive symptoms influence this relationship in the general population.
Methods: Data came from 5,234 community-dwelling participants from the Three-City prospective cohort study, aged 65 years at baseline and followed over 10 years. At baseline, anxiety trait was assessed using the Spielberger State-Trait Anxiety Inventory (STAI), and depressive symptoms using Center for Epidemiologic Studies-Depression Scale (CESD). Use of anxiolytic drugs was also considered. Diagnoses of dementia were made at baseline and every 2 years. To examine the relationship between anxiety exposures and risk of incident dementia, Cox proportional hazard regression models were performed.
Results: Taking anxiolytic drugs or having high trait anxiety (STAI score ≥ 44) increased the risk of dementia assessed over 10 years of follow-up [Hazard Ratio (HR) = 1.39, 95%CI: 1.08–1.80, p = 0.01 and HR = 1.26, 95%CI: 1.01–1.57, p = 0.04, respectively], independently of a large panel of socio-demographic variables, health behaviors, cardio-metabolic disorders, and additional age-related disorders such as cardiovascular diseases, activity limitations, and cognitive deficit. However, the associations were substantially attenuated after further adjustment for depressive symptoms.
Conclusion: Our findings suggest that depressive symptoms shape the association between anxiety trait and dementia. Further research is needed to replicate our findings and extrapolate our results to anxiety disorders.
Introduction
Anxiety and depression are common in patients with cognitive impairment and dementia (Lyketsos et al., 2002; Geda et al., 2008; Steinberg et al., 2008; Ausén et al., 2009; Rosenberg et al., 2011). The high prevalence of those neuropsychiatric symptoms reported in cognitive impaired populations raises the question of the exact nature of their relationships and the causality link regarding age-related cognitive disorders (Livingston et al., 2017).
Depression has been extensively studied in relation to dementia and Alzheimer's disease. Even if its role-prodrome (Heser et al., 2013; Singh-Manoux et al., 2017) or risk factor (Jorm, 2000)-is still under debate, its independent association with dementia has been evidenced. In contrast, very few studies examined whether anxiety is independently associated with cognitive aging outcomes. Anxiety is often viewed as a psychological reaction to cognitive deterioration and most studies examining the anxiety-cerebral aging outcomes are cross-sectional, making an assessment of the direction of the association impossible. Amongst the few available prospective studies (Palmer et al., 2007; Devier et al., 2009; Gallacher et al., 2009; Wilson et al., 2011; Rosenberg et al., 2013), a positive association between anxiety and dementia has been reported in two studies (Wilson et al., 2011; Kassem et al., 2017), but not in Gallacher et al.'s study, carried out in general populations (Gallacher et al., 2009). Similar inconsistencies have been reported in the literature examining associations between anxiety and risk of transition to dementia in Mild Cognitive Impairment (MCI—a prodromal state of dementia) patients (Palmer et al., 2007; Teng et al., 2007; Devier et al., 2009; Ramakers et al., 2010; Rosenberg et al., 2013).
The differences in anxiety assessment, the follow-up duration generally lower than 5 years (precluding to account the preclinical phase of dementia during which dementia physiopathological processes are active), the sample heterogeneity, and the choice of adjustment variables may partly explain those inconsistent findings. In particular, depression, a frequent comorbidity of anxiety (Beekman et al., 2000; Zimmerman et al., 2000) which could share some risk factors (Roy et al., 1995; Grant et al., 2009) or even could be initiated by anxiety (Potvin et al., 2013), is not considered systematically as an adjustment factor in every study while it appears to attenuate the relationship between anxiety and risk of dementia (Gallacher et al., 2009).
The main objective of the present study was to examine the association between the risk of incident dementia and trait anxiety -a measure of individual differences in anxiety-proneness which reflects the tendency to perceive stressful situations as dangerous or threatening (Spielberger, 1983)- in an elderly general population over a 10-year follow-up period. Remaining relatively stable over time and being more related to personality than state anxiety, trait anxiety is likely to be present before the clinical manifestations of dementia and we hypothesized that it could be associated with an increased dementia risk. Additionally, because of their frequent overlap, we aimed to determine the influence of depressive symptoms in the relationship between trait anxiety and risk of dementia.
Methods
Participants
Participants were recruited as part of a multisite cohort study of community-dwelling older adults conducted in three French cities Bordeaux, Dijon, and Montpellier between 1999 and 2001: The Three-City (3C) Study (3C Study Group, 2003). The inclusion criteria were to be living in these cities or their suburbs and registered on the electoral rolls, to be aged 65 years and over, and not to be institutionalized. The cohort size was set at 10,000 participants (2,500 in Bordeaux, 2,500 in Montpellier, and 5,000 in Dijon) and administrative districts were selected in each city accordingly. Eligible inhabitants of the selected districts were invited to participate through a personal letter.
Of the 9,294 participants originally included (acceptance rate of 37%), we excluded 214 with dementia diagnosed at baseline clinical examination (1999–2001). We further excluded 487 participants with cognitive impairment assessed by a Mini Mental State Examination (MMSE) score ≤ 24 at baseline (Figure 1).
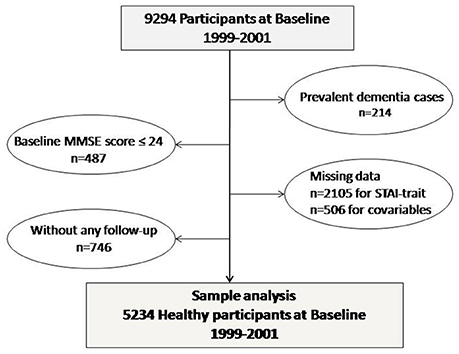
Figure 1. Sample analysis.
Seven hundred and forty-six participants did not have the next follow-ups (at 2, 4, 8, and 10 years after baseline). The present analyses carried out on 5,234 participants for whom complete and validated data on anxiety, depressive symptoms, dementia diagnosis, and covariates were available as detailed in the flow-chart diagram (Figure 1). Compared to participants included, the 3,357 excluded participants were significantly older and were more likely to have high score in anxiety and depressive symptoms scales and lower cognitive performances at baseline (data available on request).
Standard Protocol Approvals, Registrations, and Patient Consents
The study protocol was approved by the Ethics Committee of the Hospital of Kremlin-Bicêtre and Sud-Méditerranée III. A written informed consent was obtained from all patients participating in the study (consent for research).
Incidence of Dementia Over 10 Years
At baseline, diagnosis of dementia was based on a 3-step procedure (3C Study Group, 2003; Akbaraly et al., 2009). First, trained psychologists administered a battery of neuropsychological tests detailed elsewhere (3C Study Group, 2003). Second, all the participants in Montpellier were then examined by a neurologist, whereas in Dijon and Bordeaux, because of the larger number of participants, only those who screened positive underwent further examination. Finally, an independent committee of neurologists reviewed all potential prevalent and incident cases of dementia to obtain a consensus on its diagnosis and etiology according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (American Psychiatry Association, 2000). Cases of Alzheimer's Disease (AD) were classified according to the National Institute of Neurological and Communicative Disorders and Stroke–Alzheimer's Disease and Related Disorders Association (McKhann et al., 1984) and cases of mixed/vascular dementia according to the National Institute of Neurological Disorders and Stroke–Association Internationale pour la Recherche en l'Enseignement en Neurosciences (Román et al., 1993).
Same procedures were performed at the next four follow-up phases (at 2, 4, 8, and 10 years after baseline) allowing to consider incident dementia screening over a total of 10 years of follow-up.
Anxiety Exposures Assessed in 1999/2001
Anxiety was assessed using the Spielberger State-Trait Anxiety Inventory (STAI) (Spielberger, 1983)—a psychological inventory based on a self-report basis. The STAI consists of 40 items based on a 4-point Likert Scale and is commonly used to measure two types of anxiety -the state anxiety (S-anxiety) and the trait anxiety (T-anxiety). The T-anxiety subscale remains relatively stable over time corresponding to anxiety level as a personal characteristic and was considered alone in the present study. The total score of the T-anxiety subscale ranges from 20 to 80, with higher scores positively correlated with higher levels of anxiety symptoms.
An inventory of all drugs (prescription and over-the-counter drugs) used during the preceding month of the clinical examination was included in a standardized interview. Medical prescriptions and, where feasible, the medications themselves were checked by the interviewer. Use of anxiolytic drugs including benzodiazepine, diphenylmethane, dibenzo-bicyclo-octadiene, azaspirodecanedione derivatives, and carbamates, mephenoxalone, gedocarnil, and etifoxin (ATC codes: N05B) have then been considered.
Covariates Assessed in 1999/2001
Socio-Demographic
Socio-demographic variables consisted of sex, age, study center, marital status (living alone/not living alone), educational level (≤ 9 years/>9 years).
Health Behaviors
Health behaviors variables were smoking habits (never/ex or current smoker) and alcohol consumption (null/moderate if < 15 glasses of alcohol per week for women and 22 for men, or important if ≥ 15 for women and 22 for men, according to the recommendations about low and high risk alcohol consumption of the French Health High Authority (Haute Autorité de Santé, 2014).
Health Status
Health status related covariates included vascular risk factors: body mass index (BMI) calculated from height and weight measurements performed during the clinical examination at baseline, dyslipidemia (plasma cholesterol ≥6.20 mmol/l or using lipid-lowering drugs), diabetes (glycemia ≥ 5.55 mmol/l or taking anti-diabetic treatment), hypertension (systolic/diastolic blood pressure ≥140/≥90 mm Hg or taking antihypertensive drugs) and history of vascular pathology was composed of self-reported variables and included history of stroke, angina pectoris, myocardial infarction, coronary surgery, coronary angioplasty, and arterial surgery of the legs for arteritis. Limitations in activities of daily living (IADL) using the Lawton–Brody scale (Lawton and Brody, 1969) (score > 0), and “low” cognitive performances defined by a score ≤ 27 on the MMSE have also been considered. Depressive symptoms were assessed using the Center for Epidemiologic Studies-Depression Scale (CESD) (Radloff, 1977). Participants with CESD score >16 or taking antidepressant treatment (ATC code: N06A) were considered as having depressive symptoms.
Statistical Analyses
According to the norms established in the elderly population (Bergua et al., 2012), T-anxiety subscale score was considered as high trait anxiety for scores higher than the first quartile (score ≥ 44 defined as “high trait anxiety” being compared with the score < 44, “low trait anxiety”).
Wilcoxon tests for quantitative variables and Chi2 tests for qualitative variables were used to compare characteristics of participants according to the dementia status at the end of the follow-up period.
To examine the relationship between anxiety exposures and risk of incident dementia over the 10-year follow-up period, Cox proportional hazard regression models with delayed entry (Lamarca et al., 1998) were performed with age as the basic timescale and birth date as the time origin. Results of proportional-hazard regression analyses were expressed as hazard ratios (HR) with 95% confidence intervals (CI). Participants who died or were lost to follow-up without dementia were censored at their age of death or at the last cognitive examination, respectively. The date of dementia onset was set half way between the date of the last follow-up visit when the subject was classified as normal and the date of diagnosis. We first investigated the association between anxiety exposures and risk of dementia in a model adjusted for age, sex, and center. Then we progressively entered in 2 different multivariate models the others possible confounders (education achievement, living alone, smoking habits, alcohol intake, BMI, vascular risk factors, limitations in IADL, and cognitive performances). Finally, to assess whether anxiety and depressive symptoms were independently associated with the risk of dementia, a fourth model was performed in which depressive symptoms and anxiety were simultaneously included. In addition, contribution of depression to the anxiety/risk of dementia relationship, as well as the contribution of anxiety to the depressive symptoms/risk of dementia association were examined in determining the percent attenuations (MacKinnon and Dwyer, 1993). These percent attenuations were calculated using the formula [(βANXIETY − βANXIETY adjusted for DEP_SYMPTOMS)/βANXIETY] × 100 and [(βDEP_SYMPTOMS − βDEP_SYMPTOMS adjusted for ANXIETY)/βDEP_SYMPTOMS] × 100, where the βs are the coefficients estimated from the Cox models.
The level of statistical significance was set at p < 0.05. Analyses were conducted using SAS software, version 9.4 (SAS Institute).
Results
Among the 5,234 participants with anxiety assessment at baseline, a total of 378 new cases of dementia were diagnosed over the 10 years of follow-up (57 diagnosed at the 2-year follow-up, 67 at the 4-year, 153 at the 8-year, and 101 at the 10-year follow-up period) including 259 cases of probable AD (69%), 23 cases of vascular dementia (6%), 50 cases of mixed dementia (13%), and 46 cases of other dementia types.
Seven hundred and fifty-two participants died (14%) and 1173 (22%) were lost to follow-up or refused to continue the study. Participants who were lost to follow-up were significantly older, had more frequently depressive symptomatology and anxiolytic treatment, had lower MMSE scores at baseline but did not show differences in T-anxiety subscale scores (data not shown).
Table 1 describes the characteristics of the 5,234 participants included as a function of new-onset of dementia. Compared to non-demented participants, those who developed dementia over the 10 years of follow-up were significantly older, less likely to reach a high educational achievement and more likely to live alone, to have diabetes past history of vascular diseases, depressive symptoms, IADL limitations, and lower cognitive performances. They also were more likely to have higher anxiety levels measured by the T-anxiety subscale and to use anxiolytic drugs.
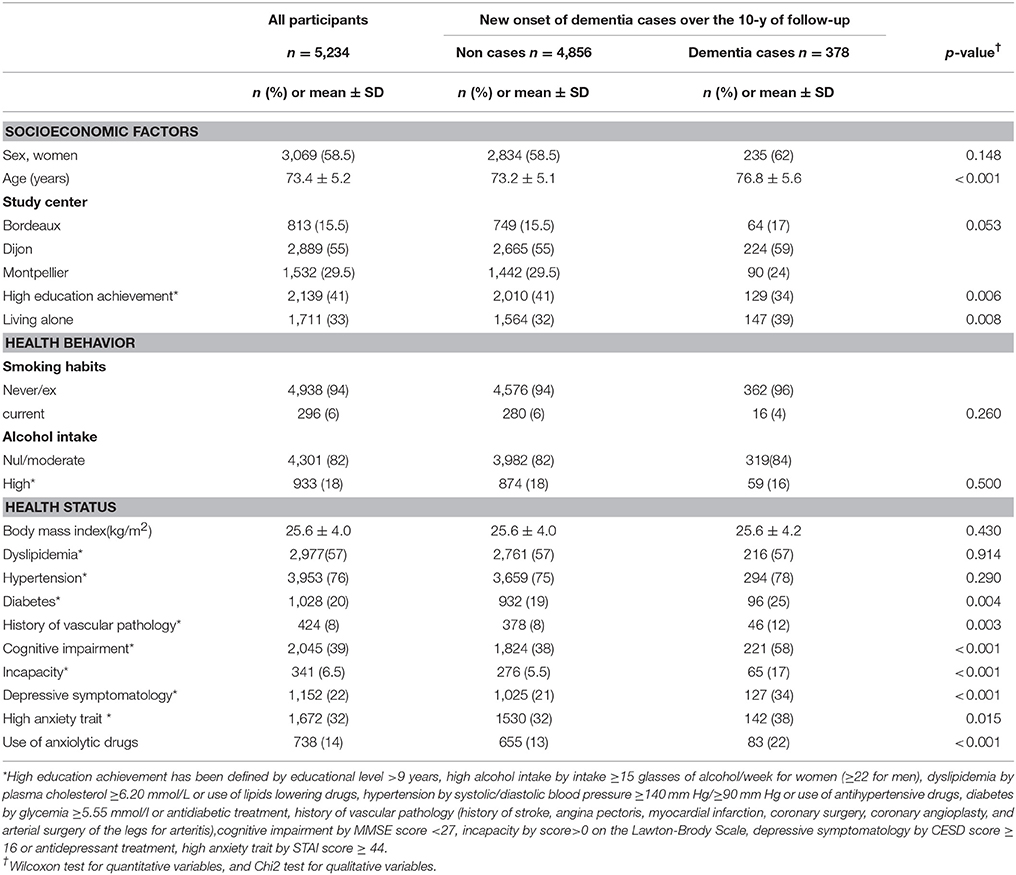
Table 1. Baseline characteristics of the 5,234 participants as a function of new onset of dementia.
The comparison of characteristics of participants according to tertiles of T-anxiety subscale score showed that participants with high anxiety trait were more likely to have lower education achievement, to live alone, to be non-smokers, to have low alcohol consumption and to present dyslipidemia, lower BMI, IADL limitations, depressive symptoms, and to take anxiolytic drugs than participants with low anxiety trait (Table S1).
The associations between anxiety exposure and 10-year incidence of dementia have been estimated by proportional hazards models in which both anxiety trait and use of anxiolytic drugs were included. Results are presented in Figure 2. After adjustment for age, sex, and study center, anxiety levels and use of anxiolytic drugs were both independently associated with higher risk of developing dementia. Participants with high trait anxiety showed a 28% increased risk of dementia compared to those with low trait anxiety, those under anxiolytic drugs had a 52% increased hazard ratio of dementia compared to participants not using anxiolytics. Further adjustment for education, marital status, health behaviors (smoking habits and alcohol intake), BMI, history of vascular pathology, metabolic disorder (hypertension, diabetes, dyslipidemia), incapacity and cognitive impairment (Model 2 and Model 3) had little effect on estimates (for T-anxiety scale: HRHigh vs. Low = 1.26; 95% CI: 1.01–1.57; for use of anxiolytic drugs: HRYes vs. No = 1.39, 95% CI: 1.08–1.80).
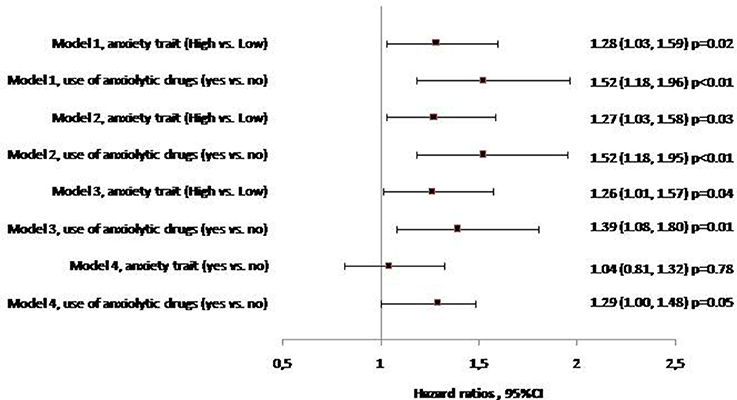
Figure 2. Relationship between anxiety trait, use of anxiolytic drugs and 10-year risk of incident dementia (Multivariate Cox Proportional Hazard Models, n = 5,234, n. event = 378).
Model 1: Adjustment for age, sex, center.
Model 2: Model 1 and smoking habits, alcohol intake, education, living alone.
Model 3: Model 2 and body mass index, history of vascular pathology, hypertension, diabetes, dyslipidemia, incapacity, MMSE at baseline.
Model 4: Model 3 and depressive symptoms.
Joint Association Between Anxiety Exposures, Depressive Symptoms, and the Risk of Incident Dementia
To further examine whether anxiety exposures and depressive symptoms were independently associated with the risk of incident dementia, a full adjusted model including simultaneously anxiety exposures and depressive symptoms was run. The T-anxiety subscale–dementia association after adjustment for depressive symptoms was substantially attenuated and did not significantly persist statistically. Similar observations were reported for the anxiolytic drugs–dementia association (Figure 2). Calculation of the percent attenuation showed that depressive symptoms attenuated the association between high trait anxiety and risk of dementia by 84.7% and the anxiolytic drugs- dementia association by 22.4% (Table 2). Conversely, high trait anxiety and use of anxiolytic drugs attenuated the association between depressive symptoms and risk of dementia by only 4.5 and 8.3%, respectively, and by 11% when included simultaneously. After adjustment for both anxiety exposures, only depressive symptoms remained significantly associated with an increased risk of dementia [β = 0.409 (0.130), p < 0.001].
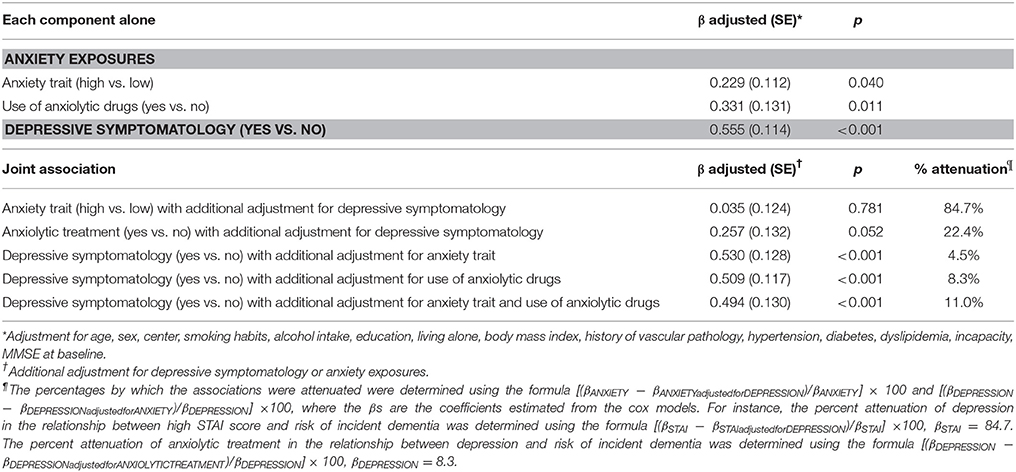
Table 2. Joint association between anxiety exposures, depression and 10-year risk of incident dementia.
To further explore whether the association between anxiety exposures and dementia risk depends on the depressive symptoms, we performed supplementary analyses to assess the interaction between trait anxiety and depressive symptoms. Main analyses assessing the association between anxiety exposures and dementia risk were also repeated by stratifying them on depressive symptoms (Figure S1). Finally the risk of dementia has been compared between the following four groups of participants: no anxiety/no depressive symptoms (reference group), no anxiety/depressive symptoms, anxiety/no depressive symptoms, and anxiety/depressive symptoms, with anxiety defined as having high trait anxiety or taking anxiolytic treatment. Results reported in Figure S2 did not evidence interaction between depressive symptoms and anxiety exposures regarding dementia risk (p = 0.90 and p = 0.86, respectively).
Discussion
The present study carried out in a large sample of elderly men and women showed that anxiolytic drugs and having high trait anxiety increased (by 40 and 25%, respectively) the risk of dementia assessed over 10 years of follow-up. Those associations were independent of a large panel of socio-demographic, health behaviors, cardio-metabolic disorders, and additional age-related disorders such as cardiovascular diseases, activity limitations, and cognitive deficit. However those anxiety exposures-dementia associations were shaped by depressive symptoms playing a strong role of confounder.
Those results are in agreement with those of the literature. In the Caerphilly dementia study (Gallacher et al., 2009), no significant association between high trait anxiety and risk of developing dementia were observed in 1,481 men followed for a 17-year period when adjusted for depression (evaluated with the 30-item general health questionnaire). However, as long as we did not consider depressive symptoms in our statistical models, our findings -showing a significant increased risk of dementia in participants with anxiety- are in line with the prospective studies in which confounding role of depressive symptoms was not considered and carried out in general populations (Wilson et al., 2011; Kassem et al., 2017) as well as in MCI patients (Palmer et al., 2007; Rosenberg et al., 2013).
In our sample, we observed that participants with a high score to T-anxiety subscale of the STAI (≥44) had a 25% higher risk of developing dementia than participants with a score < 44 independently of socio-economic, health behavior, or health status factors. However, introduction of depressive symptomatology as an adjustment factor strongly attenuated (84.7%) the relationship between trait anxiety and risk of dementia, which was no longer significant. Conversely, anxiety trait and use of anxiolytic drugs did not fundamentally change the relationship between depressive symptoms and risk of dementia, which remained significant. In addition, the absence of interaction between depressive symptoms and anxiety exposures regarding dementia risk did not support the hypothesis that the direction and the magnitude of the anxiety exposure–dementia risk association depends on the depressive symptoms. Our findings thus suggest that depressive symptomatology is a strong confounder of the anxiety-dementia relationship. In other words, when depressive symptomatology is not taken into account, the association between trait anxiety and risk of dementia may actually reflect the comorbidity of anxiety with depression. Co-occurrence of depression and anxiety are common throughout the life cycle (Regier et al., 1988; Beekman et al., 1998; Kessler et al., 2010). However, the mechanisms underlying this close relationship are still under debate. It remains unclear whether anxiety and depression share a common etiology (Roy et al., 1995; Grant et al., 2009), or whether anxiety is a prodromal stage of depression (Potvin et al., 2013). Consideration of a dimensional classification including both depression and anxiety has been suggested to be more appropriate in the elderly (Schoevers et al., 2003), and some prospective studies have even shown that the related concept of psychological distress, a mixture of anxiety and depression, was associated with AD (Wilson et al., 2003, 2005). Similarly, an overlap between anxiolytic treatment and depression is frequent. Indeed, anxiolytic drugs are commonly prescribed to people with depression in order to improve their symptoms more quickly, mitigate concomitant anxiety, and improve antidepressant treatment continuation (Bushnell et al., 2017). In our study, we observed that while the relationship between anxiety exposures and risk of dementia was substantially attenuated by depressive symptoms, anxiety exposures did not change the statistical association between depressive symptomatology and risk of dementia which remained significant. Our findings do not allow to conclude on the nature of the relationship between anxiety exposures and depression, but suggest that, whatever the nature of the link between those two entities, it is the underlying depression that drives the association between anxiety exposures and dementia. In addition, concomitant anxiety and depression do not increase the dementia risk estimated in the presence of depression alone. Taken together, those findings designate depression as the neuropsychiatric symptom to focus on in the prevention of dementia risk.
The design of the present study constitutes its main strength. Indeed, the large cohort, as well as the length of the follow-up period, provide sufficient power to estimate precisely the magnitude of the effect of anxiety trait and depression on dementia (all causes confounded) risk. The validated dementia diagnosis by an independent committee limits classification bias, while the large number of documented potential confounders, as well as the adjustment for use of anxiolytic drugs, reduce those of confounding. Limitations of our study should also be considered. Participants who were excluded from the analysis were more likely to have higher T-anxiety score at baseline and might have been at higher risk of dementia. This selection bias has probably led to an underestimation of the association reported between T-anxiety score and risk of dementia. Additionally, anxiety trait has been self-reported using the T-anxiety subscale of the Spielberger STAI. Even if its use in epidemiological framework has been validated (Spielberger, 1983), it does not capture the anxiety disorders and might reflect some aspects of depressive symptomatology. Thus, our findings on associations between anxiety trait and dementia risk in regard to depressive symptoms cannot be extrapolated to anxiety disorders.
Finally, we were not able to further conduct analyses by considering dementia subtypes (AD, vascular, and mixed dementias). Additional studies assessing the anxiety exposures, depression in relation to different dementia subtypes may provide a better understanding of anxiety, depressive symptoms and dementia relationships.
Conclusion
In this study carried out in a large cohort of older community dwellers, we showed how associations between anxiety trait and dementia are shaped by depressive symptoms and possibly reflect the high level of comorbidity between anxiety trait and depressive symptoms. Further research is needed to replicate our findings and extrapolate our results to anxiety disorders.
Author Contributions
MM and TA: Analyzed the data and drafted the manuscript. MA: Contributed to the data analysis. AG, CB, CT, and VB: Conceived and designed the experiments.
Funding
The 3C Study is conducted under a partnership agreement between the Institut National de la Santé et de la Recherche Medicale (INSERM), Victor-Segalen Bordeaux-2 University, and Sanofi-Aventis. The Fondation pour la Recherche Médicale supported the preparation and initiation of the study. The 3C Study was also supported by the Caisse Nationale Maladie des Travailleurs Salaries; Direction Générale de la Santé; MGEN; the Institut de la Longevité; Agence Nationale de la Recherche ANR PNRA 2006 (06-01-01) and Longvie 2007 (LVIE-003-01); Agence Française de Sécurité Sanitaire des Produits de Santé; the Regional Governments of Aquitaine, Bourgogne, and Languedoc-Roussillon; the Fondation de France; the Ministry of Research-INSERM Programme Cohorts and collection of biological material; and Novartis. The funders had no role in the design and conduct of the study, collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2018.00248/full#supplementary-material
References
3C Study Group (2003). Vascular factors and risk of dementia: design of the Three-City Study and baseline characteristics of the study population. Neuroepidemiology 22, 316–325. doi: 10.1159/000072920
Akbaraly, T., Portet, F., Fustinoni, S., Dartigues, J.-F., Artero, S., Rouaud, O., et al. (2009). Leisure activities and the risk of dementia in the elderly: results from the Three-City Study. Neurology 73, 854–861. doi: 10.1212/WNL.0b013e3181b7849b
American Psychiatry Association (2000). Diagnostic and Statistical Manual of Mental Disorders, 4th Edn. Washington, DC: American Psychiatric Association.
Ausén, B., Edman, G., Almkvist, O., and Bogdanovic, N. (2009). Personality features in subjective cognitive impairment and mild cognitive impairment–early indicators of dementia? Dement. Geriatr. Cogn. Disord. 28, 528–535. doi: 10.1159/000255104
Beekman, A. T., Bremmer, M. A., Deeg, D. J., van Balkom, A. J., Smit, J. H., de Beurs, E., et al. (1998). Anxiety disorders in later life: a report from the Longitudinal Aging Study Amsterdam. Int. J. Geriatr. Psychiatr. 13, 717–726. doi: 10.1002/(SICI)1099-1166(1998100)13:10<717::AID-GPS857>3.0.CO;2-M
Beekman, A. T., de Beurs, E., van Balkom, A. J., Deeg, D. J., van Dyck, R., and van Tilburg, W. (2000). Anxiety and depression in later life: co-occurrence and communality of risk factors. Am. J. Psychiatr. 157, 89–95. doi: 10.1176/ajp.157.1.89
Bergua, V., Meillon, C., Potvin, O., Bouisson, J., Le Goff, M., Rouaud, O., et al. (2012). The STAI-Y trait scale: psychometric properties and normative data from a large population-based study of elderly people. Int. Psychogeriatr. 24, 1163–1171. doi: 10.1017/S1041610212000300
Bushnell, G. A., Stürmer, T., Gaynes, B. N., Pate, V., and Miller, M. (2017). Simultaneous antidepressant and benzodiazepine new use and subsequent long-term benzodiazepine use in adults with depression, United States, 2001-2014. JAMA Psychiatry 74, 747–755. doi: 10.1001/jamapsychiatry.2017.1273
Devier, D. J., Pelton, G. H., Tabert, M. H., Liu, X., Cuasay, K., Eisenstadt, R., et al. (2009). The impact of anxiety on conversion from mild cognitive impairment to Alzheimer's disease. Int. J. Geriatr. Psychiatry 24, 1335–1342. doi: 10.1002/gps.2263
Gallacher, J., Bayer, A., Fish, M., Pickering, J., Pedro, S., Dunstan, F., et al. (2009). Does anxiety affect risk of dementia? Findings from the caerphilly prospective study. Psychosom. Med. 71, 659–666. doi: 10.1097/PSY.0b013e3181a6177c
Geda, Y. E., Roberts, R. O., Knopman, D. S., Petersen, R. C., Christianson, T. J. H., Pankratz, V. S., et al. (2008). Prevalence of neuropsychiatric symptoms in mild cognitive impairment and normal cognitive aging: population-based study. Arch. Gen. Psychiatry 65, 1193–1198. doi: 10.1001/archpsyc.65.10.1193
Grant, B. F., Goldstein, R. B., Chou, S. P., Huang, B., Stinson, F. S., Dawson, D. A., et al. (2009). Sociodemographic and psychopathologic predictors of first incidence of DSM-IV substance use, mood and anxiety disorders: results from the Wave 2 National Epidemiologic Survey on Alcohol and Related Conditions. Mol. Psychiatry 14, 1051–1066. doi: 10.1038/mp.2008.41
Haute Autorité de Santé (2014). Rapport d'Évaluation. Outil d'Aide au Repérage Précoce et Intervention Brève: Alcool, Cannabis, Tabac chez l'Adulte.
Heser, K., Tebarth, F., Wiese, B., Eisele, M., Bickel, H., Köhler, M., et al. (2013). Age of major depression onset, depressive symptoms, and risk for subsequent dementia: results of the German study on Ageing, Cognition, and Dementia in Primary Care Patients (AgeCoDe). Psychol. Med. 43, 1597–1610. doi: 10.1017/S0033291712002449
Jorm, A. F. (2000). Is depression a risk factor for dementia or cognitive decline? A review. Gerontology 46, 219–227. doi: 10.1159/000022163
Kassem, A. M., Ganguli, M., Yaffe, K., Hanlon, J. T., Lopez, O. L., Wilson, J. W., et al. (2017). Anxiety symptoms and risk of dementia and mild cognitive impairment in the oldest old women. Aging Ment. Health 22, 474–482. doi: 10.1080/13607863.2016.1274370
Kessler, R. C., Birnbaum, H. G., Shahly, V., Bromet, E., Hwang, I., McLaughlin, K. A., et al. (2010). Age differences in the prevalence and co-morbidity of DSM-IV major depressive episodes: results from the WHO World Mental Health Survey Initiative. Depress. Anxiety 27, 351–364. doi: 10.1002/da.20634
Lamarca, R., Alonso, J., Gómez, G., and Muñoz, A. (1998). Left-truncated data with age as time scale: an alternative for survival analysis in the elderly population. J. Gerontol. A Biol. Sci. Med. Sci. 53, M337–M343. doi: 10.1093/gerona/53A.5.M337
Lawton, M. P., and Brody, E. M. (1969). Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 9, 179–186. doi: 10.1093/geront/9.3_Part_1.179
Livingston, G., Sommerlad, A., Orgeta, V., Costafreda, S. G., Huntley, J., Ames, D., et al. (2017). Dementia prevention, intervention, and care. Lancet Lond. Engl. 390, 2673–2734. doi: 10.1016/S0140-6736(17)31363-6
Lyketsos, C. G., Lopez, O., Jones, B., Fitzpatrick, A. L., Breitner, J., and DeKosky, S. (2002). Prevalence of neuropsychiatric symptoms in dementia and mild cognitive impairment: results from the cardiovascular health study. JAMA 288, 1475–1483. doi: 10.1001/jama.288.12.1475
MacKinnon, D. P., and Dwyer, J. H. (1993). Estimating mediated effects in prevention studies. Eval. Rev. 17, 144–158. doi: 10.1177/0193841X9301700202
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., and Stadlan, E. M. (1984). Clinical diagnosis of Alzheimer's disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology 34, 939–944.
Palmer, K., Berger, A. K., Monastero, R., Winblad, B., Bäckman, L., and Fratiglioni, L. (2007). Predictors of progression from mild cognitive impairment to Alzheimer disease. Neurology 68, 1596–1602. doi: 10.1212/01.wnl.0000260968.92345.3f
Potvin, O., Bergua, V., Swendsen, J., Meillon, C., Tzourio, C., Ritchie, K., et al. (2013). Anxiety and 10-year risk of incident and recurrent depressive symptomatology in older adults. Depress. Anxiety 30, 554–563. doi: 10.1002/da.22101
Radloff, L. S. (1977). The CES-D Scale: a self-report depression scale for research in the general population. Appl. Phychol. Meas. 1, 385–401.
Ramakers, I. H., Visser, P. J., Aalten, P., Kester, A., Jolles, J., and Verhey, F. R. (2010). Affective symptoms as predictors of Alzheimer's disease in subjects with mild cognitive impairment: a 10-year follow-up study. Psychol. Med. 40, 1193–1201. doi: 10.1017/S0033291709991577
Regier, D. A., Boyd, J. H., Burke, J. D., Rae, D. S., Myers, J. K., Kramer, M., et al. (1988). One-month prevalence of mental disorders in the United States. Based on five Epidemiologic Catchment Area sites. Arch. Gen. Psychiatry 45, 977–986. doi: 10.1001/archpsyc.1988.01800350011002
Román, G. C., Tatemichi, T. K., Erkinjuntti, T., Cummings, J. L., Masdeu, J. C., Garcia, J. H., et al. (1993). Vascular dementia: diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop. Neurology 43, 250–260. doi: 10.1212/WNL.43.2.250
Rosenberg, P. B., Mielke, M. M., Appleby, B., Oh, E., Leoutsakos, J.-M., and Lyketsos, C. G. (2011). Neuropsychiatric symptoms in MCI subtypes: the importance of executive dysfunction. Int. J. Geriatr. Psychiatry 26, 364–372. doi: 10.1002/gps.2535
Rosenberg, P. B., Mielke, M. M., Appleby, B. S., Oh, E. S., Geda, Y. E., and Lyketsos, C. G. (2013). The association of neuropsychiatric symptoms in MCI with incident dementia and Alzheimer disease. Am. J. Geriatr. Psychiatry 21, 685–695. doi: 10.1016/j.jagp.2013.01.006
Roy, M. A., Neale, M. C., Pedersen, N. L., Mathé, A. A., and Kendler, K. S. (1995). A twin study of generalized anxiety disorder and major depression. Psychol. Med. 25, 1037–1049. doi: 10.1017/S0033291700037533
Schoevers, R. A., Beekman, A. T. F., Deeg, D. J. H., Jonker, C., and van Tilburg, W. (2003). Comorbidity and risk-patterns of depression, generalised anxiety disorder and mixed anxiety-depression in later life: results from the AMSTEL study. Int. J. Geriatr. Psychiatry 18, 994–1001. doi: 10.1002/gps.1001
Singh-Manoux, A., Dugravot, A., Fournier, A., Abell, J., Ebmeier, K., Kivimäki, M., et al. (2017). Trajectories of depressive symptoms before diagnosis of dementia: a 28-year follow-up study. JAMA Psychiatry 74, 712–718. doi: 10.1001/jamapsychiatry.2017.0660
Spielberger, C. D. (1983). Manual for the State-Trait Anxiety Inventory (Form Y). Palo Alto, CA: Consulting Psychologist Press.
Steinberg, M., Shao, H., Zandi, P., Lyketsos, C. G., Welsh-Bohmer, K. A., Norton, M. C., et al. (2008). Point and 5-year period prevalence of neuropsychiatric symptoms in dementia: the Cache County Study. Int. J. Geriatr. Psychiatry 23, 170–177. doi: 10.1002/gps.1858
Teng, E., Lu, P. H., and Cummings, J. L. (2007). Neuropsychiatric symptoms are associated with progression from mild cognitive impairment to Alzheimer's disease. Dement. Geriatr. Cogn. Disord. 24, 253–259. doi: 10.1159/000107100
Wilson, R. S., Barnes, L. L., Bennett, D. A., Li, Y., Bienias, J. L., Mendes de Leon, C. F., et al. (2005). Proneness to psychological distress and risk of Alzheimer disease in a biracial community. Neurology 64, 380–382. doi: 10.1212/01.WNL.0000149525.53525.E7
Wilson, R. S., Begeny, C. T., Boyle, P. A., Schneider, J. A., and Bennett, D. A. (2011). Vulnerability to stress, anxiety, and development of dementia in old age. Am. J. Geriatr. Psychiatry 19, 327–334. doi: 10.1097/JGP.0b013e31820119da
Wilson, R. S., Bienias, J. L., Mendes de Leon, C. F., Evans, D. A., and Bennett, D. A. (2003). Negative affect and mortality in older persons. Am. J. Epidemiol. 158, 827–835. doi: 10.1093/aje/kwg224
Keywords: anxiety, Spielberger State-Trait Anxiety Inventory, depressive symptoms, aging, dementia, risk factors, prospective cohort
Citation: Mortamais M, Abdennour M, Bergua V, Tzourio C, Berr C, Gabelle A and Akbaraly TN (2018) Anxiety and 10-Year Risk of Incident Dementia—An Association Shaped by Depressive Symptoms: Results of the Prospective Three-City Study. Front. Neurosci. 12:248. doi: 10.3389/fnins.2018.00248
Received: 18 January 2018; Accepted: 29 March 2018;
Published: 17 April 2018.
Edited by:
Hamid R. Sohrabi, Macquarie University, AustraliaReviewed by:
Domenico De Berardis, Azienda Usl Teramo, ItalyMatt Merema, Government of Western Australia, Department of Health, Australia
Copyright © 2018 Mortamais, Abdennour, Bergua, Tzourio, Berr, Gabelle and Akbaraly. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marion Mortamais, marion.mortamais@inserm.fr