Biologically-Based Complementary and Alternative Medicine (CAM) Use in Cancer Patients: The Good, the Bad, the Misunderstood
 Kathryn Knecht
Kathryn Knecht David Kinder2
David Kinder2  Amy Stockert
Amy Stockert- 1Loma Linda University School of Pharmacy, Loma Linda University, Loma Linda, CA, United States
- 2Department of Pharmaceutical and Biomedical Sciences, Raabe College of Pharmacy, Ohio Northern University, Ada, OH, United States
As complementary and alternative medicine (CAM) becomes more popular, it is being used in cancer patients to aid in recovery or to treat symptoms associated with the current chemotherapy. Numerous papers exist that discuss patients using CAM with cancer chemotherapy and their outcomes—both positive and negative. However, in the case of the negative outcomes, the reason for the dangers or interactions with drugs are not made clear. Indeed, many chemotherapy regimens are rendered less effective by the well-meaning but uninformed patient or their family members and friends. Similarly, reports of positive outcomes with CAM and chemotherapy provide a strong basis for further research, but do not identify specific mechanisms of action. These small clinical studies and in vitro studies identify a necessary area for further research and provide a much needed, although often rejected, alternative look at whole treatment plans. Careful review of the available information and evaluation of the nature of the CAM effects are necessary to combat the misunderstanding and sometimes unwarranted claims over CAM use. This mini review will explore some of the commonly used CAM agents and their mechanisms of interactions with other treatments. Suggestions as to which agents can be safe and when to use them will be an integral part of this review.
Introduction
The use of Complementary and Alternative Medicine (CAM) is prevalent in the United States. Results of the 2012 National Health Institutes Survey show that 33.2% of adults in the US reported use of CAM therapies (1) with non-vitamin, non-mineral supplements as the most common modality (17.7%). Most use of CAM is complementary (2), meaning that patients add CAM to conventional therapies (2). Among cancer patients, CAM is also used with some variation due to cancer type and other factors; Davis et al. (3) summarized studies showing CAM use between 11 and 95% among cancer patients, though most studies estimate one third to one half (4–10).
CAM Awareness
Knowledge accessibility has increased in recent years as has the patient's desire to participate in their health care. This desire is amplified for the cancer patient, who is faced with potentially life threatening news. The desire to try everything, and take a chance on what might work is overwhelmingly tempting even for patients with a significant medical background. One study found that the most prevalent reason for CAM use was “just trying to do everything that can help” (11, 12). Internet and social media provides an opportunity for patients to gain information and form opinions which guide their treatment decisions (13). Although many reputable resources exist, it is difficult for patient's to identify which sources provide peer-reviewed and scientifically sound reference. The desire to self-diagnose and self-treat grows as a result of the accessible knowledge and patient healthcare mistrust. Patients concerns over healthcare are in part born of the influence of social media. Susceptibility to medical conspiracy theories, distrust of the medical establishment, and preference for CAM are interrelated (14, 15); one of the six most common medical conspiracies is the belief that the Food and Drug Administration (FDA) is suppressing a natural cure for cancer. It is important that the media recognize their influence on healthcare decisions and inform the patients carefully.
It is also important that health care providers are aware of CAM use. Of concern is the fact that many patients, including cancer patients, do not communicate CAM use to their health care providers (3, 4, 16–18). In response to concerns of low disclosure, the National Center for Complementary and Alternative Medicine launched a “Time to Talk” campaign to encourage patient-provider communication about CAM (19). Disclosure is higher for women than for men and more likely in patients with a life-threatening illness (18). Furthermore, patients seek CAM information more from family, friends, and the internet than from health care providers (11, 20).
It may be a factor that there is in many cases a stigma placed on alternative therapies by the medical profession. A recent study evaluated healthcare providers' belief that they needed to be informed of a patient's CAM usage due to potential dangers. An overwhelming amount of the healthcare providers felt that this was essential knowledge and a patient must share it. Approximately 80% of the providers in the surveyed population cited that interactions with herbals and prescribed medications are problematic. Interestingly, only 15% of these healthcare providers were able to elaborate on the mechanism or specifics of the interaction, let alone the potential dangers (21). In some ways, this recognition of partially lacking knowledge on the part of the healthcare provider drives the CAM stigma. Recognizing their own knowledge gap only intensifies the providers' concerns, often leading to provider disregard for potential treatments. Patients recognize this disregard and opt out of reporting use of such products. These observations highlight a communication gap. Overcoming such a communication barrier with an open mind from both parties provides opportunities to evaluate the potential benefits of supplemental therapies in a safe and informed manner.
The purpose of this review is to consider not only the reports of adverse effects, both in the lab and in human populations, but also those studies demonstrating potential benefits. Evaluation of the available literature will focus on studies ranging from year 2010 to 2019 that describe the effects, both positive and negative, that address the efficacy and safety of CAM in cancer treatment. Although multiple modes of CAM exist, the focus will be on biologically-based CAM approaches, in particular dietary supplements.
Adverse Effects
Potential adverse effects of CAM, both direct and indirect due to CAM-drug interaction, are an important concern in cancer treatment, and the Society for Integrative Oncology recommends routine evaluation of a patient's supplements for possible side effects and potential interactions (20, 22).
Reporting bias (23) in general could overstate the occurrence of adverse events due to the population failing to accurately report CAM usage when no adverse effects are noted. Similarly, patients experiencing adverse effects are more likely to report and more likely to identify their response as a CAM interaction. This phenomenon could abnormally skew the data to overestimate adverse reactions. Other studies emphasize the danger of mixing CAM with prescribed medicines. Although the potential for adverse reactions most definitely exist, it is difficult to estimate the true risk given limited reporting and essentially non-existent quality control over the CAM utilized, as well as the inherent difficulty in distinguishing disease symptoms, CAM effects, and effects of cancer treatment (7).
Peer-reviewed scientific evidence does exist for many herbal/supplemental remedies. Some evidence does support the proposed adverse reactions, and are reproducibly demonstrated in in vitro lab settings or in some cases animal models. These studies suggest the potential risk is significant enough that healthcare providers need to be aware of what their patients are using for self-treatment. However, despite the risk illuminated in these studies, only a few studies in the human population with accurate reporting confirm this level of risk. The vast majority of studies completed as a meta-analysis or retroactive study fail to support the grave nature of the proposed risks. It is important to consider that if dangers can be overstated based on self-reporting bias, the apparent lack of danger suggested by these studies may also be overstated.
Possible Benefits
Biologically-based CAM (BB-CAM) approaches are used by cancer patients for a number of reasons, including cancer prevention; cancer treatment; strengthening of the immune system; improving well-being; and alleviating symptoms of either the disease or disease treatment, such as nausea, insomnia, and pain (7, 11). While numerous studies exist looking at the effects of supplements and herbals currently used as CAM on cell culture and or animal models, much less literature is available showing the long terms effects on patients using these much less on patients using them in combination with other therapies.
Prevention
Evaluation of literature suggesting the preventative effects of these therapies are endless. Although these studies provide solid and reputable scientific method to evaluate the preventative potential of CAM, the same limitation always comes into play, i.e., the lack of long term controlled human trials, exists. This leaves virtually all of the valuable information variable in the real world population and therefore makes strong and confident recommendations difficult if not impossible. Table 1 provides a number of examples of CAMs with proposed cancer prevention abilities, Many studies demonstrate tissue specific or cell specific experimentation, which although beneficial in future research decisions, does not directly apply to the general population and makes generalization difficult. On the other hand, epidemiologic studies do suggest possible benefits in larger populations from dietary approaches [e.g., vegetarian (57, 58)], but do not establish cause and effect. A focus on dietary components, such as vitamins and minerals (Table 1) does indicate that deficiencies can introduce susceptibility and suggests repletion might be beneficial.
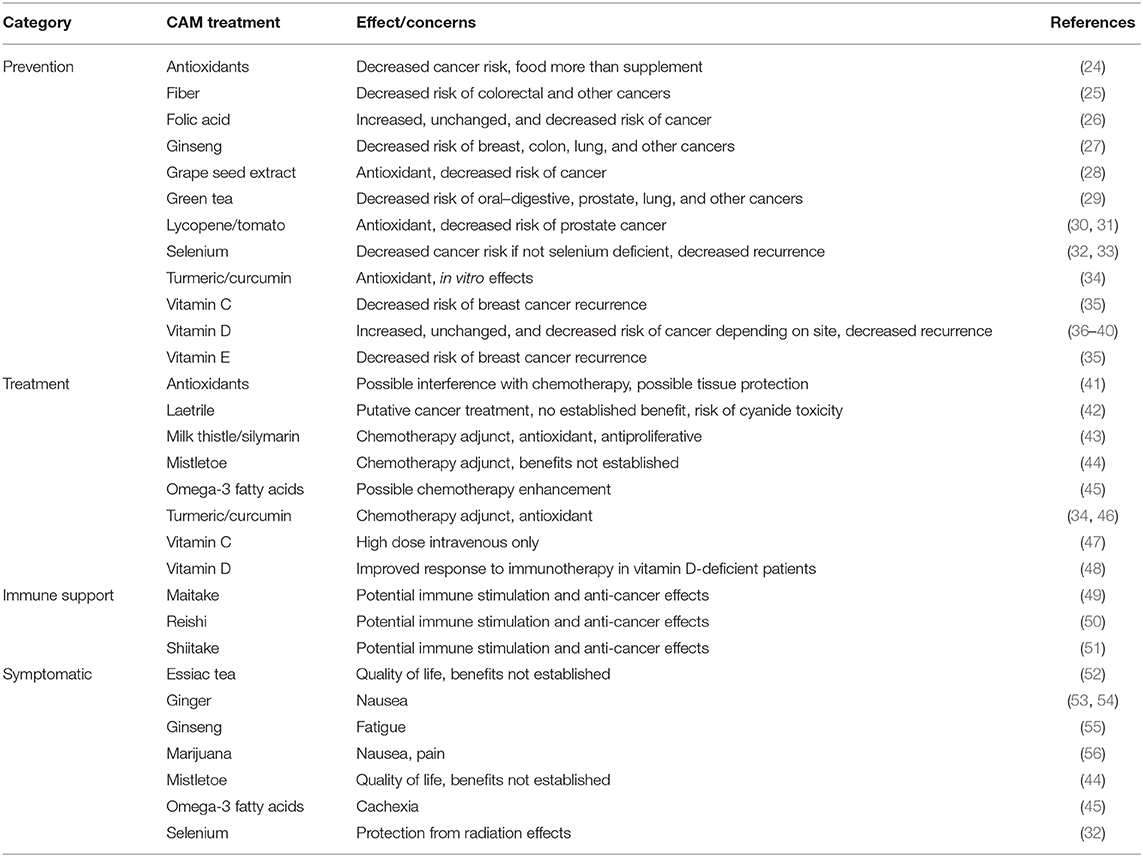
Table 1. Selected CAM approaches considered for the prevention and treatment of cancer.
Treatment
In regard to treatment, many studies have explored anti-cancer mechanisms of specific supplement products. Overall mechanisms of anti-cancer activity are often reported as effects on a single biochemical target. However, a biochemical target could alter multiple pathways in the cell. Moreover, an individual chemical component of a supplement could influence more than one biochemical target. Finally, a supplement could contain more than one biologically active component. Changes can be cell-specific or in some cases epigenetically-determined and therefore patient-specific, precluding a generalizable recommendation. Genetics can thus play a significant role in patient response and/or toxicity. Attempts to understand all of these influences targets can be never-ending, and therefore make it impossible to describe a single definitive effect to medical professionals or patients. Even the single antioxidant lycopene, for example, has been reported to affect multiple targets including cell cycle progression, matrix metalloprotein activity (MMP-9), insulin-like growth factor (IGF), apoptosis, and TNF (59). Complexity and lack of a clear mechanism can contribute to the stigma of CAM as unscientific and unproven.
Numerous non-targets, or overall general influxes on the cells signaling mechanisms indeed complicates the problem. Complexities increased yet again considering the cancer cells already has a modified signaling sequence of events. These changes can be cell specific or in some cases epigenetically movies and therefore patient specific. This, the difficulty in applying a one size fits all recommendations for CAM is virtually impossible. This review is aimed at demonstrating this impossibility and reasserting focus on safety in human population and a scene of adverse effects by opening the line of communication between HCP and patient. In reality, the patient does not always expect or require a detailed understanding. Many times, while feeling hopeless and doubtful of traditional chemotherapeutic success, a patient may be eased simply hearing that there is no evidence that alternative treatments will harm them.
It should be noted that dietary modifications are often adopted by cancer patients (60). The benefits of most dietary modifications have not been established, but there is evidence that a ketogenic diet can be helpful as an adjunct in treatment of a number of cancers with minimal adverse effects (61–63). Attention to nutrition is of course important for general patient health, since nutritional deficiencies are common in cancer patients (64). However, correction of vitamin deficiency, vitamin D in particular, could not only benefit general health (65) but could enhance treatment (48). The importance of adequate nutrition can be agreed upon by patients and even the most skeptical of practitioners and could be an area of rapprochement.
CAM-drug Interactions
A significant degree of complexity is added when considering the use of CAM as adjunct therapy. The majority of the studies showing benefit of CAM adjunctive therapy report improvements to patients' quality of life during chemotherapy rather than increased therapeutic efficacy. However, there are some studies that suggest efficacy may be increased with supplement usage. Increased survival rates for colon, gastric, and lung cancer were demonstrated with use of Pan-Asian medicine (PAM) (66–68) CAM, including supplement use, was also associated with improved quality of life (46, 69). Emotional distress, depression, insomnia, nausea, loss of appetite, and other symptoms as a result of disease or treatment can be addressed by CAM methods (see Table 1). Note that non-biologically-based CAM methods, such as meditation, deep breathing, or acupuncture can address some of these issues without risk of drug interactions and for this reason should be encouraged in CAM patients (20).
Specific Adverse Effects
A major concern is the potential for adverse effects due to supplement-drug interactions, which could be either pharmacodynamic or pharmacokinetic.
Antioxidants neutralize the free radicals that can damage DNA and other cellular targets and can therefore be seen as protective. Increased dietary antioxidant intake is inversely associated with cancer occurrence, although antioxidant supplements have not shown equally beneficial effects (24). In regard to adjunctive therapy, antioxidants could interfere with radiation or with any chemotherapy that operates via a free radical mechanism (45). In regard to lung cancer, administration of vitamin A has even been found to correlate with worsened cancer progression (70, 71). Studies of antioxidant use in general have been mixed, but it may be appropriate to suspend antioxidant therapy 48 h before and after treatment sessions (20, 72). Interestingly, omega 3 fatty acids could enhance chemotherapeutic effects by increasing the free radical formation (45).
Anticoagulation is a possible adverse effect of some dietary supplements and could be an issue in patients suffering from blood dyscrasias or undergoing surgery (31, 72). Fish oil, ginger, garlic, green tea, curcumin/turmeric, and reishi are supplements used by cancer patients that could have anticoagulative effects (11, 72, 73).
Supplements, such as milk thistle (silybin), licorice, soy, black cohosh, and curcumin could have estrogenic effects and therefore are a concern in hormone-sensitive cancers (7, 72, 74). However, evidence of adverse effects in patients has not been established.
Pharmacokinetic Concerns
Additionally, and substance that inhibits the breakdown of chemotherapeutics can increase Max concentrations of the drug and alter therapeutic intervals. Although these effects can increase drug efficacy, increased drug concentrations also lead to increased risk for toxicity. Conversely, the induction of drug metabolism can decrease drug concentrations and impair effectiveness. Effects on drug transport function similarly to effects on metabolism, altering movement of drugs into or out of the body or specific body compartments, however, many interactions are theoretical and based on in vitro rather than clinical studies (22, 72). In a cohort of 153 patients using both dietary supplements and chemotherapy, suspected drug interactions were found in 82 (54%) of patients but only one interaction was potentially clinical significant and no patient demonstrated adverse effects (22). Similarly, an analyses of 42 and 84 patients and found multiple theoretical interactions but no evidence of clinical consequences (7, 75). Nonetheless, the existence of potential interactions emphasizes the importance of good communication between patient and provider and the need for careful attention to dosing.
Conclusions and Recommendations
Biologically-based and other CAM methods are a significant factor in the prevention and treatment of cancer for many patients, yet information on the safety and efficacy of these approaches are sadly lacking. In vitro, in vivo, and preliminary clinical studies indicate promise for some products in decreasing the growth of cancer cells, the progress of cancer, and the symptoms experienced by the patients, but their usefulness has not been established. Similarly, adverse effects including pharmacokinetic interactions with drugs are suspected in a number of cases, but the clinical impact is unknown. More research is needed, but in the meantime open communication between patients and providers is important in sharing what is known, avoiding potential hazards, and providing direction for future studies.
Author Contributions
DK worked in the initial literature search and edits of the manuscript. KK added the referenced details and Table 1. AS completed the initial draft and finalized the submission.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Clarke TC, Black LI, Stussman BJ, Barnes PM, Nahin RL. Trends in the use of complementary health approaches among adults: United States, 2002–2012. Natl Health Stat Rep. (2015) 1–16.
2. National Center for Complementary and Alternative Medicine (NCCAM) What Is Complementary and Alternative Medicine? (2010). Retrieved from: http://nccam.nih.gov/health/whatiscam/ (accessed August 26, 2019).
3. Davis EL, Oh B, Butow PN, Mullan BA, Clarke S. Cancer patient disclosure and patient-doctor communication of complementary and alternative medicine use: a systematic review. Oncologist. (2012) 17:1475–81. doi: 10.1634/theoncologist.2012-0223
4. Bahall M. Prevalence, patterns, and perceived value of complementary and alternative medicine among cancer patients: a cross-sectional, descriptive study. BMC Complement Altern Med. (2017) 17:345. doi: 10.1186/s12906-017-1853-6
5. Kwon JH, Lee SC, Lee MA, Kim YJ, Kang JH, Kim JY, et al. Behaviors and attitudes toward the use of complementary and alternative medicine among Korean cancer patients. Cancer Res Treat. (2019) 51:851–60. doi: 10.4143/crt.2019.137
6. Gunes Bayir A, Guney M. Nutritional assessment and use of complementary and alternative medicine in cancer patients treated with radiotherapy and chemotherapy. Altern Ther Health Med. (2019). [Epub ahead of print].
7. Jermini M, Dubois J, Rodondi PY, Zaman K, Buclin T, Csajka C, et al. Complementary medicine use during cancer treatment and potential herb-drug interactions from a cross-sectional study in an academic centre. Sci Rep. (2019) 9:5078. doi: 10.1038/s41598-019-41532-3
8. Di Francia R, Berretta M, Benincasa G, D'Avino A, Facchini S, Costagliola D, et al. Pharmacogenetic-based interactions between nutraceuticals and angiogenesis inhibitors. Cells. (2019) 8:522. doi: 10.3390/cells8060522
9. Mwaka AD, Mangi SP, Okuku FM. Use of traditional and complementary medicines by cancer patients at a national cancer referral facility in a low-income country. Eur J Cancer Care. (2019) 28:e13158. doi: 10.1111/ecc.13158
10. Marks C, Zuniga ML. CAM practices and treatment adherence among key subpopulations of HIV plus Latinos receiving care in the San Diego-Tijuana border region: a latent class analysis. Front Public Health. (2019) 7:179. doi: 10.3389/fpubh.2019.00179
11. Buckner CA, Lafrenie RM, Dénommée JA, Caswell JM, Want DA. Complementary and alternative medicine use in patients before and after a cancer diagnosis. Curr Oncol. (2018) 25:e275–81. doi: 10.3747/co.25.3884
12. Cheng CW, Fan W, Ko SG, Song L, Bian ZX. Evidence-based management of herb-drug interaction in cancer chemotherapy. Explore. (2010) 6:324–9. doi: 10.1016/j.explore.2010.06.004
13. Holmes MM, Bishop FL, Calman L. “I just googled and read everything”: exploring breast cancer survivors' use of the internet to find information on complementary medicine. Complement Ther Med. (2017) 33:78–84. doi: 10.1016/j.ctim.2017.06.007
14. Oliver JE, Wood T. Medical conspiracy theories and health behaviors in the United States medical conspiracy theories and health behaviors letters. JAMA Intern Med. (2014) 174:817–8. doi: 10.1001/jamainternmed.2014.190
15. Lahrach Y, Furnham A. Are modern health worries associated with medical conspiracy theories? J Psychosom Res. (2017) 99:89–94. doi: 10.1016/j.jpsychores.2017.06.004
16. Shim JM, Schneider J, Curlin FA. Patterns of user disclosure of complementary and alternative medicine (CAM) use. Med Care. (2014) 52:704–8. doi: 10.1097/MLR.0000000000000165
17. Thomson P, Jones J, Evans JM, Leslie SL. Factors influencing the use of complementary and alternative medicine and whether patients inform their primary care physician. Complement Ther Med. (2012) 20:45–53. doi: 10.1016/j.ctim.2011.10.001
18. Arthur K, Belliard JC, Hardin SB, Knecht K, Chen CS, Montgomery S. Reasons to use and disclose use of complementary medicine use–an insight from cancer patients. Cancer Clin Oncol. (2013) 2:81–92. doi: 10.5539/cco.v2n2p81
19. NCCIH Health. Time to Talk About CAM: Health Care Providers and Patients Need to Ask and Tell. Bethesda: National Institutes of Health (2008).
20. Deng GE, Frenkel M, Cohen L, Cassileth BR, Abrams DI, Capodice JL, et al. Evidence-based clinical practice guidelines for integrative oncology: complementary therapies and botanicals. J Soc Integr Oncol. (2009) 7:85–120. doi: 10.3410/f.715747811.791252814
21. Pourroy B, Letellier C, Helvig A, Chanet B, De Crozals F, Alessandra C. Development of a rapid risk evaluation tool for herbs/drugs interactions in cancer patients: a multicentric experience in south of France. Eur J Cancer Care. (2017) 26:1–17. doi: 10.1111/ecc.12752
22. Drozdoff L, Klein E, Kalder M, Brambs C, Kiechle M, Paepke D. Potential interactions of biologically based complementary medicine in gynecological oncology. Integr Cancer Ther. (2019) 18:1534735419846392. doi: 10.1177/1534735419846392
23. McGauran N, Wieseler B, Kreis J, Schüler YB, Kölsch H, Kaiser T. Reporting bias in medical research–a narrative review. Trials. (2010) 11:37. doi: 10.1186/1745-6215-11-37
24. Parohan M, Anjom-Shoae J, Nasiri M, Khodadost M, Khatibi SR, Sadeghi O. Dietary total antioxidant capacity and mortality from all causes, cardiovascular disease and cancer: a systematic review and dose–response meta-analysis of prospective cohort studies. Eur J Nutr. (2019) 58:2175–89. doi: 10.1007/s00394-019-01922-9
25. Maino Vieytes CA, Taha HM, Burton-Obanla AA, Douglas KG, Arthur AE. Carbohydrate nutrition and the risk of cancer. Curr Nutr Rep. (2019) 8:230–9. doi: 10.1007/s13668-019-0264-3
26. Pieroth R, Paver S, Day S, Lammersfeld C. Folate and its impact on cancer risk. Curr Nutr Rep. (2018) 7:70–84. doi: 10.1007/s13668-018-0237-y
27. Majeed F, Malik FZ, Ahmed Z, Afreen A, Afzal MN, Khalid N. Ginseng phytochemicals as therapeutics in oncology: recent perspectives. Biomed Pharmacother. (2018) 100:52–63. doi: 10.1016/j.biopha.2018.01.155
28. Bagchi D, Swaroop A, Preuss HG, Bagchi M. Free radical scavenging, antioxidant and cancer chemoprevention by grape seed proanthocyanidin: an overview. Mutat Res. (2014) 768:69–73. doi: 10.1016/j.mrfmmm.2014.04.004
29. Yuan JM. Cancer prevention by green tea: evidence from epidemiologic studies. Am J Clin Nutr. (2013) 98:1676S−81S. doi: 10.3945/ajcn.113.058271
30. Rowles JL III, Ranard KM, Smith JW, An R, Erdman JW Jr. Increased dietary and circulating lycopene are associated with reduced prostate cancer risk: a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. (2017) 20:361. doi: 10.1038/pcan.2017.25
31. Chen P, Zhang W, Wang X, Zhao K, Negi DS, Zhuo L, et al. Lycopene and risk of prostate cancer: a systematic review and meta-analysis. Medicine (Baltimore). (2015) 94:e1260. doi: 10.1097/MD.0000000000001260
32. Puspitasari IM, Abdulah R, Yamazaki C, Kameo S, Nakano T, Koyama H. Updates on clinical studies of selenium supplementation in radiotherapy. Radiat Oncol. (2014) 9:125. doi: 10.1186/1748-717X-9-125
33. Rayman MP. Selenium and human health. Lancet. (2012) 379:1256–68. doi: 10.1016/S0140-6736(11)61452-9
34. Unlu A, Nayir E, Dogukan Kalenderoglu M, Kirca O, Ozdogan M. Curcumin (turmeric) and cancer. J BUON. (2016) 21:1050–60. Available online at: https://www.jbuon.com/archive/21-5-1050.pdf
35. Greenlee H, Kwan ML, Kushi LH, Song J, Castillo A, Weltzien E, et al. Antioxidant supplement use after breast cancer diagnosis and mortality in the Life After Cancer Epidemiology (LACE) cohort. Cancer Am Cancer Soc. (2012) 118:2048–58. doi: 10.1002/cncr.26526
36. Dimitrakopoulou VI, Tsilidis KK, Haycock PC, Dimou NL, Al-Dabhani K, Martin RM, et al. Circulating vitamin D concentration and risk of seven cancers: Mendelian randomisation study. BMJ Br Med J. (2017) 359:j4761. doi: 10.1136/bmj.j4761
37. Manson JE, Cook NR, Lee IM, Christen W, Bassuk SS, Mora S, et al. Vitamin D supplements and prevention of cancer and cardiovascular disease. N Engl J Med. (2019) 380:33–44. doi: 10.1056/NEJMoa1809944
38. Mondul AM, Weinstein SJ, Layne TM, Albanes D. Vitamin D and cancer risk and mortality: state of the science, gaps, and challenges. Epidemiol Rev. (2017) 39:28–48. doi: 10.1093/epirev/mxx005
39. Churilla TM, Brereton HD, Klem M, Peters CA. Vitamin D deficiency is widespread in cancer patients and correlates with advanced stage disease: a community oncology experience. Nutr Cancer Int J. (2012) 64:521–5. doi: 10.1080/01635581.2012.661515
40. Ince B, Yildirim MEC, Dadaci M. Assessing the effect of vitamin D replacement on basal cell carcinoma occurrence and recurrence rates in patients with vitamin D deficiency. Horm Cancer. (2019) 10:145–9. doi: 10.1007/s12672-019-00365-2
41. Singh K, Bhori M, Kasu YA, Bhat G, Marar T. Antioxidants as precision weapons in war against cancer chemotherapy induced toxicity–exploring the armoury of obscurity. Saudi Pharm J. (2018) 26:177–90. doi: 10.1016/j.jsps.2017.12.013
42. Milazzo S, Horneber M. Laetrile treatment for cancer. Cochrane Database Syst Rev. (2015) 2015:CD005476. doi: 10.1002/14651858.CD005476.pub4
43. Hosseinabadi T, Lorigooini Z, Tabarzad M, Salehi B, Rodrigues CF, Martins N, et al. Silymarin antiproliferative and apoptotic effects: insights into its clinical impact in various types of cancer. Phytother Res. (2019) 33:2849–61. doi: 10.1002/ptr.6470
44. Freuding M, Keinki C, Kutschan S, Micke O, Buentzel J, Huebner J. Mistletoe in oncological treatment: a systematic review. J Cancer Res Clin Oncol. (2019) 145:927–39. doi: 10.1007/s00432-018-02838-3
45. Harvie M. Nutritional supplements and cancer: potential benefits and proven harms. Am Soc Clin Oncol Educ Book. (2014) 34:e478–86. doi: 10.14694/EdBook_AM.2014.34.e478
46. Lin WF, Zhong MF, Zhou QH, Zhang YR, Wang H, Zhao ZH, et al. Efficacy of complementary and integrative medicine on health-related quality of life in cancer patients: a systematic review and meta-analysis. Cancer Manag Res. (2019) 11:6663–80. doi: 10.2147/CMAR.S195935
47. El Halabi I, Bejjany R, Nasr R, Mukherji D, Temraz S, Nassar FJ, et al. Ascorbic acid in colon cancer: from the basic to the clinical applications. Int J Mol Sci. (2018) 19:2752. doi: 10.3390/ijms19092752
48. Hohaus S, Tisi MC, Bellesi S, Maiolo E, Alma E, Tartaglia G, et al. Vitamin D deficiency and supplementation in patients with aggressive B-cell lymphomas treated with immunochemotherapy. Cancer Med. (2018) 7:270–81. doi: 10.1002/cam4.1166
49. Rossi P, Difrancia R, Quagliariello V, Savino E, Tralongo P, Randazzo CL, et al. B-glucans from Grifola frondosa and Ganoderma lucidum in breast cancer: an example of complementary and integrative medicine. Oncotarget. (2018) 9:24837–56. doi: 10.18632/oncotarget.24984
50. Jin X, Ruiz Beguerie J, Sze DMY, Chan GCF. Ganoderma lucidum (Reishi mushroom) for cancer treatment. Cochrane Database Syst Rev. (2016) 4:CD007731. doi: 10.1002/14651858.CD007731.pub3
51. Zhang M, Zhang Y, Zhang L, Tian Q. Chapter thirteen: mushroom polysaccharide lentinan for treating different types of cancers: a review of 12 years clinical studies in China. In: Zhang L, editor. Progress in Molecular Biology and Translational Science. Cambridge: Academic Press (2019). p. 297–328. doi: 10.1016/bs.pmbts.2019.02.013
52. Ulbricht C, Weissner W, Hashmi S, Rae Abrams T, Dacey C, Giese N, et al. Essiac: systematic review by the natural standard research collaboration. J Soc Integr Oncol. (2009) 7:73–80.
53. Marx WM, Teleni L, McCarthy AL, Vitetta L, McKavanagh D, Thomson D, et al. Ginger (Zingiber officinale) and chemotherapy-induced nausea and vomiting: a systematic literature review. Nutr Rev. (2013) 71:245–54. doi: 10.1111/nure.12016
54. Giacosa A, Morazzoni P, Bombardelli E, Riva A, Bianchi Porro G, Rondanelli M. Can nausea and vomiting be treated with ginger extract? Eur Rev Med Pharmacol Sci. (2015) 19:1291–6. doi: 10.1155/2015/915087
55. Yennurajalingam S, Tannir NM, Williams JL, Lu Z, Hess KR, Frisbee-Hume S, et al. A double-blind, randomized, placebo-controlled trial of panax ginseng for cancer-related fatigue in patients with advanced cancer. J Natl Compr Canc Netw. (2017) 15:1111–20. doi: 10.6004/jnccn.2017.0149
56. Kleckner AS, Kleckner IR, Kamen CS, Tejani MA, Janelsins MC, Morrow GR, et al. Opportunities for cannabis in supportive care in cancer. Ther Adv Med Oncol. (2019) 11:1758835919866362. doi: 10.1177/1758835919866362
57. Key TJ, Appleby PN, Crowe FL, Bradbury KE, Schmidt JA, Travis RC. Cancer in British vegetarians: updated analyses of 4998 incident cancers in a cohort of 32,491 meat eaters, 8612 fish eaters, 18,298 vegetarians, and 2246 vegans. Am J Clin Nutr. (2014) 100:378s−85s. doi: 10.3945/ajcn.113.071266
58. Le LT, Sabate J. Beyond meatless, the health effects of vegan diets: findings from the adventist cohorts. Nutrients. (2014) 6:2131–47. doi: 10.3390/nu6062131
59. Chaudhary P, Sharma A, Singh B, Nagpal AK. Bioactivities of phytochemicals present in tomato. J Food Sci Technol. (2018) 55:2833–49. doi: 10.1007/s13197-018-3221-z
60. Maria S, Snyder D, Abrams DI. Pros, cons of dietary strategies popular among cancer patients. Oncology. (2018) 32:542–7. Available online at: https://www.cancernetwork.com/dietary-strategies-cancer
61. Weber DD, Aminzadeh-Gohari S, Tulipan J, Catalano L, Feichtinger RG, Kofler B. Ketogenic diet in the treatment of cancer–where do we stand? Mol Metab. (forthcoming). doi: 10.1016/j.molmet.2019.06.026
62. Winter SF, Loebel F, Dietrich J. Role of ketogenic metabolic therapy in malignant glioma: a systematic review. Crit Rev Oncol Hemat. (2017) 112:41–58. doi: 10.1016/j.critrevonc.2017.02.016
63. Cohen CW, Fontaine KR, Arend RC, Gower BA. A ketogenic diet is acceptable in women with ovarian and endometrial cancer and has no adverse effects on blood lipids: a randomized, controlled trial. Nutr Cancer. (forthcoming). doi: 10.1080/01635581.2019.1645864
64. Virizuela JA, Camblor-Alvarez M, Luengo-Perez LM, Grande E, Alvarez-Hernandez J, Sendros-Madrono MJ, et al. Nutritional support and parenteral nutrition in cancer patients: an expert consensus report. Clin Transl Oncol. (2018) 20:619–29. doi: 10.1007/s12094-017-1757-4
65. DeMille DM, Piscitelli M, Ocker A, Vuong C, Hartner L, Lynch MP. Vitamin D deficiency in the oncology setting. J Community Support Oncol. (2014) 12:13–9. doi: 10.12788/jcso.0004
66. McCulloch M, Broffman M, van der Laan M, Hubbard A, Kushi L, Abrams DI, et al. Colon cancer survival with herbal medicine and vitamins combined with standard therapy in a whole-systems approach: ten-year follow-up data analyzed with marginal structural models and propensity score methods. Integr Cancer Ther. (2011) 10:240–59. doi: 10.1177/1534735411406539
67. McCulloch M, Broffman M, van der Laan M, Hubbard A, Kushi L, Kramer A, et al. Lung cancer survival with herbal medicine and vitamins in a whole-systems approach:ten-year follow-up data analyzed with marginal structural models and propensity score methods. Integr Cancer Ther. (2011) 10:260–79. doi: 10.1177/1534735411406439
68. Hung KF, Hsu CP, Chiang JH, Lin HJ, Kuo YT, Sun MF, et al. Complementary Chinese herbal medicine therapy improves survival of patients with gastric cancer in Taiwan: a nationwide retrospective matched-cohort study. J Ethnopharmacol. (2017) 199:168–74. doi: 10.1016/j.jep.2017.02.004
69. Jang A, Kang DH, Kim DU. Complementary and alternative medicine use and its association with emotional status and quality of life in patients with a solid tumor: a cross-sectional study. J Altern Complement Med. (2017) 23:362–9. doi: 10.1089/acm.2016.0289
70. Wiel C, Le Gal K, Ibrahim MX, Jahangir CA, Kashif M, Yao H, et al. BACH1 stabilization by antioxidants stimulates lung cancer metastasis. Cell. (2019) 178:330–45.e22. doi: 10.1016/j.cell.2019.06.005
71. Lignitto L, LeBoeuf SE, Homer H, Jiang S, Askenazi M, Karakousi TR, et al. Nrf2 activation promotes lung cancer metastasis by inhibiting the degradation of Bach1. Cell. (2019) 178:316–29.e18. doi: 10.1016/j.cell.2019.06.003
72. Brooks SL, Rowan G, Michael M. Potential issues with complementary medicines commonly used in the cancer population: a retrospective review of a tertiary cancer center's experience. Asia Pac J Clin Oncol. (2018) 14:e535–42. doi: 10.1111/ajco.13026
73. Wang CZ, Moss J, Yuan CS. Commonly used dietary supplements on coagulation function during surgery. Medicines (Basel). (2015) 2:157–85. doi: 10.3390/medicines2030157
74. Fritz H, Seely D, McGowan J, Skidmore B, Fernandes R, Kennedy DA, et al. Black cohosh and breast cancer:a systematic review. Integr Cancer Ther. (2014) 13:12–29. doi: 10.1177/1534735413477191
Keywords: CAM, alternative medicine, anti-cancer, herbal, supplemental therapy
Citation: Knecht K, Kinder D and Stockert A (2020) Biologically-Based Complementary and Alternative Medicine (CAM) Use in Cancer Patients: The Good, the Bad, the Misunderstood. Front. Nutr. 6:196. doi: 10.3389/fnut.2019.00196
Received: 03 September 2019; Accepted: 20 December 2019;
Published: 24 January 2020.
Edited by:
Akio Inui, Kagoshima University, JapanReviewed by:
Thomas N. Seyfried, Boston College, United StatesRalph Mücke, Independent Researcher, Bad Kreuznach, Germany
Copyright © 2020 Knecht, Kinder and Stockert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amy Stockert, a-stockert@onu.edu