Association between nut consumption and metabolic syndrome in Korean adults: results from the Korean Genome and Epidemiology Study–Health Examinees
 Hye Ran Shin
Hye Ran Shin SuJin Song
SuJin Song- Department of Food and Nutrition, Hannam University, Daejeon, Republic of Korea
Background: The epidemiological evidence regarding nut consumption and metabolic diseases focuses on Western populations. Nut consumption among Koreans is relatively low, and the prevalence of metabolic syndrome is rapidly increasing, highlighting the need for more focused studies in this population. This cross-sectional study aimed to investigate the relationship between nut consumption and metabolic syndrome in Korean adults.
Methods: A total of 112,501 adults (39,481 men and 73,020 women) aged 40–79 years were selected from baseline data of the Korean Genome and Epidemiology Study–Health Examinees. Nut consumption was assessed using a validated semi-quantitative food frequency questionnaire and categorized as non-consumers, <1 serving/week, ≥1 to <2 servings/week, or ≥2 servings/week (15 g per serving). Metabolic syndrome and its components were defined according to the Korean Society of CardioMetabolic Syndrome criteria. Associations between nut consumption and metabolic syndrome and its components were examined using multiple logistic regression with adjustments for potential confounders.
Results: In the study population, the prevalence of metabolic syndrome was 21.4% (26.9% in men and 18.4% in women), and the mean nut intake was 0.8 serving/week (0.7 serving/week in men and 0.8 serving/week in women). After adjusting for confounders, higher nut consumption was associated with a lower odds ratio (OR) of metabolic syndrome in individuals consuming ≥2 servings/week compared with non-consumers [OR = 0.85, 95% confidence interval (CI) = 0.80–0.91, p for trend <0.001]. Specifically, in men, this level of consumption was associated with a 14% reduction in the OR of metabolic syndrome (OR = 0.86, 95% CI = 0.77–0.95, p for trend = 0.028). In women, a similar reduction of 14% was observed (OR = 0.86, 95% CI = 0.80–0.93, p for trend <0.001). Among the metabolic syndrome components, nut consumption was inversely associated with abdominal obesity, low high-density lipoprotein-cholesterol, and elevated triglycerides in men and women, whereas no associations were observed for elevated blood pressure or elevated fasting blood glucose.
Conclusion: Our findings suggest that higher nut consumption is inversely associated with metabolic syndrome and its components in Korean adults. Further studies are needed to examine the longitudinal association between nut consumption and metabolic diseases in this population.
1 Introduction
Metabolic syndrome is defined as a combination of cardiometabolic risk factors that increase the risk of serious health problems such as cardiovascular disease (CVD) and type 2 diabetes (1, 2). The National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) diagnoses metabolic syndrome in individuals with three or more of the following components: elevated waist circumference, blood pressure, fasting blood glucose and triglycerides, and reduced high-density lipoprotein (HDL)-cholesterol (3). The development of metabolic syndrome is closely related to an unhealthy lifestyle (4).
Metabolic syndrome and its components are closely associated with dietary patterns and nutrient and food intake (5–7). To prevent metabolic diseases such as hypertension, type 2 diabetes, metabolic syndrome, and CVD, two dietary approaches, the Dietary Approaches to Stop Hypertension (DASH) and the Mediterranean dietary pattern, have been recommended (8, 9). Both of these healthy dietary patterns include nuts as one of the major food components because nuts are a good source of monounsaturated and polyunsaturated fatty acids, dietary fiber, vitamins E and K, and minerals such as magnesium, copper, potassium, selenium, carotenoids, and antioxidants (10).
Research data on nut consumption and metabolic syndrome are accumulating; however, findings on the association between nut consumption and metabolic syndrome and its components are inconsistent. A meta-analysis of prospective cohort studies revealed that an increase of 1 serving (30 g) per week of nuts decreased the risk of metabolic syndrome by 4% (11) but did not report an association between nut consumption and each metabolic syndrome component. Two additional meta-analyses of randomized controlled trials demonstrated that nut intake had favorable effects on some metabolic syndrome components, such as serum triglycerides and fasting blood glucose, whereas no effect on other metabolic syndrome components was observed (12, 13).
Furthermore, most research is concentrated in Western countries, and few studies have been conducted in Asia. Two studies on Korean adults reported inconsistent findings. A prospective cohort study reported that consuming >15 g of nuts per week was inversely associated with the incidence of metabolic syndrome in Korean adults (14), but did not examine the association of nut consumption with metabolic syndrome components. A randomized controlled trial among Korean patients with metabolic syndrome revealed that nut consumption did not improve the levels of markers of metabolic syndrome (15). Therefore, it is necessary to investigate the association of nut consumption with metabolic syndrome and its components in a larger Korean cohort sample to better understand the effect of nut consumption on metabolic syndrome in this population.
The overall age-adjusted prevalence of metabolic syndrome in Korea has increased from 27.1% in 2001 to 33.2% in 2020 (16). According to data on the causes of death from Statistics Korea, heart and cerebrovascular diseases were the second and fourth leading causes of death, respectively (17). Therefore, it is necessary to identify the dietary factors related to metabolic syndrome and incorporate them into dietary guidelines to improve cardiometabolic health in Korean adults. To fully understand the association of nut consumption with metabolic syndrome and its components, this study analyzed the association between nut consumption frequency and metabolic syndrome using a large dataset of Korean adults.
2 Materials and methods
2.1 Data and study participants
This study used baseline data from the Korean Genome and Epidemiology Study-Health Examinees (KoGES-HEXA). The KoGES-HEXA is a population-based, large-scale cohort study aimed at identifying environmental and genetic risk factors for major chronic diseases prevalent among Koreans (18). The KoGES-HEXA commenced its baseline survey in 2004 and has been conducting follow-up surveys. It focuses on city regions, centering around medical institutions, health centers, and public health clinics. The study participants were Korean men and women over 40 years who had visited medical institution screening centers in urban areas. The KoGES-HEXA collected data on sociodemographic and medical history, lifestyle, anthropometric measures and biochemical variables, and dietary variables (19).
The baseline data of the KoGES-HEXA recruited 173,195 men and women aged 40–79 years from urban medical institutions across South Korea between 2004 and 2013. From this group, 3,064 individuals who did not complete the food frequency questionnaire (FFQ) were excluded. Additionally, 834 participants whose daily energy intake calculated from the FFQ was <500 kcal or >5,000 kcal were excluded (20–22). Subsequently, 35,769 individuals who did not provide data on variables relevant to the study were excluded (2,562 for physical measurements; 26,105 for education, occupation, and household income; 555 for smoking, alcohol consumption, and physical activity; and 6,547 for biochemical measurements). Finally, 147 individuals who did not respond to questions about the diagnoses of hypertension, diabetes, and hyperlipidemia and 20,880 individuals who did not respond to questions about medication use for these conditions (hypertension, diabetes, or dyslipidemia) were also excluded. Finally, the data of 112,501 participants (39,481 men and 73,020 women) were analyzed. All study participants provided written informed consent. This study qualified for an exemption issued by the Institutional Review Board of Hannam University (2023-E-01-09-0625).
2.2 Assessment of nut consumption and nutrient intake
Dietary data collected using the validated semi-quantitative FFQ were used to assess nut consumption (23). The FFQ asked participants how often they had consumed nuts, including peanuts, almonds, and pine nuts, in the past year. The responses to this question comprised nine consumption frequency options (rarely, 1 time/month, 2–3 times/month, 1–2 times/week, 3–4 times/week, 5–6 times/week, 1 time/day, 2 times/day, and 3 times/day) and three average serving sizes per consumption (0.5, 1, and 1.5 servings). This study converted the responses into a weekly consumption frequency of nuts based on one serving (15 g) for each participant and categorized nut consumption frequency into non-consumers, <1 serving/week, 1–2 servings/week, and ≥2 servings/week, considering the distribution of participants in each category of consumption frequency.
Energy and nutrient intakes were evaluated using dietary data obtained from the FFQ. The percentage of energy from each nutrient was calculated for carbohydrate, protein, and fat intake. Vitamin and mineral intakes were evaluated as nutrient intake per 1,000 kcal/day to assess the quality of nutrient intake.
2.3 Definition of metabolic syndrome and its components
The anthropometric measurements used in this study included height, weight, body mass index (BMI), waist circumference, systolic blood pressure (SBP), and diastolic blood pressure (DBP). Height and weight were measured using an automatic height-weight measuring device in centimeters (cm) and kilograms (kg), respectively. BMI was calculated as measured weight divided by the square of measured height in meters (kg/m2). Waist circumference was measured in centimeters using a measuring tape. The SBP and DBP were measured twice at the arm at a minimum interval of 1 min, and the average of the two measurements was used. Biochemical tests were conducted according to the standardized protocols of the participating medical institutions; the biochemical indicators were total cholesterol, triglycerides, HDL-cholesterol, low-density lipoprotein (LDL)-cholesterol, and fasting blood glucose. Blood tests were performed on venous blood samples collected after fasting for >8 h. Total cholesterol, triglyceride, HDL-cholesterol, and fasting blood glucose levels were measured using enzymatic methods with the ADVIA 1650 System (Siemens, Tarrytown, NY, United States). The LDL-cholesterol level was calculated using the Friedewald formula (total cholesterol − HDL-cholesterol – [triglycerides ÷ 5]).
Metabolic syndrome was defined according to the criteria set by the Korean Society of Cardio-Metabolic Syndrome. Metabolic syndrome was identified as the presence of three or more of the following conditions: abdominal obesity (waist circumference ≥ 90 cm in men and ≥85 cm in women), low HDL-cholesterol (<40 mg/dL in men and <50 mg/dL in women or medication use), elevated triglycerides (≥150 mg/dL), elevated blood pressure (SBP ≥ 130 mmHg or DBP ≥ 85 mmHg or medication use), and elevated fasting blood glucose (≥100 mg/dL or medication use) (24, 25).
2.4 Measurement of other variables
General characteristics of the participants included age, educational level, and household income. Educational level was categorized as middle school or lower, high school or lower, and college or higher. Household income was classified as <2 million Korean Won (KRW) per month, <4 million KRW per month, or ≥4 million KRW per month. The lifestyle variables included smoking status, alcohol consumption, and physical activity. Smoking status was categorized as current smoker, former smoker, or non-smoker. Alcohol consumption was categorized as current drinkers, former drinkers, and non-drinkers. Physical activity was assessed based on the response to the question, “Do you regularly perform exercise intensely enough to cause sweating?” and classified as “yes” or “no” (26, 27).
2.5 Statistical analyses
Statistical analyses were performed using SPSS software (version 25.0; IBM Corp., Armonk, NY, United States). General characteristics were presented as mean and standard error for continuous variables and as frequencies and percentages for categorical variables. Differences in general characteristics according to nut consumption frequency were evaluated using analysis of variance for continuous variables and the chi-square test for categorical variables. Differences in energy and nutrient intake, anthropometric measurements, and biochemical test results according to nut consumption frequency were assessed using multiple regression analysis after adjusting for covariates (sex, age, educational level, household income, smoking status, alcohol consumption, physical activity, BMI, and energy intake, where applicable). The associations between nut consumption frequency and metabolic syndrome and its components were analyzed using multiple logistic regression to calculate the odds ratios (ORs), 95% confidence intervals (CIs), and p-values for trend. In this analysis, the reference group was comprised of non-consumers. The potential confounding variables adjusted for were sex, age, educational level, household income, smoking status, alcohol consumption, physical activity, BMI, and energy intake. Statistical significance was set at p < 0.05.
3 Results
3.1 Distribution of nut consumption frequency
The distribution of nut consumption frequency is illustrated in Figure 1. Among all participants, 42.3% were non-consumers, 38.4% consumed <1 serving/week, 10.0% consumed 1–2 servings/week, and 9.3% consumed ≥2 servings/week. Among men, 43.5% were non-consumers, 39.5% consumed <1 serving/week, 9.7% consumed 1–2 servings/week, and 7.3% consumed ≥2 servings/week. Among women, 41.7% were non-consumers, 37.8% consumed <1 serving/week, 10.1% consumed 1–2 servings/week, and 10.4% consumed ≥2 servings/week. The mean nut intake was 0.8 serving/week among all participants (0.7 serving/week in men and 0.8 serving/week in women).
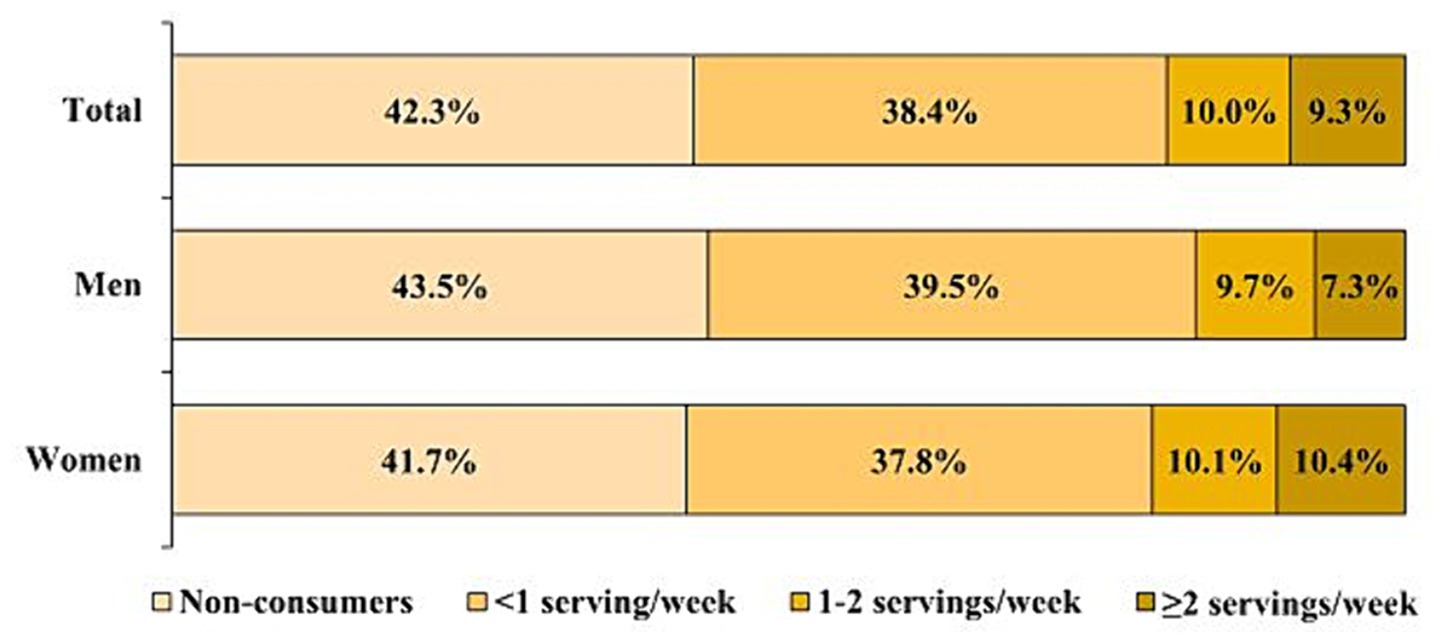
Figure 1. Percentage of subjects in each nut consumption frequency category.
3.2 Characteristics of the study participants according to nut consumption frequency
The general characteristics of the study participants according to their nut consumption frequency are presented in Table 1. The average age of participants was 53.0 years (53.8 years in men and 52.6 years in women). In both men and women, the highest nut consumption group had a higher proportion of individuals with higher levels of education and household income, non-smokers, and non-current alcohol users, and individuals who engaged in physical activity (p-values <0.001). The prevalence of metabolic syndrome in the study population was 21.4% (26.9% in men and 18.4% in women). Compared with the group of non-consumers, the prevalences of metabolic syndrome and its components were lower in the group consuming ≥2 servings/week of nuts (p-values <0.001).
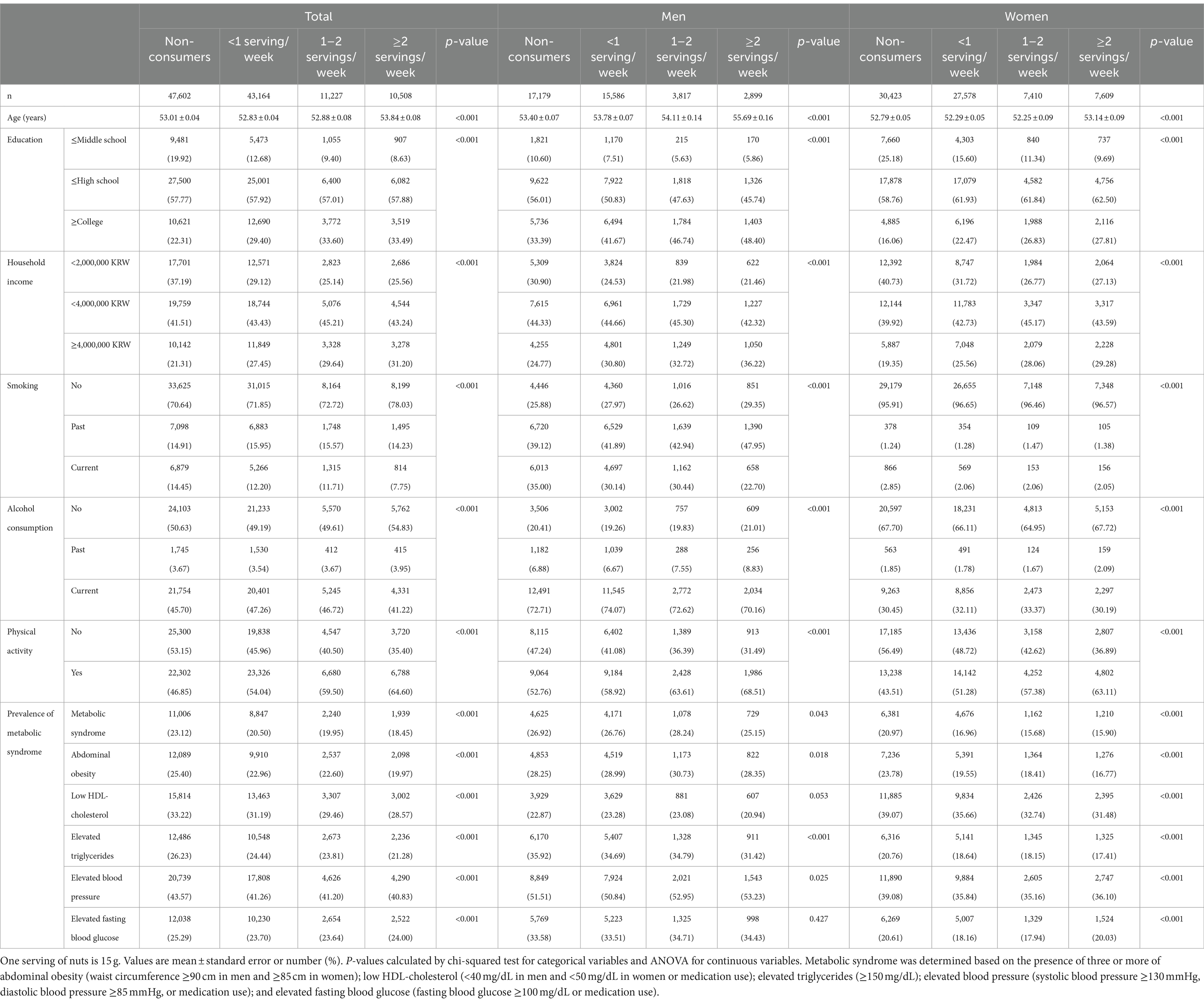
Table 1. Characteristics of the study subjects according to nut consumption frequency.
3.3 Energy and nutrient intake according to nut consumption frequency
Table 2 presents energy and nutrient intakes according to nut consumption frequency. The average daily energy intake was 1,727.0 kcal for total participants, with 1,824.3 kcal in men and 1,674.4 kcal in women. Among the total participants, men and women, total energy intake significantly increased with increasing nut consumption frequency (p for trends <0.001). In this study population, the proportions of energy intake from carbohydrate, fat, and protein were 72.2, 14.1, and 13.6%, respectively. Regarding the contribution of macronutrients to energy intake, among the total participants, men, and women, the proportion of energy derived from carbohydrate decreased with increasing nut consumption, whereas the contributions of protein and fat to energy intake showed an increasing trend (p for trend <0.001). The energy density of calcium, phosphorus, iron, sodium, potassium, vitamin A, vitamin B1, vitamin B2, niacin, vitamin C, vitamin B6, folate, dietary fiber, vitamin E, and cholesterol significantly increased with increasing nut consumption frequency among the total participants, men, and women (p for trends <0.05).
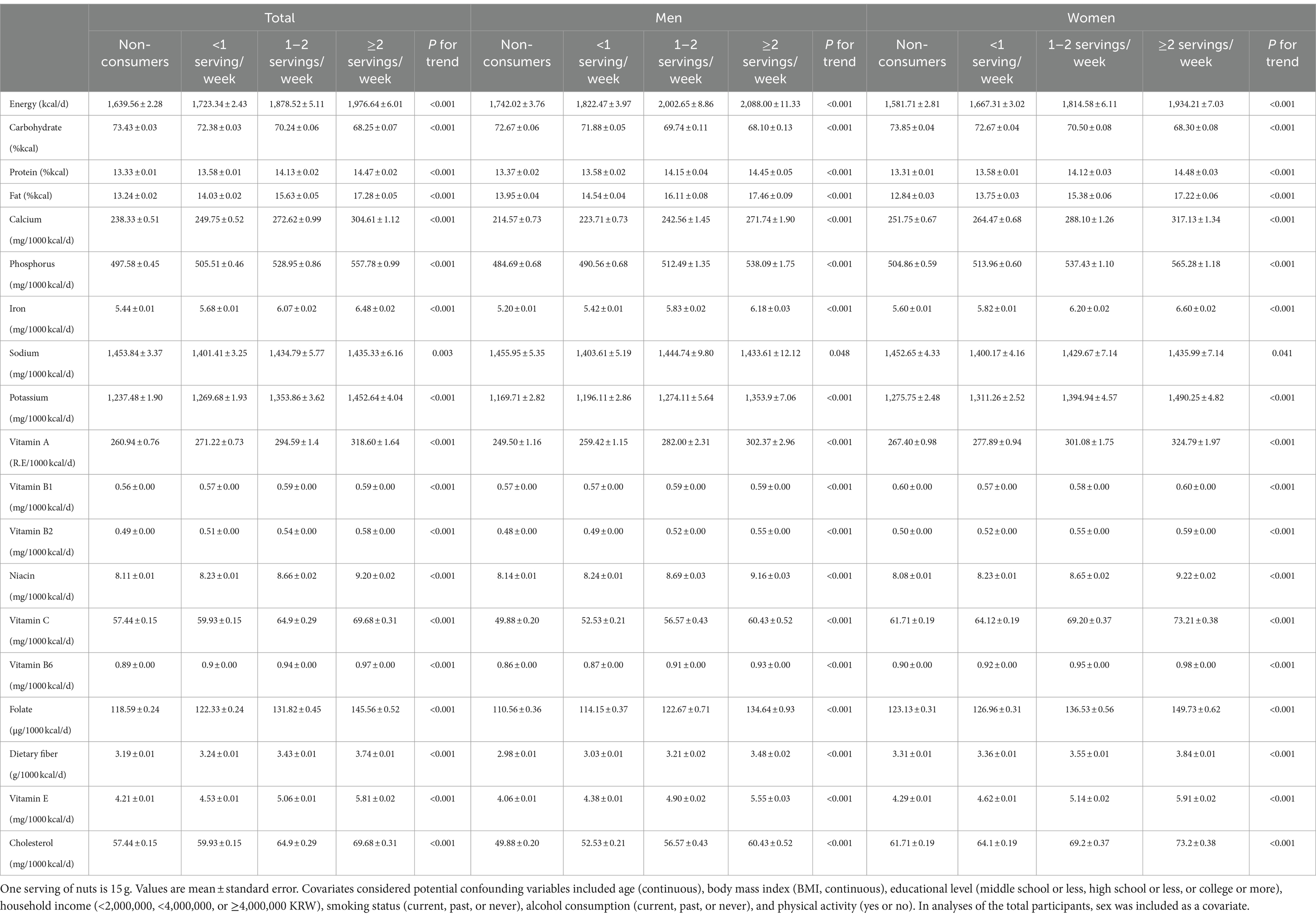
Table 2. Energy and nutrient intakes according to nut consumption frequency.
3.4 Anthropometric and biochemical variables according to nut consumption frequency
The anthropometric and biochemical variables according to nut consumption frequency are listed in Table 3. Among all participants, the highest consumption group had lower BMI, waist circumference, SBP, DBP, and triglycerides but higher levels of total cholesterol, HDL-, and LDL-cholesterol than non-consumers (p for trends <0.05). Fasting blood glucose levels were not associated with nut consumption. In men, higher nut consumption was inversely associated with waist circumference, blood pressure, and triglycerides but positively associated with levels of total cholesterol, HDL-cholesterol, and LDL-cholesterol (p for trends <0.05). Among women, individuals with a higher nut consumption frequency had a smaller waist circumference, lower BMI, DBP, and triglycerides but higher levels of total cholesterol, HDL-cholesterol, and LDL-cholesterol than non-consumers (p for trends <0.05).
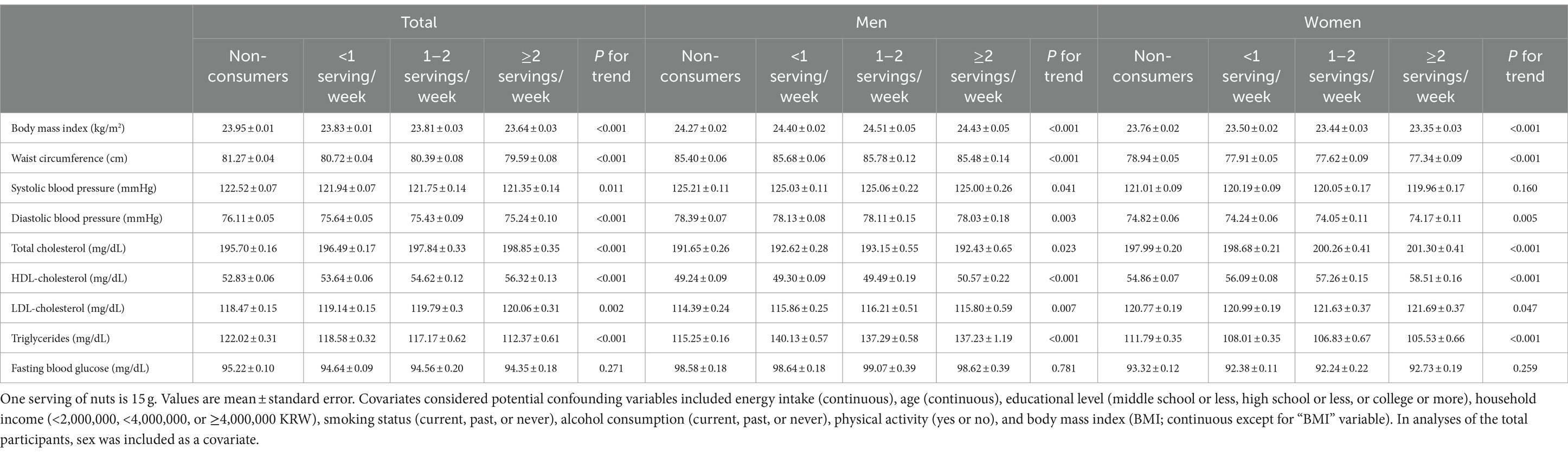
Table 3. Anthropometric and biochemical variables according to nut consumption frequency.
3.5 Association of nut consumption with metabolic syndrome and its components
Table 4 presents the association between nut consumption frequency and metabolic syndrome and its components. After adjusting for covariates, the ORs for metabolic syndrome were significantly lower in the group consuming ≥2 servings/week than the non-consumers group among the total participants (OR = 0.85, 95% CI = 0.80 to 0.91, p for trend <0.001), men (OR = 0.86, 95% CI = 0.77 to 0.95, p for trend = 0.028), and women (OR = 0.86, 95% CI = 0.80 to 0.93, p for trend <0.001). In both men and women, the group with the highest nut consumption frequency (≥2 servings/week) showed significantly lower ORs for abdominal obesity, low HDL-cholesterol, and elevated triglycerides than non-consumers. Nut consumption was not significantly associated with elevated blood pressure or fasting blood glucose. The overall concept on the role of nut intake in prevention and management of metabolic syndrome is summarized in Figure 2.
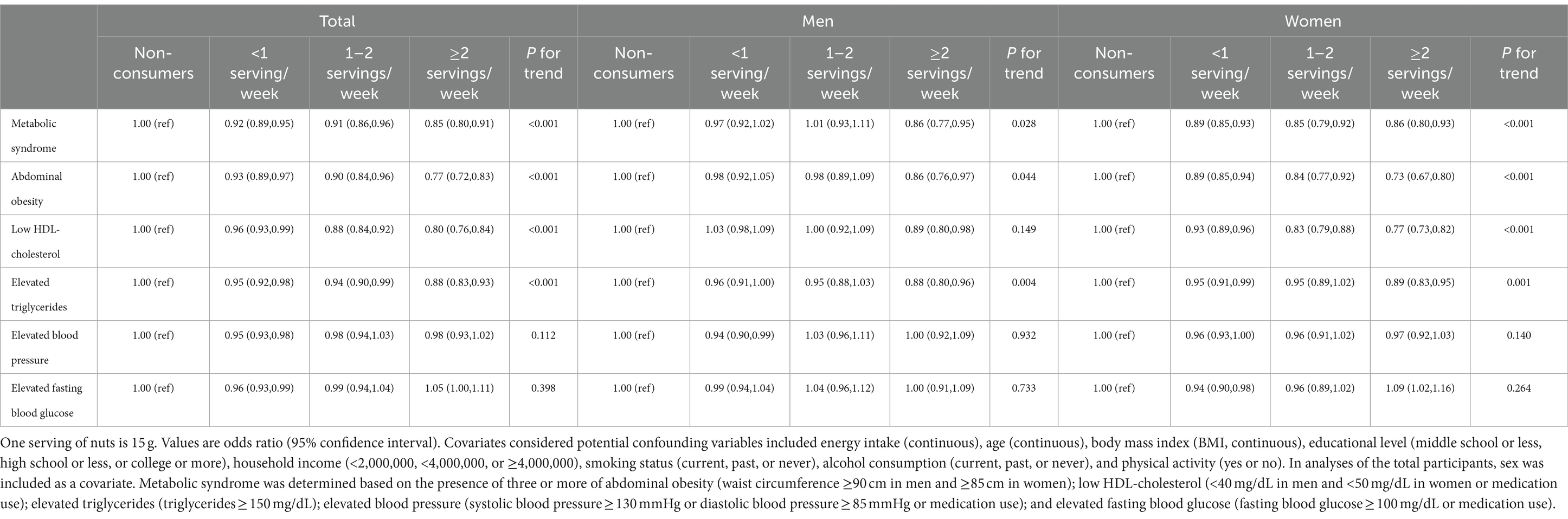
Table 4. Associations of nut consumption with metabolic syndrome and its components.
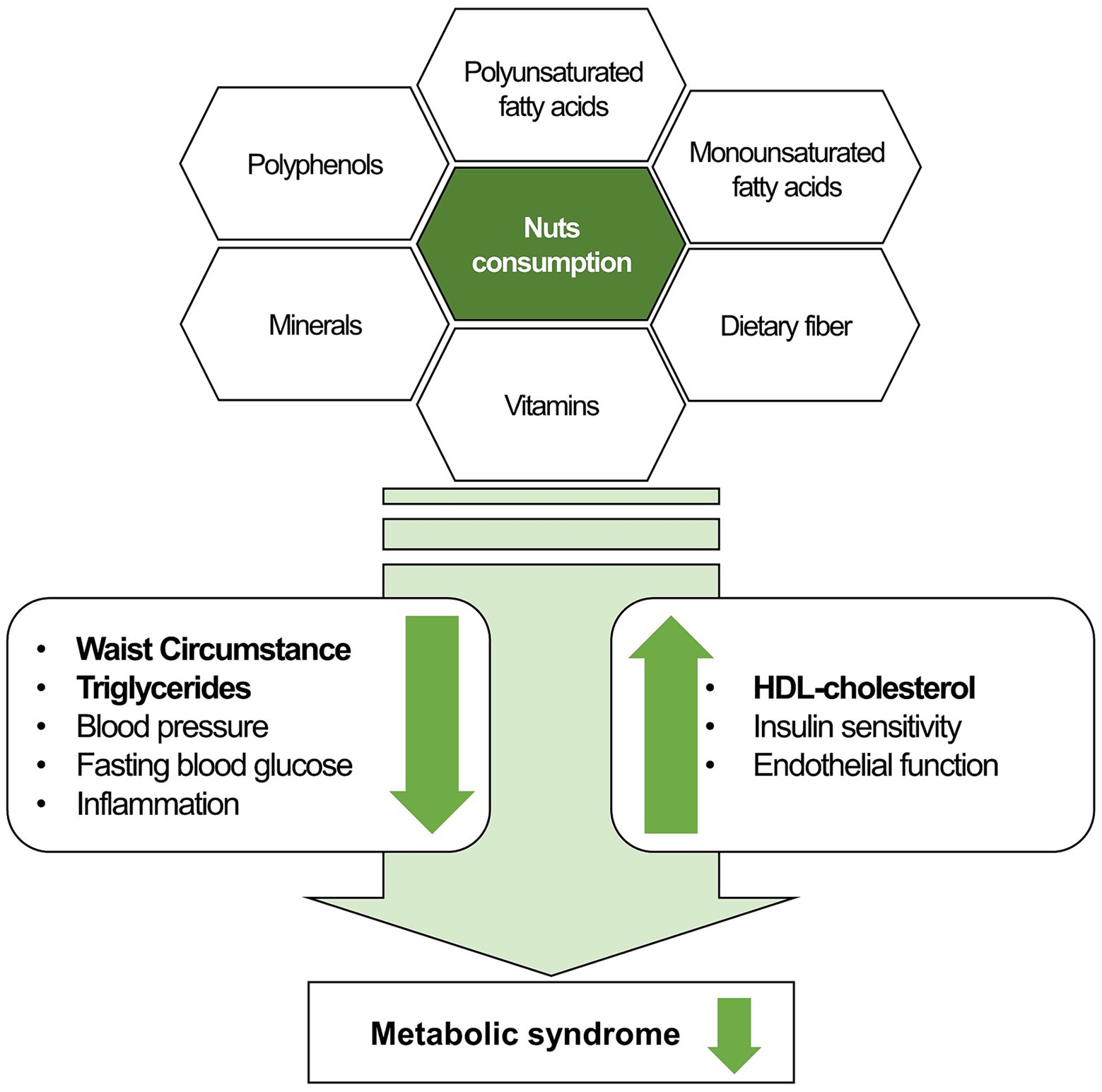
Figure 2. The role of nut consumption in prevention and management of metabolic syndrome. Bold within the figure indicates significant results from this study.
4 Discussion
4.1 Main findings of this study
This study utilized a large-scale dataset from the KoGES-HEXA to investigate the association of nut consumption frequency with metabolic syndrome and its components among Korean adults. The findings of this study indicated that an increased frequency of nut consumption was associated with a decreased prevalence of metabolic syndrome in Korean adults. Among the components of metabolic syndrome, inverse associations of nut consumption with abdominal obesity, low HDL-cholesterol levels, and elevated triglycerides levels were observed in both men and women. However, no significant association was observed between nut consumption and increased blood pressure or fasting blood glucose.
This study aligns with previous meta-analyses that revealed a decreased risk of metabolic syndrome with higher nut consumption. A meta-analysis of prospective cohort studies examined the relationship between nut consumption and the risk of metabolic syndrome and revealed that for each additional serving per week (30 g) of nuts, the risk of metabolic syndrome decreased by 4% (relative risk (RR) = 0.96, 95% CI = 0.92 to 0.99) (11). Another meta-analysis comparing high and low consumption of nuts reported an RR of 0.84 (95% CI = 0.76 to 0.92) for metabolic syndrome in the high-consumption group (28). Our finding was also consistent with a previous cohort study of Korean adults that used the Ansan–Ansung cohort study data, which discovered an inverse relationship between consuming >15 g of nuts/week and the incidence of metabolic syndrome (RR = 0.72, 95% CI = 0.56 to 0.93 in men, RR = 0.57, 95% CI = 0.41 to 0.79 in women) (14). Korean adults generally consume less nuts than individuals in the Mediterranean or Western regions; however, our research findings revealed a significant inverse association between nut consumption and risk reduction of metabolic syndrome and its components. This finding suggests that, even in populations with lower nut consumption, nuts may offer protection against metabolic syndrome because they contain beneficial nutrients. Similar to findings from previous Western studies, our results indicate that nut consumption among Koreans could have positive implications for improving cardiometabolic diseases such as CVD and metabolic syndrome.
4.2 Underlying mechanism of the association between nut consumption and metabolic syndrome
The inverse relationship between higher nut consumption and reduced risk of metabolic syndrome may be because nuts are rich in nutrients that are beneficial in preventing metabolic syndrome. Specifically, nuts have a high polyunsaturated fatty acid content, which reduces plasma triglycerides levels, thereby contributing to the amelioration of risk factors associated with metabolic syndrome (29). Dietary fiber in nuts is known to influence the gut microbiota; the fermentation of dietary fiber by these microbiota generates short-chain fatty acids as byproducts, lowering blood pressure (30). Furthermore, antioxidants such as vitamin E and carotenoids in nuts might reduce chronic inflammation and lower the risk of related diseases, thus aiding in the prevention of CVD (31, 32) (Figure 2). Therefore, dietary guidelines from the American Heart Association, DASH, and Mediterranean diet patterns consistently recommend regular moderate consumption of nuts (8, 9, 33).
Moreover, a study on a Mediterranean population with high CVD risk suggested that nut consumption is an important indicator of diet quality (34). A study using 2005–2010 National Health and Nutrition Examination Survey (NHANES) data also reported that tree nut consumption is associated with better nutrient adequacy and diet quality in adults in the US (35). In this study, the nutrient density of vitamins and minerals increased with increased nut consumption frequency, suggesting that nut consumption might be related to higher nutrient quality in the diets of Korean adults. Consequently, a higher diet quality could contribute to the prevention and management of metabolic syndrome.
4.3 Impact of nut consumption on lipid profiles and abdominal obesity
In the current study, among the metabolic syndrome components, higher nut consumption was inversely associated with abdominal obesity and dyslipidemia in both men and women. Compared with those who did not consume nuts, men and women who consumed nuts more than twice a week exhibited reduced ORs for low HDL-cholesterol and elevated triglycerides. These findings are consistent with a systematic review targeting healthy adults with overweight/obesity, which revealed that nut consumption significantly decreased triglycerides levels (weighted mean difference = −13.19 mg/dL, 95% CI = −25.90 to −0.48) (13). Additionally, a cross-sectional study involving Iranian men aged 60–74 years revealed that the highest tertile group of nut consumption resulted in 2.24 times higher HDL-cholesterol levels compared with the lowest tertile group (36). Participants with metabolic syndrome and BMI ≥ 23 kg/m2 were included in a Korean randomized, parallel, controlled study conducted over 6 weeks and revealed that women who consumed 30 g of nuts per day had significantly improved total cholesterol and non-HDL-cholesterol levels than controls (15). This inverse association between nuts and dyslipidemia could be attributed to the high content of polyunsaturated and monounsaturated fatty acids in nuts, positively affecting lipid metabolism (37).
Nuts have a high-fat content, resulting in high energy density (38). However, this study discovered that increased nut consumption among both men and women resulted in a tendency for decreased prevalence of abdominal obesity. A meta-analysis revealed that an increase of one serving per week in nut consumption was associated with a 3% reduction in the risk of overweight/obesity (RR = 0.97, 95% CI = 0.95 to 0.98) (11). Another meta-analysis of prospective cohort studies reported that nut consumption was associated with a reduction in the risk of overweight/obesity, with an RR of 0.93 (95% CI = 0.88–0.98). Moreover, replacing carbohydrate snacks with nuts during the intervention period of 16 weeks decreased waist circumference in US women, with a mean difference of −2.20 cm, and showed a trend toward reduced visceral fat, with a change of −5.27 ± 13.05 cm2 (39). Nut consumption may promote satiety because of the high protein and dietary fiber content of nuts, thereby suppressing hunger and appetite and reducing energy consumption and abdominal obesity (40, 41). The prebiotic effects of nuts on the gut microbiome may contribute to weight control (11).
4.4 Impact of nut consumption on blood pressure and fasting blood glucose
In this study, nut consumption was not significantly associated with blood pressure or fasting blood glucose levels. A cohort study in China involving participants aged ≥50 years revealed no relationship between nut consumption and the Framingham score, SBP, or DBP (42). The Seguimiento Universidad de Navarra Project, a dynamic cohort study consisting exclusively of Spanish university graduates in Spain, revealed no association between nut consumption and the risk of hypertension (RR = 0.77, 95% CI = 0.46–1.30) (43). However, a meta-analysis reported an inverse correlation between nut consumption and the risk of hypertension (RR = 0.84, 95% CI = 0.76–0.93) (44). Unsaturated fatty acids in nuts exert hypotensive effects (45). Additionally, dietary fiber, protein, arginine, and minerals such as magnesium, potassium, and calcium in nuts are potentially beneficial for hypertension (10, 32, 46).
Previous findings on nut consumption and glucose control have been inconsistent. A meta-analysis of randomized controlled trials reported that nut consumption had a favorable effect on fasting insulin and HOMA-IR but no significant effect on fasting blood glucose (47). Among healthy adults who were overweight/obese in several randomized controlled trials, nuts did not affect glycemic measures, including fasting blood glucose, fasting insulin, and HOMA-IR (13). Similarly, a study of obese adults with an average age of 40.78 years in Iran revealed that a healthful plant-based diet which included nuts showed no correlation with hyperglycemia (48). This study focused solely on fasting blood glucose levels and discovered no significant association with nut consumption. Further research is needed to completely understand the relationship between nut consumption, hypertension, and type 2 diabetes.
4.5 Variability in nut consumption and its impact on metabolic syndrome
Inconsistent results regarding the relationship between nut consumption and metabolic syndrome and its components across studies can be attributed to multiple factors. First, the frequency of nut consumption differed across the study populations. The 2012 NHANES revealed that one-third of US adults consumed at least five servings of nuts and seeds per week (1 oz. or 28.3 g) (49). Similarly, among nut consumers in Australia, the average nut intake was 11.75 g per day (50). In the Korean adults in this study, a relatively lower consumption of nuts was observed than in Western populations. Second, the types of nuts consumed by the study populations might differentially influence health outcomes due to the different nutrient and functional compound contents. For example, macadamia nuts and pecans have the highest caloric content per 100 g; walnuts contain the most polyunsaturated fatty acids; and almonds and pistachios are protein-rich. Furthermore, pistachios and cashews are notable for their high mineral contents, such as potassium and iron (51). Third, the preparation and processing of nuts, such as salting or roasting, may alter their nutritional content and health effects compared to those of raw nuts. These factors, including the amount, type, preparation, and processing of nuts consumed by study populations, might collectively influence the relationship between nut consumption and metabolic syndrome; thus, these factors need to be considered when collecting dietary data and analyses.
4.6 Limitations and strengths
This cross-sectional study had limitations in establishing causality between nut consumption and metabolic syndrome. It grouped peanuts, almonds, and pine nuts rather than analyzing them individually and did not consider other types of nuts in their association with metabolic syndrome. Additionally, the salt content and preparation methods (e.g., roasting) of the nuts consumed by the participants were not examined. Although covariates that could affect nut consumption and metabolic syndrome were adjusted, other potential confounding variables remained. For example, details regarding the exact time or frequency of physical activity were not considered. Additionally, this study could not exclude participants who followed a special diet under certain conditions.
Despite these limitations, the findings of this study provide insights into the health effects of nut consumption on metabolic syndrome based on a large-scale dataset of Korean adults. Additionally, this study is significant to understand underlying mechanism of nut intake and metabolic syndrome because it examined the association of nut consumption with metabolic syndrome components. Future studies with detailed specifications of nut varieties and nut processing conditions are necessary to further elaborate on the results of this study.
4.7 Conclusion
In Korean adults, increased frequency of nut consumption was associated with protective effects against metabolic syndrome, abdominal obesity, reduced HDL-cholesterol, and elevated triglycerides. Consistent with previous meta-analyses that predominantly involved Western populations, this study suggests that nut consumption could positively impact the reduction in metabolic syndrome and CVD risk among Koreans. Therefore, to prevent metabolic syndrome and its components, it is recommended that frequent nut consumption be incorporated into the diet.
The findings of this study may contribute to the development of dietary guidelines and public health policies for CVD prevention in this population. This study demonstrated that improving dietary habits can lower the risk of metabolic syndrome and CVD, supporting the inclusion of a balanced diet with nuts in clinical practice for the prevention and management of these diseases. Emphasizing non-pharmacological strategies, these findings encourage metabolic physicians, endocrinologists, and diabetologists to adopt these dietary recommendations. Utilizing these guidelines can facilitate early detection and targeted interventions at the primary prevention stage, essential for addressing factors influencing adult metabolism and preventing adverse cardiometabolic disorders. Further cohort and clinical studies are required to explore the complex effects of the quantity and type of nuts consumed on development of metabolic diseases.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: http://nih.go.kr/ko/main/contents.do?menuNo=300563.
Ethics statement
The studies involving humans were approved by the institutional review board of Hannam University (2023-E-01-09-0625). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HS: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. SS: Conceptualization, Project administration, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was supported by the National Research Foundation of Korea grant, funded by the Korean government (Ministry of Science and ICT) (No. 2022R1C1C1002905).
Acknowledgments
Data in this study were from the Korean Genome and Epidemiology Study (KoGES; 6635-302) and National Institute of Health, Korea Disease Control and Prevention Agency, Republic of Korea. All authors thank the participants and all members of the KoGES study Group.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. National Heart, Lung, and Blood Institute . What is metabolic syndrome? Curr Hypertens Rep. (2022) [updated May 18, 2022]. Available at: https://www.nhlbi.nih.gov/health/metabolic-syndrome.
2. Galassi, A, Reynolds, K, and He, J. Metabolic syndrome and risk of cardiovascular disease: a meta-analysis. Am J Med. (2006) 119:812–9. doi: 10.1016/j.amjmed.2006.02.031
3. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) . Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. (2002) 106:3143–3421. doi: 10.1161/circ.106.25.3143
4. Vaduganathan, M, Mensah, GA, Turco, JV, Fuster, V, and Roth, GA. The global burden of cardiovascular diseases and risk. J Am Coll Cardiol. (2022) 80:2361–71. doi: 10.1016/j.jacc.2022.11.005
5. Nikniaz, L, Mahmudiono, T, Jasim, SA, Vajdi, M, Thangavelu, L, and Farhangi, MA. Nutrient pattern analysis of mineral based, simple sugar based, and fat based diets and risk of metabolic syndrome: a comparative nutrient panel. BMC Endocr Disord. (2022) 22:51. doi: 10.1186/s12902-022-00963-2
6. Vajdi, M, Farhangi, MA, and Nikniaz, L. Diet-derived nutrient patterns and components of metabolic syndrome: a cross-sectional community-based study. BMC Endocr Disord. (2020) 20:69. doi: 10.1186/s12902-020-0547-0
7. Vajdi, M, Karimi, A, Farhangi, MA, and Ardekani, AM. The association between healthy lifestyle score and risk of metabolic syndrome in Iranian adults: a cross-sectional study. BMC Endocr Disord. (2023) 23:16. doi: 10.1186/s12902-023-01270-0
8. Appel, LJ, Moore, TJ, Obarzanek, E, Vollmer, WM, Svetkey, LP, Sacks, FM, et al. A clinical trial of the effects of dietary patterns on blood pressure. N Engl J Med. (1997) 336:1117–24. doi: 10.1056/nejm199704173361601
9. Martínez-González, MA, Gea, A, and Ruiz-Canela, M. The Mediterranean diet and cardiovascular health. Circ Res. (2019) 124:779–98. doi: 10.1161/CIRCRESAHA.118.313348
10. De Souza, RGM, Schincaglia, RM, Pimentel, GD, and Mota, JF. Nuts and human health outcomes: a systematic review. Nutrients. (2017) 9:1311. doi: 10.3390/nu9121311
11. Li, H, Li, X, Yuan, S, Jin, Y, and Lu, J. Nut consumption and risk of metabolic syndrome and overweight/obesity: a meta-analysis of prospective cohort studies and randomized trials. Nutr Metab. (2018) 15:46. doi: 10.1186/s12986-018-0282-y
12. Blanco Mejia, S, Kendall, CW, Viguiliouk, E, Augustin, LS, Ha, V, Cozma, AI, et al. Effect of tree nuts on metabolic syndrome criteria: a systematic review and meta-analysis of randomized controlled trials. BMJ Open. (2014) 4:e004660. doi: 10.1136/bmjopen-2013-004660
13. Eslami, O, Khorramrouz, F, Sohouli, M, Bagheri, N, Shidfar, F, and Fernandez, ML. Effect of nuts on components of metabolic syndrome in healthy adults with overweight/obesity: a systematic review and meta-analysis. Nutr Metab Cardiovasc Dis. (2022) 32:2459–69. doi: 10.1016/j.numecd.2022.07.015
14. Jung, JY, Park, SK, Oh, C-M, Choi, J-M, Ryoo, J-H, Kim, J, et al. The association between metabolic syndrome and peanuts, pine nuts, almonds consumption: the Ansan and Ansung study. Endocrine. (2019) 65:270–7. doi: 10.1007/s12020-019-01980-3
15. Lee, YJ, Nam, GE, Seo, JA, Yoon, T, Seo, I, Lee, JH, et al. Nut consumption has favorable effects on lipid profiles of Korean women with metabolic syndrome. Nutr Res. (2014) 34:814–20. doi: 10.1016/j.nutres.2014.08.011
16. Lobene, AJ . The increasing prevalence of metabolic syndrome in Korea: a multifarious disease with a multifactorial etiology. JACC Asia. (2023) 3:503–5. doi: 10.1016/j.jacasi.2023.05.004
18. Kim, Y, and Han, B-GKoGES Consortium. Cohort profile: the Korean genome and epidemiology study (KoGES) consortium. Int J Epidemiol. (2017) 46:e20. doi: 10.1093/ije/dyv316
19. National Institute of Health . The Korean genome and epidemiology study (KoGES). Osong: National Institute of Health (2022).
20. Kwon, YS, Ryu, J, Yang, Y, Park, YK, and Kim, S. Trends and dietary assessment according to fruit and vegetable intake in Korean elderly people: analysis based on the Korea National Health and nutrition examination survey 1998, 2008, and 2018. Food Secur. (2020) 9:1712. doi: 10.3390/foods9111712
21. Sung, H, Park, JM, Oh, SU, Ha, K, and Joung, H. Consumption of ultra-processed foods increases the likelihood of having obesity in Korean women. Nutrients. (2021) 13:698. doi: 10.3390/nu13020698
22. Jo, U, and Park, K. Carbohydrate-based diet may increase the risk of cardiovascular disease: a pooled analysis of two prospective cohort studies. Clin Nutr. (2023) 42:1301–7. doi: 10.1016/j.clnu.2023.06.013
23. Ahn, Y, Kwon, E, Shim, JE, Park, MK, Joo, Y, Kimm, K, et al. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur J Clin Nutr. (2007) 61:1435–41. doi: 10.1038/sj.ejcn.1602657
24. Kang, HT, Kim, SY, Kim, J, Kim, J, Kim, J, Park, HA, et al. Clinical practice guideline of prevention and treatment for metabolic syndrome. Korean J Fam Pract. (2015) 5:375–420.
25. Huh, JH, Kang, DR, Kim, JY, and Koh, KK. Metabolic syndrome fact sheet 2021: executive report. Cardiometab Syndr J. (2021) 1:125–34. doi: 10.51789/cmsj.2021.1.e15
26. Jung, H, Shin, J, Lim, K, and Shin, S. Edible mushroom intake and risk of all-cause and cause-specific mortality: results from the Korean genome and epidemiology study (KoGES) cohort. Food Funct. (2023) 14:8829–37. doi: 10.1039/D3FO00996C
27. Health Examinees Study Group. The health examinees (HEXA) study: rationale, study design and baseline characteristics. Asian Pac J Cancer Prev. (2015) 16:1591–7. doi: 10.7314/apjcp.2015.16.4.1591
28. Zhang, Y, and Zhang, D-Z. Relationship between nut consumption and metabolic syndrome: a meta-analysis of observational studies. J Am Coll Nutr. (2019) 38:499–505. doi: 10.1080/07315724.2018.1561341
29. Bornfeldt, KE . Triglyceride lowering by omega-3 fatty acids: a mechanism mediated by n-acyl taurines. J Clin Invest. (2021) 131:e147558. doi: 10.1172/JCI147558
30. Xu, C, and Marques, FZ. How dietary fibre, acting via the gut microbiome, lowers blood pressure. Curr Hypertens Rep. (2022) 24:509–21. doi: 10.1007/s11906-022-01216-2
31. Jackson, CL, and Hu, FB. Long-term associations of nut consumption with body weight and obesity. Am J Clin Nutr. (2014) 100:408S–11S. doi: 10.3945/ajcn.113.071332
32. de Souza, RJ, Dehghan, M, Mente, A, Bangdiwala, SI, Ahmed, SH, Alhabib, KF, et al. Association of nut intake with risk factors, cardiovascular disease, and mortality in 16 countries from 5 continents: analysis from the PURE study. Am J Clin Nutr. (2020) 112:208–19. doi: 10.1093/ajcn/nqaa108
33. American Heart Association . The American Heart Association diet and lifestyle recommendations 2023. Available at: https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/nutrition-basics/aha-diet-and-lifestyle-recommendations.
34. Bibiloni, MM, Julibert, A, Bouzas, C, Martínez-González, MA, Corella, D, Salas-Salvadó, J, et al. Nut consumptions as a marker of higher diet quality in a Mediterranean population at high cardiovascular risk. Nutrients. (2019) 11:754. doi: 10.3390/nu11040754
35. O'Neil, CE, Nicklas, TA, and Fulgoni, VL. Tree nut consumption is associated with better nutrient adequacy and diet quality in adults: National Health and nutrition examination survey 2005-2010. Nutrients. (2015) 7:595–607. doi: 10.3390/nu7010595
36. Askari, M, Daneshzad, E, Jafari, A, Bellissimo, N, and Azadbakht, L. Association of nut and legume consumption with Framingham 10 year risk of general cardiovascular disease in older adult men: a cross-sectional study. Clin Nutr ESPEN. (2021) 42:373–80. doi: 10.1016/j.clnesp.2020.12.024
37. Tapsell, L, Batterham, M, Tan, S-Y, and Warensjö, E. The effect of a calorie-controlled diet containing walnuts on substrate oxidation during 8-hours in a room calorimeter. J Am Coll Nutr. (2009) 28:611–7. doi: 10.1080/07315724.2009.10719793
38. Nishi, SK, Viguiliouk, E, Blanco Mejia, S, Kendall, CWC, Bazinet, RP, Hanley, AJ, et al. Are fatty nuts a weighty concern? A systematic review and meta-analysis and dose–response meta-regression of prospective cohorts and randomized controlled trials. Obes Rev. (2021) 22:e13330. doi: 10.1111/obr.13330
39. Sumislawski, K, Widmer, A, Suro, RR, Robles, ME, Lillegard, K, Olson, D, et al. Consumption of tree nuts as snacks reduces metabolic syndrome risk in young adults: a randomized trial. Nutrients. (2023) 15:5051. doi: 10.3390/nu15245051
40. Tan, SY, and Mattes, RD. Appetitive, dietary, and health effects of almonds consumed with meals or as snacks: a randomized, controlled trial. Eur J Clin Nutr. (2013) 67:1205–14. doi: 10.1038/ejcn.2013.184
41. Guarneiri, LL, and Cooper, JA. Intake of nuts or nut products does not lead to weight gain, independent of dietary substitution instructions: a systematic review and meta-analysis of randomized trials. Adv Nutr. (2021) 12:384–401. doi: 10.1093/advances/nmaa113
42. Sun, Y, Jiang, CQ, Cheng, KK, Zhang, WS, Leung, GM, Lam, TH, et al. Nut consumption and cardiovascular risk in older Chinese: the Guangzhou biobank cohort study. PLoS One. (2015) 10:e0137178. doi: 10.1371/journal.pone.0137178
43. Martínez-Lapiscina, EH, Pimenta, AM, Beunza, JJ, Bes-Rastrollo, M, Martínez, JA, and Martínez-González, MA. Nut consumption and incidence of hypertension: the SUN prospective cohort. Nutr Metab Cardiovasc Dis. (2010) 20:359–65. doi: 10.1016/j.numecd.2009.04.013
44. Guo, K, Jiang, Y, Zhou, Z, and Li, Y. Retracted: nut consumption with risk of hypertension and type 2 diabetes mellitus: a meta-analysis of prospective cohort studies. Eur J Prev Cardiol. (2020) 27:NP6–NP15. doi: 10.1177/2047487313501120
45. Estruch, R, Martínez-González, MA, Corella, D, Salas-Salvadó, J, Ruiz-Gutiérrez, V, Covas, MI, et al. Effects of a Mediterranean-style diet on cardiovascular risk factors: a randomized trial. Ann Intern Med. (2006) 145:1–11. doi: 10.7326/0003-4819-145-1-200607040-00004
46. Mohammadifard, N, Salehi-Abargouei, A, Salas-Salvadó, J, Guasch-Ferré, M, Humphries, K, and Sarrafzadegan, N. The effect of tree nut, peanut, and soy nut consumption on blood pressure: a systematic review and meta-analysis of randomized controlled clinical trials. Am J Clin Nutr. (2015) 101:966–82. doi: 10.3945/ajcn.114.091595
47. Tindall, AM, Johnston, EA, Kris-Etherton, PM, and Petersen, KS. The effect of nuts on markers of glycemic control: a systematic review and meta-analysis of randomized controlled trials. Am J Clin Nutr. (2019) 109:297–314. doi: 10.1093/ajcn/nqy236
48. Vajdi, M, Karimi, A, Tousi, AZ, Hosseini, B, Nikniaz, Z, and Farhangi, MA. Association between plant-based diets and metabolic syndrome in obese adults from Iran: a cross-sectional study. BMC Endocr Disord. (2023) 23:109. doi: 10.1186/s12902-023-01358-7
49. Rehm, CD, Peñalvo, JL, Afshin, A, and Mozaffarian, D. Dietary intake among US adults, 1999–2012. JAMA. (2016) 315:2542–53. doi: 10.1001/jama.2016.7491
50. Batterham, MJ, Neale, EP, Nikodijevic, CJ, Probst, YC, and Tapsell, LC. Nut consumption in a representative survey of Australians: a secondary analysis of the 2011–2012 National Nutrition and physical activity survey. Public Health Nutr. (2020) 23:3368–78. doi: 10.1017/S1368980019004117
51. U.S. Department of Agriculture . Agricultural Research Service USDA National Nutrient Database for standard reference, release 28. Beltsville, MD; (2016). Available at: http://www.ars.usda.gov/ba/bhnrc/ndl.
Keywords: nut, metabolic syndrome, KoGES, Korean adults, cardiovascular disease
Citation: Shin HR and Song S (2024) Association between nut consumption and metabolic syndrome in Korean adults: results from the Korean Genome and Epidemiology Study–Health Examinees. Front. Nutr. 11:1400212. doi: 10.3389/fnut.2024.1400212
Edited by:
Giuseppina Mandalari, University of Messina, ItalyReviewed by:
Sui Kiat Chang, Universiti Tunku Abdul Rahman, MalaysiaMahdi Vajdi, Isfahan University of Medical Sciences, Iran
Elnaz Daneshzad, Tehran University of Medical Sciences, Iran
Copyright © 2024 Shin and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: SuJin Song, sjsong@hnu.kr