Anesthesia for fetal operative procedures: A systematic review
 Miriam Duci1,†,‡
Miriam Duci1,†,‡  Rebecca Pulvirenti1,†,‡
Rebecca Pulvirenti1,†,‡  Francesco Fascetti Leon1*†
Francesco Fascetti Leon1*†  Irma Capolupo2,† Paola Veronese3,†
Irma Capolupo2,† Paola Veronese3,†  Piergiorgio Gamba1,†
Piergiorgio Gamba1,†  Costanza Tognon4
Costanza Tognon4
- 1Pediatric Surgery Unit, Department of Women’s and Children’s Health, Padua University Hospital, Padua, Italy
- 2Department of Medical and Surgical Neonatology, Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy
- 3Maternal-fetal Medicine Unit, Department of Women’s and Children’s Health, Padua University Hospital, Padua, Italy
- 4Anesthesiology Pediatric Unit, Department of Women’s and Children’s Health, Padua University Hospital, Padua, Italy
Objective: The anesthetic management of fetal operative procedures (FOP) is a highly debated topic. Literature on fetal pain perception and response to external stimuli is rapidly expanding. Nonetheless, there is no consensus on the fetal consciousness nor on the instruments to measure pain levels. As a result, no guidelines or clinical recommendations on anesthesia modality during FOP are available. This systematic literature review aimed to collect the available knowledge on the most common fetal interventions, and summarize the reported outcomes for each anesthetic approach. Additional aim was to provide an overall evaluation of the most commonly used anesthetic agents.
Methods: Two systematic literature searches were performed in Embase, Medline, Web of Science Core Collection and Cochrane Central Register of Controlled Trials up to December 2021. To best cover the available evidence, one literature search was mostly focused on fetal surgical procedures; while anesthesia during FOP was the main target for the second search. The following fetal procedures were included: fetal transfusion, laser ablation of placental anastomosis, twin-reversed arterial perfusion treatment, fetoscopic endoluminal tracheal occlusion, thoraco-amniotic shunt, vesico-amniotic shunt, myelomeningocele repair, resection of sacrococcygeal teratoma, ligation of amniotic bands, balloon valvuloplasty/septoplasty, ex-utero intrapartum treatment, and ovarian cyst resection/aspiration. Yielded articles were screened against the same inclusion criteria. Studies reporting anesthesia details and procedures’ outcomes were considered. Descriptive statistical analysis was performed and findings were reported in a narrative manner.
Results: The literature searches yielded 1,679 articles, with 429 being selected for full-text evaluation. A total of 168 articles were included. Overall, no significant differences were found among procedures performed under maternal anesthesia or maternal-fetal anesthesia. Procedures requiring invasive fetal manipulation resulted to be more effective when performed under maternal anesthesia only. Based on the available data, a wide range of anesthetic agents are currently deployed and no consistency has been found neither between centers nor procedures.
Conclusions: This systematic review shows great variance in the anesthetic management during FOP. Further studies, systematically reporting intraoperative fetal monitoring and fetal hormonal responses to external stimuli, are necessary to identify the best anesthetic approach. Additional investigations on pain pathways and fetal pain perception are advisable.
1. Introduction
The recent advancement of minimally invasive techniques, together with a deeper knowledge of maternal-fetal physiology, led to major progresses in the field of fetal surgery. As a result, the treatment of congenital malformations, historically planned after delivery, has become feasible at the prenatal stage. Nonetheless, the maternal and fetal anesthetic management during such procedures is still controversial. Indeed, based on the invasiveness of the procedure, either general or regional maternal anesthesia can be required, in conjunction or not with fetal direct anesthesia (1). Generally, fetal operative procedures (FOP) are challenging, and anesthetic care needs to take into account not only maternal and fetal physiology, but also the anesthetic drugs’ interaction with the maternal-fetal health (2). Furthermore, it is still debated whether the fetus is able to experience pain during a fetal procedure. Recent studies describing an increase in cortisol and adrenaline levels or the development of bradycardia after painful stimuli in fetuses of 16–25 weeks of gestational age (GA), demonstrated a reaction to pain during prenatal life (3, 4). Additionally, available evidence on fetal physiology showed that between 16–24 weeks of GA the thalamus, an essential organ for pain perception, seems to be adequately developed (5–7). However, how much these changes imply a conscious pain processing and how to best measure the pain level in fetuses is still poorly understood. No anesthesia guidelines or standardized protocols for FOP are available, and the decision mainly depends on the expert’s opinion and expertise.
The lack of evidence prompted us to perform a systematic review on the use of maternal-fetal anesthesia in FOP. Therefore, this study aimed to collect the available knowledge on the most common fetal interventions and summarize the reported outcomes for each anesthetic approach. For every prenatal intervention, outcomes were compared between procedures performed under maternal anesthesia and those performed under maternal and fetal anesthesia; when applicable to the retrieved data, further distinction among loco-regional and general maternal anesthesia was made. Additional objective was to provide a general evaluation of the most commonly used anesthetics for all the included procedures.
2. Methods
This review was performed according to an a priori designed protocol and recommended for systematic reviews (8, 9). Additionally, the principles of the “preferred reporting items for systematic reviews” (PRISMA) statement were adhered to (10). This study is registered in the PROSPERO database (registration number CRD42022302979). A systematic literature search was performed in Embase, Medline, Web of Science Core Collection and Cochrane Central Register of Controlled Trials until December 14 2021. The fetal operative procedures considered were: fetal transfusion, laser ablation of placental anastomosis, twin-reversed arterial perfusion treatment, fetoscopic endoluminal tracheal occlusion (FETO) in congenital diaphragmatic hernia (CDH), thoraco-amniotic shunt, vesico-amniotic shunt, myelomeningocele (MMC) repair, resection of sacrococcygeal teratoma, ligation of amniotic bands, balloon valvuloplasty/septoplasty, ex-utero intrapartum treatment (EXIT), and ovarian cyst resection/aspiration. Since combining each procedure with the search term “anesthesia” yielded a limited number of studies, a second search focused on the provision of maternal-fetal anesthesia was performed. Databases screened and search date were the same for both systematic searches. The search strategies are attached in the Supplementary Material. The search and selection criteria were restricted to English language articles and limited to humans. No publication year restriction was considered. Due to the known clinical heterogeneity of included studies a meta-analysis method would have been inappropriate. Therefore, we described our findings in a narrative manner.
2.1. Inclusion criteria and exclusion criteria
Studies were assessed according to the following criteria: population characteristics, intervention and reported outcome. All studies describing outcomes for fetal procedures and providing details on maternal-fetal anesthesia were included. Studies describing maternal-fetal anesthesia, but no procedure outcome were only included in the overall analysis of anesthesia modality and in the report of anesthetic drugs used. Since many studies refer to anesthesia and analgesia interchangeably, both terms were considered during the studies’ screening against inclusion criteria.
Conference abstracts, editorials, letters, short surveys, studies reporting non-original data (systematic reviews, meta-analysis, narrative reviews) and unavailable full-text articles were excluded. Absence of discrete patients data was an additional exclusion criteria.
2.2. Study selection
Two review authors (MD and RP) independently screened titles and abstracts to select eligible studies. Disagreements about study selection were resolved by discussion. MD and RP screened full-texts of selected studies against the inclusion and exclusion criteria. During all stages of study selection, any uncertainties or discrepancies were discussed until consensus was achieved. If consensus was not reached, disagreements were resolved by discussing them with senior researchers (FFL, PV, IC and CT).
2.3. Data extraction
The following variables were extracted and entered into a standard data extraction form: author, publication year, country treating hospital, study type, number of included patients, GA at time of fetal procedure, type of disease, fetal procedure performed, anesthesia modality (both maternal and fetal), anesthetic drugs used, duration of procedure, maternal and fetal perioperative complications, gestational age at delivery, procedure outcome and effectiveness.
2.4. Synthesis
Fetal procedures were addressed as effective whenever they led to the delivery of vital neonates. Exception was the MMC repair, in which the reversal of the hindbrain herniation was considered as additional criteria. Referring to the laser ablation of placental anastomosis (in twin-to-twin transfusion syndrome), effectiveness was assumed when both fetuses survived.
Perioperative complications were divided between intraoperative, maternal postoperative, and fetal postoperative complications. Maternal postoperative complications were gathered into five groups: chorioamnionitis, abruptio placentae, chorioamniotic membrane separation, acute respiratory distress syndromes and “other”. All postoperative fetal complications were independently considered.
Premature rupture of membranes (PROM) and perinatal deaths (within the first 24 h) were considered as separate outcomes. When evaluating the proportion of perinatal deaths on the total number of patients, twin and triplet pregnancies were considered two and three times, respectively. Miscarriages and termination of pregnancies were considered as perinatal deaths. Additional outcomes evaluated were the length of hospitalization (LOH) after the fetal intervention and GA at delivery.
In order to verify whether the anesthesia modality has an influence on the procedure outcome, subgroups analysis was performed evaluating maternal and fetal anesthesia (MFA) vs. maternal anesthesia (MA) only. Similar evaluations were performed for the most represented fetal procedures. Additionally, considering only the procedures requiring invasive fetal manipulation (MMC repair, FETO, shunting, resection of sacrococcygeal teratoma, ligation of amniotic bands, balloon valvuloplasty/septoplasty, and ovarian cyst resection/aspiration), further evaluations on the impact of fetal anesthesia were conducted. Lastly, the most commonly used anesthetic agents for both, general maternal anesthesia and fetal anesthesia, were described.
2.5. Statistical analysis
Aggregated continuous baseline variables were calculated as means or medians of extracted variables from the included studies. Categorical and continuous variables were summarized as numbers with percentages. Statistical analysis was performed using Fisher's exact test for categorical data, while continuous data were compared using Mann Whitney U-test. P <0.05 was considered statistically significant.
3. Results
The systematic search strategies yielded 1,679 articles, and 429 of them were further assessed for eligibility. After full-text screening against inclusion criteria, 168 articles, accounting for 6,761 procedures, were selected (Figure 1) (11–178). Fourteen of the included studies, not providing information on the procedure outcome, were only considered for the initial description of anesthesia modality and in the summary of anesthetic drugs used (13, 25, 31, 42, 53, 60, 66, 109, 110, 123, 142, 147, 148, 165). Characteristics of the included studies can be found in Supplementary Material.
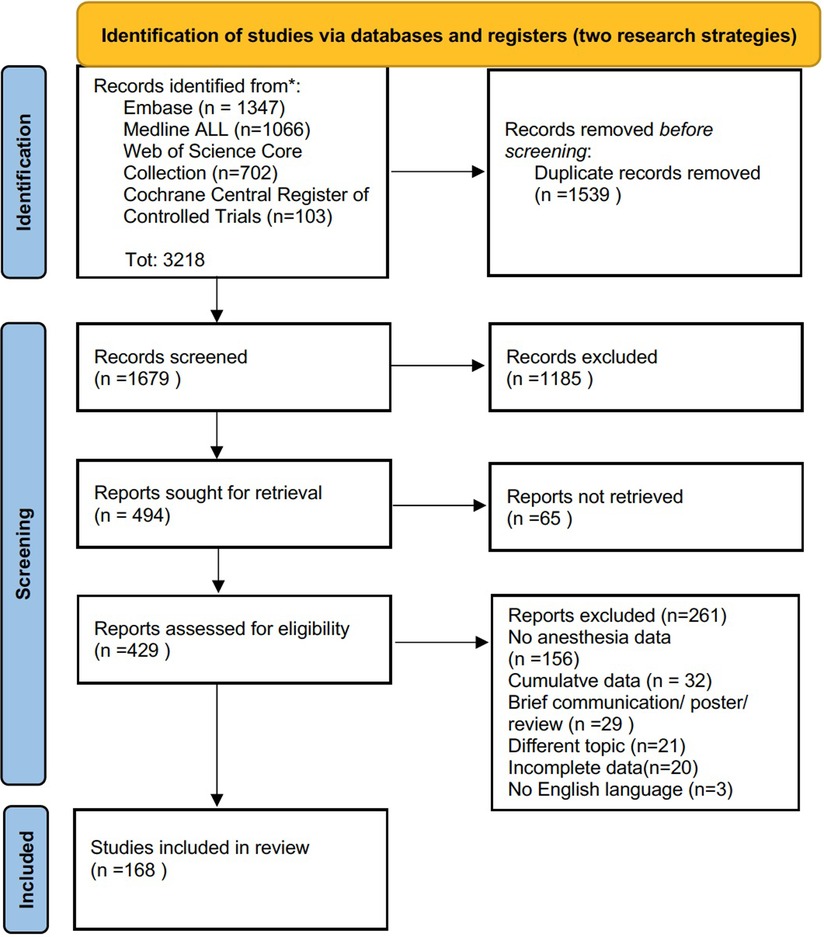
Figure 1. PRISMA flow diagram of literature search (10).
3.1. Anesthesia modality
A total of 165 studies reported detailed information on the anesthesia modality, accounting for 6,751 patients. In 106 of them (5,087 procedures) only MA was provided, while MFA was delivered in 64 studies (1,664 procedures) (1–13, 14–69, 71–123, 125–178). Fetal anesthesia was more frequently administered in case of general maternal anesthesia (p = 0.0001).
3.1.1. Maternal anesthesia
Ninety-seven studies, accounting for 4,070 pregnancies, were included in the baseline characteristics and outcome analysis for MA (11, 15, 21–24, 26–29, 33, 35, 38–40, 46, 48, 50–52, 58, 61–65, 67–69, 71–82, 84, 87, 89–94, 96, 97, 99, 101–103, 105, 107, 111, 113–117, 120, 122, 126, 128–134, 137–139, 149, 151, 152, 154–157, 159–162, 164, 166–169, 171, 173–175, 178). The aggregated mean GA at procedure, based on data from 85 studies (3,801 pregnancies), was 27.03 weeks (11, 15, 22–24, 26–29, 33, 35, 38, 40, 46, 48, 50–52, 58, 61–63, 65, 67–69, 71–82, 87, 89, 90, 92–94, 96, 97, 99, 101–103, 105, 107, 111, 113, 116, 117, 120, 122, 126, 128–134, 137, 138, 149, 151, 154–157, 160, 162, 164, 166–169, 171, 173, 175, 178). The mean LOH resulted to be 4.98 days, based on 24 studies involving 903 women (21, 24, 28, 29, 40, 46, 52, 64, 73, 77, 84, 90, 91, 93, 99, 105, 114, 115, 120, 134, 137, 149, 155, 173). Sixty-four studies, with 3,032 pregnancies, resulted in an aggregated mean GA at delivery of 33.39 weeks (11, 22, 27–29, 33, 39, 40, 46, 50, 51, 58, 61, 64, 65, 69, 73–78, 80, 81, 87, 90–93, 94, 96, 99, 101, 102, 105, 107, 113–117, 120, 122, 130–134, 137–139, 152, 154–157, 159, 160, 164, 166–169, 171, 173, 175, 178). Overall, PROM occurred in 888 pregnancies (21.8%). A total of 1,493 fetuses died during pregnancy or within the first 24 h of life (21.45%). The procedures were reported as effective in 73.99% of cases.
A total of 44 intraoperative complications were reported (1.08%), while fetal postoperative complications were observed in 77 cases (1.89%). Maternal postoperative complications were encountered in 332 women (8.15%), consisting of 115 chorioamniotic membrane separations, 104 abruptio placentae, 54 chorioamnionitis, 17 acute respiratory distress syndromes, and 42 “other”. Complications’ details can be found in Supplementary material.
3.1.1.1. Loco-regional vs. general maternal anesthesia
Ninety-five studies (3,905 pregnancies) were included for the comparative analysis of the anesthesia administration's routes (11, 15, 21–24, 26–29, 33, 35, 38–40, 46, 48, 50–52, 58, 61–65, 67–69, 71–82, 84, 87, 89–94, 96, 97, 99, 101–103, 105, 107, 111, 113–116, 120, 122, 126, 128–134, 137–139, 149, 151, 152, 154–157, 159–162, 164, 166–169, 171, 173–175). No statistically significant differences were found in the baseline characteristics and outcomes between patients receiving loco-regional and general anesthesia (Table 1).

Table 1. Baseline characteristics and outcomes for loco-regional anesthesia vs general anesthesia in procedures performed under maternal anesthesia.
3.1.2. Maternal and fetal anesthesia
MFA was provided in 1,551 procedures from 59 studies (12, 16–20, 30, 32, 34, 36, 37, 41, 43–45, 47, 49, 50, 52, 54–57, 59, 62, 63, 68, 83, 85, 86, 88, 95, 98, 100, 104, 106, 108, 112, 118, 119, 121, 125, 127, 136, 140, 141, 143–146, 150, 153, 158, 163, 170, 172, 176, 177). Fetal anesthesia administration was specified in 50 studies, consisting of 635 intramuscular injections (45 studies), 292 subcutaneous injections (three studies) and four intravenous injections (two studies) (16–20, 30, 32, 34, 36, 37, 41, 43, 44, 47, 49, 50, 52, 54, 55, 57, 59, 63, 83, 86, 95, 98, 100, 104, 106, 108, 118, 119, 121, 125, 127, 136, 140, 141, 143–146, 150, 153, 158, 163, 170, 176, 177). An aggregate mean GA at procedure of 27.99 weeks was calculated on 49 studies and 1,404 pregnancies (12, 16–19, 30, 32, 34, 36, 37, 41, 43–45, 47, 49, 50, 52, 54–57, 59, 62, 63, 68, 83, 85, 86, 88, 95, 98, 100, 104, 106, 108, 112, 118, 119, 121, 125, 127, 135, 136, 140, 141, 143–146, 150, 153, 158, 163, 170, 172, 176, 177). Mean LOH, based on data from 18 studies and 92 women, was 3.79 days (16, 18, 19, 32, 36, 43–45, 47, 52, 55, 86, 98, 100, 106, 118, 153, 176). A total of 33 studies (1,196 pregnancies) provided information on the GA at delivery, resulting in an aggregate mean of 34.89 weeks (17–19, 37, 41, 45, 49, 54, 59, 108, 118, 121, 125, 127, 135, 136, 140, 141, 143–145, 158, 170, 176, 177). PROM occurred in 401 pregnancies (25.85%) and 197 fetal deaths were reported (11.37%). Overall, effectiveness of the procedures was 75.85%.
Complications during the procedure occurred in 12 cases (0.74%). Postoperative complications, either fetal or maternal, were reported for 27 (1.6%) and 174 (10.8%) procedures, respectively. Maternal complications comprised 121 chorioamniotic membrane separation, 25 chorioamnionitis, twelve abruptio placentae, three acute respiratory distress syndromes, and thirteen “other”. Complications’ details can be found in Supplementary material.
3.1.2.1 Loco-regional vs. general maternal anesthesia in MFA
All studies providing MFA were included in the comparison. The mean LOH resulted to be significantly longer in women who underwent general anesthesia, compared to those who underwent loco-regional anesthesia (p = 0.0088) (16, 18, 19, 32, 36, 43–45, 47, 52, 55, 86, 98, 100, 106, 118, 153, 176). No other statistically significant differences were found (Table 2).
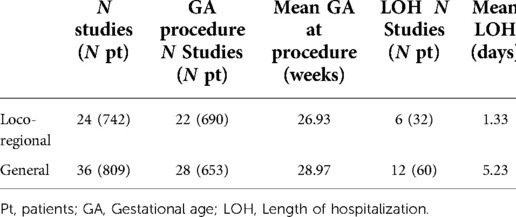
Table 2. Baseline characteristics and outcomes in maternal loco-regional anesthesia vs general anesthesia in procedures performed under maternal and fetal anesthesia.
3.2. Laser ablation of placental anastomosis
Twenty-nine studies, accounting for 2,964 pregnancies with twin-to-twin transfusion syndrome (TTTS), were included (22, 27, 48, 61, 64, 69, 72, 79, 87, 94, 96, 102, 105, 107, 114, 117, 122, 131–133, 149, 155, 156, 164, 167–169, 174). All but one study performed MA; the one study describing laser ablation of placental anastomosis under MFA was excluded from the sub analysis (135). Patients baseline characteristics and procedure outcomes were compared between the administration of loco-regional and general MA, without identifying any statistical difference (Table 3).
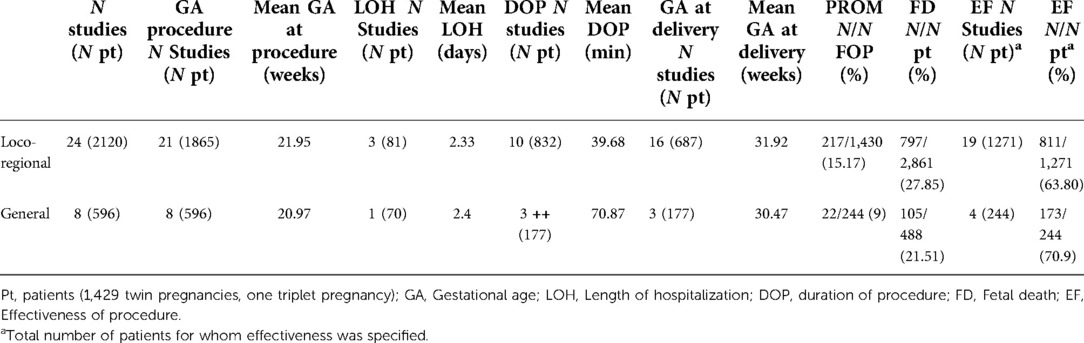
Table 3. Baseline characteristics and outcomes in maternal loco-regional anesthesia vs general anesthesia in laser ablation of placental anastomosis procedures.
3.3. Myelomeningocele repair
MMC repair was described in 35 studies, totaling 1,372 patients. Open (16, 20, 24, 28, 40, 46, 54, 73, 85, 86, 91, 113, 115, 120, 121, 127, 137, 154, 156, 158, 166, 172, 176, 177) and fetoscopic (17–19, 28, 29, 33, 99, 134, 140, 171, 178) repair were individually evaluated. One study was excluded due to cumulative data on both surgical approaches (41). For each operative technique, baseline characteristics and procedure outcomes were evaluated based on the provision of MA or MFA. In both analysis there were no statistically significant differences (Tables 4, 5).
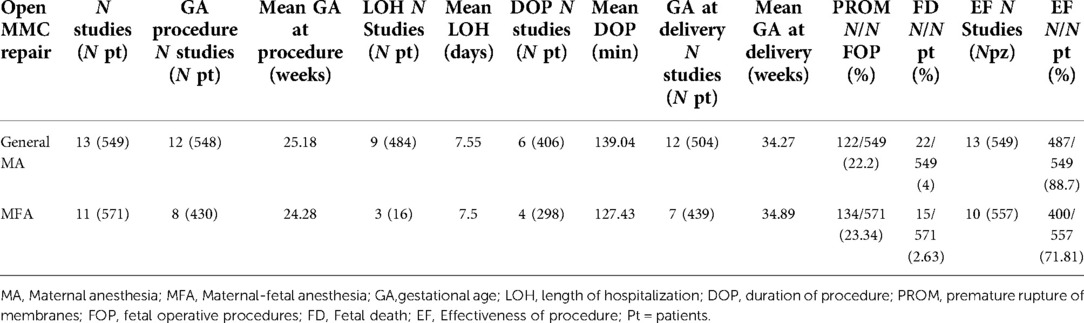
Table 4. Baseline characteristics and outcomes in maternal general anesthesia vs maternal and fetal anesthesia in open myelomeningocele repair.

Table 5. Baseline characteristics and outcomes in maternal general anesthesia vs maternal and fetal anesthesia in fetoscopic myelomeningocele repair.
3.4. Fetoscopic endoluminal tracheal occlusion
A total of 508 fetuses with CDH, from twelve studies, underwent FETO (44, 50, 51, 56, 78, 88, 135, 136, 141, 143, 146, 172). In 58 cases only MA was performed (50, 51, 78). Aggregate mean GA at procedure and at delivery were 26.5 and 32.8 weeks, respectively. The procedure resulted effective in 91.4% of cases, with 30 PROM and 7 fetal deaths being described.
MFA was provided in nine studies and 450 procedures (44, 56, 88, 135, 136, 141, 143, 146, 172). Seven studies reported the GA at procedure, which resulted in an aggregate mean of 27.3 weeks (44, 56, 88, 135, 136, 143, 146). Aggregated mean GA at delivery was 34.1 weeks, based on data from six studies (50, 88, 136, 141, 143, 146). PROM and fetal deaths rates were 43.3% and 6.9%, respectively. Overall, effectiveness of the procedure was 79.3%.
3.5. Ex-utero intrapartum treatment
Forty-one of the included studies, accounting for 129 patients, described the EXIT procedure (12, 15, 21, 23, 26, 30, 32, 34, 35, 38, 52, 55, 57, 62, 63, 67, 68, 71, 82–84, 89, 92, 95, 97, 98, 100, 103, 104, 106, 111, 119, 124, 126, 128, 129, 151, 153, 160–162). Six studies provided cumulative data on the anesthesia modality and therefore were excluded from the subgroup analysis (21, 38, 62, 68, 124, 129). Studies describing MA or MFA were compared, and no statistically significant differences were found (Table 6).

Table 6. Baseline characteristics and outcomes in maternal general anesthesia vs maternal and fetal anesthesia in ex-utero intrapartum treatment procedure.
3.6. Shunting
Seven studies, accounting for 39 patients, described a shunting procedure due to pleural effusion (n = 2), lower urinary tract occlusion (n = 3) and congenital lung malformation (n = 2) (11, 39, 75, 145, 152, 170, 175). Maternal anesthesia was performed in eleven patients from five studies (11, 39, 75, 152, 175). The aggregated mean GA at procedure, based on three studies, was 29.6 weeks (11, 75, 175). All studies provided information on GA at delivery, resulting in an aggregate mean of 35.22 weeks. PROM and fetal death rates were 45.45% and 1.8%, respectively; effectiveness of the procedure was 81.8%. Two studies, totaling 28 patients, preferred MFA (145, 170). Aggregated mean GA was 21.65 weeks at procedure, and 31.6 weeks at delivery. Fetal deaths occurred in 53.5% of cases; the procedure effectiveness was 43.75%.
3.7. Impact of fetal anesthesia in procedures requiring invasive fetal manipulation
To evaluate the impact of fetal anesthesia, 81 studies, accounting for 2,112 patients, were considered. MA was performed in 827 procedures (11, 24, 28, 29, 33, 39, 40, 46, 50, 51, 58, 65, 73, 75–78, 81, 90, 91, 99, 101, 113, 115, 120, 130, 134, 137–139, 152, 154, 157, 159, 166, 171, 173, 175, 178), while MFA in 1,285 (14, 16–20, 36, 37, 41, 43–45, 47, 49, 50, 54, 56, 59, 70, 85, 86, 88, 108, 112, 118, 121, 125, 127, 135, 136, 140, 141, 143–146, 150, 158, 163, 170, 172, 176, 177).
PROM and fetal deaths showed a higher prevalence in the MFA group (p < 0.0001 and p = 0.0169, respectively). Subsequently, the procedures performed under MA resulted to be more effective (88.63% vs. 74.57%, p < 0.0001). The remaining parameters did not show any statistical differences (Table 7).
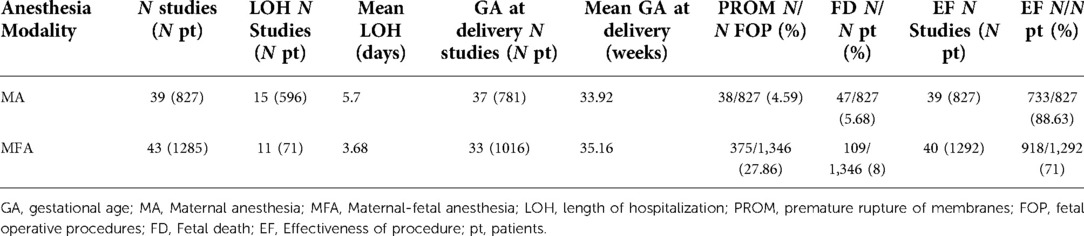
Table 7. Outcomes comparison in maternal anesthesia vs maternal and fetal anesthesia in procedures requiring invasive fetal manipulations.
3.8. Fetal and maternal anesthetic agents
3.8.1. Anesthetic agents for fetal anesthesia
Sixty studies, accounting for 1,524 procedures, described the anesthetic agents used to provide direct fetal anesthesia (14, 16–20, 30, 32, 34, 36, 37, 41, 43–45, 47, 49, 50, 52, 54–57, 59, 62, 63, 66, 68, 70, 83, 85, 86, 88, 95, 98, 100, 104, 106, 108–110, 118, 121, 125, 127, 135, 140, 141, 143–148, 153, 158, 163, 170, 176, 177). The most common anesthetic agents are summarized in Table 8.

Table 8. Most commonly used fetal anesthetic agents.
3.8.2. Anesthetic agents for general maternal anesthesia
Fifty-six studies, with a total of 1,127 patients, specified the drugs used to provide general maternal anesthesia (11, 13, 15, 19, 22, 24–26, 30–32, 35, 41, 42, 46, 50, 52, 53, 55, 57, 63, 64, 66, 71, 73, 78, 81, 82, 84, 86, 90, 95, 97, 99, 103, 104, 106, 108–110, 115, 119, 124, 126, 128, 134, 141, 142, 151, 153, 158, 160–162, 173). The extreme variability between the studies did not allow a specific analysis. The preferably used induction agents for general MA included thiopental, associated with neuromuscular blocking drugs (e.g., succinylcholine, rocuronium) or propofol. Following, MA was maintained with either a volatile anesthetic agent (e.g., desflurane, sevoflurane, isoflurane) or a combination of volatile and intravenous (e.g., propofol) anesthetic agents. Seldom, an epidural catheter was inserted for postoperative analgesia.
4. Discussion
4.1. Summary of main results
The studies included in this systematic review widely varied in terms of study design, population and outcome. Several anesthesia approaches were used, with no standardized protocols nor common strategies based on the fetal procedure.
Overall, no significant differences were found among procedures performed under MA or MFA, reflecting the absence of a close link between reported outcomes and anesthesia modality. Complicating furthermore, several factors influencing the procedures’ outcome (e.g., maternal comorbidities, pregnancy-related health conditions, etc.) were not systematically reported.
Procedures requiring invasive fetal manipulation resulted to be more effective when performed under MA only. Indeed, higher rates of PROM and fetal deaths were found in the MFA group. Based on the retrieved data, the combined use of maternal and fetal anesthetics could translate in fetal over treatment and, consequently, greater risk of fetal death. Additionally, fetal direct anesthesia mostly involved the administration of curare, which exposure-related effects on fetuses have not been fully understood yet. Nevertheless, further studies are necessary to properly evaluate such results and identify an eventual physiopathological explanation.
Lastly, a significant preference for the use of fentanyl, atropine, vecuronium or pancuronium was found in the provision of direct fetal anesthesia. Anyhow, dosages used in different studies were extremely heterogeneous, varying among hundreds of micrograms. The same conclusions can be drawn referring to maternal general anesthetics, thus only few studies reported dosages for the maternal drugs used. Based on the available data, no specific anesthetic modality proved to be superior to the others.
4.2. Potential biases in the review process
The quality of the available evidence on the maternal-fetal anesthesia management during fetal surgery is poor. Although included studies provided some anesthesia data, most of them aimed to describe the surgical technique or the effectiveness of the procedure as primary outcome. As a consequence, anesthesia details were missing, as those referring to intraoperative monitoring. Indeed, only few studies included information regarding intraoperative fetal heartbeat variations or fetal movements. Hence, defining the impact of anesthesia on the procedure's performance was not possible.
Additionally, in order to incorporate a large group of patients for this systematic review, studies with wide variance in terms of methodology were included, and no limitation on publication date was defined. As a consequence, the overall quality of the studies might have been negatively influenced.
Complicating furthermore, fetal surgical procedures became more popular over time and several authors who started with a case report description are now sharing their experience on a large cohort of patients. This translates in a potential population bias, with the inclusion of some patients more than once.
4.3. Agreements and disagreements with other studies or reviews
The need for adequate MFA during fetal interventions is a highly debated topic. Indeed, the ever-increasing performance of invasive prenatal surgery brought some authors to address concerns on the fetuses’ pain perception. Studies on intraoperative fetal monitoring revealed that neuroinhibiting substances (adenosine, pregnanolone, prostaglandine D2) (179), ensuring a continuous sleep status during pregnancy, are inadequate to ensure fetal anesthesia (7). Subsequently, starting from the second trimester, fetuses seem to be awakened by external stimuli (180).
Additionally, current evidence highlights how an early form of pain could appear in fetuses starting from 15 weeks of GA, mainly depending on the reticular formation of the mesodiencephalon. Later on, the diencephalon seems to occupy a leading role in the fetal pain experience and, only toward the end of pregnancy, the nociceptive pathway is completed by the cortex cerebri development (6).
Nevertheless, exact pain processing pathways during fetal life are yet to be extensively evaluated; and whether an external stimuli is able to trigger a conscious cortical processing is still debated. As a consequence, no standardized recommendations for anesthesia during FOP are available.
Some authors consider fetal direct anesthesia to be justified, as it provides intraoperative fetal immobilization and, at the same time, ensures no pain perception (181). This way, it might avoid the long-term impact of early painful experiences, which proved to alter the course of sensory development (182). Conversely, other authors have concerns on the potentially negative effects of direct early-life exposure to general anesthetics. Neurotoxicity or behavioral and cognitive deficits have been previously demonstrated, yet only a few longitudinal studies on this topic are available (183, 184). Adding up to this, some studies proved that fetal immobilization can be obtained through maternal sedative drugs administration (e.g., diazepam or remifentanil), overcoming the need for combined MFA (185).
Results from this systematic review do not provide an answer to this controversy. Anyhow, based on the retrieved data, anesthesia modality seems to have no impact on the fetal procedure's outcome. The great variety of anesthetic approaches used, even when comparing the same procedure, does not translate into different perioperative or delivery-related complication rates. Nevertheless, when comparing anesthesia modalities for invasive fetal procedures, interventions involving direct fetal anesthesia resulted in a worse outcome (higher PROM and fetal deaths rates). This result highlights the need for future evaluation on early-life anesthetic administration, bearing in mind that the retrieved data are insufficient to entirely prove a causal association between the two events.
Another point to consider is that no study fully analyzed fetal reactions to the surgical procedure, complicating the choice of outcome parameters to use in order to evaluate the impact of different anesthesia modalities. Indeed, the outcome criteria used in this review are not uniquely linked to the anesthetic approach, yet influenced by several fetal and maternal factors.
Ring / Ginosar and Van de Velde et al. provided some general suggestions on the anesthesia modality to be used, based on the invasiveness and fetal direct manipulation of different FOP's categories (182, 186). However, the real need for fetal direct anesthesia has not been properly assessed and, based on this systematic review, no study explicitly takes into account the transplacental passage of anesthetics while providing MFA.
Referring to the anesthetic drugs used, included studies describing fetal direct anesthesia mostly administered fentanyl, atropine, and vecuronium/pancuronium. This is in line with previous reports and necessary to obtain complete fetal immobilization (186).
Conversely, maternal anesthesia did not follow a specific pattern nor required the use of particular drugs. The involved studies widely varied in terms of maternal anesthetic agents, most likely depending on each center policy. Worth mentioning, more recent studies showed a trend toward new maternal anesthetic drug, combinations aiming to ensure adequate uterine relaxation. This is in line with the American consensus statement on anesthesia for maternal-fetal intervention (187). Indeed, high doses of volatile anesthetic agents were traditionally used to maintain uterine relaxation. However, this practice can be associated with significant fetal bradycardia. More recently, intravenous anesthesia with remifentanil allowed to reduce the dosages of volatile anesthetics and minimize fetal cardiac dysfunction.
4.4. Implication for practice
One of the primary aims of this systematic review was to evaluate the impact of different anesthetic approaches on FOP's outcome. Due to the heterogeneity of the included studies and the lack of standardized intraoperative fetal monitoring, defining the best anesthesia modality between MA and MFA is difficult. When referring to the procedures' outcome, and based on the retrieved data, fetal direct anesthesia does not seem to be an added value in FOP, not positively influencing neither perioperative complications nor fetal deaths rates.
Nonetheless, recent literature on fetal pain perception opens up to a pathophysiological and ethical discussion, encouraging the use of MFA. Although fetal direct anesthesia might not be technically essential, it might be paramount for the fetal wellbeing and neurological development.
4.5. Implication for research
This systematic review highlights the lack of standardized anesthetic approaches to FOP. The ongoing improvement of prenatal surgical care requires a parallel implementation of anesthesia guidelines and protocols. Further studies aiming to evaluate fetal reaction to pain and comparing different anesthesia approaches are needed. Fetal intraoperative parameters, together with hormonal responses to different stimuli and anesthetic approaches, should be systematically investigated. Alongside, as long-term neurocognitive impairment has been proved to be caused by early-life exposure to both, anesthetics agents and painful experiences, prospective studies on neurodevelopment for school-aged children who underwent FOP with different anesthetic approaches, might solve the dilemma between MA and MFA.
5. Conclusions
This systematic review shows great variance in the anesthetic management for maternal-fetal interventions. Available evidence is too diverse to define the best modality for drug delivery and the optimal drug to be used for these procedures. Further studies systematically reporting intraoperative fetal monitoring (e.g., heartbeat variations, fetal movements) and fetal hormonal responses to external stimuli are necessary to identify the best anesthetic approach. Moreover, a standardized reporting of such parameters might help evaluate fetal response to pain, and serve as a basis to better understand fetal pain perception. Afterwards, expert consensus would be advisable to improve both maternal and fetal outcomes.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
MD and RP provided study conception and design, data collection, statistical analysis and writing—first draft and revised versions. FFL provided statistical analysis and writing—editing and revision. IC, PV, PG and CT provided study conception and design, writing—editing and revised versions. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors wish to thank Marjolein Udo, Maarten F.M. Engel and Wichor from the Erasmus MC Medical Library (Rotterdam—The Netherlands) for developing and updating the search strategies
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpain.2022.935427/full#supplementary-material.
References
1. Lin EE, Tran KM. Anesthesia for fetal surgery. Semin Pediatr Surg. (2013) 22:50–5. doi: 10.1053/j.sempedsurg.2012.10.009
2. Chang AB. Physiology changes of pregnancy. In: Elsevier-Mosby, editor. Obstet anesth princ pract. Philadelphia: Elsevier-Mosby (2004). p. 15–36.
3. Giannakoulopoulos X, Teixeira J, Fisk N, Glover V. Human fetal and maternal noradrenaline responses to invasive procedures. Pediatr Res. (1999) 45:494–9. doi: 10.1203/00006450-199904010-00007
4. Mayorga-Buiza MJ, Marquez-Rivas J, Gomez-Gonzalez E. Can fetus feel pain in the second trimester? Lessons learned from a sentinel event. Child’s Nerv Syst. (2018) 34:195–6. doi: 10.1007/s00381-017-3677-6
5. Yen C-T, Lu P-L. Thalamus and pain. Acta Anaesthesiol Taiwanica. (2013) 51:73–80. doi: 10.1016/j.aat.2013.06.011
6. Sekulic S, Gebauer-Bukurov K, Cvijanovic M, Kopitovic A, Ilic D, Petrovic D, et al. Appearance of fetal pain could be associated with maturation of the mesodiencephalic structures. J Pain Res. (2016) 9:1031–8. doi: 10.2147/JPR.S117959
7. Bellieni C V. Analgesia for fetal pain during prenatal surgery: 10 years of progress. Pediatr Res. (2021) 89:1612–8. doi: 10.1038/s41390-020-01170-2
8. CfRa D. CRD’s guidance for undertaking reviews in health care. Vol. 32. York: York Publ Serv Ltd. (2009).
9. Henderson LK, Craig JC, Willis NS, Tovey D, Webster AC. How to write a Cochrane systematic review. Nephrology. (2010) 15:617–24. doi: 10.1111/j.1440-1797.2010.01380.x
10. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) 62:e1–e34. doi: 10.1016/j.jclinepi.2009.06.006
11. Adzick NS, Harrison MR, Flake AW, Howell LJ, Golbus MS, Filly RA. Fetal surgery for cystic adenomatoid malformation of the lung. J Pediatr Surg. (1993) 28:806–12. doi: 10.1016/0022-3468(93)90332-f
12. Agarwal A, Rosenkranz E, Yasin S, Swaminathan S. EXIT Procedure for fetal mediastinal teratoma with large pericardial effusion: a case report with review of literature. J Matern Neonatal Med. (2018) 31:1099–103. doi: 10.1080/14767058.2017.1306851
13. Arens C, Koch C, Veit M, Greenberg RS, Lichtenstern C, Weigand MA, et al. Anesthetic management for percutaneous minimally invasive fetoscopic surgery of spina bifida aperta: a retrospective, descriptive report of clinical experience. Anesth Analg. (2017) 125:219–22. doi: 10.1213/ANE.0000000000001896
14. Ashmead GG, Mercer B, Herbst M, Moodley J, Bota A, Elder JS. Fetal bladder outlet obstruction due to ureterocele: in utero “colander” therapy. J Ultrasound Med. (2004) 23:565–8. doi: 10.7863/jum.2004.23.4.565
15. Baker PA, Aftimos S, Anderson BJ. Airway management during an EXIT procedure for a fetus with dysgnathia complex. Paediatr Anaesth. (2004) 14:781–6. doi: 10.1111/j.1460-9592.2004.01284.x
16. Barini R, Barreto MWG, Cursino K, Zambelli H, Prando A, Sbragia L. Abruptio placentae during fetal myelomeningocele repair. Fetal Diagn Ther. (2006) 21:115–7. doi: 10.1159/000089060
17. Baschat AA, Ahn ES, Murphy J, Miller JL. Fetal blood-gas values during fetoscopic myelomeningocele repair performed under carbon dioxide insufflation. Ultrasound Obstet Gynecol. (2018) 52:400–2. doi: 10.1002/uog.19083
18. Belfort MA, Whitehead WE, Shamshirsaz AA, Ruano R, Cass DL, Olutoye OO. Fetoscopic repair of meningomyelocele. Obstet Gynecol. (2015) 126:881–4. doi: 10.1097/AOG.0000000000000835
19. Belfort MA, Whitehead WE, Shamshirsaz AA, Bateni ZH, Olutoye OO, Olutoye OA, et al. Fetoscopic open neural tube defect repair: development and refinement of a two-port, carbon dioxide insufflation technique. Obstet Gynecol. (2017) 129:734–43. doi: 10.1097/AOG.0000000000001941
20. Bennett KA, Carroll MA, Shannon CN, Braun SA, Dabrowiak ME, Crum AK, et al. Reducing perinatal complications and preterm delivery for patients undergoing in utero closure of fetal myelomeningocele: further modifications to the multidisciplinary surgical technique. J Neurosurg Pediatr. (2014) 14:108–14. doi: 10.3171/2014.3.PEDS13266
21. Benonis JG, Habib AS. Ex utero intrapartum treatment procedure in a patient with arthrogryposis multiplex congenita, using continuous spinal anesthesia and intravenous nitroglycerin for uterine relaxation. Int J Obstet Anesth. (2008) 17:53–6. doi: 10.1016/j.ijoa.2007.01.007
22. Bergh EP, Mann LK, Jain RR, Donepudi R, Moise KJJ, Johnson A, et al. Effect of intra-amniotic fluid pressure from polyhydramnios on cervical length in patients with twin-twin transfusion syndrome undergoing fetoscopic laser surgery. Ultrasound Obstet Gynecol. (2019) 54:774–9. doi: 10.1002/uog.20228
23. Berrington JE, Stafford FW, Macphail S. Emergency EXIT for preterm labour after FETO. Arch Dis Child Fetal Neonatal Ed. (2010) 95:F376–7. doi: 10.1136/adc.2009.177303
24. Botelho RD, Imada V, Rodrigues da Costa KJ, Watanabe LC, Rossi Júnior R, De Salles AAF, et al. Fetal myelomeningocele repair through a mini-hysterotomy. Fetal Diagn Ther. (2017) 42:28–34. doi: 10.1159/000449382
25. Bouwman FCM, Klein WM, de Blaauw I, Woiski MD, Verhoeven BH, Botden SMBI. Lymphatic malformations adjacent to the airway in neonates: risk factors for outcome. J Pediatr Surg. (2021) 56:1764–70. doi: 10.1016/j.jpedsurg.2021.03.011
26. Braden A, Maani C, Nagy C. Anesthetic management of an ex utero intrapartum treatment procedure: a novel balanced approach. J Clin Anesth. (2016) 31:60–3. doi: 10.1016/j.jclinane.2015.12.010
27. Brock CO, Bergh EP, Hernandez-Andrade EA, Ruano R, Johnson A, Papanna R. Risk factors and outcomes following septostomy during fetoscopic surgery for twin-to-twin transfusion syndrome. J Clin Med. (2021) 10:3693. doi: 10.3390/jcm10163693
28. Bruner JP, Tulipan NB, Richards WO, Walsh WF, Boehm FH, Vrabcak EK. In utero repair of myelomeningocele: a comparison of endoscopy and hysterotomy. Fetal Diagn Ther. (2000) 15:83–8. doi: 10.1159/000020981
29. Bruner JP, Richards WO, Tulipan NB, Arney TL. Endoscopic coverage of fetal myelomeningocele in utero. Am J Obstet Gynecol. (1999) 180:153–8. doi: 10.1016/s0002-9378(99)70167-5
30. Bui TH, Grunewald C, Frenckner B, Kuylenstierna R, Dahlgren G, Edner A, et al. Successful EXIT (ex utero intrapartum treatment) procedure in a fetus diagnosed prenatally with congenital high-airway obstruction syndrome due to laryngeal atresia. Eur J Pediatr Surg. (2000) 10:328–33. doi: 10.1055/s-2008-1072385
31. Bussey JG, Luks F, Carr SR, Plevyak M, Tracy TFJ. Minimal-access fetal surgery for twin-to-twin transfusion syndrome. Surg Endosc. (2004) 18:83–6. doi: 10.1007/s00464-003-8179-9
32. Butwick A, Aleshi P, Yamout I. Obstetric hemorrhage during an EXIT procedure for severe fetal airway obstruction. Can J Anaesth. (2009) 56:437–42. doi: 10.1007/s12630-009-9092-z
33. Carrabba G, Macchini F, Fabietti I, Schisano L, Meccariello G, Campanella R, et al. Minimally invasive fetal surgery for myelomeningocele: preliminary report from a single center. Neurosurg Focus. (2019) 47:E12. doi: 10.3171/2019.8.FOCUS19438
34. Castillo F, Peiró JL, Carreras E, Ruiz C, Linde A, Ribes C, et al. The exit procedure (ex-utero intrapartum treatment): management of giant fetal cervical teratoma. J Perinat Med. (2007) 35:553–5. doi: 10.1515/JPM.2007.120
35. Chang LC, Kuczkowski KM. The ex utero intrapartum treatment procedure: anesthetic considerations. Arch Gynecol Obstet. (2008) 277:83–5. doi: 10.1007/s00404-007-0402-9
36. Chmait RH, Chon AH, Anselmo D, Vanderbilt DL, Townsend J, Julian-Wang B, et al. In utero fetal intubation for a large neck mass: a minimally invasive EXIT option. Fetal Diagn Ther. (2019) 45:275–80. doi: 10.1159/000487394
37. Ciccolo ML, Rothman A, Galindo A, Acherman RJ, Evans WN. Successful immediate newborn ross-konno and mitral valve repair following fetal aortic valvuloplasty. World J Pediatr Congenit Heart Surg. (2012) 3:264–6. doi: 10.1177/2150135111433471
38. Clark KD, Viscomi CM, Lowell J, Chien EK. Nitroglycerin for relaxation to establish a fetal airway (EXIT procedure). Obstet Gynecol. (2004) 103:1113–5. doi: 10.1097/01.AOG.0000125158.61232.b3
39. Clark SL, Vitale DJ, Minton SD, Stoddard RA, Sabey PL. Successful fetal therapy for cystic adenomatoid malformation associated with second-trimester hydrops. Am J Obstet Gynecol. (1987) 157:294–5. doi: 10.1016/s0002-9378(87)80154-0
40. Corral E, Sepulveda W, Ravera F, Muller JM, Tapia M, Reascos M, et al. Use of plastic wound retractor at hysterotomy site in prenatal repair of myelomeningocele: a new technique. J Matern Neonatal Med. (2020) 33:3010–5. doi: 10.1080/14767058.2019.1566902
41. Corroenne R, Yepez M, Barth J, Pan E, Whitehead WE, Espinoza J, et al. Chorioamniotic membrane separation following fetal myelomeningocele repair: incidence, risk factors and impact on perinatal outcome. Ultrasound Obstet Gynecol. (2020) 56:684–93. doi: 10.1002/uog.21947
42. Cruz-Martínez R, Gámez-Varela A, Cruz-Lemini M, Martínez-Rodríguez M, Luna-García J, López-Briones H, et al. Doppler Changes in umbilical artery, middle cerebral artery, cerebroplacental ratio and ductus venosus during open fetal microneurosurgery for intrauterine open spina bifida repair. Ultrasound Obstet Gynecol. (2021) 58:238–44. doi: 10.1002/uog.22177
43. Cruz-Martinez R, Moreno-Alvarez O, Garcia M, Méndez A, Pineda H, Cruz-Martinez MA, et al. Fetal endoscopic tracheal intubation: a new fetoscopic procedure to ensure extrauterine tracheal permeability in a case with congenital cervical teratoma. Fetal Diagn Ther. (2015) 38:154–8. doi: 10.1159/000362387
44. Cruz-Martínez R, Martínez-Rodríguez M, Gámez-Varela A, Nieto-Castro B, Luna-García J, Juárez-Martínez I, et al. Survival outcome in severe left-sided congenital diaphragmatic hernia with and without fetal endoscopic tracheal occlusion in a country with suboptimal neonatal management. Ultrasound Obstet Gynecol. (2020) 56:516–21. doi: 10.1002/uog.21993
45. Cruz-Martínez R, Martínez-Rodríguez M, Gámez-Varela A, Luna-García J, López-Briones H, Chávez-González E, et al. Fetoscopic urethral meatotomy in fetuses with lower urinary tract obstruction by congenital megalourethra. Prenat Diagn. (2021) 41:772–7. doi: 10.1002/pd.5946
46. Cruz-Martínez R, Chavelas-Ochoa F, Martínez-Rodríguez M, Aguilar-Vidales K, Gámez-Varela A, Luna-García J, et al. Open fetal microneurosurgery for intrauterine spina bifida repair. Fetal Diagn Ther. (2021) 48:163–73. doi: 10.1159/000513311
47. Cruz-Martinez R, Méndez A, Perez-Garcilita O, Monroy A, Aguilar-Vidales K, Cruz-Martinez MA, et al. Fetal bronchoscopy as a useful procedure in a case with prenatal diagnosis of congenital microcystic adenomatoid malformation. Fetal Diagn Ther. (2015) 37:75–80. doi: 10.1159/000361015
48. De Lia JE, Kuhlmann RS, Lopez KP. Treating previable twin-twin transfusion syndrome with fetoscopic laser surgery: outcomes following the learning curve. J Perinat Med. (1999) 27:61–7. doi: 10.1515/JPM.1999.007
49. Dębska M, Koleśnik A, Kretowicz P, Olędzka A, Rebizant B, Gastoł P, et al. Urethroplasty with balloon catheterization in fetal lower urinary tract obstruction: observational study of 10 fetuses. Ultrasound Obstet Gynecol. (2020) 56:916–20. doi: 10.1002/uog.21932
50. Deprest J, Gratacos E, Nicolaides KH. Fetoscopic tracheal occlusion (FETO) for severe congenital diaphragmatic hernia: evolution of a technique and preliminary results. Ultrasound Obstet Gynecol. (2004) 24:121–6. doi: 10.1002/uog.1711
51. Deprest JA, Nicolaides KH, Benachi A, Gratacos E, Ryan G, Persico N, et al. Randomized trial of fetal surgery for severe left diaphragmatic hernia. N Engl J Med. (2021) 385:107–18. doi: 10.1056/NEJMoa2027030
52. Dinges E, Heier J, Delgado C, Bollag L. Multimodal general anesthesia approach for Ex Utero Intrapartum Therapy (EXIT) procedures: two case reports. Int J Obstet Anesth. (2019) 38:142–5. doi: 10.1016/j.ijoa.2018.08.009
53. Duron VD, Watson-Smith D, Benzuly SE, Muratore CS, O’Brien BM, Carr SR, et al. Maternal and fetal safety of fluid-restrictive general anesthesia for endoscopic fetal surgery in monochorionic twin gestations. J Clin Anesth. (2014) 26:184–90. doi: 10.1016/j.jclinane.2013.10.010
54. Elbabaa SK, Gildehaus AM, Pierson MJ, Albers JA, Vlastos EJ. First 60 fetal in-utero myelomeningocele repairs at Saint Louis Fetal Care Institute in the post-MOMS trial era: hydrocephalus treatment outcomes (endoscopic third ventriculostomy versus ventriculo-peritoneal shunt). Child’s Nerv Syst. (2017) 33:1157–68. doi: 10.1007/s00381-017-3428-8
55. Elliott R, Vallera C, Heitmiller ES, Isaac G, Lee M, Crino J, et al. Ex utero intrapartum treatment procedure for management of congenital high airway obstruction syndrome in a vertex/breech twin gestation. Int J Pediatr Otorhinolaryngol. (2013) 77:439–42. doi: 10.1016/j.ijporl.2012.11.023
56. Engels AC, Van Calster B, Richter J, DeKoninck P, Lewi L, De Catte L, et al. Collagen plug sealing of iatrogenic fetal membrane defects after fetoscopic surgery for congenital diaphragmatic hernia. Ultrasound Obstet Gynecol. (2014) 43:54–9. doi: 10.1002/uog.12547
57. Eschertzhuber S, Keller C, Mitterschiffthaler G, Jochberger S, Kühbacher G. Verifying correct endotracheal intubation by measurement of end-tidal carbon dioxide during an ex utero intrapartum treatment procedure. Anesth Analg. (2005) 101:658–60. doi: 10.1213/01.ANE.0000175206.91231.77
58. Fan D, Wu S, Wang R, Huang Y, Fu Y, Ai W, et al. Successfully treated congenital cystic adenomatoid malformation by open fetal surgery: a care-compliant case report of a 5-year follow-up and review of the literature. Medicine (Baltimore). (2017) 96:e5865. doi: 10.1097/MD.0000000000005865
59. Ferschl MB, Moon-Grady AJ, Rollins MD, Gilliss B, Schulman SR, Tulzer G, et al. CASE 8-2016 Percutaneous fetal cardiac intervention for severe aortic stenosis and evolving hypoplastic left-heart syndrome. J Cardiothorac Vasc Anesth. (2016) 30:1118–28. doi: 10.1053/j.jvca.2016.03.155
60. Ferschl MB, Feiner J, Vu L, Smith D, Rollins MD. A comparison of spinal anesthesia versus monitored anesthesia care with local anesthesia in minimally invasive fetal surgery. Anesth Analg. (2020) 130:409–15. doi: 10.1213/ANE.0000000000003947
61. Fichera A, Azzaretto VV, Fratelli N, Mancino S, Marella D, Negri B, et al. Fetoscopic laser ablation therapy in monochorionic diamniotic twin pregnancies with twin-to-twin transfusion syndrome treated at a single centre over 10 years: a retrospective study. J Perinat Med. (2022) 50:34–41. doi: 10.1515/jpm-2021-0058
62. Fink RJ, Allen TK, Habib AS. Remifentanil for fetal immobilization and analgesia during the ex utero intrapartum treatment procedure under combined spinal-epidural anaesthesia. Br J Anaesth. (2011) 106:851–5. doi: 10.1093/bja/aer097
63. Gaiser RR, Cheek TG, Kurth CD. Anesthetic management of cesarean delivery complicated by ex utero intrapartum treatment of the fetus. Anesth Analg. (1997) 84:1150–3. doi: 10.1097/00000539-199705000-00039
64. Galinkin JL, Gaiser RR, Cohen DE, Crombleholme TM, Johnson M, Kurth CD. Anesthesia for fetoscopic fetal surgery: twin reverse arterial perfusion sequence and twin-twin transfusions syndrome. Anesth Analg. (2000) 91:1394–7. doi: 10.1097/00000539-200012000-00017
65. Garcia AM, Morgan WM 3rd, Bruner JP. In utero decompression of a cystic grade IV sacrococcygeal teratoma. Fetal Diagn Ther. (1998) 13:305–8. doi: 10.1159/000020859
66. García I, Suárez E, Maiz N, Pascual M, Perera R, Arévalo S, et al. Fetal heart rate monitoring during fetoscopic repair of open spinal neural tube defects: a single-centre observational cohort study. Int J Obstet Anesth. (2021) 48:103195. doi: 10.1016/j.ijoa.2021.103195
67. Garcia PJ, Olutoye OO, Ivey RT, Olutoye OA. Case scenario: anesthesia for maternal-fetal surgery: the Ex Utero Intrapartum Therapy (EXIT) procedure. Anesthesiology. (2011) 114:1446–52. doi: 10.1097/ALN.0b013e31821b173e
68. George RB, Melnick AH, Rose EC, Habib AS. Case series: combined spinal epidural anesthesia for Cesarean delivery and ex utero intrapartum treatment procedure. Can J Anaesth. (2007) 54:218–22. doi: 10.1007/BF03022643
69. Gil Guevara E, Pazos A, Gonzalez O, Carretero P, Molina FS. Doppler Assessment of patients with twin-to-twin transfusion syndrome and survival following fetoscopic laser surgery. Int J Gynaecol Obstet. (2017) 137:241–5. doi: 10.1002/ijgo.12143
70. Giorlandino C, Rivosecchi M, Bilancioni E, Bagolan P, Zaccara A, Taramanni C, et al. Successful intrauterine therapy of a large fetal ovarian cyst. Prenat Diagn. (1990) 10:473–5. doi: 10.1002/pd.1970100710
71. Gonzales SK, Goudy S, Prickett K, Ellis J. EXIT (Ex utero intrapartum treatment) in a growth restricted fetus with tracheal atresia. Int J Pediatr Otorhinolaryngol. (2018) 105:72–4. doi: 10.1016/j.ijporl.2017.12.010
72. Greimel P, Zenz A, Csapó B, Haeusler M, Lang U, Klaritsch P. Maternal complications and hemodynamic changes following intrauterine interventions for twin-to-twin transfusion syndrome in monochorionic diamniotic twin pregnancies. J Clin Med. (2019) 8:605. doi: 10.3390/jcm8050605
73. Guilbaud L, Maurice P, Lallemant P, De Saint-Denis T, Maisonneuve E, Dhombres F, et al. Open fetal surgery for myelomeningocele repair in France. J Gynecol Obstet Hum Reprod. (2021) 50:102155. doi: 10.1016/j.jogoh.2021.102155
74. Gul A, Gungorduk K, Yildirim G, Gedikbasi A, Yildirim D, Ceylan Y. Fetal therapy in twin reversed arterial perfusion sequence pregnancies with alcohol ablation or bipolar cord coagulation. Arch Gynecol Obstet. (2008) 278:541–5. doi: 10.1007/s00404-008-0640-5
75. Hannah DM, Badell ML, Woodham PC. In utero congenital chylothorax treatment with fetal thoracoamniotic shunt: case report. J Neonatal Perinatal Med. (2020) 13:427–30. doi: 10.3233/NPM-190235
76. Hara T, Mimura K, Endo M, Fujii M, Matsuyama T, Yagi K, et al. Diagnosis, management, and therapy of fetal ovarian cysts detected by prenatal ultrasonography: a report of 36 cases and literature review. Diagnostics (Basel, Switzerland). (2021) 11:2224. doi: 10.3390/diagnostics11122224
77. Harrison MR, Adzick NS, Jennings RW, Duncan BW, Rosen MA, Filly RA, et al. Antenatal intervention for congenital cystic adenomatoid malformation. Lancet (London, England). (1990) 336:965–7. doi: 10.1016/0140-6736(90)92420-m
78. Harrison MR, Keller RL, Hawgood SB, Kitterman JA, Sandberg PL, Farmer DL, et al. A randomized trial of fetal endoscopic tracheal occlusion for severe fetal congenital diaphragmatic hernia. N Engl J Med. (2003) 349:1916–24. doi: 10.1056/NEJMoa035005
79. Hecher K, Plath H, Bregenzer T, Hansmann M, Hackelöer BJ. Endoscopic laser surgery versus serial amniocenteses in the treatment of severe twin-twin transfusion syndrome. Am J Obstet Gynecol. (1999) 180:717–24. doi: 10.1016/s0002-9378(99)70278-4
80. Hecher K, Lewi L, Gratacos E, Huber A, Ville Y, Deprest J. Twin reversed arterial perfusion: fetoscopic laser coagulation of placental anastomoses or the umbilical cord. Ultrasound Obstet Gynecol. (2006) 28:688–91. doi: 10.1002/uog.3816
81. Hedrick HL, Flake AW, Crombleholme TM, Howell LJ, Johnson MP, Wilson RD, et al. Sacrococcygeal teratoma: prenatal assessment, fetal intervention, and outcome. J Pediatr Surg. (2004) 39:430–8. doi: 10.1016/j.jpedsurg.2003.11.005
82. Helfer DC, Clivatti J, Yamashita AM, Moron AF. Anesthesia for ex utero intrapartum treatment (EXIT procedure) in fetus with prenatal diagnosis of oral and cervical malformations: case reports. Rev Bras Anestesiol. (2012) 62:411–23. doi: 10.1016/S0034-7094(12)70141-1
83. Hirose S, Farmer DL, Lee H, Nobuhara KK, Harrison MR. The ex utero intrapartum treatment procedure: looking back at the EXIT. J Pediatr Surg. (2004) 39:375–80. doi: 10.1016/j.jpedsurg.2003.11.011
84. Hofer IS, Mahoney B, Rebarber A, Beilin Y. An ex utero intrapartum treatment procedure in a patient with a family history of malignant hyperthermia. Int J Obstet Anesth. (2013) 22:146–8. doi: 10.1016/j.ijoa.2012.12.009
85. Horzelska EI, Zamlynski M, Horzelski T, Zamlynski J, Pastuszka A, Bablok R, et al. Open fetal surgery for myelomeningocele—is there the learning curve at reduction mother and fetal morbidity? Ginekol Pol. (2020) 91:123–31. doi: 10.5603/GP.2020.0028
86. Howley L, Wood C, Patel SS, Zaretsky M V, Crombleholme T, Cuneo B. Flow patterns in the ductus arteriosus during open fetal myelomeningocele repair. Prenat Diagn. (2015) 35:564–70. doi: 10.1002/pd.4573
87. Ishii K, Murakoshi T, Numata M, Kikuchi A, Takakuwa K, Tanaka K. An experience of laser surgery for feto-fetal transfusion syndrome complicated with unexpected feto-fetal hemorrhage in a case of monochorionic triamniotic triplets. Fetal Diagn Ther. (2006) 21:339–42. doi: 10.1159/000092462
88. Jani JC, Nicolaides KH, Gratacós E, Valencia CM, Doné E, Martinez J-M, et al. Severe diaphragmatic hernia treated by fetal endoscopic tracheal occlusion. Ultrasound Obstet Gynecol. (2009) 34:304–10. doi: 10.1002/uog.6450
89. Jayagobi PA, Chandran S, Sriram B, Chang KTE. Ex-utero intrapartum treatment (EXIT) procedure for giant fetal epignathus. Indian Pediatr. (2015) 52:893–5. doi: 10.1007/s13312-015-0740-9
90. Johnson MD, Birnbach DJ, Burchman C, Greene MF, Datta S, Ostheimer GW. Fetal surgery and general anesthesia: a case report and review. J Clin Anesth. (1989) 1:363–7. doi: 10.1016/0952-8180(89)90077-9
91. Johnson MP, Sutton LN, Rintoul N, Crombleholme TM, Flake AW, Howell LJ, et al. Fetal myelomeningocele repair: short-term clinical outcomes. Am J Obstet Gynecol. (2003) 189:482–7. doi: 10.1067/s0002-9378(03)00295-3
92. Johnson N, Shah PS, Shannon P, Campisi P, Windrim R. A challenging delivery by EXIT procedure of a fetus with a giant cervical teratoma. J Obstet Gynaecol Canada. (2009) 31:267–71. doi: 10.1016/S1701-2163(16)34126-3
93. Johnston R, Shrivastava VK, Chmait RH. Term vaginal delivery following fetoscopic laser photocoagulation of type II vasa previa. Fetal Diagn Ther. (2014) 35:62–4. doi: 10.1159/000355600
94. Kanazawa S, Ozawa K, Muromoto J, Sugibayashi R, Wada Y, Wada S, et al. Risk profiling of the solomon technique versus selective technique of fetoscopic laser surgery for twin-twin transfusion syndrome. Twin Res Hum Genet. (2021) 24:42–8. doi: 10.1017/thg.2020.94
95. Kaneko M, Tokunaga S, Mukai M, Machigashira S, Maki Y, Kodama Y, et al. Application of a fetal scalp electrode for continuous fetal heart rate monitoring during an ex utero intrapartum treatment. J Pediatr Surg. (2011) 46:e37–40. doi: 10.1016/j.jpedsurg.2010.10.026
96. Kohl T, Tchatcheva K, Berg C, Geipel A, Van de Vondel P, Gembruch U. Partial amniotic carbon dioxide insufflation (PACI) facilitates fetoscopic interventions in complicated monochorionic twin pregnancies. Surg Endosc. (2007) 21:1428–33. doi: 10.1007/s00464-006-9183-7
97. Kornacki J, Szydłowski J, Skrzypczak J, Szczepańska M, Rajewski M, Koziołek A, et al. Use of ex utero intrapartum treatment procedure in fetal neck and high airway anomalies—report of four clinical cases. J Matern Neonatal Med. (2019) 32:870–4. doi: 10.1080/14767058.2017.1390740
98. Laje P, Howell LJ, Johnson MP, Hedrick HL, Flake AW, Adzick NS. Perinatal management of congenital oropharyngeal tumors: the ex utero intrapartum treatment (EXIT) approach. J Pediatr Surg. (2013) 48:2005–10. doi: 10.1016/j.jpedsurg.2013.02.031
99. Pedreira DA L, Acacio GL, Gonçalves RT, Sá RAM, Brandt RA, Chmait RH, et al. Percutaneous fetoscopic closure of large open spina bifida using a bilaminar skin substitute. Ultrasound Obstet Gynecol. (2018) 52:458–66. doi: 10.1002/uog.19001
100. Lazar DA, Olutoye OO, Moise KJJ, Ivey RT, Johnson A, Ayres N, et al. Ex-utero intrapartum treatment procedure for giant neck masses–fetal and maternal outcomes. J Pediatr Surg. (2011) 46:817–22. doi: 10.1016/j.jpedsurg.2011.02.006
101. Lee FL, Said N, Grikscheit TC, Shin CE, Llanes A, Chmait RH. Treatment of congenital pulmonary airway malformation induced hydrops fetalis via percutaneous sclerotherapy. Fetal Diagn Ther. (2012) 31:264–8. doi: 10.1159/000336226
102. Li W-F, Chao A-S, Chang S-D, Cheng P-J, Yang L-Y, Chang Y-L. Effects and outcomes of septostomy in twin-to-twin transfusion syndrome after fetoscopic laser therapy. BMC Pregnancy Childbirth. (2019) 19:397. doi: 10.1186/s12884-019-2555-5
103. Liechty KW, Crombleholme TM, Weiner S, Bernick B, Flake AW, Adzick NS. The ex utero intrapartum treatment procedure for a large fetal neck mass in a twin gestation. Obstet Gynecol. (1999) 93:824–5. doi: 10.1016/s0029-7844(98)00374-3
104. Liechty KW, Crombleholme TM, Flake AW, Morgan MA, Kurth CD, Hubbard AM, et al. Intrapartum airway management for giant fetal neck masses: the EXIT (ex utero intrapartum treatment) procedure. Am J Obstet Gynecol. (1997) 177:870–4. doi: 10.1016/s0002-9378(97)70285-0
105. Lombardo ML, Watson-Smith DJ, Muratore CS, Carr SR, O’Brien BM, Luks FI. Laser ablation of placental vessels in twin-to-twin transfusion syndrome: a paradigm for endoscopic fetal surgery. J Laparoendosc Adv Surg Tech A. (2011) 21:869–72. doi: 10.1089/lap.2011.0119
106. Luo D, Wu L, Wu H, Huang W, Huang H. Anesthetic management of a neonate receiving prenatal repair of gastroschisis. Int J Clin Exp Med. (2015) 8:8234–7.26221401
107. Maggio L, Carr SR, Watson-Smith D, O’Brien BM, Lopes V, Muratore CS, et al. Iatrogenic preterm premature rupture of membranes after fetoscopic laser ablative surgery. Fetal Diagn Ther. (2015) 38:29–34. doi: 10.1159/000369250
108. Mallmann MR, Herberg U, Gottschalk I, Strizek B, Hellmund A, Geipel A, et al. Fetal cardiac intervention in critical aortic stenosis with severe mitral regurgitation, severe left atrial enlargement, and restrictive foramen ovale. Fetal Diagn Ther. (2020) 47:440–7. doi: 10.1159/000502840
109. Manrique S, Maiz N, García I, Pascual M, Perera R, Arévalo S, et al. Maternal anaesthesia in open and fetoscopic surgery of foetal open spinal neural tube defects: a retrospective cohort study. Eur J Anaesthesiol. (2019) 36:175–84. doi: 10.1097/EJA.0000000000000930
110. Marsh BJ, Sinskey J, Whitlock EL, Ferschl MB, Rollins MD. Use of remifentanil for open in utero fetal myelomeningocele repair maintains uterine relaxation with reduced volatile anesthetic concentration. Fetal Diagn Ther. (2020) 47:810–6. doi: 10.1159/000509384
111. Mayer S, Till H, Stepan H. EXIT Procedure in a neonate with a prenatally diagnosed granular cell tumor. Pediatr Surg Int. (2010) 26:935–7. doi: 10.1007/s00383-010-2674-6
112. Mawad W, Chaturvedi RR, Ryan G, Jaeggi E. Percutaneous fetal atrial balloon septoplasty for simple transposition of the great arteries with an intact atrial septum. Can J Cardiol. (2018) 34:342.e9–11. doi: 10.1016/j.cjca.2017.12.010
113. Mazzola CA, Albright AL, Sutton LN, Tuite GF, Hamilton RL, Pollack IF. Dermoid inclusion cysts and early spinal cord tethering after fetal surgery for myelomeningocele. N Engl J Med. (2002) 347:256–9. doi: 10.1056/NEJMoa013325
114. Meriki N, Smoleniec J, Challis D, Welsh AW. Immediate outcome of twin-twin transfusion syndrome following selective laser photocoagulation of communicating vessels at the NSW Fetal Therapy Centre. Aust N Z J Obstet Gynaecol. (2010) 50:112–9. doi: 10.1111/j.1479-828X.2009.01127.x
115. Meuli M, Moehrlen U, Flake A, Ochsenbein N, Huesler M, Biro P, et al. Fetal surgery in Zurich: key features of our first open in utero repair of myelomeningocele. Eur J Pediatr Surg. (2013) 23:494–8. doi: 10.1055/s-0032-1329700
116. Middeldorp JM, Sueters M, Lopriore E, Klumper FJCM, Oepkes D, Devlieger R, et al. Fetoscopic laser surgery in 100 pregnancies with severe twin-to-twin transfusion syndrome in the Netherlands. Fetal Diagn Ther. (2007) 22:190–4. doi: 10.1159/000098715
117. Middeldorp JM, Lopriore E, Sueters M, Klumper FJCM, Kanhai HHH, Vandenbussche FPHA, et al. Twin-to-twin transfusion syndrome after 26 weeks of gestation: is there a role for fetoscopic laser surgery? BJOG. (2007) 114:694–8. doi: 10.1111/j.1471-0528.2007.01337.x
118. Migliorelli F, Martínez JM, Gómez O, Bennasar M, Crispi F, García L, et al. Successful fetoscopic surgery to release a complete obstruction of the urethral meatus in a case of congenital megalourethra. Fetal Diagn Ther. (2015) 38:77–80. doi: 10.1159/000365988
119. Miwa I, Sase M, Nakamura Y, Hasegawa K, Kawasaki M, Ueda K. Congenital high airway obstruction syndrome in the breech presentation managed by ex utero intrapartum treatment procedure after intraoperative external cephalic version. J Obstet Gynaecol Res. (2012) 38:854–7. doi: 10.1111/j.1447-0756.2011.01801.x
120. Moldenhauer JS, Soni S, Jatres J, Gebb J, Khalek N, Paidas Teefey C, et al. Open fetal surgical outcomes for myelomeningocele closure stratified by maternal body mass index in a large single-center cohort. Fetal Diagn Ther. (2020) 47:889–93. doi: 10.1159/000511781
121. Moron AF, Barbosa MM, Milani H, Sarmento SG, Santana E, Suriano IC, et al. Perinatal outcomes after open fetal surgery for myelomeningocele repair: a retrospective cohort study. BJOG. (2018) 125:1280–6. doi: 10.1111/1471-0528.15312
122. Murata S, Matsumoto R, Nishimura H, Moriya T, Shimoya K, Sugino N. A case of total hysterectomy due to massive maternal bleeding immediately after fetoscopic laser surgery for twin-twin transfusion syndrome. J Obstet Gynaecol Res. (2021) 47:2215–9. doi: 10.1111/jog.14780
123. Mustafa HJ, Krispin E, Tadbiri H, Espinoza J, Shamshirsaz AA, Nassr AA, et al. Efficacy of long-term indomethacin therapy in prolonging pregnancy after fetoscopic laser surgery for twin-to-twin transfusion syndrome: a collaborative cohort study. BJOG. (2022) 129:597–606. doi: 10.1111/1471-0528.17017
124. Mychaliska GB, Bealer JF, Graf JL, Rosen MA, Adzick NS, Harrison MR. Operating on placental support: the ex utero intrapartum treatment procedure. J Pediatr Surg. (1997) 32:221–7. doi: 10.1016/s0022-3468(97)90184-6
125. Noia G, Riccardi M, Visconti D, Pellegrino M, Quattrocchi T, Tintoni M, et al. Invasive fetal therapies: approach and results in treating fetal ovarian cysts. J Matern Neonatal Med. (2012) 25:299–303. doi: 10.3109/14767058.2011.574300
126. Ogamo M, Sugiyama T, Maeda Y, Kusaka H, Utsunomiya H, Tsubouchi M, et al. The ex utero intrapartum treatment (EXIT) procedure in giant fetal neck masses. Fetal Diagn Ther. (2005) 20:214–8. doi: 10.1159/000083908
127. Olejek A, Horzelska E, Zamłyński J, Horzelski T, Zamłyński M, Nowak L, et al. Alternative hysterotomy technique for the reduction of prenatal complications of intrauterine myelomeningocele repair. Fetal Diagn Ther. (2020) 47:894–901. doi: 10.1159/000510815
128. Oliveira E, Pereira P, Retroz C, Mártires E. Anesthesia for EXIT procedure (ex utero intrapartum treatment) in congenital cervical malformation–a challenge to the anesthesiologist. Brazilian J Anesthesiol. (2015) 65:529–33. doi: 10.1016/j.bjane.2013.07.020
129. Ossowski K, Suskind DL. Airway management in conjoined twins: a rare indication for the EXIT procedure. Arch Otolaryngol Head Neck Surg. (2005) 131:58–60. doi: 10.1001/archotol.131.1.58
130. Pang C, Zhou C, Zhang Z, Li Y, Zhang X, Han F, et al. Fetal pulmonary valvuloplasty in fetuses with right ventricular outflow tract obstructive disease: experience and outcome of the first five cases in China. Pediatr Cardiol. (2021) 42:340–8. doi: 10.1007/s00246-020-02488-8
131. Papanna R, Johnson A, Ivey RT, Olutoye OO, Cass D, Moise KJ. Laparoscopy-assisted fetoscopy for laser surgery in twin-twin transfusion syndrome with anterior placentation. Ultrasound Obstet Gynecol. (2010) 35:65–70. doi: 10.1002/uog.7495
132. Papanna R, Mann LK, Moise KY, Johnson A, Moise KJJ. Absorbable gelatin plug does not prevent iatrogenic preterm premature rupture of membranes after fetoscopic laser surgery for twin-twin transfusion syndrome. Ultrasound Obstet Gynecol. (2013) 42:456–60. doi: 10.1002/uog.12487
133. Paramasivam G, Wimalasundera R, Wiechec M, Zhang E, Saeed F, Kumar S. Radiofrequency ablation for selective reduction in complex monochorionic pregnancies. BJOG. (2010) 117:1294–8. doi: 10.1111/j.1471-0528.2010.02624.x
134. Pedreira DAL, Zanon N, Nishikuni K, Moreira de Sá RA, Acacio GL, Chmait RH, et al. Endoscopic surgery for the antenatal treatment of myelomeningocele: the CECAM trial. Am J Obstet Gynecol. (2016) 214:111.e1–111.e11. doi: 10.1016/j.ajog.2015.09.065
135. Peiró JL, Carreras E, Guillén G, Arévalo S, Sánchez-Durán MA, Higueras T, et al. Therapeutic indications of fetoscopy: a 5-year institutional experience. J Laparoendosc Adv Surg Tech A. (2009) 19:229–36. doi: 10.1089/lap.2007.0149
136. Persico N, Fabietti I, Ciralli F, Gentilino V, D’Ambrosi F, Boito S, et al. Fetoscopic endoluminal tracheal occlusion in fetuses with severe diaphragmatic hernia: a three-year single-center experience. Fetal Diagn Ther. (2017) 41:215–9. doi: 10.1159/000448096
137. Pruthi V, Abbasi N, Ryan G, Drake J, Kulkarni A V, Kwan-Wong T, et al. Fetal surgery for open spina bifida in Canada: initial results. J Obstet Gynaecol Canada. (2021) 43:733–739.e1. doi: 10.1016/j.jogc.2020.10.014
138. Quintero RA, Morales WJ, Phillips J, Kalter CS, Angel JL. In utero lysis of amniotic bands. Ultrasound Obstet Gynecol. (1997) 10:316–20. doi: 10.1046/j.1469-0705.1997.10050316.x
139. Richter J, Wergeland H, DeKoninck P, De Catte L, Deprest JA. Fetoscopic release of an amniotic band with risk of amputation: case report and review of the literature. Fetal Diagn Ther. (2012) 31:134–7. doi: 10.1159/000335026
140. Riddle S, Peiro JL, Lim F-Y, Kingma PS. Complex fetal care cases: fetoscopic myelomeningocele repair. Neoreviews. (2020) 21:e66–71. doi: 10.1542/neo.21-1-e66
141. Rosen MA, Andreae MH, Cameron AG. Nitroglycerin for fetal surgery: fetoscopy and ex utero intrapartum treatment procedure with malignant hyperthermia precautions. Anesth Analg. (2003) 96:698–700. doi: 10.1213/01.ANE.0000049686.20464.3B
142. Rossi AC, Kaufman MA, Bornick PW, Quintero RA. General vs local anesthesia for the percutaneous laser treatment of twin-twin transfusion syndrome. Am J Obstet Gynecol. (2008) 199:137.e1–7. doi: 10.1016/j.ajog.2007.12.008
143. Ruano R, Klinkner DB, Balakrishnan K, Novoa Y, Novoa VA, Davies N, et al. Fetoscopic therapy for severe pulmonary hypoplasia in congenital diaphragmatic hernia: a first in prenatal regenerative medicine at mayo clinic. Mayo Clin Proc. (2018) 93:693–700. doi: 10.1016/j.mayocp.2018.02.026
144. Ruano R, Ibirogba ER, Wyatt MA, Balakrishnan K, Qureshi MY, Kolbe AB, et al. Sequential minimally invasive fetal interventions for two life-threatening conditions: a novel approach. Fetal Diagn Ther. (2021) 48:70–7. doi: 10.1159/000510635
145. Ruano R, Sananes N, Sangi-Haghpeykar H, Hernandez-Ruano S, Moog R, Becmeur F, et al. Fetal intervention for severe lower urinary tract obstruction: a multicenter case-control study comparing fetal cystoscopy with vesicoamniotic shunting. Ultrasound Obstet Gynecol. (2015) 45:452–8. doi: 10.1002/uog.14652
146. Ruano R, Peiro JL, da Silva MM, Campos JADB, Carreras E, Tannuri U, et al. Early fetoscopic tracheal occlusion for extremely severe pulmonary hypoplasia in isolated congenital diaphragmatic hernia: preliminary results. Ultrasound Obstet Gynecol. (2013) 42:70–6. doi: 10.1002/uog.12414
147. Ruano R, Yoshisaki CT, da Silva MM, Ceccon MEJ, Grasi MS, Tannuri U, et al. A randomized controlled trial of fetal endoscopic tracheal occlusion versus postnatal management of severe isolated congenital diaphragmatic hernia. Ultrasound Obstet Gynecol. (2012) 39:20–7. doi: 10.1002/uog.10142
148. Ruano R, Duarte SA, de Almeida Pimenta EJ, Takashi E, da Silva MM, Tannuri U, et al. Comparison between fetal endoscopic tracheal occlusion using a 1.0-mm fetoscope and prenatal expectant management in severe congenital diaphragmatic hernia. Fetal Diagn Ther. (2011) 29:64–70. doi: 10.1159/000311944
149. Rustico MA, Lanna MM, Faiola S, Schena V, Dell’avanzo M, Mantegazza V, et al. Fetal and maternal complications after selective fetoscopic laser surgery for twin-to-twin transfusion syndrome: a single-center experience. Fetal Diagn Ther. (2012) 31:170–8. doi: 10.1159/000336227
150. Said SM, Qureshi MY, Taggart NW, Anderson HN, O’Leary PW, Cetta F, et al. Innovative 2-step management strategy utilizing EXIT procedure for a fetus with hypoplastic left heart syndrome and intact atrial septum. Mayo Clin Proc. (2019) 94:356–61. doi: 10.1016/j.mayocp.2018.08.004
151. Sangaletti M, Garzon S, Raffaelli R, D’Alessandro R, Bosco M, Casarin J, et al. The ex utero intrapartum treatment (EXIT) procedure: case report of a multidisciplinary team approach. Acta Biomed. (2021) 92:e2021142. doi: 10.23750/abm.v92iS1.9964
152. Schmidt S, Hofmann R, Tekesin I, Sierra F, Becker T. Operative fetoscopical management of intrauterine obstructive uropathia by urethral stent. J Perinat Med. (2003) 31:313–6. doi: 10.1515/JPM.2003.044
153. Schwartz DA, Moriarty KP, Tashjian DB, Wool RS, Parker RK, Markenson GR, et al. Anesthetic management of the exit (ex utero intrapartum treatment) procedure. J Clin Anesth. (2001) 13:387–91. doi: 10.1016/s0952-8180(01)00287-2
154. Segura LG, Arendt KW, Sviggum HP, Haider CR, Qureshi MY, Weingarten TN, et al. Spiral electrode for continuous fetal heart rate monitoring during in-utero myelomeningocele repair. Int J Obstet Anesth. (2020) 44:16–9. doi: 10.1016/j.ijoa.2020.06.004
155. Sela HY, Miller R, Abellar RG, Simpson LL. Placental hematoma mimicking twin anemia-polycythemia sequence following selective laser photocoagulation for twin-twin transfusion syndrome. Prenat Diagn. (2014) 34:1123–5. doi: 10.1002/pd.4457
156. Sepulveda W, Wong AE, Dezerega V, Devoto JC, Alcalde JL. Endoscopic laser surgery in severe second-trimester twin-twin transfusion syndrome: a three-year experience from a Latin American center. Prenat Diagn. (2007) 27:1033–8. doi: 10.1002/pd.1829
157. Sepulveda W, Corral E, Alcalde JL, Otayza F, Müller JM, Ravera F, et al. Prenatal repair of spina bifida: a 2-center experience with open intrauterine neurosurgery in Chile. Fetal Diagn Ther. (2020) 47:873–81. doi: 10.1159/000509242
158. Snegovskikh D, Svokos K, Souza D, Renaud E, Carr SR, Kendall MC, et al. Successful anesthesia management of postoperative maternal pulmonary edema and uterine hyperactivity following open fetal myelomeningocele repair. Case Rep Anesthesiol. (2021) 2021:6679845. doi: 10.1155/2021/6679845
159. Soothill PW, Bartha JL, Tizard J. Ultrasound-guided laser treatment for fetal bladder outlet obstruction resulting from ureterocele. Am J Obstet Gynecol. (2003) 188:1107–8. doi: 10.1067/mob.2003.179
160. Stevens GH, Schoot BC, Smets MJW, Kremer B, Manni JJ, Gavilanes AWD, et al. The ex utero intrapartum treatment (EXIT) procedure in fetal neck masses: a case report and review of the literature. Eur J Obstet Gynecol Reprod Biol. (2002) 100:246–50. doi: 10.1016/s0301-2115(01)00467-5
161. Subramanian R, Mishra P, Subramaniam R, Bansal S. Role of anesthesiologist in ex utero intrapartum treatment procedure: a case and review of anesthetic management. J Anaesthesiol Clin Pharmacol. (2018) 34:148–54. doi: 10.4103/joacp.JOACP_239_16
162. Suenaga M, Hidaka N, Kido S, Otera Y, Fukushima K, Kato K. Successful ex utero intrapartum treatment procedure for prenatally diagnosed severe micrognathia: a case report. J Obstet Gynaecol Res. (2014) 40:2005–9. doi: 10.1111/jog.12423
163. Suh E, Quintessenza J, Huhta J, Quintero R. How to grow a heart: fibreoptic guided fetal aortic valvotomy. Cardiol Young. (2006) 16(Suppl 1):43–6. doi: 10.1017/S1047951105002313
164. Takano M, Nakata M, Ishii K, Wada S, Sumie M, Yamamoto R, et al. Outcomes of fetoscopic laser surgery for twin-to-twin transfusion syndrome between 26 and 27 weeks of gestation in Japan. J Obstet Gynaecol Res. (2021) 47:3821–7. doi: 10.1111/jog.14922
165. Tonni G, Grisolia G, Zampriolo P, Prefumo F, Fichera A, Bonasoni P, et al. TRAP Sequence in monochorionic/monoamniotic (MC/MA) discordant twins: two cases treated with fetoscopic laser surgery. Fetal Pediatr Pathol. (2018) 37:433–47. doi: 10.1080/15513815.2018.1526240
166. Tulipan N, Bruner JP. Myelomeningocele repair in utero: a report of three cases. Pediatr Neurosurg. (1998) 28:177–80. doi: 10.1159/000028645
167. Valsky DV, Eixarch E, Martinez-Crespo JM, Acosta E-R, Lewi L, Deprest J, et al. Fetoscopic laser surgery for twin-to-twin transfusion syndrome after 26 weeks of gestation. Fetal Diagn Ther. (2012) 31:30–4. doi: 10.1159/000330369
168. Ville Y, Hyett J, Hecher K, Nicolaides K. Preliminary experience with endoscopic laser surgery for severe twin-twin transfusion syndrome. N Engl J Med. (1995) 332:224–7. doi: 10.1056/NEJM199501263320404
169. Ville Y, Hyett JA, Vandenbussche FPHA, Nicolaides KH. Endoscopic laser coagulation of umbilical cord vessels in twin reversed arterial perfusion sequence. Ultrasound Obstet Gynecol. (1994) 4:396–8. doi: 10.1046/j.1469-0705.1994.04050396.x
170. Vinit N, Gueneuc A, Bessières B, Dreux S, Heidet L, Salomon R, et al. Fetal cystoscopy and vesicoamniotic shunting in lower urinary tract obstruction: long-term outcome and current technical limitations. Fetal Diagn Ther. (2020) 47:74–83. doi: 10.1159/000500569
171. Volochovič J, Vaigauskaitė B, Varnelis P, Kosinski P, Wielgos M. Intrauterine fetoscopic closure of myelomeningocele: clinical case and literature review. Taiwan J Obstet Gynecol. (2021) 60:766–70. doi: 10.1016/j.tjog.2021.05.032
172. Wilson RD, Johnson MP, Crombleholme TM, Flake AW, Hedrick HL, King M, et al. Chorioamniotic membrane separation following open fetal surgery: pregnancy outcome. Fetal Diagn Ther. (2003) 18:314–20. doi: 10.1159/000071972
173. Wohlmuth C, Tulzer G, Arzt W, Gitter R, Wertaschnigg D. Maternal aspects of fetal cardiac intervention. Ultrasound Obstet Gynecol. (2014) 44:532–7. doi: 10.1002/uog.13438
174. Yamamoto M, El Murr L, Robyr R, Leleu F, Takahashi Y, Ville Y. Incidence and impact of perioperative complications in 175 fetoscopy-guided laser coagulations of chorionic plate anastomoses in fetofetal transfusion syndrome before 26 weeks of gestation. Am J Obstet Gynecol. (2005) 193:1110–6. doi: 10.1016/j.ajog.2005.07.003
175. Yonemoto H, Itoh S, Nakamura Y, Yoshida K, Kinoshita K. Hemodynamic evaluation of a prenatal thoracoamniotic shunt for fetal pleural effusion. Early Hum Dev. (2006) 82:411–4. doi: 10.1016/j.earlhumdev.2005.10.017
176. Zambelli H, Barini R, Iscaife A, Cursino K, de Braga AFA, Marba S, et al. Successful developmental outcome in intrauterine myelomeningocele repair. Child’s Nerv Syst. (2007) 23:123–6. doi: 10.1007/s00381-006-0169-5
177. Zamłyński M, Zamłyński J, Horzelska E, Maruniak-Chudek I, Bablok R, Szukiewicz D, et al. The use of indomethacin with complete amniotic fluid replacement and classic hysterotomy for the reduction of perinatal complications of intrauterine myelomeningocele repair. Fetal Diagn Ther. (2019) 46:415–24. doi: 10.1159/000496811
178. Ziemann M, Fimmers R, Khaleeva A, Schürg R, Weigand MA, Kohl T. Partial amniotic carbon dioxide insufflation (PACI) during minimally invasive fetoscopic interventions on fetuses with spina bifida aperta. Surg Endosc. (2018) 32:3138–48. doi: 10.1007/s00464-018-6029-z
179. Mellor DJ, Diesch TJ, Gunn AJ, Bennet L. The importance of “awareness” for understanding fetal pain. Brain Res Brain Res Rev. (2005) 49:455–71. doi: 10.1016/j.brainresrev.2005.01.006
180. Bellieni C V, Vannuccini S, Petraglia F. Is fetal analgesia necessary during prenatal surgery? J Matern Neonatal Med. (2018) 31:1241–5. doi: 10.1080/14767058.2017.1311860
181. Bellieni C V, Tei M, Stazzoni G, Bertrando S, Cornacchione S, Buonocore G. Use of fetal analgesia during prenatal surgery. J Matern Neonatal Med (2013) 26:90–5. doi: 10.3109/14767058.2012.718392
182. Van de Velde M, Jani J, De Buck F, Deprest J. Fetal pain perception and pain management. Semin Fetal Neonatal Med. (2006) 11:232–6. doi: 10.1016/j.siny.2006.02.012
183. Vutskits L, Davidson A. Update on developmental anesthesia neurotoxicity. Curr Opin Anaesthesiol. (2017) 30:337–42. doi: 10.1097/ACO.0000000000000461
184. Chinn GA, Sasaki Russell JM, Sall JW. Is a short anesthetic exposure in children safe? Time will tell: a focused commentary of the GAS and PANDA trials. Ann Transl Med. (2016) 4:408. doi: 10.21037/atm.2016.10.43
185. Van de Velde M, Van Schoubroeck D, Lewi LE, Marcus MAE, Jani JC, Missant C, et al. Remifentanil for fetal immobilization and maternal sedation during fetoscopic surgery: a randomized, double-blind comparison with diazepam. Anesth Analg. (2005) 101:251–8. doi: 10.1213/01.ANE.0000156566.62182.AB
186. Ring LE, Ginosar Y. Anesthesia for fetal surgery and fetal procedures. Clin Perinatol. (2019) 46:801–16. doi: 10.1016/j.clp.2019.08.011
187. Chatterjee D, Arendt KW, Moldenhauer JS, Olutoye OA, Parikh JM, Tran KM, et al. Anesthesia for maternal-fetal interventions: a consensus statement from the American society of anesthesiologists committees on obstetric and pediatric anesthesiology and the North American fetal therapy network. Anesth Analg. (2021) 132:1164–73. doi: 10.1213/ANE.0000000000005177
Keywords: fetal surgery, perinatal outcome, fetal analgesia, maternal-fetal anesthesia, fetal pain
Citation: Duci M, Pulvirenti R, Fascetti Leon F, Capolupo I, Veronese P, Gamba P and Tognon C (2022) Anesthesia for fetal operative procedures: A systematic review. Front. Pain Res. 3:935427. doi: 10.3389/fpain.2022.935427
Received: 3 May 2022; Accepted: 24 August 2022;
Published: 12 September 2022.
Edited by:
Maria Antonieta Flores Muñoz, General Hospital of Mexico, MexicoReviewed by:
Chimaobi Nnaji, Federal Medical Centre, NigeriaCaridad Velazquez Cardona, Grey’s Hospital, South Africa
© 2022 Duci, Pulvirenti, Fascetti Leon, Capolupo, Veronese, Gamba and Tognon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Fascetti Leon francesco.fascettileon@unipd.it
†ORCID Miriam Duci orcid.org/0000-0003-1382-3527 Rebecca Pulvirenti orcid.org/0000-0003-0558-9806 Francesco Fascetti Leon orcid.org/0000-0002-7175-3013 Irma Capolupo orcid.org/0000-0002-3090-2887 Paola Veronese orcid.org/0000-0003-2907-1040 Piergiorgio Gamba orcid.org/0000-0003-2068-342X
‡These authors have contributed equally to this work and share first authorship.
Specialty Section: This article was submitted to Pediatric Pain, a section of the journal Frontiers in Pain Research