 Wei-Hsin Lu1†
Wei-Hsin Lu1† Cheng-Fang Yen
Cheng-Fang Yen- 1Department of Psychiatry, Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chia-Yi City, Taiwan
- 2Department of Child and Adolescent Psychiatry, Chang Gung Memorial Hospital, Kaohsiung Medical Center and College of Medicine, Chang Gung University, Kaohsiung, Taiwan
- 3Department of Psychiatry and Behavioral Sciences, University of Washington School of Medicine, Seattle, WA, United States
- 4Department of Psychiatry, Children’s Hospital and Regional Medical Center, Seattle, WA, United States
- 5Department of Psychiatry, Tainan Municipal Hospital (Managed by Show Chwan Medical Care Corporation), Tainan, Taiwan
- 6Department of Psychiatry, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
- 7Department of Psychiatry, School of Medicine, and Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan
Background: Deviations in reinforcement sensitivity and frustration-related reactions have been proposed as components of the biopsychosocial mechanisms, which explained the high vulnerability to internet addiction (IA) among individuals with attention-deficit/hyperactivity disorder (ADHD). There is currently limited knowledge on the relationship of IA symptoms with reinforcement sensitivity and frustration intolerance, as well as factors moderating those correlations in this population.
Objective: The aims of this study were (1) to examine the associations of IA symptoms severity with reinforcement sensitivity and frustration intolerance and (2) identify the moderators of these associations among adolescents diagnosed with ADHD in Taiwan.
Methods: A total of 300 adolescents aged between 11 and 18 years who had been diagnosed with ADHD participated in this study. Their levels of IA severity, reinforcement sensitivity, and frustration intolerance were assessed using the Chen Internet Addiction Scale, behavioral inhibition system (BIS) and behavioral approach system (BAS), and Frustration Discomfort Scale, respectively. The associations of IA severity with reinforcement sensitivity and frustration intolerance were examined using multiple regression analysis. Possible moderators, including medications for ADHD, were tested using the standard criteria.
Results: Higher fun seeking on the BAS (p = .003) and higher frustration intolerance (p = .003) were associated with more severe IA symptoms. Receiving medication for treating ADHD moderated the association between fun seeking on the BAS and severity of IA symptoms.
Conclusion: Fun seeking on the BAS and frustration intolerance should be considered as targets in prevention and intervention programs for IA among adolescents with ADHD.
Introduction
The negative effects of internet addiction (IA) have become a concern in the past decades. IA is characterized by persistent internet use despite negative consequences, loss of control, preoccupation with internet use, increasing amounts of time spent online, and withdrawal symptoms (1). Internet gaming disorders are listed in the “Conditions for Further Study” section in the Fifth Edition of Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (2). Adolescents were raised in an era in which the internet rapidly expanded its influence in daily life.
Attention-deficit/hyperactivity disorder (ADHD) is the most common comorbidity among adolescents referred for treatment of IA (3). Relevant studies have consistently reported associations between IA and ADHD. One study reported that 14% of adults with IA have also been diagnosed with ADHD (4). Individuals with IA have a 2.5 times higher risk of being diagnosed with ADHD according to a meta-analysis (5). Ko et al. (6) discovered that during a 2-year follow-up period, adolescents with significant ADHD symptoms were more likely to develop IA than were those without. Moreover, ADHD symptoms, including inattention and impulsivity/hyperactivity, were more severe in individuals with IA than in healthy controls (5). Evidence suggests that the relationship between ADHD and IA is likely to be bidirectional and mutually interactive. For example, although a 3-year follow-up study reported that children and adolescents with more severe attention problems spent more time playing video games during follow-up (7), a 2-year prospective study discovered that heavy digital media users without ADHD symptoms at baseline had a higher risk of developing ADHD symptoms during the follow-up period (8).
Ko et al. (9) proposed possible biopsychosocial mechanisms to explain the high correlation between ADHD and IA, including avoidance of boredom and delayed reward, striatal dopamine release, compensation for real-life frustrations, impaired inhibition, and deviation in reinforcement sensitivity. Reinforcement sensitivity and frustration may play important roles among these mechanisms. Firstly, patients with ADHD were reported to have deviations in responses to reinforcements, such as rapid habituation to repeated rewards and decreased responses to punishments, which may predispose these individuals to IA because internet activities often provide quick rewards and responses (10). Secondly, adolescents with ADHD often encounter various frustrations in their daily life because of their symptoms. Striatal dopamine release during video gaming (11) may enhance the performance of the game players, thereby helping adolescents with ADHD to compensate for real-life frustrations. In addition, impulsivity, inattention and hyperactivity usually produce frustrations in an interpersonal relationship; therefore, individuals with ADHD may rely more on the internet because it is easier to establish interpersonal relationships online than that in real world. In this view, IA may be a consequence of poor tolerance to frustrations. Recognizing these possible factors which contribute to the strong association between ADHD and IA is crucial to prevention and providing interventions for IA in adolescents with ADHD. However, previous reseaches supporting these proposed mechanisms are still limited. To the best of our knowledge, only one study examined the predictors of IA symptoms in adolescents clinically diagnosed with ADHD (12). Hence, in this study, we focused on the roles of reinforcement sensitivity and frustration intolerance to address these knowledge gaps.
Reinforcement Sensitivity Theory (RST) was developed by Gray and consists of the behavioral inhibition system (BIS) and behavioral approach system (BAS), which are used to identify an individual’s sensitivity to punishment and reward, respectively (13). BAS and BIS can provide explanations for impulsivity and anxiety, respectively (14). Although Gray revised his theory in 2000, making some adjustments to account for the complexity of the constitution and interaction of RST systems (15), many prominent studies have utilized the older RST model (14). Most research on the role of RST in IA has also used the older RST model (12, 16–20). To maintain consistent methodology, we also used the original RST model in this study. Cross-sectional and prospective research on adolescents and adults has identified associations between reinforcement sensitivity and IA symptoms. Specifically, high BAS fun seeking and high BIS have been demonstrated to be positively correlated with the severity of IA in cross-sectional studies (17, 21). A 1-year follow-up study revealed that individuals with higher total BAS and BAS fun seeking were more likely to develop IA (18).
Internet activities are usually characterized by immediate responses and rapid rewards; therefore, deviations in sensitivity to reinforcement may contribute to vulnerability to IA in patients with ADHD (9). Abnormal reinforcement sensitivity is considered a fundamental characteristic of ADHD (10, 22, 23). Research has indicated that patients with ADHD have higher reward sensitivity to immediate reinforcements (24), more rapid habituation to repeated reinforcements (25), and lower response to punishment (25, 26). Impulsivity, a prominent symptom of ADHD, is commonly reported in individuals with IA (19, 27), and it has been linked to BAS functioning (28). Studies on subjects with ADHD have also reported that higher BAS fun seeking, BAS drive, and BIS are positively associated with IA symptoms (12, 19). However, few studies have been conducted on patients clinically diagnosed with ADHD, and more information is required to support the role of reinforcement sensitivity in patients with ADHD. Moreover, evidence suggests that the effects of reinforcement sensitivity vary under different conditions. Research has found that increased age and low parental occupational SES were significantly associated with severe internet addiction symptoms in adolescents with ADHD (12). Family factors have been reported to moderate the association between reinforcement sensitivity and behavioral problems in children and adolescents (29). Adolescents receiving medication for ADHD exhibited problematic online gaming symptoms and concurrent decreases in BAS and BIS scores (20). Moreover, reinforcement sensitivity was reported to be a vulnerable factor of psychiatric disorders, such as depression, anxiety, and substance abuse (30). However, no study has explored the moderating effects of socio-demographic characteristics, medical treatment for adolescents with ADHD, and concurrent psychiatric disorders on the association between IA symptoms and reinforcement sensitivity in adolescents with ADHD.
Frustration intolerance refers to the difficulty accepting that reality does not correspond to personal desires (31). It is a type of irrational belief related to emotional and behavioral problems based on the theory of rational emotive behavior therapy (32). Adolescents with IA have been reported to have higher frustration intolerance that healthy controls (21), indicating that frustration intolerance is associated with difficulty with self-control (33). Aversion to delayed reward, which may be a source of frustration, is a core feature of ADHD (22). Researchers have observed high frustration intolerance in youths with ADHD (34–36). Hypothesizing that frustration intolerance is a predictor of IA symptoms in individuals with ADHD is therefore reasonable. Nevertheless, no study has examined the relationship between frustration intolerance and IA symptoms in adolescents with ADHD. Considering the high risk of IA in adolescents with ADHD, understanding the role of frustration intolerance in predicting IA may facilitate the design of effective cognitive behavioral therapies targeting ADHD adolescents with IA. Furthermore, sex is currently the only factor that has been proven to moderate the correlation between frustration intolerance and IA in adolescents (21). In the present study, we investigated whether socio-demographic characteristics, medical treatment for adolescents with ADHD, and concurrent psychiatric disorders moderate this relationship between frustration intolerance and IA symptoms in adolescents with ADHD.
The aims of the present study were to examine the correlations between IA severity and reinforcement sensitivity and frustration intolerance as well as identify moderators of these correlations in adolescents in Taiwan who have been diagnosed with ADHD. We hypothesized that both reinforcement sensitivity and frustration intolerance exhibit significant correlations with IA severity, and that these correlations may be moderated by sociodemographic characteristics, ADHD symptoms and treatment, psychiatric comorbidities, and parental factors.
Materials and Methods
Participants
Participants for this study were recruited from the child and adolescent psychiatric outpatient clinics of two medical centers in Kaohsiung, Taiwan. Adolescents aged between 11 and 18 years, who visited the outpatient clinics and have been diagnosed with ADHD according to the diagnostic criteria specified in the DSM-5 (2), were consecutively invited to participate in this study during the period from August 2013 to July 2015. ADHD was diagnosed on the basis of multiple data sources, including (i) an interview with a child psychiatrist; (ii) clinical observation of the participant’s behavior; and (iii) medical history provided by parents and parent-reported severity of ADHD symptoms assessed from the short version of Swanson, Nolan, and Pelham, Version IV Scale (SNAP-IV)-Chinese version (37, 38). Adolescents with intellectual disabilities, schizophrenia, bipolar disorder, autistic disorder, communication difficulties, or cognitive deficits that adversely affect their ability to understand the study purpose or complete the questionnaires were excluded. A total of 333 adolescents who had been diagnosed with ADHD and their parents were selected for this study, 300 of which (90.0%) agreed to participate in this study and were interviewed by research assistants through a questionnaire. Of the 33 adolescents who refused to join this study, 19 refused because of their parents’ opinions and 14 refused because of their own opinions. The Institutional Review Boards of Kaohsiung Medical University and Chang Gung Memorial Hospital, Kaohsiung Medical Center, approved the study. Written informed consent was obtained from all participants before assessment.
Measures
Internet addiction. We used the Chen Internet Addiction Scale (CIAS) to assess participant self-reported severity of IA symptoms in the recent 1 month. The CIAS contains 26 items evaluated on a 4-point Likert scale, with scores ranging from 26 to 104 (39); a higher total score indicates more severe IA symptoms. The CIAS has been commonly used to assess internet addiction among children and adolescents in Taiwan (1, 40). The internal reliability (Cronbach’s α) of the CIAS was .94 in the present study.
Reinforcement sensitivity. The Chinese version of BIS and BAS scales contain 20 items evaluated on a 4-point Likert scale; these scales assess participants’ self-reported sensitivity for the two motivational systems according to RST (13, 28, 41). The BIS measures the degree to which respondents expect to feel anxiety when confronted with cues for punishment. The BAS includes subscales of reward responsiveness, drive, and fun seeking, which measure the degree to which rewards lead to positive emotions, an individual’s tendency to actively pursue goals, and the tendency to seek out and impulsively engage in potentially rewarding activities, respectively. A higher total score on the subscale indicates a higher level of reinforcement sensitivity. The Chinese versions of BIS and BAS scales were translated from the original version using the standard forward-, backward-, and pretest-step method and have been reported to have good criterion and construct validity in the previous study on Taiwanese population (41). The BIS and BAS scales have been used to assess reinforcement sensitivity among adolescents in Taiwan (12). The Cronbach’s α of the four subscales ranged from .68 to .83 in the present study.
Frustration intolerance. In the present study, the Chinese version of Frustration Discomfort Scale (FDS) was used to evaluate the self-reported frustration intolerance belief of participants (21, 42). The FDS contains 28 items evaluated on a 5-point Likert scale, with scores ranging from 28 to 140; a higher total score indicates higher frustration intolerance beliefs. The Chinese versions of FDS scales was translated from the original version using the standard forward-, backward-, and pretest-step method and have been used to evaluate frustration intolerance beliefs in Taiwanese adolescents (21). The Cronbach’s alpha of the FDS was.90 in the present study.
ADHD symptoms and treatment. In the present study, the short version of SNAP-IV-Chinese version was used to assess the parent-reported severity of ADHD symptoms for adolescents in the recent 1 month. This short version of SNAP-IV-Chinese version is a 26-item rating instrument that includes the core Fourth Edition of DSM (DSM-IV)-derived ADHD subscales of inattention, hyperactivity/impulsivity, and symptoms of oppositional defiant disorder with good criterion and construct validity (37, 38). Each item was rated on a 4-point Likert scale from 0 (not at all) to 3 (very much). In this study, the total scores for the inattention and hyperactivity/impulsivity subscales were used for analysis. The Cronbach’s α of these two subscales was .86 and .88, respectively. Whether the participants received medication for ADHD was determined based on parent reports and participant medical records.
Psychiatric comorbidities. The depressive disorders, anxiety disorders, tic disorders, and autism spectrum disorders (ASDs) of participants were assessed based on the clinical interviews and chart reviews by three child psychiatrists. Those who had been diagnosed with any ASD and low intelligence (defined as a score less than 70 on the Chinese version of the Fourth Edition of the Wechsler Intelligence Scale for Children [43]) or those who had communication difficulties were not invited to participate in this study. For the purpose of analysis, psychiatric diagnoses were categorized as depressive or anxiety disorders, tic disorders, and ASDs.
Parental factors. The present study evaluated the marital status of the parents of participants (married and living together vs. divorced or separated) and assessed their occupational socioeconomic status (SES) using Close-Ended Questionnaire of the Occupational Survey (CEQ-OS) (44). Parents choose their occupations from 14 categories in the CEQ-OS, which were further classified into five levels according to their occupational socioeconomic status. A higher level indicates higher occupational socioeconomic status. The CEQ-OS has been proven to possess excellent reliability and validity and has been commonly used in studies on children and adolescents in Taiwan (44). In the present study, levels I, II, and III of the CEQ-OS were classified as low occupational SES, whereas levels IV and V were classified as high occupational SES. This questionnaire was completed by parents.
Procedure
The research assistants conducted interviews using the CIAS, BIS/BAS, and FDS to collect data from adolescents. Their parents completed SNAP-IV under the direction of the research assistants. Data analysis was performed using SPSS 20.0 statistical software (SPSS Inc., Chicago, IL, USA).
Statistical Analysis
Because that there were several factors examined in this study, we used two-step statistical analyses to examine the correlation of IA severity with reinforcement sensitivity and frustration intolerance and reduced the possibility of multiple comparison. In the first step, we used Pearson’s correlation and t test to select possible factors predicting IA severity for further analysis, including sociodemographic characteristics, ADHD symptoms and treatment, psychiatric comorbidities, parental factors, reinforcement sensitivity, and frustration intolerance. The significant factors in the first step were used in the second step, which consisted of a multiple regression analysis that was used to evaluate the correlations of reinforcement sensitivity and frustration intolerance with IA severity by controlling for the effects of other factors. A two-tailed p value of less than 0.05 was considered statistically significant.
We also used standard criteria (45) to examine whether the associations of reinforcement sensitivity and frustration intolerance with IA severity differed in terms of sociodemographic characteristics, ADHD symptoms and treatment, psychiatric comorbidities, or parental factors. According to the criteria, moderation occurred when the interaction term for the predictor (reinforcement sensitivity and frustration intolerance) and the hypothesized moderator were significantly associated with the dependent variable (IA severity) in multiple regression analysis after controlling for the main effects of both the predictors and hypothesized moderator variables. In this study, if reinforcement sensitivity, frustration intolerance, and hypothesized moderators were significantly associated with IA symptoms, then the interactions (reinforcement sensitivity or frustration intolerance × hypothesized moderators) were further selected for multiple regression analysis to examine the moderating effects.
Results
Sociodemographic Characteristics and Correlates of IA Symptoms
Table 1 presents the sociodemographic and ADHD characteristics, comorbidities, IA severity, and BAS/BIS and FDS scores of participants. Table 2 lists the correlations of IA severity with age, ADHD symptoms, BIS/BAS and FDS scores, as examined using Pearson’s correlation. According to Cohen (46), older age, more severe inattention and oppositional symptoms, higher score for fun seeking on the BAS, and higher frustration intolerance belief on the FDS were weakly but significantly correlated with more severe IA symptoms. Figure 1 shows the scatter plots of the correlations between IA symptoms and fun seeking on the BAS and between IA symptoms and FDS score.
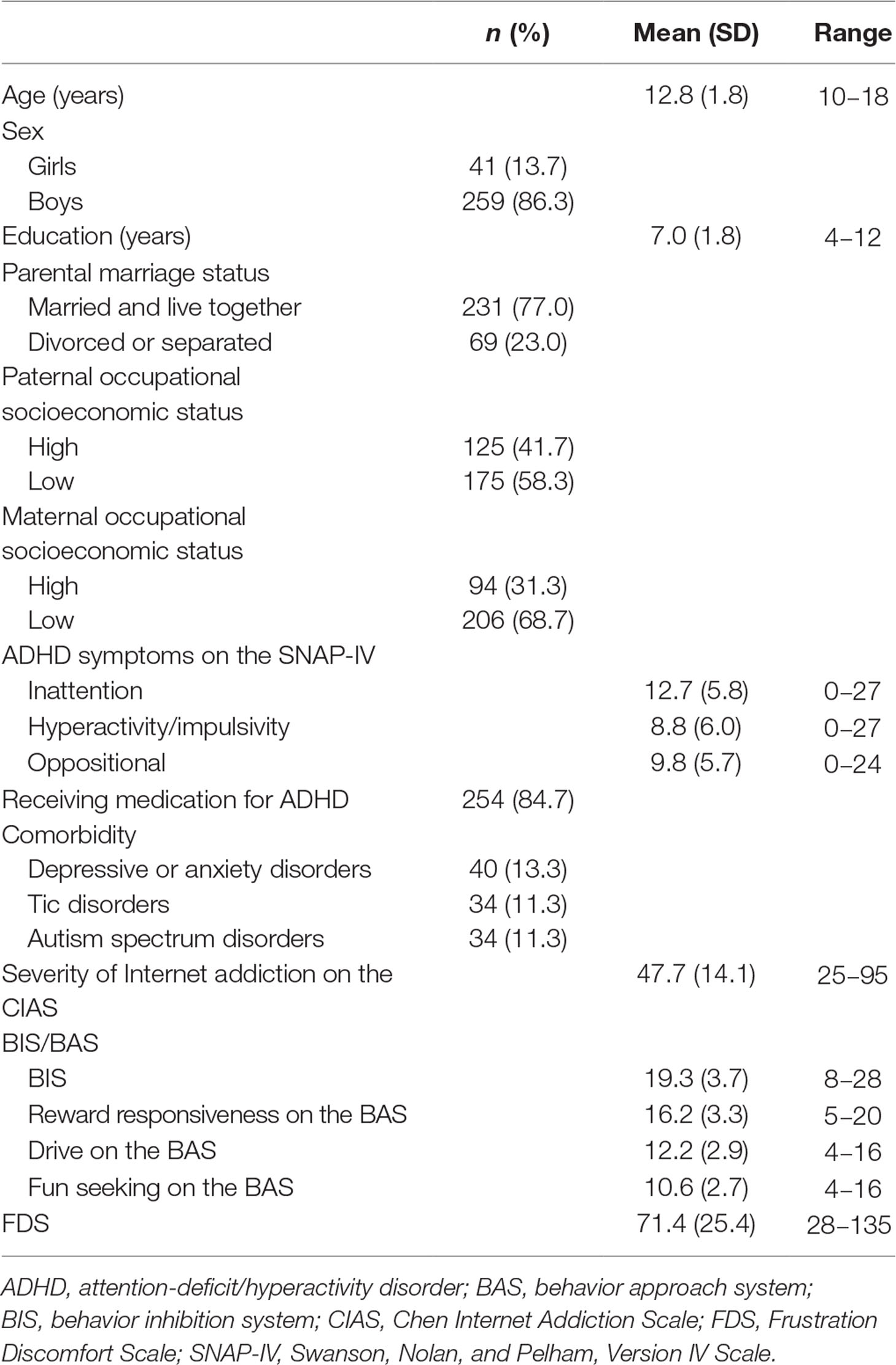
Table 1 Sociodemographic and ADHD characteristics, comorbidities, internet addiction severity, and levels of BAS/BIS and FDS (N = 300).
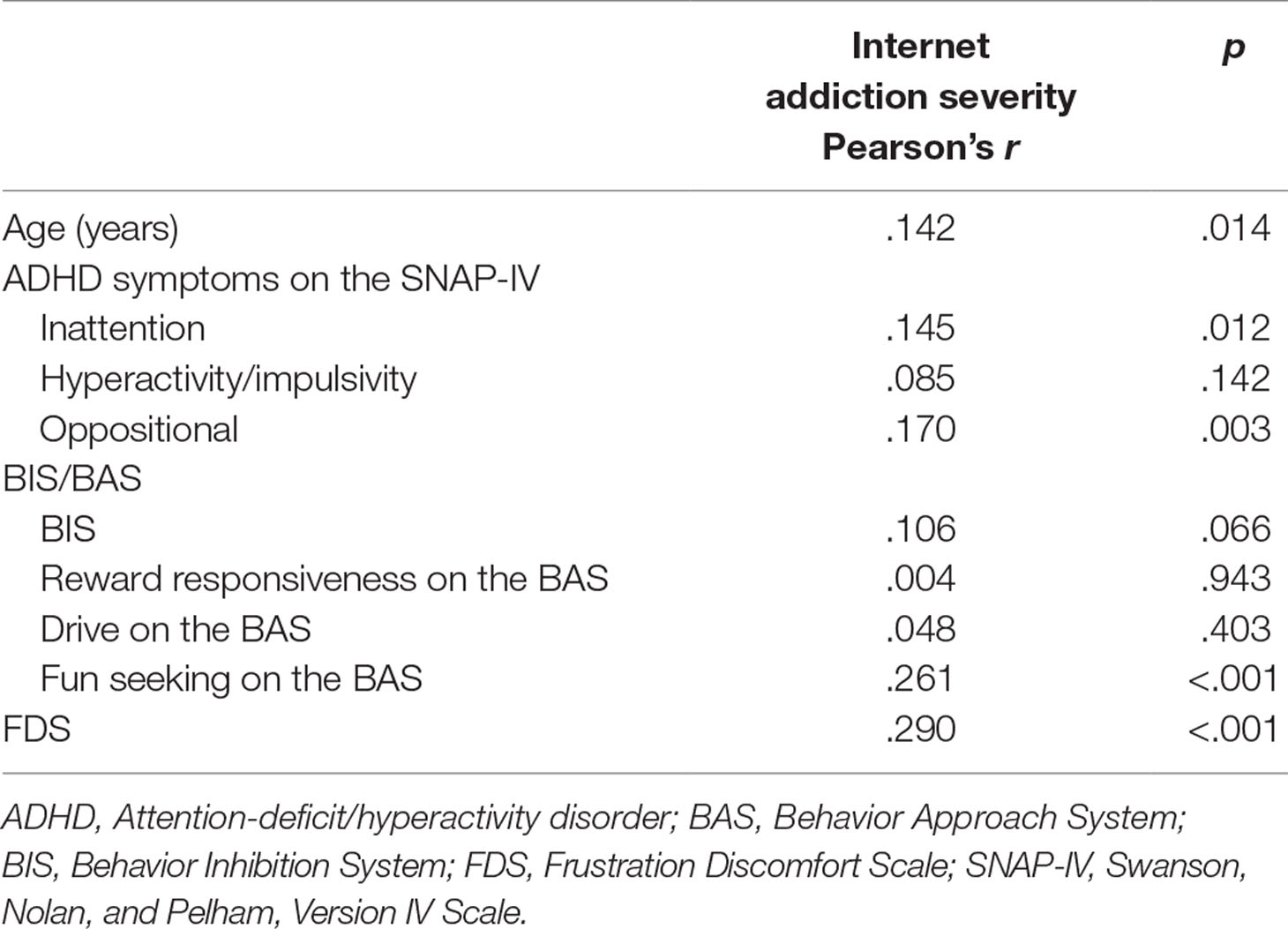
Table 2 Correlation of age, ADHD symptoms, BIS/BAS, and FDS with internet addiction severity: Pearson’s correlation.
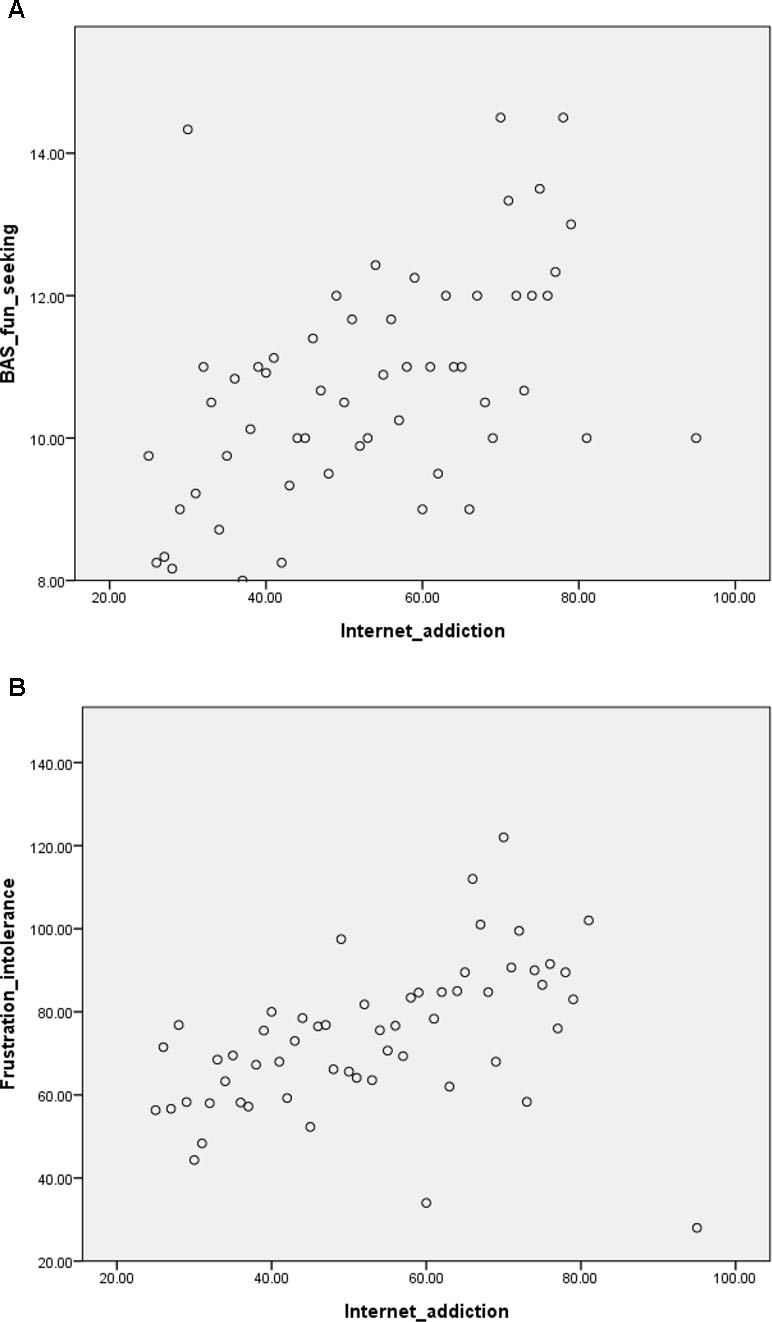
Figure 1 Scatter plots of correlations between internet addiction symptoms and fun seeking on the Behavioral Approach System (BAS) scale (Figure 1A) and between internet addiction symptoms and frustration intolerance (Figure 1B).
Table 3 presents the differences in IA severity between participants with various sociodemographic characteristics, medication status, and psychiatric comorbidities. The results indicated that adolescents with low paternal and maternal occupational SES exhibited more severe IA symptoms than did those with high paternal and maternal occupational SES. Adolescents receiving medication for ADHD had less severe IA symptoms than did those not receiving medication for ADHD.
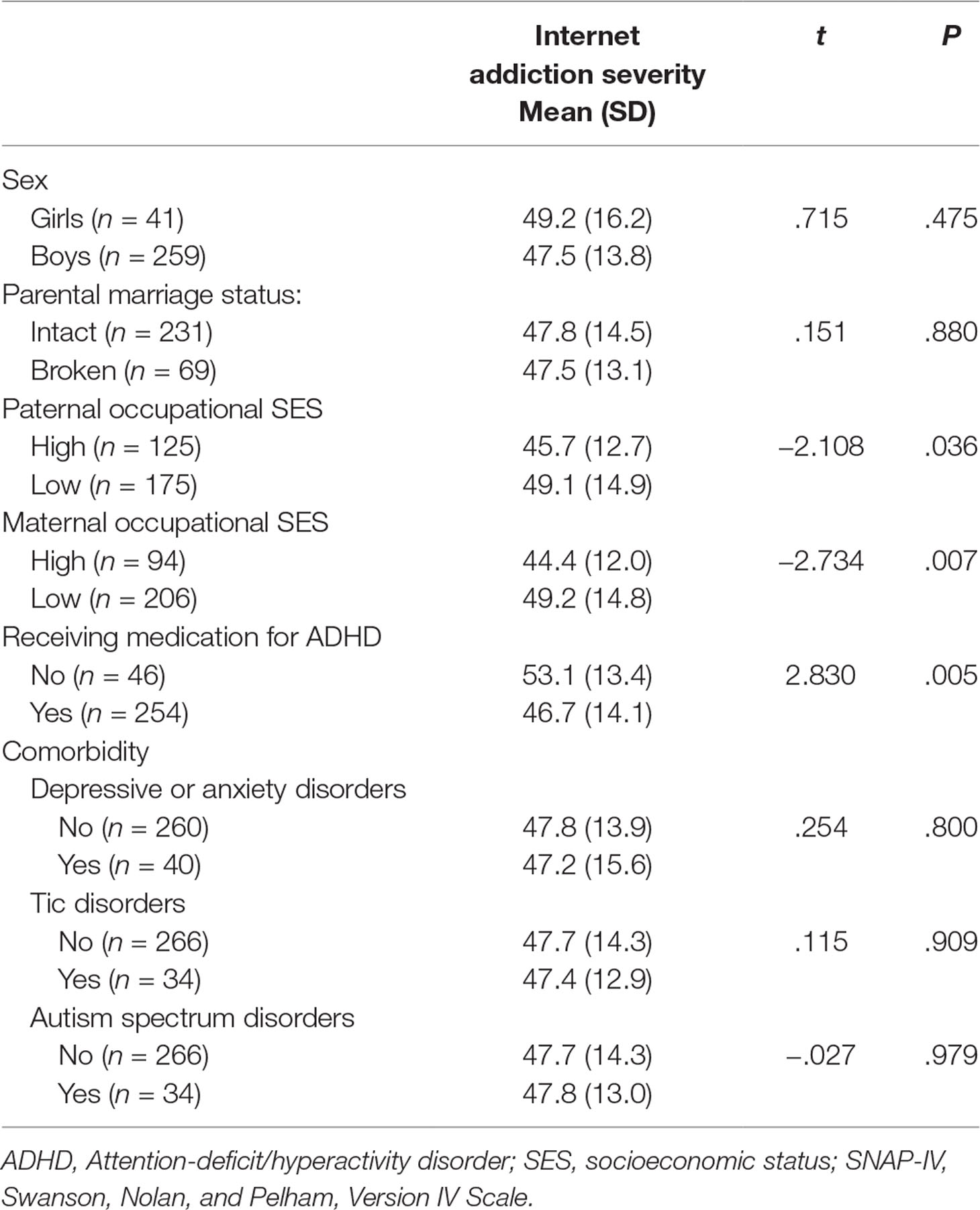
Table 3 Comparison of internet addiction severity of participants according to sociodemographic characteristics, ADHD characteristics, and comorbidities.
Testing of Moderators
As described in the Statistical analysis section, significant factors in the first step were selected for further multiple regression analysis in the second step to detect the independent factors related to IA symptoms (Model I in Table 4). The results indicated that low maternal occupational SES, higher fun seeking on the BAS, and higher frustration intolerance belief on the FDS were associated with more severe IA symptoms, whereas receiving medication for ADHD was associated with less severe IA.
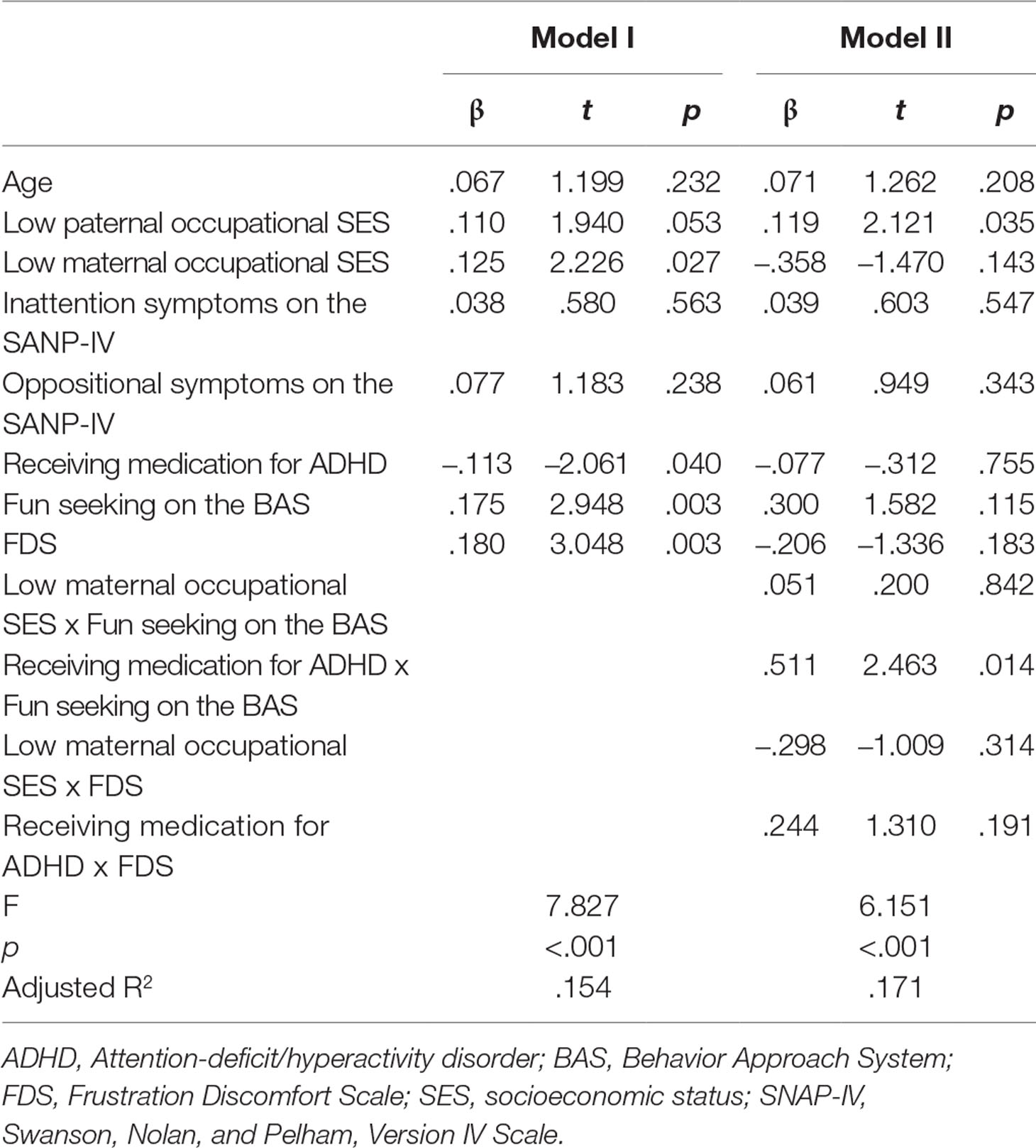
Table 4 Associated factors and moderators of internet addiction severity.
Because maternal occupational SES and receiving medication for ADHD were significantly associated with IA symptoms, the interactions among the predictors (reinforcement sensitivity and frustration intolerance) and possible moderators (maternal occupational SES and receiving medication for ADHD) were included in the multiple regression analysis based on the standard criteria proposed by Baron and Kenny (45) described in the Statistical analysis section (Model II in Table 4). The results indicated that the interaction between fun seeking on the BAS and receiving medication for ADHD was significantly associated with IA severity, suggesting that receiving medication for ADHD moderated the association between fun seeking on the BAS and IA severity. The results of further analysis revealed a significant association between fun seeking on the BAS and IA severity only in participants receiving medication for ADHD (β = .154, t = 2.301, p = .022) and not in those not receiving medication for ADHD (β = .291, t = 2.004, p = .052).
Discussion
The results of this study revealed that although both BAS fun seeking and frustration intolerance were positively associated with IA symptoms, medication treatment for ADHD moderated the relationship between fun seeking on the BAS and IA severity. To the best of our knowledge, this is the first study to identify the moderators of correlations of IA symptoms with reinforcement sensitivity and frustration intolerance in adolescents with ADHD.
BAS fun seeking represents the tendency to seek stimuli and response to proximal rewards (47). Internet use provides individuals with activities having various modes of stimulation and rapid rewards; therefore, individuals with high BAS scores may be more likely to develop IA. A bidirectional relationship remains possible, as indicated in a longitudinal study (18). The present study discovered that the association between BAS fun seeking and IA severity is significant only in adolescents receiving medication for ADHD. This finding is different from the results of other studies, which have concluded significant associations of BAS fun seeking and IA severity in adolescents or young adults (16–18) and adolescents with ADHD (12). The results of our study may indicate that the effects of RST subsystems on IA severity are complex and interactive. Gray’s revised version of the RST includes the subsystems of the BAS, Fight/Flight/Freeze System (FFFS), and BIS (14, 15). BAS controls approach behavior, and FFFS controls avoidance behavior to aversive stimuli. Both BAS and FFFS are activated during an event that includes both rewarding and aversive stimuli, resulting in a motivational conflict. BIS is then activated by the motivational conflict, and the ongoing behavior is inhibited while directing the individual’s attention to the source of conflict (14). Although internet use produces immediate rewards and relief from boredom, it also frequently results in negative consequences that may lead to motivational conflict. Therefore, IA symptoms may be influenced by the result of these mixed interactions of RST subsystems. Moreover, BAS functioning is considered to be based on dopaminergic systems in the CNS (48), which has also been the primary focus of hypotheses on ADHD etiology (49, 50). Deviation in the dopaminergic process may be a mechanism underlying the difference in association between BAS fun seeking and IA in adolescents with ADHD with and without medication. Dopaminergic and noradrenergic neurotransmission are targets of the most commonly used ADHD medications (i.e. methylphenidate and atomoxetine) in Taiwan. One study discovered that 3 months of methylphenidate and atomoxetine treatment in adolescents with ADHD was associated with a decreased score on the BAS scale (20). ADHD medications may modulate the dopaminergic and noradrenergic systems in the brain and thus affect the relationship between BAS fun seeking and IA severity. The association between BAS fun seeking and IA in general adolescents from the general population and those treated with medication for ADHD, but not in ADHD adolescents without medication, may reflect the normalizing effect of ADHD medications on reinforcement sensitivity. This renders the association between BAS fun seeking and IA in adolescents with ADHD who take medication as more similar to that in adolescents from the general population. However, other possible explanations include differences between medication-treated and medication-free groups in terms of baseline demographic or symptom characteristics. The causal relationship of the effects of ADHD medication on the association between BAS fun seeking and IA severity requires further clarification by prospective studies.
In the present study, frustration tolerance was demonstrated to be a significant predictor of IA severity after controlling for other correlates in the regression model. The theory underlying rational emotive behavior therapy proposes that irrational beliefs triggered by events lead to subsequent negative consequences (51). Conversely, Ko et al. suggested that early internet exposure may lead adolescents to become accustomed to environments with immediate gratification, and they may have a limited ability to tolerate frustrations, prompting the development of the irrational belief of frustration intolerance (21). Individuals with ADHD may experience a great deal of frustration in daily life because of deficits in attention and executive function. After thoughts characteristic of frustration intolerance have been provoked, internet activities may serve as coping strategies for tension relief. The results of this study suggest that the frustration intolerance belief requires adequate evaluation and intervention when managing or preventing IA in adolescents with ADHD.
The current study discovered that lower maternal SES was associated with higher IA severity in adolescents with ADHD. Family SES has been proven to play a pivotal role in adolescent health conditions, and parental SES has been demonstrated to influence depression, obesity, and self-rated health among adolescents in the US (52). Children and adolescents from families with higher SES tend to exhibit healthier behaviors (53). Moreover, parenting is crucial to managing ADHD symptoms, and parents with higher SES may be more likely to have access to ADHD-related psychoeducational information. Additionally, parents with higher SES may have more knowledge on appropriate internet use, and therefore, may be more likely to monitor their children. In traditional Taiwanese families, mothers more commonly manage home routines and primarily serve as child caretakers. Therefore, the responsibility of monitoring and controlling internet use may be more commonly taken up by mothers in Taiwan. However, because the concept of gender equality has evolved alongside the increasing prevalence of double-income households in Taiwan, parental influence on IA still warrants careful consideration. One study reported that parental SES predicts IA severity in adolescents with ADHD, but maternal SES does not (12). Overall, evidence supports the phenomenon that parental SES is a critical correlate of IA in adolescents with ADHD.
Established treatment modality for IA is lacking. Medications that have been studied included escitalopram, bupropion, methylphenidate, and atomoxetine (54). Methylphenidate and atomoxetine were reported to be associated with decreased severity of online gaming and BAS/BIS scores in adolescents with ADHD (20). The results of this study support the need for further investigation on the role of ADHD medications in treatment for adolescents with ADHD. Cognitive behavioral therapy is the major non-pharmacological intervention for IA among previous studies (54). Our study indicates that future research may examine the efficacy of incorporating management of frustration intolerance belief and the tendency of fun seeking in cognitive behavioral interventions in treating patients with ADHD and IA. Moreover, the effect of ADHD medications on both fun seeking and IA severity should be monitored during such interventions.
Several limitations of this study require careful consideration. Measurements were all self-reported; therefore, common method bias cannot be completely ruled out. Adding clinical interview in the evaluation process will improve the diagnostic validity in future studies. Psychometrics of the Chinese versions of BIS-BAS scale and FDS used in the adolescent population warrant further examination. The cross-sectional design limited the capability of forming conclusions regarding causality. Participants were recruited from outpatient departments, and individuals with ADHD who were not receiving clinical care were not approached, meaning that the results may not be generalizable to all adolescents with ADHD. Medications for treating ADHD were not specified in our study; therefore, variety in the effects of medications may have introduced bias into the results. However, methylphenidate and atomoxetine are the only two compounds that have been approved for treating ADHD in Taiwan and comprise almost all medications used for treating ADHD (55, 56). Last but not least, the types of internet activities were not reported in this study. There have been debates on whether different problematic online behaviors, such as interent gaming, online social networking and online shopping should be viewed as one single entity or different distinct behaviors driven by various gratifications (57). Whether differences exist among correlations of various internet activities with reinforcement sensitivity and frustration intolerance requires further study. It is also recommended in further research to apply a prospective design, as well as examine the effects of various ADHD medications.
Conclusion
The results of the current study indicated that BAS fun seeking and frustration intolerance belief were significantly associated with IA severity in adolescents with ADHD. Differences were observed in the association between BAS fun seeking and IA between participants receiving ADHD medication and those not receiving ADHD medication. Reward sensitivity and frustration intolerance require attention during prevention and management programs for IA in adolescents with ADHD. The effect of ADHD medication should also be considered when evaluating the relationship between reinforcement sensitivity and IA.
Ethics Statement
This study was carried out in accordance with the recommendations of Kaohsiung Medical University with written informed consent from all subjects. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the Kaohsiung Medical University.
Author Contributions
W-HL: conception and design of the study, drafting the manuscript. W-JC: conception and design of the study, drafting the manuscript. RH: drafting the manuscript. H-FH: acquisition and analysis of data. C-FY: conception and design of the study, acquisition and analysis of data, drafting the manuscript or figures.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgment
This study was supported by a grant from Chang Gung Memorial Hospital Medical Research Project, 102-CMRPG8C0881 and 103-CMRPG8D1281, grant MOST 105-2314-B-182A-055, and 105-2314-B-037 -025-MY3 from the Ministry of Science and Technology, Taiwan, ROC, and grant KMUH105-M507 awarded by Kaohsiung Medical University Hospital. The funding agencies did not play a role in this study.
References
1. Ko C-H, Yen J-Y, Chen C, Chen S-H, Yen C-F. Proposed diagnostic criteria of internet addiction for adolescents. J Nerv Ment Dis (2005) 193:728–33. doi: 10.1097/01.nmd.0000185891.13719.54
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Publishing (2013).
3. Bozkurt H, Coskun M, Ayaydin H, Adak İ., Zoroglu SS. Prevalence and patterns of psychiatric disorders in referred adolescents with internet addiction. Psychiatry Clin Neurosci (2013) 67:352–9. doi: 10.1111/pcn.12065
4. Bernardi S, Pallanti S. Internet addiction: a descriptive clinical study focusing on comorbidities and dissociative symptoms. Compr Psychiatry (2009) 50:510–6. doi: 10.1016/j.comppsych.2008.11.011
5. Wang B-Q, Yao N-Q, Zhou X, Liu J, Lv Z-T. The association between attention deficit/hyperactivity disorder and internet addiction: a systematic review and meta-analysis. BMC Psychiatry (2017a) 17:260. doi: 10.1186/s12888-017-1408-x
6. Ko CH, Yen JY, Chen CS, Yeh YC, Yen CF. Predictive values of psychiatric symptoms for internet addiction in adolescents: a 2-year prospective study. Arch Pediatr Adolesc Med (2009) 163:937–43. doi: 10.1001/archpediatrics.2009.159
7. Gentile DA, Swing EL, Lim CG, Khoo A. Video game playing, attention problems, and impulsiveness: evidence of bidirectional causality. Psychol Popular Media Cult (2012) 1:62–70. doi: 10.1037/a0026969
8. Ra CK, Cho J, Stone MD, De La Cerda J, Goldenson NI, Moroney E, et al. Association of digital media use with subsequent symptoms of attention-deficit/hyperactivity disorder among adolescents. JAMA (2018) 320:255–63. doi: 10.1001/jama.2018.8931
9. Ko CH, Yen JY, Yen CF, Chen CS, Chen CC. The association between Internet addiction and psychiatric disorder: a review of the literature. Eur Psychiatry (2012) 27:1–8. doi: 10.1016/j.eurpsy.2010.04.011
10. Berger A, Kofman O, Livneh U, Henik A. Multidisciplinary perspectives on attention and the development of self-regulation. Prog Neurobiol (2007) 82:256–86. doi: 10.1016/j.pneurobio.2007.06.004
11. Koepp MJ, Gunn RN, Lawrence AD, Cunningham VJ, Dagher A, Jones T, et al. Evidence for striatal dopamine release during a video game. Nature (1998) 393:266–8. doi: 10.1038/30498
12. Chou W-J, Liu T-L, Yang P, Yen C-F, Hu H-F. Multi-dimensional correlates of Internet addiction symptoms in adolescents with attention-deficit/hyperactivity disorder. Psychiatry Res (2015) 225:122–8. doi: 10.1016/j.psychres.2014.11.003
13. Gray JA. The neuropsychology of temperament. In: Explorations in temperament: international perspectives on theory and measurement. New York, NY: Plenum Press (1991). p. 105–28. doi: 10.1007/978-1-4899-0643-4_8
14. Smillie LD, Pickering AD, Jackson CJ. The new reinforcement sensitivity theory: implications for personality measurement. Pers Soc Psychol Rev (2006) 10:320–35. doi: 10.1207/s15327957pspr1004_3
15. Gray JA, Mcnaughton N. The Neuropsychology of Anxiety: an Enquiry Into the Function of the Septo-hippocampal System. Oxford, England: Oxford University Press (2000).
16. Ko CH, Yen J-Y, Yen CF, Chen CS, Weng CC, Chen CC. The association between internet addiction and problematic alcohol use in adolescents: the problem behavior model. Cyberpsychol Behav (2008) 11:571–6. doi: 10.1089/cpb.2007.0199
17. Yen JY, Ko CH, Yen CF, Chen CS, Chen CC. The association between harmful alcohol use and Internet addiction among college students: comparison of personality. Psychiatry Clin Neurosci (2009) 63:218–24. doi: 10.1111/j.1440-1819.2009.01943.x
18. Yen JY, Cheng-Fang Y, Chen CS, Chang YH, Yeh YC, Ko CH. The bidirectional interactions between addiction, behaviour approach and behaviour inhibition systems among adolescents in a prospective study. Psychiatry Res (2012) 200:588–92. doi: 10.1016/j.psychres.2012.03.015
19. Li W, Zhang W, Xiao L, Nie J. The association of Internet addiction symptoms with impulsiveness, loneliness, novelty seeking and behavioral inhibition system among adults with attention-deficit/hyperactivity disorder (ADHD). Psychiatry Res (2016) 243:357–64. doi: 10.1016/j.psychres.2016.02.020
20. Park JH, Lee YS, Sohn JH, Han DH. Effectiveness of atomoxetine and methylphenidate for problematic online gaming in adolescents with attention deficit hyperactivity disorder. Hum Psychopharmacol (2016) 31:427–32. doi: 10.1002/hup.2559
21. Ko CH, Yen JY, Yen CF, Chen CS, Wang SY. The association between Internet addiction and belief of frustration intolerance: the gender difference. Cyberpsychol Behav (2008) 11:273–78. doi: 10.1089/cpb.2007.0095
22. Castellanos FX, Tannock R. Neuroscience of attention-deficit/hyperactivity disorder: the search for endophenotypes. Nat Rev Neurosci (2002) 3:617–28. doi: 10.1038/nrn896
23. Nigg JT. Neuropsychologic theory and findings in attention-deficit/hyperactivity disorder: the state of the field and salient challenges for the coming decade. Biol Psychiatry (2005) 57:1424–35. doi: 10.1016/j.biopsych.2004.11.011
24. Tripp G, Alsop B. Sensitivity to reward frequency in boys with attention deficit hyperactivity disorder. J Clin Child Psychol (1999) 28:366–75. doi: 10.1207/S15374424jccp280309
25. Iaboni F, Douglas VI, Ditto B. Psychophysiological response of ADHD children to reward and extinction. Psychophysiology (1997) 34:116–23. doi: 10.1111/j.1469-8986.1997.tb02422.x
26. Toplak ME, Jain U, Tannock R. Executive and motivational processes in adolescents with Attention-Deficit-Hyperactivity Disorder (ADHD). Behav Brain Funct (2005) 1:8–8. doi: 10.1186/1744-9081-1-8
27. Mihajlov M, Vejmelka L. Internet addiction: a review of the first twenty years. Psychiatr Danub (2017) 29:260–72. doi: 10.24869/psyd.2017.260
28. Carver CS, White TL. Behavioral inhibition, behavioral activation, and affective responses to impending reward and punishment: the BIS/BAS Scales. J Pers Soc Psychol (1994) 67:319–33. doi: 10.1037/0022-3514.67.2.319
29. Kuznetsova VB. Family factors as moderators of link between reinforcement sensitivity and child and adolescent problem behaviour. Personal Ment Health (2015) 9:44–57. doi: 10.1002/pmh.1280
30. Johnson SL, Turner RJ, Iwata N. BIS/BAS levels and psychiatric disorder: an epidemiological study. J Psychopathol Behav Assess (2003) 25:25–36. doi: 10.1023/A:1022247919288
31. Harrington N. Frustration intolerance beliefs: their relationship with depression, anxiety, and anger, in a clinical population. Cogn Ther Res (2006) 30:699–709. doi: 10.1007/s10608-006-9061-6
32. Digiuseppe RA, Doyle KA, Dryden W, Backx W. A practitioner’s guide to rational-emotive behavior therapy. New York, NY: Oxford University Press (2015).
33. Harrington N. Dimensions of frustration intolerance and their relationship to self-control problems. J Ration Emot Cogn Behav Ther (2005a) 23:1–20. doi: 10.1007/s10942-005-0001-2
34. Walcott CM, Landau S. The relation between disinhibition and emotion regulation in boys with attention deficit hyperactivity disorder. J Clin Child Adolesc Psychol (2004) 33:772–82. doi: 10.1207/s15374424jccp3304_12
35. Scime M, Norvilitis JM. Task performance and response to frustration in children with attention deficit hyperactivity disorder. Psychol Sch (2006) 43:377–86. doi: 10.1002/pits.20151
36. Seymour KE, Macatee R, Chronis-Tuscano A. Frustration tolerance in youth with ADHD. J Atten Disord (2016). doi: 10.1177/1087054716653216 [Epub ahead of print]
37. Swanson JM, Kraemer HC, Hinshaw SP, Arnold LE, Conners CK, Abikoff HB, et al. Clinical relevance of the primary findings of the MTA: success rates based on severity of ADHD and ODD symptoms at the end of treatment. J Am Acad Child Adolesc Psychiatry (2001) 40:168–79. doi: 10.1097/00004583-200102000-00011
38. Gau SS, Shang CY, Liu SK, Lin CH, Swanson JM, Liu YC, et al. Psychometric properties of the Chinese version of the Swanson, Nolan, and Pelham, version IV scale - parent form. Int J Methods Psychiatr Res (2008) 17:35–44. doi: 10.1002/mpr.237
39. Chen S-H, Weng L-J, Su Y-J, Wu H-M, Yang P-F. Development of a Chinese internet addiction scale and its psychometric study. Chin J Psychol (2003) 45:279–94. doi: 10.1037/t44491-000
40. Chen Y-L, Gau SS. Sleep problems and internet addiction among children and adolescents: a longitudinal study. J Sleep Res (2016) 25:458–65. doi: 10.1111/jsr.12388
41. Chen C-H, Ko H-C, Lu R-B. Behavioral inhibition and activation systems: male alcoholic patients with and without anxiety disorders. Taiwan J Psychiatry (2005) 19:119–27. doi: 10.29478/TJP.200506.0005
42. Harrington N. The frustration discomfort scale: development and psychometric properties. Clin Psychol Psychother (2005b) 12:374–87. doi: 10.1002/cpp.465
43. Wechsler D. Wechsler Intelligence Scale for Children. 4th ed. The Chinese Behavioral Science Corporation (2007).
44. Hwang Y-J. An analysis of the reliability and validity of the close-ended questionnaire of the occupational survey in the educational research. Bull Educ Res (2005) 51:43–71.
45. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol (1986) 51:1173–82. doi: 10.1037/0022-3514.51.6.1173
46. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New York, NY: Lawrence Erlbaum Associates (1988).
47. Corr PJ. Reinforcement Sensitivity Theory (RST): Introduction. In: The reinforcement sensitivity theory of personality. New York, NY: Cambridge University Press (2008). p. 1–43. doi: 10.1017/CBO9780511819384.002
48. Reuter M, Schmitz A, Corr P, Hennig J. Molecular genetics support Gray’s personality theory: the interaction of COMT and DRD2 polymorphisms predicts the behavioural approach system. Int J Neuropsychopharmacol (2006) 9:155–66. doi: 10.1017/S1461145705005419
49. Kirley A, Hawi Z, Daly G, Mccarron M, Mullins C, Millar N, et al. Dopaminergic system genes in ADHD: toward a biological hypothesis. Neuropsychopharmacology (2002) 27:607–19. doi: 10.1016/S0893-133X(02)00315-9
50. Bush G, Valera EM, Seidman LJ. Functional neuroimaging of attention-deficit/hyperactivity disorder: a review and suggested future directions. Biol Psychiatry (2005) 57:1273–84. doi: 10.1016/j.biopsych.2005.01.034
51. Ellis A, Dryden W. The practice of rational-emotive therapy (RET). New York, NY, US: Springer Publishing Co. (1987).
52. Goodman E. The role of socioeconomic status gradients in explaining differences in US adolescents’ health. Am J Public Health (1999) 89:1522–28. doi: 10.2105/AJPH.89.10.1522
53. Moore GF, Littlecott HJ. School- and family-level socioeconomic status and health behaviors: multilevel analysis of a national survey in wales, United Kingdom. J Sch Health (2015) 85:267–75. doi: 10.1111/josh.12242
54. Zajac K, Ginley MK, Chang R, Petry NM. Treatments for Internet gaming disorder and Internet addiction: a systematic review. Psychol Addict Behav (2017) 31:979–94.
55. Wang LJ, Yang KC, Lee SY, Yang CJ, Huang TS, Lee TL, et al. Initiation and persistence of pharmacotherapy for youths with attention deficit hyperactivity disorder in Taiwan. PLoS One (2016) 11:e0161061. doi: 10.1371/journal.pone.0161061
56. Wang LJ, Lee SY, Yuan SS, Yang CJ, Yang KC, Huang TS, et al. Prevalence rates of youths diagnosed with and medicated for ADHD in a nationwide survey in Taiwan from 2000 to 2011. Epidemiol Psychiatr Sci (2017b) 26:624–34. doi: 10.1017/S2045796016000500
Keywords: adolescent, attention-deficit/hyperactivity disorder, internet addiction, reinforcement sensitivity, behavior approach system, behavioral inhibition system, frustration intolerance
Citation: Lu W-H, Chou W-J, Hsiao RC, Hu H-F and Yen C-F (2019) Correlations of Internet Addiction Severity With Reinforcement Sensitivity and Frustration Intolerance in Adolescents With Attention-Deficit/Hyperactivity Disorder: The Moderating Effect of Medications. Front. Psychiatry 10:268. doi: 10.3389/fpsyt.2019.00268
Received: 11 December 2018; Accepted: 08 April 2019;
Published: 26 April 2019.
Edited by:
Takahiro A. Kato, Kyushu University, JapanReviewed by:
Wan-Sen Yan, Guizhou Medical University (GMU), ChinaTomohiro Shirasaka, Teine Keijinkai Hospital, Japan
Copyright © 2019 Lu, Chou, Hsiao, Hu and Yen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cheng-Fang Yen chfaye@cc.kmu.edu.tw
Huei-Fan Hu cych07205@gmail.com
†These authors have contributed equally to this work.