 Sylvia Böhme
Sylvia Böhme Babette Renneberg
Babette Renneberg- Department of Psychology, Freie Universität Berlin, Berlin, Germany
Purpose: Self-rated health (SRH) is a powerful predictor of health-related outcomes such as morbidity and mortality. Aim of the current study was to examine the role of comorbidity, well-being, functional health, and physical limitations as possible predictors of SRH in diabetes and chronic heart failure (CHF).
Methods: Three large samples with persons suffering from diabetes (n = 974), CHF (n = 955), or both diseases combined (n = 934) were analyzed longitudinally over the course of 4 months. To test the mediating effect of comorbidity, well-being, functional health, and physical limitations in association with former and future SRH multiple mediator models were applied.
Results: Across all groups emotional well-being was a consistent and powerful determinant of SRH. The effects of functional health and physical limitations on SRH were also significant but varied between diagnostic groups. The number of comorbid diseases did not predict SRH.
Conclusion: Emotional well-being and physical health appraisal were strong predictors of SRH. Thus, SRH may be improved by influencing well-being and physical health appraisal via targeted interventions.
Introduction
The importance of self-rated health (SRH) for various health-related outcomes such as morbidity and mortality is well documented (1, 2). SRH is defined as “a summary statement about the way in which numerous aspects of health, both subjective and objective, are combined within the perceptual framework of the individual respondent” [(3), p. 93]. The importance of SRH was demonstrated initially by Mossey and Shapiro who reported that it was a strong predictor of mortality, especially in the elderly, and even after controlling for potential confounding variables (4). Since then SRH has frequently been shown to predict various health-related outcomes (5–11).
The association between SRH and key outcomes like morbidity and mortality has not been clarified, yet. More information about SRH is required to explain its effect on morbidity and mortality. As SRH cannot be improved directly the determinants are our only means to indirectly affect the important measure of SRH. In order to improve SRH, we have to understand, which variables affect SRH to what extent and how these mechanisms differ for example between different diseases. The knowledge of how people rate their health and the health aspects involved may lead to intervention strategies to improve (self-rated) health. Short definitions of the key constructs for the following analyses are displayed in Figure 1.
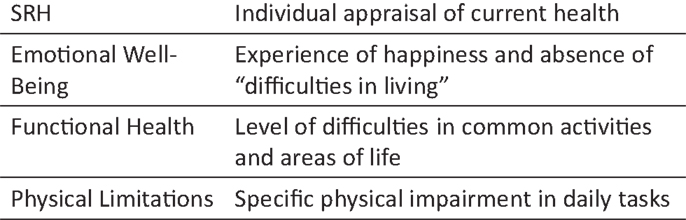
Figure 1. Short definition of key constructs.
Health- and lifestyle-related determinants of SRH have been addressed in a few studies [e.g., see Ref. (12–18)]. In order to understand the concept of SRH the influencing role of functional health might be particularly important. A recent study showed the key role of functional health status for SRH especially in the elderly (19). Functional health is often used synonymously with health-related quality of life as both concepts describe the functional ability to perform daily tasks. This ability might be reduced due to symptoms of a disease and the corresponding physical limitations. The emotional consequences of functional limitations (such as pain, depression, or anxiety) are related to the concept of functional health as well. Emotional well-being is considered to be another important predictor of SRH. It is often also referred to as psychological or mental well-being and reflects the subjective experience of happiness (20). Emotional well-being has been shown to be positively associated with SRH especially in the elderly (21). In a large meta-analysis emotional well-being was identified as a significant determinant of physical health (22). Perrucio et al. (2012) reported that it is not medical comorbidity alone that contributes to health perceptions but different aspects of functional and mental health (14). Steinhauser et al. compared health-related factors between three life-limiting diseases [cancer, chronic heart failure (CHF), and chronic obstructive pulmonary disease (COPD)]. They showed that functional limitation was more dependent on the specific disease than on the individual, whereas the other health-related factors did not differ between diseases but between subjects (18). Hence, the severity of functional limitations differentiates between diseases when other health-related factors are comparable. Nutzel et al. (23) confirmed the importance of disease-dependent health appraisal for multimorbid patients. They showed that the specific consequences of diseases in terms of limited functional ability and well-being were associated with SRH. Furthermore, Schuez et al. (13) concluded in their study that predictors of SRH varied depending on individual physical health: with increasing number of diseases the association of SRH with functional health increased. Thus, functional limitations and well-being are key concepts in understanding individual health appraisal especially in chronically ill individuals.
Consequently, in order to understand and possibly change SRH, it is crucial to identify and explain the factors that have an impact on it. Research findings so far suggest that people base their SRH on different aspects of health that depend on the individual appraisal. Thus, SRH might not directly depend on comorbidity but on specific appraisal that may be associated with comorbidity.
These associations have not yet been investigated within a larger sample of multimorbid individuals. Thus, in the current study the effects of health appraisal and comorbidity on SRH are analyzed longitudinally in three large multimorbid samples of persons with diabetes, CHF, or both diseases combined.
Hypotheses
We expect former SRH to be the strongest predictor of future SRH. Additionally, future SRH is also predicted by a number of variables that reflect health appraisal such as general well-being, functional health, and physical limitations (hypothesis 1). Further, within the association of former and future SRH, the number of comorbid diseases has no additional mediating effect when measures of health appraisal are included into the model (hypothesis 2).
Materials and Methods
Participants and Procedure
From a pool of insurants of a German health insurance company (Techniker Krankenkasse), a sample of individuals suffering from diabetes, CHF, or both conditions [double diagnosis (DD)] was randomly selected and asked to answer self-report questionnaires regarding their health. The data collection was conducted and ethically approved by the insurance company. The participants did not participate in any intervention over the course of the data collection. The questionnaires were sent by mail to the participants by the insurance company. Individuals who did not suffer from dementia or severe mental diseases and provided written informed consent were included in the study. The already processed and de-identified data were transmitted to the authors and analyzed according to a pre-assigned study-protocol. At the two assessment points, T1 (baseline) and T2 (after four months), participants were asked to evaluate their SRH, general well-being, functional health as well as their physical limitations. During the 4 months, they continued to receive their usual medical treatment. Of initially, n = 3706 persons (n = 1240 with diabetes, n = 1229 with CHF, n = 1237 with DD) a subsample of n = 2863 (77.25%) participants returned both questionnaires at time 1 and time 2 [n = 974 (78.50%) with diabetes; n = 955 (77.71%) with CHF; n = 934 (77.51%) with DD]. Current analyses are based on these samples.
Table 1 presents the sociodemographic characteristics of the three groups. On average participants were 67.9 years old, the proportion of male participants was high (about 80%). All individuals in our study were suffering from chronic diseases that imposed a great burden on their lives. On average they had 4.9 comorbid diseases (like COPD, cancer, arthritis or coronary heart disease). Their SRH, emotional well-being, functional health, and physical limitations were in medium range and did not change significantly during assessment time.
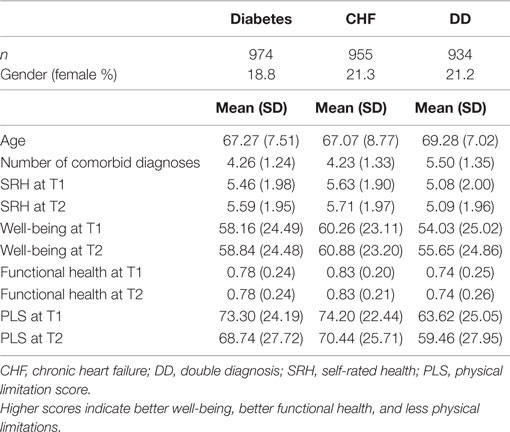
Table 1. Sample description.
Measures
Self-rated health, emotional well-being, functional health, and physical limitations were assessed at T1 (baseline) and T2 (4 months later) by questionnaires. Diagnoses, age, and gender were derived from insurance data at baseline.
Self-rated health was assessed using a well-established single-item measure [e.g. see Ref. (7, 24)]. Participants were asked to estimate their SRH on a scale ranging from 0 to 10. The exact wording of the single-item measure was: “If you were to rate your general state of health on a scale from 0 to 10 – (“0” meaning “couldn’t be worse” and “10” meaning “couldn’t be better”) – how would you rate your current state of health?” Research results and psychometric properties concerning this specific measure are described elsewhere (25, 26).
Functional Health and Physical Limitations
Functional Health
The EQ-5D questionnaire was used to assess functional health (27). Based on the five subscales, mobility, anxiety/depression, usual activities, pain/discomfort, and self-care and the level of difficulties were summarized in global scores, which were computed according to the EQ-5D value sets (28). For Germany, global scores range between −0.207 and 1, where −0.207 indicates “severe problems on all dimensions” and a score of 1 indicates “no problems on any dimension.” Hence, larger scores indicate a better functional health. Several studies [e.g., see Ref. (29–31)] evaluated psychometric characteristics of the EQ-5D in various samples and different diseases and found moderate to high retest-reliability scores (k = 0.67–0.85). Also, construct (29–31) and criterion validity (30) of the EQ-5D were consistently good. All authors conclude that the EQ-5D generates valid and reliable evaluation of functional health.
Physical Limitations
In order to assess perceived physical limitations in terms of impairment in daily activities, the physical limitation subscale from Kansas City Cardiomyopathy Questionnaire [KCCQ; (32, 33)] was applied. The physical limitations subscale assesses how much a patient’s condition affects his functional ability to do the following seven activities over the past 2 weeks: “dressing yourself,” “showering/bathing,” “walking 1 block on level ground,” “doing yardwork or housework,” “carrying groceries,” “climb a flight of stairs without stopping,” and “hurrying or jogging as if to catch a bus”. Participants responded on a 5-point scale from “extremely limited” to “not at all limited” with the additional option “limited for other reasons or did not do the activity.” According to the KCCQ-scoring instructions, if at least three of the questions were not missing, a mean score of the actual responses was transformed to a 0–100 scale with 0 meaning “extremely limited on all measured dimensions” and 100 meaning “no limitations on the measured dimensions”. The KCCQ shows good internal consistency (Cronbach’s alpha > 0.70) and satisfactory external validity (34, 35), especially the physical limitation scale used in the current study is a reliable measure [Cronbach’s alpha = 0.85, Ref. (34)].
Well-Being
To assess well-being, we used the World-Health-Organization-Five scale (WHO-5), a brief and commonly used measure of emotional well-being [e.g., See Ref. (36)] ranging from 0 to 100. Higher scores indicate better well-being. The WHO-5 has shown excellent internal consistency (Cronbach’s alpha = 0.91) and good external validity against SCID (Structured Clinical Interview for DSM Disorders; depression rating agreement of 80%) (37, 38). Also, the comparative validity with physicians’ diagnoses is reported to be excellent. While physician sensitivity for detecting major depressive disorder was only 40%, WHO-5 screening identified 94% of patients with major depressive disorder (37). According to the WHO, a score <52 indicates poor emotional well-being, and a score <28 is regarded as an indicator of a major depressive disorder (38).
Comorbidity
The number of comorbid diseases was calculated from insurance data by summing up all diagnoses from a list of 11 diseases that a participant had been diagnosed with in the previous 12 months before participation (e.g., arthrosis, coronary heart disease, CHF, COPD, diabetes).
Data Analysis
Data from all participants who returned both questionnaires at time 1 and time 2 (n = 2863) were included in the analyses.
To test multiple mediation for the three subsamples (diabetes, CHF, and DD), the following longitudinal multiple mediator model was proposed (Figure 2).
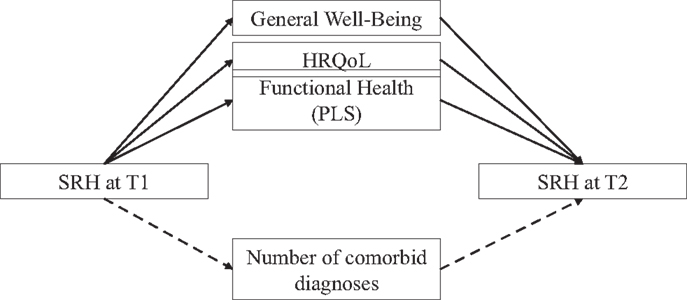
Figure 2. Proposed longitudinal multiple mediator model.
Self-rated health at T1 was the focal predictor of SRH at T2. The number of comorbid diagnoses was included as a first mediator into the model. Further proposed mediators were emotional well-being, functional health, and perceived physical limitations. The mediator analysis was conducted separately for the three groups (diabetes, CHF, and DD). Age and gender were entered as covariates into the model. To compare the magnitudes of the indirect effects, pairwise contrasts were estimated.
The traditional way to conduct a mediation analysis is the causal steps approach by Baron and Kenny (39). This approach imposes a number of difficulties, most importantly the inability to quantify the relative magnitude of the mediating effect as well as its significance. Therefore, current recommendations for testing mediation hypotheses use the product-of-coefficients-approach in line with bootstrapping strategies to obtain a bootstrapped estimate of the indirect effects and to deal with the rarely achieved assumption of multivariate normality (40). As this approach allows to include several mediators in one model, the comparison of specific indirect effects is possible and their magnitudes are quantifiable. In multiple mediator models, a specific indirect effect through a mediator might not be the same as the indirect effect of this mediator in a single mediator model because the mediators are likely to be intercorrelated. Therefore, the specific indirect effect in a multiple mediator model has to be seen as the ability of a mediator to mediate the effect of the predictor on the outcome within a set of other mediators in the model (40). The current statistic procedure involved bootstrapping analyses with 5000 bootstrap samples. For each mediating effect a sample was drawn 5000 times with replacement from the original sample and the mediating effect was computed. The resulting 5000 estimates were averaged to a bootstrapped estimate for the specific indirect effect. Confidence intervals of bootstrapped estimates are asymmetrically distributed, therefore they have to be corrected [e.g., See Ref. (41, 42)]. Thus, bias-corrected and accelerated 95% confidence intervals are reported in the current study.
Statistical analyses were conducted using IBM SPSS Statistics Version 20. To test multiple mediator models the SPSS macro provided by Preacher and Hayes (40) was used.
Results
Sample Characteristics
Table 1 presents the sample characteristics of the three groups. Individuals in the diabetes or CHF only groups were slightly younger (mean of 67.3 and 67.1 years) than those in the double diagnosis group (mean of 69.3 years). In contrast to most studies in clinical research, about 80% of the sample was male. This is due to the insurants’ structure of the Techniker Krankenkasse, where most of the older insurants worked in engineering, technical and therefore male-dominated fields of work. Results of a one-factor-ANOVA showed that the double diagnosis group differed significantly from the single diagnosis groups with consistently poorer health ratings on all measures at both assessment points. At baseline and at follow-up, persons with diabetes reported significantly lower functional health than persons with CHF (0.78 vs. 0.83; p < 0.001). Other than that the single diagnosis groups do not differ significantly on any other of the health-related measures at baseline or follow-up.
Table 2 shows the results of the correlation analyses. All proposed mediator variables (except number of comorbidities) were highly intercorrelated.
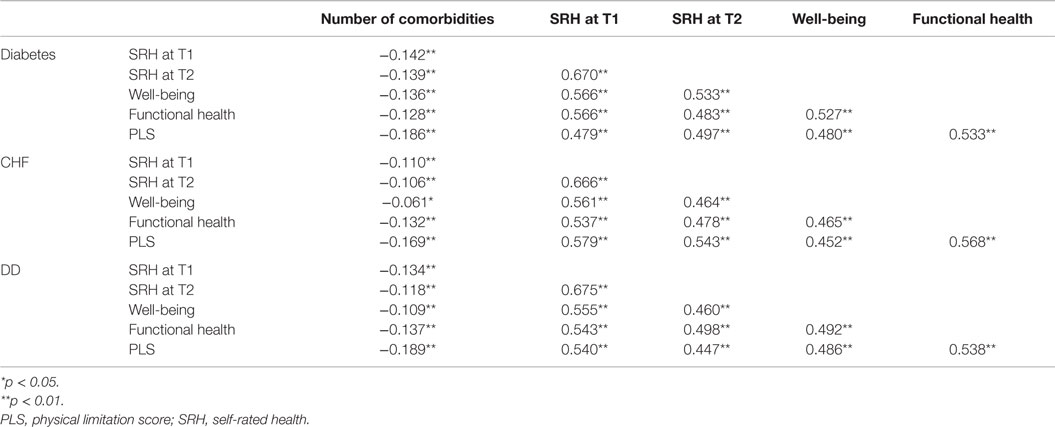
Table 2. Correlations of predictors in the three diagnostic groups.
Multiple Mediator Analyses
Results for all three multiple mediator analyses are presented in Table 3. To test whether comorbidity and health appraisal (emotional well-being, functional health and physical limitations) contributed to the effect of former SRH on future SRH multiple mediator models were tested. For all three subgroups, there was a significant total, direct, and indirect total effect demonstrating a partial mediation by the proposed variables (hypothesis 1). Specific indirect effects revealed no mediating effect of the number of comorbid diagnoses in any of the tested models (hypothesis 2).
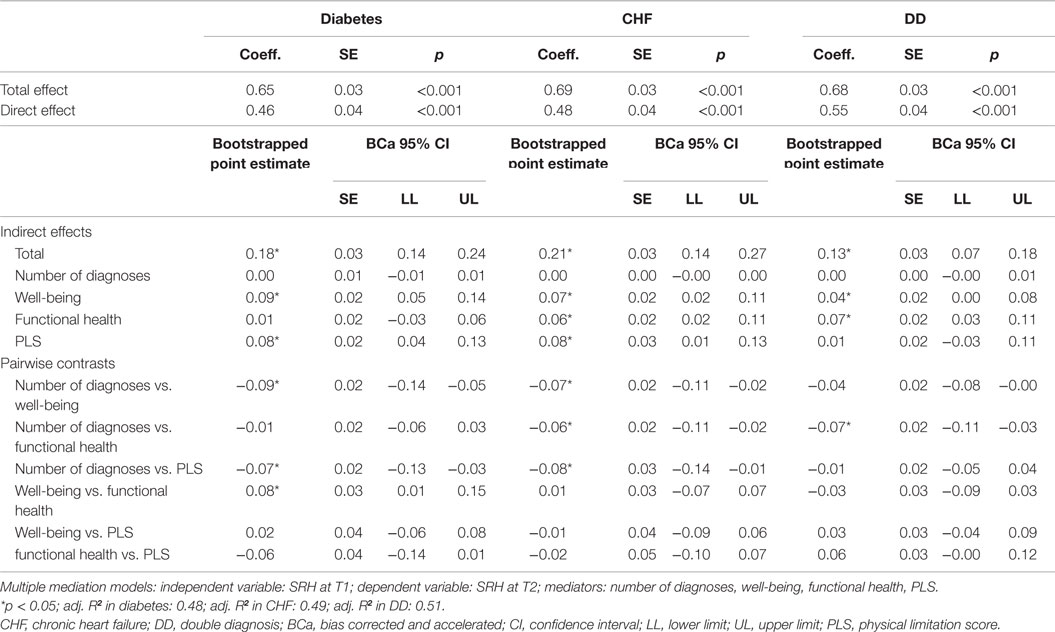
Table 3. Mediation models.
Furthermore, analyses showed strong effects of the health-related mediator variables (functional health and physical limitations) that differed between the diagnostic groups.
Diabetes
Multiple mediator analysis revealed that the total indirect effect of SRH at T1 on SRH at T2 through the proposed mediators was significant [0.18, BCa 95% CI (0.14;0.24)] with an explained variance of adj. R2 = 0.48. The examination of the specific indirect effects showed that for persons with diabetes (controlling for all other mediators) only well-being and physical limitations were significant mediators of the relationship between SRH at baseline and SRH at follow-up. No other variable contributed significantly to the indirect effect. To compare the magnitudes of the indirect effects, pairwise contrasts were estimated. The indirect effects’ magnitudes of physical limitations and well-being on SRH at T2 were significantly larger compared to the number of comorbidities (see pairwise contrasts in Table 3). Also, the magnitude of the indirect effect of well-being was significantly larger than the magnitude of the indirect effect of functional health on SRH. Physical limitations and well-being were equal in size in terms of their magnitude indicating a comparable mediating effect in the proposed mediator model.
Chronic Heart Failure
For the leading diagnosis, CHF multiple mediator analysis also showed a significant total, direct, and total indirect effect [0.21, BCa 95% CI (0.14;0.27)], indicating partial mediation of the proposed mediators taken as a set (adj. R2 = 0.49). Each mediator alone (except number of diagnoses) also had a significant mediating effect over and above the SRH autoregression. Thus, well-being, functional health, and physical limitations, specifically mediated the association of former and future SRH in this diagnostic group. The magnitudes of the specific indirect effects via well-being, functional health, and physical limitations were significantly larger than the effect via number of diagnoses. The three measures of health appraisal did not significantly differ in strength compared to each other. Thus, their mediating effects in the proposed model can be regarded as similar.
Double Diagnosis
For persons with both diagnoses (diabetes and CHF) the multiple mediator analysis also revealed significant total, direct, and total indirect effects [0.13, BCa 95% CI (0.07;0.18)] indicating a partial mediation of the mediators taken as a set (adj. R2 = 0.51). Only well-being and functional health showed significant specific indirect effects. Physical limitations and the number of diagnoses did not have a specific mediating effect over and above the SRH autoregression, well-being, and functional health. Pairwise contrasts showed significant differences in the strengths of the indirect effect only for functional health compared to the number of diagnoses, indicating that the indirect effect via functional health was stronger than the effect via number of diagnoses. The specific indirect effects of the other mediators were not significantly different from each another.
Discussion
The findings confirm that emotional well-being, functional health and physical limitations partially mediate the association between former and future SRH. These mediators contributed to SRH differently in each group (see below). The number of comorbid diseases did not predict SRH beyond the proposed mediators.
Across all groups emotional well-being consistently mediated the effect of former on future SRH. The mediation via physical limitations was significant for diabetes and CHF but not for the DD group. Functional health mediated the effect on SRH for persons with CHF and those with DD but had no mediating effect for persons with diabetes.
Between-groups differences in determinants of SRH appeared in terms of specific health appraisal indicators such as functional health and physical limitations. While physical limitations reflect the specific functional ability in daily activities, functional health gives a broader perspective on health appraisal as it additionally considers experiencing anxiety and depressive symptoms as well as pain and discomfort. Regarding health appraisal, persons with diabetes based their health rating rather on the limited ability to perform daily activities (physical limitations). These findings confirmed recent results that showed the strong association of a decrease in functional health and a declining physical health in diabetes (43). Persons with CHF additionally considered functional health in order to self-rate their health. For the most affected group with the double diagnosis (diabetes and CHF combined) functional health but not physical limitations contributed to SRH beyond former SRH and emotional well-being. When functional health appraisal and well-being were included into the model, the number of comorbid diseases had no mediating effect anymore. Thus, it seems to be the appraisal of comorbidity and not the mere number of diseases that affects SRH.
Previous research has shown that individuals with poorer health reported stronger associations of SRH with functional status (13, 15, 16). In those studies, functional health was also assessed as the ability to perform daily activities, thus as a specific task-oriented measure like the current physical limitations measure. However, our results revealed different effects of functional health and physical limitations on SRH. The less healthy individuals in the current study (double diagnosis) based their self-rating of health mostly on functional health aspects whereas the individuals with a comparatively better health (single diagnosis of diabetes or CHF) seemed to base their self-rating more on the specific aspects of physical limitations.
Within the DD-group, the proposed model had the largest amount of explained variance (R2 = 0.51) of future SRH mainly because of the large direct effect of former SRH. The direct effects in the diabetes and the CHF group were small compared to the DD-group but with larger indirect effects indicating a greater impact of the proposed mediators for single leading diagnoses. The considerably greater direct effect in the DD group suggests that individuals with both diagnoses based their self-rating more on former SRH than individuals with a single diagnosis. This finding should be examined further as it indicates a mechanism in the establishment of SRH depending on the appraisal of comorbidity. Heller et al. (17) concluded that younger individuals and those with low comorbidity were more likely to reduce self-ratings of health following changes in diagnosis than older persons with higher comorbidity. Hence, low comorbidity might be associated with greater cognitive flexibility in health appraisal. Therefore, research should focus on self-efficacy, control-beliefs, and cognitive flexibility associated with comorbidity to reveal further mechanisms of SRH constitution. Also, the question when which aspects of health become relevant for health appraisal should be addressed. Are the currently most limited abilities taken into account when persons self-rate their health?
Although our results indicate independence of SRH from the number of comorbid diseases, comorbidity is a strong predictor of mortality and should not be underestimated. However, research should focus on the processes behind the strong relationship of comorbidity and mortality. The individual appraisal of comorbidity might be more relevant than the simple number of comorbid diseases.
Summary
Our data confirm that SRH cannot be captured as a stable construct with fixed determinants and that it is highly dependent on individual appraisal of physical health. The results show different determinants of SRH depending on diagnosis. However, emotional well-being was a consistent and powerful factor of SRH across all groups. Thus, by improving emotional well-being SRH may be enhanced. Future SRH depended strongly on former SRH but the magnitude of this effect differed between diagnostic groups. The effect was stronger for persons with a greater health burden (double diagnosis vs. single diagnosis). For comparatively healthier individuals (single diagnosis) the indirect effect via the proposed mediators was larger than for less healthy individuals (double diagnosis). That, again, suggests different mechanisms underlying health appraisal that depend on physical health. Also, in terms of specific health appraisal less healthy individuals seem to base their self-ratings of health rather on functional health including affective aspects, whereas healthier persons (single diagnosis) focus on specific aspects of physical limitations when they self-rate their health.
Limitations
Unfortunately, we did not have the data to compare our results with a healthy sample. Future research should address potential differences in the constitution of SRH between different diagnostic patterns including healthy individuals.
Another limitation of our study is that due to the drop out over time the analyzed sample differed from the original sample. For methodological reasons, we included only those participants into the analyses that returned the second questionnaire (T2). Therefore the analyses are based on 77% of the baseline sample, which reflects our very high response rate. To test whether the participants who returned both questionnaires differed at baseline from those who returned only one, we ran an ANOVA. Results showed significant differences on all proposed variables consistently in the same direction. Compared to the participants who had to be excluded, the final sample reported higher SRH (5.39 vs. 4.9; p < 0.001), higher well-being (57.56 vs. 52.28; p < 0.001), better functional health (0.79 vs.0.74; p < 0.001), and less physical limitations (70.43 vs. 66.86; p < 0.001). Therefore, participants who were included into the analyses were significantly less affected in terms of health appraisal but had a slightly significantly higher number of comorbid diseases (4.65 vs. 4.54, p = 0.045) than those who could not be included into the analyses. We can only suspect that it might have been the even higher disease burden in terms of health appraisal that was responsible for non-participation due to higher physical/mental distress or less self-efficacy. In several studies with the health insurance company, we noticed a very high response rate (26, 44, 45). We assume that a reminder letter that was sent 2 weeks after the initial questionnaire added to this excellent response rate. Nonetheless, our results might be slightly biased because the overall health in the current sample was better than in the original sample.
Furthermore, the percentage of male participants (about 80%) was rather high. That allows us to supply information especially on men but also reduces the degree to which the results can be generalized.
As shown in Table 2, variables were highly correlated, which can compromise the significance of the effects found in the analyses. Especially the indirect effects might be biased due to intercorrelation between the measures. Regarding the topic of correlated mediators Preacher and Hayes (40) state that “… an intervention is sometimes designed to impact multiple intervening variables to achieve a desired outcome. In such cases, the mediators are almost necessarily correlated by virtue of their mutual reliance on a common cause…”. This conceptual similarity of the mediators may in part explain the strong correlations between the measures, however, it should be noted that all correlations were <0.6, indicating a substantial amount of discriminant validity.
Conclusion
Self-rated health is a highly individual rating. It is influenced by emotional well-being, functional health, and perceived physical limitations. Emotional well-being affected SRH consistently across all disease groups in our study. Functional health and physical limitations differed in their effect on SRH depending on diagnostic group. SRH might have a different meaning in different diagnoses or combinations of diagnoses. Future research should focus on individual appraisal of comorbidity, compare disease patterns of different diseases, and also address healthy individuals to answer the question when which health aspects are taken into account to rate one’s own health. By affecting emotional well-being we might be able to improve SRH.
Ethical Approval
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975 as revised in 2013. This study was carried out in accordance with the recommendations of the ethical guidelines of the health insurance company (Techniker Krankenkasse). Further ethics approval was not required as per German ethical guidelines. The individuals in the current study provided written informed consent, and they did not participate in any intervention over the course of data collection.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank Marina Benoit for proofreading and Ulrike Zetsche for helpful comments on the methods and an earlier draft of the paper.
Funding
In the current study, a subset of data from a larger evaluation study were analyzed. The original study was funded by the Techniker Krankenkasse (German Health Insurance Company). Present data were analyzed independently and upon approval by the insurance company.
References
1. Idler EL, Benyamini Y. Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav (1997) 38(1):21–37. doi: 10.2307/2955359
2. Jylha M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc Sci Med (2009) 69(3):307–16. doi:10.1016/j.socscimed.2009.05.013
3. Tissue T. Another look at self-rated health among the elderly. J Gerontol (1972) 27(1):91–4. doi:10.1093/geronj/27.1.91
4. Mossey JM, Shapiro E. Self-rated health – a predictor of mortality among the elderly. Am J Public Health (1982) 72(8):800–8. doi:10.2105/AJPH.72.8.800
5. Benyamini Y. The Bases for Predicting One’s Mortality: The Relationship Between the Predictors of Self-Assessments of Health and the Predictors of Mortality. New Brunswick, NJ: Rutgers, the State University of New Jersey (1997).
6. Benyamini Y, Idler EL, Leventhal H, Leventhal EA. Positive affect and function as influences on self-assessments of health: expanding our view beyond illness and disability. J Gerontol Ser B Psychol Sci Soc Sci (2000) 55(2):107–16. doi:10.1093/geronb/55.2.P107
7. Benyamini Y, Leventhal EA, Leventhal H. Self-assessments of health: what do people know that predicts their mortality? Res Aging (1999) 21(3):477–500. doi:10.1177/0164027599213007
8. Esteban y Pena MM, Hernandez Barrera V, Fernandez Cordero X, Gil de Miguel A, Rodriguez Perez M, Lopez-de Andres A, et al. Self-perception of health status, mental health and quality of life among adults with diabetes residing in a metropolitan area. Diabetes Metab (2010) 36(4):305–11. doi:10.1016/j.diabet.2010.02.003
9. Ho SY, Mak KK, Thomas GN, Schooling M, Fielding R, Janus ED, et al. The relation of chronic cardiovascular diseases and diabetes mellitus to perceived health, and the moderating effects of sex and age. Soc Sci Med (2007) 65(7):1386–96. doi:10.1016/j.socscimed.2007.05.032
10. Idler EL, Kasl SV. Self-ratings of health: do they also predict change in functional ability? J Gerontol B Psychol Sci Soc Sci (1995) 50B(6):S344–53. doi:10.1093/geronb/50B.6.S344
11. Konstam V, Salem D, Pouleur H, Kostis J, Gorkin L, Shumaker S, et al. Baseline quality of life as a predictor of mortality and hospitalization in 5,025 patients with congestive heart failure. Am J Cardiol (1996) 78(8):890–5. doi:10.1016/s0002-9149(96)00463-8
12. Kelleher CC, Whelan J, Daly L, Fitzpatrick P. Socio-demographic, environmental, lifestyle and psychosocial factors predict self rated health in Irish Travellers, a minority nomadic population. Health Place (2012) 18(2):330–8. doi:10.1016/j.healthplace.2011.10.009
13. Schuez B, Wurm S, Schollgen I, Tesch-Romer C. What do people include when they self-rate their health? Differential associations according to health status in community-dwelling older adults. Qual Life Res (2011) 20(10):1573–80. doi:10.1007/s11136-011-9909-4
14. Perruccio AV, Katz JN, Losina E. Health burden in chronic disease: multimorbidity is associated with self-rated health more than medical comorbidity alone. J Clin Epidemiol (2012) 65(1):100–6. doi:10.1016/j.jclinepi.2011.04.013
15. Benyamini Y, Leventhal EA, Leventhal H. Elderly people’s ratings of the importance of health-related factors to their self-assessments of health. Soc Sci Med (2003) 56(8):1661–7. doi:10.1016/s0277-9536(02)00175-2
16. Cott CA, Gignac MAM, Badley EM. Determinants of self rated health for Canadians with chronic disease and disability. J Epidemiol Community Health (1999) 53(11):731–6. doi:10.1136/jech.53.11.731
17. Heller DA, Ahern FM, Pringle KE, Brown TV. Among older adults, the responsiveness of self-rated health to changes in Charlson comorbidity was moderated by age and baseline comorbidity. J Clin Epidemiol (2009) 62(2):177–87. doi:10.1016/j.jclinepi.2008.05.009
18. Steinhauser KE, Arnold RM, Olsen MK, Lindquist J, Hays J, Wood LL, et al. Comparing three life-limiting diseases: does diagnosis matter or is sick, sick? J Pain Symptom Manage (2011) 42(3):331–41. doi:10.1016/j.jpainsymman.2010.11.006
19. Meng Q, Xie Z, Zhang T. A single-item self-rated health measure correlates with objective health status in the elderly: a survey in suburban beijing. Front Public Health (2014) 2:27. doi:10.3389/fpubh.2014.00027
20. Bradburn NM, Noll CE. The Structure of Psychological Well-being. Chicago: Aldine Publishing Company (1969).
21. Herman DR, Solomons NW, Mendoza I, Qureshi AK. Self-rated health and its relationship to functional status and well-being in a group of elderly Guatemalan subjects. Asia Pac J Clin Nutr (2001) 10(3):176–82. doi:10.1046/j.1440-6047.2001.00245.x
22. Lamers SA, Bolier L, Westerhof G, Smit F, Bohlmeijer E. The impact of emotional well-being on long-term recovery and survival in physical illness: a meta-analysis. J Behav Med (2012) 35(5):538–47. doi:10.1007/s10865-011-9379-8
23. Nutzel A, Dahlhaus A, Fuchs A, Gensichen J, Konig HH, Riedel-Heller S, et al. Self-rated health in multimorbid older general practice patients: a cross-sectional study in Germany. BMC Fam Pract (2014) 15:1. doi:10.1186/1471-2296-15-1
24. DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality Prediction with a Single General Self-Rated Health Question. J Gen Intern Med (2006) 21(3):267–75. doi:10.1111/j.1525-1497.2005.00291.x
25. Boehme S, Geiser C, Muehlenhoff T, Holtmann J, Renneberg B. Telephone counseling for patients with chronic heart failure: results of an evaluation study. Int J Behav Med (2012) 19(3):288–97. doi:10.1007/s12529-011-9179-0
26. West SG, Cham H, Thoemmes F, Renneberg B, Schulze J, Weiler M. Propensity scores as a basis for equating groups: basic principles and application in clinical treatment outcome research. J Consult Clin Psychol (2014) 82(5):906–19. doi:10.1037/a0036387
27. Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Ann Med (2001) 33(5):337–43. doi:10.3109/07853890109002087
28. Devlin N, Parkin D. Guidance to users of EQ-5D value sets EQ-5D Value Sets. In: Szende A, Oppe M, Devlin N, editors. EQ-5D Value Sets – Inventory, Comparative Review and User Guide. EuroQol Group Monographs. Dordrecht: Springer (2007). p. 39–52.
29. Horowitz E, Korek IA, Shani M, Shemer J. EQ-5D as a generic measure of health-related quality of life in Israel: reliability, validity and responsiveness. Isr Med Assoc J (2010) 12(12):715–20.
30. Hunger M, Sabariego C, Stollenwerk B, Cieza A, Leidl R. Validity, reliability and responsiveness of the EQ-5D in German stroke patients undergoing rehabilitation. Qual Life Res (2012) 21(7):1205–16. doi:10.1007/s11136-011-0024-3
31. Stark RG, Reitmeir P, Leidl R, Konig HH. Validity, reliability, and responsiveness of the eq-5d in inflammatory bowel disease in Germany. Inflamm Bowel Dis (2010) 16(1):42–51. doi:10.1002/ibd.20989
32. Faller H, Steinbüchel T, Schowalter M, Spertus JA, Störk S, Angermann CE. Der Kansas City Cardiomyopathy Questionnaire (KCCQ)-Ein neues krankheitsspezifisches Messinstrument zur Erfassung der Lebensqualität bei chronischer Herzinsuffizienz: Psychometrische Prüfung der deutschen Version. Psychotherapie Psychosomatik Medizinische Psychologie (2005) 55(3–4):200–8. doi:10.1055/s-2004-834597
33. Green CP, Porter CB, Bresnahan DR, Spertus JA. Development and evaluation of the Kansas City Cardiomyopathy Questionnaire: a new health status measure for heart failure. J Am Coll Cardiol (2000) 35(5):1245–55. doi:10.1016/s0735-1097(00)00531-3
34. Ortega T, Diaz-Molina B, Montoliu MA, Ortega F, Valdes C, Rebollo P, et al. The utility of a specific measure for heart transplant patients: reliability and validity of the Kansas City Cardiomyopathy Questionnaire. Transplantation (2008) 86(6):804–10. doi:10.1097/TP.0b013e318183eda4
35. Pettersen KI, Reikvam A, Rollag A, Stavem K. Reliability and validity of the Kansas City cardiomyopathy questionnaire in patients with previous myocardial infarction. Eur J Heart Fail (2005) 7(2):235–42. doi:10.1016/j.ejheart.2004.05.012
36. Bech P, Olsen LR, Kjoller M, Rasmussen NK. Measuring well-being rather than the absence of distress symptoms: a comparison of the SF-36 Mental Health subscale and the WHO-Five Well-Being Scale. Int J Methods Psychiatr Res (2003) 12(2):85–91. doi:10.1002/mpr.145
37. Löwe B, Spitzer RL, Gärfe K, Kroenke K, Quenter A, Zipfel S, et al. Comparative validity of three screening questionnaires for DSM-IV depressive disorders and physicians’ diagnoses. J Affect Disord (2004) 78(2):131–40. doi:10.1016/s0165-0327(02)00237-9
38. World Health Organization. Interpretation of the Items of the WHO-5 Questionnaire (2012). Available from: http://www.who-5.org/
39. Baron RM, Kenny DA. The moderator mediator variable distinction in social psychological-research – conceptual, strategic, and statistical considerations. J Pers Soc Psychol (1986) 51(6):1173–82. doi:10.1037/0022-3514.51.6.1173
40. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods (2008) 40(3):879–91. doi:10.3758/brm.40.3.879
43. Väätäinen S, Keinänen-Kiukaanniemi S, Saramies J, Uusitalo H, Tuomilehto J, Martikainen J. Quality of life along the diabetes continuum: a cross-sectional view of health-related quality of life and general health status in middle-aged and older Finns. Qual Life Res (2014) 23(7):1935–44. doi:10.1007/s11136-014-0638-3
44. Boehme S, Geiser C, Renneberg B. Functional and self-rated health mediate the association between physical indicators of diabetes and depressive symptoms. BMC Fam Pract (2014) 15(1):157. doi:10.1186/1471-2296-15-157
Keywords: self-rated health, functional health, well-being, comorbidity, multimorbidity, chronic disease
Citation: Böhme S and Renneberg B (2015) Predicting Self-Rated Health in Diabetes and Chronic Heart Failure – A Multiple Mediation Model. Front. Public Health 3:266. doi: 10.3389/fpubh.2015.00266
Received: 03 July 2015; Accepted: 09 November 2015;
Published: 25 November 2015
Edited by:
Michal Grivna, United Arab Emirates University, United Arab EmiratesReviewed by:
William Augustine Toscano, University of Minnesota School of Public Health, USACheryl Lynn Addy, University of South Carolina, USA
Copyright: © 2015 Böhme and Renneberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sylvia Böhme, sylvia.boehme@fu-berlin.de