 Charles Marks1,2*
Charles Marks1,2* María Luisa Zúñiga1,2*
María Luisa Zúñiga1,2*- 1School of Social Work, San Diego State University, San Diego, CA, United States
- 2SDSU-UCSD Joint Doctoral Program in Interdisciplinary Research on Substance Use, San Diego, CA, United States
Latinos living in the United States-Mexico border region bear a disproportionate HIV/AIDS burden compared to individuals living in the interior of both nations and face a constellation of barriers that determine their ability to access and adhere to HIV care. Use of complementary and alternative medicine (CAM) may be associated with suboptimal treatment adherence. Sociodemographic factors, health practices, and social determinants of health unique to the border region may further contribute to health disparities that undermine care engagement and continuity. Improved understanding of HIV-positive Latino subgroups and their risk profiles can lead to more effective, targeted clinical and public health interventions. We undertook this study to identify and characterize distinct classes of HIV-positive Latinos in the San Diego-Tijuana border region, differentiated by HIV and border-related factors, utilizing latent class analysis. We investigated relationships between class membership and CAM utilization and self-reported antiretroviral therapy (ART) adherence. Five distinct classes were identified with unique demographic, HIV risk, and border mobility profiles. CAM was recently used by nearly half of each class, though there were significant differences in the proportion of CAM use by class ranging from 44.4 to 90.9%. As well, all classes were currently receiving ART at similarly high rates and ART adherence outcomes were not significantly different based on class. Findings highlight the significant use of CAM by all HIV-positive Latinos in the border region and imply the need for a research framework which appropriately acknowledges the heterogeneous nature of this population, such as intersectionality. Further research is recommended into understanding how patients integrate CAM into HIV treatment and the risks and benefits of incorporating CAM into HIV treatment.
Introduction
In order to meet the United Nations goal of identifying, treating, and achieving viral suppression in 90% of all people living with HIV/AIDS (PLWHA) globally (1), it is necessary to understand the specific barriers and challenges faced by subpopulations that are disproportionately impacted by HIV. For Latinos in the United States (US) and Mexico, especially those residing in the shared border region, efforts to improve HIV-related health outcomes will require further attention to the unique needs of Latino subpopulations, especially those factors that place this vulnerable group at higher risk for falling out of care (2).
It is well-documented that US Latino immigrants face unique challenges to remain engaged in care throughout the continuum of HIV care (3–6). Yet, there is a need to better understand the barriers faced by specific Latino subpopulations in the US-Mexico border region where binational mobility is, for many, a part of daily life. The United States-Mexico Border Health Commission (USMBHC) identified slowing the spread of HIV in the border region as a primary objective by 2020, doing so after failing to meet their 2010 goal of significantly reducing the HIV incidence rate (7). In border cities such as Tijuana, studies have documented that HIV is concentrated within different high-risk communities, such as men who have sex with men (MSM), people who inject drugs (PWID), and female sex workers (FSW) (8). Though there is literature dedicated to understanding and addressing HIV-related health needs amongst MSM (9, 10), PWID (11–13), and FSW (14–17) in the US-Mexico border context, there is a need to understand the experiences of different subpopulations as they engage with health care services. While limited research into the attitudes of primary HIV care providers in the border region indicates that clinicians understand that there exist both personal and structural barriers to care for PLWHA (18), identifying which PLWHA populations are accessing care in the region remains an area of research need. Improved understanding of border patient profiles can inform clinical and health system efforts to promote care continuity and improved health outcomes.
The San Diego-Tijuana region provides an ideal setting for understanding the complex nature of living with HIV in the border region. As described by the USMBHC, the border region should not be conceptualized as two distinct neighboring nations, but as a set of independent twin cities, each of which represent environments requiring unique consideration (7). While comparisons of HIV rates between Tijuana and San Diego are difficult to ascertain due to different reporting standards in each country (19), HIV and AIDS disproportionately impact the region with higher rates than their respective national averages. In the state of Baja California, whose most populous city is Tijuana, the AIDS-related mortality rate is double the national average and this rate increased by nearly 20% from 2003 to 2013 (20). The HIV incidence rate for Latinos in San Diego County exceeds both the state and national general incidence rates (21, 22) and Latinos in the County went from representing 35% of new HIV cases in 2000 to 43% in 2014 (22). Further alarming is that 36% of all Latino PLWHA in San Diego County progress to AIDS within 30 days of their initial diagnosis, the highest rate amongst any race or ethnicity in the county (22). Overall, it is clear that much work is needed to achieve the United Nations 90% viral suppression goal, as overall in San Diego County in 2015 less than half of those diagnosed with HIV achieve viral suppression (22).
Characterizing PLWHA subpopulations in the San Diego-Tijuana region is not simply an exercise in identifying known high-risk communities, such as MSM and PWID, but must also account for the ways in which the border impacts individual mobility and access to care. The San Diego-Tijuana border is home to the busiest land border crossing in the western hemisphere where daily, tens-of-thousands of the region's citizens cross back and forth for work, family, shopping, school, and health care-related activities (23). Fluidity of dwelling (U.S. or Mexico or both) and binational mobility are hallmarks of living in the region (24). As the population of approximately 60 million Latinos in the US continues to grow by over 1 million people per year (25), achieving goals related to the HIV care cascade will require understanding of the barriers that Latino PLWHA face in accessing and remaining in HIV care. This includes understanding complex relationships between HIV-related risk factors, the impact of the border, as well as other relevant socio-demographic variables.
Additionally, the use of complementary and alternative medicine (CAM), such as herbal remedies or treatment from traditional healers, may play a complicating role in ensuring effective HIV care administration to PLWHA due both to inhibiting communication between patient and care provider (26, 27), as well as concerns about possible interactions between CAM and antiretroviral therapy (ART) (28). In the US, it is estimated that 32–55% of PLWHA utilize CAM to treat HIV-related symptoms (27, 29) and that rates of use are likely even higher amongst Latino PLWHA in the US-Mexico border region (26, 30). It appears, as well, that some Latino PLWHA utilize CAM when their care provider is unable to provide culturally appropriate treatment (31). Qualitative research has indicated that some HIV care providers in the San Diego-Tijuana region do not communicate with their patients about CAM, do not feel that they know enough about the interactions of CAM with ART medication to make recommendations, and have limited understanding of the role CAM use plays in ART adherence (32). For these reasons, it is important to understand CAM utilization among different Latino PLWHA subpopulations in San Diego and Tijuana to support clinicians in their efforts to have culturally-effective CAM dialogue with their patients.
One approach to understanding subpopulation profiles is the application of latent class analysis (LCA), a statistical tool that has been utilized to identify and characterize meaningful subpopulations, herein referred to as “classes.” Earlier studies have applied LCA to better understand subpopulation HIV risk profiles (33–35), with a primacy of literature focused specifically on class differences in HIV risk based on substance use behaviors (36–40). These studies have largely focused on characterizing substance using populations in both San Diego and Tijuana, identifying distinct classes of PWID with varying HIV risk profiles (36, 37, 40). Additionally, LCA has been utilized to identify PLWHA classes and predict their ART adherence (41, 42). In this study, we apply LCA to classify and characterize Latino sub-populations of PLWHA receiving HIV care in clinics in Tijuana and San Diego for the purpose of identifying present classes and to assess the barriers to adhering to and remaining in care the members of these classes face. Utilizing LCA, the primary objectives of this study are to: (1) identify and characterize classes of a population of PLWHA in San Diego-Tijuana based on HIV-risk factors and the impact of the border; (2) assess the relationship between class membership and CAM utilization; and (3) assess the relationship between class membership and care adherence.
Methods
Study Design
We conducted secondary data analysis using data from the cross-sectional study Complementary and Alternative Care Behavior in HIV+ Latinos in the US-Mexico Region (09/2009-07/2012), a mixed-methods study whose primary goal was to understand the relationship between CAM and factors associated with HIV care seeking and treatment adherence in the San Diego-Tijuana region. Participants were recruited simultaneously in San Diego and Tijuana from HIV health care and social services agencies. Trained interviewers administered a quantitative survey addressing CAM, ART, and other factors associated with HIV care seeking behavior in the U.S.-Mexico border region. The study adapted the Anderson and Aday Health Care Utilization model (43), which establishes a framework for integrating individual, structural, and provider-related factors in accessing healthcare service utilization. The study was approved by the UCSD Human Research Protection Program.
Participants
The inclusion criteria for the study were that participants be Latino, diagnosed as HIV-antibody positive, having resided in San Diego or Tijuana for at least 1 month in the year prior, able to speak English or Spanish, be at least 18 years old, and be able to give informed consent. Participants were recruited from HIV care clinics and social services agencies in San Diego (n = 100) and Tijuana (n = 101).
Measures
The survey was comprised of 11 sections based on existing scales and the author's prior work in binational care practices in the U.S.-Mexico border. The sections were as follows: Demographics, including age, education, language preference, living situation, and reported weekly income in US dollars (conversion rate of 12.5 Mexican pesos per 1 USD used based on 2009–2012 rates) (44); Health History and Utilization of HIV Medical Services, including health insurance status and recent medication history; HIV Testing, inquiring about HIV testing history, the progression from HIV positive test result to receiving care, as well as ART adherence; Complementary and Alternative Medicine, measuring CAM utilization and related attitudes [adapted from CAM domains defined by the National Center for Complementary and Alternative Medicine and on the California Health Interview Survey-Complementary and Alternative Medicine Questionnaire (45)]; Religion/Spirituality, asking about religious identification and role of spirituality in living with and managing HIV; HIV-Related Felt Stigma Scale, measuring HIV-related stigma utilizing measures validated for Spanish-speaking Latinos (46) and region-specific indicators defined in previous research (47, 48); Knowledge, Attitudes, and Beliefs About HIV Care, asking about attitudes around treatment adherence and CAM use as appropriate treatment modalities; Border Crossing and Deportation, asking about border crossing behaviors and related complications; Sexual, Drug Use, and Other Risk Behaviors, asking about history of substance use, sexual history, and other risk factors such as prior incarceration; Mental Health/Depression, utilizing the CES-D scale (49) to assess mental health status; and Physician-Patient Relationship Quality Scales, measuring elements of perceived relationship with primary HIV care provider based on HIV Cost and Services Utilization Study measures (50).
Statistical Analyses
Our primary objective was to identify and characterize subpopulations of study participants. Latent class analysis (LCA) was utilized (RStudio v1.0.153, poLCA library) to assign individuals into classes based on the following dichotomous indicators: sexuality [heterosexual/Lesbian Gay Bisexual Transgender (LGBT)]; lifetime history of illicit drug use (never/ever); lifetime history of trading sex (never/ever); having health coverage in Mexico (yes/no); and having health coverage in the United States (yes/no). These were chosen to capture factors related to known HIV risk populations (MSM, PWID, and FSW) and to include border-related factors that are thought to be associated with HIV care access. Lifetime history of injection drug use was a preferred indicator, but due to low response rates (n = 138), lifetime history of illicit drug use was used in its place. As well, health coverage status was viewed to be a strong indicator for border impact because, (a) nearly all (n = 196) participants reported having health coverage and (b) it accounted for participant ability to access care on either side of the border, as opposed to only accounting for the location where the participant was surveyed. Missing indicator values were imputed as a part of the poLCA library's LCA implementation.
LCA models were fit to 2, 3, 4, 5, 6, and 7 classes and the Akaike's information criteria (AIC) and the Bayesian information criteria (BIC) were applied to assess and compare the goodness-of-fit of each of the models (51). To choose the best fit model, the AIC and BIC were considered in addition to a qualitative determination of which model provided the most clinically meaningful classification. The LCA assigns a probability that each participant is a member of each class. The participants were assigned to the class of the chosen model of which they had the highest probability of being a member. Then, descriptive statistics for each class were generated (tableone library) and were utilized to characterize each class. In addition, Chi-squared tests and ANOVA were applied to determine significant class differences on demographic, HIV-related risk, CAM utilization, and ART adherence factors.
Results
Of 201 total participants, 69.3% reported residence in Mexico at the time of the interview, 82.4% were male, the mean age was 48 years (median 48.00), and half had not completed secondary school. The mean income (in US $) was $137.50/week though 17.9% reported having no income at all and 45.8% were unemployed. In the prior 6 months, 36.7% reported having made at least one round-trip border crossing. In total, 62.8% identified as LGBT, 58.7% reported lifetime use of illicit drugs (excluding cannabis), and 34.7% had traded sex. Twelve individuals, all men, reported having between 10 and 30 sex partners in the prior 3 months. In all, 71.1% had reported using CAM in the prior 6 months with teas (60%), vitamins (60%), herbs and plants (27.9%), and body work (23.4%) representing a majority of the reported use. While 72.5% reported being at least in “good” health, 40.1% had been diagnosed with AIDS at the time of their interview. Almost 90% were currently taking ART medication of whom 28.5% reported missing taking their medication at least once in the prior month. Of those who had been diagnosed over 3 months prior to being interviewed, 18.5% had at gone at least a 3-month span without taking ART medication.
Latent Subpopulations
LCA fit statistics indicated that the 3-class and 5-class solutions presented the best fits (see Table 1), and here we present the results of the 5-class solution which was determined to provide the most clinically meaningful classification. First, we shall describe the classes individually based on the model indicators, demographic factors, and factors related to the border. For each such variable, there was a statistically significant difference across the five classes (see Table 2 to examine these differences and their significance values). Classes have been ordered by the proportion of the class which reported having health coverage in the US (highest to lowest) and are described here:
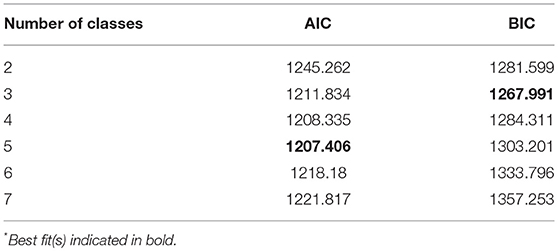
Table 1. LCA goodness-of-fit statistics*.
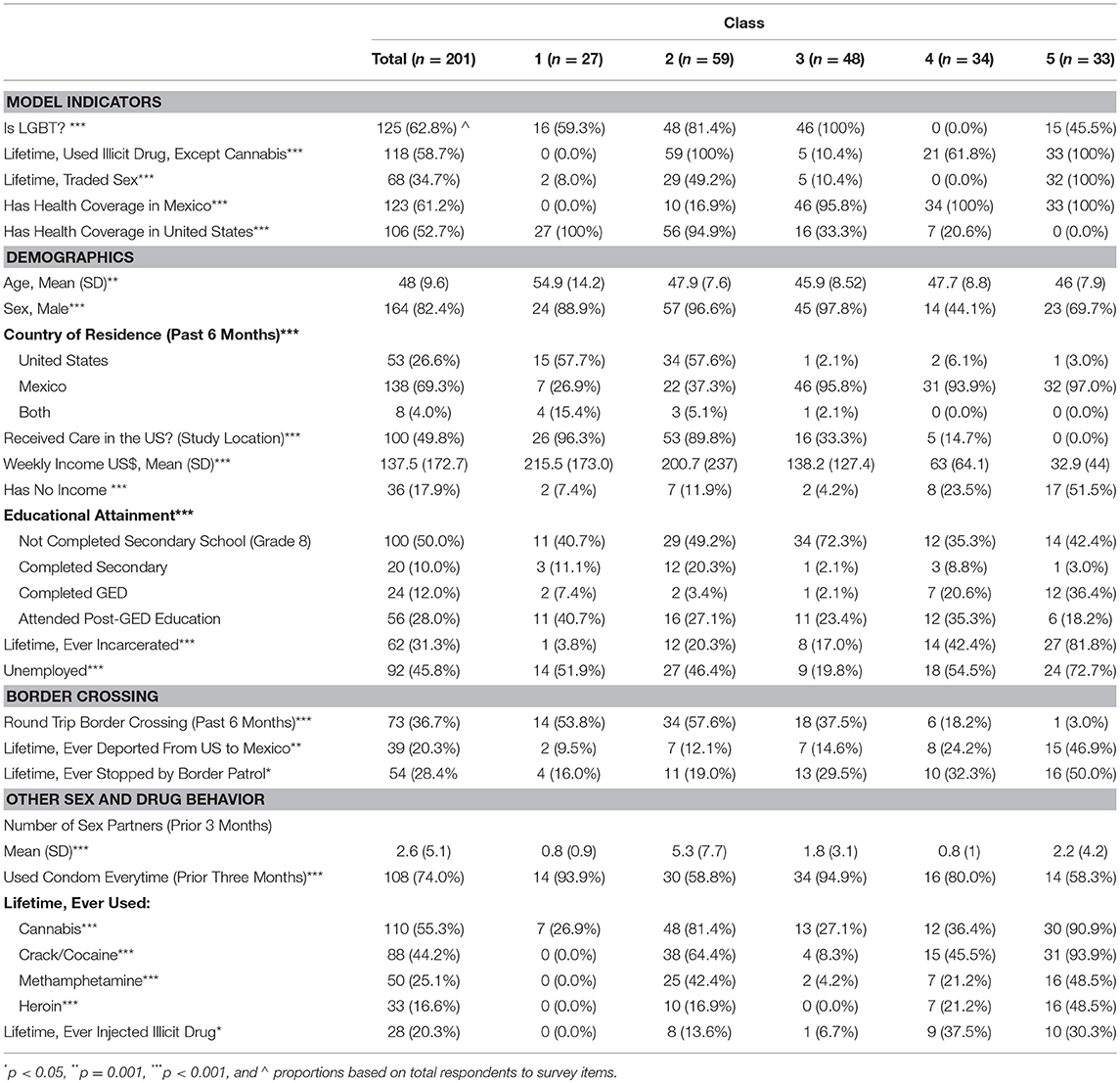
Table 2. Model indicators, demographics, border crossing, and HIV risk behaviors (by class).
Class 1 (n = 27)
In this class, every member was recruited in the US and all but 26.9% reported residing in the US over the prior 6 months. Every member reported having health coverage in the US and none in Mexico. Members were significantly older with a mean age of 55 years. In total, 88.9% were men and 59.3% of members identified as LGBT. This class had the highest mean income at $215.52/week and only 7.4% reported having no income despite 51.9% reporting not being employed, though this may be explained by retirement. Educational background was wide-ranging as 40.7% of individuals had not completed secondary school and the same proportion had received post-GED education. Only 8% reported ever having traded sex, members reported an average of 0.81 sexual partners in the prior 3 months, and 93.3% identified using a condom during sex every time in that same time span. Zero members reported lifetime illicit drug use or injection drug use. As well, only 3.8% reported ever having been incarcerated. In all, 53.8% had made a round-trip border crossing in the previous 6 months and 9.5% had ever been deported from the US to Mexico. Overall, this class can be characterized as older, wealthier individuals (potentially retired), primarily LGBT men, living in both Mexico and the US, receiving care in the US, with border mobility, with no history of using illicit drugs or trading sex.
Class 2 (n = 59)
In this class, 89.8% of members were recruited in the US, 62.7% had residence there in the prior 6 months, 94.9% had health coverage in the US and 16.9% had health coverage in Mexico. The mean age was 45.91 years. In total, 96.9% were men and 81.4% of members identified as LGBT. This class had the second highest mean income at $200.74/week and only 11.9% reported having no income despite 46.6% reporting not being employed. Approximately half, 49.2%, had not finished secondary school and 47.4% had completed high school. In total, 49.2% had ever traded sex, members reported an average of 5.29 sexual partners in the prior 3 months, skewed by multiple members reporting as many as 30, and 58.8% identified using a condom during sex every time in that same time span. Every member had a lifetime history of using illicit drugs, though only 13.6% had reported ever injecting. Just over 20% reported ever having been incarcerated. In all, 57.6% had made a round trip border crossing in the previous 6 months and 12.1% had ever been deported from the US to Mexico. Overall, this class can be characterized as men, primarily LGBT, living in both the US and Mexico, receiving care in the US, with a history of illicit drug use, with many members having traded sex, with a relatively higher income, border mobility, with lower likelihood of ever having been incarcerated.
Class 3 (n = 48)
In this class, 67.7% of members were recruited in Mexico, 95.8% lived there the prior 6 months, 95.8% had health coverage in Mexico and 33.3% had health coverage in the US. The mean age was 45.91 years. Men made up 97.8% of the class and every member identified as LGBT. Though the class average income was slightly less than the mean of the entire population at $138.17/week, this class had the lowest proportion of unemployed individuals at 19.8% and the lowest proportion of individuals with no income at 4.2%. Almost three-quarters of members had not completed secondary school. Only 10.4% reported ever having traded sex, members reported an average of 1.75 sexual partners in the prior 3 months, and 94.9% identified using a condom during sex every time in that same time span. In total, 10.4% reported lifetime us of illicit drugs, and of those that responded, 6.7% reported lifetime injection drug use. As well, 17% had ever been incarcerated. In all, 37.5% had made a round trip border crossing in the previous 6 months and 14.6% had ever been deported from the US to Mexico. Overall, this class can be characterized as LGBT men living in Mexico, likely working-class with low educational attainment, with minimal history of illicit drug use or sex work.
Class 4 (n = 34)
In this class, 85.3% of members were recruited in Mexico, 93.9% lived there the prior 6 months, and all group members had health coverage in Mexico. The mean age was 47.7 years. Men made up 44.1% of the class and every member identified as heterosexual. The mean income was the second lowest at $62.97/week, 23.5% reported no income at all, and 54.5% reported being unemployed. Educational background was wide ranging as 35.3% of individuals had not completed secondary school and the same proportion had received post-GED education. Zero members of the group reported ever having traded sex, members reported an average of 0.82 sexual partners in the prior 3 months, and 80% identified using a condom during sex every time in that same time span. In total, 61.8% reported lifetime use of illicit drugs, and of those that responded, 37.5% reported lifetime injection drug use. As well, 42.4% had been incarcerated. Only 18.2% reported making a round trip border crossing in the previous 6 months and 25% had ever been deported from the US to Mexico. Overall, this class can be characterized as heterosexual, low-income men and women with a high probability of illicit and injection drug use living and receiving HIV care in Mexico with limited cross-border mobility.
Class 5 (n = 33)
In this class, every member was recruited in Mexico, 97% had residence there the prior 6 months, 100% had health coverage there and none had health coverage in the US. The mean age was 45.97 years. In total, 69.7% were men and 45.5% of members identified as LGBT. This class had the lowest income at $32.94/week with 51.5% reporting having no income and 72.7% being unemployed. While 42.4% had not completed secondary school, 54.6% had completed high school. Every member reported having traded sex, members reported an average of 2.25 sexual partners in the prior 3 months, and 58.3% identified having used a condom every time during sex over the same time span. Every member had a lifetime history of illicit drug use and 30.3% reported having ever injected drugs. Members reported ever having been incarcerated at the highest proportion of any class at 81.8%. In all, only 3% had made a round trip border crossing in the previous 6 months and almost half (46.9%) had ever been deported from the US to Mexico. Overall, this class can be characterized as men and women, living and receiving care in Mexico, with history of illicit drug use, trading sex, deportation, and incarceration, with no cross-border mobility, and no or low income.
Class Comparison of CAM Utilization and Attitudes/Beliefs
While 71.1% of all participants reported utilizing CAM in the prior 6 months, there were significant differences in usage rates between classes (p < 0.001; see Table 3). While 81.2, 88.2, and 90.9% of members of Classes 3, 4, and 5, respectively, reported using CAM, only 44.4% of Class 1 and 54.2% of Class 2 reported using CAM. While all classes utilized herbal/plant remedies and vitamin supplements at similar rates, there were significant differences in the utilization of both teas (p < 0.05) and body work (p < 0.001; i.e., acupuncture, chiropractors, and massage). Zero members of Class 1 identified using body work, whereas approximately 40% of both Classes 4 and 5 did so in the prior 6 months. As well, only 25% of Class 1 reported using teas, compared to 63.4, 73.3, and 71.0% of Classes 3, 4, and 5, respectively. There were almost no reports of accessing CAM practitioners, such as curanderos, espiritistas, or herbalists.
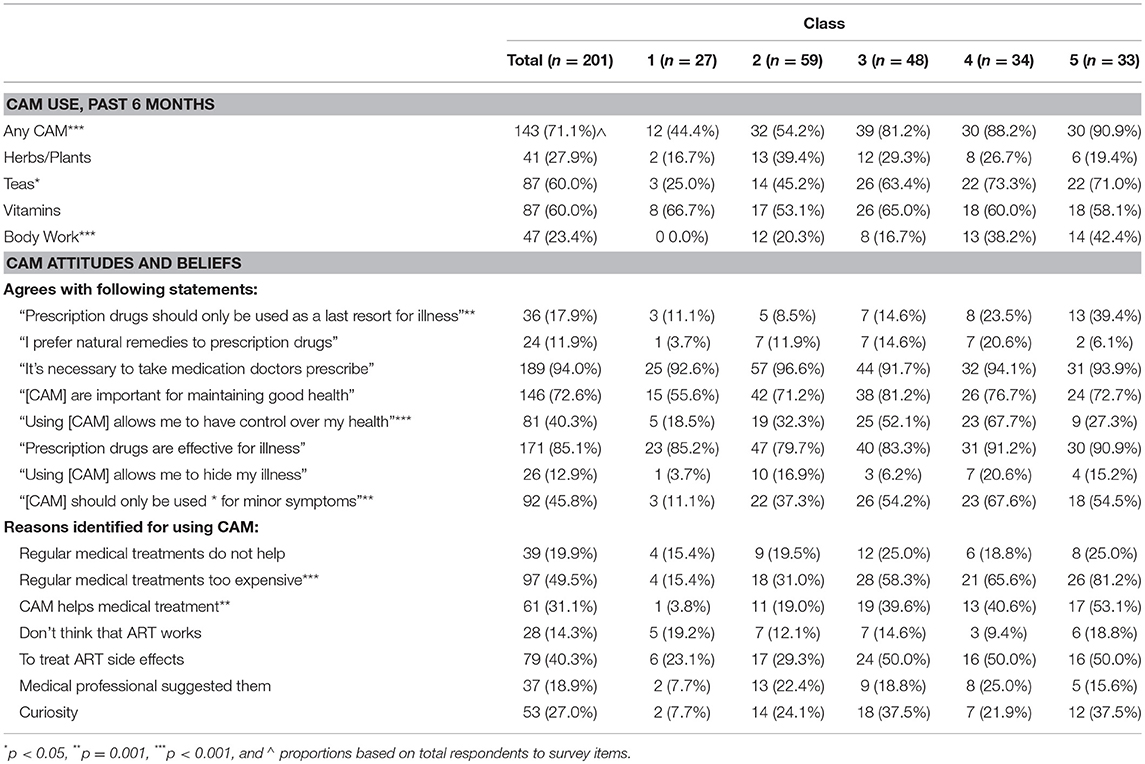
Table 3. CAM utilization and related attitudes and beliefs (by class).
Nearly all participants believed that prescription medication is effective and that it is necessary to take the medications prescribed by a doctor, but at least 11% of every class stated that prescription drugs should only be taken as a last resort, with 23.5% of Class 4 and 39.4% of Class 5 believing such (p = 0.001). A majority of participants in all classes, ranging from 55.6% of Class 1 to 81.2% of Class 3, identified CAM as being an important part of maintaining good health and 11.9% of participants identified preferring CAM to prescription medication, ranging from only 3.7% of Class 1 to 20.6% of Class 4. Overall, 40.3% of participants identified that CAM can help them hide their HIV symptoms from others, but there was a significant difference between groups (p < 0.001); only 25–33% of participants in Classes 1, 2, and 5 agreed to such compared to 50% of Class 3 and 67% of Class 4.
Class Comparison of HIV Care Engagement and Adherence
Overall, a majority (72.5%) of all participants identified as being in “good” or better health, 40.1% had been diagnosed with AIDS, and 89.9% were currently taking ART, with no significant difference amongst classes (see Table 4). In the prior month, 28.5% reported missing taking their ART at least once, 39.7% reported not always following the exact time schedule for their ART doses, and 17.8% reported not taking their ART medication for at least 1 weekend. However, there were notable differences between classes. Only 8.3% of Class 1 reported missing any ART in the prior month, whereas between 20.7 and 37.9% in the other classes reported doing so. The only significant difference identified was that while 0% of Class 1 identified not taking ART for at least 1 weekend in the same time span, over 20% of Classes 2 and 3 and over 30% of Class 5 identified as such (p < 0.05). Of participants who had been diagnosed with HIV at least 3 months prior to the interview, 18.5% identified having had at least one 3-month period not taking ART, with rates ranging from 9.8% of Class 3 to 29.1% of Class 2.
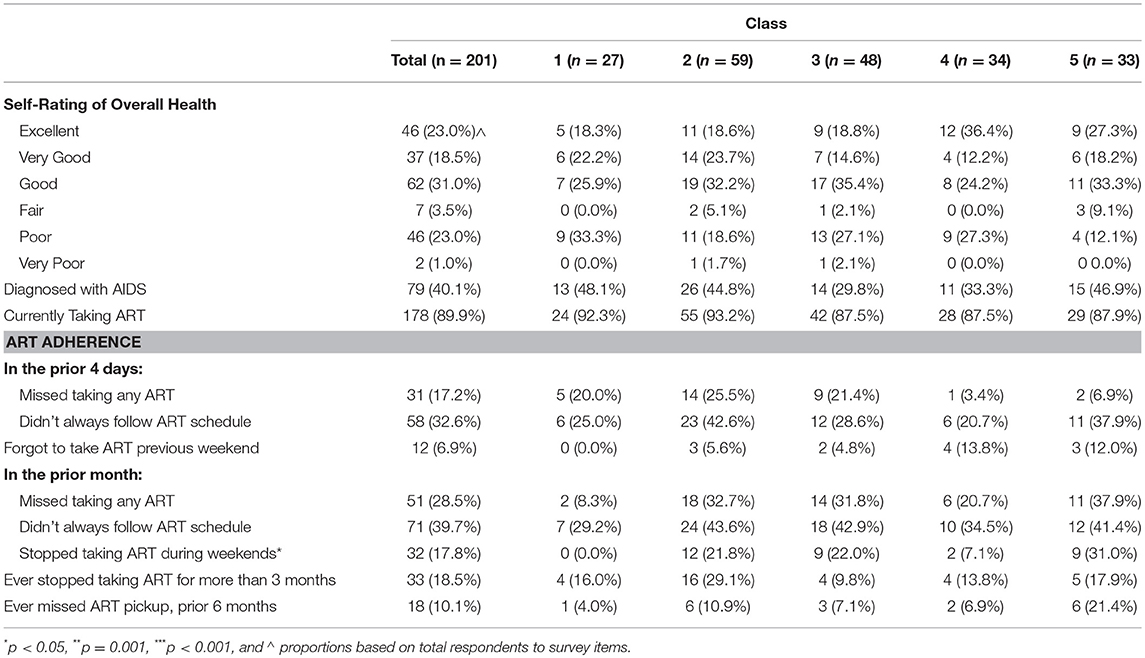
Table 4. ART adherence and health indicators (by class).
Discussion
Study findings reveal that the five distinct classes represent a highly heterogeneous group of Latino PLWHA, the profiles of which also indicate a spectrum of risk behaviors and relationship to the US-Mexico border region. Significant differences were noted between classes, including privileges associated with factors such as higher income and cross-border mobility, and barriers such as poverty, unemployment, engagement in sex work, and illicit substance use. Across all classes, CAM utilization was high and barriers to ART adherence were present, though study participants were largely well-engaged in HIV treatment.
The differences in CAM utilization by class appear to be correlated to which country individuals had access to care in, with Classes 1 and 2, the two classes with greater US health coverage, reporting less CAM utilization than the other classes. This relationship between country and CAM utilization could be indicative of cultural differences or of different environmental and structural factors in accessing CAM and HIV care in Tijuana and San Diego. Future research should focus on illuminating the nature of this relationship. Despite these significant differences in recent CAM utilization by class, the CAM utilization rates ranging from nearly 50% to over 90% indicate that CAM use is prevalent across all classes and is ubiquitous in some. These utilization rates are consistent with the prior literature (26, 30). It is thus clear that addressing CAM use must be a component of any HIV treatment modality for Latino PLWHA in the border region. Research into the interaction between CAM use and ART adherence is of immediate importance. We were unable to undertake such an analysis due to a lack of statistical power, but if a significant relationship between CAM use and ART adherence were to be found, this would provide valuable direction for research and interventions aimed at improving ART adherence amongst Latino PLWHA. As well, HIV care providers in the border region would benefit from increased CAM education opportunities and CAM-related protocols to empower them to continue providing effective care to their patients (32).
Given that Latino PLWHA are already at increased risk of being diagnosed with HIV later than non-Latino Whites and given the high rate of Latinos in San Diego County who progress to AIDS within a month of their HIV diagnosis (22), it is imperative that all classes of individuals living with HIV/AIDS be identified and that barriers to HIV care access remain an area of ongoing research. An immediate research question is whether the classes identified here represent populations fully engaged in HIV care or if they represent a subset of a population in which many are not able to access care. For example, it may be fair to hypothesize that Class 1, characterized by higher income, border mobility, and low risk profile, is reflective of a population in which all members are able to and do access HIV care. In comparison, it may be hypothesized that there is an un-sampled population with a similar risk profile as Class 5, characterized by high rates of illicit drug use, sex work, and incarceration, no income, and no border mobility, which is unable to access HIV care. While this research is only reflective of classes of individuals who have made contact with HIV-related services, the results provide a foundation for investigating and understanding the context of Latino PLWHA living in the border region who are not in contact with HIV care services. Research in identifying such populations is crucial in ensuring improved HIV-related health care engagement and outcomes for PLWHA Latinos in the border region.
As well, given that the US-Mexico border is at the forefront of the current North American political climate, it is important to reflect on how these results can inform how U.S. border policies may impact ability to access necessary care among Latino PLWHA living within the border region. The most important connection between this research and border policy implementation is that not all Latino PLWHA will be affected in the same way. Policy initiatives which seek to diminish or even stop border crossings, as the Trump Administration has recently called for (52), will disparately impact binational Latino PLWHA. Interestingly, though, new local binational insurance companies may mitigate the effects of federal policy aimed at decreasing border mobility. For example, SIMNSA and MediExcel are health insurance companies, that are approved by the State of California to provide health care services on both sides of the California-Mexico border (53). As a growing industry, binational insurance plans represent a promising solution for increasing access to care along the border, especially in the context of sister cities (such as San Diego and Tijuana) where crossing the border, for many, is a part of daily life. Future research should investigate the impact of U.S. border policies and bi-national insurance providers on access to care for the heterogeneous groups of Latino PLWHA living in the US-Mexico border region.
Finally, these findings indicate that, for future research and interventions directed toward Latino border populations, a theoretical foundation which recognizes the heterogeneity of the population and thus, which accurately reflects the population's narratives and needs, is necessary. Intersectionality provides such a framework and its relevance to addressing global health issues is gaining increased attention (54, 55). Intersectionality posits that individuals' experiences cannot be considered to be the causal result of a singular personal attribute, such as gender, race, or class, but instead, are the result of the interaction of all of these attributes with the many environmental contexts to which individuals are simultaneously subjected (52) Kapilashrami and Hankivsky discuss two strengths of applying intersectional theory to issues of global health which are of immediate relevance to the findings of this research: (1) that intersectional theory can be used to understand the heterogeneity of populations “that are often portrayed as relatively homogenous” [(54), p. 2,589]; and (2) that it can illuminate the many environmental contexts which shape individual and group experiences and thus, can provide a more accurate depiction of the source of health disparities (54). The findings presented here indicate that the population of Latinos seeking HIV care in the San Diego-Tijuana border region is heterogeneous; each group is subject to unique barriers to receiving care based on their geographic location, ability to cross the border, and class, amongst other factors. Intersectionality provides a helpful theoretical foundation for addressing health disparities faced by Latinos in the US-Mexico border region and should be considered in the design of future research and interventions to address them.
Limitations
This study faces several limitations. First, in regard to the analysis itself, it is convenient to discuss “class membership” as though the five classes identified are distinct communities. It is important to understand that “class membership” does not necessarily refer to individuals belonging to a tangible group, but that individuals share a similar profile across a constellation of relevant variables. Next, the sampling method ensured that only individuals engaging with care and social services organizations were included in the study. Thus, the results are not generalizable to all Latino PLWHA in the San Diego-Tijuana region, but only to those in contact with such care organizations. It must be added, though, that the sampling method does not imply participants are necessarily currently receiving HIV care, as some of the recruitment service facilities did not directly provide care, but only helped connect individuals with care providers. In regard to measuring ART adherence, it would have been preferable to utilize a biological measure as opposed to self-report, though research indicates that self-report is a valuable tool for assessing ART adherence (56). As a cross-sectional study, participant circumstances that may underlie categorization in one category are not fixed, and temporally-sensitive factors, such as location of home or service access may change over time. Finally, given that the data is cross sectional, no causal inference can be made about any of the findings presented. Nevertheless, this study provides insights into diverse categories of Latino PLWHA in the U.S.-Mexico border region, and as such, can provide a framework from which to understand health needs and serve to inform service delivery models for diverse populations.
Conclusion
This study establishes the heterogeneity of Latino PLWHA living in the border region and the widespread utilization of CAM across the population. The results of this study indicate the ability to access and adhere to care for Latino PLWHA is complicated by demographic factors, HIV risk profile, and binational mobility. The distinct experiences of this heterogeneous population must be illuminated to ensure the provision of culturally appropriate and necessary care to all individuals in need. As CAM use was prevalent (or ubiquitous) across all classes identified, incorporating CAM into HIV/AIDS care provision protocols is crucial for ensuring both effective and culturally relevant treatment. In addition, it is vital that classes not identified in this study, representing individuals not engaged with at any stage within the HIV continuum of care, be sought and understood to ensure that they are able to access needed care. Finally, it is crucial that future research utilize a guiding framework, such as intersectionality, which acknowledges the wide heterogeneity of Latino PLWHA in the US-Mexico border region.
Ethics Statement
This research was conducted in accordance with the recommendations of the University of California, San Diego Human Research Protection Program, and the San Diego State University Human Subjects Institutional Review Board. All subjects gave written informed consent in accordance with the Declaration of Helsinki. The protocol was approved by the San Diego State University Human Subjects Institutional Review Board.
Author Contributions
CM and MZ are responsible for all components of manuscript producing including the conceptualization, hypothesis formation, statistical analysis, and manuscript production. Both provide approval for the publication of its contents.
Funding
This study was supported in part by the NIH/National Center for Complementary and Alternative Medicine [R21 AT004676- 01A1]; National Institute of Mental Health [1R21MH084266-01, 5K01 MH072353].
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer CHS declared a shared affiliation, with no collaboration, with the authors to the handling editor at time of review.
Acknowledgments
The authors gratefully acknowledge the following: Our dedicated research staff, our community partners, and collaborators on both sides of the border, as well as the participants, without whom the study could not have been possible. This work was conducted under the Joint Doctoral Program in Interdisciplinary Research on Substance Use.
References
1. Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90 An Ambitious Treatment Target to Help End the AIDS Epidemic. (2014). Available online at: http://unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf. (accessed September 19, 2018).
2. Gant Z, Dailey A, Hu X, Johnson A. HIV Care Outcomes Among Hispanics or Latinos With Diagnosed HIV Infection — United States, 2015. Morbidity and Mortality Weekly Report (2015).
3. Campo RE, Alvarez D, Santos G, Latorre J. Antiretroviral treatment considerations in Latino patients. AIDS Patient Care STDS. (2005) 19:366–74. doi: 10.1089/apc.2005.19.366
4. Castañeda H, Holmes SM, Madrigal DS, Young M-ED, Beyeler N, Quesada J. Immigration as a social determinant of health. Annu Rev Public Health. (2015) 36:375–92. doi: 10.1146/annurev-publhealth-032013-182419
5. Ojikutu BO, Mazzola E, Fullem A, Vega R, Landers S, Gelman RS, et al. HIV testing among black and hispanic immigrants in the United States. AIDS Patient Care STDS. (2016) 30:307–14. doi: 10.1089/apc.2016.0120
6. Levison JH, Bogart LM, Khan IF, Mejia D, Amaro H, Alegría M, et al. “Where it falls apart”: barriers to retention in HIV care in latino immigrants and migrants. AIDS Patient Care STDS. (2017) 31:394–405. doi: 10.1089/apc.2017.0084
7. United States-Mexico Border Health Commission. Healthy Borders 2020. United States-Mexico Border Health Commission. (2015). Available online at: https://www.hhs.gov/sites/default/files/res__2805.pdf (accessed September 19, 2018).
8. Smith LR, Patterson TL, Magis-Rodriguez C, Ojeda VD, Burgos JL, Rojas SA, et al. Engagement in the HIV care continuum among key populations in Tijuana, Mexico. AIDS Behav. (2016) 20:1017–25. doi: 10.1007/s10461-015-1186-8
9. Pitpitan EV, Goodman-Meza D, Burgos JL, Abramovitz D, Chavarin CV, Torres K, et al. Prevalence and correlates of HIV among men who have sex with men in Tijuana, Mexico. J Int AIDS Soc. (2015) 18:19304. doi: 10.7448/IAS.18.1.19304
10. Pines HA, Goodman-Meza D, Pitpitan EV, Torres K, Semple SJ, Patterson TL. HIV testing among men who have sex with men in Tijuana, Mexico: a cross-sectional study. BMJ Open. (2016) 6:e010388. doi: 10.1136/bmjopen-2015-010388
11. Werb D, Garfein R, Kerr T, Davidson P, Roux P, Jauffret-Roustide M, et al. A socio-structural approach to preventing injection drug use initiation: rationale for the PRIMER study. Harm Reduct J. (2016) 13:25. doi: 10.1186/s12954-016-0114-1
12. Rafful C, Zule W, González-Zúñiga PE, Werb D, Medina-Mora ME, Magis-Rodriguez C, et al. High dead-space syringe use among people who inject drugs in Tijuana, Mexico. Am J Drug Alcohol Abuse. (2015) 41:220–5. doi: 10.3109/00952990.2015.1011742
13. Melo JS, Mittal ML, Horyniak D, Strathdee SA, Werb D. Injection drug use trajectories among migrant populations: a narrative review. Subst Use Misuse. (2018) 2018:1–13. doi: 10.1080/10826084.2017.1416404
14. Robertson AM, Ojeda VD, Nguyen L, Lozada R, Martínez GA, Strathdee SA, et al. Reducing harm from HIV/AIDS misconceptions among female sex workers in Tijuana and Ciudad Juarez, Mexico: a cross sectional analysis. Harm Reduct J. (2012) 9:35. doi: 10.1186/1477-7517-9-35
15. Servin AE, Brouwer KC, Gordon L, Rocha-Jimenez T, Staines H, Vera-Monroy RB, et al. Vulnerability factors and pathways leading to underage entry into sex work in two Mexican-US border cities. J Appl Res Child. (2015) 6:1.
16. Nowotny KM, Cepeda A, Perdue T, Negi N, Valdez A. Risk environments and substance use among Mexican female sex work on the US–Mexico border. J Drug Issues. (2017) 47:528–42. doi: 10.1177/0022042616678609
17. Semple SJ, Pitpitan EV, Chavarin CV, Strathdee SA, Mendoza DV, Aarons GA, et al. Correlates of unprotected sex with male clients among female sex workers in 13 Mexican cities. Glob Public Health. (2017) 12:1538–52. doi: 10.1080/17441692.2016.1206603
18. Servin AE, Muñoz FA, Zúñiga ML. Healthcare provider perspectives on barriers to HIV-care access and utilisation among Latinos living with HIV in the US-Mexico border. Cult Health Sex. (2014) 16:587–99. doi: 10.1080/13691058.2014.886131
19. Carrillo G, Uribe F, Lucio R, Ramirez Lopez A, Korc M. The United States–Mexico border environmental public health: the challenges of working with two systems. Rev Panam Salud Publica. (2017) 41:e98.
20. Bravo-García E, Ortiz-Pérez H. Analysis of HIV/AIDS mortality in Mexico from 1990 to 2013: an assessment of the feasibility of millennium development goals by 2015. Gac Med Mex. (2016) 152:819–30.
21. AIDSVu. HIV Statistics Map. (2018). Available online at: http://map.aidsvu.org/map?state=CA (accessed April 15, 2018).
22. Macchione N, Wooten W, Waters-Montijo K, McDonald E. HIV/AIDS Epidemiology Report 2015: San Diego County. San Diego (2016). Available online at: https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/phs/documents/HIV__Epi__Report__2015__FINAL.PDF (accessed September 19, 2018).
23. San Diego Association of Governments (SANDAG). San Diego–Baja California Land Ports Of Entry: Fact Sheet. (2003). Available online at: http://sandiegohealth.org/sandag/sandag__pubs__2009-7-25/publicationid__1184__5148.pdf (accessed September 19, 2018).
24. Servin AE, Muñoz FA, Strathdee SA, Kozo J, Zúñiga ML. Choosing sides: HIV health care practices among shared populations of HIV-positive Latinos living near the US-Mexico border. J Int Assoc Physicians AIDS Care. (2012) 11:348–55. doi: 10.1177/1545109712453854
25. Krogstad JM Posts. U.S. Hispanic Population Growth Has Leveled Off. Pew Research Center. (2017). Available online at: http://www.pewresearch.org/fact-tank/2017/08/03/u-s-hispanic-population-growth-has-leveled-off/. Published August 3, 2017 (accessed September 19, 2018).
26. Shedlin MG, Anastasi JK, Decena CU, Rivera JO, Beltran O, Smith K. Use of complementary and alternative medicines and supplements by Mexican-origin patients in a U.S.-Mexico border HIV clinic. J Assoc Nurses AIDS Care. (2013) 24:396–410. doi: 10.1016/j.jana.2012.07.001
27. Bahall M. Prevalence, patterns, and perceived value of complementary and alternative medicine among HIV patients: a descriptive study. BMC Complement Altern Med. (2017) 17:422. doi: 10.1186/s12906-017-1928-4
28. Lee LS, Andrade AS, Flexner C. Interactions between natural health products and antiretroviral drugs: pharmacokinetic and pharmacodynamic effects. Clin Infect Dis. (2006) 43:1052–9. doi: 10.1086/507894
29. Lorenc A, Robinson N. A review of the use of complementary and alternative medicine and HIV: issues for patient care. AIDS Patient Care STDS. (2013) 27:503–10. doi: 10.1089/apc.2013.0175
30. Rivera JO, González-Stuart A, Ortiz M, Rodríguez JC, Anaya JP, Meza A. Herbal product use in non-HIV and HIV-positive Hispanic patients. J Natl Med Assoc. (2005) 97:1686–91.
31. Sandberg JC, Quandt SA, Graham A, Stub T, Mora DC, Arcury TA. Medical pluralism in the use of sobadores among Mexican immigrants to North Carolina. J Immigr Minor Health. (2018) 20:1197–205. doi: 10.1007/s10903-017-0660-y
32. Muñoz FA, Servin AE, Kozo J, Lam M, Zúñiga ML. A binational comparison of HIV provider attitudes towards the use of complementary and alternative medicine among HIV-positive Latino patients receiving care in the US-Mexico border region. AIDS Care. (2013) 25:990–7. doi: 10.1080/09540121.2012.729806
33. Chan PA, Rose J, Maher J, Benben S, Pfeiffer K, Almonte A, et al. A latent class analysis of risk factors for acquiring HIV among men who have sex with men: implications for implementing pre-exposure prophylaxis programs. AIDS Patient Care STDS. (2015) 29:597–605. doi: 10.1089/apc.2015.0113
34. Brantley ML, Kerrigan D, German D, Lim S, Sherman SG. Identifying patterns of social and economic hardship among structurally vulnerable women: a latent class analysis of HIV/STI Risk. AIDS Behav. (2017) 21:3047–56. doi: 10.1007/s10461-017-1673-1
35. Bohora S, Chaffin M, Shaboltas A, Bonner B, Isurina G, Batluk J, et al. Latent class analysis of HIV risk behaviors among Russian women at risk for alcohol-exposed pregnancies. AIDS Behav. (2017) 21(Suppl 2):243–52. doi: 10.1007/s10461-017-1929-9
36. Meacham MC, Rudolph AE, Strathdee SA, Rusch ML, Brouwer KC, Patterson TL, et al. Polydrug use and HIV risk among people who inject heroin in Tijuana, Mexico: a latent class analysis. Subst Use Misuse. (2015) 50:1351–9. doi: 10.3109/10826084.2015.1013132
37. Meacham MC, Roesch SC, Strathdee SA, Lindsay S, Gonzalez-Zuniga P, Gaines TL. Latent classes of polydrug and polyroute use and associations with human immunodeficiency virus risk behaviours and overdose among people who inject drugs in Tijuana, Baja California, Mexico. Drug Alcohol Rev. (2018) 37:128–36. doi: 10.1111/dar.12524
38. Shiu K, Brincks AM, Feaster DJ. Patterns of substance use and arrest among hospitalized people living with HIV: a latent class analysis [abstract]. Drug Alcohol. (2017) 171:e189–90. doi: 10.1016/j.drugalcdep.2016.08.519
39. Noor SW, Ross MW, Lai D, Risser JM. Use of latent class analysis approach to describe drug and sexual HIV risk patterns among injection drug users in Houston, Texas. AIDS Behav. (2014) 18(Suppl. 3):276–83. doi: 10.1007/s10461-014-0713-3
40. Roth AM, Armenta RA, Wagner KD, Roesch SC, Bluthenthal RN, Cuevas-Mota J, et al. Patterns of drug use, risky behavior, and health status among persons who inject drugs living in San Diego, California: a latent class analysis. Subst Use Misuse. (2015) 50:205–14. doi: 10.3109/10826084.2014.962661
41. Carter A, Roth EA, Ding E, Milloy MJ, Kestler M, Jabbari S, et al. Substance use, violence, and antiretroviral adherence: a latent class analysis of women living with HIV in Canada. AIDS Behav. (2018) 22:971–85. doi: 10.1007/s10461-017-1863-x
42. Starks TJ, Millar BM, Lassiter JM, Parsons JT. Preintervention profiles of information, motivational, and behavioral self-efficacy for methamphetamine use and HIV medication adherence among gay and bisexual men. AIDS Patient Care STDS. (2017) 31:78–86. doi: 10.1089/apc.2016.0196
43. Phillips KA, Morrison KR, Andersen R, Aday LA. Understanding the context of healthcare utilization: assessing environmental and provider-related variables in the behavioral model of utilization. Health Serv Res. (1998) 33(3 Pt 1):571–96.
44. US Dollar to Mexican Peso Chart: 10 Years. XE. Available online at: https://www.xe.com/currencycharts/?from=USD&to=MXN&view=10Y (accessed July 8, 2018).
45. Brown RE, Goldstein MS. California Health Interview Survey-Complementary and Alternative Medicine Questionnaire: A CHIS 2001 Follow-Back Study. (2003). Available online at: https://healthpolicy.ucla.edu/chis/design/Documents/CHIS2001__chiscam__q.pdf (accessed September 19, 2018).
46. Jimenez JC, Puig M, Ramos JC, Morales M, Asencio G, Sala AC. A new and concise self-administered instrument in Spanish to measure felt-stigma among people living with HIV. In: Presented at the: World AIDS Conference. Mexico City (2008).
47. USAID. Can We Measure HIV/AIDS-Related Stigma and Discrimination? Current Knowledge About Quantifying Stigma in Developing Countries. (2006). Available online at: https://www.icrw.org/wp-content/uploads/2016/10/Can-We-Measure-HIV-Stigma-and-Discrimination.pdf (accessed September 19, 2018).
48. Zúñiga ML, Brennan J, Scolari R, Strathdee SA. Barriers to HIV care in the context of cross-border health care utilization among HIV-positive persons living in the California/Baja California US-Mexico border region. J Immigr Minor Health. (2008) 10:219–27. doi: 10.1007/s10903-007-9073-7
49. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. (1977) 1:385–401. doi: 10.1177/014662167700100306
50. Schneider J, Kaplan SH, Greenfield S, Li W, Wilson IB. Better physician-patient relationships are associated with higher reported adherence to antiretroviral therapy in patients with HIV infection. J Gen Intern Med. (2004) 19:1096–103. doi: 10.1111/j.1525-1497.2004.30418.x
51. Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a monte carlo simulation study. Struct Equ Model. (2007) 14:535–69. doi: 10.1080/10705510701575396
52. Morin R. Trump Threatens to Close the U.S.-Mexico Border Next Week: ‘I’m Not Playing Games'. Politico. (2019). Available online at: https://www.politico.com/story/2019/03/29/trump-close-us-mexico-border-1243493
53. Dibble S. Two Countries, One Insurance Plan: San Diego Workers Find Medical Care in Tijuana. The San Diego Union-Tribune. (2018). Available online at: https://www.sandiegouniontribune.com/news/border-baja-california/sd-me-simnsa-tijuana-20180108-story.html
54. Kapilashrami A, Hankivsky O. Intersectionality and why it matters to global health. Lancet. (2018) 391:2589–91. doi: 10.1016/S0140-6736(18)31431-4
55. Crenshaw K. Demarginalizing the intersection of race and sex: a black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. Univ Chic Leg Forum. (1989) 1989:139–67.
Keywords: border health, complementary and alternative medicine, Latino health equity, HIV/AIDS, ART adherence
Citation: Marks C and Zúñiga ML (2019) CAM Practices and Treatment Adherence Among Key Subpopulations of HIV+ Latinos Receiving Care in the San Diego-Tijuana Border Region: A Latent Class Analysis. Front. Public Health 7:179. doi: 10.3389/fpubh.2019.00179
Received: 19 October 2018; Accepted: 13 June 2019;
Published: 28 June 2019.
Edited by:
Shane Andrew Thomas, Shenzhen International Primary Healthcare Research Institute, ChinaReviewed by:
Nilesh Chandrakant Gawde, Tata Institute of Social Sciences, IndiaCarleen Harriet Stoskopf, San Diego State University, United States
Copyright © 2019 Marks and Zúñiga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Charles Marks, cmarks@sdsu.edu; María Luisa Zúñiga, mlzuniga@mail.sdsu.edu