 Paulina Maravilla-Herrera1
Paulina Maravilla-Herrera1 María Merino1*Santiago Alfonso Zamora2Jesús Balea Filgueiras3
María Merino1*Santiago Alfonso Zamora2Jesús Balea Filgueiras3 José Manuel Carrascosa Carrillo4Olga Delgado Sánchez5,6Francisco Dolz Sinisterra7Antonio García-Ruiz8
José Manuel Carrascosa Carrillo4Olga Delgado Sánchez5,6Francisco Dolz Sinisterra7Antonio García-Ruiz8 Pedro Herranz Pinto9Antonio Manfredi2José Martínez Olmos10Paloma Morales de los Ríos Luna11
Pedro Herranz Pinto9Antonio Manfredi2José Martínez Olmos10Paloma Morales de los Ríos Luna11 Lluís Puig12,13Sandra Ros14Álvaro Hidalgo-Vega15,16
Lluís Puig12,13Sandra Ros14Álvaro Hidalgo-Vega15,16- 1Department of Health Outcomes Research, Weber, Madrid, Spain
- 2Department of Management, Psoriasis and Psoriatic Arthritis Patient and Family Association (Acción Psoriasis), Barcelona, Spain
- 3Department of Pharmacy, Ferrol University Hospital Complex, La Coruña, Spain
- 4Department of Dermatology, Germans Trias i Pujol University Hospital, Badalona, Spain
- 5Department of Management, Spanish Society of Hospital Pharmacy (SEFH), Madrid, Spain
- 6Department of Pharmacy, Son Espases University Hospital, Illes Balears, Spain
- 7Department of Management, Doctor Peset University Hospital, Valencia, Spain
- 8Health Economics and Rational Use of Medicines, Department of Pharmacology and Clinical Therapeutics, Biomedical Research Institute of Malaga (IBIMA), University of Malaga, Malaga, Spain
- 9Department of Dermatology, La Paz University Hospital, Madrid, Spain
- 10Andalusian Public Health School (EASP), Granada, Spain
- 11Department of Nursing, Gregorio Marañón University Hospital, Madrid, Spain
- 12Department of Dermatology, Santa Creu i Sant Pau Hospital, Barcelona, Spain
- 13Universitat Autònoma de Barcelona, Barcelona, Spain
- 14Psychologist, Departments of Dermatology and Rheumatology, and Cardiac Transplant Unit, Santa Creu i Sant Pau Hospital, Barcelona, Spain
- 15Department of Economic Analysis and Finances, University of Castilla-La Mancha, Toledo, Spain
- 16Fundación Weber, Madrid, Spain
Introduction: Psoriasis is a chronic disease involving the skin, which significantly impacts the quality of life. Disease severity and treatment efficacy (i.e., response) are assessed through the Psoriasis Area and Severity Index (PASI). A PASI 75 response, i.e., an improvement of at least 75% with respect to the baseline PASI score, has traditionally been used as a therapeutic benchmark in clinical trials. Therapeutic advances have made PASI 90 or PASI 100 responses possible in most patients treated with some biologics. A greater response may generate social value beyond clinical outcomes that would benefit both patients and society.
Methods: A 1-year economic model was applied to estimate the impact of having a PASI 75, PASI 90, or PASI 100 response in four areas of analysis (quality of life, activities of daily living, work productivity, and out-of-pocket expenditures) and the social value of having a PASI 90 or PASI 100 response in comparison with a PASI 75 response. A mixed-methods approach based on the scientific literature, a focus group with patient, and an advisory committee with psoriasis stakeholders was used. The model included three different scenarios: having a PASI 90 vs a PASI 75 response; a PASI 100 vs a PASI 90 response; and a PASI 100 vs a PASI 75 response. A sensitivity analysis was included.
Results: The annual economic impact per patient with moderate-to-severe plaque psoriasis having a PASI 75 response was estimated at Ł 6,139, mainly related to labour productivity losses and quality of life reductions. Having a PASI 90 or a PASI 100 response would reduce this impact to €3,956 or €1,353, respectively. Accordingly, the social value of having a PASI 90 instead of a PASI 75 response was estimated at €2,183, and €4,786 with a PASI 100 response.
Discussion: A PASI 90 or PASI 100 response would have a lower economic impact and a greater social value than a PASI 75 response for patients with moderate-to-severe plaque psoriasis.
1. Introduction
Psoriasis is a chronic non-communicable disease that can cause systemic inflammation and is associated with multiple comorbidities (1). It is a painful, pruritic, and disabling disease that involves the skin and nails, causing a significant impact on the quality of life of patients (1). Psoriasis can occur at any age but normally appears before the age of 40 (2). Approximately 2.3% of the Spanish population is affected by this condition; plaque psoriasis is the most common form of psoriasis accounting for 90% of all cases (3, 4).
The clinical diagnosis of psoriasis is based on the assessment of the patient's history and the presence of skin lesions with characteristic morphology and distribution (5). Disease severity is usually assessed through the Psoriasis Area and Severity Index (PASI), which combines an evaluation of the severity of the lesions with erythema, infiltration, and peeling, scored on a scale of 0 to 4 (0 = none, 1 = mild, 2 = moderate, 3 = marked, and 4 = very marked) and the percentage of skin involved on the head, trunk, upper limbs, and lower limbs. Moderate or severe disease can be defined by a PASI score of 5–10 or a PASI score of >10, respectively (6). In Spain, 29.5% of patients with psoriasis have a diagnosis of moderate-to-severe plaque psoriasis (7). According to this data, nearly 300,000 inhabitants of Spain suffer from moderate-to-severe plaque psoriasis (7).
Moreover, the PASI is also used to assess the efficacy of treatment. For example, a PASI 75 response means an improvement in the PASI score of at least 75% with respect to the baseline (pre-treatment) PASI score (6). Previously, achieving a PASI 75 response was considered a relevant therapeutic goal, yet nowadays achieving a PASI 90 response or even a PASI 100 response is possible given recent therapeutic advances (5, 8–10). Accordingly, the optimal therapeutic response may be defined by the equivalent of PASI 90 or PASI 100 responses in clinical trials. The course of the disease, the morphology, the severity, and the body surface area involved are different for each patient and may not only have an impact on the clinical dimension but also the personal, work-life, social, and intimacy dimensions of the patient (10–13). Therefore, disease management should be personalized and patient-centered, with a clear therapeutic goal agreed upon between clinician and patient (1).
According to the literature, benefits outside the clinical dimension may be achieved by setting more ambitious therapeutic objectives, as patients with improved skin clearance further report emotional, psychological, and social functioning improvements (14–16). Accordingly, the economic impact (i.e., related costs) associated with a poor quality of life or work productivity losses in psoriasis patients who have not achieved an optimal therapeutic response may be reduced by increasing the degree of response. Therefore, achieving a PASI 90 or PASI 100 response in patients with moderate-to-severe plaque psoriasis may reduce this economic impact, which translates into a social value gain. Estimating the social value from a holistic perspective can help to understand how achieving a greater PASI response may improve different aspects of the patients' lives, considering both tangible and intangible aspects that are meaningful for patients.
To our knowledge, no other study to date has analyzed the social value of achieving a PASI 90 or PASI 100 response in patients with moderate-to-severe plaque psoriasis in Spain.
2. Materials and methods
An economic model with a one-year time horizon was applied to estimate the economic impact of having achieved a PASI response of 75, 90 or 100, and the social value of having achieved a complete or almost complete response in patients with moderate-to-severe plaque psoriasis in Spain. The economic impact was estimated from a social perspective and included costs related to the following four areas of analysis: (1) reduction in quality of life (including the need for informal care and quality-adjusted life-years lost because of the disease); (2) impact on activities of daily living, defined by the activities patients stop doing or their willingness to pay to improve this sphere; (3) work productivity losses, i.e., missing working hours due to the disease (medical visits and/or sick leaves); and (4) psoriasis-related out-of-pocket expenditures; in three different response scenarios: (1) a PASI 75 response compared to a PASI 90 response; (2) a PASI 90 response compared to a PASI 100 response; and (3) a PASI 75 compared to a PASI 100 response (Figure 1).
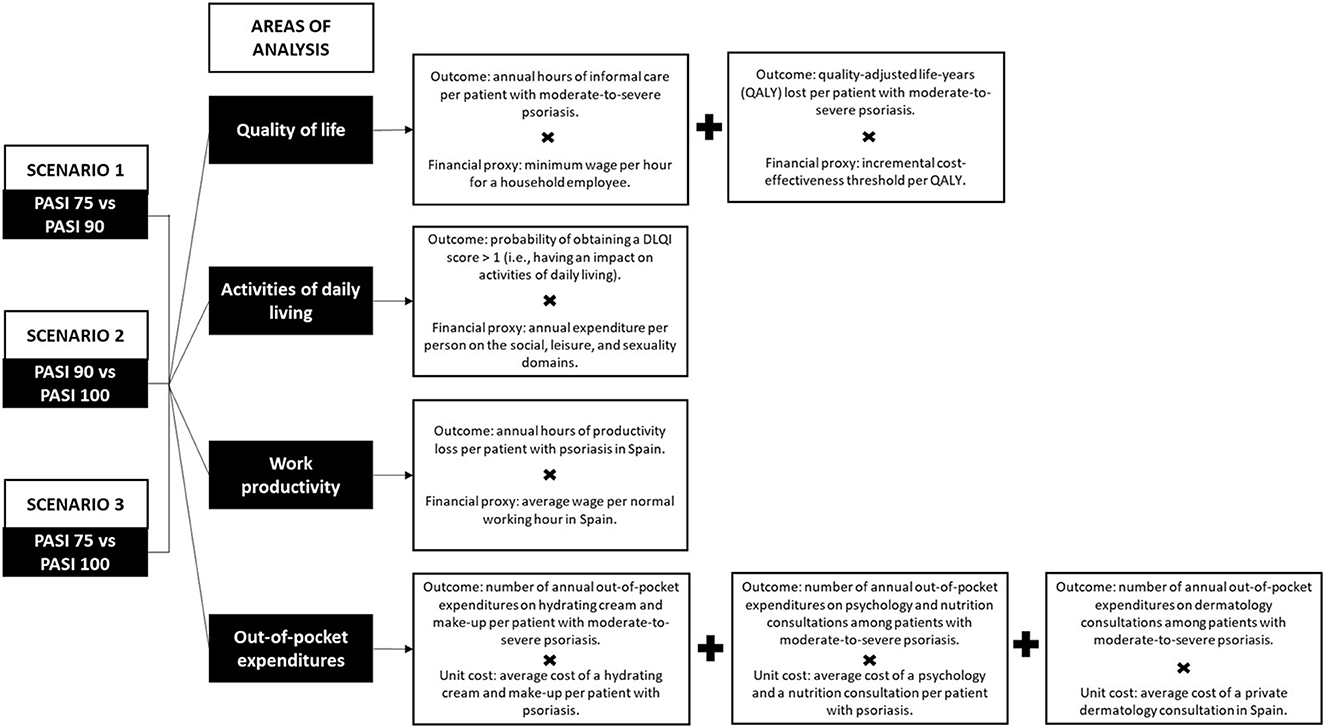
Figure 1. PASI scenarios and areas of analysis.
The economic impact generated by a patient with a PASI 75, PASI 90, or PASI 100 response was estimated by multiplying the outcomes associated with presenting each response (Table 1) by their financial value or financial proxy (Table 2) within each area of analysis (Figure 1). Moreover, the social value was estimated by subtracting the economic impact (i.e., associated costs) of presenting a PASI 75 or PASI 90 response from the economic impact of a more complete response, according to the three different scenarios (Figure 1). Both the economic impact and the social value are reported per patient and year, expressed in 2021 euros (€). Unit prices prior to 2021 were updated to the year 2021 according to the corresponding general or medical Consumer Price Index whenever needed (20).
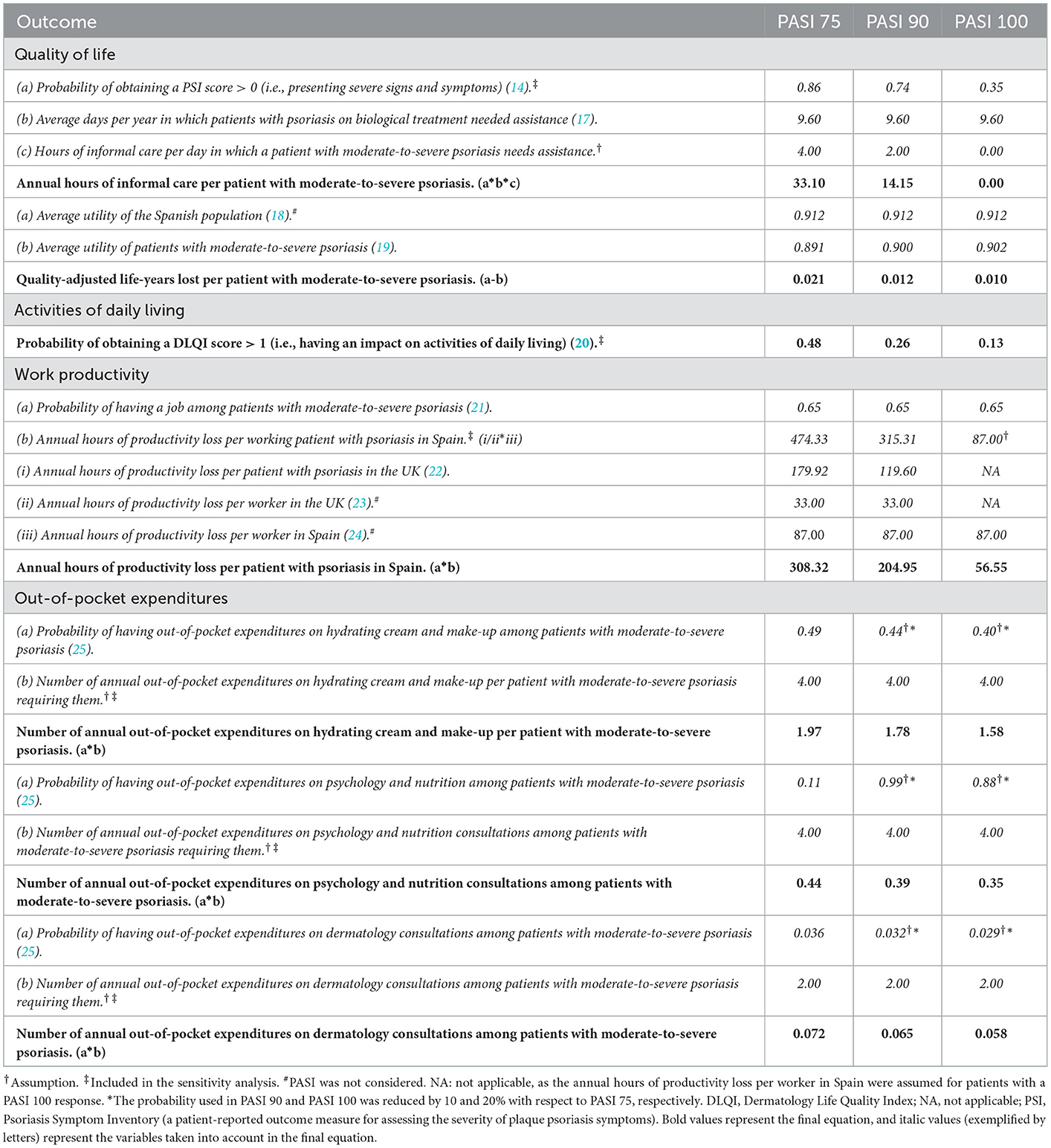
Table 1. Outcomes by areas of analysis and PASI responses.
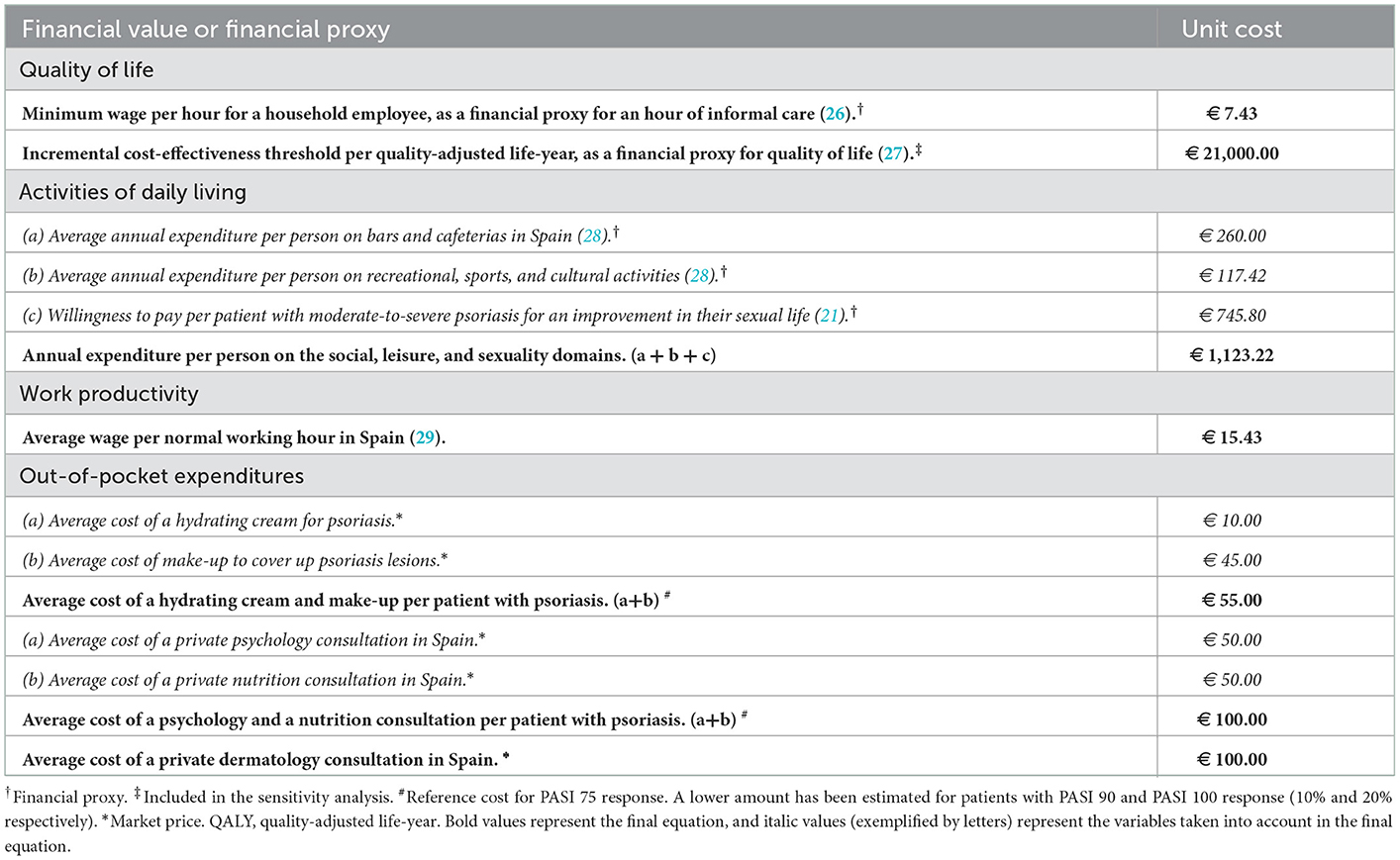
Table 2. Financial values or proxies by areas of analysis.
The economic model was developed using a mixed-methods approach to gather relevant information from the scientific literature, a focus group (FG) with patients, and an advisory committee with experts. First of all, a literature review was carried out on the PubMed® search engine by combining PASI response terms (PASI 75, PASI 90, and PASI 100) and their synonyms with an extensive list of impact terms (cost, resource, impairment, pain, itch, burn, sting, cracking, redness, scaling, flaking, anxiety, depression, caregiving, work productivity, activities of daily living, quality of life, suicide, bullying, sex, relationships, and leisure) and their synonyms through AND/OR Boolean operators, to identify and extract data on the economic impact of having achieved a PASI 75, PASI 90, or PASI 100 response. The search retrieved 383 studies of which 14 were selected as they included relevant information in line with the purpose of the study. These studies did not include information on the impact on healthcare resource consumption and costs generated by patients with different PASI responses.
Thereafter, a FG comprising six patients with moderate-to-severe psoriasis from different regions in Spain was carried out to understand the impact of the disease on the patients' lives, especially within the four areas of analysis, their unmet needs, their willingness to pay for symptom improvement, and their perceived benefits of having obtained a PASI 90 or PASI 100 response in terms of quality of life, physical and emotional state, labor productivity, activities of daily living, informal care, and out-of-pocket expenditures. Finally, an advisory committee comprising a multidisciplinary group of twelve experts representing the main stakeholders regarding psoriasis in Spain (dermatologists, nurses, psychologists, pharmacists, hospital managers, health economists, policymakers, and patients) was created to discuss and agree on the most appropriate inputs, obtained from the literature review and the FG (e.g., study selection based on the quality of the methods), that would be included in the model to quantify the social value of a PASI 90 or PASI 100 response with respect to a PASI 75 response.
In the absence of relevant data, sensible assumptions were made following a conservative approach, supported by the scientific literature and validated by the advisory committee. A sensitivity analysis was carried out to test the strength of the model when varying assumptions as follows: the reference scenario, the lower limit or best-case scenario (that which would result in a lower impact) and the upper limit or worst-case scenario (that which would result in a greater impact). Outcomes, financial values, or financial proxies included in the sensitivity analysis are displayed in Table 3.
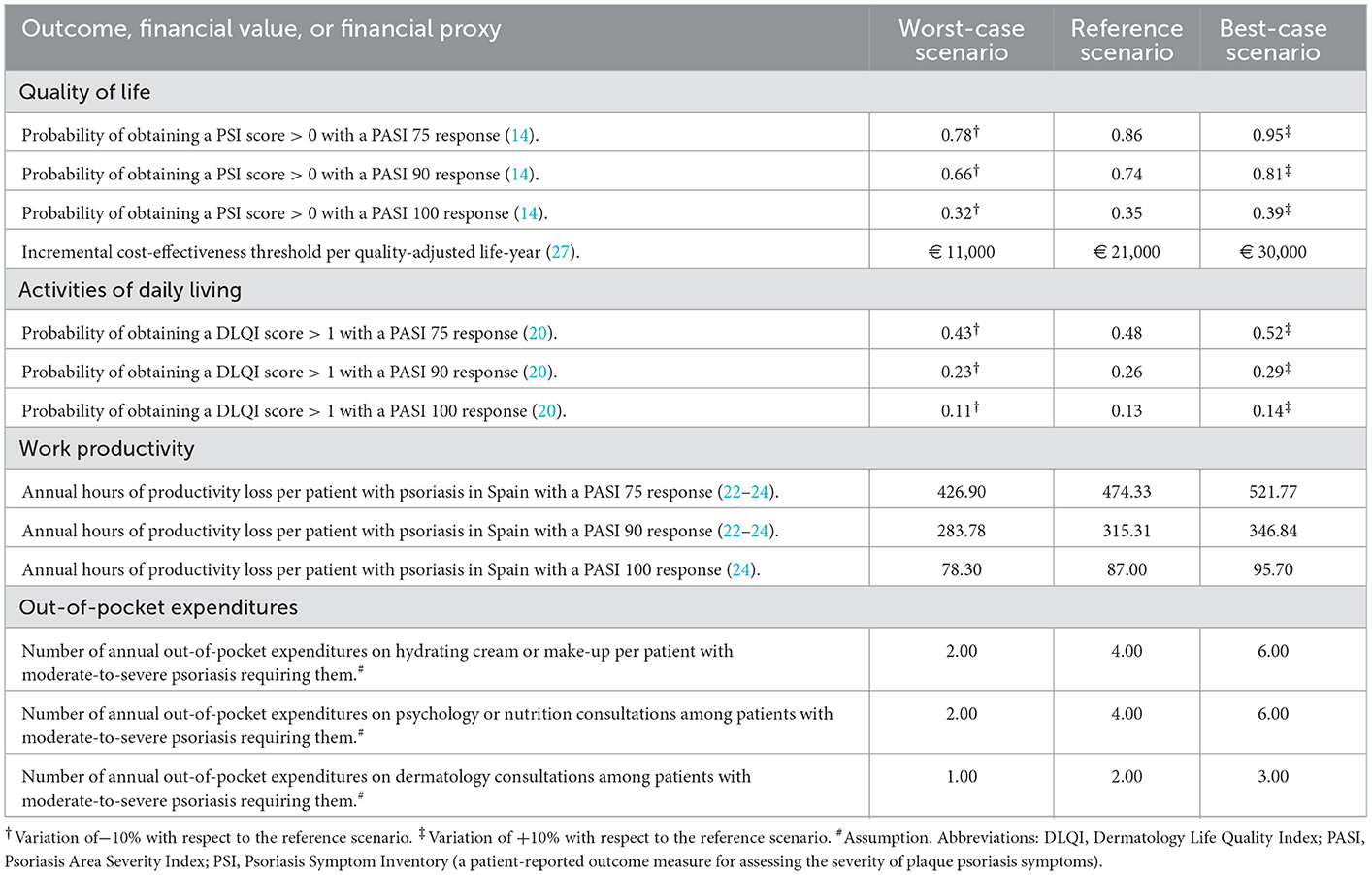
Table 3. Outcomes, financial values, or financial proxies included in the sensitivity analysis.
Given the nature of this study, approval by an institutional review board or an ethical review board was not required. Nevertheless, study procedures were in accordance with the Declaration of Helsinki 1975/83.
3. Results
The annual economic impact of having a PASI 75 response in patients with moderate-to-severe psoriasis was estimated at € 6,139 per patient. A PASI 90 response would result in a smaller economic impact (€ 3,956) and even lower with a PASI 100 response or completely clear skin, estimated at € 1,353 per patient (Table 4).
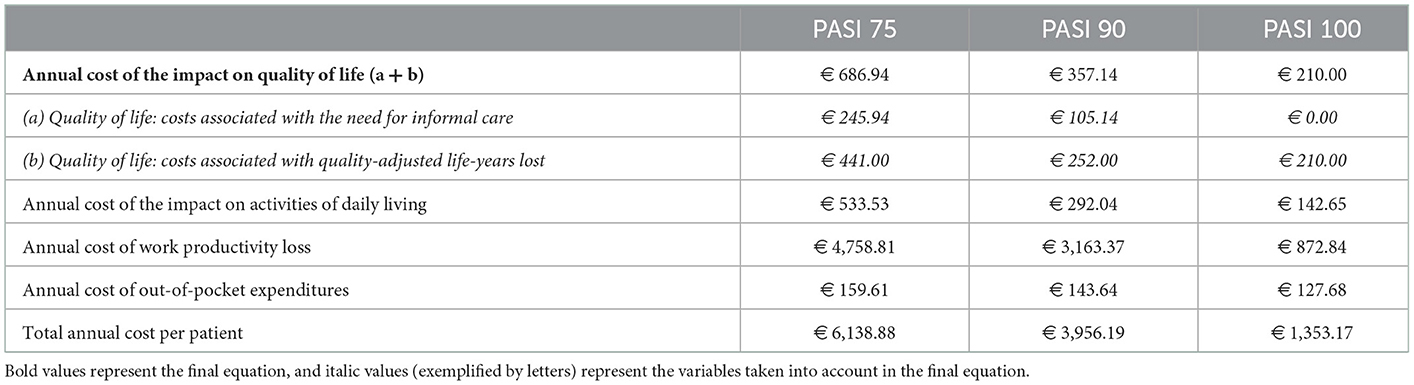
Table 4. Economic impact by area of analysis and PASI response in the reference scenario.
Regarding the quality of life associated with the need for informal care, a PASI 75 response would involve an annual cost of € 246, higher than the estimated cost associated with a PASI 90 response (€ 105). On the contrary, patients with PASI 100 response would not generate informal care costs. Similarly, the economic impact associated with the number of quality-adjusted life-years lost by patients with moderate-to-severe psoriasis would be higher in those with a PASI 75 response (€ 441) than in those with a PASI 90 or PASI 100 response (€ 252 and € 210, respectively) (Table 4).
Concerning the impact of moderate-to-severe psoriasis in activities of daily living, according to the results in Table 4, a PASI 75 response would have a higher economic impact (€ 534) than a PASI 90 (€ 292) or PASI 100 response (€ 143).
Regarding work productivity losses in patients with moderate-to-severe psoriasis, the associated economic impact would be higher in those patients with a PASI 75 response (€ 4,759), compared with a PASI 90 (€ 3,163) and PASI 100 response (€ 873) (Table 4).
Finally, patients with a PASI 75 response would generate an annual cost of € 160 in out-of-pocket expenditures, slightly more than those with a PASI 90 or PASI 100 response (€ 144 and € 128, respectively) (Table 4).
Concerning the social value, obtaining a PASI 90 response instead of a PASI 75 response would represent an added social value of € 2,183 and more than double with a PASI 100 response (€ 4,786). Additionally, obtaining a PASI 100 response instead of a PASI 90 response would imply an additional social value of € 2,603 (Figure 2). This tendency was observed in all four areas of analysis.
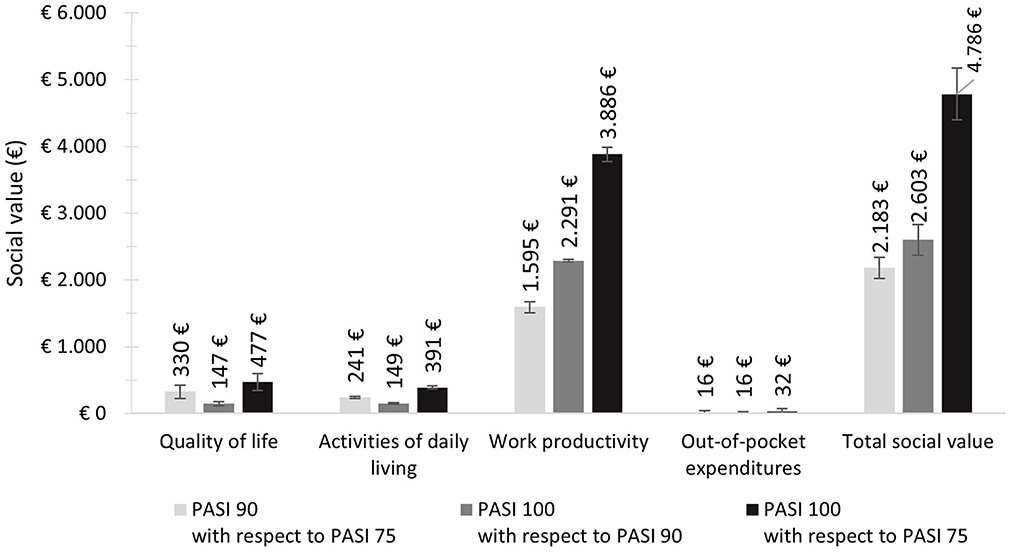
Figure 2. Potential social value according to PASI scenarios, areas of analysis, and total.
The greatest proportion of the social value attained when obtaining a PASI 90 or PASI 100 response instead of a PASI 75 response would be attributed to work productivity gains (73.1 and 81.2% of the social impact, respectively). Similarly, 88% of the social value attained when obtaining a PASI 100 response instead of a PASI 90 response would be attributed to work productivity gains. Improvements in the quality of life, activities of daily living, and reductions in out-of-pocket expenditures would account for 15.1, 11.1, and 0.7% of the total social value attained when obtaining a PASI 90 response instead of a PASI 75 response, and for 10, 8.2, and 0.7% of the social value attained when obtaining a PASI 100 response instead of a PASI 75 response. For those patients obtaining a PASI 100 response instead of a PASI 90 response, the social value in these areas would be 5.7, 5.7, and 0.6%, respectively (Figure 3).
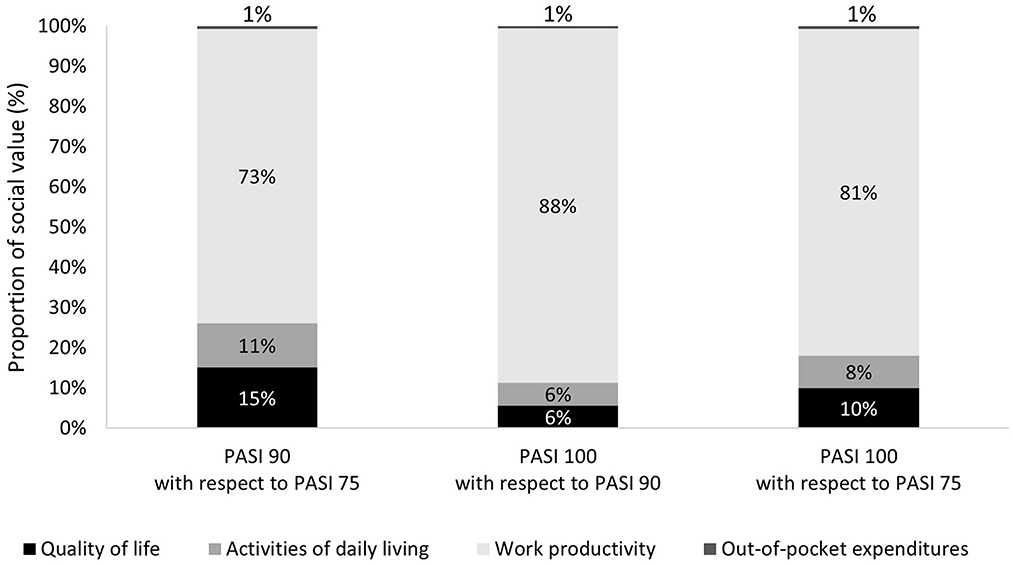
Figure 3. Distribution of social value according to areas of analysis and PASI scenarios.
According to the sensitivity analysis, the greatest variability of the economic impact was associated with a PASI 100 response, which could decrease by 20% to € 1,088, or increase by 23% to € 1,609. Meanwhile, the economic impact associated with a PASI 75 or PASI 90 response could decrease by 14% in the worst-case scenario or increase by 16% in the best-case scenario. The corresponding social value would vary accordingly.
4. Discussion
Having a PASI 90 or PASI 100 response would generate a higher social value and have a lower economic impact for patients with moderate-to-severe plaque psoriasis compared with a PASI 75 response. According to the overall results, the economic impact of a PASI 75 response would be 66 and 78% higher than PASI 90 or 100 response, respectively.
In terms of quality of life, this study aligns with previous research indicating that psoriasis patients with greater improvements from the baseline PASI scores are less severely affected, have reduced symptomatology, and consequently present a better quality of life (14, 20, 30). On one hand, this impact may be reflected as the cost of informal care or assistance in activities of daily living. According to the information collected from the FG and the scientific literature, psoriasis symptomatology interferes with household and basic activities, therefore some patients may need help to accomplish them (17). On the other hand, Pickard et al. (19) indicated that the utility of patients that achieved a PASI 75 response was slightly smaller than for patients who achieved a PASI 90 or PASI 100 response. Regarding the quality of life, the results of the present study estimated that if a patient achieves a PASI 90 or 100 response, instead of a PASI 75 response, € 330 and € 477 of social value would be generated per year, respectively.
According to the patients in the FG, the area of activities of daily living generates the largest impact on patients' lives. Not being able to do activities because of lesions in exposed areas (e.g., sports or having intimate relationships, among others) may have a great psychological impact or lead to stigmatization (31). Contrary to the information collected in the FG, this area was not one of major impact, possibly associated with its subjectiveness and difficulty of assessment. Accordingly, results may not reflect the whole impact this area represents on patients. One of the most frequently used methods to assess this is contingent valuation through the willingness to pay. Several studies have observed that in patients with dermatologic conditions, willingness to pay for improving certain spheres of their lives (including activities of daily living) could vary when treatment improved their condition (32–35). Accordingly, the results of the present study showed a greater economic impact associated with a PASI 75 response (€ 534) than that of a PASI 90 (€ 292) or PASI 100 response (€ 143).
The greatest impact of psoriasis has been associated with the area of work productivity, as previous studies have shown that productivity losses reflect the overall impact of psoriasis (22, 36, 37). According to our results, achieving a PASI 90 or PASI 100 response, compared to a PASI 75 response, would translate into an additional social value of € 1,595 and € 3,886, respectively.
Concerning out-of-pocket expenditures, despite psoriasis treatment being covered by the Spanish National Health System, there is still room for improvement. Health services may vary depending on the area of residence or may not cover all of the patient's needs, having them pay to address them on their own (38). According to Richard et al. (25) out-of-pocket expenditures of patients with psoriasis in France were more than twice the expenditures for other medical conditions. In Spain, patients in the FG mentioned that their out-of-pocket expenditures are usually related to private health care (dermatology, psychology, and nutrition), personal care products or services (hydrating cream, make-up, and hairstyling), or special clothing, among others. This situation may imply private financing from the patients that, according to the results, may have a greater impact on patients who only achieve PASI 75 response.
The present study has some limitations. First, there was a lack of scientific literature regarding the impact of psoriasis on patients' lives according to different levels of the PASI response. Relevant information was found in only 14 studies out of 383 revised. Specifically, there was a lack of information on healthcare resource consumption and costs, work productivity, and out-of-pocket expenditures in Spanish psoriasis patients: regarding work productivity losses, British figures were extrapolated to the Spanish context; concerning out-of-pocket expenditures, only those mentioned by patients in the FG were considered. Moreover, the reduced number of studies and the large differences between them further hindered the use of statistical analyses to compare PASI responses. Second, the impact of psoriasis may vary from patient to patient and hence be experienced in different ways according to each reality. Therefore, a conservative approach was adopted when quantifying the economic impact of the disease and the social value of achieving better PASI responses. Finally, despite the small number of representatives of psoriasis patients in the FG and experts in the advisory committee, all data and information collected from these groups were supported by scientific literature. The results in this study should be taken with precaution when interpreted, always considering the sensitivity analysis. In this regard, the sensitivity analysis considered variations in most especially relevant parameters (i.e., ±10% for probabilities), variations based on the scientific literature available, and variations for assumptions based on information provided by the FG. Including the remaining variables in the sensitivity analysis to test the strength of the model would have implied making additional assumptions that may have biased the results and hindered the conservative approach of this study.
Despite these limitations, this study adds an understanding of the impact of the disease from the patient's perspective. Several studies have highlighted the importance of considering the social perspective in health economic analyses since it ideally captures health impacts that are particularly important for the understanding of health interventions and the effects on the population (39–41). Nevertheless, future studies are encouraged to assess the impact of new therapeutic goals on healthcare resource consumption and costs, with respect to the investment required to achieve such goals.
Considering the patient's view may add relevant information to psoriasis-related economic evaluations, giving a wide view of the impact of the disease from a multidimensional perspective.
5. Conclusions
Achieving PASI 90 or PASI 100 responses would have a lower economic impact, in comparison to a PASI 75 response, and hence generate a greater social value in terms of improved quality of life and activities of daily living, and reduced labor productivity losses and out-of-pocket expenditures for patients. This could be very significant not only for patients but also for their families and society at large.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
PM-H, MM, and ÁH-V conceived and designed the research. PM-H and MM acquired the data. PM-H, MM, SA, JB, JC, OD, FD, AG-R, PH, AM, JM, PM, LP, SR, and ÁH-V analyzed and interpreted the data. PM-H developed the original draft of the manuscript and MM substantively reviewed it. All authors critically revised and approved the manuscript.
Funding
This study received funding from UCB Pharma. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Acknowledgments
The authors would like to thank Dr. Teresa Martín Lorenzo for providing scientific writing assistance and all psoriasis patients who participated in this study for their time and contribution. Finally, the authors would like to thank the Acción Psoriasis association for their kind collaboration.
Conflict of interest
PM-H and MM are employed by the consultancy firm Weber, which received funding from UCB Pharma for the development of this project. SA, JB, JC, OD, FD, AG-R, PH, AM, JM, PM, LP, and SR received fees from the consultancy firm Weber for the participation in the project.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
DLQI, Dermatology Life Quality Index; FG, Focus Group; PASI, Psoriasis Area and Severity Index; PSI, Psoriasis Symptom Inventory.
References
1. World Health Organization. Global Report on Psoriasis. (2016). Available online at: https://apps.who.int/iris/handle/10665/204417 (accessed May 31, 2021).
2. Langley RGB, Krueger GG, Griffiths CEM. Psoriasis: epidemiology, clinical features, and quality of life. Ann Rheum Dis. (2005) 64:ii18–23. doi: 10.1136/ard.2004.033217
3. Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. (2007) 370:263–71. doi: 10.1016/S0140-6736(07)61128-3
4. Ferrándiz C, Carrascosa JM, Toro M. Prevalence of psoriasis in Spain in the age of biologics. Actas Dermo-Sifiliográficas. (2014) 105:504–9. doi: 10.1016/j.adengl.2014.04.016
5. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. (2021) 397:1301–15. doi: 10.1016/S0140-6736(20)32549-6
6. Grupo de Trabajo de Psoriasis de la Academia Española de Dermatología y Venereología (AEDV). ¿‘Cómo se mide la gravedad de la psoriasis? Principales índices.
7. Carrascosa J, Pujol R, Daudén E, Hernanz-Hermosa J, Bordas X, Smandia J, et al. A prospective evaluation of the cost of psoriasis in Spain (EPIDERMA project: Phase II). J Eur Acad Dermatol Venereol. (2006) 20:840–5. doi: 10.1111/j.1468-3083.2006.01659.x
8. Strober BE, van der Walt JM, Armstrong AW, Bourcier M, Carvalho AV, Chouela E, et al. Clinical goals and barriers to effective psoriasis care. Dermatol Ther Heidelb. 9:5–18. doi: 10.1007/s13555-018-0279-5
9. Armstrong AW, Betts KA, Signorovitch JE, Sundaram M, Li J, Ganguli AX, et al. Number needed to treat and costs per responder among biologic treatments for moderate-to-severe psoriasis: a network meta-analysis. Curr Med Res Opin. (2018) 34:1325–33. doi: 10.1080/03007995.2018.1457516
10. Ryan C, Sadlier M, De Vol E, Patel M, Lloyd AA, Day A, et al. Genital psoriasis is associated with significant impairment in quality of life and sexual functioning. J Am Acad Dermatol. (2015) 72:978–83. doi: 10.1016/j.jaad.2015.02.1127
11. Wahl A, Loge JH, Wiklund I, Hanestad BR. The burden of psoriasis: a study concerning health-related quality of life among Norwegian adult patients with psoriasis compared with general population norms. J Am Acad Dermatol. (2000) 43:803–8. doi: 10.1067/mjd.2000.107501
12. Møller AH, Erntoft S, Vinding GR, Jemec GB, A. systematic literature review to compare quality of life in psoriasis with other chronic diseases using EQ-5D-derived utility values. Patient Relat Outcome Meas. (2015) 6:167–77. doi: 10.2147/PROM.S81428
13. Villacorta R, Teeple A, Lee S, Fakharzadeh S, Lucas J, McElligott S, et al. multinational assessment of work-related productivity loss and indirect costs from a survey of patients with psoriasis. Br J Dermatol. (2020) 183:548–58. doi: 10.1111/bjd.18798
14. Lacour J-P, Bewley A, Hammond E, Hansen JB, Horne L, Paul C, et al. Association between patient- and physician-reported outcomes in patients with moderate-to-severe plaque psoriasis treated with biologics in real life (PSO-BIO-REAL). Dermatol Ther. (2020) 10:1099–109. doi: 10.1007/s13555-020-00428-1
15. Honma M, Cai Z, Burge R, Zhu B, Yotsukura S, Torisu-Itakura H. Relationship between rapid skin clearance and quality of life benefit: post hoc analysis of japanese patients with moderate-to-severe psoriasis treated with Ixekizumab (UNCOVER-J). Dermatol Ther. (2020) 10:1397–404. doi: 10.1007/s13555-020-00441-4
16. Puig L, Thom H, Mollon P, Tian H, Ramakrishna GS. Clear or almost clear skin improves the quality of life in patients with moderate-to-severe psoriasis: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol. (2017) 31:213–20. doi: 10.1111/jdv.14007
17. Polistena B, Calzavara-Pinton P, Altomare G, Berardesca E, Girolomoni G, Martini P, et al. The impact of biologic therapy in chronic plaque psoriasis from a societal perspective: an analysis based on Italian actual clinical practice. J Eur Acad Dermatol Venereol JEADV. (2015) 29:2411–6. doi: 10.1111/jdv.13307
18. Instituto Nacional de Estadística. Encuesta Nacional de Salud 2011–2012. Cuestionario de Adultos. (2012). Available online at: https://www.mscbs.gob.es/estadisticas/microdatos.do (accessed Oct 30, 2018).
19. Pickard AS, Gooderham M, Hartz S, Nicolay C. EQ-5D health utilities: exploring ways to improve upon responsiveness in psoriasis. J Med Econ. (2017) 20:19–27. doi: 10.1080/13696998.2016.1219359
20. Blauvelt A, Sofen H, Papp K, Gooderham M, Tyring S, Zhao Y, et al. Tildrakizumab efficacy and impact on quality of life up to 52 weeks in patients with moderate-to-severe psoriasis: a pooled analysis of two randomized controlled trials. J Eur Acad Dermatol Venereol. (2019) 33:2305–12. doi: 10.1111/jdv.15862
21. Carretero G, Moreno D, González Domínguez A, Trigos D, Ledesma A, Sarquella E, et al. Multidisciplinary approach to psoriasis in the Spanish National Health System: A social return on investment study. Glob Reg Health Technol Assess. (2020) 7:50–6. doi: 10.33393/grhta.2020.2146
22. Warren RB, Halliday A, Graham CN, Gilloteau I, Miles L, McBride D. Secukinumab significantly reduces psoriasis-related work impairment and indirect costs compared with ustekinumab and etanercept in the United Kingdom. J Eur Acad Dermatol Venereol JEADV. (2018) 32:2178–84. doi: 10.1111/jdv.15094
23. Office for National Statistics. Sickness absence in the UK labour market—Office for National Statistics. (2020). Available online at: https://www.ons.gov.uk/employmentandlabourmarket/peopleinwork/labourproductivity/articles/sicknessabsenceinthelabourmarket/2020 (accessed Jan 2, 2022).
24. Blasco de Luna FJ, Barceló Larran D, Blázquez Agudo EM, Checa Martín JL, Cirujano González A, Pendás Pevida E, et al. VIII Informe Adecco sobre absentismo. Madrid: The Adecco Group Institute. (2019). Available online at: https://www.adeccoinstitute.es/wp-content/uploads/2019/06/VIII-Informe-Absentismo.pdf (accessed Aug 21, 2020).
25. Richard M-A, Paul C, De Pouvourville G, Jullien D, Mahe E, Bachelez H, et al. Out-of-pocket expenditures in France to manage psoriasis in adult patients: results from an observational, cross-sectional, non-comparative, multicentre study. J Eur Acad Dermatol Venereol. (2021) 35:912–8. doi: 10.1111/jdv.17000
26. España. Real Decreto 231/2020, de 4 de febrero, por el que se fija el salario mínimo interprofesional para 2020. BOE núm. 31, de 5 de febrero de 2020. (2020). Available online at: https://www.boe.es/eli/es/rd/2020/02/04/231 (accessed Feb 12, 2020).
27. Ortega Eslava A. Guía de Evaluación Económica e Impacto Presupuestario en los Informes de Evaluación de Medicamentos. Madrid: SEFH, Sociedad Española de Farmacia Hospitalaria (2017).
28. Instituto Nacional de Estadística. Gasto total, gastos medios y distribución del gasto de los hogares. Consumiciones en bares y cafeterías. (2020). Available online at: https://www.ine.es/dynt3/inebase/es/index.htm?padre=3777&capsel=3778 (accessed Jan 2, 2022).
29. Instituto Nacional de Estadística. Encuesta Anual de Estructura Salarial 2016. Resultados Nacionales y por Comunidades Autónomas. Ganancia por hora normal de trabajo. (2016). Available online at: https://www.ine.es/jaxiT3/Datos.htm?t=28205 (accessed Dec 21, 2018).
30. Strober B, Papp KA, Lebwohl M, Reich K, Paul C, Blauvelt A, et al. Clinical meaningfulness of complete skin clearance in psoriasis. J Am Acad Dermatol. (2016) 75:77–82.e7. doi: 10.1016/j.jaad.2016.03.026
31. Jankowiak B, Kowalewska B, Krajewska-Kułak E, Khvorik DF. Stigmatization and quality of life in patients with psoriasis. Dermatol Ther. (2020) 10:285–96. doi: 10.1007/s13555-020-00363-1
32. Schiffner R, Schiffner-Rohe J, Gerstenhauer M, Hofstädter F, Landthaler M, Stolz W. Willingness to pay and time trade-off: sensitive to changes of quality of life in psoriasis patients? Br J Dermatol. (2003) 148:1153–60. doi: 10.1046/j.1365-2133.2003.05156.x
33. Seidler AM, Bayoumi AM, Goldstein MK, Cruz PD, Chen SC. Willingness to pay in dermatology: assessment of the burden of skin diseases. J Invest Dermatol. (2012) 132:1785–90. doi: 10.1038/jid.2012.50
34. Stefanidou M, Evangelou G, Kontodimopoulos N, Koumaki D, Krueger-Krasagakis S-E, Yosipovitch G, et al. Willingness to pay and quality of life in patients with pruritic skin disorders. Arch Dermatol Res. (2019) 311:221–30. doi: 10.1007/s00403-019-01900-5
35. Maymone MBC, Rajanala S, Widjajahakim R, Secemsky E, Saade D, Vashi NA. Willingness-to-pay and time trade-off: the burden of disease in patients with benign hyperpigmentation. J Clin Aesthetic Dermatol. (2019) 12:46–8.
36. Graham CN, Miles L, McBride D, Zhao Y, Herrera V. Estimation of Annual Indirect Costs Associated With Moderate-to-Severe Plaque Psoriasis in the United States. (2016). doi: 10.1016/j.jval.2015.09.547
37. Lebwohl M, Soliman AM, Yang H, Wang J, Freimark J, Puig L. Impact of PASI response on work productivity and the effect of risankizumab on indirect costs using machine learning in patients with moderate-to-Severe psoriasis. J Dermatol Treat. (2021) 33:1–26.
38. Zozaya N, Villoro R, Abdalla F, Alfonso Zamora S, Balea Filgueiras J, Carrascosa Carrillo JM, et al. Unmet needs in the management of moderate-to-severe psoriasis in spain: a multidimensional evaluation. Acta Derm Venereol. (2022) 102:adv00678. doi: 10.2340/actadv.v102.583
39. Wilder-Smith A, Longini I, Zuber PL, Bärnighausen T, Edmunds WJ, Dean N, et al. The public health value of vaccines beyond efficacy: methods, measures and outcomes. BMC Med. (2017) 15:138. doi: 10.1186/s12916-017-0911-8
40. Luyten J, Beutels P. The social value of vaccination programs: beyond cost-effectiveness. Health Aff Proj Hope. (2016) 35:212–8. doi: 10.1377/hlthaff.2015.1088
Keywords: social return, socioeconomic impact, psoriasis, Psoriasis Area and Severity Index (PASI), quality of life, out-of-pocket (OOP) expenses, activities of daily living
Citation: Maravilla-Herrera P, Merino M, Alfonso Zamora S, Balea Filgueiras J, Carrascosa Carrillo JM, Delgado Sánchez O, Dolz Sinisterra F, García-Ruiz A, Herranz Pinto P, Manfredi A, Martínez Olmos J, Morales de los Ríos Luna P, Puig L, Ros S and Hidalgo-Vega Á (2023) The social value of a PASI 90 or PASI 100 response in patients with moderate-to-severe plaque psoriasis in Spain. Front. Public Health 11:1000776. doi: 10.3389/fpubh.2023.1000776
Received: 22 July 2022; Accepted: 09 January 2023;
Published: 26 January 2023.
Edited by:
Hai Fang, Peking University, ChinaReviewed by:
Hongguo Rong, Beijing University of Chinese Medicine, ChinaJose Luis Trillo-Mata, Health Area Pharmacy Manager, Spain
Copyright © 2023 Maravilla-Herrera, Merino, Alfonso Zamora, Balea Filgueiras, Carrascosa Carrillo, Delgado Sánchez, Dolz Sinisterra, García-Ruiz, Herranz Pinto, Manfredi, Martínez Olmos, Morales de los Ríos Luna, Puig, Ros and Hidalgo-Vega. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Merino,  maria.merino@weber.org.es
maria.merino@weber.org.es