 Abraham García-Gil1
Abraham García-Gil1 Beatriz Itzel Hernández-Jurado2Marco Antonio Luna-Ruiz-Esparza1Eduardo Espinoza-Angulo2Héctor Machado-Jiménez2Humberto Gómez-Campaña3
Beatriz Itzel Hernández-Jurado2Marco Antonio Luna-Ruiz-Esparza1Eduardo Espinoza-Angulo2Héctor Machado-Jiménez2Humberto Gómez-Campaña3 Abraham Campos-Romero1
Abraham Campos-Romero1 Jonathan Alcántar-Fernández1*
Jonathan Alcántar-Fernández1*- 1Innovation and Research Department, Salud Digna, Culiacán, Mexico
- 2Optometry Department, Salud Digna, Culiacán, Mexico
- 3Medical Direction, Salud Digna, Culiacán, Mexico
Background: Refractive errors (RE) are the leading cause of visual impairment and blindness worldwide. With ongoing demographic shifts, including population growth, aging, and lifestyle changes, the global prevalence of RE is expected to rise. Robust epidemiological data are essential to mitigate their public health impact. However, in Mexico, comprehensive studies assessing the burden of RE across age groups and regions are scarce.
Objective: This study aimed to characterize the epidemiological profile of RE in Mexico using a large outpatient sample, focusing on geographic distribution and variation by sex and age.
Methods: We analyzed an electronic database of eye examinations from 3.8 million outpatients who attended Salud Digna clinics across Mexico in 2024. Prevalence estimates were calculated with 95% confidence intervals (CIs), and statistical comparisons were performed to assess differences by sex and age.
Results: The overall prevalence of RE was 74.61% (95% CI, 74.57–74.65) with 2,841,067 outpatients affected. Myopia was the most common condition, affecting 1,469,377 outpatients (38.6, 95% CI, 38.54–38.64), followed by hyperopia (1,234,403 affected outpatients, 32.4, 95% CI, 32.37–32.47) and astigmatism (1,205,400 affected outpatients, 31.7, 95% CI, 31.61–31.71). Astigmatism was significantly more prevalent in males across all age groups (p < 0.001). Myopia and hyperopia showed similar prevalence between sexes during childhood and early adulthood, but diverged in later adulthood, with higher rates of myopia in males (p < 0.001) and hyperopia in females (p < 0.001). All three RE types exhibited a marked shift in prevalence in the 40–49 age group. Geographic variation was observed, with central states showing higher astigmatism and myopia prevalences rates whereas coastal states showed higher hyperopia prevalence rates. Notably, a large proportion of outpatients have never undergone an eye examination, indicating substantial gaps in access to care.
Conclusion: This outpatient-based study provides critical insights into the epidemiology of RE in Mexico, revealing significant demographic and geographic disparities. The findings underscore the urgent need for targeted public health strategies to improve access to eye care services, particularly for underserved populations and high-risk age groups.
1 Introduction
Vision impairment arises when an ocular condition impacts the visual system and one or more visual functions (1). It is estimated that at least 2.2 billion individuals globally experience vision impairment, and at least 1 billion cases could have been prevented. Vision impairment predominantly affects individuals in low- and middle-income countries and is more common among older populations (1, 2). The increasing population, aging, lifestyle changes, and urbanization are expected to significantly increase the proportion of individuals living with ocular conditions, visual impairment, and blindness in the coming decades, posing substantial challenges to public health systems (1).
Uncorrected refractive errors are the leading cause of vision impairment, followed by cataracts, age-related macular degeneration, glaucoma, and diabetic retinopathy (3, 4). Refractive errors (RE) are ocular conditions resulting from discrepancies between the eye’s axial length and its dioptric power, leading to blurry vision (5). There are three types of RE: myopia, characterized by excessive dioptric power relative to the eye’s axial length, causing blurry vision of distant objects (nearsightedness) (6), hyperopia, where insufficient dioptric power relative to the eye’s axial length results in blurry vision of nearby objects (farsightedness) (7); and astigmatism, where an irregular corneal surface causes distorted vision of both near and distant objects (7).
The most common symptoms of RE include blurry vision, diplopia, headaches, and asthenopia (8, 9). Given that some of these symptoms may go unnoticed, regular eye examinations are crucial for maintaining optimal visual health. RE is diagnosed through eye examination conducted by vision health professionals. Although RE cannot be cured, timely detection and professional treatment can mitigate vision impairment through corrective measures such as eyeglasses, contact lenses, or ocular surgery (8, 10). Despite the high cost-effectiveness of eyeglasses as a health intervention, it is estimated that globally, only 36% of individuals with RE have access to appropriate eyeglasses (11).
Meta-analyses have estimated that globally, the prevalence of astigmatism in children (14.9%) exceeds that of myopia (11.7%) and hyperopia (4.6%), with a similar pattern observed in adults: astigmatism (40.1%), myopia (26.5%), and hyperopia (30.9%). However, prevalence rates vary significantly between countries (12). Notably, a global analysis of RE prevalence indicated a sustained increase in myopia over time, increasing from 10.4% in 1993 to 34.2% by 2016. East Asia is the most affected region, with an estimated prevalence of 47% among adults aged 20 to 29 years (12). Projections estimate that by 2050, more than 50% of the global population will be affected by myopia (13).
In Latin America, the prevalence of visual impairment associated with UREs is estimated at 1.4% with 7.2 million people affected (14, 15). In Ecuador, UREs contributed to almost 30% of the total cases of visual impairment while contributing to 1.4% of blindness in Colombia, 2.1% in Chile, 2.3% in Brazil, and 5.0% in Venezuela (16).
Significant disparities in the prevalence of RE across different countries, ethnic groups, and age ranges indicate that both age and genetic factors contribute to its development. It has been implicated that genes involved in light response, light processing, and post-transcriptional regulation mediate a retina-to-sclera signaling cascade that may induce a scleral remodeling in response to light stimuli, influencing the onset of RE development (17, 18), which correlates with environmental factors, such as reduced exposure to natural light due to limited outdoor activity and increased near work, which have also been independently associated with the development of RE (5, 12).
Furthermore, outdoor activities have become increasingly limited. At the same time, digital screen use dominates both occupational and recreational time, leading not only to eye strain but also to musculoskeletal complaints, including neck, shoulder, and back pain (19). Nevertheless, as stated by Rosenfield et al. (19) “Perhaps it is not the form of the visual stimulus that matters, but rather factors such as working distance, gaze angle, and the length of time spent viewing the display without breaks.” Beyond vision impairment, RE have a substantial social and economic impact, limiting employment and educational opportunities, and diminishing productivity (1).
The 2020 Population and Housing Census in Mexico reported that 2,691,338 individuals have a visual impairment (20). Additional studies estimate that 11.01 million Mexicans (8.7% of the population) are either blind or have a visual impairment, with RE accounting for 2.61 million cases (21). Unfortunately, Mexico lacks a national registry for individuals with visual health conditions, and existing research has predominantly focused on school-aged children. There is a notable deficiency of nationally representative studies encompassing all age groups and all three types of refractive errors (RE) in relation to the burden of RE in Mexico. This absence of comprehensive, population-based research that includes all age groups and RE types hinders the development of targeted public health strategies.
This study addresses a critical gap by analyzing the largest outpatient dataset of refractive errors (RE) in Mexico to date, collected from Salud Digna, a non-profit institution with over 200 clinics nationwide and the leading provider of eyeglasses in the country since 2015. REs are the leading cause of vision impairment globally, yet they are among the most easily preventable and treatable ocular conditions. Uncorrected REs can progress to avoidable blindness, particularly in underserved populations, making their detection and correction a key priority for global eye health.
Using data from patients examined in 2024, we present a comprehensive analysis of RE prevalence stratified by age, sex, and geographic region. We highlight age-related trends, including a notable inflection point in the 40–49 age group, and report both relative and absolute numbers of affected individuals. These findings aim to inform public health strategies, support screening and treatment programs, and directly contribute to the WHO’s VISION 2030 initiative, which seeks to reduce avoidable blindness and ensure universal access to eye care services (1, 22).
2 Methods
2.1 Study population
In a cross-sectional, retrospective study, we examined anonymized electronic health records from non-cycloplegic eye exams of all eligible outpatients who visited Salud Digna clinics across all 32 Mexican states between 1 January 2024 and 31 December 2024.
Our clinics follow a standardized eye examination procedure, always conducted by a certified optometrist. The process begins with verifying the patient’s identity and completing a clinical history questionnaire. All equipment is meticulously sanitized. If the patient wears corrective lenses, a lensometry test is performed. The patient’s interpupillary and nasopupillary distances are measured, and their uncorrected visual acuity is assessed. A refractometer (AKR550, WAM 800, Essilor Instruments, Paris, France) is used to evaluate the individual’s objective refraction. The optometrist then refines the objective prescription and assesses both distance and near visual acuity. The results of the eye exam, including any refractive errors and recommendations for eyeglass materials and usage, are shared with the patient. If necessary, the patient is referred to an ophthalmologist or a retinography service.
Data collected during eye examinations, including demographic information, were included. A unique, standardized, validated survey was used to collect data from all clinics. Data from the right eye were used throughout the whole study, and RE were defined as follows: myopia, ≤−0.50 diopter (D) spherical equivalent (SE) (6); hyperopia, ≥0.50 D SE (7); astigmatism, ≤ −1.00 D cylinder (7).
2.2 Consent for using information, handling data, and protecting information privacy
Consent for using information from health records was obtained in accordance with the Mexican Federal Law on Personal Data Protection (LFPDPPP, Spanish acronym). Individuals attending Salud Digna clinics agreed to our privacy policy, which includes the use of their information for scientific research purposes. Therefore, specific informed consent from each individual included in this study was not required, as this research involved a cross-sectional analysis of an electronic health registry. Data protection and privacy were managed in accordance with the national laws and guidelines of Mexico. The data were anonymized by assigning a unique ID code to protect the individual’s identity and prevent duplication in subsequent analyses.
2.3 Ethical statement
This study was approved by the Ethical Review and Research Board of Salud Digna (SDI-202503). All methods adhered to the approved guidelines for clinical management information, the Declaration of Helsinki, and the national regulations of the country (Federal Law on Data Privacy Protection). The data were anonymized for the study.
2.4 Statistical analysis
Descriptive statistical analyses were conducted using Microsoft Power Query and Microsoft Excel to summarize demographic and clinical characteristics of the study population. All inferential statistical analyses were performed in R (version 4.4.0) (23). Prevalence estimates and age-adjusted prevalence rates of RE were calculated using the dplyr package (v1.1.4) and the ageadjust.direct() function from the epitools package (v0.5–10.1). Age standardization was performed using the direct method, applying the World Health Organization (WHO) standard population as the reference to minimize age-related bias across Mexican states and between sexes (24).
Exact 95% confidence intervals (CIs) for prevalence proportions were computed using the binom.exact() function from the epitools package, which applies the Clopper-Pearson method based on the binomial distribution. This method was chosen for its accuracy in estimating CIs for proportions.
Chi-square tests for independence were conducted using the chisq.test() function from the base stats package to assess associations between categorical variables. Risk ratios (RRs) and their corresponding 95% CIs were estimated using the riskratio() function from the epitools package, which calculates the ratio of probabilities of the outcome occurring in exposed versus unexposed groups.
To evaluate trends in age-specific prevalence, we applied the chi-squared test for trend using the prop.trend.test() function from the stats package. This test assesses whether there is a statistically significant linear trend in proportions across ordered age groups.
All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant.
3 Results
Between 1 January 2024 and 31 December 2024, 3,807,547 individuals underwent eye examinations at Salud Digna diagnostic clinics. The mean age of the individuals was 42.16 years (SD 19.7); of these, 2,382,045 were female (62.6%) and 1,425,502 were male (37.4%). Among the participants, 1,872,681 (49.2%) declared never having undergone a previous eye examination, and 3,733,240 (98%) indicated that they had not undergone an ophthalmologic evaluation. The most common symptom was blurry vision of distant objects, reported by 2,329,589 individuals (61.2%), followed by blurry vision of near objects reported by 1,879,567 (49.4%), while 679,827 (17.9%) reported no symptoms. Additionally, 366,087 and 471,602 (9.6 and 12.4%, respectively) of the overall individuals declared having a previous diabetes or high blood pressure diagnosis. Table 1 summarizes the characteristics of the individuals included in this study.
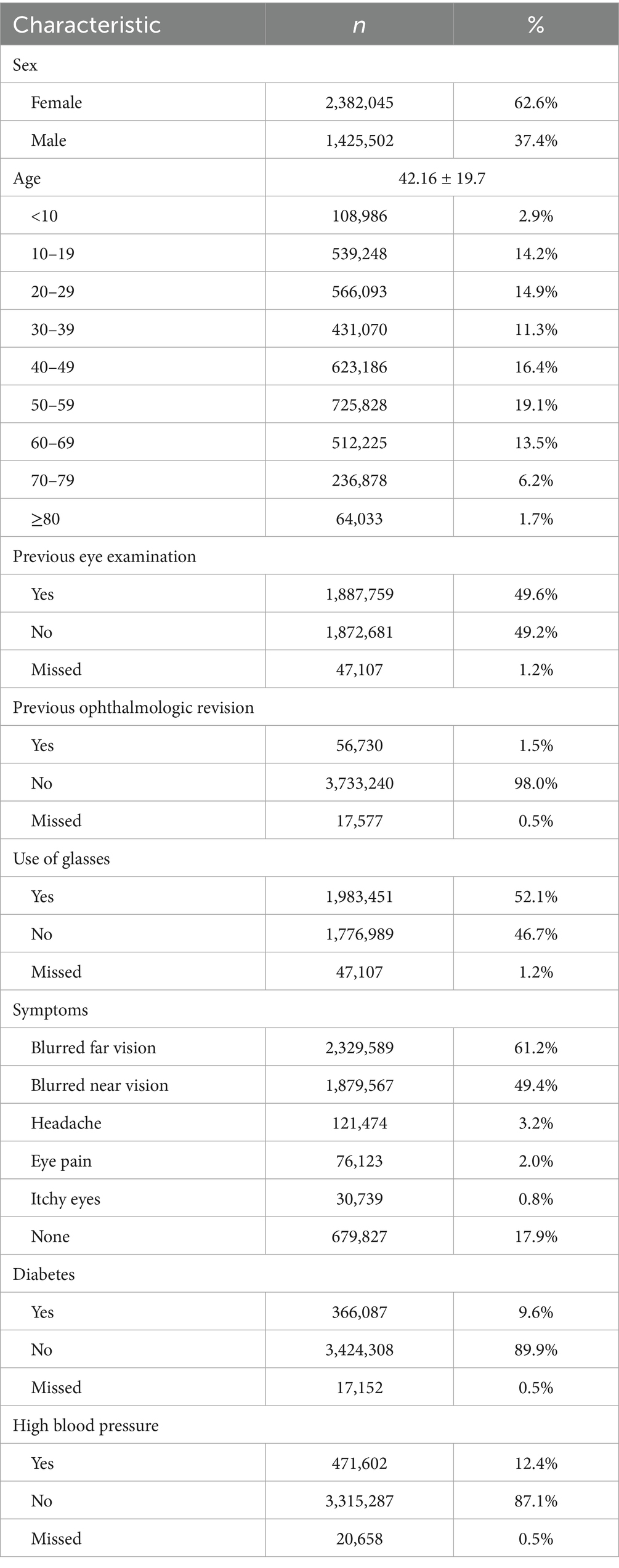
Table 1. Demographic characteristics of the outpatients included in this study.
Concerning the overall RE, we found 2,841,067 affected individuals (74.61, 95% CI: 74.57–74.65), with myopia being the most prevalent affecting 1,469,377 outpatients (38.6, 95% CI: 38.54–38.64), followed by hyperopia and astigmatism affecting 1,234,403 (32.4, 95% CI: 32.37–32.47) and 1,205,400 (31.7, 95% CI: 31.61–31.71) outpatients, respectively (Figures 1A, 2A, 3A, Supplementary Table 1). When stratified by compound RE, the prevalence rates were as follows: simple astigmatism, 3.6% (137,238 outpatients, 95% CI: 3.58–3.62); myopic astigmatism, 22.2% (846,16 outpatients, 95% CI:22.18–22.26); hyperopic astigmatism, 5.8% (222,034 outpatients, 95% CI:5.80–5.85); simple myopia, 16.4% (623,234 outpatients, 95% CI:16.30–16.40); and simple hyperopia, 26.6% (1,012,395 outpatients, 95% CI:26.54–26.63) (Supplementary Table 1).
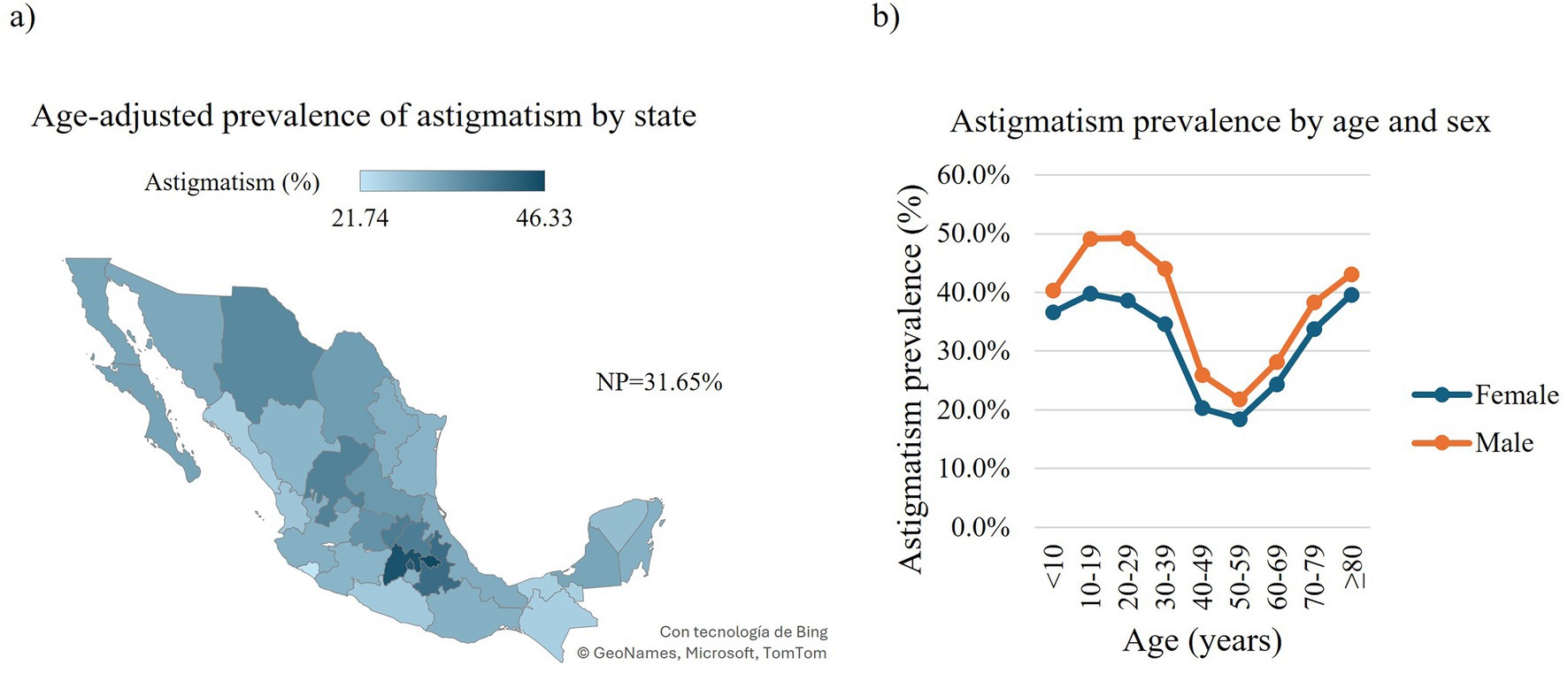
Figure 1. Prevalence of astigmatism in Mexican outpatients. Choropleth map of the age-adjusted prevalence of astigmatism in Mexican outpatients by state (a). Prevalence of astigmatism in Mexican outpatients by age and sex (b). Trend of age-specific prevalence evaluated with the chi-squared (χ2) test for trend: Females: χ2 = 32,353, df = 1, p-value < 0.0001; males: χ2 = 34,451, df = 1, p-value < 0.0001. NP, national prevalence.
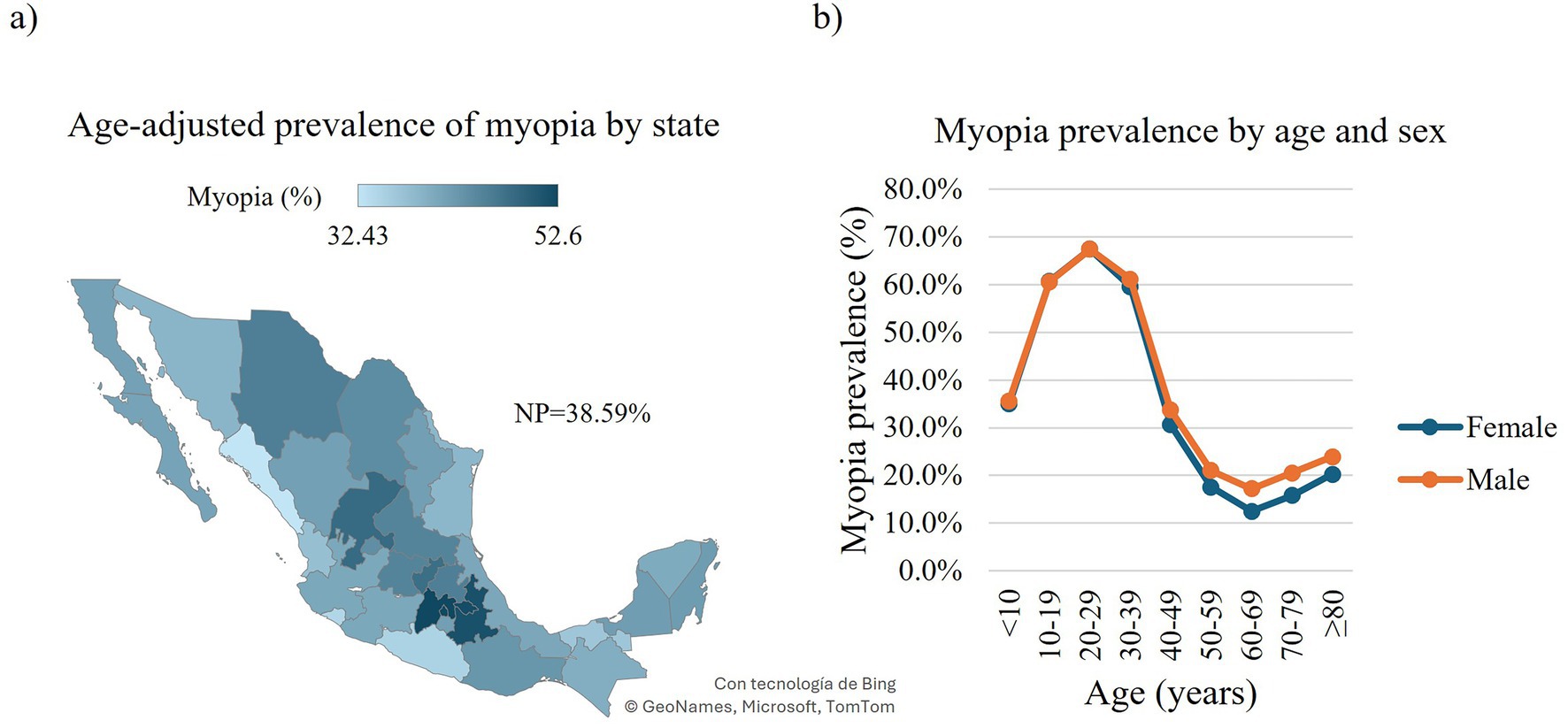
Figure 2. Prevalence of myopia in Mexican outpatients. Choropleth map of the age-adjusted prevalence of myopia in Mexican outpatients by state (a). Prevalence of myopia in Mexican outpatients by age and sex (b). Trend of age-specific prevalence evaluated with the chi-squared (χ2) test for trend: Females: χ2 = 353,458, df = 1, p-value < 0.0001; males, χ2 = 161,030, df = 1, p-value < 0.0001. NP, national prevalence.
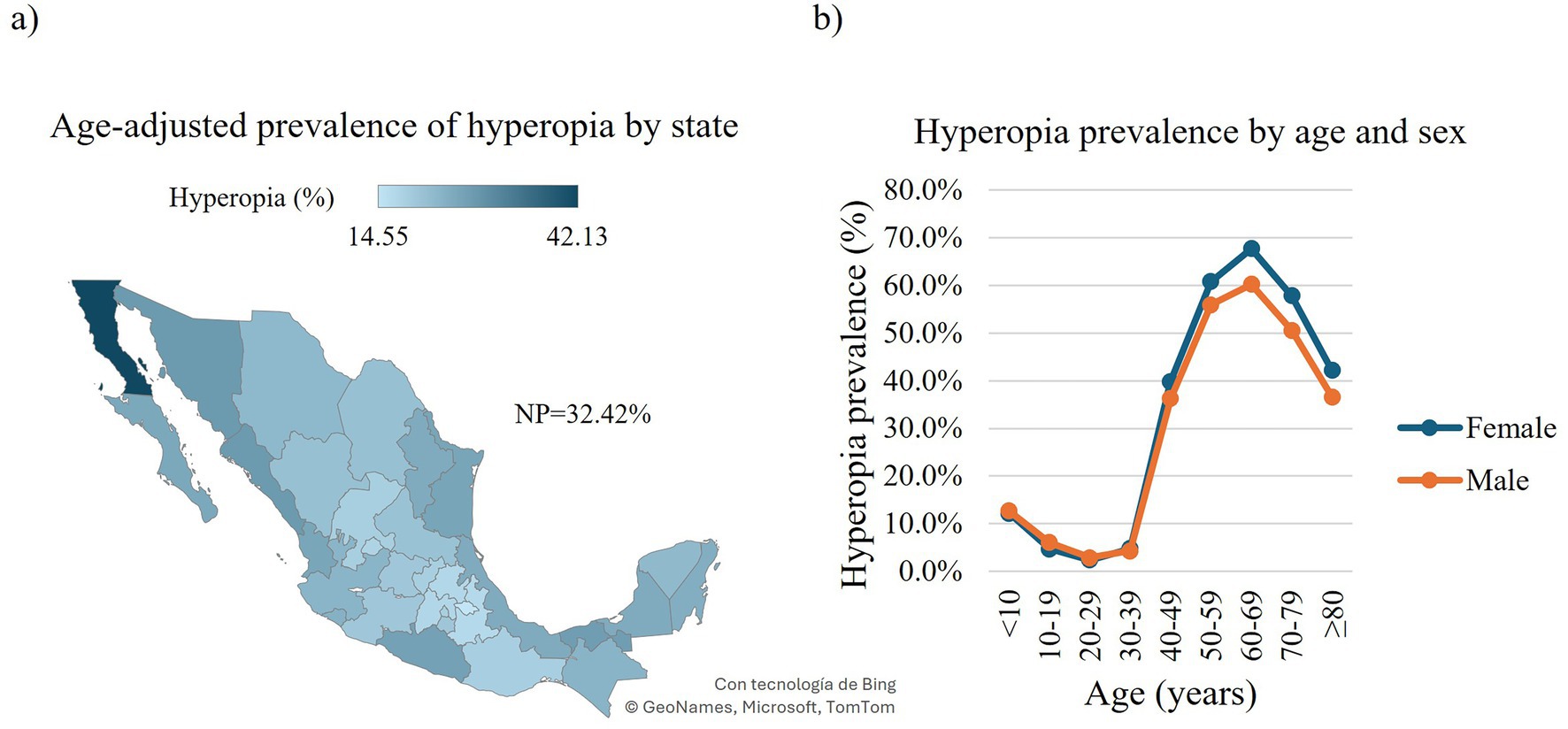
Figure 3. Prevalence of hyperopia in Mexican outpatients. Choropleth map of the age-adjusted prevalence of hyperopia in Mexican outpatients by state (a). Prevalence of hyperopia in Mexican outpatients by age and sex (b). Trend of age-specific prevalence evaluated with the chi-squared (χ2) test for trend: Females, χ2 = 110,443, df = 1, p-value < 0.0001; males, χ2 = 71,020, df = 1, p-value < 0.0001. NP = national prevalence.
Regarding the national distribution of astigmatism, Tlaxcala exhibited the highest age-adjusted prevalence affecting 5,147 outpatients (46.3, 95% CI: 44.61–48.13), followed by Estado de Mexico with 235,387 affected outpatients (44.8, 95% CI: 44.58–45.03). In contrast, Colima and Chiapas showed the lowest age-adjusted prevalence with 6,284 (21.7, 95% CI: 20.98–22.53) and 16,787 (25.2, 95% CI: 24.57–25.77) affected outpatients, respectively (Figure 1A, Supplementary Table 2). When analyzed by sex, males presented a higher age-adjusted overall prevalence of astigmatism with 516,154 (39.3, 95% CI: 39.17–39.44) affected outpatients than females with 689,246 affected outpatients (32.4, 95% CI: 32.32–32.54) (Supplementary Table 3). We observed comparable patterns in the prevalence of astigmatism across sexes with regard to age groups. In both males and females, the prevalence increased with age, peaking during the 10–29-year age range (females: 10–19 years, 125,497 outpatients, 39.7 95% CI: 39.6–39.9; 20–29 years, 137,372 outpatients, 38.6 95% CI: 38.5–38.8; males: 10–19 years, 109,822 outpatients, 49.1 95% CI: 48.9–49.3; 20–29 years, 103,576 outpatients, 49.2 95% CI: 49.0–49.4). This was followed by a declining trend, reaching the lowest prevalence in the 50–59-year age group (females: 86,456 outpatients, 18.4 95% CI: 18.3–18.5; males: 55,793 outpatients, 21.7 95% CI: 21.6–21.9). Thereafter, the prevalence began to rise again, closely returning to the peak levels observed in early adulthood. (Figure 1B).
Concerning the national distribution of myopia, Estado de Mexico exhibited the highest age-adjusted prevalence with 280,488 affected outpatients at 52.6% (95% CI: 52.37–52.84), followed by Ciudad de Mexico with 193,529 affected outpatients at 52.5% (95% CI: 52.24–52.82). In contrast, Sinaloa and Colima showed the lowest age-adjusted prevalence with 50,497 (32.4, 95% CI: 32.08–32.78) and 8,394 (34.4, 95% CI: 33.45–35.37) affected outpatients, respectively (Figure 2A, Supplementary Table 2). When analyzed by sex, males presented a higher age-adjusted overall prevalence of myopia with 577,936 affected outpatients (45.1, 95% CI: 45.01–45.28) than females with 891,441 affected outpatients (43.5, 95% CI: 43.42–43.66; Supplementary Table 3). We identified similar age-related patterns in the prevalence of myopia among males and females. In both sexes, the prevalence increased markedly and consistently, reaching a peak in the 20–29-year age group (females: 239,978 affected outpatients 67.5 95% CI: 67.3–67.6; males: 141,867 affected outpatients, 67.4 95% CI: 67.2–67.6). This was followed by a declining trend, with the lowest prevalence observed in the 60–69-year age group (females: 40,165 affected outpatients, 12.5 95% CI: 12.3–12.6; males: 32,627 affected outpatients, 17.2 95% CI: 17.0–17.3). Subsequently, prevalence began to rise again, although it did not return to the peak levels observed in early adulthood (Figure 2B).
Regarding the national distribution of hyperopia, Baja California exhibited the highest age-adjusted prevalence with 88,217 affected outpatients at 42.1% (95% CI: 41.79–42.49), followed by Sonora with 59,901 affected outpatients at 27.8% (95% CI: 27.5–28.08). In contrast, Tlaxcala and Puebla showed the lowest age-adjusted prevalence with 2,279 (14.5, 95% CI: 13.68–15.52) and 36,993 (16.6, 95% CI: 16.36–16.82) affected outpatients, respectively (Figure 3A, Supplementary Table 2). When analyzed by sex, females presented a higher age-adjusted overall prevalence of hyperopia with 809,299 affected outpatients (22.4, 95% CI: 22.34–22.48) than males with 425,104 affected outpatients (20.1, 95% CI: 20.87–21.03; Supplementary Table 3). We observed comparable age-related trends in the prevalence of hyperopia among men and women. In both sexes, the prevalence declined with age, reaching its lowest point in the 20–29-year age group (females: 8,360 affected outpatients, 2.4 95% CI: 2.3–2.4; males: 6,029 affected outpatients 2.9 95% CI: 2.8–2.9). This was followed by a steady increase, peaking in the 60–69-year age group (females: 218,365 affected outpatients 67.8% CI: 67.6–67.9; males: 114,473 affected outpatients, 60.3 95% CI: 60.1–60.5). The prevalence began to decline again, although it did not return to the minimum levels observed in early adulthood (Figure 3B).
4 Discussion
As previously noted, demographic growth, population aging, lifestyle changes, and increasing urbanization are projected to substantially elevate the global burden of ocular conditions. Comprehensive epidemiological research is essential to effectively mitigate the impact of RE and other vision-related disorders. Such data can inform the development of targeted public health strategies at both the local and national levels, ultimately contributing to a reduction in the prevalence and impact of these conditions.
Unfortunately, Mexico lacks comprehensive national studies that encompass all 32 states, all age groups, and all three types of refractive errors (RE). This research constitutes the most extensive examination of refractive errors in Mexico to date, utilizing a database that includes outpatients from every age group and region across the nation. Its extensive national reach and large sample size provide a detailed and representative overview of the visual health of the Mexican population, rendering it a crucial resource for public health decision-making. The study involved a significant number of outpatients and covered the entire Mexican territory. By analyzing clinical eye examination data from Salud Digna, we aimed to map the national distribution of RE and explore its variations by gender and age. It is important to consider that our findings are based on an outpatient population. Nonetheless, the results are intended to aid vision health professionals and policymakers in crafting strategies to enhance access to eye care services and to guide policies on screening, treatment, and long-term management of RE in the future.
4.1 National astigmatism prevalence
In examining the prevalence of astigmatism, our findings indicate a higher prevalence than the global estimates for children as reported by Hashemi et al. (12), yet lower than the figures reported for adults in their study. Within the context of Mexican research, our observed prevalence of astigmatism surpasses that documented in most previous studies (25–30), with the exception of Barba-Gallardo et al. (31), who reported a higher prevalence than that identified in our study. The observed discrepancies in estimates not only for astigmatism, but also for myopia, and hyperopia can be attributed to differences in sample collection, sample size, the definition of refractive error (RE) employed, as well as genetic and ethnic factors, complicating direct comparisons of RE prevalence between this study and prior research. Regarding the geographical distribution of astigmatism cases, a higher prevalence is noted in the central region of the country, which is both highly industrialized and densely populated. Genetic factors, given Mexico’s status as one of the most ancestrally diverse nations in the Americas (32), alongside environmental factors, may contribute to these observed patterns.
4.2 National myopia prevalence
In recent decades, there has been a concerning global increase in the prevalence of myopia, particularly in Asian countries such as China, South Korea, and Singapore (13). This trend has been attributed to factors including rapid urbanization, intensified educational activities, prolonged use of electronic devices, and reduced outdoor time. These developments raise public health concerns due to the risk of high myopia and its associated visual complications (13).
The prevalence of myopia in our study exceeded the global figures reported by Hashemi et al. (12) and Holden et al. (13), although it remained lower than the prevalence recently reported by Hönekopp et al. (33) among German primary school children. In the context of myopia estimates in Mexico, our findings indicate a higher prevalence than that documented by previous authors (25–31). As with astigmatism, these differences in estimates can be attributed to variations in distinct factors as previously stated.
In line with the geographical distribution of astigmatism cases, myopia was found to be more common in the central part of the country. This is expected, as many of the myopia cases identified in this study also involve astigmatism. Genetic factors might play a role in these patterns, along with environmental influences such as the balance between near and distance vision tasks, since outdoor activities have been shown to significantly delay both the onset and progression of myopia (34). In Mexico, factors like rapid urbanization, an aging population, increased screen time, and decreased outdoor activities may be contributing to the rise in myopia and other refractive errors. Recent research has connected these factors to changes in visual behavior, particularly among children and adolescents, highlighting the importance of considering these elements in preventive measures (35, 36).
4.3 National hyperopia prevalence
Our study identified a higher prevalence of hyperopia compared to the global figures reported by Hashemi et al. (12) and Delpizzo et al. (37). Conversely, when compared to Mexican studies, the prevalence of hyperopia in this study aligns with the national estimates provided by Ramirez-Ortiz et al. (26) for primary school children. This prevalence exceeds the figures reported by Ortiz et al. (25) for the general population, slightly surpasses those reported by Teran et al. (27, 28, 30) for school-aged children (6–18 years), and is marginally below the prevalence noted by Barba-Gallardo et al. (31) in children. However, it remains higher than the prevalence reported by Barba-Gallardo et al. (31) in adults.
Similar to astigmatism, the differences in estimates can be attributed to variations in several factors as previously mentioned.
The analysis of the geographical distribution of refractive errors (RE) indicated a higher prevalence of hyperopia in coastal states. The reasons behind the coastal distribution of hyperopia cases warrant further investigation. As with the geographical distribution of astigmatism and myopia, genetics may play a role, although there is significant genetic variation in the Mexican coastal states exhibiting these patterns (32). Therefore, environmental factors, such as the frequency of near versus distance vision tasks, might be more influential, as the Mexican coastal states are less industrialized and densely populated compared to the central region.
It is important to note that our study encompasses all 32 Mexican states and includes participants from all age groups. In contrast, previous studies on the prevalence of RE in Mexico have primarily been regional in scope, with specific areas underrepresented (25), or have predominantly focused on specific age groups, particularly school-aged children. These differences, along with substantial variations in sample size, may partially account for the discrepancies between our findings and those of earlier reports. Additionally, it is worth noting that our study population consists of self-selected outpatients seeking optical services. In contrast, some previous studies have employed population-based screening approaches targeting the general public which may lead to an overestimation in our study.
4.4 RE relation to sex and age
Our investigation into the association between refractive error (RE), gender, and age revealed that males consistently exhibited a higher prevalence of astigmatism compared to females across all age categories. In contrast, the incidence of myopia and hyperopia was comparable between the sexes during childhood and early adulthood. However, as outpatients aged, a divergence emerged, with males demonstrating a greater propensity for myopia and females for hyperopia. The gender-based differences in refractive error prevalence may be attributed to hormonal, occupational, and behavioral factors. For instance, sex hormones may affect ocular biomechanics, while variations in occupational roles and visual habits between males and females could account for the increased incidence of myopia in males and hyperopia in females in older age groups (38–40).
Our findings also suggest a subtle physiological transition in the visual system beginning in the 30–39 age range, which becomes more pronounced in the 40–49 age group, where a marked shift in the prevalence of all three types of RE is observed. This pattern may be linked to age-related biomechanical changes in the ocular structures. Notably, previous research has identified two distinct aging-related metabolomic shifts occurring around the ages of 44 and 60 (41), which could underline the changes in RE prevalence in the population of the current study. However, the specific factors and their interactions that contribute to the observed sex differences, with males exhibiting a greater tendency toward myopia and females toward hyperopia in these age groups, remain poorly understood and require further research.
To further explore sex as a potential risk factor for RE development, we calculated risk ratios (Supplementary Table 5). Although these analyses yielded statistically significant results, they should be interpreted cautiously. The large sample size in our study increased the likelihood of detecting statistically significant differences, which may not necessarily reflect clinically meaningful effects. Similarly, chi-square tests assessing sex-based differences in RE prevalence produced several statistically significant outcomes (Supplementary Table 6); however, many of these may be spurious and should also be interpreted within a clinical, rather than purely statistical, context.
Our research indicates that myopia and astigmatism are highly prevalent among children and young adults, presenting significant social and economic challenges by limiting educational achievements, employment opportunities, and overall productivity (1). Uncorrected refractive errors constitute a major cause of preventable visual impairment, adversely affecting academic performance, work efficiency, and quality of life. Furthermore, the cost of optical correction can be substantial, particularly for at-risk populations (15, 42). Therefore, it is imperative to implement visual screening initiatives and public policies that ensure access to affordable eyewear and strategies to mitigate myopia progression in children.
In contrast, hyperopia was more prevalent in older adults, representing a substantial burden in this population group. This is particularly noteworthy, as visual impairment in later life is strongly associated with reduced quality of life and increased risk of falls and fractures (43).
4.5 Strengths and limitations
The strength of our study lies in its large, nationally representative sample, encompassing all 32 states of Mexico, making our findings highly generalizable and reflective of the Mexican population. Additionally, the eye examination procedures are standardized across our clinics and are consistently performed by certified optometrists.
It is important to highlight that the data used in this research were derived from eye examinations conducted without cycloplegia. Differences between refractive evaluations with and without cycloplegia have been reported, as non-cycloplegic assessments might overestimate myopia and underestimate hyperopia, especially in younger individuals (44, 45). This variation could potentially lead to bias when determining the prevalence of these refractive errors in children and young adults.
Additionally, the age recorded in our study corresponds to the time of the eye examination, which may not reflect the true age at which the refractive error developed. This could introduce a degree of reporting bias in the age-related prevalence estimates.
Although data on systemic conditions such as hypertension and diabetes were collected, they were not analyzed as stratifying variables due to the primary focus of the study. Future research may explore these associations in greater depth.
Our study group comprised outpatients who independently opted to seek diagnostic services at Salud Digna, resulting in a self-selected cohort that included both insured and uninsured participants from diverse socioeconomic backgrounds. This self-selection may introduce potential bias, as these outpatients might already exhibit symptoms warranting an eye examination, potentially leading to an overestimation of the prevalence of refractive errors compared to the general population. Although this self-selection presents a possible bias, it is somewhat mitigated by the extensive data collected, which allows for more detailed analyses under specific conditions of interest. Therefore, the results derived from the Salud Digna data should be interpreted with an understanding of this population, taking into account the inherent selection bias.
4.6 Concluding remarks
Reliable data on RE in Mexico remains scarce, limiting the development of effective public health strategies. This study provides a comprehensive overview of the current landscape of RE in the country, aiming to promote multisectoral collaboration both within Mexico and in nations with similar cultural and ancestral contexts.
One of the most pressing public health findings is the substantial proportion of outpatients who have never undergone an eye examination, revealing critical gaps in access to basic eye care services. Furthermore, the high unmet need for corrective lenses highlights the urgency of implementing policies that improve the availability, affordability, and accessibility of vision screening and eyeglasses.
Addressing these challenges requires coordinated efforts between public and private sectors. Strategic partnerships can empower communities by reallocating infrastructure and human resources to strengthen ophthalmological services and preventive care. These initiatives should prioritize early detection and treatment of RE and other visual conditions, especially among the most affected groups identified in this and other studies, namely, school-aged children and adults over 40 years of age.
To advance visual health equity, it is essential to integrate eye care into national public health agendas. Longitudinal studies and population-based surveys using standardized methodologies are recommended to monitor the evolution of RE, assess the impact of interventions, identify emerging risk factors, and guide future policy decisions.
Data availability statement
The datasets presented in this article are not readily available because under the Mexican Federal Law on Personal Data Protection we are not allowed to. Requests to access the datasets should be directed to am9uYXRoYW4uYWxjYW50YXJAc2FsdWQtZGlnbmEub3Jn.
Ethics statement
The studies involving humans were approved by Ethical Review and Research Board of Salud Digna. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
AG-G: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. BH-J: Conceptualization, Investigation, Methodology, Writing – review & editing. ML-R-E: Data curation, Resources, Writing – review & editing. EE-A: Resources, Writing – review & editing. HM-J: Resources, Writing – review & editing. HG-C: Resources, Writing – review & editing. AC-R: Conceptualization, Resources, Supervision, Writing – review & editing. JA-F: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to acknowledge MSc Omar Rodríguez López for his support in data extraction, as well as all the Salud Digna collaborators from the Optometry Service Department, who contributed to the data used in this study through their daily work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1675138/full#supplementary-material
References
2. Dai, M, and Ouyang, Y. Global, regional, and national burden of refraction disorders: findings from the global burden of disease study 2021 and projections to 2050. BMC Public Health. (2025) 25:1247. doi: 10.1186/s12889-025-22440-w
3. Bourne, RRA, Steinmetz, JD, Saylan, M, Mersha, AM, Weldemariam, AH, Wondmeneh, TG, et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the right to sight: An analysis for the global burden of disease study. Lancet Glob Health. (2021) 9:e144–60. doi: 10.1016/S2214-109X(20)30489-7
4. Fricke, TR, Tahhan, N, Resnikoff, S, Papas, E, Burnett, A, Ho, SM, et al. Global prevalence of presbyopia and vision impairment from uncorrected presbyopia: systematic review, Meta-analysis, and modelling. Ophthalmology. (2018) 125:1492–9. doi: 10.1016/j.ophtha.2018.04.013
5. Harb, EN, and Wildsoet, CF. Origins of refractive errors: environmental and genetic factors. Annu Rev Vis Sci. (2019) 5:47–72. doi: 10.1146/annurev-vision-091718-015027
6. Baird, PN, Saw, SM, Lanca, C, Guggenheim, JA, Smith Iii, EL, Zhou, X, et al. Myopia (primer). Nat Rev Dis Primers. (2020) 6:99. doi: 10.1038/s41572-020-00231-4
7. Galvis, V, Tello, A, Camacho, PA, Gómez, LM, Rey, JJ, and Serrano, AA. Definition of refractive errors for research studies: spherical equivalent could not be enough. J Optom. (2021) 14:224–5. doi: 10.1016/j.optom.2020.10.003
8. National Eye Institute. Refractive errors (2023). Available online at: https://www.nei.nih.gov/learn-about-eye-health/eye-conditions-and-diseases/refractive-errors (Accessed 15, 2024).
9. Kierstan, Boyd. What is presbyopia? (2022), Am Acad Ophthalmol. Available online at: https://www.aao.org/eye-health/diseases/what-is-presbyopia (Accessed May 15, 2024).
10. Jacobs, DS, Afshari, NA, Bishop, RJ, Keenan, JD, Lee, J, Shen, TT, et al. Refractive errors preferred practice pattern®. Ophthalmology. (2023) 130:P1–P60. doi: 10.1016/j.ophtha.2022.10.031
11. WHO. Blindess and visual impairment (2023). Available online at: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment (Accessed May 15, 2024)
12. Hashemi, H, Fotouhi, A, Yekta, A, Pakzad, R, Ostadimoghaddam, H, and Khabazkhoob, M. Global and regional estimates of prevalence of refractive errors: systematic review and meta-analysis. J Curr Ophthalmol. (2018) 30:3–22. doi: 10.1016/j.joco.2017.08.009
13. Holden, BA, Fricke, TR, Wilson, DA, Jong, M, Naidoo, KS, Sankaridurg, P, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. (2016) 123:1036–42. doi: 10.1016/j.ophtha.2016.01.006
14. Durr, NJ, Dave, SR, Lage, E, Marcos, S, Thorn, F, and Lim, D. From unseen to seen: tackling the global burden of uncorrected refractive errors. Annu Rev Biomed Eng. (2014) 16:131–53. doi: 10.1146/annurev-bioeng-071813-105216
15. Resnikoff, S, Pascolini, D, Mariotti, SP, and Pokharel, GP. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ. (2008) 86:63–70. doi: 10.2471/BLT.07.041210
16. Furtado, JM, Lansingh, VC, Carter, MJ, Milanese, MF, Peña, BN, Ghersi, HA, et al. Causes of blindness and visual impairment in Latin America. Surv Ophthalmol. (2012) 57:149–77. doi: 10.1016/j.survophthal.2011.07.002
17. Tedja, MS, Wojciechowski, R, Hysi, PG, Eriksson, N, Furlotte, NA, Verhoeven, VJM, et al. Genome-wide association meta-analysis highlights light-induced signaling as a driver for refractive error. Nat Genet. (2018) 50:834–48. doi: 10.1038/s41588-018-0127-7
18. Hysi, PG, Choquet, H, Khawaja, AP, Wojciechowski, R, Tedja, MS, Yin, J, et al. Meta-analysis of 542,934 subjects of European ancestry identifies new genes and mechanisms predisposing to refractive error and myopia. Nat Genet. (2020) 52:401–7. doi: 10.1038/s41588-020-0599-0
19. Rosenfield, M, Kollbaum, P, and Prenat, O. Eye strain and near work: both an ancient problem and a modern concern. Ophthalmic Physiol Opt. (2025) 45:1037–9. doi: 10.1111/opo.13520
20. INEGI. ESTADÍSTICAS A PROPÓSITO DEL DÍA INTERNACIONAL DE LAS PERSONAS CON DISCAPACIDAD (DATOS NACIONALES) (2021). Available online at: https://www.inegi.org.mx/contenidos/saladeprensa/aproposito/2021/EAP_PersDiscap21.pdf (Accessed May 20, 2024).
21. Madueña-Angulo, SE, Beltran-Ontiveros, SA, Leal-Leon, E, Contreras-Gutierrez, JA, Lizarraga-Verdugo, E, Gutierrez-Arzapalo, PY, et al. National sex- and age-specific burden of blindness and vision impairment by cause in Mexico in 2019: a secondary analysis of the global burden of disease study 2019. Lancet Reg Health Am. (2023) 24:100552. doi: 10.1016/j.lana.2023.100552
22. World Health Organization. SPECS 2030. (2025). Available online at: https://www.who.int/initiatives/specs-2030 (Accessed September 16, 2025)
23. R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2023).
24. Ahmad, OB, Boschi-Pinto, C, Lopez, AD, Murray, CJ, Lozano, R, and Inoue, M. Age standardization of rates: A new WHO standard. GPE Discussion Paper Series: No. 31. Geneva: World Health Organization (2001). 31 p.
25. Ortiz, MI, Campuzano Revilla, GP, Muñoz Pérez, V, and Cuevas Suárez, CE. Prevalencia de miopía, hipermetropía y astigmatismo en México: Una revisión sistemática. Educación y Salud Boletín Científico Instituto de Ciencias de la Salud Universidad Autónoma del Estado de Hidalgo. (2022) 10. doi: 10.29057/icsa.v10i20.8591
26. Ramírez-Ortiz, MA, Amato-Almanza, M, Romero-Bautista, I, Klunder-Klunder, M, Aguirre-Luna, O, Kuzhda, I, et al. A large-scale analysis of refractive errors in students attending public primary schools in Mexico. Sci Rep. (2023) 13:13509. doi: 10.1038/s41598-023-40810-5
27. Teran, E, Ramírez-Jaime, R, Martínez-Gaytán, C, Romo-García, E, and Costela, FM. Refractive error of students (15- to 18-year-olds) in Northwest Mexico. Optom Vis Sci. (2021) 98:1127–31. doi: 10.1097/OPX.0000000000001779
28. Terán, E, Romo-García, E, Félix-Medina, MH, Martínez-Gaytán, C, Ramírez-Jaimes, R, and Santiago, H. Refractive error of students (12–15-years-old) in northwestern Mexico. Revista Mexicana de Oftalmología. (2023) 97:73–9. doi: 10.5005/rmo-11013-0043
29. Gomez-Salazar, F, Campos-Romero, A, Gomez-Campaña, H, Cruz-Zamudio, C, Chaidez-Felix, M, Leon-Sicairos, N, et al. Refractive errors among children, adolescents and adults attending eye clinics in Mexico. Int J Ophthalmol. (2017) 10:796–802. doi: 10.18240/ijo.2017.05.23
30. Teran, E, Romo-García, E, and Santiago, HC. Refractive errors of school children from economically disadvantaged areas in Northwest México. J Clin Med. (2024) 13:3094. doi: 10.3390/jcm13113094
31. Barba-Gallardo, LF, Salas-Hernández, LH, Villafán-Bernal, JR, Marín-Nájera, P d S, García-López, DM, López-Garcia, ADC, et al. Refractive status of patients attending eye clinics of the public health system from Aguascalientes, Mexico. J Optom. (2021) 14:328–34. doi: 10.1016/j.optom.2020.08.011
32. Sohail, M, Palma-Martínez, MJ, Chong, AY, Quinto-Cortés, CD, Barberena-Jonas, C, Medina-Muñoz, SG, et al. Mexican biobank advances population and medical genomics of diverse ancestries. Nature. (2023) 622:775–83. doi: 10.1038/s41586-023-06560-0
33. Hönekopp, A, Tommes, LM, Doebler, P, and Weigelt, S. Myopia prevalence, refractive status and uncorrected myopia among primary and secondary school students in Germany. Front Med. (2024) 11:1483069. doi: 10.3389/fmed.2024.1483069
34. Wu, PC, Chen, CT, Lin, KK, Sun, CC, Kuo, CN, Huang, HM, et al. Myopia prevention and outdoor light intensity in a school-based cluster randomized trial. Ophthalmology. (2018) 125:1239–50. doi: 10.1016/j.ophtha.2017.12.011
35. Morgan, IG, French, AN, Ashby, RS, Guo, X, Ding, X, He, M, et al. The epidemics of myopia: aetiology and prevention. Prog Retin Eye Res. (2018) 62:134–49. doi: 10.1016/j.preteyeres.2017.09.004
36. Janssen, I, Medina, C, Pedroza, A, and Barquera, S. Screen time in mexican children: findings from the 2012 national health and nutrition survey (ENSANUT 2012). Salud Publica Mex. (2013) 55:484–91. doi: 10.21149/spm.v55i5.7248
37. Castagno, VD, Fassa, AG, Carret, MLV, Vilela, MAP, and Meucci, RD. Hyperopia: a meta-analysis of prevalence and a review of associated factors among school-aged children. BMC Ophthalmol. (2014) 14:163. doi: 10.1186/1471-2415-14-163
38. Hyman, L. Myopic and hyperopic refractive error in adults: an overview. Ophthalmic Epidemiol. (2007) 14:192–7. doi: 10.1080/09286580701535517
39. Lee, KE, Klein, BEK, Klein, R, and Wong, TY. Changes in refraction over 10 years in an adult population: the beaver dam eye study. Invest Ophthalmol Vis Sci. (2002) 43:2566–71.
40. Mansfield, A, Addis, M, and Mahalik, J. Why won’t He go to the doctor?: the psychology of men’s help seeking. Int J Mens Health. (2003) 2:93–109. doi: 10.3149/jmh.0202.93
41. Shen, X, Wang, C, Zhou, X, Zhou, W, Hornburg, D, Wu, S, et al. Nonlinear dynamics of multi-omics profiles during human aging. Nat Aging. (2024) 4:1619–34. doi: 10.1038/s43587-024-00692-2
42. Fricke, T, Holden, B, Wilson, D, Schlenther, G, Naidoo, K, Resnikoff, S, et al. Global cost of correcting vision impairment from uncorrected refractive error. Bull World Health Organ. (2012) 90:728–38. doi: 10.2471/BLT.12.104034
43. Mehta, J, Czanner, G, Harding, S, Newsham, D, and Robinson, J. Visual risk factors for falls in older adults: a case-control study. BMC Geriatr. (2022) 22:134. doi: 10.1186/s12877-022-02784-3
44. Guo, X, Shakarchi, AF, Block, SS, Friedman, DS, Repka, MX, and Collins, ME. Noncycloplegic compared with Cycloplegic refraction in a Chicago school-aged population. Ophthalmology. (2022) 129:813–20. doi: 10.1016/j.ophtha.2022.02.027
Keywords: refractive errors, prevalence, astigmatism, myopia, hyperopia
Citation: García-Gil A, Hernández-Jurado BI, Luna-Ruiz-Esparza MA, Espinoza-Angulo E, Machado-Jiménez H, Gómez-Campaña H, Campos-Romero A and Alcántar-Fernández J (2025) Prevalence and age-related trends of refractive errors in Mexican outpatients: a cross-sectional study. Front. Public Health. 13:1675138. doi: 10.3389/fpubh.2025.1675138
Edited by:
Siti Nurliyana Abdullah, Raja Isteri Pengiran Anak Saleha Hospital, BruneiReviewed by:
Thiago Gonçalves dos Santos Martins, Federal University of São Paulo, BrazilKourosh Sheibani, Basir Eye Health Research Center, Iran
Copyright © 2025 García-Gil, Hernández-Jurado, Luna-Ruiz-Esparza, Espinoza-Angulo, Machado-Jiménez, Gómez-Campaña, Campos-Romero and Alcántar-Fernández. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jonathan Alcántar-Fernández, am9uYXRoYW4uYWxjYW50YXJAc2FsdWQtZGlnbmEub3Jn