Family-centred service in paediatric acquired brain injury rehabilitation: Bridging the gaps
 Taylor Jenkin
Taylor Jenkin Vicki A. Anderson
Vicki A. Anderson Kate D'Cruz5
Kate D'Cruz5  Adam Scheinberg
Adam Scheinberg Sarah Knight
Sarah Knight- 1Neurodisability & Rehabilitation, Murdoch Children's Research Institute, Melbourne, VIC, Australia
- 2Melbourne School of Psychological Sciences, The University of Melbourne, Melbourne, VIC, Australia
- 3Brain and Mind, Murdoch Children's Research Institute, Melbourne, VIC, Australia
- 4Psychology Service, The Royal Children's Hospital, Melbourne, VIC, Australia
- 5Summer Foundation, Melbourne, VIC, Australia
- 6Department of Paediatrics, The University of Melbourne, Melbourne, VIC, Australia
- 7Victorian Paediatric Rehabilitation Service, The Royal Children's Hospital, Melbourne, VIC, Australia
Background: Children and adolescents who sustain an acquired brain injury (ABI) can experience acute and ongoing difficulties in a range of cognitive and functional domains, and their families often experience significant life changes and challenges. Family-centred service is therefore considered best practice in paediatric ABI rehabilitation. Despite widespread acceptance of family-centred service in this context, recent literature indicates that family needs are often unrecognised and unmet following paediatric ABI. Although family-centred service was introduced in the field of developmental disability over five decades ago, there remains a lack of clarity about how this approach is implemented in practice. Additionally, limited literature has discussed the implementation of family-centred service in paediatric ABI rehabilitation despite key differences between ABI and developmental disability, including nature and timing of onset, rehabilitation foci, and impacts on families.
Aims: In this review, we aim to: (i) outline common sequelae of paediatric ABI with a focus on family outcomes; (ii) summarise paediatric rehabilitation and highlight opportunities for family support and involvement; (iii) discuss and synthesise literature across paediatric ABI rehabilitation and family-centred service to highlight gaps in knowledge and practice; and (v) identify clinical implications and future research directions.
Conclusions: There is a clear need for greater clarity and consensus regarding the implementation of family-centred service in paediatric ABI rehabilitation. This review highlights the importance of providing professional development opportunities for clinicians to increase competency in practising in a family-centred manner, and opportunities to actively involve, empower and support families within rehabilitation. This review also emphasises the importance of services implementing relevant supports to address family needs where possible and developing clear referral pathways so that families can access further support elsewhere when needed.
Introduction
Paediatric acquired brain injury (pABI) is a leading cause of death and acquired disability in children and adolescents, and refers to a brain insult sustained after birth (the term “children” will henceforth be used to refer to children and adolescents) (1–3). pABI can arise as a result of a range of causes, including traumatic brain injury (TBI), cerebrovascular accident (stroke), brain tumour, cerebral anoxia (oxygen deprivation), or infections such as encephalitis or meningitis (3–5). This wide range of pABI causes has led to difficulty in accurately estimating incidence. Hospital emergency department (ED) presentations for TBI, the most common form of pABI, have been reported to be approximately 2008 per 100,000 children (6). The consequences of pABI are complex and can profoundly impact children and their families. Family-centred services are widely accepted as best practice and emphasise the importance of supporting and involving families in pABI rehabilitation (7–10). While there are varying approaches to the delivery of family-centred service (9, 11, 12), evidence suggests that family needs are often unrecognised and unmet in rehabilitation following pABI (13–16).
This review aimed to: (i) outline common sequelae of pABI with a focus on family outcomes; (ii) summarise paediatric rehabilitation and highlight opportunities for family support and involvement; (iii) discuss recent literature regarding family-centred services; (iv) summarise literature across pABI rehabilitation and family-centred service to highlight gaps in knowledge and practice; and (v) identify clinical implications and future research directions.
Developmental considerations in paediatric ABI
Children who sustain an ABI can experience a range of acute and persisting difficulties in cognitive, academic, emotional, and behavioural functioning, which vary in severity from mild to severe and are associated with reduced participation and quality of life (3, 17, 18). In considering the impacts of pABI on the lives of children, it is also important to recognise the developmental context in which a pABI occurs. Childhood and adolescence are periods of rapid and dynamic brain development, with maturation continuing into the early 20s (19, 20). pABI can therefore disrupt acquired skills and derail ongoing skill development (21, 22), with children with ABIs “growing into” their deficits, and falling increasingly further behind their age peers over time (21–25). Thus pABI can cause long-term disability that persists into adulthood and associated lifetime consequences (3, 26).
Impact on families
Given the potentially significant acute and long-term impacts of pABI on children, it is unsurprising that families can also experience a dynamic constellation of changes and challenges following pABI. The sudden and unforeseen onset of these insults can contribute to acute and long-term injury-related distress, anxiety, reduced quality of life, reduced wellbeing, and caregiving burden in family members (14, 27–34). Family functioning and dynamics can also change as family members adapt their roles and responsibilities to adjust to a “different life rhythm” (27, 35, 36). While most families adapt to caring for a child with pABI over time (29, 33, 37–39), deterioration in family functioning may continue for several years, particularly for families of children with more severe injuries (29, 40–43). Several interventions have been developed to support families in adapting to life following paediatric ABI and coping with trauma. For example, Family Forward (31, 44) is delivered to families during inpatient rehabilitation and combines family counselling and multifamily groups to support family adaptation and coping. Stepping Stones Triple P Plus Acceptance and Commitment Therapy (SSTP + ACT) (45, 46) also addresses parent coping through an acceptance and commitment therapy approach, coupled with parenting skills training.
The developmental context of pABI relates not only to the development of the injured child, but to the development of the family. Expectations and hopes for the future often change when a child sustains a brain insult, after which families may lack a “road map” to anticipate the future (47–51). Parents and caregivers may grieve the loss of a “normal” future for their child and family, as well as the loss of the child they had known (14, 35, 52, 53). This loss may differ from that experienced by families of children with congenital or developmental disabilities which are present “from the beginning” of a child's life (54). The sudden, unforeseen, and often traumatic onset of pABI has important implications for families' support needs and rehabilitation.
The outcomes of children with pABI and their families are bi-directional and children's outcomes are closely associated with family functioning and the family's capacity to meet the changing needs of the child (39, 55–59). Taylor and colleagues (60) found a reciprocal relationship between parent distress and behaviour problems of children with moderate TBI, and others have found that better family functioning is predictive of better long-term outcomes for children (61, 62). These findings align with Family Systems Theory, which posits that each member of a family impacts all others, and the wellbeing of family members influences their capacity to facilitate child development (7, 63–65). Evidence for child-family interactions in pABI recovery highlights the need for rehabilitation to focus on the child and their family, not only to facilitate family adjustment and outcomes but also to enable families to better support the child with pABI.
Contemporary approaches to rehabilitation for paediatric ABI
pABI can give rise to complex patterns of acute and persisting deficits and needs. Many children with moderate to severe ABIs therefore require specialist rehabilitation (3, 4). Rehabilitation refers to “a set of interventions designed to optimize functioning and reduce disability in individuals with health conditions in interaction with their environment,” and aims to enable participation in meaningful life roles (66). Given the developmental context, pABI rehabilitation seeks to both target the effects of the pABI and support progress towards normative developmental milestones (67, 68). Additionally, as the impacts of pABI on children may not fully manifest for many years, rehabilitation requires an understanding of children's changing needs and a focus on providing ongoing support (3, 69–73). This is particularly relevant during transition periods such as the transition from home to school or from childhood to adolescence, at which point the functional impacts of pABI often become most apparent as developmental demands increase (4, 25, 74).
While early rehabilitation models were predominantly unimodal or domain-specific, there have been recent advances towards more holistic, context-sensitive, and integrated care (58, 67). To facilitate this approach, interdisciplinary rehabilitation is considered best practice and requires integration of disciplines’ efforts through collaboration and communication, such that team members function synchronously to work towards a superordinate goal that transcends discipline boundaries, with a shared understanding of each other's knowledge and methods (75–80). Strengths-based approaches are also gaining increasing recognition in pABI rehabilitation (81–83). This orientation emphasises individuals' and families' resilience and strengths, and recognises opportunities for healing, growth, and hope for the future following pABI (84).
Shifting the focus from impairment to functioning
Traditional views of childhood disability and rehabilitation have been strongly influenced by the biomedical model which focuses on “fixing” health conditions or disability through intervention provided by health professionals (85, 86). In 2001, the World Health Organization published the International Classification of Functioning (ICF) (87), a biopsychosocial framework that conceptualises health as a person's functioning within their social-ecological context (85, 86). This holistic framework depicts the interconnections between body structure and function, activity, participation, environmental factors, and personal factors, and recognises that no one factor is more important than the others (85). Within childhood disability, the Children and Youth Version of the ICF (88) encourages consideration of factors that are important to children's development, including their participation (i.e., involvement in life situations), activities (i.e., execution of tasks and actions), and environment (i.e., physical, social, and attitudinal environments in which people live)(85, 87, 89). To encourage the implementation of the ICF, Rosenbaum and Gorter (85) formulated six “F-words” (function, family, fitness, fun, friends, and future) to apply when working with children with disabilities and their families. These “F-words” are embedded within the components of the ICF and illustrate a biopsychosocial approach to disability, focusing on children's strengths and what they can do, rather than disability-related limitations (85, 90). Within this framework, “family” represents the child's environment or context. Implementation of the “F-words” supports improvements in children's health and functional outcomes, family empowerment and satisfaction, and overall family-centred service (90).
Family-centred service
Family-centred service is considered best practice in contemporary pABI rehabilitation (7–9, 91, 92). While family-centred service acknowledges clinicians' knowledge regarding medical conditions and their treatments, this approach emphasises that “each family is unique; that the family is the constant in the child's life; and that they are the experts on the child's abilities and needs” (93). Consistent with a family systems approach, family-centred service is underpinned by an understanding that better family functioning means that families are better equipped to care for their children and facilitate their development (7, 64, 65, 94). It also emphasises the role of the family in care planning, implementation, and evaluation, such that clinicians “work with patients and families, rather than just doing to or for them” (95).
Family involvement, engagement, and participation in rehabilitation
Family-centred service requires partnership between healthcare providers and families; thus, it is essential to understand what family participation, attendance, and engagement mean in rehabilitation. Parent participation in therapy refers to the actions they take to be actively involved in all stages of their child's care, for example, through sharing information to inform assessment or treatment, or implementing therapeutic exercises at home (96–98). Imms and colleagues (99) further define participation as comprising two elements: attendance and involvement. Given that the term “engagement” is used more commonly than “involvement” in healthcare literature, the term “engagement” will henceforth be used. Attendance refers to “being there” (100), and while this is often considered a behavioural indicator of parents' and caregivers' engagement, attendance alone does not necessarily constitute their engagement (96, 101). Rather, parent engagement is complex and multifaceted, representing a process of “engaging with” and a state of “engaging in” children's therapy (96, 102–104). Engagement “with” therapy is a relational, co-constructed, collaborative process between individuals and clinicians or services, whereas engaging “in” therapy is a state of affective, behavioural and cognitive commitment or investment in therapy that involves “being with what you are doing” (102–105). In a recent constructivist grounded theory study, Phoenix and colleagues (106) explored parent attendance, engagement, and participation in children's developmental rehabilitation services. They highlighted the impacts of parents' feelings, skills, knowledge, logistics, values and beliefs, and relationships with healthcare professionals on participation, attendance, and engagement, and considered the influence of family composition, service complexity (i.e., number of organisations and professionals involved in the child's healthcare), and health complexity (i.e., child, sibling, and parent physical and mental health). While most of this literature has focused on only parents or caregivers, the concepts of participation, attendance, and engagement can also be applied to other family members.
While limited literature has investigated family participation, attendance, and engagement in pABI rehabilitation, a recently published qualitative study explored family participation in pABI rehabilitation from the perspectives of children and adolescents with pABIs and their parents/caregivers and siblings (107). Findings highlighted how families can be involved in “doing rehabilitation together” with the child or adolescent, including participating in collaborative decision-making, actively supporting the child's or adolescent's input and engagement, and learning through observation and conversations with clinicians. Findings demonstrated that family participation in rehabilitation spans the entire care trajectory, from involvement in early inpatient rehabilitation to supporting the child to engage in rehabilitation activities at home. Importantly, this study highlighted that family participation in rehabilitation is shaped by families' unique lives and contexts and relies on two-way communication and information sharing between clinicians and families.
Given the importance of family participation in rehabilitation and the significant impacts of pABI on families, several family-centred interventions have been developed and implemented in rehabilitation. Cermak and colleagues (108) conducted a systematic review and meta-analysis of parent interventions following paediatric TBI and outlined interventions targeting parent outcomes, including parent-child interaction therapies (109, 110), problem-solving interventions (111, 112), and interventions combining parenting and cognitive behaviour therapy (113). In addition to parent interventions, several other family-centred interventions have been developed in the context of pABI that involve partnering with parents and caregivers to deliver context-sensitive rehabilitation, collaborative goal setting, parent psychoeducation, and family psychosocial support (31, 114, 115). Interventions of this nature enable family participation in rehabilitation and provide much needed support to families following pABI.
Understanding family needs in rehabilitation
pABI can have significant impacts on families, and protective factors such as interpersonal support, coping skills, and access to knowledge and information can buffer against decrements in family adaptation, burden, and distress (116, 117). While a family-centred approach that involves and supports families is considered best practice in pABI rehabilitation, a recent scoping review revealed that children and young people with pABI and their families report unrecognised or unmet information and emotional support needs across the care trajectory (13). This included the need for individualised information regarding the impact of the child's injury, as well as current and future treatment plans (13, 14). Families may also have high needs for emotional support, particularly following the child's return home (13–15). Greater recognition of the impacts of pABI on the whole family is also needed, as is increased support for siblings (118–120). While social support and peer connection are important for families following pABI, they may require assistance accessing such resources (73, 121). Long-term follow-up and family support in managing the ongoing sequelae of pABI, including behavioural and psychological difficulties is also a consideration (13, 14, 107).
Collaborative goal setting
Collaborative goal setting, a core component of adopting a family-centred approach in paediatric rehabilitation, is the process by which individual rehabilitation goals are identified and negotiated (122–124). Collaborative goal setting between children, families, and clinicians is considered best practice in paediatric rehabilitation, representing an opportunity for children and families to have input into care planning (11, 125, 126). Through collaboration, meaningful goals can be identified, facilitating rapport, increasing children's and families' engagement and motivation in rehabilitation and enhancing parents' feelings of competency (127–130). There is wide variability in goal setting processes among services (124, 131, 132) and formalised goal setting methods are inconsistently implemented (133, 134). Several researchers have proposed frameworks to promote engagement in goal generation. For example, Prescott and colleagues (135, 136) developed the Client-Centred Goal Setting Practice Framework for goal setting with adults with ABI in community-based rehabilitation, and Pritchard-Wiart and colleagues (137) developed a child-focused approach to goal setting, Enhancing Child Engagement in Goal Setting (ENGAGE). While neither of these frameworks are specific to pABI rehabilitation, both have potential for adaptation in this context.
Limited literature has investigated collaborative goal setting in pABI rehabilitation. Evidence regarding goal setting in the context of childhood disability more broadly has found that meaningful goals are linked to greater engagement and motivation in therapy, improved rehabilitation outcomes, and enhanced family-clinician partnership (130, 138–141). When children are involved in rehabilitation goal setting, they feel valued and heard (142), but when children's preferences are not considered, they may feel “powerless and depersonalized” (143–145). Two recent qualitative studies explored experiences of goal setting in outpatient pABI rehabilitation from the perspectives of rehabilitation clinicians (146) and children and their caregivers (147). Findings emphasised the importance of clinicians, children, and parents/caregivers collaboratively generating meaningful rehabilitation goals, and highlighted the active role of clinicians in educating young people and their parents about goal setting and supporting their engagement in goal setting. The findings of these two qualitative studies suggest that collaborative goal setting provides important opportunities for young people with pABI and their families to have input into, and direct, their own healthcare, thus aligning with a family-centred approach to rehabilitation.
Discussion
Gaps in knowledge and practice
Lack of consensus around the definition of family- centred service
Although the concept of family-centred service was introduced over five decades ago, a consensus definition has not yet been achieved and there remains a lack of clarity about how this approach should be implemented in practice (9, 11, 12). Many definitions of family-centred service have been proposed and several general principles are common among these definitions, including the open exchange of information with families, respect for family differences and care preferences, partnership and collaboration with families in decision-making at the level they choose, and the provision of care in the context of the family and their community (9). In recognition of the lack of a universal model of family-centred service, Kokorelias and colleagues (10) conducted a scoping review of family-centred models of care in paediatric and adult healthcare. A common goal of the 55 included models was the development and implementation of care plans within the context of the family. Key components to facilitate family-centred service were also identified, including: collaboration and communication among the healthcare provider, patient, and family across the illness and care trajectory; condition-specific education and support for family wellbeing; consideration of the family context, including strengths and cultural values; and the need for dedicated policies and procedures to support implementation of family-centred service models. Evidently there are many components underpinning family-centred service, and it is essential to consider how these components can be best implemented in the context of pABI rehabilitation.
Clinical implementation of family-centred service in paediatric ABI rehabilitation
Family-centred service has predominantly been investigated in the context of paediatric disability; however, most of this literature has focused on implementation in relation to congenital or developmental disabilities which are present “from the beginning” of a child's life (54). Although the key premises and elements of family-centred service are applicable and important in the care of children with pABI, rehabilitation focuses on children's recovery, whereas the “habilitation” of children with congenital or acquired disabilities focuses on optimising developmental gains (148). pABI also presents unique challenges to family adaptation due to its sudden and unforeseen nature, thus the implementation of family-centred service in this context must consider and attend to the unique needs of these families.
Limited literature has investigated the implementation of family-centred service in pABI rehabilitation. In a recent qualitative study, Botchway and colleagues (149) investigated rehabilitation models of care across a range of services, with a focus on family-centred service, psychosocial support, and transition periods. They described variability in approaches to delivering family-centred service, such as services hosting regular family meetings, providing tailored care to families, supporting families in care coordination, and engaging families in collaborative decision making. In keeping with previous literature, they also reported several barriers to family-centred service implementation, including insufficient funding and difficulty managing family dynamics, preferences, and expectations (7, 150). While family-centred service was often valued and included in services' models of care, the extent and success with which this approach was applied was often not evaluated. This suggests that services may have a limited understanding of the effectiveness of their current approaches and associated outcomes, aligning with previous literature that highlighted the need for regular evaluation of family-centred service processes to identify what is effective, and what requires modification (149, 150).
Clinical implications
There is growing evidence that involving and supporting families in pABI rehabilitation can lead to improved outcomes for children and families. This poses significant implications for clinicians working in this context (Table 1). Clinicians work together in collaboration with children and families as “advocates, knowledge brokers, collaborators, facilitators, educators and coaches” (105), “rather than just doing ‘to’ or ‘for’ them.” (95). This active role requires clinicians to be equipped with skills in two-way communication and active listening, co-constructed engagement, assessing family needs, addressing psychological challenges, negotiating child and family voices and priorities, and tailoring rehabilitation to families' unique circumstances, strengths, priorities, cultures, and values across the entire care trajectory (7, 35, 85, 90, 102, 106, 142, 149, 151–154). It is essential that clinicians are provided with adequate opportunities to develop these skills and competencies, both during their training and through ongoing professional development. Increased competence in these skills can enable clinicians to better meet families' needs and support their participation, engagement, and attendance in rehabilitation, which may in turn improve children's and families’ outcomes following pABI.
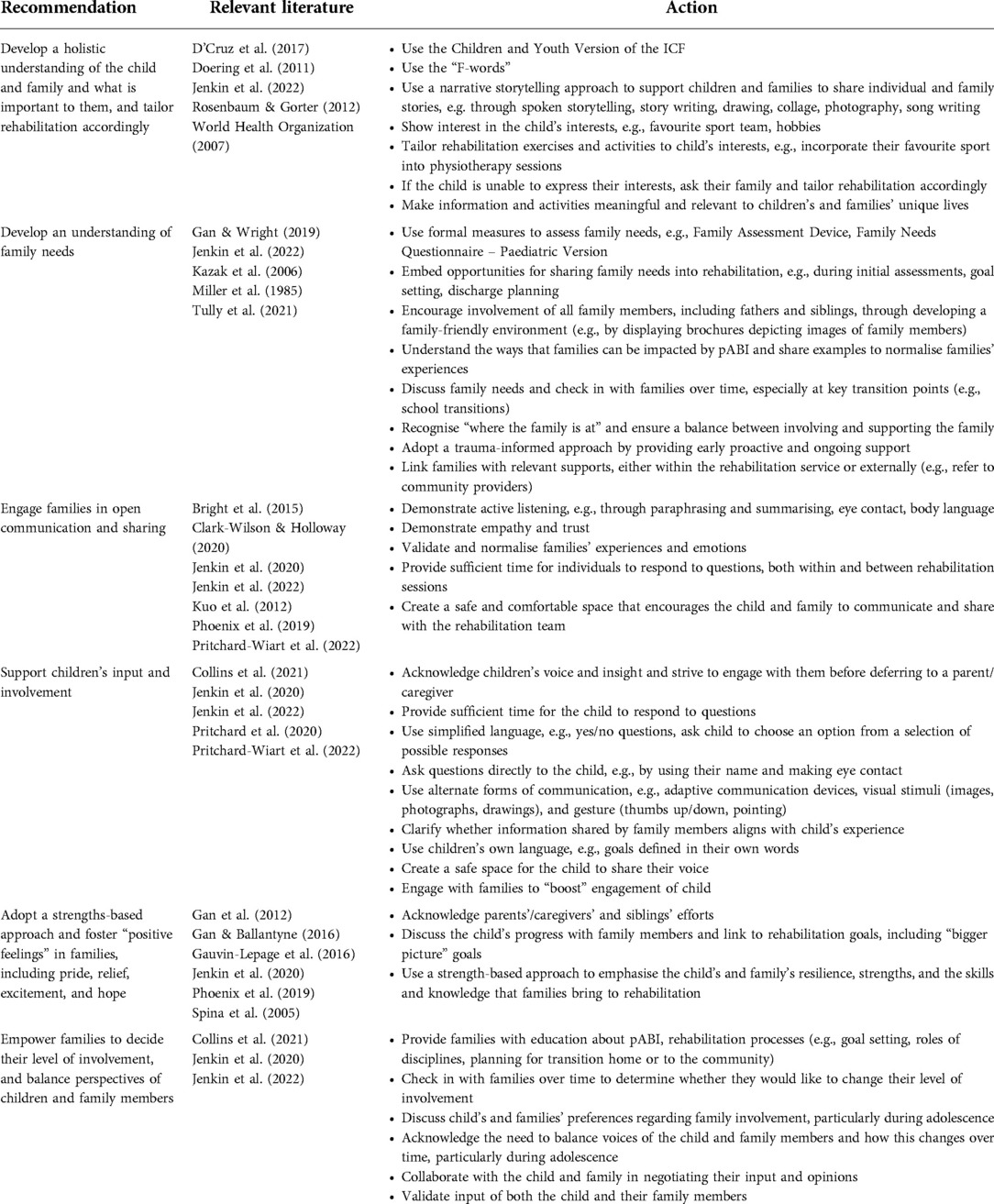
Table 1. Key recommendations and actions for clinicians.
True partnership is central to family-centred service, and it is the responsibility of clinicians to put this in place and “create space for the voice of the family to be properly heard” (35, 155). Although family-centred service represents a shift, rather than a major departure, from previous healthcare, the change in power relations that is characteristic of family-centred service may lead to clinicians feeling threatened, devalued, and unskilled (7, 152). Clinicians may feel that they lack competence and confidence to practice in a family-centred way (7, 88, 152), and may instead feel more comfortable adhering to a more traditional, biomedical model of service delivery (7). These concerns may be alleviated by increasing the focus of clinicians' training and professional development on family-centred service, and emphasising the role of clinicians in skilfully involving families in rehabilitation (152).
The implementation of family-centred service requires “innovation at multiple levels” (151), including at individual, service, and policy levels. In addition to supporting implementation through clinician training and education, it is essential that family-centred service is implemented at a service level. Professionals within organisations that emphasise family-centred values are more willing to embrace a family-centred approach, and clinicians are more willing to accept new practice approaches when guided by managers and leaders (88, 156). Importantly, rehabilitation services should strive to better articulate what they mean by “family-centred service” within their models of care, particularly given the documented variability in definitions and service approaches (9, 149, 157). This may be facilitated through the development of evidence-based best practice guidelines and targeted interventions at individual, service, and policy levels.
Future research directions
Family-centred service literature stresses that families are different and unique and that understanding family contexts is central to family-centred service delivery; however, the best approach for gaining and applying this understanding in pABI rehabilitation remains unclear. The Children and Youth Version of the ICF (158) and “F-words” (85) provide models that can assist clinicians to develop a holistic understanding of the child and their family, but have not yet been investigated in the context of pABI. Optimally clinicians should develop an understanding of, and address, family needs across the care trajectory following pABI. Although tools have been developed to assess family functioning and needs [e.g., Family Needs Questionnaire – paediatric version (159), Family Assessment Device (160)], their usefulness in pABI rehabilitation remains unclear. In developing an understanding of family needs following pABI, it is important to consider how to address families' changing needs across the care trajectory. For example, trauma-informed approaches to care may be particularly important during early, sub-acute rehabilitation to support family adaptation and coping. In contrast, later rehabilitation may focus on developing an understanding of families' unique lives and contexts to maximise children's participation in school and the community. It is therefore essential that service delivery is tailored to families' changing needs across the care trajectory and the child's developmental stages, highlighting the complexity of delivering family-centred service within the context of pABI rehabilitation.
In addition to considering family needs during rehabilitation, it would be beneficial to develop resources to support clinicians' understanding of family interests and values. There are no existing measures that assess child and family values within healthcare settings, thus this represents an area for future research innovation. Given that time is a key barrier to implementing family-centred service within rehabilitation, it is important that key stakeholders, including clinicians, are actively involved in such research efforts to ensure that such resources and tools can be feasibly implemented in practice. The use of such resources and tools would enable clinicians to adapt service delivery to families' unique needs, preferences, and values, thus enhancing family-centred service delivery.
Family participation, attendance, and engagement in children's healthcare represent under-investigated elements of family-centred service. While a recent qualitative study outlined the ways that families participate in pABI rehabilitation (107), further investigation is required to determine how clinicians and services can better support family participation and engagement in rehabilitation. For example, collaborative goal setting represents a key opportunity for families to have input into their children's healthcare. It is therefore essential that clinicians working in pABI rehabilitation develop and enhance their skills in collaborative goal setting, for example, through training packages. Providing psychoeducation and evidence-informed resources to families to support their understanding of, and engagement in, collaborative goal setting, is also key to empowering them to be actively involved in this process. Greater consideration must also be given to the participation, attendance, and engagement of family members in rehabilitation. Literature investigating family needs following pABI typically focuses on mothers' perspectives, and fathers are often under-represented in parent-focused interventions for child mental health (161–165), with common barriers including work commitments and a lack of time (166). Flexible service delivery (e.g., face-to-face and online options) is therefore essential to support fathers' engagement in children's healthcare (167). While literature focusing on family participation in children's healthcare typically focuses on parents and caregivers only, future research should also consider siblings' needs and participation.
Family-centred service is considered best practice in pABI rehabilitation, yet there remains no evidence-based clinical practice guidelines to support implementation. Given that rehabilitation tailored to children's and families' dynamic needs and preferences is essential, future research in this context must involve early, ongoing, and meaningful engagement of children with pABI and their families in study design, implementation, and evaluation to optimise feasibility and implementation of findings into clinical practice. Partnership with families, including in future research efforts, is an important step towards further improving aspects of family-centred service in pABI rehabilitation, and requires skills in family engagement across all stages of the research process. Using co-design methods to develop and evaluate training packages that support clinicians and researchers in enhancing their skills in family-centred service will also be important. Given that there is currently limited research that has investigated the effectiveness of aspects of family-centred service post-pABI, future research should aim to better understand the application of components of family-centred service in paediatric ABI rehabilitation to ensure that the unique needs of children with ABI and their families are considered.
Conclusions
Working with children with pABI and their families in rehabilitation is complex, and there is growing evidence for a family-centred approach addressing child and family needs. Despite this, there remains a lack of clarity and evidence-based guidance about how family-centred service should be delivered in pABI rehabilitation. Current literature across pABI rehabilitation and family-centred service demonstrates the active role of clinicians in implementing family-centred service and underscores the importance of family-centred approaches being adopted at the level of services' models of care. This review highlights the need for ongoing, collaborative research efforts to inform development of evidence-based guidelines for the implementation of family-centred service in pABI rehabilitation.
Author contributions
All authors contributed to the conceptualization of the review. The first author (TJ) prepared the manuscript, and VA, K'DC, AS, and SK contributed to revision of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors acknowledge the funding support for this project from the Research Training Program scholarship made available through The University of Melbourne and the Australian Commonwealth Government, and the Victorian Government's Operational Infrastructure Support Program.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Araki T, Yokota H, Morita A. Pediatric traumatic brain injury: characteristic features, diagnosis, and management. Neurol Med Chir (Tokyo). (2017) 57:82–93. doi: 10.2176/nmc.ra.2016-0191
2. Bruns J, Hauser WA. The epidemiology of traumatic brain injury: a review. Epilepsia. (2003) 44:2–10. doi: 10.1046/j.1528-1157.44.s10.3.x
3. McKinlay A, Linden M, DePompei R, Aaro Jonsson C, Anderson V, Braga L, et al. Service provision for children and young people with acquired brain injury: practice recommendations. Brain Inj. (2016) 30:1656–64. doi: 10.1080/02699052.2016.1201592
4. Chevignard M, Toure H, Brugel D, Poirier J, Laurent-Vannier A. A comprehensive model of care for rehabilitation of children with acquired brain injuries. Child Care Health Dev. (2010) 36:31–43. doi: 10.1111/j.1365-2214.2009.00949.x
5. Nutton L. Chapter 11 - acquired brain injury: acute management. In: Pountney T, editors. Physiotherapy for children. Great Britain: Butterworth-Heinemann (2007). p. 163–84.
6. Crowe L, Babl F, Anderson V, Catroppa C. The epidemiology of paediatric head injuries: data from a referral centre in Victoria, Australia. J Paediatr Child Health. (2009) 45:346–50. doi: 10.1111/j.1440-1754.2009.01499.x
7. Rosenbaum P, King S, Law M, King G, Evans J. Family-Centred service: a conceptual framework and research review. Phys Occup Ther Pediatr. (1998) 18:1–20. doi: 10.1080/J006v18n01_01
8. Shelton TL, Jeppson ES, Johnson BH. Family-centred care for children with special health care needs. Washington, DC: Association for the Care of Children’s Health (1987).
9. Kuo DZ, Houtrow AJ, Arango P, Kuhlthau KA, Simmons JM, Neff JM. Family-centered care: current applications and future directions in pediatric health care. Matern Child Health J. (2012) 16:297–305. doi: 10.1007/s10995-011-0751-7
10. Kokorelias KM, Gignac MAM, Naglie G, Cameron JI. Towards a universal model of family centered care: a scoping review. BMC Health Serv Res. (2019) 19:1–11. doi: 10.1186/s12913-019-4394-5
11. Bamm E, Rosenbaum P. Family-centered theory: origins, development, barriers, and supports to implementation in rehabilitation medicine. Arch Phys Med Rehabil. (2008) 89:1618–24. doi: 10.1016/j.apmr.2007.12.034
12. Jolley J, Shields L. The evolution of family-centered care. J Pediatr Nurs. (2009) 24:164–70. doi: 10.1016/j.pedn.2008.03.010
13. Keetley R, Radford K, Manning JC. A scoping review of the needs of children and young people with acquired brain injuries and their families. Brain Inj. (2019) 33:1117–28. doi: 10.1080/02699052.2019.1637542
14. Kirk S, Fallon D, Fraser C, Robinson G, Vassallo G. Supporting parents following childhood traumatic brain injury: a qualitative study to examine information and emotional support needs across key care transitions. Child Care Health Dev. (2014) 41:303–13. doi: 10.1111/cch.12173
15. Jones S, Davis N, Tyson SF. A scoping review of the needs of children and other family members after a child’s traumatic injury. Clin Rehabil. (2018) 32:501–11. doi: 10.1177/0269215517736672
16. Aitken M, Mele N, Barrett K. Recovery of injured children: parent perspectives on family needs. Arch Phys Med Rehabil. (2004) 85:567–73. doi: 10.1016/j.apmr.2003.06.018
17. Bedell G. Functional outcomes of school-age children with acquired brain injuries at discharge from inpatient rehabilitation. Brain Inj. (2008) 22:313–24. doi: 10.1080/02699050801978948
18. Limond J, Dorris L, McMillan T. Quality of life in children with acquired brain injury: parent perspectives 1–5 years after injury. Brain Inj. (2009) 23:617–22. doi: 10.1080/02699050902997870
19. Toga AW, Thompson PM, Sowell ER. Mapping brain maturation. Trends Neurosci. (2006) 29:148–59. doi: 10.1016/j.tins.2006.01.007
20. Sowell ER, Thompson PM, Leonard CM, Welcome SE, Kan E, Toga AW. Longitudinal mapping of cortical thickness and brain growth in Normal children. J Neurosci. (2004) 24:8223–31. doi: 10.1523/JNEUROSCI.1798-04.2004
21. Anderson V, Catroppa C, Morse S, Haritou F, Rosenfeld J. Functional plasticity or vulnerability after early brain injury? Pediatrics. (2005) 116:1374–82. doi: 10.1542/peds.2004-1728
22. Benz B, Ritz A, Kiesow S. Influence of age-related factors on long-term outcome after traumatic brain injury (TBI) in children: a review of recent literature and some preliminary findings. Restor Neurol Neurosci. (1999) 14:135–41. PMID: 12671257
23. Ewing-Cobbs L, Barnes M, Fletcher J, Levin H, Swank P, Song J. Modeling of longitudinal academic achievement scores after pediatric traumatic brain injury. Dev Neuropsychol. (2004) 25:107–33. doi: 10.1080/87565641.2004.9651924
24. Koskiniemi M, Kyykkä T, Nybo T, Jarho L. Long-term outcome after severe brain injury in preschoolers is worse than expected. Arch Pediatr Adolesc Med. (1995) 149:249–54. doi: 10.1001/archpedi.1995.02170150029004
25. Taylor H, Alden J. Age-related differences in outcomes following childhood brain insults: an introduction and overview. J Int Neuropsychol Soc. (1997) 3:555–67. doi: 10.1017/s1355617797005559
26. Linden M, McKinlay A. Childhood acquired brain injury affects adult outcomes. Disabil Rehabil. (2020) 42:2381–2. doi: 10.1080/09638288.2019.1660916
27. Bursnall S, Kendall E, Degeneffe CE. Regaining equilibrium: understanding the process of sibling adjustment to pediatric acquired brain injury. Rehabil Psychol. (2018) 63:447–59. doi: 10.1037/rep0000225
28. Wagner M, Stenger K. Acute brain injury: A guide for family and friends. Iowa: University of Iowa Health Care, University Hospital School (2000).
29. Wade S, Taylor H, Drotar D, Stancin T, Yeates K, Minich N. A prospective study of long-term caregiver and family adaptation following brain injury in children. J Head Trauma Rehabil. (2002) 17:96–111. doi: 10.1097/00001199-200204000-00003
30. Wade S, Taylor H, Drotar D, Stancin T, Yeates K. Childhood traumatic brain injury: initial impact on the family. J Learn Disabil. (1996) 29:652–61. Available at: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=8942309 doi: 10.1177/002221949602900609
31. Hickey L, Anderson V, Jordan B. Family forward: promoting family adaptation following pediatric acquired brain injury. J Soc Work Disabil Rehabil. (2016) 15:179–200. doi: 10.1080/1536710X.2016.1220884
32. Micklewright JL, King TZ, O’Toole K, Henrich C, Floyd FJ. Parental distress, parenting practices, and child adaptive outcomes following traumatic brain injury. J Int Neuropsychol Soc. (2012) 18:343–50. doi: 10.1017/S1355617711001792
33. Wade S, Taylor H, Yeates K, Drotar D, Stancin T, Minich N, et al. Long-term parental and family adaptation following pediatric brain injury. J Pediatr Psychol. (2006) 31:1072–83. doi: 10.1093/jpepsy/jsj077
34. Analytis P, Warren N, Crichton A, Knight S, Ponsford J. Coping and wellbeing in families with a child with acquired brain injury compared with families in the community. Disabil Rehabil. (2021): 1–8. doi: 10.1080/09638288.2021.2008522
35. Clark-Wilson J, Holloway M. Family experience of brain injury: surviving, coping, adjusting. Oxon: Routledge (2020).
36. Gill D, Wells D. Forever different: experiences of living with a sibling who has a traumatic brain injury. Rehabil Nurs. (2000) 25:48–53. doi: 10.1002/j.2048-7940.2000.tb01862.x
37. Catroppa C, Anderson V, Morse S, Haritou F, Rosenfeld J. Outcome and predictors of functional recovery 5 years following pediatric traumatic brain injury (TBI). J Pediatr Psychol. (2008) 33:707–18. doi: 10.1093/jpepsy/jsn006
38. Anderson V, Catroppa C, Haritou F, Morse S, Pentland L, Rosenfeld J, et al. Predictors of acute child and family outcome following traumatic brain injury in children. Pediatr Neurosurg. (2001) 34:138–48. doi: 10.1159/000056009
39. Ryan N, van Bijnen L, Catroppa C, Beauchamp M, Crossley L, Hearps S, et al. Longitudinal outcome and recovery of social problems after pediatric traumatic brain injury (TBI): contribution of brain insult and family environment. Int J Dev Neurosci. (2016) 49:23–30. doi: 10.1016/j.ijdevneu.2015.12.004
40. Robson T, Ziviani J, Spina S. Personal experiences of families of children with a traumatic brain injury in the transition from hospital to home. Brain Impair. (2005) 6:45–55. doi: 10.1375/brim.6.1.45.65477
41. Wade S, Taylor H, Drotar D, Stancin T, Yeates K, Minich N. Parent-adolescent interactions after traumatic brain injury: their relationship to family adaptation and adolescent adjustment. J Head Trauma Rehabil. (2003) 18:164–76. doi: 10.1097/00001199-200303000-00007
42. Rivara JB, Fay G, Jaffe KM, Polissar NL, Shurtleff HA, Martin KM. Predictors of family functioning one year following traumatic brain injury in children. Arch Phys Med Rehabil. (1992) 73:899–910. doi: 10.5555/uri:pii:000399939290259Y
43. Rivara JB, Jaffe KM, Polissar NL, Fay GC, Liao S, Martin KM. Predictors of family functioning and change 3 years after traumatic brain injury in children. Arch Phys Med Rehabil. (1996) 77:754–64. doi: 10.1016/S0003-9993(96)90253-1
44. Hickey L, Anderson V, Hearps S, Jordan B. Family appraisal of paediatric acquired brain injury: a social work clinical intervention trial. Dev Neurorehabil. (2018) 21:457–64. doi: 10.1080/17518423.2018.1434697
45. Brown F, Whittingham K, McKinlay L, Boyd R, Sofronoff K. Efficacy of stepping stones triple P plus a stress management adjunct for parents of children with an acquired brain injury: the protocol of a randomised controlled trial. Brain Impair. (2013) 14:253–69. doi: 10.1017/BrImp.2013.18
46. Brown F, Whittingham K, Boyd R, McKinlay L, Sofronoff K. Does stepping stones triple P plus acceptance and commitment therapy improve parent, couple, and family adjustment following paediatric acquired brain injury? A randomised controlled trial. Behav Res Ther. (2015) 73:58–66. doi: 10.1016/j.brat.2015.07.001
47. Kauffman J. Loss of the assumptive world: a theory of traumatic loss. New York and London: Brunner-Routledge (2002).
48. Collings C. That’s not my child anymore! parental grief after acquired brain injury (ABI): incidence, nature and longevity. Br J Soc Work. (2008) 38:1499–517. doi: 10.1093/bjsw/bcm055
49. DeMarle D, Roux P. The life cycle and disability: experiences of discontinuity in child and family development. J Loss Trauma. (2001) 6:29–43. doi: 10.1080/108114401753197459
50. Jordan J, Linden MA. “It’s like a problem that doesn’t exist”: the emotional well-being of mothers caring for a child with brain injury. Brain Inj. (2013) 27:1063–72. doi: 10.3109/02699052.2013.794962
51. Savage RC, Depompei R, Tyler J, Lash M. Paediatric traumatic brain injury: a review of pertinent issues. Pediatr Rehabil. (2005) 8:92–103. doi: 10.1080/13638490400022394
52. Analytis P. The sibling relationship after acquired brain injury: family dynamics across the lifespan. Oxon: Routledge (2021).
53. Guerriere D, McKeever P. Mothering children who survive brain injuries: playing the hand you’re dealt. J Spec Pediatr Nurs. (1997) 2:105–15. doi: 10.1111/j.1744-6155.1997.tb00067.x
54. Bragg R, Brown R, Berninger V. The impact of congenital and acquired disabilities on the family system: implications for school counseling. Sch Couns. (1992) 39:292–9. ISSN-0036-6536
55. Schmidt A, Orsten K, Hanten G, Li X, Levin H. Family environment influences emotion recognition following paediatric traumatic brain injury. Brain Inj. (2010) 24:1550–60. doi: 10.3109/02699052.2010.523047
56. Taylor H, Drotar D, Wade S, Yeates K, Stancin T, Klein S. Recovery from TBI in children: the importance of the family. In: Michel ME, editors. Traumatic head injury in children. New York, NY: Oxford University Press (1995). p. 188–216.
57. Lax Pericall MT, Taylor E. Family function and its relationship to injury severity and psychiatric outcome in children with acquired brain injury: a systematized review. Dev Med Child Neurol. (2014) 56:19–30. doi: 10.1111/dmcn.12237
58. Ylvisaker M, Adelson PD, Braga LW, Burnett SM, Glang A, Feeney T, et al. Rehabilitation and ongoing support after pediatric TBI: twenty years of progress. J Head Trauma Rehabil. (2005) 20:95–109. doi: 10.1177/089431849801100310
59. Yeates K, Taylor H, Walz N, Stancin T, Wade S. The family environment as a moderator of psychosocial outcomes following traumatic brain injury in young children. Neuropsychology. (2010) 24:345–56. doi: 10.1037/a0018387
60. Taylor H, Yeates K, Wade S, Drotar D, Stancin T, Burant C. Bidirectional child-family influences on outcomes of traumatic brain injury in children. J Int Neuropsychol Soc. (2001) 7:755–67. doi: 10.1017/S1355617701766118
61. Taylor H. Research on outcomes of pediatric traumatic brain injury: current advances and future directions. Dev Neuropsychol. (2004) 25:199–225. doi: 10.1080/87565641.2004.9651928
62. Rivara JB, Jaffe KM, Polissar NL, Fay GC, Martin KM, Shurtleff HA, et al. Family functioning and children’s academic performance and behavior problems in the year following traumatic brain injury. Arch Phys Med Rehabil. (1994) 75:369–79. doi: 10.1016/0003-9993(94)90157-0
65. Bowen M. The use of family theory in clinical practice. Compr Psychiatry. (1966) 7:345–74. doi: 10.1016/S0010-440X(66)80065-2
66. World Health Organization. Rehabilitation (2021). https://www.who.int/news-room/fact-sheets/detail/rehabilitation
67. Anderson V, Catroppa C. Advances in postacute rehabilitation after childhood-acquired brain injury: a focus on cognitive, behavioral, and social domains. Am J Phys Med Rehabil. (2006) 85:767–77. doi: 10.1097/01.phm.0000233176.08480.22
68. Giza C, Kolb B, Harris N, Asarnow R, Prins M. Hitting a moving target: basic mechanisms of recovery from acquired developmental brain injury. Dev Neurorehabil. (2009) 12:255–68. doi: 10.3109/17518420903087558
69. Cronin AF. Traumatic brain injury in children: issues in community function. Am J Occup Ther. (2001) 55:377–84. doi: 10.5014/ajot.55.4.377
70. Slomine BS, McCarthy ML, Ding R, MacKenzie EJ, Jaffe KM, Aitken ME, et al. Health care utilization and needs after pediatric traumatic brain injury. Pediatrics. (2006) 117:e663–74. doi: 10.1542/peds.2005-1892
71. Greenspan A, MacKenzie E. Use and need for post-acute services following paediatric head injury. Brain Inj. (2000) 14:417–29. doi: 10.1080/026990500120529
72. Aukema EJ, Last BF, Schouten-Van Meeteren AYN, Grootenhuis MA. Explorative study on the aftercare of pediatric brain tumor survivors: a parents’ perspective. Support Care Cancer. (2011) 19:1637–46. doi: 10.1007/s00520-010-0995-6
73. Manning JC, Hemingway P, Redsell SA. Survived so what? Identifying priorities for research with children and families post-paediatric intensive care unit. Nurs Crit Care. (2018) 23:68–74. doi: 10.1111/nicc.12298
74. Anderson V, Northam E, Wrennall J. Developmental neuropsychology: a clinical approach. 2nd ed. New York: Routledge (2019).
75. Fordyce W. ACRM Presidential address on interdisciplinary peers. Arch Phys Med Rehabil. (1981) 62:51–3. PMID: 7235885
76. Prigatano GP. Principles of neuropsychological rehabilitation. New York: Oxford University Press (1999).
77. Mandy P. Interdisciplinary rather than multidisciplinary or generic practice. Br J Ther Rehabil. (1996) 3:110–2. doi: 10.12968/bjtr.1996.3.2.14871
78. Fay D, Borrill C, Amir Z, Haward R, West M. Getting the most out of multidisciplinary teams: a multi-sample study of team innovation in health care. J Occup Organ Psychol. (2006) 79:553–67. doi: 10.1348/096317905X72128
79. Wilson B, Gracey F, Evans JJ, Bateman A. Neuropsychological rehabilitation: theory, models, therapy and outcome. London: Cambridge University Press (2009).
80. Singh R, Küçükdeveci A, Grabljevec K, Gray A. The role of interdisciplinary teams in physical and rehabilitation medicine. J Rehabil Med. (2018) 50:673–8. doi: 10.2340/16501977-2364
81. Gan C, DePompei R. Lash M. “family assessment and intervention.,” brain injury medicine. New York: Demos Medical Publishing (2012). 621–34.
82. Spina S, Ziviani J, Nixon J. Children, brain injury and the resiliency model of family adaptation. Brain Impair. (2005) 6:33–44. doi: 10.1375/brim.6.1.33.65478
83. Gauvin-Lepage J, Lefebvre H, Malo D. Resilience in families of adolescents with traumatic brain injuries: development of a support intervention. Brain Inj. (2016) 30(5–6):552–3. doi: 10.3109/02699052.2016.1162060
84. Gan C, Ballantyne M. Brain injury family intervention for adolescents: a solution-focused approach. NeuroRehabilitation. (2016) 38:231–41. doi: 10.3233/NRE-1601315
85. Rosenbaum P, Gorter JW. The ‘F-words’ in childhood disability: i swear this is how we should think!. Child Care, Heal Dev. (2012) 38:457–63. doi: 10.1111/j.1365-2214.2011.01338.x
86. Kraus de Camargo O. Chapter 1 the ICF and the biopsychosocial model of health: from ‘disease’ to ‘health condition’. In: Kraus de Canargo O, Simon L, Ronen GM, Rosenbaum PL, editors. ICF: a hands-on approach for clinicians and families. London: Mac Keith Press (2019). p. 8–18.
87. World Health Organization. International classification of functioning, disability and health (ICF). Geneva, Switzerland: World Health Organization (2001).
89. CanChild. F-Words in Childhood Disability (2021). Available at: https://www.canchild.ca/en/research-in-practice/f-words-in-childhood-disability (Accessed September 27, 2021).
90. Soper A, Cross A, Rosenbaum P, Gorter JW. Service Providers’ perspectives on using the ‘F-words in childhood disability’: an international survey. Phys Occup Ther Pediatr. (2020) 40:534–45. doi: 10.1080/01942638.2020.1726551
91. Coyne I. Families’ and health-care professionals’ perspectives and expectations of family-centred care: hidden expectations and unclear roles. Heal Expect. (2015) 18:796–808. doi: 10.1111/hex.12104
92. Shields L, Nixon J. Hospital care of children in four countries. J Adv Nurs. (2004) 45:475–86. doi: 10.1046/j.1365-2648.2003.02930.x
93. Law M, Rosenbaum P, King G, King S, Burke-Gaffney J, Moning-Szkut T, et al. What is family-centred service [Fact sheet]. ON, Canada (2003). Available at: https://canchild.ca/system/tenon/assets/attachments/000/003/749/original/FCS_Sheet_1.pdf
94. Odom SL, Yoder P, Hill G. Developmental intervention for infants with handicaps: purposes and programs. J Spec Educ. (1988) 22:11–24. doi: 10.1177/002246698802200105
95. Institute for Patient- and Family-Centered Care. What is Patient- and Family-Centered Care? Available at: http://www.ipfcc.org/about/pfcc.html
96. Phoenix M, Jack S, Rosenbaum P, Missiuna C. Parents’ attendance, participation and engagement in children’s developmental rehabilitation services: part 1. Contextualizing the journey to child health and happiness. Disabil Rehabil. (2020) 42:2141–50. doi: 10.1080/09638288.2018.1555617
97. Siebes R, Wijnroks L, Ketelaar M, van Schie P, Gorter J, Vermeer A. Parent participation in paediatric rehabilitation treatment centres in The Netherlands: a parents’ viewpoint. Child Care Health Dev. (2007) 33:196–205. doi: 10.1111/j.1365-2214.2006.00636.x
98. Littell J, Alexander L, Reynolds W. Client participation: central and underinvestigated elements of intervention. Soc Serv Rev. (2001) 75:1–28. doi: 10.1086/591880
99. Imms C, Granlund M, Wilson PH, Steenbergen B, Rosenbaum PL, Gordon AM. Participation, both a means and an end: a conceptual analysis of processes and outcomes in childhood disability. Dev Med Child Neurol. (2017) 59:16–25. doi: 10.1111/dmcn.13237
100. Imms C, Adair B, Keen D, Ullenhag A, Rosenbaum P, Granlund M. “Participation”: a systematic review of language, definitions, and constructs used in intervention research with children with disabilities. Dev Med Child Neurol. (2015) 58:29–38. doi: 10.1111/dmcn.12932
101. Staudt M. Treatment engagement with caregivers of at-risk children: gaps in research and conceptualization. J Child Fam Stud. (2007) 16:183–96. doi: 10.1007/s10826-006-9077-2
102. Bright F, Kayes N, Worrall L, Mcpherson K. A conceptual review of engagement in healthcare and rehabilitation. Disabil Rehabil. (2015) 37:643–54. doi: 10.3109/09638288.2014.933899
103. D’Arrigo R, Ziviani J, Poulsen A, Copley J, King G. Child and parent engagement in therapy: what is the key? Aust Occup Ther J. (2017) 64:340–3. doi: 10.1111/1440-1630.12279
104. King G, Currie M, Petersen P. Child and parent engagement in the mental health intervention process: a motivational framework. Child Adolesc Ment Health. (2014) 19:2–8. doi: 10.1111/camh.12015
105. Imms C. Therapy as a life situation. In: Christine Imms & Dido Green. Participation: optimising outcomes in childhood-onset neurodisability. London: Mac Keith Press (2020). p. 97–104.
106. Phoenix M, Jack S, Rosenbaum P, Missiuna C. A grounded theory of parents’ attendance, participation and engagement in children’s developmental rehabilitation services: part 2. The journey to child health and happiness. Disabil Rehabil. (2019) 42:2151–60. doi: 10.1080/09638288.2018.1555618
107. Jenkin T, D’Cruz K, Anderson V, Scheinberg A, Knight S. Family-centred service in paediatric acquired brain injury rehabilitation: perspectives of children and adolescents and their families. Disabil Rehabil. (2022):1–12. doi: 10.1080/09638288.2022.2121864
108. Cermak CA, McCabe SA, Kuchurean B, Schaefer J, Tendera A, Beal DS. Parent interventions improve behavior after pediatric traumatic brain injury. J Head Trauma Rehabil. (2022):293–302. doi: 10.1097/htr.0000000000000766
109. Aguilar J, Cassedy A, Shultz E, Kirkwood M, Stancin T, Yeates K, et al. A comparison of 2 online parent skills training interventions for early childhood brain injury: improvements in internalizing and executive function behaviors. J Head Trauma Rehabil. (2019) 34:65–76. doi: 10.1097/HTR.0000000000000443
110. Wade S, Cassedy A, Shultz E, Zang H, Zhang N, Kirkwood M, et al. Randomized clinical trial of online parent training for behavior problems after early brain injury. J Am Acad Child Adolesc Psychiatry. (2017) 56:930–939.e2. doi: 10.1016/j.jaac.2017.09.413
111. Wade S, Michaud L, Maines Brown T. Putting the pieces together: preliminary efficacy of a family problem-solving intervention for children with traumatic brain injury. J Head Trauma Rehabil. (2006) 21:57–67. doi: 10.1097/00001199-200601000-00006
112. Wade S, Carey J, Wolfe C. The efficacy of an online cognitive-behavioral family intervention in improving child behavior and social competence following pediatric brain injury. Rehabil Psychol. (2006) 51:179–89. doi: 10.1037/0090-5550.51.3.179
113. Brown F, Whittingham K, Boyd R, McKinlay L, Sofronoff K. Improving child and parenting outcomes following paediatric acquired brain injury: a randomised controlled trial of stepping stones triple P plus acceptance and commitment therapy. J Child Psychol Psychiatry. (2014) 55:1172–83. doi: 10.1111/jcpp.12227
114. Holthe IL, Rohrer-Baumgartner N, Svendsen EJ, Hauger SL, Forslund MV, Borgen IMH, et al. Feasibility and acceptability of a Complex telerehabilitation intervention for pediatric acquired brain injury: the child in context intervention (CICI). J Clin Med. (2022) 11:1–23. doi: 10.3390/jcm11092564
115. Braga L, Da Paz Júnior A, Ylvisaker M. Direct clinician-delivered versus indirect family-supported rehabilitation of children with traumatic brain injury: a randomized controlled trial. Brain Inj. (2005) 19:819–31. doi: 10.1080/02699050500110165
116. Stancin T, Wade S, Walz N, Yeates K, Taylor H. Traumatic brain injuries in early childhood: initial impact on the family. J Dev Behav Pediatr. (2008) 29:253–61. doi: 10.1097/DBP.0b013e31816b6b0f
117. Wade S, Stancin T, Taylor H, Drotar D, Yeates K, Minich N. Interpersonal stressors and resources as predictors of parental adaptation following pediatric traumatic injury. J Consult Clin Psychol. (2004) 72:776–84. doi: 10.1037/0022-006X.72.5.776
118. Hermans E, Winkens I, Winkel-Witlox S, van Iperen A. Caregiver reported problems of children and families 2-4 years following rehabilitation for pediatric brain injury. NeuroRehabilitation. (2012) 30:213–7. doi: 10.3233/NRE-2012-0747
119. Manning JC, Hemingway P, Redsell SA. Long-term psychosocial impact reported by childhood critical illness survivors: a systematic review. Nurs Crit Care. (2014) 19:145–56. doi: 10.1111/nicc.12049
120. Soanes L, Hargrave D, Smith L, Gibson F. What are the experiences of the child with a brain tumour and their parents? Eur J Oncol Nurs. (2009) 13:255–61. doi: 10.1016/j.ejon.2009.03.009
121. Roscigno CI, Swanson KM, Vavilala MS, Solchany J. Children’s longing for everydayness: life following traumatic brain injury in the USA. Brain Inj. (2011) 25:882–94. doi: 10.3109/02699052.2011.581638
122. Evans J. Goal setting during rehabilitation early and late after acquired brain injury. Curr Opin Neurol. (2012) 25:651–5. doi: 10.1097/WCO.0b013e3283598f75
123. Evans J, Krasny-Pacini A. Goal setting in rehabilitation. In: Wilson B, Winegardner J, Van Heugten CM, Ownsworth T, editors. Neuropsychological rehabilitation: the international handbook. London and New York: Routledge (2017). p. 49–57.
124. Wade D. Goal setting in rehabilitation: an overview of what, why and how. Clin Rehabil. (2009) 23:291–5. doi: 10.1177/0269215509103551
125. Hanna K, Rodger S. Towards family-centred practice in paediatric occupational therapy: a review of the literature on parent-therapist collaboration. Aust Occup Ther J. (2002) 49:14–24. doi: 10.1046/j.0045-0766.2001.00273.x
126. Brewer K, Pollock N, Wright F. Addressing the challenges of collaborative goal setting with children and their families. Phys Occup Ther Pediatr. (2014) 34:138–52. doi: 10.3109/01942638.2013.794187
127. Armstrong J. The benefits and challenges of interdisciplinary, client-centred, goal setting in rehabilitation. New Zeal J Occup Ther. (2008) 55:20–5. ISSN:1171-0462
128. Østensjo S, Øien I, Fallang B. Goal-oriented rehabilitation of preschoolers with cerebral palsy - a multi-case study of combined use of the Canadian occupational performance measure (COPM) and the goal attainment scaling (GAS). Dev Neurorehabil. (2008) 11:252–9. doi: 10.1080/17518420802525500
129. Lammi B, Law M. The effects of family-centred functional therapy on the occupational performance of children with cerebral palsy. Can J Occup Ther. (2003) 70:285–97. doi: 10.1177/000841740307000505
130. King G, Chiarello L. Family-Centered care for children with cerebral palsy: conceptual and practical considerations to advance care and practice. J Child Neurol. (2014) 29:1046–54. doi: 10.1177/0883073814533009
131. Playford ED, Siegert R, Levack W, Freeman J. Areas of consensus and controversy about goal setting in rehabilitation: a conference report. Clin Rehabil. (2009) 23:334–44. doi: 10.1177/0269215509103506
132. Scobbie L, Duncan EA, Brady MC, Wyke S. Goal setting practice in services delivering community-based stroke rehabilitation: a United Kingdom (UK) wide survey. Disabil Rehabil. (2015) 37:1291–8. doi: 10.3109/09638288.2014.961652
133. Nijhuis BJG, Reinders-Messelink HA, de Blécourt ACE, Ties JG, Boonstra AM, Groothoff JW, et al. Needs, problems and rehabilitation goals of young children with cerebral palsy as formulated in the rehabilitation activities profile for children. J Rehabil Med. (2008) 40:347–54. doi: 10.2340/16501977-0182
134. Darrah J, Wiart L, Magill-Evans J, Ray L, Andersen J. Are family-centred principles, functional goal setting and transition planning evident in therapy services for children with cerebral palsy? Child Care Health Dev. (2012) 38:41–7. doi: 10.1111/j.1365-2214.2010.01160.x
135. Prescott S, Fleming J, Doig E. Rehabilitation goal setting with community dwelling adults with acquired brain injury: a theoretical framework derived from clinicians’ reflections on practice. Disabil Rehabil. (2018) 40:2388–99. doi: 10.1080/09638288.2017.1336644
136. Prescott S, Fleming J, Doig E. Refining a clinical practice framework to engage clients with brain injury in goal setting. Aust Occup Ther J. (2019) 66:313–25. doi: 10.1111/1440-1630.12556
137. Pritchard-Wiart L, Thompson-Hodgetts S, McKillop AB, Rosychuk R, Mrklas K, Zwaigenbaum L, et al. A multi-center, pragmatic, effectiveness-implementation (hybrid I) cluster randomized controlled trial to evaluate a child-oriented goal-setting approach in paediatric rehabilitation (the ENGAGE approach): a study protocol. BMC Pediatr. (2022) 22:1–11. doi: 10.1186/s12887-022-03381-4
138. Pritchard-Wiart L, Phelan SK. Goal setting in paediatric rehabilitation for children with motor disabilities: a scoping review. Clin Rehabil. (2018) 32:954–66. doi: 10.1177/0269215518758484
139. Cuskelly M, King G. Know the child: maximizing engagement and persistence. In: Ziviani J, Poulsen A, Cuskelly M, editors. The art and science of motivation: a therapist’s guide to working with children. London: Jessica Kingsley Publishers (2013). p. 193–223.
140. Ziviani J, Poulsen A. Autonomy in the process of goal setting. In: Poulsen A, Ziviani J, Cuskelly M, editors. Goal setting and motivation in therapy. Philadelphia (PA): Jessica Kingsley (2015). p. 40–50.
141. Poulsen A, Rodger S, Ziviani J. Understanding children’s motivation from a self-determination theoretical perspective: implications for practice. Aust Occup Ther J. (2006) 53:78–86. doi: 10.1111/j.1440-1630.2006.00569.x
142. Pritchard L, Phelan S, McKillop A, Andersen J. Child, parent, and clinician experiences with a child-driven goal setting approach in paediatric rehabilitation. Disabil Rehabil. (2022) 44(7):1–8. doi: 10.1080/09638288.2020.1788178. [Epub ahead of print]32393074
143. Runeson I, Hallström I, Elander G, Hermerén G. Children’s participation in the decision-making process during hospitalization: an observational study. Nurs Ethics. (2002) 9:583–98. doi: 10.1191/0969733002ne553oa
144. Coyne I. Children’s participation in consultations and decision-making at health service level: a review of the literature. Int J Nurs Stud. (2008) 45:1682–9. doi: 10.1016/j.ijnurstu.2008.05.002
145. Coyne I, Hallström I, Söderbäck M. Reframing the focus from a family-centred to a child-centred care approach for children’s healthcare. J Child Heal Care. (2016) 20:494–502. doi: 10.1177/1367493516642744
146. Jenkin T, Anderson V, D’Cruz K, Collins A, Muscara F, Scheinberg A, et al. Engaging children and adolescents with acquired brain injury and their families in goal setting: the clinician perspective. Neuropsychol Rehabil. (2022) 32(1):1–27. doi: 10.1080/09602011.2020.1801470. [Epub ahead of print]32677539
147. Collins A, D’Cruz K, Jackman A, Anderson V, Jenkin T, Scheinberg A, et al. Engaging children and adolescents with acquired brain injury and their families in goal setting: the family perspective. Neuropsychol Rehabil. (2021):1–23. doi: 10.1080/09602011.2021.1977154. [Epub ahead of print]34538207
148. Hayton J, Dimitriou D. What’s in a word? Distinguishing between habilitation and Re-habilitation. Int J Orientat Mobil. (2019) 10:1–4. doi: 10.21307/ijom-2019-007
149. Botchway E, Knight S, Muscara F, Greenham M, D’Cruz K, Bonyhady B, et al. Rehabilitation models of care for children and youth living with traumatic brain and/or spinal cord injuries: a focus on family-centred care, psychosocial wellbeing, and transitions. Neuropsychol Rehabil. (2022) 32(4):537–59. doi: 10.1080/09602011.2020.1833945. [Epub ahead of print]33108961
150. Uhl T, Fisher K, Docherty SL, Brandon DH. Insights into patient and family-centered care through the hospital experiences of parents. JOGNN - J Obstet Gynecol Neonatal Nurs. (2013) 42:121–31. doi: 10.1111/1552-6909.12001
151. Lawlor MC, Mattingly CF. The complexities embedded in family-centered care. Am J Occup Ther. (1998) 52:259–67. doi: 10.5014/ajot.52.4.259
152. Litchfield R, MacDougall C. Professional issues for physiotherapists in family-centred and community-based settings. Aust J Physiother. (2002) 48:105–12. doi: 10.1016/S0004-9514(14)60204-X
153. King G, Currie M, Bartlett D, Gilpin M, Willoughby C, Tucker M, et al. The development of expertise in pediatric rehabilitation therapists: changes in approach, self-knowledge, and use of enabling and customizing strategies. Dev Neurorehabil. (2007) 10:223–40. doi: 10.1080/17518420701302670
154. Bright F, Kayes N, Cummins C, Worrall L, McPherson K. Co-constructing engagement in stroke rehabilitation: a qualitative study exploring how practitioner engagement can influence patient engagement. Clin Rehabil. (2017) 31:1396–405. doi: 10.1177/0269215517694678
155. Shields L. What is “family-centered care”? Eur J Pers Centered Healthc. (2015) 3:139. doi: 10.5750/ejpch.v3i2.993
156. Lloyd B, Elkins M, Innes L. Barriers and enablers of patient and family centred care in an Australian acute care hospital: perspectives of health managers. Patient Exp J. (2018) 5:55–64. doi: 10.35680/2372-0247.1270
157. Uniacke S, Browne TK, Shields L. How should we understand family-centred care? J Child Heal Care. (2018) 22:460–9. doi: 10.1177/1367493517753083
158. World Health Organization. International classification of functioning disability and health – children and youth version. 1st ed. Geneva World Health Organization (2007).
159. Gan C, Wright F. Development of the family needs questionnaire - pediatric version [FNQ-P] - phase I. Brain Inj. (2019) 33:623–32. doi: 10.1080/02699052.2019.1566836
160. Miller I, Bishop D, Epstein N, Keitner G. The McMaster family assessment device: reliability and validity. J Marital Fam Ther. (1985) 11:345–56. doi: 10.1111/j.1752-0606.1985.tb00028.x
161. Tiano J, McNeil C. The inclusion of fathers in behavioral parent training: a critical evaluation. Child Fam Behav Ther. (2005) 27:1–28. doi: 10.1300/J019v27n04_01
162. Fabiano G. Father participation in behavioral parent training for ADHD: review and recommendations for increasing inclusion and engagement. J Fam Psychol. (2007) 21:683–93. doi: 10.1037/0893-3200.21.4.683
163. Bögels S, Phares V. Fathers’ role in the etiology, prevention and treatment of child anxiety: a review and new model. Clin Psychol Rev. (2008) 28:539–58. doi: 10.1016/j.cpr.2007.07.011
164. Panter-Brick C, Burgess A, Eggerman M, McAllister F, Pruett K, Leckman J. Practitioner review: engaging fathers: recommendations for a game change in parenting interventions based on a systematic review of the global evidence. J Child Psychol Psychiatry. (2014) 55:1187–212. doi: 10.1111/jcpp.12280
165. Flippin M, Crais E. The need for more effective father involvement in early autism intervention: a systematic review and recommendations. J Early Interv. (2011) 33:24–50. doi: 10.1177/1053815111400415
166. Tully L, Collins D, Piotrowska P, Mairet K, Hawes D, Moul C, et al. Examining practitioner competencies, organizational support and barriers to engaging fathers in parenting interventions. Child Psychiatry Hum Dev. (2018) 49:109–22. doi: 10.1007/s10578-017-0733-0
167. Tully L, Hawes D, Dadds M. Engaging fathers in family-based interventions for child mental health. In: Allen JL, Hawes DJ, Essau CA, editors. Family-Based intervention for child and adolescent mental health: a core competencies approach. London: Cambridge University Press (2021). p. 53–66. doi: 10.1017/9781108682053.006
Keywords: acquired brain injury (ABI), family-centred service, paediatric rehabilitation, family-centred care, rehabilitation
Citation: Jenkin T, Anderson VA, D'Cruz K, Scheinberg A and Knight S (2022) Family-centred service in paediatric acquired brain injury rehabilitation: Bridging the gaps. Front. Rehabilit. Sci. 3:1085967. doi: 10.3389/fresc.2022.1085967
Received: 31 October 2022; Accepted: 30 November 2022;
Published: 23 December 2022.
Edited by:
Erika Molteni, King's College London, United KingdomReviewed by:
Gillian Hotz, University of Miami, United StatesSandra Strazzer, Eugenio Medea (IRCCS), Italy
Linda Ewing-Cobbs, University of Texas Health Science Center at Houston, United States
© 2022 Jenkin, Anderson, D'Cruz, Scheinberg and Knight. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sarah Knight sarah.knight@mcri.edu.au
Specialty Section: This article was submitted to paediatric Rehabilitation, a section of the journal Frontiers in Rehabilitation Sciences