Virtual reality and music's impact on psychological well-being
 Stephen Alexanian
Stephen Alexanian Maxwell Foxman
Maxwell Foxman Danny Pimentel2
Danny Pimentel2
- 1School of Journalism and Communication, University of Oregon, Eugene, OR United States
- 2University of Oregon, Oregon Reality Labs, School of Journalism and Communication, Portland, OR, United States
Quality of life is bound to psychological well-being, which in turn is affected by the frequency and magnitude of negative mood states. To regulate mood states, humans often consume media such as music and movies, with varied degrees of effectiveness. The current investigation examined the effectiveness of virtual reality (VR) vs. two-dimensional (2D) online interventions with various stimuli (audiovisual vs. visual only vs. audio only) to assess which interventions were most effective for improved well-being. Additionally, this study examined which groups displayed the highest amount of perceived presence to understand what components are essential when maximizing a person's subjective feeling of being “in” a new place and if this translated toward therapeutic results. Our data suggests that even though VR participants generally experienced more presence and had similar benefits as 2D groups for increasing positive mood, only participants in the 2D groups had a reduction in negative mood overall with 2D audiovisual participants experiencing the best results. These results contradict past studies which indicate that there could be other psychological and theoretical considerations that may play a role in determining what online experiences are more effective than just examining presence and immersive stimuli. Further research and development into using VR as a tool for improved well-being is needed to understand its efficacy in remote and in-person setting.
Introduction
A person's psychological (subjective) well-being relates to a person's anxiety and mood levels (1–3). Research on alleviating stress and negative mood is essential since stress can trigger and influence many diseases (4). A more recent study also indicated that negative mood states can increase inflammation in the brain (5), which can lead to cancer and tumor progression (6). In an increasingly stressful environment heightened by the COVID-19 pandemic, which has seen 40% of people reporting at least one adverse mental condition (7), it is essential to find solutions to help people's psychological well-being.
This study seeks to examine a possible promising method of enhancing well-being for the general public by combining online environments (two-dimensional and virtual reality) with music. Both VR (8) and music (9) have been used in the past to improve people's well-being. However, there has been limited research conducted using VR and music together to understand if there are any additional potential health benefits for improving people's well-being.
Music used in therapeutic ways (Music therapy) “is the clinical and evidence-based use of music interventions to accomplish individualized goals within a therapeutic relationship by a credentialed professional who has completed an approved music therapy program” (10). Music used in this study was not guided by a licensed music therapist, but participants followed the receptive music therapy model in which participants are asked to listen and respond to recorded music (11). Additionally, the music selected was based on criteria from other music therapy studies (12–14) that include music based on (1) steady pulse, (2) quiet mood, (3) predictable melodic lines, (4) little dynamic change, (5) supportive bass line, (6) stability in volume and (7) low pitches to ensure the quality was similar to that of a music therapy session. Music is not only able to stimulate the brain area (basal ganglia) that regulates feeling of reward (15), but also can decrease the release of cortisol (a stress hormone) such as when a person is attending a musical performance (16). Furthermore, several pilot and experimental studies focused on positive aspects of music when relieving stress for patients such as those who are terminally ill (17, 18) and indicating that music alone can reduce stress and arousal (9) by lowering blood pressure (19).
Research has indicated that listening to “soothing and calming music” is the type of audio most beneficial for reducing stress compared to listening to nature sounds such as rippling water (20), p. 4. Additional research has concluded that classical music and designer music (music that is designed to have an effect such as Doc Lew Childre's composition of Heart Zones) showed the most promising results for relaxation and mental clarity (21) because those genres are more efficient in stimulating the sympathetic nerve (22). Other research focused on the effectiveness of preferred music of people versus non- preferred music and concluded that while preferred genres and artists by people are significantly more effective at reducing pain (23), preferred music was not significantly more stress-relieving than non-preferred music (24).
In addition to audio's noted impact on mental health, visual media, particularly virtual reality (VR), also exerts influence over users' psychological well-being as a modality. Virtual reality is associated with head-mounted displays (HMDs), which are used in tandem with three-dimensional (3D) or 360-degree video virtual environments (25). While there are differences in defining this technology, the clinical and cognitive viewpoint of virtual reality mainly provides a subjective experience that makes the user believe the experience is real and he/she is there (26).
VR research has indicated that the immersive environments can create strong feelings of “presence for participants” (27, 28). In addition, Lombard and Ditton (29) have studied the various components of presence, which includes (1) realism, (2) transportation, (3) immersion, and (4) media richness. Realism can be characterized to the extent of which the virtual environment emulates the real world (30) and requires high costs for improving quality environments, which can be challenging. Furthermore, researchers examined three different types of transportation that relate to spatial presence such as: (1) when a user is transported to another place, (2) an object or place moves toward a user and (3) two or more users are moved to a certain place (29).
The present study focuses on the first type of transportation (i.e., self-transportation). While some may mistakenly define “presence” and “immersion” being the same thing; immersion is an objective level of sensory engagement provided by VR whereas presence is a subjective sense of a user being “in” a new place (31). While immersion and presence are different in terms of definition, they are closely tied together and if immersion is significantly high, higher levels of presence will also be reported (32). Additionally, another researcher's study indicated that people who are more cooperative and self-transcendent may experience more presence indicating how personality may play a role in how a person interacts in immersive environments (33).
VR is particularly promising in the context of mental health because of the platform's media richness, or the number of sensory inputs provided by the platform (e.g., audio, visual, haptic). The Media Richness Theory indicates that communication outcomes depend on a variety of cues that help the receiver resolve uncertainty (34) and some forms (e.g., modalities) are more effective in conveying information (35). Cable and Yu (36) further explored modalities compared to media richness in their study finding that certain technologies have certain qualities that allow for the possibility of higher levels of media richness such as electronic bulletin boards compared to websites. Furthermore, it is generally regarded that visual input dominates the other senses, but auditory perception is also equally important. As Larsson et al (37) states: the “temporal natural of sound” leads to the view that “something is happening” – even if visuals aren't present (p. 5). Hruby (38) reported the positive impact of sound on a user's level of “being there” in a review of virtual cartography.
VR continues to develop in terms of increased presence due to substantial improvements in technology including: (1) computer graphics, (2) processing power and (3) head mounted displays (25), which results in higher levels of interactivity between the environment and person (39, 40). VR has been increasingly studied in a diverse amount of online environments (41, 42) as a health relief for people, even though it is a relatively new technique in the field (43). A 2017 review of VR in medical health settings indicated that its use has been relatively safe and resulted in patient satisfaction (44). When researchers are exploring VR relaxation and stress reduction, they either focus on using “generic environments” in which participants are passive users or environments that require users to be active by interacting with the VR place to train emotion (45). Further studies have indicated that VR provides beneficial health outcomes such as lowering symptoms of depression, relieving stress, and increasing positive mood states (46–48). A newer study confirmed the positive capabilities of VR in counteracting anxiety while drawing blood, increasing happiness and calmness and reducing negative mood states like tension and fatigue (49).
While there are exciting possibilities with music in VR environments such as live concerts (50) and people indicating high satisfaction in those environments that have music (51, 52), there has been limited research within this area for enhancing well-being. Past research combining VR with music has focused on using nature sounds having a positive effect on people in virtual environments (41), increasing enjoyment from exercising (53), and better learning outcomes (54). Research that used VR and music found success in rehabilitation of memory-related cognitive processes (55) and anxiety with phobias such as heights (56). There is limited research when it relates to examining positive mood, but one study examined how music and VR can help patients during chemotherapy improve their mood states and alleviate anxiety. Furthermore, there has been a lack of research as it relates to enhancing well-being for the general population using VR and music compared to specifically using it for clinical populations (i.e. people with depression, cancer, and PTSD).
Therefore, in light of the presented gap in knowledge concerning music combined with VR online environments, the following research questions are proposed:
RQ1: Are the effects of music stimuli on mood different across VR and 2D modalities?
HP1: Individuals that are in VR environments across audiovisual conditions are likely to experience a different total mood than those who are in 2D audiovisual conditions?
RQ2: What are the independent and combined effects of audio and visual stimuli on total mood across VR and 2D modalities?
HP2: Individuals who experience (1) virtual reality and (2) experience more media richness (i.e., both visuals and audio) are more likely to report better perceived well-being than those who experience (1) 2D and (2) less media richness (i.e., only visuals or audio).
RQ3: What are the independent and combined effects of audio and visual stimuli on on people's perceived presence across VR and 2D modalities?
HP3: Individuals who experience (1) virtual reality and (2) experience more media richness (i.e., both visuals and audio) are more likely to report higher perceived presence than those who experience (1) 2D and (2) less media richness (i.e., only visuals or audio).
Materials and methods
Design
To understand how delivering music through VR may contribute to someone's mental well-being, the current study employed a 2 (modality: VR vs. 2D) x3 (media richness: audio only vs. visual only vs. audiovisual) between-subjects experimental design. The study used a pretest and posttest with participants experiencing either one of the 2D groups (2D audiovisual, 2D visual only, or 2D audio only) or VR groups (VR audiovisual, VR visual only, or VR audio only). While there was no control group in this study, participants were randomly assigned to one of six conditions based on questions assessing their certain criteria, such as their access/use of VR equipment. Informed Consent and University Institutional Review Board approval was obtained before collection.
Participation and recruitment
Participants were recruited via convenience sampling between April 4—April 10 (2021) and were older than 18 years of age. They were recruited online from Amazon Mechanical Turk (online crowdsourcing website) due to restricted effects from recruiting and conducting the study in-person because of the current covid-19 pandemic in 2021. Participants received $2.50 by completing the study. Ultimately, we recruited 90 participants (56 males, 33 females, 1 prefer not to say) internationally. Full participant demographics are available in Table 1.
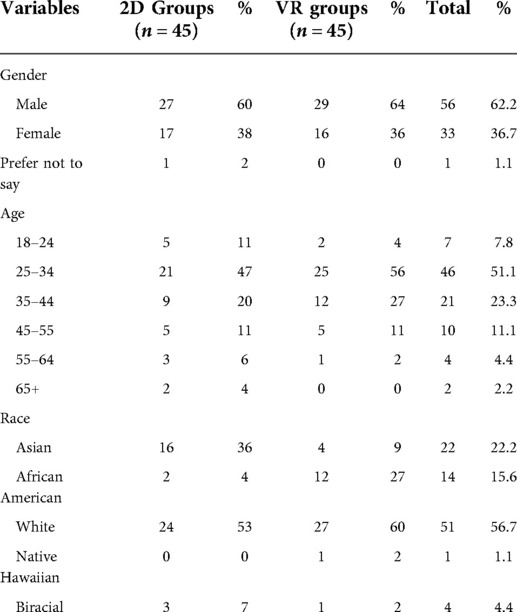
Table 1. Demographics of participants.
We did not formally screen participants for mental or physical health ailments. However, we did screen participants’ susceptibility to simulation-sickness, which is defined as characterized when there is a conflict between visual motion information and the VR scene that causes blurred vision and vertigo (57). Any participant who answered “somewhat likely” to “very likely” to the simulation-sickness question item concerning experiencing simulation-sickness was excluded from the VR groups. Additionally, to attain valid responses, participants were also excluded if they failed the attention check questions.
Online experience footage
Participants in the 2D groups were exposed to calming visualizations via a 2D screen. Participants in the VR groups were exposed to the same visualizations via an HMD, immersing users in a 360-degree environment that created spatial sound around them. Across these conditions, participants were also randomly assigned to one of three versions of the stimuli: audiovisual, audio only, and visual only. Participants in the audiovisual condition were exposed to both visual and auditory stimuli. Participants in the audio only were exposed to only the auditory sounds (music). Participants in the visual only were exposed to the visualization without audio accompaniment.
The six groups consisted of a choice of music based on empirical studies and theories of music that are associated with slow tempo and low pitches as being beneficial for reducing anxiety (12). The footage for this interaction was originally taken from a YouTube video named “Nocturnes by Candlelight - Deep Sleep and Relaxation”, which included the instrumental song, Piano at Midnight, composed by Andrew Holdworth (58). The full video on YouTube was imported into Adobe Premiere Pro to create a video lasting 3 min and 13 s long while also creating the three environments (audiovisual vs. visual only vs. audio only) that varied in sensory richness. Additionally, this video was selected due to the specific color shades and movement to fit with beats of the song in order to achieve the emotional purpose of the song (relaxation). The 2D experience consisted of only these elements. Conversely, The VR experience was created from using the above approach while additionally using Adobe Premiere Pro to create visuals to be on every side as the participant moves their head around in a 360-degree video. Both Figures 1 and 2 show visuals that participants would experience in both 2D and VR conditions but those in the VR (visual only and audiovisual) would be able to see visuals in all directions. Furthermore, as the participant moves their head around in the YouTube 360–degree environment, they experience spatial audio, but the researchers won't collect information regarding participants head movements due to not being able to have access to their VR devices.

Figure 1. Frame from the 2D experience.
Figure 2. Frame from the 360-degree VR experience.
Device used to access survey
The one-item question collected the participants' device that was used to access the study on Amazon Mechanical Turk to assess their eligibility for continuing the study. Participants who did not select “laptop” or “desktop” were dropped from the study due to the study needing a bigger screen to fully view the experience in 2D and understand the questions asked of them.
VR inclusion/exclusion assessment questionnaire
Due to this study being conducted online via Amazon Mechanical Turk, participants had to own their own VR devices to be included in the VR treatment. To assess if participants were eligible to be in one of the three VR conditions (audiovisual, visual only, or audio only), participants answered up to three questions regarding owning their own VR headset. If participants met all three conditions, they were randomly placed into one of the three VR conditions. Participants were asked if they currently own a VR headset and if they indicated “Yes,” they continued to the next VR question. The next one-item question was collected as a means of identifying any group of potential VR simulation sickness symptoms (e.g., nausea and dizziness) that could cause a negative reaction for the participant. The item was assessed on a 4-point Likert scale and any participant who selected “somewhat likely” or “very likely” to experience simulation-sickness was randomly assigned to one of the 2D groups. Conversely, any participant who selected “somewhat unlikely” or “very unlikely” was randomly assigned to one of the VR groups (audiovisual, visual only, or audio only). Additionally, the last question related to what VR device they owned and if they selected “Other,” they were randomly assigned to one of the 2D conditions instead of continuing to the VR experience due to the YouTube VR App only being compatible with certain VR devices.
Mood
To evaluate participant's perceived mood and psychological distress, all participants completed the Abbreviated Profile of Mood States Questionnaire (POMS) before and after the online 2D or VR experience. The POMS (59) consists of seven mood dimensions but one dimension, confusion, was dropped from the study due to past studies indicating that it was less reliable (60). In addition, this questionnaire was shortened due to concerns with the reliability of data collected through Amazon Mechanical Turk (61) to reduce measurement bias (62), p. 129. The abbreviated POMS consists of a 5-point Likert scale with 35-items that evaluates the current emotional mood state of participants in terms of their level of tension, anger, fatigue, depression, esteem-related affect, and vigor. The total mood distance (TMD) is calculated by [tension + depression + anger + fatigue] - [vigor + esteem-related affect]. Overall, higher scores for TMD and negative mood states indicate higher negative mood while higher scores for positive subscales indicate better mood outcomes for participants. Reliability coefficients (Cronbach's alpha) scores for pre-test and post-test POMS subscales ranged from tension as (α = 0.90) and (α = 0.92), anger as (α = 0.93) and (α = 0.93), fatigue as (α = 0.91) and (α = 0.92), depression as (α = 0.93) and (α = 0.95), vigor as (α = 0.79) and (α = 0.82), and esteem-effect as (α = 0.65) and (α = 0.75).
Spatial presence
To evaluate participants' perceived sense of being in the virtual space (spatial presence), participants completed the Spatial Presence Experience Scale (SPEC) after completing the experience and post-test POMS. The SPEC (63) consists of 8-items on a 5-point Likert scale. The Spatial Presence Experience Scale was calculated by taking the average of the 8-items. Higher scores for the participants indicate higher perceived presence. The reliability coefficient (Cronbach alpha) for the scale was very reliable (α = .93).
Procedure
The experiment lasted approximately between 15 and 25 min, with all participants completing the study individually without the researchers interfering with the process other than to provide written instructions that were on Qualtrics. Participants could take as long as they needed to read through the instructions but there were time minimums for each page and attention check questions to make sure they understood the instructions as to ensure quality of what was being measured. Participants provided online written informed consent upon entering the study from Amazon Mechanical Turk. After agreeing to the informed consent form, participants completed the demographic and inclusion/exclusion questions, the latter dictating the random assignment of participants to the 2D or VR conditions.
Participants in the VR conditions completed additional questions to determine how much experience they had in immersive virtual environments. After completing the initial stage questions, participants completed the abbreviated POMS scale (pre-test) and then were evenly randomly assigned to one of the following: (1) 2D groups (audiovisual, visual only, or audio only) or (2) VR groups (audiovisual, visual only, or audio only). Participants in the 2D conditions completed the experience after reading instructions on how to launch the content on their browsers. Participants in the VR conditions were also given detailed instructions on how to successfully access the content through the YouTube VR App on their personal virtual reality devices, after which they watched and/or listened to the experience in their headsets. Additional instructions ensured participants across all groups removed/minimized any toolbars and accessed the content in “full-screen mode”.
After the experience was completed, participants completed the online experience attention check question. Participants who passed the attention check were then directed to the remaining survey items, consisting of the abbreviated POMS scale (post-test) and the short-form SPEC. After participants completed the post-test questions, all participants filled out three additional questions concerning their experience. Participants were also afforded the opportunity to comment on the experience and pose any questions/concerns.
Results
Data analysis
All of the analyses for the three research questions were performed using SPSS 27 application (IBM Corporation, Somers, New York, USA). Additionally, all participants who completed the pre-test and post-test were included in the analysis study. Participants were asked how clearly they were able to see and/or the experience and 87 participants said that the experience was either “extremely clear” or “somewhat clear” indicating that the data could be used for the study though 5/15 participants in the VR visual only group indicated that some visuals seemed to be “strobing”.
Individual participant scores for the pre-test and post-test were averaged and differences in means were compared to create the mood change variables used for the analysis. To assess differences in mood across the experimental groups, a one-way ANOVA was conducted. The results demonstrated that there were no significant differences across Time1(pre-test) Mood Disturbance, [F(5, 84)=1.66, p = .15].
To address RQ1, a two-way repeated-measures analysis (ANOVA) was applied to compare the pre-test and post-test group mean scores (mood change) between the six (3 VR vs. 3 2D) groups from the psychological test questionnaires (POMS).
To address RQ2, a series of pairwise comparisons using Fisher's LSD test were conducted from the same data used from the two-way repeated analysis (ANOVAs) to examine differences in mood disturbance over time across the experimental conditions. Furthermore, analysis using post-hoc pairwise comparisons using Fisher's LSD test for all groups were conducted to further understand what experimental condition was needed for effective improved well-being and if any conditions were more effective than others when reducing total mood disturbance.
Additional analyses using post-hoc pairwise comparisons using LSD test were conducted to understand which (if any) intervention(s) were more effective when reducing negative mood subscales (i.e., anger, tension, depression, and fatigue) and increasing positive mood subscales (i.e., vigor and esteem-related effect) compared to other groups. Higher means scores for mood change indicated a worse mood change while lower scores in the post-test indicated that the intervention was effective.
To address RQ3, a two-way analysis of variance (ANOVA) was used to assess if there were any significant differences across online interventions and a person's perceived presence. Further analyses using post hoc pairwise comparisons using Fisher's LSD tests were also conducted to further illustrate which groups experienced the most presence.
Differences in VR and 2D environments
Changes in mood from pre- to post-test were examined across the six conditions. Overall, the results of the two-way repeated measures (ANOVA) showed a significant difference in interaction effect between online experiences and total mood disturbance (p = 0.026). Additionally, the results indicated a main effect in mood change over time across online environments (p < .001). Results are reported in Table 2.
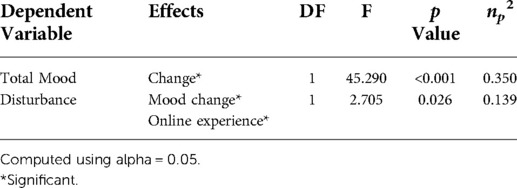
Table 2. Univariate Effects for the two-way ANOVA analysis.
Media richness and modality differences across environments
The study then investigated whether (modality: VR vs. 2D) and/or (media richness: audio only vs. visual only vs. audiovisual) influenced the magnitude of mood change among online interventions across time (mood change) to understand which online interventions were effective. A series of pairwise comparisons were conducted and the results indicated a main effect of modality on mood disturbance such that participants in every 2D condition experienced a significant decrease in mood disturbance, whereas there were no significant changes in the VR conditions as is illustrated in Table 3.
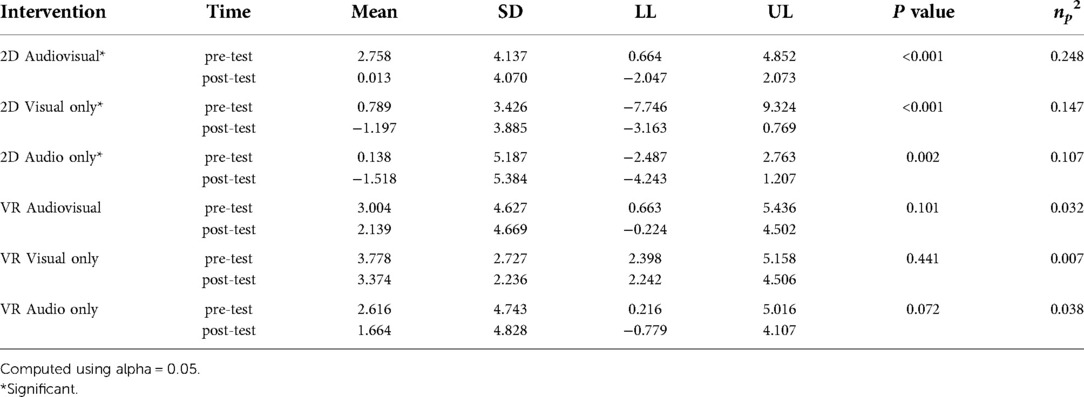
Table 3. Descriptive statistics for total mood disturbance levels by POMS.
Moreover, pairwise comparisons indicated that there was significantly less mood disturbance for participants in the 2D visuals only group than those in the VR visuals only group (p = 0.014). Lastly, the 2D audio only participants experienced significantly less mood disturbance than participants in the VR audiovisuals group (p = 0.034) and the VR visual only group (p = 0.006). There were no other significant differences between any of the other groups. Figure 3 reports the mood disturbance estimated means for each of the online experiences between pre-test and post-test.
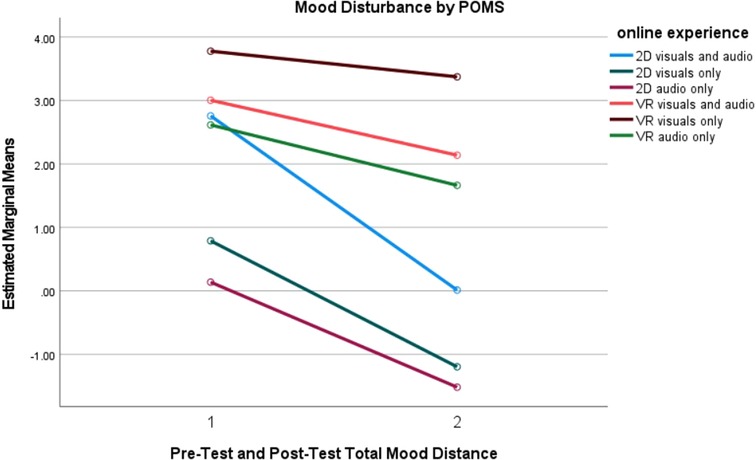
Figure 3. Mood disturbance measured by POMS for online experiences.
Mood subscale results
Additionally, a series of repeated measures analysis (ANOVAs) with the levels of the six mood states, as measured by POMS (i.e., tension, depression, anger, fatigue, vigor and esteem-related affect) and online experience were conducted using the ANOVA test. Results of the univariate effects from the analysis of covariance (ANOVAs) are reported in Table 4.
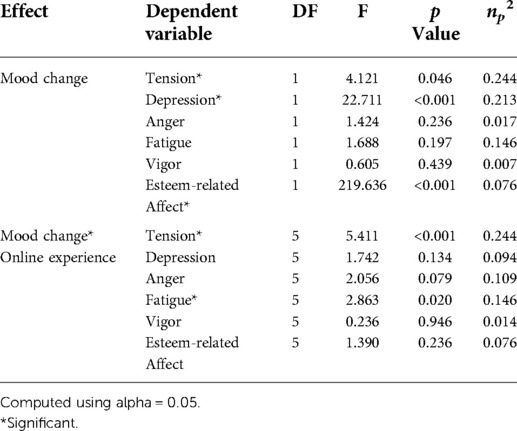
Table 4. Univariate effects for analysis of covariance (ANCOVA).
The results from the two-way repeated measures analysis (ANOVAs) of the subscales indicated that an interaction between the time (mood change) and across online experiences was only significantly different for both tension and fatigue subscales (p < .05). Conversely, there was a significant main effect of online experiences for participant's mood change for tension (p = 0.046), depression (p < .001), and esteem-related affect (p < .001).
Furthermore, a series pairwise comparisons were conducted for tension, depression and esteem-related affect subgroups to understand what online experiences were more effective than others. The mean differences between online experiences are reported in Figures 4–6. Full results for both positive and negative subscales are reported in Table 5.
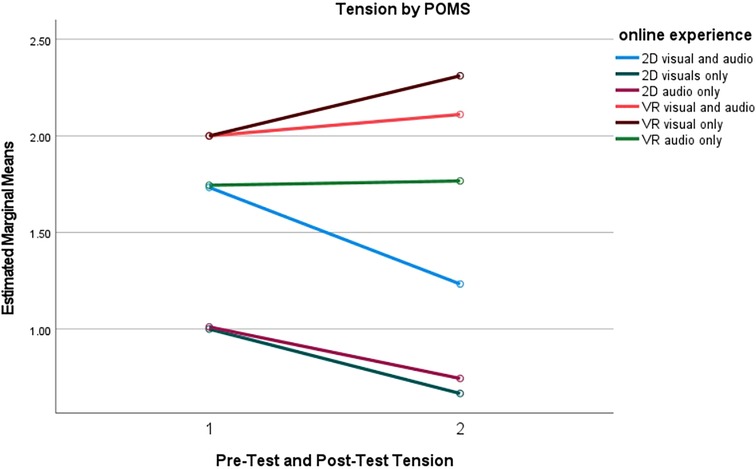
Figure 4. Tension measured by POMS for online experience.
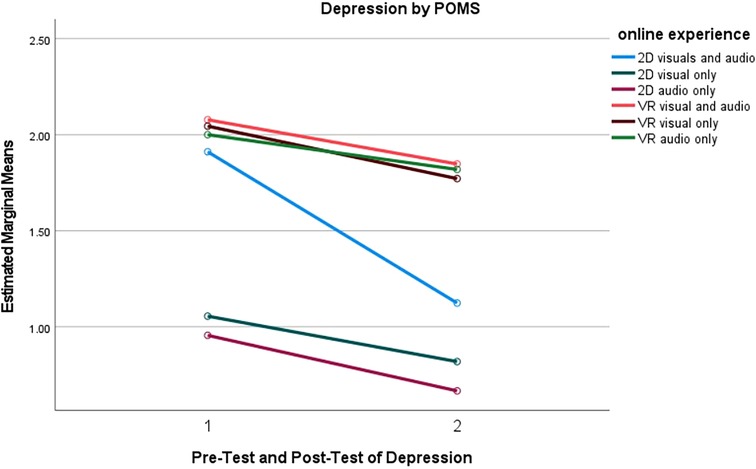
Figure 5. Depression measured by POMS for online experience.
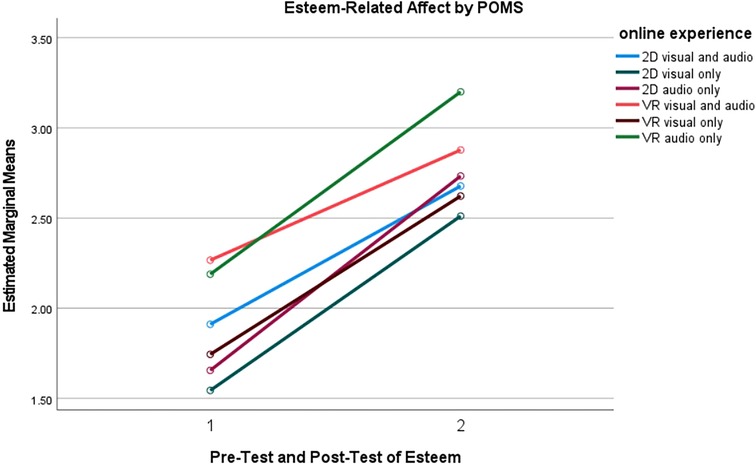
Figure 6. Self-esteem affect measured by POMS for online experience.
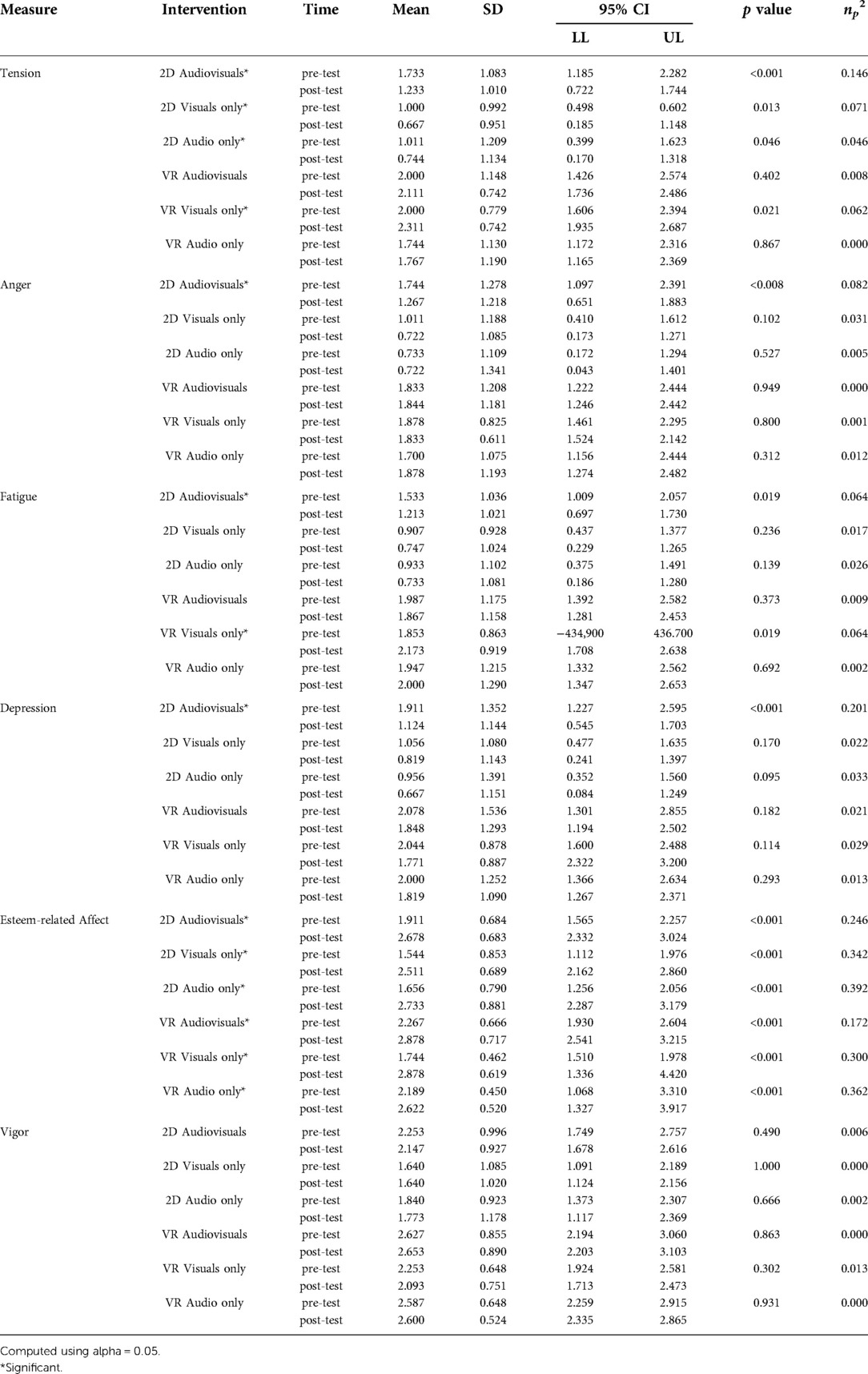
Table 5. Descriptive statistics for the Profile of Mood States negative subscales, for each group by the TIME factor, and significance differences from pairwise comparisons.
Tension
Pairwise comparisons indicated significant decreases in tension levels between pretest and the posttest for every 2D group. Conversely, while caution should be used when indicating any clear significance due to a small effect size, tension significantly increased for the participants in the VR visual only group. Full results can be found in Table 5. Moreover, pairwise comparisons indicated that participants in the 2D visuals only group experienced less tension than participants in the VR audiovisual (p = 0.012) and VR visuals only (p = 0.012) groups. Figure 4 reports the tension estimated means for each of the online experiences between pre-test and post-test.
Depression
The results from the POMS scores for depression indicated that the sample (N = 90) used was not above the cutoff of >7 for clinical depression. Individuals were asymptomatic so caution should be used when indicating any significance for clinically depressed populations. Pairwise comparisons indicated significant reductions in the depression levels between the pretest and the posttest for only the participants in the 2D audiovisuals group as illustrated in Table 5. Moreover, pairwise comparisons indicated that participants in the 2D visuals only group had significantly less depression levels than those in the participants in the VR audiovisual (p = 0.016), VR visual only (p = 0.022), and VR audio only (p = 0.022) groups. Additionally, participants in the 2D audio only online experienced significantly less depression level than those in the VR audiovisuals (p = 0.007), VR visuals only (p = 0.010), and VR audio only (p = 0.010). There were no other significant interventions or differences among the groups for depression. Figure 5 reports the depression estimated means for each of the online experiences between pre-test and post-test.
Esteem-related affect
Pairwise comparisons showed significant increases in esteem-related affect levels between the pretest and the posttest for every VR and 2D group in Table 5. Pairwise comparisons indicated that participants in the VR audio only group experienced more esteem-related affect than participants in the 2D visuals only (p = 0.002), 2D audio only (p = 0.013), and VR visuals only (p = 0.037) groups. Additionally, participants in the VR visuals only group experienced more esteem-related affect than participants in the 2D visuals only (p = 0.008) and 2D audio only (p = 0.043) groups. There were no significant differences between any of the conditions for esteem-related affect. Figure 6 reports the esteem-related affect estimated means for each of the online experiences between pre-test and post-test.
Online interventions and perceived presence
In order to assess if any of the online intervention groups had a significant impact on someone's perceived presence, a two-way analyses of variance (ANOVA) was conducted and the results indicated that there were significant differences across the various online intervention groups and someone's perceived presence [F(5, 84)=7.482, p < 0.001, np2 = 0.308)]. Moreover, pairwise comparison showed participants in the VR audiovisuals and VR audio only groups experienced more perceived presence than participants in the 2D visual only and 2D audio only groups (p < 0.001). Participants in the VR visual only group experienced more perceived presence than participants in the 2D visual only and 2D audio only group (p = 0.002). Additionally, participants in the 2D audiovisuals group experienced more perceived presence than participants in the 2D visuals only group (p = 0.005) and the 2D audio only (p = 0.004). See Figure 7 for estimated mean differences for perceived presence by online experience.
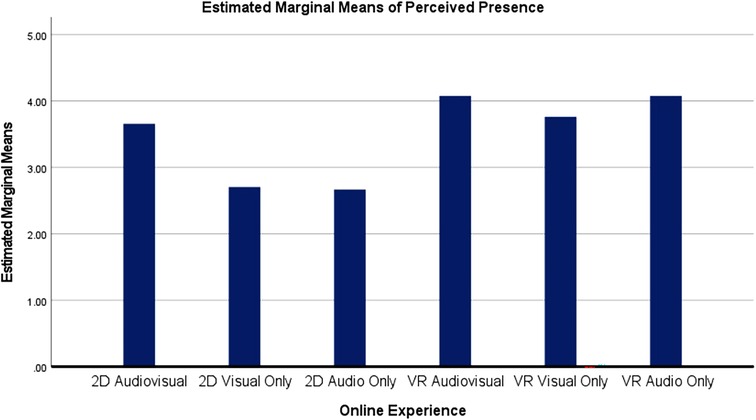
Figure 7. Graph of estimated mean differences for perceived presence by online experience.
Discussion
In this study, participants were randomly placed in various online environments to understand if there were any differences between the experimental conditions and mood. Overall, the results from the various statistical analyses indicated that broadly speaking, there were significant differences across the 2D and VR groups, which indicated that modality and media richness may play a role in people's music experience (RQ1).
Furthermore, additional analysis also showed that 2D environments were the only conditions to significantly reduce total mood disturbance (TMD). Examining the results more closely showed significant benefits for the participants who were in the 2D audiovisual group as that condition led to every negative mood subscale significantly decreasing over time. 2D audio only and 2D visuals only conditions both were beneficial in reducing tension. Conversely, no VR group significantly reduced any negative mood states. In fact, the VR visual only group was the worst online treatment since participants had adverse effects in which their tension and fatigue levels increased. However, as reported in Table 5, the effect size was very small so one should use caution when concluding that VR has negative consequences on people's well-being in general.
Despite these counterintuitive findings for reducing negative mood, participants in every 2D and VR groups significantly increased in esteem-related affect (positive mood). Furthermore, as reported in Table 5 the effect sizes for these results were the largest of the results from this study and VR groups had significantly better esteem-related affect than the 2D audio and visual groups. These findings indicate that modality and media richness do play a significant role into what online environment is effective but runs counter to the prior assumption that these conditions would make VR environments more effective for both positive and negative mood (RQ2).
While the results from RQ2 might predict that the 2D groups would experience the greatest amount of presence, the results indicated that VR groups experienced more presence than every 2D group other than 2D audiovisual. These results generally align with past research indicating that people in VR would experience the most presence, but these results also suggest that if participants are in a sensory rich environment (2D audiovisual), it may not be as essential for people to only experience online environments meant to enhancing well-being in VR (RQ3).
Theoretical and applied implications
The results from the analyses support past literature showing promising results for music (21). However, these findings partly contradict past research presented in the literature indicating that VR would be a very effective tool for improved well-being (46, 48) and deserves discussion. Additionally, the findings appear to mostly suggest that presence may not play as significant a role in determining what experience is most effective treatment since 2D groups were overall significantly more effective.
Furthermore, discussion around presence should not solely focus on immersion of various visual and audio stimuli but also explore how users can interact more within their online environment. Additionally, using VR has mostly been studied in specific research populations, such as chemo patients, burn wound victims, and people with depression (47, 64, 65), indicating that there should be serious inquiry into how VR can be applied to the general public and be effective.
These results also suggest that there are psychological challenges when implementing VR online that are not prevalent for 2D experimental conditions. Instructions for participants for VR conditions were much more strenuous than the 2D participants due to the onboarding process of downloading the YouTube app and selecting the right settings for the experience. While the instructions were not intentionally designed to be confusing, it was still a more tedious process, which could have presented a cognitive overload (i.e. when a person's memory is overloaded due to limited working and short-term capacity) for the participant (66). While taking this theory under consideration, it makes sense that VR groups would increase in fatigue, which would then impact how people experience the environment and would degrade performance, attention, and other mood states (67). This also relates to appraisal of emotion theory in which participants may have based their emotions off their experience with the set-up resulting in a negative appraisal of response (68) causing unintended consequences.
Participants were also allowed to leave comment(s) at the end of the survey with additional feedback and 5/15 participants in the VR visual only group specifically indicated they found the visuals to have a “strobing” effect. Based on the results and some of the participants' comments, participants could have become photosensitive to the stronger visuals within VR compared to the 2D conditions. A former study also found that people diagnosed with Parkinson's disease started developing visual hallucinations that were not included in the VR environment (69) which further brings up the question if VR is only for a subset of people that are not photosensitive or have cognitive impairments. Furthermore, there appears to be very few additional studies that specifically address unwanted negative effects of the use of VR as a therapeutic tool that are not related to cybersickness (70) or exacerbation of negative side effects with treating PTSD (71). While Albani et al (69) and our current study have some limitations, these studies can be used to alert the scientific community about the possibility of unwanted negative effects that can be resulted when using VR immersive reality for some participants.
The study's results also imply that because research within for VR is still in its infancy, there are no set procedures and/or stimuli that are primarily effective when reducing negative mood as our study concludes. Additionally, the use of VR in the medical field is relatively novel and the experiences might need to be tailored to the individual. For example, children may respond better to more game based online experiences whereas adults show preference toward natural and relaxing environments (72). Additionally, VR stimuli has also ranged in time ranging from 5 min to 60 min (73) to reduce anxiety and/or depression. These varied results further demonstrate the need to validate the most effective time of the VR experiences along with other variables in order to produce the most effective experience.
Limitations
There are several possible limitations in this study that should be considered when examining the results. This study is unblinded and lacks a concurrently randomized control group and the participants were not completely randomly assigned to one of the six experimental conditions as those who owned a VR device were automatically placed into a VR condition and, therefore, is at risk of bias even though participants were evenly randomly assigned to one the six groups. Additionally, we were not able to control the environment atmosphere, the current condition of the VR headset, or know if there were any internet connectivity issues. While these may have been possible problems, almost all participants (97%) of participants said the experience was either “extremely clear” or “somewhat clear.” Moreover, only self-reported measurements were analyzed and thus, future studies should explore physiological variables (such as heart rate) to provide a more comprehensive evaluation of distress (74) and provide potential measurement bias online.
Due to ethical concerns of potentially transmitting Covid-19, the researchers were constrained in our ability to have participants be very active in the environment other than moving their heads around to various visuals in their experience as there were already many instructions that the participants had to follow on their own without direct help from the researchers themselves. While this approach contradicts some past research that indicated that people who can be more engaged and interact with their environment get better health results (75, 76), health standards and feasibility of increasing interaction would potentially cause other problems. Further research that can be conducted in-person would allow for there to be more interaction and engagement with what participants could do with the visuals and audio.
Another limitation is that this trial analyzed only short-term effects. Measurements were taken only at two time points (pre-intervention and post-intervention) and each patient participated in only one session. While length of traditional therapy administered by clinicians varies upon the individual, several studies indicate that in-person sessions happen over longer time and multiple sessions (77, 78) for positive psychotherapy outcomes. However, longer periods of VR intervention could lose efficacy over several sessions since individuals might habituate to it and become ineffective (i.e., VR might become less effective for increasing the positive self-esteem for people). This does remain to be assessed since a past study concluded that the benefits of VR intervention were not lost across at least three sessions, thus indicating that novelty may not play a significant role in VR enhancing well-being (79).
Furthermore, given that our sample were people that we cannot confirm nor diagnose with major depression, the generalizability of our results are limited to non-depressive adults. In other words, while our results highlight the potential positive outcomes for mood concerning depression, the results cannot firmly indicate if we'd find the same result with a population diagnosed with depression. Lastly, it should be noted that a post-hoc power analysis found the study to be statistically underpowered. Given the number of conditions and analyses, interpretations of modality effects, while in line with previous research, should be interpreted with caution. Furthermore, with the study being underpowered, there may have been some effects that were undetected.
Future research
This study aimed to provide a modest contribution to an emerging field of study – immersive media with music for enhanced well-being. In doing so, we hope to have yielded novel insights into the effectiveness of music when delivered through VR. To our knowledge, this was a novel study in that it specifically examined the differences between 2D and VR online experiences with music to determine effectiveness of enhancing well-being. Taking into account the theoretical implications and limitations, future research should explore online environments by finding solutions to (1) shorten instructions for the setup, (2) include videos to guide the participants more clearly pictures and/or (3) have participants join online with the researcher on a video conferencing platform (e.g., Zoom or Skype) to help them with the setup of the experience and more fully control elements that were not available in this study. Additionally, researchers could explore with focus groups visual stimuli beforehand to reduce potential photosensitive images that could possibly make the environments not as effective. Furthermore, these results may indicate that 2D online environment sessions could be just as beneficial as VR but further research needs to be conducted bearing in mind the limitations and psychological considerations discussed earlier. Future research should not only explore repeated exposures for online environments but also specifically compare 2D, VR, and in-person groups to understand what is the most effective.
Conclusion
The results of our study suggest that while both VR and 2D environments can be useful tools for improving mood for people, 2D environments were assessed as the most beneficial treatments for impacting people's psychological-well-being over a short amount of time. Sensory richness played a significant role in making 2D audiovisual the most beneficial experience for this study, but this result may be the result of psychological limitations to the VR groups. In summary, this study proposes that e-health developers and researchers should not only focus on using audiovisuals in their research but also focusing on making the onboarding process easier and exploring what visual stimuli would be most effective for enhancing well-being to meet the global clinical need for non-pharmaceutical methods. This study should provide a template for future researchers and clinicians who want to use VR and other online environments for therapeutic results and/or enhancing well-being for people.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Research Ethics and Compliance University of Oregon. The patients/participants provided their written informed consent to participate in this study.
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SA contributed study conception, design, data collection, statistical analysis, and served as the primary writer of the manuscript. DP assisted in statistical analysis, results reporting, and assisted in manuscript writing. MF assisted in both creation of the design of study and assisted in manuscript writing. All authors contributed to the article and approved the submitted version.
Funding
Both SA and MF contributed to the funding for recruitment of participants for this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Moum T. Yea-saying and mood-of-the-day effects in self-reported quality of life. Soc Indic Res. (1988) 20(2):117–39. doi: 10.1007/BF00302458
2. Schwarz N, Clore GL. Mood, misattribution, and judgments of well-being: Informative and directive functions of affective states. J Pers Soc Psychol. (1983) 45(3):513–23. doi: 10.1037/0022-3514.45.3.513
3. Yardley JK, Rice RW. The relationship between mood and subjective well-being. Soc Indic Res. (1991) 24(1):101–11. doi: 10.1007/BF00292653
4. Cohen S, Janicki-Deverts D, Doyle WJ, Miller GE, Frank E, Rabin BS, et al. Chronic stress, glucocorticoid receptor resistance, inflammation, and disease risk. Proc Natl Acad Sci U S A. (2012) 109(16):5995–9. doi: 10.1073/pnas.1118355109
5. Graham-Engeland JE, Sin NL, Smyth JM, Jones DR, Knight EL, Sliwinski MJ, et al. Negative and positive affect as predictors of inflammation: Timing matters. Brain Behav Immun. (2018) 74:222–30. doi: 10.1016/j.bbi.2018.09.011
6. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. (2008) 454(7203):436–44. doi: 10.1038/nature07205
7. Czeisler MÉ, Lane RI, Petrosky E, Wiley JF, Christensen A, Njai R, et al. Mental Health, substance use, and suicidal ideation during the COVID-19 pandemic — United States. MMWR Morb Mortal Wkly Rep. (2020) 69(32):1049–57. doi: 10.15585/mmwr.mm6932a1
8. Maples-Keller JL, Bunnell BE, Kim SJ, Rothbaum BO. The use of virtual reality technology in the treatment of anxiety and other psychiatric disorders. Harv Rev Psychiatry. (2017) 25(3):103–13. doi: 10.1097/HRP.0000000000000138
9. Pelletier CL. The effect of music on decreasing arousal due to stress: A meta-analysis. J Music Ther. (2004) 41(3):192–214. doi: 10.1093/jmt/41.3.192
10. About Music Therapy & AMTA. American Music Therapy Association. Retrieved November 15, 2020 from: https://guides.himmelfarb.gwu.edu/APA/web-page-no-author (n.d.).
11. Stanczyk M. Music therapy in supportive cancer care. Rep Pract Oncol Radiother. (2011) 16(5):170–2. doi: 10.1016/j.rpor.2011.04.005
12. de la Torre-Luque A, Caparros-Gonzalez RA, Bastard T, Vico FJ, Buela-Casal G. Acute stress recovery through listening to Melomics relaxing music: A randomized controlled trial. Nord J Music Ther. (2017) 26(2):124–41. doi: 10.1080/08098131.2015.1131186
13. Bonny HL. Music and consciousness: The evolution of guided imagery and music. Barcelona: Barcelona Publishers (2002).
14. Byrns A, Abdessalem HB, Cuesta M, Bruneau M-A, Belleville S, Frasson C. EEG Analysis of the contribution of music therapy and virtual reality to the improvement of cognition in Alzheimer's Disease. J Biomed Sci Eng. (2020) 13(8):187–201. doi: 10.4236/jbise.2020.138018
15. Brodal HP, Osnes B, Specht K. Listening to rhythmic music reduces connectivity within the basal ganglia and the reward system. Front Neurosci. (2017) 11:153. doi: 10.3389/fnins.2017.00153.28400717
16. Fancourt D, Williamon A. Attending a concert reduces glucocorticoids, progesterone and the cortisol/DHEA ratio. Public Health. (2016) 132:101–4. doi: 10.1016/j.puhe.2015.12.005
17. Lueders-Bolwerk CA. Effects of relaxing music on state anxiety in myocardial infarction patients. Crit Care Nurs Q. (1990) 13(2):63–72. doi: 10.1097/00002727-199009000-00009
18. Curtis SL. The effect of music on pain relief and relaxation of the terminally ill. J Music Ther. (1986) 23(1):10–24. doi: 10.1093/jmt/23.1.10
19. Bradt J, Dileo C, Magill L, Teague A. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Libr. (2016) 8:CD006911. doi: 10.1002/14651858.CD006911.pub3
20. Thoma MV, La Marca R, Brönnimann R, Finkel L, Ehlert U, Nater UM. The effect of music on the human stress response. PLoS ONE. (2013) 8:8. doi: 10.1371/journal.pone.0070156
21. McCraty R, Barrios-Choplin B, Atkinson M, Tomasino D. The effects of different types of music on mood, tension, and mental clarity. Altern Ther Health Med. (1998) 4(1):75–84. https://pubmed.ncbi.nlm.nih.gov/9439023/9439023
22. Umemura M, Honda K. Influence of music on heart rate variability and comfort–a consideration through comparison of music and noise. J Hum Ergol (Tokyo). (1998) 27(1–2):30–8. doi: 10.11183/jhe1972.27.30
23. Mitchell LA, MacDonald RAR. An experimental investigation of the effects of preferred and relaxing music listening on pain perception. J Music Ther. (2006) 43(4):295–316. doi: 10.1093/jmt/43.4.295
24. Walworth DDL. The effect of preferred music genre selection versus preferred song selection on experimentally induced anxiety levels. J Music Ther. (2003) 40(1):2–14. doi: 10.1093/jmt/40.1.2
25. Gregg L, Tarrier N. Virtual reality in mental health. A review of the literature. Soc Psychiatry Psychiatr Epidemiol. (2007) 42(5):343–54. doi: 10.1007/s00127-007-0173-4
26. Riva G, Baños RM, Botella C, Mantovani F, Gaggioli A. Transforming experience: The potential of augmented reality and virtual reality for enhancing personal and clinical change. Front Psychiatry. (2016) 7:164–164. doi: 10.3389/fpsyt.2016.00164
27. Riva G, Waterworth JA, Waterworth EL, Mantovani F. From intention to action: The role of presence. New Ideas Psychol. (2011) 29(1):24–37. doi: 10.1016/j.newideapsych.2009.11.002
28. Riva G, Waterworth JA. Being present in a virtual world. New York: Oxford University Press (2014). https://doi.org/10.1093/oxfordhb/9780199826162.013.015.
29. Lombard M, Ditton T. At the heart of it all: The concept of presence. J Comput Mediat Commun. (1997) 3(2). doi: 10.1111/j.1083-6101.1997.tb00072.x
30. Alexander AL, Brunyé TT, Sidman J, Weil SA. From gaming to training: A review of studies on fidelity, immersion, presence, and buy-in and their effects on transfer in PC-based simulations and games. DARWARS Train Impact Group. (2005) 5:1–14.
32. Bowman DA, McMahan R. Virtual reality: How much immersion is enough? Computer (Long Beach Calif). (2007) 40(7):36–43. doi: 10.1109/MC.2007.257
33. Song H, Park S, Kim H, Jo S, Lee J-I, Han S-J, et al. Is anxiety-inducing VR experienced differently depending on personality? The mediating role of presence. IEEE Access. (2021) 9:42161–8. doi: 10.1109/ACCESS.2021.3064251
34. Otondo RF, Van Scotter JR, Allen DG, Palvia P. The complexity of richness: Media, message, and communication outcomes. Inf Manage. (2008) 45(1):21–30. doi: 10.1016/j.im.2007.09.003
35. Allen DG, Scotter JRV, Otondo RF. Recruitment communication media: Impact on rehire outcomes. Pers Psychol. (2004) 57(1):143–71. doi: 10.1111/j.1744-6570.2004.tb02487
36. Cable DM, Yu KYT. Managing job seekers’ organizational image beliefs. J Appl Psychol. (2006) 91(4):828–40. doi: 10.1037/0021-9010.91.4.828
37. Larsson P, Väljamäe A, Västfjäll D, Tajadura-Jiménez A, Kleiner M. Auditory-induced presence in mixed reality environments and related technology. Hum. Comput. Interact. (2010) 1:143–63. doi: 10.1007/978-1-84882-733-28
38. Hruby F. The sound of being there: Audiovisual cartography with immersive virtual environments. J Cartogr Geogr Info. (2019) 69(1):19–28. doi: 10.1007/s42489-019-00003-5
39. Ryan M-L. Immersion vs. interactivity: Virtual reality and literary theory. SubStance. (1999) 28(89):110–37. doi: 10.1353/sub.1999.0015
40. Bailenson J, Patel K, Nielsen A, Bajscy R, Jung SH, Kurillo G. The effect of interactivity on learning physical actions in virtual reality. Media Psychol. (2008) 11(3):354–76. doi: 10.1080/15213260802285214
41. Annerstedt M, Jönsson P, Wallergård M, Johansson G, Karlson B, Grahn P, et al. Inducing physiological stress recovery with sounds of nature in a virtual reality forest - Results from a pilot study. Physiol Behav. (2013) 118:240–50. doi: 10.1016/j.physbeh.2013.05.023
42. Anderson AP, Mayer MD, Fellows AM, Cowan DR, Hegel MT, Buckey JC. Relaxation with immersive natural scenes presented using virtual reality. Aerosp Med Hum Perform. (2017) 88(6):520–6. doi: 10.3357/AMHP.4747.2017
43. Rizzo A, Kim GJ. A SWOT analysis of the field of virtual reality rehabilitation and therapy. Presence. (2005) 14(2):119–46. doi: 10.1162/1054746053967094
44. Dascal J, Reid M, Ishak WW, Spiegel B, Recacho J, Rosen B, et al. Virtual reality and medical inpatients: A systematic review of randomized, controlled trials. Innov Clin Neurosci. (2017) 14(1-2):14–21.28386517
45. Pizzoli SFM, Mazzocco K, Triberti S, Monzani D, Alcañiz Raya ML, Pravettoni G. User-centered virtual reality for promoting relaxation: An innovative approach. Front Psychol. (2019) 10:479. doi: 10.3389/fpsyg.2019.00479
46. Baños RM, Botella C, Alcañiz M, Liaño V, Guerrero B, Rey B. Immersion and emotion: Their impact on the sense of presence. Cyberpsychology and Behavior. (2004) 7(6):734–41. doi: 10.1089/cpb.2004.7.734
47. Lindner P, Hamilton W, Miloff A, Carlbring P. How to treat depression with low-intensity virtual reality interventions: perspectives on translating cognitive behavioral techniques into the virtual reality modality and how to make anti-depressive use of virtual reality–unique experiences. Front Psychiatry. (2019) 10:1–6. doi: 10.3389/fpsyt.2019.00792
48. Riva G, Mantovani F, Capideville CS, Preziosa A, Morganti F, Villani D, et al. Affective interactions using virtual reality: The link between presence and emotions. Cyberpsychol Behav. (2007) 10(1):45–56. doi: 10.1089/cpb.2006.9993
49. Tarrant J. The impact of virtual reality on mood states prior to blood donation. Sch J Psychol Behav Sci. (2019) 2:5. doi: 10.32474/sjpbs.2019.02.000150
50. Charron J-P. Music audiences 3.0: Concert-Goers’ psychological motivations at the dawn of virtual reality. Front Psychol. (2017) 8:800. doi: 10.3389/fpsyg.2017.00800
51. Brungardt A, Wibben A, Tompkins AF, Shanbhag P, Coats H, LaGasse AB, et al. Virtual reality-based music therapy in palliative care: A pilot implementation trial. J Palliat Med. (2021) 24(5):736–42. doi: 10.1089/jpm.2020.0403
52. Deacon T, Stockman T, Barthet M. User experience in an interactive music virtual reality system: An exploratory study. Bridging People Sound. (2017) 10525:192–216. doi: 10.1007/978-3-319-67738-5_12
53. Bird JM, Karageorghis CI, Baker SJ, Brookes DA, Nowicky AV. Ready exerciser one: Effects of music and virtual reality on cycle ergometer exercise. Br J Health Psychol. (2021) 26(1):15–32. doi: 10.1111/bjhp.12445
54. Story KM. Music therapy and avatars: Reflections on virtual learning environments for music therapy students. Voices. (2014) 14:1. doi: 10.15845/voices.v14i1.722
55. Optale G, Capodieci S, Pinelli P, Zara D, Gamberini L, Riva G. Music-enhanced immersive virtual reality in the rehabilitation of memory related cognitive processes and functional abilities: A case report. Presence. (2001) 10(4):450–62. doi: 10.1162/1054746011470217
56. Seinfeld S, Bergstrom I, Pomes A, Arroyo-Palacios J, Vico F, Slater M, et al. Influence of music on anxiety induced by fear of heights in virtual reality. Front Psychol. (2015) 6:1969–1969. doi: 10.3389/fpsyg.2015.01969
57. Nooij SAE, Pretto P, Oberfeld D, Hecht H, Bülthoff HH. Vection is the main contributor to motion sickness induced by visual yaw rotation: Implications for conflict and eye movement theories. PLoS ONE. (2017) 12:4. doi: 10.1371/journal.pone.0175305
58. Holdworth A. Nocturnes by candlelight - deep sleep and relaxation [Video]. YouTube. Available at: https://www.youtube.com/watch?v=IHFx3xOJf0g (2014, May 9).
59. Grove JR, Prapavessis H. Preliminary evidence for the reliability and validity of an abbreviated Profile of Mood States. Int J Sport Psychol. (1992) 23(2):93–109.
60. Curran SL, Andrykowski MA, Studts JL. Short form of the Profile of Mood States (POMS-SF): Psychometric information. Psychol Assess. (1995) 7(1):80–3. doi: 10.1037/1040-3590.7.1.80
61. Thomas KA, Clifford S. Validity and mechanical Turk: An assessment of exclusion methods and interactive experiments. Comput Human Behav. (2017) 77:184–97. doi: 10.1016/j.chb.2017.08.038
62. Weisberg HF. The total survey error approach: A guide to the new science of survey research. Chicago: University of Chicago Press (2005).
63. Hartmann T, Wirth W, Schramm H, Klimmt C, Vorderer P, Gysbers A, et al. The spatial presence experience scale (SPES). J Media Psychol. (2015) 28:1. doi: 10.1027/1864-1105/a000137
64. Chirico A, Maiorano P, Indovina P, Milanese C, Giordano GG, Alivernini F, et al. Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J Cell Physiol. (2020) 235(6):5353–62. doi: 10.1002/jcp.29422
65. Hoffman HG, Chambers GT, Meyer WJ III, Arceneaux LL, Russell WJ, Seibel EJ, et al. Virtual reality as an adjunctive non-pharmacologic analgesic for acute burn pain during medical procedures. Ann Behav Med. (2011) 41(2):183–91. doi: 10.1007/s12160-010-9248-7
66. Sweller J. Element interactivity and intrinsic, extraneous, and germane cognitive load. Educ Psychol Rev. (2010) 22(2):123–38. doi: 10.1007/s10648-010-9128-5
67. Wickens CD, Lee JD, Liu Y, Becker SE. An introduction to human factors engineering. 2nd ed. New York: Pearson (2004).
68. Moors A, Ellsworth PC, Scherer KR, Frijda NH. Appraisal theories of emotion: State of the art and future development. Emot Rev. (2013) 5(2):119–24. doi: 10.1177/1754073912468165
69. Albani G, Pedroli E, Cipresso P, Bulla D, Cimolin V, Thomas A, et al. Visual hallucinations as incidental negative effects of virtual reality on parkinson's Disease patients: A link with neurodegeneration? Park Dis. (2015) 2015:194629–6. doi: 10.1155/2015/194629
70. Rebenitsch L, Owen C. Review on cybersickness in applications and visual displays. Virtual Real. (2016) 20(2):101–25. doi: 10.1007/s10055-016-0285-9
71. Biedel D, Fruech C, Neer S, Bowers C, Rizzo A. Using virtual reality as part of an intensive treatement programs for PTSD. In Interservice/Industry Training, Simulation, and Education Conference (I/ITSEC). https://ict.usc.edu/pubs/Using%20Virtual%20Reality%20as%20Part%20of%20an%20Intensive%20Treatment%20Program%20for%20PTSD.pdf (2014).
72. Ioannou A, Papastavrou E, Avraamides MN, Charalambous A. Virtual reality and symptoms management of anxiety, depression, fatigue, and pain: A systematic review. SAGE Open Nurs. (2020) 6:2377960820936163. doi: 10.1177/2377960820936163
73. Shah LBI, Torres S, Kannusamy P, Chng CML, He H, Klainin-Yobas P. Efficacy of the virtual reality-based stress management program on stress-related variables in people with mood disorders: The feasibility study. Arch Psychiatr Nurs. (2015) 29(1):6–13. doi: 10.1016/j.apnu.2014.09.003
74. La Montagna R, Canonico R, Alfano L, Bucci E, Boffo S, Staiano L, et al. Genomic analysis reveals association of specific SNPs with athletic performance and susceptibility to injuries in professional soccer players. J Cell Physiol. (2019) 235:2139–48. doi: 10.1002/jcp.29118
75. Dahlquist LM, McKenna KD, Jones KK, Dillinger L, Weiss KE, Ackerman CS. Active and passive distraction using a head-mounted display helmet. Health Psychol. (2007) 26(6):794–801. doi: 10.1037/0278-6133.26.6.794
76. Gutierrez-Maldonado J, Gutierrez-Martinez O, Cabas-Hoyos K. Interactive and passive virtual reality distraction: Effects on presence and pain intensity. J Cyber Ther Rehabil. (2011) 4(2):147. https://pubmed.ncbi.nlm.nih.gov/21685644/
77. Dugas MJ, Freeston MH, Ladouceur R, Léger E, Langlois F, Provencher MD, et al. Group cognitive-behavioral therapy for generalized anxiety disorder: treatment outcome and long-term follow-up. J Consult Clin Psychol. (2003) 71(4):821–5. doi: 10.1037/0022-006X.71.4.821
78. Erekson DM, Lambert MJ, Eggett DL. The relationship between session frequency and psychotherapy outcome in a naturalistic setting. J Consult Clin Psychol. (2015) 83(6):1097–107. doi: 10.1037/a0039774
79. Indovina P, Barone D, Gallo L, Chirico A, De Pietro G, Giordano A. Virtual reality as a distraction intervention to relieve pain and distress during medical procedures. Virtual reality as a distraction intervention to relieve pain and distress during medical procedures. Clin J Pain. (2018) 34(9):858–77. doi: 10.1097/AJP.0000000000000599
Keywords: virtual reality, music therapy, mood, media, well-being
Citation: Alexanian S, Foxman M and Pimentel D (2022) Virtual reality and music's impact on psychological well-being. Front. Rehabilit. Sci. 3:864990. doi: 10.3389/fresc.2022.864990
Received: 29 January 2022; Accepted: 27 July 2022;
Published: 11 August 2022.
Edited by:
James R Bagley, San Francisco State University, United StatesReviewed by:
Rachel M Flynn, San Francisco State University, United StatesOlimpia Pino, University of Parma, Italy
© 2022 Alexanian, Foxman and Pimentel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stephen Alexanian salexanian25@gmail.com
Specialty Section: This article was submitted to Interventions for Rehabilitation, a section of the journal Frontiers in Rehabilitation Sciences