 Camilla Højgaard Nejst
Camilla Højgaard Nejst Chalotte Glintborg
Chalotte Glintborg- 1Neurorehabilitation Copenhagen, Municipality of Copenhagen, Copenhagen, Denmark
- 2Department of Communication and Psychology, Aalborg University, Aalborg, Denmark
Background: There has been an increasing interest in the concept of hope within the field of brain injury rehabilitation. Existing reviews have nevertheless focused on stroke, leaving out the broad population of people with acquired brain injury (ABI). Furthermore a majority of the included studies in those reviews excluded the subgroup of people with communication difficulties, thus primarily giving voice to a select group of people with ABI.
Methods: A qualitative systematic review was conducted with the purpose of systematically reviewing and thematically synthesise findings about hope as experienced by adults with ABI in a rehabilitation or recovery process. The search strategy included peer-reviewed qualitative studies published after 2000 in English or Scandinavian languages. Searches of EBSCO databases incorporating CINAHL, MEDLINE, and PsycINFO were conducted together with SocINDEX, Social Work Abstracts, Eric and Web of Science. Ten qualitative studies were included, and the Critical Appraisal Skills Program (CASP) was used for assessing the quality and relevance of the ten studies. Qualitative findings were synthesized using Thomas and Harden's methodology.
Results: Through a thematic synthesis eleven subthemes were identified relating to experiences of hope. These were grouped into four analytical themes: (1) hope a two folded phenomenon; (2) time and temporality; (3) progress, goals and visibility and (4) the alliance; a balancing act requiring good communication skills.
Conclusion: This review has shown that even though hope has both a positive and negative side to it, it is necessary as a driving force for people with ABI in terms of supporting them to keep going and not give up. Rehabilitation professionals are advised to embrace the ambiguity of hope, customizing the support of hope to each person with ABI. Attention is needed on how to make progress visible for persons with ABI during their rehabilitation process just as rehabilitation professionals should acknowledge the alliance with the person with ABI as a core component of rehabilitation. This requires a focus on professionals' communication skills if hope promoting relationships between professionals and persons with ABI are to be achieved.
1 Introduction
When thinking of hope, one might come across stories of the nurse Florence Nightingale, also called “the Lady with the Lamp”. Florence Nightingale is particularly known for walking through the infirmaries at night with a lamp in her hand—tending to the wounded, often with a comforting word on her lips. It is therefore often referenced that Florence Nightingale walked the dark corridors and spread hope and light to the patients (1).
Since the 1950s, the concept of hope has gained relevance across disciplines and research cultures such as positive psychology, psychiatry, and nursing research (2–4). Many researchers have depicted the meaning of hope to human beings and described hope in numerous ways (5–8). However, researchers across disciplines agree that hope is both universal and specific (concrete) (5, 8, 9). Universal hope, according to Hammer, can be described as “a general belief in the future and a safeguard for human being by illuminating life itself”, whereas specific hope is described by Hammer as “connected to time and object” (8). Snyder et al. (10) have worked on a definition of hope (within rehabilitation) where hope is described as a goal-directed cognitive motivational process focused on the importance of particularized hope and goals (10). In contrast, research on hope within the field of chronic illness is defined and described differently. The researcher Barnard for instance says: “hoping is a posture, not a motive for achievement of a particular goal. It is a mode of experiencing oneself in relation to reality and time” (11).
Earlier studies often focused on hopelessness rather than hope, especially for persons with mental illness. But as researchers began to expand their horizons, they ended up exploring the construct of hope across diverse illness contexts, including the chronically ill, critically ill and terminally ill (9). Later, also research within vulnerable groups such as people with dual diagnosis have been explored as to how hope is experienced by people with co-occurring mental health and substance use problems (12–14), just as hope within the population of patients with spinal cord injury has been explored in recent years (15–19). Hope is therefore a well-known theme in relation to serious illness and disability. Many anthropological and sociological studies have emphasized the despair that can follow chronic and serious conditions (20–25), often connected with lack of hope or the struggle for hope (26).
1.1 Hope and acquired brain injury
When a person acquires a brain injury, something happens not only to the brain and body, but also the anticipated future. Experiencing an ABI can thus be conceptualized as a “critical event” that disrupts the structure of everyday life, The sociologist Bury refers to this event as a form of biographical disruption (23). In other words, an unexpected interruption of an otherwise expected normal course of life.
An acquired brain injury may be caused by stroke, hemorrhages in the brain other than stroke, trauma, tumors (benign and malignant), infections, poisoning, lack of oxygen (e.g., by drowning accidents and cardiac arrest with successful resuscitation) etc. (27). The consequences of brain injury can be physical, cognitive, psychological, linguistic, and communicative and often have a major impact on a person's life and identity According to Cantor et al., persons with ABI live with two images of the self: “Who I am now” and “Who I was before” (28). This identity reconstruction process is a dynamic process of contraction and expansion in which the person with ABI strikes a tentative balance between new and old selves. This process might call for professional support to revise self-narratives and to validate the loss of some identities (e.g., working identity) (29).
The rehabilitation of people with acquired brain injury strives for a holistic approach, where the bio-psycho-social model forms the basis for all rehabilitation (30, 31). However, Danish research within brain injury rehabilitation has shown that rehabilitation continues to mostly focus on the rehabilitation of practical functions in everyday life (Activities of Daily Living), physical functions and vocational rehabilitation (29, 32, 33). Thus, rehabilitation is primarily aimed at physical and functional rehabilitation, and not a holistic focus where the person's existential and emotional situation is also considered. Within a bio-psycho-social rehabilitation framework, there has been an increasing interest in the concept of hope. Having a hopeful stance and being able to identify possible pathways into a meaningful future is essential in times of uncertainty and despair.
Nochi (34) found that hope of recovery was used as a strategy by persons who had sustained a traumatic brain injury to reduce this experience of “loss of self”. Kuipers and colleagues (35), have identified a need for clinically relevant research on hope, which can guide practitioners in fostering hope to enhance the experiences and outcomes for persons with ABI and their family members (35).
1.1.1 Reviews on hope and stroke
In 2011, Bright and colleagues conducted a systematic review on hope after stroke (36). Nineteen articles were included, but only seven of these articles sought to explore hope (37–43). For the remaining 12 articles, hope was a key finding that was present when related topics such as recovery or quality of life were explored (36). Bright et al.'s review revealed that hope was complex and multidimensional. Moreover, hope was influenced by internal and external sources and had a positive impact on recovery following stroke. Their proposed conceptualization identified three attributes of hope: (1) an inner state, (2) outcome orientation, and (3) an active process (2, 36).
Soundy and colleagues published two reviews in 2014 (44, 45). The first being a narrative review focusing on factors promoting or hindering hope in persons with stroke or spinal cord injury. Moreover, it focused on identifying how (health) professionals could support the promotion of hope during rehabilitation (44). The second review proposed a framework for hope, arguing for a more generalized view of understanding why a certain hope exists or is identified by a patient (45).
Whereas Bright et al. included nineteen studies in their review, Soundy et al. ended up including ten studies. A total of four studies overlapped and were thus included in both reviews (37, 38, 43, 46). The above-mentioned reviews have contributed both in enhancing our understanding of hope. However, we still do not know much about the role of hope in persons following an ABI as both research teams only focused on people with stroke. Furthermore, more than half of the included studies in the three reviews either completely excluded persons with communication difficulties or only included persons if they didn't have pronounced communication difficulties. As a result, we know even less about experiences of hope when it comes to persons with communication difficulties (47).
Therefore, the purpose of this review is to capture the phenomenon of hope as experienced by the broad population of persons with ABI. Through a systematic search in relevant databases and a thematic synthesis, we aim to expand our understanding of hope as experienced and described by persons with acquired brain injury during a rehabilitation or recovery process. This knowledge can inform rehabilitation theory and practice further.
1.1.2 Review question
The specific question guiding this review is: “How is hope (as a phenomenon) experienced in the rehabilitation or recovery process of persons with acquired brain injury”? The qualitative PICo worksheet adapted from Miller, S.A. (2001) was used as a framework for building the search strategy1 (48). The different search terms for each of the three blocks in PICo are presented in Table 1.
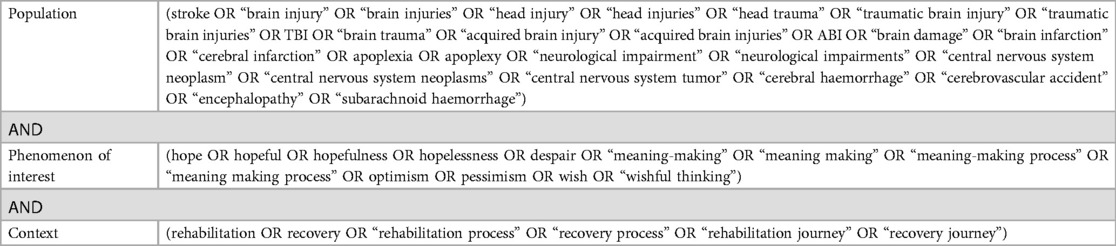
Table 1. PICo describing database search strategy.
2 Methods
A qualitative systematic literature review was conducted, and the approach and reporting were guided by the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) statement (49) and the PRISMA statement (50). To answer the research question, study results were synthesized, applying a thematic synthesis, as described by Thomas and Harden (51).
The research team conducting the search, screening and final inclusions of studies consist of the two authors (CHN and CG). The first author has several years of clinical experience within the field of ABI rehabilitation. The second author has done research within the field of ABI rehabilitation for more than 10 years and also holds clinical rehabilitation experience. Having a phenomenological standpoint, the authors are interested in exploring the lived experience of hope, thereby looking at hope from a first person perspective (persons with ABI).
2.1 Search strategy
A “subject-based strategy” was chosen since the approach has been shown to be more effective than the alternative (“research methodology-based strategy”) in retrieving qualitative patient-reported health-related quality of life research (52).
To develop relevant keywords (synonyms, near synonyms, broader and narrower concepts), pilot searches in selected databases were conducted (52, 53). The search was initially conducted in December 2021 with a follow up search in January 2023 (see Supplementary Appendices S1, S2 for search protocols) to ensure that any new studies meeting the inclusion criteria were included. However, no relevant studies were identified in this new search. The literature search included English and Scandinavian peer-reviewed articles published between 2000 and 2023.
In the attempt to find relevant studies in journals across different subjects—and research areas—a thorough and extensive search of seven databases was performed (53). To secure high recall without compromising precision, the following terms were included for block two about the phenomenon: “hope”, “hopeful”, “hopefulness”, “meaning making (process)”, “optimism”, “wish”, “wishful thinking” (see Supplementary Appendix S1 for the search in its entirety). Both “rehabilitation” and “recovery” were used as search terms for block three, as we wanted to include studies performed in an inpatient, as well as in an outpatient setting. Recovery is often linked to hope, thus a relevant term to include. The search terms and keywords were modified with input from an experienced librarian. Searches of EBSCO databases incorporating CINAHL, MEDLINE, and PsycINFO were undertaken together with SocINDEX, Social Work Abstracts, Eric and Web of Science (for further considerations on the choice of databases and the final search strategy see Supplementary Appendix S2). Any relevant protocol papers or conference abstracts identified from the database searches were followed up. A manual search of reference lists of relevant studies was also performed to complement the database search (53, 54).
2.1.1 Study selection
Search results from the seven databases were combined in the bibliographic software RefWorks and duplicates removed. The primary aim was to identify studies exploring the perspective of persons with ABI, where the phenomenon of interest was hope. From initial pilot searches, it quickly became clear that the inclusion criteria had to be adjusted if the review was to include more than five or six studies. Thus, inclusion criteria were revised so that studies were included if they had hope as a substantial part of their findings even if hope had not been the initial focus of the study. Although this final search strategy also generated a significant number of irrelevant hits, it was seen as a necessary process to ensure that appropriate literature was captured.
2.1.2 Eligibility criteria
The inclusion and exclusion criteria shown in Table 2 were used to determine eligible papers for study inclusion.
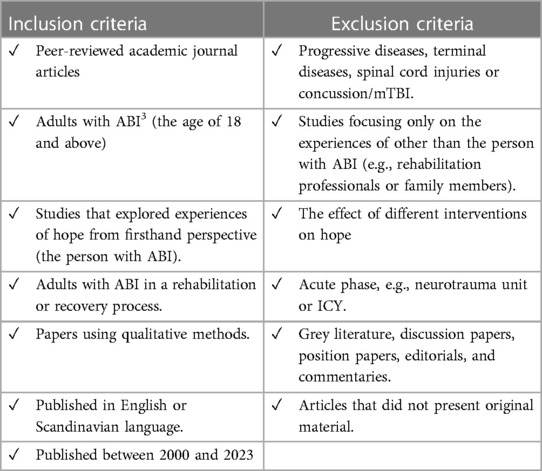
Table 2. Inclusion and exclusion criteria for study selection.
The selection of studies followed a two-stage process of screening and final selection. In order to ensure, systematicity and transparency the software Covidence was used in this process. Stage 1 (Screening): Titles and abstracts were screened against the inclusion and exclusion criteria and items deemed ineligible were removed. Stage 2 (Final selection): When articles appeared possibly to fit the inclusion criteria, full text copies of the articles were obtained. If it was not possible to determine the relevance by the title or abstract, a full text was also obtained to confirm or deny eligibility for inclusion (55). Full-text articles were then screened to ensure they met the inclusion and exclusion criteria and were relevant to the research question. Moreover, reference lists of the included studies were screened for further relevant studies.
2.1.3 Quality assessment
After having completed full-text readings of the final studies, the Critical Appraisal Skills Program (CASP), a checklist for qualitative research, was used for the evaluation of the ten studies. The CASP toolkit consists of 10 questions to facilitate rapid evaluation (56). All articles were determined to be of good quality and although some studies were small scale studies, they could potentially be a of valuable contribution to understanding the experience of hope. Full details of the CASP quality appraisal are provided in Table 3.
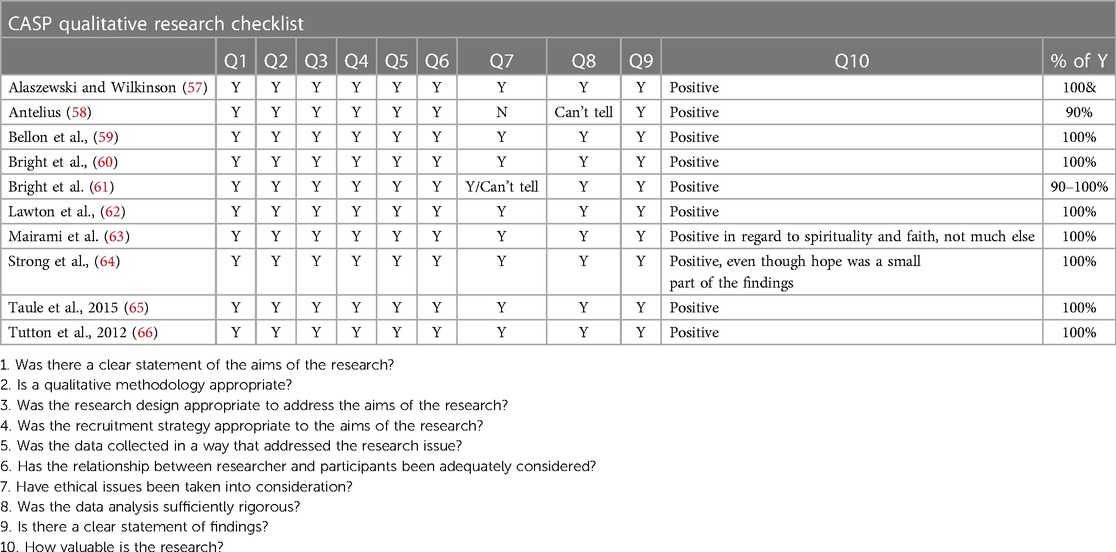
Table 3. CASP quality appraisal for all ten articles.
2.1.4 Data extraction and synthesis methodology
The included studies were categorized according to their primary focus. For each study, the following data were obtained and put into the result table: Author & year, aim (of study), time since injury, sample (size, sex, and population), methods (e.g., type of qualitative study), data analysis and results.
To syntizese findings, the thematic synthesis methodology developed by Thomas and Harden was used (51). The approach outlines a three-step process to guide the thematic synthesis. It involves (1) close reading of text to identify data-driven patterns that become “categories for analysis” (67). (2) Next, codes are developed inductively using the results sections from the first article and transfere these to the succeeding articles after which new codes are added. Based on this process, authors then develop descriptive themes representative of groups of identified codes, that align closely to the literature being synthesized. The last step of the process is where (3) authors develop analytical themes which require them to apply their own interpretation of article findings (51). Both authors (51) read the articles multiple times. The initial reading was performed to develop an understanding of the topic and to get an overview on how each study met the purpose of this review. First author did the initial coding and extracted information about hope in the article findings, leaving out sections/themes that did not deal with this topic. Afterwards both authors discussed all the initial codes. Finally the first author established broader descriptive themes based on codes and with confirmed consistency of the ascribed text. Descriptive themes were put into a matrix and organized into analytical themes which were discussed by the authors to ensure agreement.
3 Results
Figure 1 provides the results of the database search in total within a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) flow diagram (50). A total of 4,722 abstracts were identified. After the removal of duplicate records and records marked as ineligible by automation tools, 1,239 abstracts were left. Following review of titles and abstracts, 40 publications were identified for potential inclusion. The full texts of these were read and assessed for eligibility.
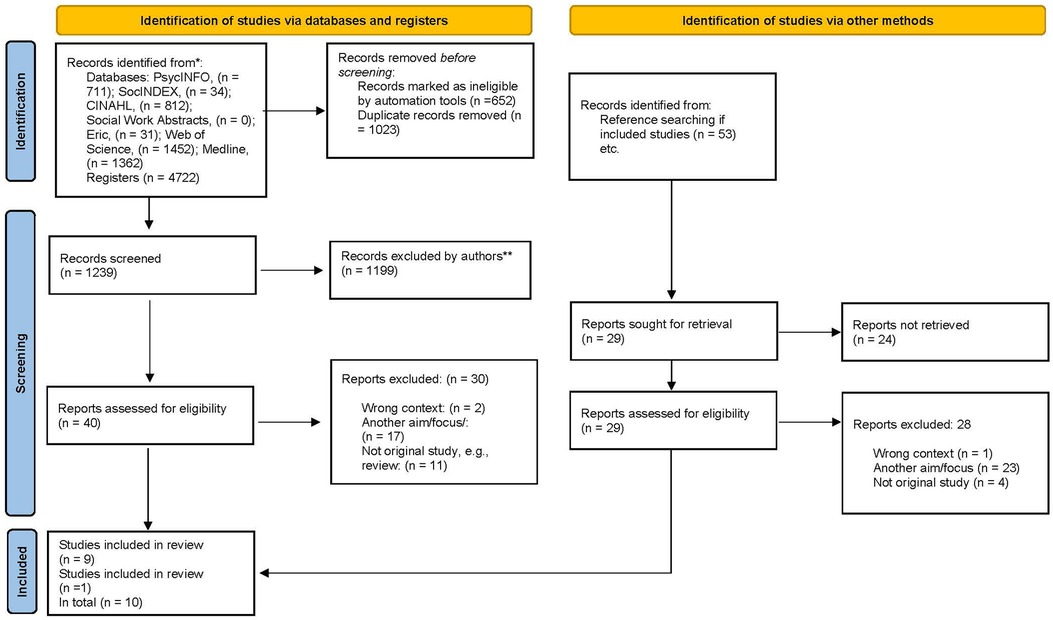
Figure 1. Prisma flow diagram.
Of the 40 studies retrieved for full text reading, only nine studies met the inclusion criteria. Hand-searching of the included articles' reference lists was also employed, where 29 studies were retrieved for full text reading, but only one additional study was identified which made a total of ten. The characteristics of these ten studies are presented in Table 4.
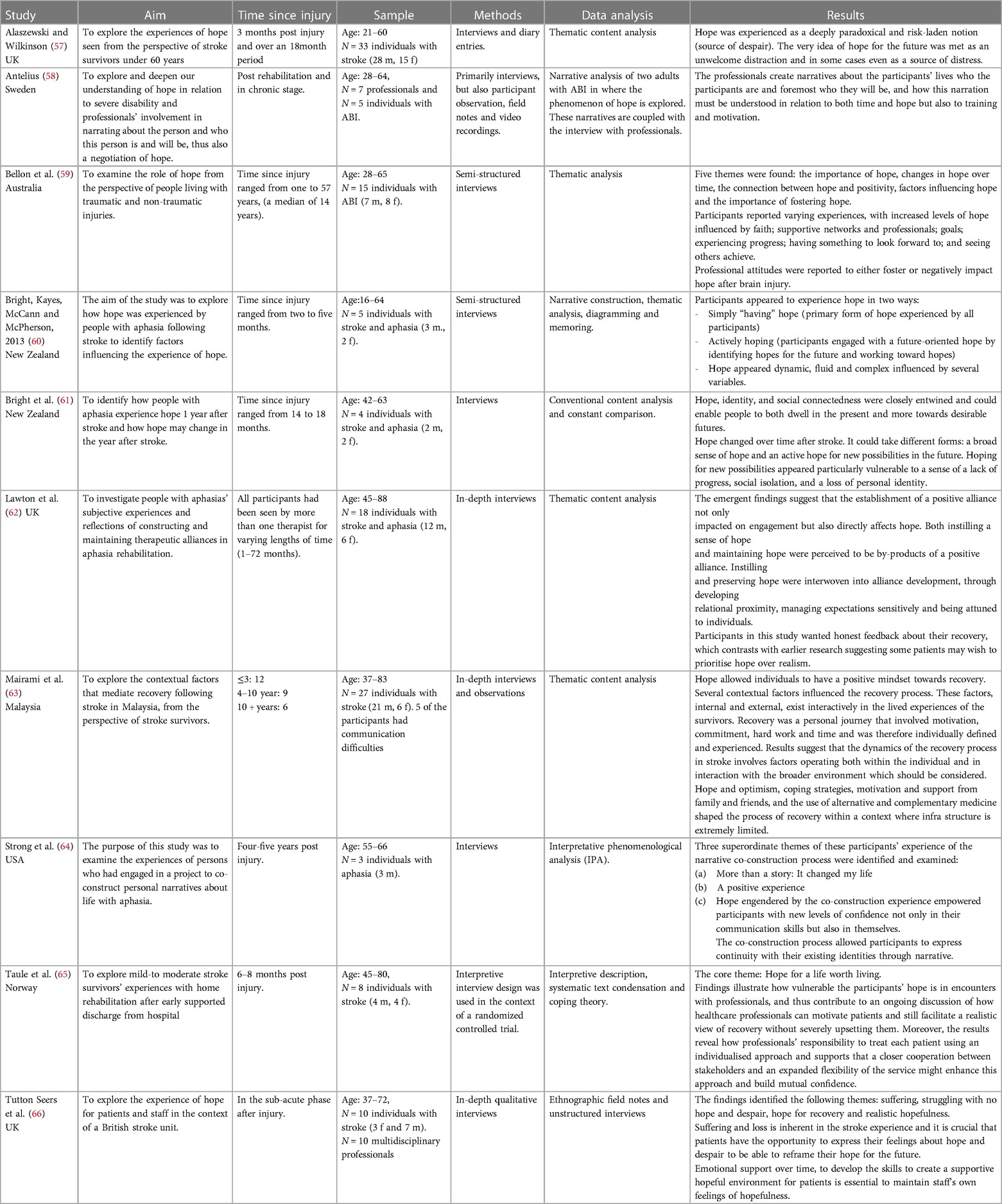
Table 4. Characteristics of included studies.
3.1 Characteristics of the included studies
As shown in Table 4, half of the studies were carried out in the UK, Norway and Sweden (57, 58, 62, 65, 66) two in New Zealand (60, 61), and the rest in the USA (64), Australia (59), and Malaysia (63). The numbers of participants across studies varied considerably from three (64) to 33 participants (57). The age of the persons with ABI varied from 21 to 88 years old.
Six of the studies (59–62, 64, 65) used semi-structured or in-depth interviews to collect data whereas four of the studies collected data through a wider range of ethnographic approaches (57, 58, 63, 66) such as observations, diary entries, and video recordings. While eight of the studies focused on the experience of the person with an ABI, two examined the perspective of both the person with the ABI and of the professionals (58, 66). In these cases, only the persons with acquired brain injury's experiences of hope were included. All ten studies tended to include both female and male participants, but with a preponderance of male participants (46 females and 87 males).
The ten included studies in this review support the claim that most research on the phenomenon of hope has been conducted within the stroke population. Eight studies had persons with stroke as their population of interest, leaving only two on ABI as a broad population, including both people with stroke and traumatic brain injuries etc. (58, 59). A total of four studies focused specifically on persons with stroke and aphasia (60–62, 64).
Most studies were performed in the post-acute to chronic phase. Across studies, time since injury ranged from 2 months to 57 years. Bellon et al. and Antelius focused on the chronic phase with Bellon having participants ranging from one to 57 years since injury (median age of 14 years) (59), and Antelius exploring the understanding of hope through fieldwork in the context of a daily activity center rather than a rehabilitation center (58). On the other hand, Bright et al. (60) and Tutton et al. (66) focused on the post-acute phase, namely outpatient community-based rehabilitation at two to four months after injury at a regional acute stroke unit.
The qualitative studies revealed hope to be a very fluid and paradoxical notion. However, at the same time also something of great importance for the persons' rehabilitation or recovery process. This will be unfolded in the thematic synthesis of findings.
3.2 Thematic synthesis
Four analytical themes and eleven sub-themes were identified in the thematic synthesis and are shown in Table 5. Only two out of ten studies included persons with ABI (e.g., stroke and TBI etc.) thereby having a primary interest in the broad population of people with ABI. In all four analytical themes, studies with participants with TBI as well as participants with stroke are represented. Thus, themes were identified across the broad ABI population. The four analytical themes being: (1) hope a two folded phenomenon; (2) time and temporality; (3) progress, goals, and visibility; and (4) the alliance; a balancing act requiring good communication skills. The themes are described in the following section and selected quotations from the reviewed studies are used to support the analysis.
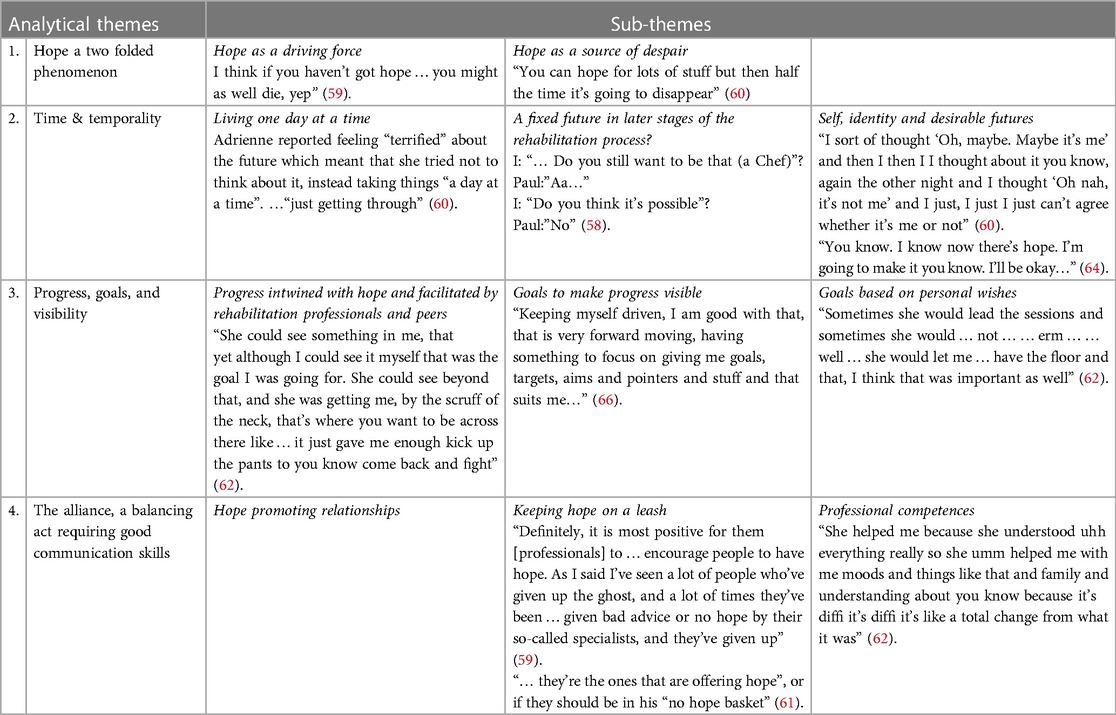
Table 5. The four analytical themes and sub-themes, with examples of quotes.
3.2.1 Theme 1: hope a two folded phenomenon
Hope turned out to be a very paradoxical phenomenon in which both a positive and negative side was embedded. Two sub-themes were identified in hope as a phenomenon.
3.2.1.1 Sub-theme: hope as a driving force
Four of the studies identified hope as having a protective effect, supporting persons with ABI to continue and not give up (59, 60, 65, 66). Taule et al. went so far as to describe hope as the most important driving force in the person's struggle to make their situation comprehensible and worthwhile (65). According to Tutton et al., there was a real contrast between persons with stroke who were highly motivated and determined and for whom hope came easily, and those that felt low, lacking motivation or “flat with dense weakness and apparently had no hope” (66). As described by one of the participants with ABI in the study by Bellon: “I think if you haven’t got hope … you might as well die, yep” (59).
Two of the studies identified the fact that hope became something that allowed persons with ABI to have a positive mindset (59, 63). Through interviews, Mairami et al. identified that hope could originate either from within the person or from those around them, fostering optimism for a functional life (63). Factors identified by Bellon et al. as “drivers” for maintaining or increasing hope were, among other things:
• support
• having something to look forward to
• mental health (59).
For people with communication difficulties such as aphasia, the most common source of hope was social relations (other people) as well as spiritual beliefs (60). The meaning of faith and spiritual experiences was also mentioned in other studies. Mairami found that some people who were not spiritual or religious before the stroke turned to faith after their injury. This faith provided them with solace and hope for recovery (63). Similarly, persons with ABI in the study by Bellon et al. felt that faith was an important factor influencing hope: “I have faith and that gives me hope” (59).
3.2.1.2 Sub-theme: hope as a source of despair
A connection between unfulfilled hopes and despair or emotional distress was identified in several studies, making it the flip side of hope (57, 59, 60, 65, 66). Persons with stroke experienced how hope could become a source of distress when it was connected to thoughts about the future (57). For persons with aphasia, hope was generally experienced as a good thing, but at the same time also difficult, since it could go unfulfilled (60). Uncertainty combined with thoughts about the future and having to redefine it, seemed to make persons with stroke vulnerable to feelings of distress and despair. Also, if the person had previous experiences of things gone wrong, they could be afraid that this would happen again and thus afraid to hope: “You can hope for lots of stuff but then half the time it's going to disappear” (60).
In the study by Bellon et al. some of the persons with ABI said that it could be difficult to gain hope and that hope was not always there:
“I guess I put hope in the same place I put happiness. Because … you’re always wanting to achieve it, or you’re always wanting to be in that state, but is that a realistic possibility? I don’t know” (59).
In a similar vain, one study described feelings of despair that could undermine hope and risk individuals falling into depression (66). Taken as a whole, the results indicate that hope is a multifaceted concept which can also have a negative side.
3.2.2 Theme 2: time and temporality
Three of the studies included in this review illuminated the temporality connected to hope and hoping (58, 60, 61). Three sub-themes were identified in relation to this analytical theme.
3.2.2.1 Sub-theme: living one day at a time
A present form of hope was identified as being dominant in people with stroke and aphasia. “Living in the moment” or “living one day at a time” was for many a response to the uncertainty inherent in thinking of the future—in effect, a way not to think about the future and to deal with the vulnerability that surfaced (60). In another study looking at how people with aphasia experienced hope one year post stroke and how it may have changed in that year (61), it was illustrated that the sense of hope was entwined with persons' views of their past and their present. Their perception of their poststroke recovery, well-being and view of the future was crucial in fostering—or threatening—their sense of hope for the future. Interestingly, Bright et al.'s study from 2020 suggested that the reference point for past comparisons shifted over time: in the post-acute phase, the comparisons were with their pre-stroke experience, whereas in the chronic phase they were with their immediate post-stroke experience (61). This could be seen as representing a process in which the persons revisited their hopes for the future and adjusted these based on their sense of what was possible and desirable: “I don’t believe hope can be the same [over time] as you [are not] the same” (61).
Bright et al. considered this movement in time to reflect the individual's desire, readiness, and capacity to move forward in life, actively constructing a future that they found both meaningful and imaginable (61).
3.2.2.2 Sub-theme: a fixed future in later stages of the rehabilitation process
The concept of time and temporality was amplified when people were in later stages of their rehabilitation or recovery process, especially regarding the present. In a study in persons with severe brain injuries at a day center in Sweden, the future of the persons (in this stage of rehabilitation) was characterized as less open and limited in possibilities (58). In the quote below, a young seemed to have a less positive view of impressionable possibilities:
Interviewer (I): “If you hadn’t been in that car accident, what do you think would have happened then”?
Paul (P): “Chef. Chef”.
I: “Chef? Right, you were going to train to be a chef”?
P: “I was”
I: “You were in chef training? [P nods.] In high school”?
P: “KOMVUX” [municipal adult education].
[…]
I: “Do you still want to be that?”
P: “Aa”
I: “Do you think it's possible”?
P: “No” (58).
To him the horizon seemed rather distant as the future did not hold the possibility of becoming a chef again (58).
Persons with ABI resided in the present because they would never fully recover. Some of the persons with ABI talked about a fragile time horizon, dependent on their physical abilities in the future, and located their hope in their ability in the present to maintain their functional level (58). In temporal terms, you might therefore say that the horizon was further away than in the earlier stages of the persons' rehabilitation or recovery process.
For persons with stroke and aphasia it was described that a sense of hope persisted in the light of challenges, and the hope of things could be better was pivotal to getting through each day (61). By contrast, actively engaging in a future-oriented hope was identified by Bright et al. as quite troublesome for people with stroke and aphasia (60). Nevertheless, Strong et al. suggested that participation in a co-construction process2 with a speech-language pathologist was supporting persons with aphasia to engage in an intentional exploration of this process of actively hoping (64) making it into a sort of bridge and offering the possibility of getting the individual closer to that horizon.
3.2.2.3 Sub-theme: self, identity, and desirable futures
Both studies that focused on self and identity centered on persons with stroke and aphasia (60, 64). It was experienced by persons in these studies that there was a disruption to their identity, leading to feelings of loss of identity. This loss of identity could also influence their experience of hope:
“I sort of thought ‘Oh, maybe. Maybe it's me’ and then I then I I thought about it you know, again the other night and I thought ‘Oh nah, it's not me’ and I just, I just I just can’t agree whether it's me or not” (60).
It was found that hope arose from what was perceived as meaningful to the participants and their sense of self, e.g., roles in life, sense of identity, faith, or an outlook on life. Hopes appeared to be relatively easy to identify and appeared from reflecting on past hopes and ways of being, the present and on their possible future (60). However, actively hoping could be more difficult for persons with communication difficulties as it was strongly language-based and involved identification of specific hopes. Hope, identity, and social connectedness were closely intertwined as hope could enable people with aphasia both to dwell in the present and to move towards to more desirable futures (61). The same study also found that persons with aphasia recalibrated their hopes for the future. This calibration process was influenced by the person's corresponding journey of identity re and co-construction. These two factors were therefore identified as significant in the recalibration of hope (61).
Strong et al. also found that the process of co-constructing a personal narrative with persons with stroke and aphasia was experienced as being positive (64). One of the individuals in this study felt it changed his life, suggesting that this process supported a positive view of identity. Hope engendered by the co-construction experience seemed to empower persons with stroke and aphasia with new levels of confidence, not only in their communication skills but also in themselves:
“You know. I know now there's hope. I’m I’m going to make it you know. I’ll be okay. I’ll get better and better. And and take time, but I’m getting better and better. And I I can do it. You know? I can I can I can do anything” (64).
As described earlier, Antelius stated in her study that: “In temporal terms there might be a horizon far away, but in narrative terms it is not an open one” (58). Applying a co-constructing intervention, as Strong et al. did in their study, seems to be a process that supports persons with communication difficulties (aphasia) to engage in an intentional exploration of the process of actively hoping (64), thus having the potential to open the horizon in narrative terms as well.
3.2.3 Theme 3: progress, goals and visibility
Four of the included studies dealt specifically with progress and its significance in relation to hope (59–62). Three sub-themes were identified.
3.2.3.1 Subtheme: progress intwined with hope and facilitated by rehabilitation professionals and peers
Seeing one's own progress as well as the progress of others was something that persons with stroke found to be a source of hope. Hope and progress appeared to have a mutually reinforcing effect (60, 61, 63).
For persons with aphasia, meeting other persons with aphasia was found to be important and instilled hope. Many had never heard of aphasia before, just as they had never met someone with aphasia, making it impossible for them to know what kind of progress was possible (60). In another study four persons were interviewed one year after their stroke, focusing on how hope might have changed during that year. The interviewees described increased hope for the future when they perceived they were making progress; conversely, a lack of progress threatened their sense of hope (60).
One study investigated the subjective experiences and reflections of persons with communication difficulties (aphasia) about constructing and maintaining therapeutic alliances in rehabilitation (62). In this process, the relationship between the person with aphasia and the health professional was shown to be of great importance. Even though this study focused on a specific group of professionals (speech and language therapists), the same may be true for other rehabilitation professionals. When progress was perceived as slow or imperceptible by the person, feedback from the therapist was of great importance as it was found to inculcate confidence and hope (62). As Terry in Lawton et al.'s study put it:
“[…] She could see something in me, that, yet although I could see it myself that was the goal I was going for. She could see beyond that, and she was getting me, by the scruff of the neck [gesturing], that's where you want to be across there like…it just gave me enough kick up the pants [laughs] to you know come back and fight” (62).
Thus, the therapist played a pivotal role, not only in making progress visible, but also in believing in the person, offering them hope for future improvement. It was precisely this kind of progress which was identified by persons with ABI as important in the maintenance and growth of hope (59). When persons with ABI in the study by Bellon et al. were asked to reflect on times where they felt they had made functional improvements or progress, they were thinking of milestones such as getting rid of a walking stick or being able to read a book in bed. Thus, every day events which showed their improvement and gave hope (59). Thus, the rehabilitation team was important for the participant's ability to build hope for recovery:
“They (municipal health care team) really came and stayed here and did something. They showed faith in positive development and supported me in that. It's important to convey that recovery can still happen, although the progress is slow” (65).
3.2.3.2 Sub-theme: goals to make progress visible
Across the included studies, goals were identified as another important theme regarding hope (60–62, 64, 66). As expressed by one of the persons with ABI:
“…One aspect that they’ve really got right is focusing on the goal setting. It makes people more positive, and it gives them hope for the future” (59).
Persons with ABI emphasized the importance of setting goals that were achievable and realistic and warned of the dangers of having unachievable goals: “If I set my goals too high, I fall into a, like my depression goes up, and I get all, it's not worth it. So, I do things little by little” (59).
In studies including persons with stroke (60, 62, 64, 66), goals were found to be of importance since hope for recovery reflected the determination to move forward or to meet aspirational goals:
“Keeping myself driven, I am good with that, that is very forward moving, having something to focus on giving me goals, targets, aims and pointers and stuff and that suits me…” (66).
A strong multidisciplinary approach to rehabilitation using tangible goals to direct recovery seemed important for persons with stroke, as they used goals as a way of being hopeful about the future:
“I want to get rid of the sexy stockings (compression stockings) by the end of this week, you have to walk 10 meters unaided before they go. So they are going this week. I have decided” (66).
3.2.3.3 Sub-theme: goals based on personal wishes
Professionals could risk undermining the hopes of the persons with ABI, and thereby increasing hopelessness or resignation about their future, by clinging to unrealistic hopes. This made it crucial to support people in imagining future possibilities when lack of progress hit (61). According to Lawton et al., genuine collaboration was dependent on the therapist's ability to listen carefully to the person with aphasia's narrative if they wanted to generate goals concordant with the person's priorities and needs (62). Persons who felt that their therapist had attempted to incorporate their personal wishes felt highly engaged with the process, which directly impacted on their engagement in rehabilitation:
“Sometimes she would lead the sessions and sometimes she would … not … … erm … … well … she would let me … have the floor and that, I think that was important as well” (62).
On the other hand, persons with stroke could feel inadequately understood, if the rehabilitation was not based on their personal wishes:
“They just had a plan of returning me back to work. It was their goal. When they repeated that every time we met, then I started to cry I think, every time” (65).
Strong et al. also found that the process of co-constructing a personal narrative with persons with aphasia was experienced as being positive, offering an opportunity for the individual to actively contemplate the future and their own goals (64).
3.2.4 Theme four: the alliance; a balancing act requiring good communication skills
The importance of the therapeutic alliance and rehabilitation professionals' skills is a theme in more than half of the included studies in this review, making it a substantial factor relating to hope in a rehabilitation or recovery process (59–62, 64, 65). This theme seemed to be even more decisive when it came to persons with stroke and communication difficulties (aphasia) (60–62, 64). Three sub-themes were identified in relation to this analytical theme.
3.2.4.1 Sub-theme: hope promoting relationships
The professionals' ability to provide hope for persons with stroke and aphasia appeared to be influenced by the strength of the therapeutic relationship (60). At the same time, engagement in the therapeutic process was described as central to the establishment of a partnership between the person with stroke and the health professional. An effective alliance could promote adherence and instill hope whereas an ineffective alliance eroded hope (60, 65). If the professionals were perceived to be too distant, maintaining rigid and inflexible boundaries, it could directly affect persons' engagement in rehabilitation as this was incompatible with their needs (62). This was especially true in the early stages of rehabilitation, during which persons with ABI were highly vulnerable and therefore needed more than professional distance.
On the other hand, being too attached posed a risk to independence and encouraged overreliance (62). Close alliances were characterized as genuine, friendly, non-judgmental, caring, open and connected. In order to provide the necessary infrastructure for establishing positive therapeutic relationships, the therapist needed to base it on honesty, trust, and respect (62). The therapeutic alliance was challenged when the person with ABI experienced unmanageable pressure about what to do or manage, as the confidence in the professional then was challenged. Also, professionals’ lack of expertise could challenge the alliance as this constituted a source of frustration for the person with ABI, as could controversies developing between persons with ABI and professionals or among professionals (65).
3.2.4.2 Sub-theme: keeping hope on a leash
In the study by Bellon et al. the persons with ABI had mixed experiences of how professionals had encouraged or discouraged their hope, some recalling positive and some negative experiences. Negative experiences could involve the professionals being negative about the(ir) future (59). As a participant in the study by Bellon et al. explained:
“Definitely, it is most positive for them [professionals] to … encourage people to have hope. As I said I’ve seen a lot of people who’ve given up the ghost, and a lot of times they’ve been … given bad advice or no hope by their so-called specialists, and they’ve given up” (59).
Receiving a bleak prognosis or meeting professionals that were negative about their future had a negative impact on the person with ABI's experiences of hope.
Some persons with ABI felt that the therapists had a responsibility to mask their lack of faith in their progress. However, they also requested a balance between optimism and realism (65). Some even expressed that hope and encouragement from others were essential for them. Like in the case of Matthew in Bright et al.'s study (2020), who evaluated people for their hope giving qualities considering whether: “… they’re the ones that are offering hope”, or if they should be in his “no hope basket” (61).
3.2.4.3 Sub-theme: professional competences
The skill set of professionals was of considerable importance across studies as professionals had the potential to discourage or encourage hope in the person with ABI (59, 60, 62, 65). According to Bellon et al., professionals could beneficially impact upon a person's experience of hope through person-centered and supportive therapeutic relationships (59). Taule and colleagues identified that successful encounters involving encouragement, empathy and equality seemed to promote the person with stroke's confidence in the professional's ability to help them manage their condition, as well as their sense of empowerment and their hope that they would be able to cope successfully in the future (65).
Participants appreciated and expressed a desire to cooperate with professionals who displayed essential therapeutic qualities, described as follows:
• Empathetic
• Taking time to listen
• Offering comfort
• Being nice
• Enthusiastic
• Making optimistic statements (65).
One skill that persons with stroke and aphasia identified as particularly important in helping them to think positive and be hopeful about the future was the professionals’ ability to be supportive. It was also perceived as necessary for the therapist to have highly attuned communication skills in order for the person with aphasia to have a sense of being heard and understood (60, 62). Skills like empathetic understanding (not just understanding), giving time and getting to know the human being (not just the diagnosis) were potentially of even greater importance if the persons were to avoid isolation, build trust and maintain hope. As the participant in the study by Lawton expressed it:
“She (professional) helped me because she understood uhh everything really so she umm helped me with me moods and things like that and family and understanding about you know because it's diffi it's diffi it's like a total change from what it was” (62).
4 Discussion
4.1 Summary of main findings
This qualitative synthesis of evidence highlights several key issues for persons with ABI to sustain and instill hope in a time of uncertainty and hopelessness. The four analytical themes and eleven sub-themes identified through thematic synthesis were (1) hope a two folded phenomenon, with the sub-themes “hope as a driving force” and “hope as a source of despair”; (2) time and temporality, with the sub-themes “living one day at a time”, “a fixed future in later stages of the rehabilitation process?” and “self, identity and desirable futures”; (3) progress, goals and visibility, with the sub-themes “progress intwined with hope and facilitated by rehabilitation professionals and peers”, “goals to make progress visible”; and “goals based on personal wishes” and lastly (4) the alliance; a balancing act requiring good communication skills, with the sub-themes “hope promoting relationships”, “keeping hope on a leash” and “professional competences”.
Previous systematic qualitative reviews have primarily explored hope in persons with stroke and left out other subgroups of ABI such as people with traumatic brain injury, hemorrhages in the brain other than stroke etc. (36, 44, 45). Moreover, most of the included studies in these reviews did not give voice to people with communication difficulties following ABI as they were often excluded (ibid).
This review includes all ABI groups and the findings are in line with previous reviews, in that hope is multifaceted (potentially having a positive as well as a negative effect), influenced by several factors (e.g., personal, or social), and crucially related to the establishment of goals (36, 44, 45). All four analytical themes were identified based on experiences that included both persons with TBI, haemorrhage etc. as well as stroke.
Our review highlights several good reasons to pay attention to time and temporality. First, time and temporality serve as a frame within which everything else unfolds, including the rehabilitation or recovery process. Secondly, time and temporality are shown to be of great importance for persons with ABI, especially in the later stages of their rehabilitation or recovery process. The results suggest that hope is to be found elsewhere in the more chronic phases of the rehabilitation, calling for different perspectives and amplifying the importance of the present instead of having a fixed view of the future. For persons with communication difficulties, time and temporality seems to play into their necessity to be rooted in time—specifically, in the present, which serves as an anchor and makes it possible to look at the future with the support of rehabilitation professionals. This leaves us with the question of whether it is easier to maintain or instill hope in earlier stages of rehabilitation compared to later stages? A study by Bright et al. showed that conversations about the future also seems to be constrained and limited in the inpatient setting poststroke (68). The study explored how clinicians talk about the future with patients and Bright et al. found that these types of conversations were constrained to short-term futures and limited to what aspects of life after stroke were discussed. According to Bright et al. being able to create conversational and relational spaces where people are supported to look into the future with a sense of possibility, hope, and potential is vital for persons to move forward in their lives post stroke. Based on their findings they conclude that, communication must be seen as a core clinical skill and a clinical intervention in its own right (68).
Our findings suggests that the relationship to professionals can promote adherence and instill hope, especially for persons with aphasia. This is supported by a meta-synthesis from 2020, where relationships were identified as being critical for persons experiencing communication impairment after stroke (69). In practice, this requires strong communicative competences in rehabilitation professionals (70, 71).
Communication partner training is an approach that has shown to be useful in supporting communication skills (72–76). In Denmark the method Supported Conversation for Adult with Aphasia (SCA) is relatively widespread in practice. A review by Christensen et al. shows that also cognitive communication disorders of people with TBI challenge the interaction between rehabilitation professionals and persons with TBI. Their findings demonstrate that the communicative barrier is closely related to the professionals' communicative approach. Moreover, that rehabilitation professionals holding a collaborative and acknowledging approach using supportive strategies are the ones that may facilitate successful communicative interactions (77). This point to the fact that rehabilitation professionals must be given the opportunity to acquire the necessary competencies in communication strategies.
Rehabilitation strives for a coherent approach, with the bio-psycho-social model forming the basis for rehabilitation (32, 33). Danish research in the field of brain injury has nevertheless shown that rehabilitation continues to primarily be aimed at physical and functional rehabilitation and does not adopt a holistic focus where the person's existential and emotional situation is considered (32, 33). Rehabilitation of the person's “inner life world” (inside-perspective), understood as dealing and coping with personal, identity-related, and emotional challenges, including hope, is given less focus, although it is an important and central aspect of a bio-psycho-social approach (32, 33). Being a professionally skilled occupational therapist or neuropsychologist is therefore not enough. In addition professionals need personal competences (70). According to Deegan, who has lived experience with disabilities, a decisive step toward understanding the experience of the person with a disability is that rehabilitation professionals embrace and accept their own woundedness and vulnerability because in doing so, “we share a common humanity” (78).
According to the Mattingly, professionals often focus on what she calls “the medical hope”, a narrow understanding where hope alone is tied to curation and rehabilitation in a more traditional sense. The hope of persons with an illness or disability, however, often involves a much broader understanding of hope as a journey towards healing or recovery, trying to find a positive meaning in what has happened (79–83).
The biomedical model offers no definitive cure when it comes to the physical and psychological consequences of an ABI. However, recovery is not only a pathological matter. Regaining quality of life can happen despite pathological consequences. Thus, there is an imperative need to hope even when everything seems hopeless. Hopelessness can have major consequences for the person, as it has been shown to be associated with depression and suicide across diagnoses (84–86). Hope, on the other hand, has been shown to have a positive impact on rehabilitation outcomes both for persons with mental and physical impairments (32, 33, 84, 87, 88). Within neurorehabilitation, it has been seen as good practice to confront persons with ABI with their disabilities since this could lead to greater insight and acceptance of difficulties and thus to a greater motivation to explore their limitations. In practice, however, it appears that confrontations do not necessarily lead to increased motivation. On the contrary, confrontations can lead either to individuals giving up and thus losing motivation and hope, or to mental resistance (89). This leaves rehabilitation professionals to walk a thin line between encouraging and discouraging hope when it comes to especially persons with ABI lacking insight in their own impairments.
Our analysis furthermore reveals that hope, identity, and social connectedness are closely intertwined as hope gives persons with aphasia the possibility both to dwell in the present but also to move forward. The co-construction of identity change are significant in the person's ability to recalibrate hope, which is often necessary during a rehabilitation or recovery process. For years anthropologists have written about the positive traits of narratives, in that story—told or acted upon—carry a healing potential through their contribution to the transformation of identity, interpretation of the past and even the creation of future scenarios (82, 90). When persons acquire a brain injury and are faced with an uncertain future, focusing on life as lived in and over time can therefore make good sense, since such life-changing experiences create a natural focus on both the past and the future. Our review suggests that collaborating with the person on co-constructing a personal narrative holds the potential to support a positive view of identity and to empower persons with aphasia (or other communication difficulties) with new levels of confidence in themselves. This is in line with research within the field of communication disorders, where several studies talk about co-constructed communication as being essential in offering communication partners a way to approach everyday conversation and supporting positive narratives that reaffirm a sense of self (91–93).
Professionals may be afraid of giving false hope, which is why they may end up promoting too little hope to the person with ABI. Being with persons who have wishes, hopes, and dreams for the future, and who at the same time are in a situation that complicates the achievement of these, can be experienced as difficult for professionals. Findings in this review suggest that there is an opposite relationship between professionals playing a vital role, not only in making progress visible, but also in offering persons with ABI hope for future improvement.
Being the “holder” of another human being's hope is not an easy task. In fear of giving false hope, professionals may imply and maintain a less hopeful rehabilitation perspective instead (66). It appears that professionals’ capacity to contain despair and maintain hope prevents the person from giving up and feeling devastated by the brain injury. This require professional skills to tolerate the uncertainty and despair of the person's life. This kind of support is particularly crucial in times when progress is slow.
As we clearly see in this and other reviews, goals are connected to hope. In an ethnographic study by Tonnesen and Nielsen among persons with Parkinson's disease, they found that rehabilitation goals could appear as steppingstones towards hope (94). The correlation between goals and hope is also emphasized in this review. Progress seems to be paramount for the person's ability to maintain hope over time, thereby making goals a way for professionals to make progress visible. Researchers such as Levack and colleagues have also linked rehabilitation goals and hope. Levack et al. found that rehabilitation goals may keep hope alive by symbolizing possible progress (95). In a Cochrane review from 2008, Levack and colleagues concluded that there is low quality evidence that goal setting may improve outcomes for adults in rehabilitation with various disabilities, and moreover that the best graded evidence favors positive effects for psychosocial outcomes (such as emotional status, health-related quality of life, etc.) rather than physical outcomes (95). In this review, persons with ABI and professionals have a clear focus on goal setting in relation to their physical functions, whereas functions in relation to psychosocial conditions are absent. Once again, it is important to stress that goals relating to the psychosocial dimension are equally important when trying to uphold a bio-psycho-social approach in rehabilitation.
Future research should consider looking at experiences of hope in specific stages of the person's rehabilitation or recovery process. This could be of importance for further understanding of the concept of hope as it develops especially over time and in time. Furthermore, future research should consider exploring whether gender, age, social network or pre-injury personality influence the way in which persons with ABI experience hope in their rehabilitation or recovery process. Last, a specific focus on persons with communication difficulties—specifically the subgroup of persons with TBI and cognitive communication disorders, could be of great value as this is often an overlooked group. This group of persons may have unique needs that warrant separate exploration which is why it is important to also include studies that provide persons with communication difficulties with a voice (47).
4.2 Implications for practice
In light of our results, professionals are advised to consider the impact of giving or taking hope away when it comes to the population of persons with ABI. This review supports the need for practice to acknowledge the deep and fundamental importance of the concept of hope as a major part of the rehabilitation and recovery of persons with ABI, and even more so for persons with communication difficulties such as aphasia.
The literature included in this study provides an insight into why hope is often described as a paradox, having both positive and negative qualities embedded. This paradoxical concept requires professionals to make individual assessments of each person with ABI to find out how hope can best be supported, in the light of the person's personality, social network, etc., as well as where the person is in their rehabilitation or recovery process.
Especially for the subgroup of persons with communication difficulties, there seems to be a need for professionals to acquire skills in how to support conversation and the co-construction of narratives. This entails knowledge on how to work with the personal narratives of the individual, making it crucial that professionals gain qualifications on how to use supportive conversation techniques and tools.
At the same time, this review underlines that professionals play a crucial role when it comes to maintaining supportive relationships and instilling hope throughout the rehabilitation or recovery process. The role requires professionals to value the humanity and personhood of the persons, making them feel heard and understood and keeping a hopeful stance about their potential for recovery. This calls for highly attuned communication skills, along with the ability to contain despair and uncertainty on behalf of the person without losing hope entirely.
If practice therefore wants to offer rehabilitation grounded in a bio-psycho-social approach, then the psychosocial wellbeing of the person needs to be a primary outcome of the rehabilitation on an equal footing with outcomes concerning physical functions. Thus, professionals need to have a raised awareness of the emotional support required if an individual is to recover from a brain injury as a whole person. That is to refer to appropriate health professionals and have cross disciplinary collaborations. This again points to the necessity of setting goals for the physical and more practical part of the person's rehabilitation as well as the psychosocial part of the person's overall recovery.
Professionals should be knowledgeable about the emotional dimensions of rehabilitation during their training and education. The current professional training sequence includes limited information about the relational impact professionals can have on persons in rehabilitation and the psychosocial dimensions of this process. If we are to pay greater attention to social and psychological factors in the lives of people with disabilities and chronic health conditions, there need to be opportunities for cross-disciplinary professionals in general to have continuing education in psychosocial rehabilitation and to work with and develop their own personal skills at various levels of training.
4.3 Limitations
We have used an aggregative review form, namely a systematic review of qualitative research, as we wanted to accumulate knowledge relevant to the phenomenon of hope and show relationships among the pieces of knowledge across the included studies (96). In doing so we have tried to guide the selection of studies by clear eligibility criteria just as a systematic approach has been applied in the different steps of the review process. A review protocol was outlined and adapted along with the search process but only used as a working tool for the authors and therefore not registered at e.g., PROSPERO.
With this review we wanted to explore hope as experienced by the broad ABI population in a rehabilitation or recovery setting. This resulted in studies that cut across diagnostic groups covering many different impairments and taking place in a mixture of in- and outpatient services at several different stages of the rehabilitation or recovery process. In our thematic synthesis we have tried to be transparent about the different contexts of the included studies, but nevertheless the broad scope of this review is both a strength and a weakness. There is a limitation upon transferability of the findings in relation to the contextual data presented in the studies that could have been followed more closely throughout the review if the context of the studies had been more alike.
Although some of the included studies in this review only had few participants the data from these qualitative studies were of great importance as they gave valuable insight into an often-excluded group: People with ABI and communication difficulties (aphasia). So even though some would argue it to be a limitation (small sample size), it proved to be necessary in this qualitative review in order to represent the broad group of people with ABI.
Most of the included studies were gathered in high or middle-income countries which probably has a significance in that other perspectives could be imagined to be present in low-income countries, which possibly do not have the same infrastructure around healthcare.
The thematic synthesis methodology applied to this review offers a transparent approach to the synthesis of the primary studies; however, future research should consider whether other approaches used to analyse data could help bring other aspects of hope to the surface.
4.4 Conclusions
According to the findings of this review, rehabilitation professionals should embrace the ambiguity of hope, as a driving force as well as a source of despair. Attention must be paid to time and temporality and how to make progress visible as well as tangible for persons with ABI during their rehabilitation or recovery process. Finally, rehabilitation professionals must acknowledge the relationship with the individual with ABI as a core component of the rehabilitation in general. This requires a focus on professionals' personal competences, as a hope-promoting relationship between the professional and the person with ABI seems to be needed in order to accommodate to the psycho-social part of the bio-psycho-social approach.
Author contributions
CH: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CG: Conceptualization, Data curation, Formal Analysis, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This review is part of a full PhD scholarship funded by the rehabilitation center “Neurorehabilitation Copenhagen”, Municipality of Copenhagen, Denmark (DK).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2024.1376895/full#supplementary-material
Footnotes
1PICo worksheet and search strategy. US National Center for Dental Hygiene Research. The form is accessible at KUB’s (Det kongelige bibliotek) website [Forskningsspørgsmål, PICO og andre metoder—Systematiske reviews—Index at The Royal Danish Library (kb.dk)].
2A co-construction process where the person with aphasia was supported in having their story written down (who I was before my stroke/aphasia, my stroke and aphasia, who I am today, my future/goals), potentially including support from a family member, for instance clarifying a specific point in the story, or the clinician, for instance uploading a photo.
References
1. tfe From Wikipedia. Florence Nightingale (2022). Available online at: en.Wikipedia.org (Accessed August 29, 2022).
2. Snyder CR, Rand KL, Sigmon DR. Hope theory: a member of the positive psychology family. In: Snyder CR, Lopez SJ, editors. Handbook of Positive Psychology. Oxford (UK): Oxford University Press (2002). p. 231–43.
6. Fromm E. The Revolution of Hope: Toward a Humanized Technology. New York (NY): Harper & Row. (1968).
7. Kylma J, Vehvilainen-Julkunen K. Hope in nursing research: a meta-analysis of the ontological and epistemological foundations of research on hope. J Adv Nurs. (1997) 25:364–71. doi: 10.1046/j.1365-2648.1997.1997025364.x
8. Hammer K, Mogensen O, Hall EOC. The meaning of hope in nursing research: a meta-synthesis. Scand J Caring Sci. (2009) 23:549–57. doi: 10.1111/j.1471-6712.2008.00635.x
9. Nekolaichuk CL, Jevne RF, Maguire TO. Structuring the meaning of hope in health and illness. Soc Sci Med. (1999) 48:591–605. doi: 10.1016/S0277-9536(98)00348-7
10. Snyder CR, Lehman KA, Kluck B, Monsson Y. Hope for rehabilitation and vice versa. Rehabil Psychol. (2006) 51:89–112. doi: 10.1037/0090-5550.51.2.89
11. Barnard D. Chronic illness and dynamics of hoping. In: Toombs D, Carson RA, editors. Chronic Illness from Experience to Policy. Indianapolis (IN): Indiana University Press (1995). p. 38–58.
12. Sælør K, Ness O, Holgersen H, Davidson L. Hope and recovery: a scoping review. Adv Dual Diagn. (2014) 7:63–72. doi: 10.1108/ADD-10-2013-0024
13. Davidson L, Andres-Hyman R, Bedregal L, Tondora J, Frey J, Kirk TA. From double trouble to dual recovery: integrating models of recovery in addiction and mental health. J Dual Diagn. (2008) 4:273–90. doi: 10.1080/15504260802072396
14. Sælør K, Ness O, Semb R. Taking the plunge service users’ experience of hope. Scand Psychol. (2015) 2:1–20. Article e9.
15. Lohne V. Back to life again—patients’ experiences of hope three to four years after a spinal cord injury. A longitudinal study. Can J Neurosci Nurs. (2009) 31:20–5.19522458
16. Lohne V, Severinsson E. The power of hope: patients’ experiences of hope a year after acute spinal cord injury. J Clin Nurs. (2006) 15:315–23. doi: 10.1111/j.1365-2702.2006.01301.x
17. Lohne V, Severinsson E. Hope and despair: the awakening of hope following acute spinal cord injury—an interpretative study. Int J Nurs Stud. (2004) 41:881–90. doi: 10.1016/j.ijnurstu.2004.04.002
18. Lohne V, Severinsson E. Patients’ experiences of hope and suffering during the first year following acute spinal cord injury. J Clin Nurs. (2005) 14:285–93. doi: 10.1111/j.1365-2702.2004.01088.x
19. Lohne V, Severinsson E. Hope during the first months after acute spinal cord injury. J Adv Nurs. (2004) 47:279–86. doi: 10.1111/j.1365-2648.2004.03099.x
20. Frank AW. The Wounded Storyteller: Body, Illness, and Ethics. Chicago (IL): University of Chicago Press (1995).
21. Kleinman A. The Illness Narratives: Suffering, Healing, and the Human Condition. New York (NY): Basic Books (1989).
22. Murphy R. Encounters: the body silent in America. In: Ingestad B, Whyte S, editors. Disability and Culture. Berkeley (CA): University of California Press (1995). p. 108–20.
23. Bury M. Chronic illness as biographical disruption. Sociol Health Illn. (1982) 4:167–82. doi: 10.1111/1467-9566.ep11339939
24. Charmaz K. Loss of self: a fundamental form of suffering in the chronically ill. Sociol Health Illn. (1983) 5:168–95. doi: 10.1111/1467-9566.ep10491512
25. Whyte S. Uncertain undertakings: practicing health care in the subjunctive mood. In: Steffen V, Jessen H, Jenkins R, editors. Managing Uncertainty, Ethnographic Studies of Illness, Risk and Struggle for Control. Copenhagen: Museum Tusculanum Press (2005). p. 245–65.
26. Mattingly C. The Paradox of Hope. Journeys Through a Clinical Borderland. Berkeley (CA): University of California Press (2010).
27. Danish Health Authority (Sundhedsstyrelsen), Recommendations for intersectoral courses for adults with acquired brain injury—stroke and transient cerebral ischemia (TCI)—trauma, infection, tumor, subarachnoid hemorrhage and encephalopathy (2021).
28. Cantor JB, Ashman TA, Schwartz ME, Gordon WA, Hibbard MR, Brown M, et al. The role of self-discrepancy theory in understanding post-traumatic brain injury affective disorders: a pilot study. J Head Trauma Rehabil. (2005) 20:527–43. doi: 10.1097/00001199-200511000-00005
30. World Health Organization. International Classification of Functioning, Disability and Health. (2024). Available online at: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (Accessed March 20, 2024).
31. Engel GL. The need for a new medical model: a challenge for biomedicine. Psychodyn Psychiatry (2012) 40:377–96. doi: 10.1521/pdps.2012.40.3.377
32. Glintborg C, Hansen TGB. Psychosocial sequelae after acquired brain injury: a 5-year follow-up. Nord Psychol (2021) 73:119–35. doi: 10.1080/19012276.2020.1817769
33. Glintborg C, Hansen TGB. Bio-psycho-social effects of a coordinated neurorehabilitation programme: a naturalistic mixed methods study. NeuroRehabilitation. (2016) 38:99–113. doi: 10.3233/NRE-161301
34. Nochi M. “Loss of self” in the narratives of people with traumatic brain injuries: a qualitative analysis. Soc Sci Med. (1998) 46:869–78. doi: 10.1016/S0277-9536(97)00211-6
35. Kuipers P, Doig E, Kendall M, Turner B, Mitchell M, Fleming J. Hope: a further dimension for engaging family members of people with ABI. NeuroRehabilitation. (2014) 35:475–80. doi: 10.3233/NRE-141139
36. Bright F, Kayes NM, McCann CM, McPherson KM. Understanding hope after stroke: a systematic review of the literature using concept analysis. Top Stroke Rehabil. (2011) 18:490–508. doi: 10.1310/tsr1805-490
37. Arnaert A, Filteau N, Sourial R. Stroke patients in the acute care phase: role of hope in self-healing. Holist Nurs Pract. (2006) 20:137–46. doi: 10.1097/00004650-200605000-00008
38. Bays CL. Older adults’ descriptions of hope after a stroke. Rehabil Nurs (2001) 26:18–27. doi: 10.1002/j.2048-7940.2001.tb02203.x
39. Popovich JM, Fox PG, Burns KR. “Hope” in the recovery from stroke in the U.S. Int J Psychiatr Nurs Res (2003) 8:905–20.12683340
40. Popovich J, Fox P, Bandagi R. Coping with stroke: psychological and social dimensions in U.S. Patients. Int J Psychiatr Nurs Res (2007) 12:1474–87.17682588
41. Gum A, Snyder CR, Duncan PW. Hopeful thinking, participation, and depressive symptoms three months after stroke. Psychol Health. (2006) 21:319–34. doi: 10.1080/14768320500422907
42. Bluvol A. The codman award paper: quality of life in stroke survivors and their spouses: predictors and clinical implications for rehabilitation teams. Axone. (2003) 25:10–9.14733173
43. Cross A, Schneider M. A preliminary qualitative analysis of the impact of hope on stroke recovery in women. Top Stroke Rehabil (2010) 17:484–95. doi: 10.1310/tsr1706-484
44. Soundy A, Stubbs B, Freeman P, Coffee P, Roskell C. Factors influencing patients’ hope in stroke and spinal cord injury: a narrative review. Int J Ther Rehabil. (2014) 21:210–8. doi: 10.12968/ijtr.2014.21.5.210
45. Soundy A, Liles C, Stubbs B, Roskell C. Identifying a framework for hope in order to establish the importance of generalised hopes for individuals who have suffered a stroke. Adv Med. (2014) 2014:1–8. doi: 10.1155/2014/471874
46. Barker RN, Brauer SG. Upper limb recovery after stroke: the stroke survivors’ perspective. Disabil Rehabil (2005) 27:1213–23. doi: 10.1080/09638280500075717
47. Lloyd A, Bannigan K, Sugavanam T, Freeman J. Experiences of stroke survivors, their families and unpaid carers in goal setting within stroke rehabilitation: a systematic review of qualitative evidence. JBI Database System Rev Implement Rep (2018) 16:1418–53. doi: 10.11124/JBISRIR-2017-003499
49. Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol (2012) 12:181. doi: 10.1186/1471-2288-12-181
50. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (2021) 372:n71. doi: 10.1136/bmj.n71
51. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. (2008) 8:45. doi: 10.1186/1471-2288-8-45
52. Gorecki CA, Brown JM, Briggs M, Nixon J. Evaluation of five search strategies in retrieving qualitative patient-reported electronic data on the impact of pressure ulcers on quality of life. J Adv Nurs (2010) 66:645–52. doi: 10.1111/j.1365-2648.2009.05192.x
53. Shaw RL, Booth A, Sutton AJ, Miller T, Smith JA, Young B, et al. Finding qualitative research: an evaluation of search strategies. BMC Med Res Methodol (2004) 4:5. doi: 10.1186/1471-2288-4-5
54. Papaioannou D, Sutton A, Carroll C, Booth A, Wong R. Literature searching for social science systematic reviews: consideration of a range of search techniques. Health Info Libr J (2010) 27:114–22. doi: 10.1111/j.1471-1842.2009.00863.x
55. Dixon-Woods M, Shaw RL, Agarwal S. The problem of appraising qualitative research. Qual Saf Health Care. (2004) 13:114–22. doi: 10.1136/qshc.2003.008714
57. Alaszewski A, Wilkinson I. The paradox of hope for working age adults recovering from stroke. Health (London) (2015) 19:172–87. doi: 10.1177/1363459314555242
58. Antelius E. The meaning of the present: hope and foreclosure in narrations about people with severe brain damage. Med Anthropol Q. (2007) 21:324–42. doi: 10.1525/maq.2007.21.3.324
59. Bellon M, Kelley J, Fisher A. “The bucket of gold at the end of the rainbow”: personal experiences of hope after acquired brain injury. Disabil Rehabil (2022) 44:7974–84. doi: 10.1080/09638288.2021.2005162
60. Bright FAS, Kayes NM, McCann CM, McPherson KM. Hope in people with aphasia. Aphasiology (2013) 27:41–58. doi: 10.1080/02687038.2012.718069
61. Bright FAS, McCann CM, Kayes NM. Recalibrating hope: a longitudinal study of the experiences of people with aphasia after stroke. Scand J Caring Sci. (2020) 34:428–35. doi: 10.1111/scs.12745
62. Lawton M, Haddock G, Conroy P, Serrant L, Sage K. People with aphasia’s perception of the therapeutic alliance in aphasia rehabilitation post stroke: a thematic analysis. Aphasiology (2018) 32:1397–417. doi: 10.1080/02687038.2018.1441365
63. Mairami FF, Warren N, Allotey PA, Reidpath DD. Contextual factors that shape recovery after stroke in Malaysia. Disabil Rehabil. (2020) 42:3189–98. doi: 10.1080/09638288.2019.1588399
64. Strong KA, Lagerwey MD, Shadden BB. More than a story: my life came back to life. Am J Speech Lang Pathol. (2018) 27:464–76. doi: 10.1044/2017_AJSLP-16-0167
65. Taule T, Strand LI, Skouen JS, Råheim M. Striving for a life worth living: stroke survivors’ experiences of home rehabilitation. Scand J Caring Sci. (2015) 29:651–61. doi: 10.1111/scs.12193
66. Tutton E, Seers K, Langstaff D, Westwood M. Staff and patient views of the concept of hope on a stroke unit: a qualitative study. J Adv Nurs (2012) 68:2061–9. doi: 10.1111/j.1365-2648.2011.05899.x
67. Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods (2006) 5(1):80–92.
68. Bright FAS, Kayes NM, Soundy A, Drown J. Limited conversations about constrained futures: exploring clinicians’ conversations about life after stroke in inpatient settings. Brain Impair. (2024) 25:1–12. doi: 10.1071/IB23067
69. Bright F, Reeves B. Creating therapeutic relationships through communication: a qualitative metasynthesis from the perspectives of people with communication impairment after stroke. Disabil Rehabil. (2020) 44:2670–82. doi: 10.1080/09638288.2020.1849419
70. Maribo T, Ibsen C, Thuesen J, Vinther Nielsen C, Sau Johansen J, Bonnerup Vind A. White Pater on Rehabilitation [Hvidbog om rehabilitering]. 1st ed. Aarhus (DK): Rehabiliteringsforum Danmark (2022).
71. Elman R. Aphasia centers and the life participation approach to aphasia: a paradigm shift. Top Lang Disorders (2016) 36:154–67. doi: 10.1097/TLD.0000000000000087
72. Avramović P, Rietdijk R, Kenny B, Power E, Togher L. Developing a digital health intervention for conversation skills after brain injury (convers-ABI-lity) using a collaborative approach: mixed methods study. J Med Internet Res (2023) 25:e45240. doi: 10.2196/45240
73. Behn N, Francis J, Togher L, Hatch E, Moss B, Hilari K. Description and effectiveness of communication partner training in TBI: a systematic review. J Head Trauma Rehabil (2021) 36:56–71. doi: 10.1097/HTR.0000000000000580
74. Simmons-Mackie N, Raymer A, Cherney LR. Communication partner training in aphasia: an updated systematic review. Arch Phys Med Rehabil (2016) 97:2202–21. doi: 10.1016/j.apmr.2016.03.023
75. Togher L, Wiseman-Hakes C, Douglas J, Stergiou-Kita M, Ponsford J, Teasell R, et al. INCOG Recommendations for management of cognition following traumatic brain injury, part IV: cognitive communication. J Head Trauma Rehabil (2014) 29:353–68. doi: 10.1097/HTR.0000000000000071
76. Wiseman-Hakes C, Ryu H, Lightfoot D, Kukreja G, Colantonio A, Matheson FI. Examining the efficacy of communication partner training for improving communication interactions and outcomes for individuals with traumatic brain injury: a systematic review. Arch Rehabil Res Clin Transl (2020) 2:100036. doi: 10.1016/j.arrct.2019.100036
77. Christensen I, Power E, Togher L, Brassel S, Elbourn E, Folder N, et al. Communication between rehabilitation staff and people with traumatic brain injury: a systematic review. Neuropsychol Rehabil (2023):1–39. doi: 10.1080/09602011.2023.2274625
78. Deegan PE. Recovery: the lived experience of rehabilitation. Psychosoc Rehabil J (1988) 11:11–9. doi: 10.1037/h0099565
79. Mattingly C. The narrative nature of clinical reasoning. Am J Occup Ther. (1991) 45:998–1005.1793123
80. Mattingly C. Acted narratives: from storytelling to emergent dramas. In: Clandinin DJ, editors. Handbook of Narrative Inquiry: Mapping a Methodology. Thousand Oaks (CA): Sage Publications, Inc. (2007). p. 405–25.
81. Mattingly C. Performance narratives in the clinical world. In: Hurwitz B, Greenhalgh T, Skultans V, editors. Narrative Research in Health and Illness. London: Blackwell Publishing (2004). p. 73–94.
82. Mattingly C. Healing Dramas and Clinical Plots. the Narrative Structure of Experience. Cambridge (UK): Cambridge University Press (1998).
83. Mattingly C. In search of the good: narrative reasoning in clinical practice. Med Anthropol Q (1998) 12:273–97. doi: 10.1525/maq.1998.12.3.273
84. Schrank B, Stanghellini G, Slade M. Hope in psychiatry: a review of the literature. Acta Psychiatr Scand (2008) 118:421–33. doi: 10.1111/j.1600-0447.2008.01271.x
85. Pompili M, Forte A, Palermo M, Stefani H, Lamis DA, Serafini G, et al. Suicide risk in multiple sclerosis: a systematic review of current literature. J Psychosom Res. (2012) 73:411–7. doi: 10.1016/j.jpsychores.2012.09.011
86. Soundy A, Smith B, Dawes H, Pall H, Gimbrere K, Ramsay J. Patient’s expression of hope and illness narratives in three neurological conditions: a meta-ethnography. Health Psychol Rev (2013) 7:177–201. doi: 10.1080/17437199.2011.568856
87. Blake J, Greenbaum H, Chan F. Attachment and employment outcomes for people with SCI, the intermediary role of hope. Rehabil Couns Bull (2017) 60:77–87. doi: 10.1177/0034355215621036
88. Chan JYC, Chan F, Ditchman N, Phillips B, Chou C. Evaluating snyders hope therapy as as a motivational model of participation and life satisfaction for individuals. Rehabil Res Policy Educ (2013) 27:171–85. doi: 10.1891/2168-6653.27.3.171
89. Rollnick S, Miller WR, Butler CC. Motivationssamtalen I Sundhedssektoren. Copenhagen: Hans Reitzels Forlag (2013).
90. Mattingly C. Den narrative udvikling i nyere medicinsk antropologi. Narrativer (2005) 2:13–40. doi: 10.7146/tfss.v2i2.460
91. Hall Z, Elbourn E, Togher L, Carragher M. Co-constructed communication therapy for individuals with acquired brain injury: a systematic review. Intl J Lang Comm Disor. (2022) 59:496–518. doi: 10.1111/1460-6984.12841
92. Candlish L, Fadyl JK, D’cruz K. Storytelling as an intervention in traumatic brain injury rehabilitation: a scoping review. Disabil Rehabil. (2022) 45:2248–62. doi: 10.1080/09638288.2022.2084778
93. Elbourn E, Brassel S, Steel J, Togher L. Perceptions of communication recovery following traumatic brain injury: a qualitative investigation across 2 years. Int J Lang Commun Disord (2022):1–20. doi: 10.1111/1460-6984.12795
94. Tonnesen M, Vinther C. Hope and haunting images: the imaginary in Danish Parkinson's disease rehabilitation. Med. Anthropol. Theory. (In press)
95. Levack WM, Weatherall M, Hay-Smith EJ, Dean SG, McPherson K, Siegert RJ. Goal setting and strategies to enhance goal pursuit for adults with acquired disability participating in rehabilitation. Cochrane Database Syst Rev (2015) 2015(7):CD009727. doi: 10.1002/14651858.CD009727.pub2
Keywords: hope, acquired brain injury, rehabilitation, recovery, literature review, qualitative studies, thematic synthesis
Citation: Højgaard Nejst C and Glintborg C (2024) Hope as experienced by people with acquired brain injury in a rehabilitation—or recovery process: a qualitative systematic review and thematic synthesis. Front. Rehabil. Sci. 5:1376895. doi: 10.3389/fresc.2024.1376895
Received: 26 January 2024; Accepted: 26 April 2024;
Published: 14 May 2024.
Edited by:
Brendan McCormack, The University of Sydney, AustraliaReviewed by:
Andrew Soundy, University of Birmingham, United KingdomMelissa Kendall, Metro South Health, Australia
© 2024 Højgaard Nejst and Glintborg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Camilla Højgaard Nejst, Y2FtaWxsYWhuQGlrcC5hYXUuZGs=