The use of virtual technologies with music in rehabilitation: a scoping systematic review
 Pipsa P. A. Tuominen1*†
Pipsa P. A. Tuominen1*†  Lea A. Saarni2†
Lea A. Saarni2†- 1Social Services and Health Care, Tampere University of Applied Sciences, Tampere, Finland
- 2Applied Research Center, Tampere University of Applied Sciences, Tampere, Finland
Introduction: The use of virtual environments in rehabilitation has been growing. The current systematic review aimed to evaluate how and where virtual technologies are combined with music in rehabilitation.
Methods: A literature search was conducted in seven databases (ACM Digital Library, CINAHL Complete, Cochrane Library, Computer Science database, Medline, Nursing & Allied Health database, and Scopus). It included articles published from 2006 to February 2023. The search followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for study selection. Twelve studies with 160 participants were included in the review. In addition, a descriptive approach was used to gather data from the studies for the areas of interest.
Results: Virtual Reality (VR) and Augmented Reality were most familiar and used in rehabilitation, but Mixed Reality, and Extended Reality were less studied. It became evident that equipment, diverse applications, assessment metrics, training environments, and methodologies were highly varied. Most of the studies were pilots, the overall quality of included studies was rated moderate, and the risk of bias was high in the included studies. The studies on motor rehabilitation after stroke showed a clinical improvement in hand functions, specifically fractionation. Furthermore, studies that included motivation, adherence, and mental health, slightly supported the idea that VR technologies with music have the potential to promote motivation and exercise adherence, increase positive emotions, and decrease anxiety. In addition, user experience and feasibility studies presented technologies combined with music to be safe and acceptable in rehabilitation.
Discussion: In light of these findings, it can be inferred that virtual technologies with music offer promising avenues for future rehabilitation research. However, some confusion was obtained related to the included studies’ definitions of technologies and management terms. Furthermore, it is important to note the limited number of studies and participants, the heterogeneity among participants, and the overall quality of the studies that restrict the generalizability of these results to a larger population. Therefore, future researchers should define concepts and terms, delve deeper into this area to uncover the potential benefits, and clarify the specific mechanisms through which virtual technologies with music can positively impact rehabilitation outcomes.
1 Introduction
1.1 Background for virtual reality
The use of virtual environments in rehabilitation has been growing. The definition of virtual reality (VR) is extensive. According to the following descriptions, it can be used as a generic term or as a specifically defined concept. Virtual reality is a computer-human interface that allows users to interact with computers that generate virtual environments where the users can perform different tasks in real-time. Virtual technologies could be divided into non-immersive and immersive VR. Non-immersive VR setups are usually based on a combination of a computer or video game console, a screen, and various input devices such as keyboards, mice, and controllers. These technologies are also commonly used in everyday life (Ventura et al., 2019). An immersive VR refers to a system that allows users to perceive the environment through the natural interaction between sensory inputs and motor responses (Slater and Sanchez-Vives, 2016). Users need the proper VR glasses or a head mount display (HMD) for immersive VR. The simulation experience uses both sight (visual) and sound (audio) and sometimes tactile (haptic) means to create a real-like, believable environment (Ventura et al., 2019). Further, Slater et al. (2016) define immersive VR as including remote communication and collaboration (Slater and Sanchez-Vives, 2016).
Immersive technology uses computer-generated simulation to give a sense of immersion. Immersive VR allows users to engage in digitally alternated or synthesized realities (Snoswell and Snoswell, 2019). In VR, two different elements can be utilized: the virtual environment and the virtual world. Virtual environments use 2D/3D settings, including characters and objects that users can see, hear, and interact with realistically in real-time. The virtual world is a constant and social world where users can interact with other users using an artificial avatar (Morie and Chance, 2011; Triberti and Chirico, 2016). Non-immersive VR systems display a virtual environment to the user on a computer or mobile phone display without head tracking (Snoswell and Snoswell, 2019).
Technically accurate and stable tracking of the user’s head and possibly body motions, low latency updating of the visual image provided to the user, a high display resolution, and a wide field of view help to achieve a sense of presence. Varied levels of immersion can be achieved by using computer or television screens and head-mounted devices, such as helmets or glasses. Some of these are supplemented by floor-supported displays, panoramic projections, and/or virtual tables or a CAVE to improve the immersion experience (Snoswell and Snoswell, 2019). Immersive VR systems can also integrate with other sensors and input modalities, such as eye tracking (Gerber et al., 2017) or brain-computer interfaces (Amaral et al., 2017).
In the current context, VR allows users to interact with a multisensory simulated environment and receive real-time feedback on performance (Saposnik and Levin, 2011). The virtual environment can be controlled and manipulated in advance, allowing pre-determined scenarios and specific exercises to be defined for individual needs (Pareto et al., 2016). VR involves the user in the virtual environment, but Augmented Reality (AR) displays virtual images (Xiong et al., 2021), text, sound, and graphics in the user’s natural visual and auditory fields (Wong et al., 2018). In their narrative review, Gorman and Gustafsson (2020) concluded that no clear definition of AR was established, and some confusion between VR and AR was noticed (Gorman and Gustafsson, 2020).
Mubin et al. (2019) described how users had a more realistic feel when they received more control over virtual objects by interacting with real objects (Mubin et al., 2019). VR applications for rehabilitation addressed the combination of motor and cognitive training and also focused on motivational issues. The growing evidence has shown that virtual technologies have several health-exchanging possibilities for rehabilitation. Studies concerning the benefits of VR treatment for motor function after stroke have reported promising results (Saposnik and Levin, 2011). Rodríguez-Hernández et al. (2021) showed that VR was more effective than traditional rehabilitation methods in improving stroke patients’ quality of life (Rodríguez-Hernández et al., 2021).
VR is an effective treatment for reducing the intensity of feelings related to mental health, such as anxiety and depression (Freeman et al., 2017; Ioannou et al., 2020), pain management (Benham et al., 2019; Ioannou et al., 2020), physical rehabilitation (Vourvopoulos et al., 2019), and fatigue (Ioannou et al., 2020). AR and gaming control interfaces reduced pain with chronic phantom upper limb pain sufferers in long-term follow-up (Ortiz-Catalan et al., 2016). In their systematic review, Xie et al. (2021) found that in-clinic and at-home VR-based vestibular rehabilitation benefited patients (Xie et al., 2021). Concerning stroke rehabilitation, Yang et al. (2022) presented significant improvement in the upper and lower extremity motor function, balance, and quality of life while using AR training as an extension of the human trainers (Yang et al., 2022). Additionally, Zhu et al. (2023) reported that rehabilitation robots plus VR had an advantage over other interventions in improving upper limb motor function amongst subjects with stroke (Zhu et al., 2023). Therefore, rehabilitation robots plus VR, intelligent rehabilitation, and Brain-Computer Interface techniques can be recommended as the preferred treatment method for upper limb functional rehabilitation in subjects with stroke.
The AR glasses platform connected remotely to healthcare providers gave the opportunity to follow patients and empower them to cope with their diseases (Cerdán de las Heras et al., 2022).
According to Rauschnabel et al. (2022), there was a need to update the definition of the term Extended Reality (XR) (Rauschnabel et al., 2022). They concluded that “1) XR should not be used to connote extended reality, but as a more open approach where the X implies the unknown variable: xReality; 2) AR and VR have fundamental differences and thus should be treated as different experiences; 3) AR experiences can be described on a continuum ranging from assisted reality to mixed reality (based on the level of local presence); and 4), VR experiences can be conceptualized on a telepresence-continuum ranging from atomistic to holistic VR”. Therefore, they proposed to use XR as an abbreviation for xReality; the variable x serves as a placeholder for Augmented, Assisted, Mixed, Virtual, Atomistic Virtual, Holistic Virtual, or Diminished Reality (Rauschnabel et al., 2022).
1.2 Background for music in rehabilitation
Using music in exercise, sports, and rehabilitation has numerous scientifically documented health benefits (Barwood et al., 2009; Hutchinson et al., 2015; Clark et al., 2016; Karageorghis and Karageorghis, 2016; Terry et al., 2019). A piece of music can seem like a relatively simple stimulus with a number of elements, such as rhythm, tempo, melody, harmony, meter, timbre, and dynamics, and in some cases lyrics as well (Karageorghis and Karageorghis, 2016). Karageorghis (2016) stated that there are three primary types of musical effects to be explored, including psychological, psychophysical, and ergogenic effects (Karageorghis and Karageorghis, 2016). The use of music, specifically listening, has been found to provide motor control (Sihvonen et al., 2017; Pereira et al., 2019; Lopes and Keppers, 2021), gait parameters (Weller and Baker, 2011; Pereira et al., 2019), cognitive abilities (Sihvonen et al., 2017), pain (Lopes and Keppers, 2021), and quality of life (Pereira et al., 2019) in several diseases. Further, motivation and adherence to exercise have been found to increase (Barwood et al., 2009; Weller and Baker, 2011; Hutchinson et al., 2015; Clark et al., 2016). Thus, music-based therapies, such as rhythmic stimulation and dance, have been found to be better than conventional therapy or no intervention (Pereira et al., 2019).
As a conceptual framework for predicting responses to motivational music has been presented, music’s motivational qualities led to psychophysical effects, such as regulating arousal control, reducing rates of perceived exertion, and improving mood (Karageorghis et al., 1999; Karageorghis and Priest, 2012). Also, it was found that there was greater work output, an improvement in skill acquisition and flow state (Terry and Karageorghis, 2006; Priest and Karageorghis, 2008; Karageorghis and Priest, 2012), as well as improving other health outcomes (Murrock and Higgins, 2009). Since structured exercises that are provided regularly increase both the amount and intensity of physical activity, listening to music could promote behavioral change that is also needed in rehabilitation through increased exercise adherence and participation (Clark et al., 2016).
Research on singing and rehabilitation has mainly been reported among the adult and elderly populations with chronic illnesses, such as Alzheimer’s disease and Dementia (Young et al., 2016; Särkämö, 2018), Parkinson’s disease (Barnish et al., 2016; Barnish and Barran, 2020), and COPD (McNamara et al., 2017; Fang et al., 2022), just a few to mention. Positive responses related to physical health, for example, the function of respiratory muscles, have been reported (McNamara et al., 2017; Fang et al., 2022), as well as improved quality of life (Särkämö, 2018; Fang et al., 2022) and positive effects on cognition (Barnish and Barran, 2020), specifically among people with mild to moderate dementia (Särkämö, 2018). In addition, musical activities such as singing have multiple psychosocial benefits and musical activities have been found to be enjoyable and to maintain participants’ attentiveness (Young et al., 2016; Särkämö, 2018), even when no changes in cognitive functions were observed (Young et al., 2016).
Playing a musical instrument in association with the training of hand motor function with integrated auditory, visual, and tactile feedback is a process that recruits multiple brain regions (Alves-Pinto et al., 2016). Playing an instrument as a part of rehabilitation has been focused on upper limb rehabilitation after a stroke (McIntyre et al., 2016) and in Cerebral Palsy (Alves-Pinto et al., 2016), as well as respiratory function in patients with neurological conditions (Ang et al., 2017). In addition, playing an instrument can promote sensorimotor interactions required for motor rehabilitation (Alves-Pinto et al., 2016). Playing, for example, MIDI virtual piano or other keyboards, an electronic drum set, other percussion instruments, or even wind instruments has been found as an effective method of upper limb rehabilitation (Alves-Pinto et al., 2016; McIntyre et al., 2016) and a trend toward improved respiratory function in rehabilitation (Ang et al., 2017).
1.3 Impact of audiovisual techniques and VR in rehabilitation
Less is known about where and how the virtual technologies and music combined could be used and do they influence rehabilitation progress. Earlier studies have shown that audiovisual elements could shift attention from an internal stimulus, such as physical sensations, to external cues, such as music or movies (Barwood et al., 2009; Hutchinson et al., 2015). Gibbs, Gillies, and Pan (2022) summarize that visual and auditory feedback is predominating (Gibbs et al., 2022). However, increasing attention is paid to haptics, while other modalities have remained in the experimental stage (Gibbs et al., 2022). Naef et al. (2022) found that participants were objectively more relaxed after receiving audiovisual and auditory input when comparing independent auditory or visual inputs or no artificial sensory input at all (Naef et al., 2022). Additionally, the participants reported being less aware of their surroundings compared to receiving only a single input (Naef et al., 2022). Also, Gerber, Jeitziner, Wyss, et al. (2017) showed that VR stimulation had a relaxing effect, as shown in vital markers of physical stress. Their study indicated that an HMD-based VR setup using visual and acoustic stimulation is feasible and has great potential for critically ill patients in the Intensive Care Unit (Gerber et al., 2017).
Dance games and other exergames (i.e., active video games) allowed the participant to interact with the platform by performing movements in front of the screen. This kind of exercise has been found to positively affect physical activity and behavioral change toward a healthier lifestyle, for example, in cardiac rehabilitation (Ruivo, 2014), Parkinson’s disease (Garcia-Agundez et al., 2019), and neurocognitive disorders (Swinnen et al., 2022), and be feasible and safe in these populations. Even though dance games and other exergames are widely studied in the context of rehabilitation, combining music with virtual technologies and visual or tactile elements is shrouded in obscurity. Further, all these games could not be defined as VR (Slater and Sanchez-Vives, 2016; Ventura et al., 2019). Based on our experience, the use of music has yet to be defined or demonstrated adequately in earlier VR studies. Similarly, virtual, visual, or tactile elements could be better described in music studies.
As we like to broadly define it, music in virtual environments can include a wide range of elements such as sounds, samples, effects, and different genres, tracks, and pieces from low-latency audio alongside a separate video image (for example, in video conferencing platforms) up to full 360° audio-visual immersion (a real-life-like perspective with high-quality interactive content). However, there is a lack of knowledge about the possibilities for combining music and virtual technologies for rehabilitation. Thus, the objectives of the current review were to evaluate where and how these technologies are combined with music and whether they influence the rehabilitation progress.
2 Materials and methods
2.1 Aims and objectives
The aim of the current scoping systematic review was to compile and integrate the existing body of literature related to virtual technologies, music, and rehabilitation. The current research question and subquestions are developed according to the recommended format “PCC” (Population, Concept, and Context) mnemonic, such as described in Pollock et al. (2021) (Pollock et al., 2021).
Our primary research question is: What evidence is available about with whom and how virtual technologies and music combined could be used for rehabilitation purposes?
As part of our objectives, we aimed to explore the scientific literature that combines these areas by gathering the research aims, scope, methodological approaches, and with whom and how the virtual technologies and music combined could be used and do they influence rehabilitation progress.
Our subquestions are:
1) What kind of virtual technologies are developed and used with music in rehabilitation processes?
2) Which groups of patients can benefit from this type of rehabilitation?
Answers to these questions will not only enable researchers and practitioners, but also designers to develop virtual technologies and use those with music in rehabilitation settings. We focused on virtual technologies in general and music as widely defined in rehabilitation context by scoping the written literature.
2.2 Design
In light of the above aims and objectives, we employed a scoping systematic review. According to Arksey and O’Malley (2005), the scoping review process includes the following five stages: identifying the research question, identifying the relevant studies, study selection, charting the data, and collating, summarizing, and reporting the results (Arksey and O’Malley, 2005). To this end, we utilized a methodical search to survey the literature and offered a comprehensive synthesis. The overarching objective was to chart the literature related to a specific topic or research area, enabling the identification of key concepts, research gaps, and various types and sources of evidence that could inform development, practice, and further research.
2.3 Information sources and search strategy
This systematic review followed the recommendations of the PRISMA statement (Page et al., 2021). A search from an electronic database was conducted from inception to February 2023 on the following databases: ACM Digital library, CINAHL Complete (Ebsco), Cochrane Library, Computer science database (ProQuest Central), Medline (Ovid/Ebsco), Nursing & allied health database (ProQuest Central), and Scopus (Elsevier). In the search, Medical Subject Headings (MeSH) and related terms used in the Title, Abstract, or Keywords, or in NOFT (anywhere except full text) were searched (Table 1). Manual searches of the reference list of related reviews, protocols, and conference publications accompanied the database searches.
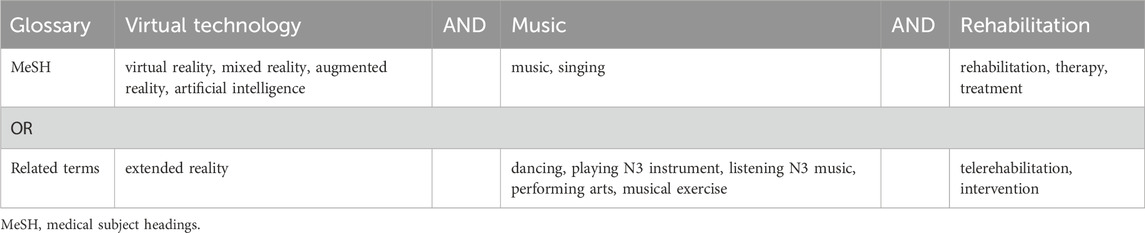
Table 1. The terms used in the search.
The search was limited to articles in English that were published in scholarly, peer-reviewed journals. In addition, the full text of the article had to be available.
2.4 Eligibility criteria and selection process
Studies which were included based on the following criteria:
(1) The study focused on adolescents or adults and older adults.
(2) The study was related to both music and VR, AR, XR, MR, or AI.
(3) The outcome was related to rehabilitation.
(4) The study was empirical or theoretical.
(5) The study fulfills the criteria above, identified via Conference abstracts, publications, or books.
(6) The study fulfills the criteria above, identified via study protocol or review.
Studies were excluded with the following criterion:
(1) The study focused on children under 10 years or animals.
(2) The study was related only to music or VR, AR, XR, MR, or AI.
(3) The outcome did not have a connection to rehabilitation.
(4) The study was for validation.
(5) The study was a review.
One researcher (PPAT) undertook the search. Next, two independent researchers (LS, PPAT) screened each record (title and abstract) and discussed inconsistencies until a consensus was obtained for further screening. Then, the researchers independently reviewed full-text articles for inclusion. Again, inconsistencies were discussed until a consensus was obtained. Finally, articles outside our domain’s scope that did not meet our criteria were excluded.
For further articles, references were checked from excluded protocols, conference publications, reviews, and book chapters. In addition, studies were identified via reported results of published protocols and personal contacts. The procedure for the identification of studies is presented in Figure 1.

Figure 1. The PRISMA Flow Chart presents the procedure for identifying studies.
2.5 The quality assessment
The quality assessment was based on a critical appraisal of studies using the model created by Hoy et al. (2012) (Hoy et al., 2012). The quality assessment relies on the selected studies’ external (four items) and internal qualities (six items). For assessing the quality of selected studies, the following data were extracted from the included articles: representation of the national population, sampling frame, use of random selection, the bias of nonresponse, data collection directly from subjects, case definition, validity and reliability of measurement instruments, mode of data collection, the length of prevalence period, and appropriation of parameters of interests.
The Cochrane Collaboration description (Higgins et al., 2011) was not used to assess the quality of selected studies since none were RCTs.
3 Results
3.1 Study characteristics and risk of bias in studies
We identified 12 eligible studies based on our criteria, including five studies in Europe, four in the USA, and one each from Australia, Brazil, and Taiwan (Table 2). The total sample of studies included 160 participants. None of the studies were related to AI, and thus, not discussed further. Table 2 summarizes the studies included in this review, presenting their aims, target groups, design, data collection, and metrics used. Further, Table 2 also highlights the main results and Table 3 the overall quality of the studies.

Table 2. Summary of studies investigating music- and VR/AR/MR/XR-technology-based interventions in rehabilitation.
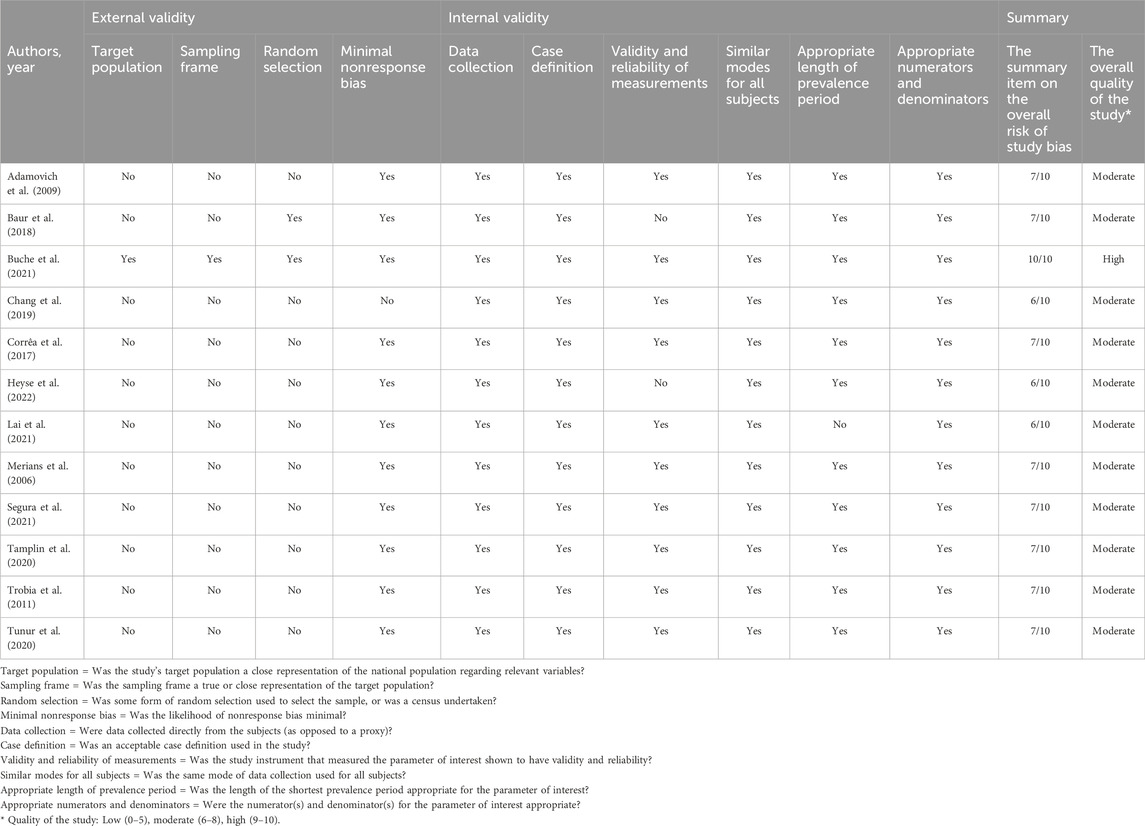
Table 3. External and internal validity of the selected studies and risk of bias.
Altogether six studies were quantitative (Adamovich et al., 2009; Trobia et al., 2011; Baur et al., 2018; Chang et al., 2019; Buche et al., 2021; Segura et al., 2021). In addition, six studies had both quantitative and qualitative approaches (Merians et al., 2006; Corrêa et al., 2017; Tamplin et al., 2020; Tunur et al., 2020; Lai et al., 2021; Heyse et al., 2022).
Unfortunately, most of the studies were in the form of pilot studies, with only a few participants (ranging from 2 to 52). The participants of case studies did not necessarily represent the target population properly, and the small number of participants prevented the generalization of the results to the national population. Further, the risk for selection bias, i.e., selecting individuals or groups for analysis from small and deviant populations, was high. The detection bias was also high since only three studies (Chang et al., 2019; Segura et al., 2021; Heyse et al., 2022) had separate intervention and control groups, and one study (Buche et al., 2021) had a randomized order of different conditions. Attrition bias, as selective dropout, was not reported in these studies. The afore-mentioned reasons set the external validity of studies as low.
The internal quality of the studies was mainly good. However, due to the nature of developing processes for rehabilitation, instruments used to measure the parameters of interest were not necessarily validated. In addition, all the studies reported at least some positive effects among participants or in their technological development processes. Table 3 summarizes the external and internal validity of the selected studies and the risk of bias.
3.2 The use of virtual technologies
Six studies were related to VR technologies (Merians et al., 2006; Trobia et al., 2011; Tamplin et al., 2020; Buche et al., 2021; Lai et al., 2021; Heyse et al., 2022), and further one with the music-supported app (Segura et al., 2021). In addition, two studies reported using robotic or robot-assisted training (Adamovich et al., 2009; Baur et al., 2018), two studies were related with AR (Corrêa et al., 2017; Tunur et al., 2020), and one with MR (Chang et al., 2019). Immersive VR technologies were used in seven studies (Corrêa et al., 2017; Chang et al., 2019; Tamplin et al., 2020; Tunur et al., 2020; Buche et al., 2021; Lai et al., 2021; Heyse et al., 2022) and non-immersive VR technologies in five studies (Merians et al., 2006; Adamovich et al., 2009; Trobia et al., 2011; Baur et al., 2018; Segura et al., 2021).
3.2.1 Immersive VR technologies
In the Buche et al. (2021) study, an Oculus Go R headset included a remote control that allowed navigation in the virtual world and an accessory allowing the helmet to be worn with glasses (Buche et al., 2021). This device was entirely autonomous. Unlike other VR systems, it did not require a computer or game console. Lai et al. (2021) underwent VR gaming sessions as part of the early mobilization care, using an Oculus Rift head-mounted display and adaptive software (WalkinVR) that promoted complete gameplay in bed (Lai et al., 2021). Additionally, Tamplin et al. (2020) tested Gear VR headsets and vTime, a social VR application that allows up to four users to meet in a private virtual environment (Tamplin et al., 2020). They assisted participants in entering VR via the app, selecting their avatar and virtual location, and singing together with the music therapist in VR.
Heyse et al. (2022) studied Musical Neglect Therapy, a therapy method that incorporated multiple modalities by asking patients to make music (Heyse et al., 2022). They translated Musical Neglect Therapy into a VR therapy tool. The designed VR therapy tool for Unilateral Spatial Neglect consisted of two modules: the VR therapy module, for the patient, who had to wear a head-mounted display and use controllers and the dashboard, accessible on a computer, where the therapist can control and oversee the session.
Among these studies, AR was less used, but in the study of Corrêa et al. (2017), they tested AR musical software (GenVirtual) (Corrêa et al., 2017). Software is a technology that needs a computer and webcam, allowing users to develop music activities for rehabilitation. GenVirtual adds 3D musical elements into the real world. Using these virtual objects, it is possible to play the sounds of musical instruments, such as stringed (guitar, piano, and violin), wind (flute), and percussion instruments (drum). Further, in the study by Tunur et al. (2020) participants with Parkinson’s disease used AR glasses (Google Glass, defaulted to an offline environment) and the Moving Through Dance modules with different tempo options (Tunur et al., 2020). In addition, Google Glass superimposes Moving Through Dance videos of various exercises (Tunur et al., 2020).
Finally, Chang et al. (2019) studied a mixed reality music rehabilitation (MR2) system where participants interacted with the hologram music rehabilitation contents through the MR glasses, HoloLens (Chang et al., 2019).
3.2.2 Non-immersive VR technologies
Merians et al. (2006) tested a computerized VR system, two instrumented gloves, an 18-sensor CyberGlove, and the Rutgers Master II-ND force feedback prototype glove (Merians et al., 2006). Range of motion, speed of movement, and fractionation (a measure of independent finger motion) exercises were performed using the CyberGlove, whereas the strengthening exercise used the Rutgers Master II glove.
In the study by Trobia et al. (2011), patients observed the virtual movements displayed on the VR Mirror while listening to music pieces to support performing mental practice (Trobia et al., 2011). Also, VR and music-supported therapy app with a MIDI piano and percussion instruments was studied by Segura et al. (2021) (Segura et al., 2021).
Furthermore, robotic and virtual piano training was used as a part of rehabilitation. The Virtual Piano Trainer is a complex simulation intended to train individual finger motion that provides realistic auditory and visual feedback of appropriate piano notes, sounds, and music and combines them in the study by Adamovich et al. (2009) (Adamovich et al., 2009). Baur et al. (2018) used ARMin, an exoskeleton robot, for arm therapy of patients with neurological disease (Baur et al., 2018). The ARMin system recorded the total training time, free movement time, i.e., final phase duration, and root-mean-square of the end effector velocity profile. The interaction between the robot and the subject is transferred by cuffs at the upper arm, lower arm, and hand module.
3.3 The role and diversity of music
Using music as a part of rehabilitation included listening to music, playing piano or other instruments, and singing. Piano playing was used in three studies (Merians et al., 2006; Adamovich et al., 2009; Segura et al., 2021), playing different musical instruments (such as strings, wind, and percussion) were used in three studies (Corrêa et al., 2017; Segura et al., 2021; Heyse et al., 2022), and further, singing was used in one study (Tamplin et al., 2020). Listening to music during the task was used in six studies (Trobia et al., 2011; Baur et al., 2018; Chang et al., 2019; Tunur et al., 2020; Buche et al., 2021; Lai et al., 2021).
Examples of music, genres, or pieces used were mentioned in one study (Tamplin et al., 2020). Tamplin et al. (2020) used popular and familiar songs for singing, such as “Knocking on Heaven’s Door” by Bob Dylan, “Buffalo Soldier” by Bob Marley, and “Let it Be” by The Beatles, in the immersive VR environment (Tamplin et al., 2020). Different kind music, songs, or scales were used in eight studies (Merians et al., 2006; Adamovich et al., 2009; Trobia et al., 2011; Chang et al., 2019; Tunur et al., 2020; Lai et al., 2021; Segura et al., 2021; Heyse et al., 2022). Relaxing sounds or other samples and effects were mentioned in three studies (Corrêa et al., 2017; Baur et al., 2018; Buche et al., 2021). The idea of why and how music was used in the mentioned studies can be described as follows.
3.3.1 Rhythm of the movement
Chang et al. (2019) implemented several music contents into their immersive MR system (Chang et al., 2019). Participants were instructed to follow the tempo of the music while walking and playing the MR music game. However, the music used was not described. Nevertheless, improvements in the flexion angle of the hemiplegic knee were reported when the music tempo was followed.
Lai et al. (2021) used different VR gaming sessions, and participants could choose an active game with rhythmic movement to music (Beat Saber by Beat Games), among other exergame possibilities (Lai et al., 2021). However, the role and diversity of music were not described further. Participants were reported to increase their upper extremities’ range of motion during the game.
Further, Trobia et al. (2011) extended the non-immersive VR mirror display by adding music for exercise sessions, arguing that music could support mental practice (Trobia et al., 2011). They selected music to support the movement of the upper limbs with rhythm and tempo, associate with positive emotional states, and be familiar to participants. However, the selection of music was not described further. Nevertheless, the results of two patients showed promising increases in motor scores and improvements in activities of daily living.
In addition, Tunur et al. (2020) evaluated a mobile dance intervention using Moving Through Glass applications for Google Glasses (Tunur et al., 2020). Music with the possibility to adjust tempo was played in all four included modules (warm-up, balance, unfreeze, and walk). However, similarly to other studies, the music used was not described.
3.3.2 Feedback for rehabilitation from exercises
Adamovich et al. (2009) used a simulated piano system that presented visual, auditory, and tactile feedback for the participants, including exercises that could be performed with one or both hands (Adamovich et al., 2009). In addition, the piano system included a full keyboard and an algorithm-adjusted task difficulty for each participant. Furthermore, configurations of the scales and songs were listened to, and each note, current key, and the corresponding finger were shown before the participant started to play. Also, Merians et al. (2006) used virtual piano playing to train the ability to move each finger independently (Merians et al., 2006). These two experiments showed improvement with finger fractionation and other functions of hands and arms.
Heyse et al. (2022) used the adjustable virtual xylophone in four tasks (Heyse et al., 2022). Playing was used to assess the severity of participants’ neglect, and scales, memory, and free-to-play were used to help participants respond to triggers in their environment by changing the number and locations of keys. In addition, gamified elements were used, such as falling balls, the possibility to correct mistakes, and positive feedback. All the tasks had several difficulty levels. Furthermore, their results indicated that the tasks were challenging enough, and participants showed to adjust their head direction increasingly, and their enjoyment related to rehabilitation increased (Heyse et al., 2022).
Baur et al. (2018) described their game environment where the idea was to promote or not promote creativity, with similar sound samples in all conditions by participants’ selection (Baur et al., 2018). In their study, the sound samples and the modulators were designed to play simultaneously, and instrumental sounds were planned to give feedback about the participant’s position in the game. They found that conditions promoting creativity with or without visual display were preferred compared to those that did not and that increased interest and enjoyment (Baur et al., 2018).
3.3.3 Shifting attention, exercise adherence, and social aspects
In a range of different conditions, Buche et al. (2021) used relaxing sounds with visual environments and “Spring” from Four Seasons by Vivaldi (Buche et al., 2021). They intended to find which method might shift attention during the scar massage sessions. All the methods increased positive emotions and decreased anxiety; thus, differences between the conditions were not found.
Segura et al. (2021) organized non-immersive training sessions with the app to warm up with the percussion instruments for the upper limb and the MIDI-piano to train fine motor skills (Segura et al., 2021). Participants were asked to play percussion instruments, such as tambourine, tambourine with beater, djembe, maracas, egg shaker, rain stick, castanets, and guiro, with a specific tempo for improving gross motor skills. The piano exercises were classified into different difficulty levels, including the sequence presentation and the hand and fingers used. Red marks were used to inform participants of the mistakes, and further possibility for self-correction was used. Furthermore, as feedback, a scoring system was used to motivate participants to exercise further. As a result, participants clinically improved their upper limb motor functions (Segura et al., 2021).
Corrêa et al. (2017) tested immersive AR musical software that was expected to restore or improve motor functions and cognitive skills using recreation activities, reproduction, imitation, listening games, and rhythmic games (Corrêa et al., 2017). Different virtual objects offered possibilities to play sounds of several instruments, such as guitar, piano, violin, flute, and drum, using musical symbol cards. Increased motivation among participants facilitated therapeutic processes, and the tool used in a multidisciplinary way with different goals was found as an important strategy of the system (Corrêa et al., 2017).
Tamplin et al. (2020) tested the group-singing approach online for spinal cord injured people, and participants’ experiences of the equipment and online singing trials were collected (Tamplin et al., 2020). The group-singing combined with immersive VR was a positive experience and reduced inhibitions about singing with others and social cues.
3.4 Result of individual studies in rehabilitation
Most of the included studies investigated rehabilitation after a stroke or acquired brain injury (Merians et al., 2006; Adamovich et al., 2009; Trobia et al., 2011; Chang et al., 2019; Segura et al., 2021; Heyse et al., 2022), one related to breast cancer (Buche et al., 2021), intensive care unit patients (Lai et al., 2021), spinal cord injury patients (Tamplin et al., 2020), and Parkinson’s disease (Tunur et al., 2020). Also, healthy individuals were included in five studies as participants (Corrêa et al., 2017; Baur et al., 2018) or controls (Chang et al., 2019; Segura et al., 2021; Heyse et al., 2022).
3.4.1 Motor rehabilitation after a stroke and in Parkinson’s disease
Studies of rehabilitation after a stroke or acquired brain injury reported results of upper extremity function (Merians et al., 2006; Adamovich et al., 2009; Trobia et al., 2011; Segura et al., 2021), unilateral spatial neglect (Heyse et al., 2022), and measurements related to gait analysis (Chang et al., 2019). Further, one study reported gait analysis results in Parkinson’s disease (Tunur et al., 2020).
Adamovich et al. (2009) studied the concurrent validity of robotically measured kinematic and performance measures to behavioral measures of upper extremity function (n = 4) (Adamovich et al., 2009). They found that three of the four subjects demonstrated improvements in fractionation, i.e., the ability to move each finger individually. In addition, two subjects improved their aggregate time on the Jebsen Test of Hand Function and three of the four on the Wolf Motor Function Test (Adamovich et al., 2009). Similarly, Merians et al. (2006) reported improvements in the Jebsen Test of Hand Function in their study of computerized VR training on hemiparetic hand function with post-stroke patients in the chronic phase (n = 8) (Merians et al., 2006). In addition, subjects improved in fractionation, thumb and finger range of motion, and speed (Merians et al., 2006).
Segura et al. (2021) also studied the functionality of the paretic upper extremity measured with the Action Research Arm Test (Segura et al., 2021). They found that patients (n = 5) clinically improved in upper limb motor function, such as grasp, grip, pinch, and gross movement. In addition, Trobia et al. (2011) reported sensible or moderate improvement in the upper limb motor function of hemiplegic patients (n = 2) using a VR mirror with the accompanying music tracks (Trobia et al., 2011). Both patients showed increased motor scores and reported an improvement in activities of daily living.
Heyse et al. (2022) reported using VR musical instrument playing in unilateral spatial neglect rehabilitation with four patients and four controls (n = 8) (Heyse et al., 2022). Measurements showed that reaction times and the number of mistakes differed between patients and controls. However, during 2-weeks of intervention, patients increased time on the neglected side of the body, and exercises triggered them to use the whole environment. Patients also corrected their head position toward their neglected side (Heyse et al., 2022).
The study by Chang et al. (2019) included two stroke patients and three healthy controls (Chang et al., 2019). Measurements such as gait analysis using real-time streaming by the inertial measurement unit sensors -based wearable motion capture device (Notch) during the standing-walking-resting procedure with the MR music showed significant activation of motor function. It also showed significant improvement in the flexion angle of the hemiplegic knee during walking when following the tempo of the music (Chang et al., 2019).
Further, gait among patients with Parkinson’s disease was studied by Tunur et al. (2020). Patients with Parkinson’s disease (n = 7) used an AR mobile dance intervention for 3 weeks. Changes in balance and mobility were evaluated before and after the intervention, and improved mobility was found. However, there were no significant changes in the participants’ balance (Tunur et al., 2020).
3.4.2 Motivation, psychological, and cognitive factors in rehabilitation
Baur et al. (2018) assessed the effects of creativity and visual display on motivation in robot-assisted motor training among healthy young adults (n = 16) (Baur et al., 2018). Their principal findings showed that promoting creativity significantly increased interest/enjoyment and perceived choice in the Intrinsic Motivation Inventory scale. They also concluded that promoting creativity in a visual-audio-haptic or audio-haptic environment increased motivation in robot-assisted therapy. Corrêa et al. (2017) also studied healthy adults, in this case, health professionals (such as music, occupational, and physiotherapists, and speech and language therapists; n = 19) who worked with patients with physical and cognitive disabilities (Corrêa et al., 2017). Based on the perceptions of health professionals, they found that AR musical software has great potential for motor and cognitive rehabilitation in children and adults (Corrêa et al., 2017).
Buche et al. (2021) studied the benefits of VR use during scar massage sessions among breast cancer patients (n = 52) (Buche et al., 2021). They assessed four experimental conditions in random order, including participatory virtual immersion, contemplative virtual immersion, music listening, and standard care. An increase in positive emotions (i.e., joy and happiness) and a decrease in anxiety, regardless of which support methods were offered. They also found that participatory VR created a feeling of more intense spatial presence. Further, Trobia et al. (2011), who combined music and VR to support stroke patients (n = 2), outlined that both patients reported reduced anxiety after 4 weeks (Trobia et al., 2011).
Among intensive care unit patients, Lai et al. (2021) reported that two patients whose health and symptoms fluctuated could perform active VR gaming using a head-mounted display at moderate exercise intensity, as indicated by their heart rate (Lai et al., 2021). In addition, VR gaming was found to improve participants’ affect and alertness and motivate them to be more engaged in early mobilization therapy.
Furthermore, Tunur et al. (2020) reported that patients with Parkinson’s disease (n = 7) had no significant mood and quality of life changes in the 3-week intervention using AR mobile dancing (Tunur et al., 2020).
3.4.3 User experiences and feasibility of studies
Concerning the feasibility of combining music and VR, Trobia et al. (2011) concluded that those can be successfully integrated into mental practice protocols in stroke rehabilitation (Trobia et al., 2011). Also, Segura et al. (2021) concluded that a music-supported therapy program at home could be a feasible intervention for patients with chronic stroke (Segura et al., 2021). They studied the app usability and feasibility of a home-based enriched music-supported therapy program and reported that patients felt competent completing the intervention. Patients also felt comfortable playing both midi-piano and percussion instruments.
Corrêa et al. (2017) recommended AR musical software as a complementary tool to conventional clinical practice for children and adults with physical and cognitive disabilities (Corrêa et al., 2017). Also, AR mobile dancing was found to have a high retention and adherence rate and be safe and acceptable by participants with Parkinson’s disease (Tunur et al., 2020).
Baur et al. (2018) demonstrated a visual-audio-haptic music creation task as a feasible intervention and recommended trying the robotic system on patients with neuromuscular disorders (Baur et al., 2018). Further, Heyse et al. (2022) reported that applying musical neglect therapy with auditory, visual, and motor sensory modalities in VR showed promising results (Heyse et al., 2022). Patients also stated that using the tool increased their enjoyment of the therapy.
Tamplin et al. (2020) developed a low-latency telehealth solution for real-time group singing therapy for patients with spinal cord injuries (Tamplin et al., 2020). They were interested in user experience, as well as the acceptability and feasibility of the software. The thematic analysis of validated questionnaire results revealed five themes: VR was a positive experience, it was immersive and transportive, it reduced inhibitions about singing in front of others, and it may reduce social cues. Further, they found that VR equipment was comfortable, accessible, and easy to use.
4 Discussion
The present systematic review provided an overview of using VR/AR/MR/XR and music for rehabilitation. The objectives of the current review were to evaluate where and how these technologies and music were combined and what kind of utilities can be used in rehabilitation settings. To the best of our knowledge, this is the first systematic review assessing the use of VR/AR/MR/XR and music in rehabilitation. Our systematic review presented studies from 2006 to 2/2023; the total included studies was 12.
We found that VR and AR were most familiar and used in rehabilitation, but MR, and XR were less studied. None of the studies were related to AI. There is still a little confusion about the terms used in this area. Similarly to our review, Gorman and Gustafsson (2020) found that there was no clear definition of AR, and some confusion between VR and AR was noted (Triberti and Chirico, 2016).
The future of immersive and non-immersive VR technologies is promising. Both are making healthcare more personalized, efficient, and effective. Virtual technologies will give endless possibilities for rehabilitation. Wearable devices could monitor our health in real-time and provide data-driven insights to healthcare professionals. To this end, there is a need for closer integration of technical and clinical team members to maximize the efficacy of any new or proposed systems and technologies.
4.1 Study populations and risk of bias
We identified several limitations and rated a high risk of bias in the included studies. First, the risk of selection bias in selecting individuals or groups for analysis was high in almost all studies. The sample sizes were small, ranging from 2 to 52, thereby failing to ensure that the sample obtained was representative of the population level. Small sample sizes might be related to the developmental nature of technologies, collecting user experiences, and examining the feasibility of different systems.
Further, any of the studies did not present proper randomization. Due to the small number of participants and lack of comparable groups, the detection bias, which generally refers to systematic differences between groups in how outcomes are determined, cannot be assessed. In addition, reporting bias is possible if results related to the developmental processes of technologies are poor or unfinished and, because of that, not published. Here, all the studies reported at least some positive effects among participants or in their technological development processes. Attrition bias as the selective dropout of participants was not reported in these studies.
Finally, the overall external quality of studies was poor. However, the internal quality of the studies was mainly good, noting that instruments used to measure the parameter of interest were not necessarily validated.
4.2 Virtual reality technologies
As a definition, both immersive and non-immersive VR allows users to interact with a multisensory simulated environment and receive real-time feedback on performance. Additionally, VR allows pre-determined scenarios and specific exercises to be defined (Saposnik and Levin, 2011). In this review, different studies defined VR and used the definition in various ways and with differing objectives in rehabilitation. Many of the studies were testing, piloting, or developing VR solutions, like a proof-of-concept. For example, the virtual environment system has been used to simulate a piano and presents visual, auditory, and tactile feedback comparable to an actual piano (Adamovich et al., 2009). Virtual is not always defined as a virtual-like or game-like environment in the virtual world. Another example was the definition of the virtual table that was aimed to restrict the downward movements of the robot-assisted upper limb (Baur et al., 2018). Further, any glasses or displays were not obligatory (Trobia et al., 2011; Baur et al., 2018), and most VR glasses included head-mounted displays and use controllers (Buche et al., 2021; Lai et al., 2021; Heyse et al., 2022). VR applications also allowed users to meet in a private virtual environment, selecting their avatar and virtual location (Trobia et al., 2011). Due to different technologies included under the concept of “virtual”, in further research, it was necessary to define these concepts carefully. Also, it would be important to increase the knowledge of these definitions not only in the healthcare environments or among researchers but on commercial sites too. The sense of this idea is the rationale for creating a common and transparent conceptual framework for clinical work, for researchers, and for consumers.
VR involves the user in the virtual environment, but AR displays virtual images (Snoswell and Snoswell, 2019), text, sound, and graphics in the user’s natural visual and auditory fields (Morie and Chance, 2011). VR applications for rehabilitation usually address the combination of motor and cognitive training and focus on motivational issues (Mubin et al., 2019). XR and MR are defined as a kind of mixed reality. Rauschnabel et al. (2022) called the XR an abbreviation for xReality, meaning the variable x serves as a placeholder for Augmented, Assisted, Mixed, Virtual, Atomistic Virtual, Holistic Virtual, or Diminished Reality (Rauschnabel et al., 2022).
Our results indicated that AR, MR, and XR were less commonly used than VR, but the walking studies by Tunur et al. (2020) used AR technologies among Parkinson’s disease patients (Tunur et al., 2020) and Chang et al. (2019) utilized XR technologies among stroke patients also demonstrated that kind of multitasking increases activation also in motor training (Chang et al., 2019). Corrêa et al. (2017) demonstrated the use of AR musical software called GenVirtual with groups of rehabilitation professionals (Corrêa et al., 2017). By using a computer and webcam, GenVirtual added 3D musical elements into the real world, allowed participants to play different instruments. They found that AR musical software had great potential for motor and cognitive rehabilitation in children and adults. These findings were in line with music studies which presented that rhythmic stimulation and dance were better than conventional therapy or no intervention (Pereira et al., 2019). Additionally, Corrêa et al. (2017) found that increased motivation among participants also facilitated therapeutic processes (Corrêa et al., 2017), a result, that supported earlier findings (Barwood et al., 2009; Weller and Baker, 2011; Hutchinson et al., 2015; Clark et al., 2016).
The combination of different virtual reality technologies would have the potential for more effective rehabilitation, but it would need a comparative research design. Hence, there is a need for new studies, for example, focusing on comparing Augmented Virtual Glasses and Virtual Glasses with two experimental groups.
In addition, the further benefits of using VR and AR in rehabilitation can be seen as a type of personalized rehabilitation and telerehabilitation. VR and AR systems can be tailored to an individual’s specific and personalized needs, making rehabilitation more individualized. Therapists can customize the intensity, difficulty level, and feedback of exercises based on the patient’s abilities and progress, leading to more effective treatments.
VR-based rehabilitation relies on technologies such as video conferencing systems or virtual reality platforms designed for the purpose of delivering rehabilitation therapies. Hao et al. (2023) reviewed that the rehabilitation experience and functional recovery outcomes were enriched when combining telerehabilitation and virtual reality (Hao et al., 2023). Telerehabilitation, allowing patients to access therapy sessions from their homes, provides increased accessibility for individuals who have limited mobility, live far from therapy centers, or face other constraints. It also allows therapists to monitor progress, educate, provide feedback, enhance continuity of care, and support patients in their own environment (Nuara et al., 2022). Telerehabilitation can potentially reduce healthcare costs by minimizing the need for in-person visits, hospital stays, and transportation expenses (Burdea, 2003; Peretti et al., 2017).
It is noticeable that poor internet connection can introduce delays in the telerehabilitation systems, making it challenging for therapists to instruct the patient, and also for patients to follow the instructions. Another notable thing is that in many rural or underdeveloped areas, where internet infrastructure is lacking or unreliable, it is difficult for individuals in these regions to access online VR content or telerehabilitation session. Additionally, a poor internet connection may result in inconsistent data transmission, leading to inaccuracies or data loss. This can hinder accurate rehabilitation data assessment and real time progress changes, monitoring, and adjustment of the rehabilitation program. (Lange et al., 2009).
Overall, the practical usefulness of VR, AR, MR, and XR in rehabilitation lies in their ability to create immersive, interactive, and tailored interventions that can enhance motor and cognitive rehabilitation outcomes, improve motivation, and provide personalized and adaptive therapy. Further research is needed to explore the potential benefits and optimal integration of these technologies in rehabilitation settings.
4.3 The role and diversity of music
Earlier papers have demonstrated that rhythmic stimulation and dance provide motor, cognitive, and quality-of-life benefits (Barwood et al., 2009; Weller and Baker, 2011; Hutchinson et al., 2015; Sihvonen et al., 2017; Pereira et al., 2019; Lopes and Keppers, 2021). However, as we found in the current review, the facts and knowledge of how and what kind of music has been used seemed to be under-reported, specifically in the studies where music was listened to and used only to rhythm the movement. Further, part of the studies used playing (mainly piano) and singing combined with virtual technologies. Within these studies, it was partly unclear whether the application of music played a functional role in rehabilitation through interactivity promoting performance quality, or merely promoting enjoyment and adherence.
When music is listened to during the rehabilitation exercises, the main idea is to use rhythm and tempo for supporting movements. Four studies (Trobia et al., 2011; Chang et al., 2019; Tunur et al., 2020; Lai et al., 2021) presented this as the most important factor in using music. Unfortunately, these studies described the selection processes, role and diversity, and effects of music poorly. Further, the effects of music were not able to separate from the effects of virtual technologies due to the inaccurate and incomplete design of these studies. A more sensitive measurement system, such as EEG or fMRI, is needed to more accurately distinguish between the factors involved. Also, it would be beneficial to compare different groups, for example, music, virtual technologies, music and VR combined, and control. Since these sections were under-reported in included studies, assessing what kind of music would be reasonable and helpful to combine with virtual technologies as part of rehabilitation is impossible.
Based on previous research, there is no such thing as universal music for everyone. However, the strongest response has been found with the music of participants’ choice (Ukkola-Vuoti, 2019). Naturally, this sets the demand for researchers to report how they choose the music. For example, it makes sense that motivational music results in an improvement in physical exercises such as running or cycling compared with non-motivational music. Barwood et al. (2009) proposed that a change in attentional processing from internal (physical sensations) to external perspective (music and video in their study) may have facilitated improvement (Barwood et al., 2009). Thus, a description of the selection process for music used in interventions should be properly defined. This would also help to assess the real effects of music both in studies and practical settings. Further researchers and practitioners should justify what kind of music has been used, why and how music is expected to provide motor control or gait parameters, or how it is expected to change a mood or improve mental health, just a few examples mentioned.
In the current review studies, feedback refers to audio, visual, and tactile cues, such as falling balls, the possibility of correcting mistakes, and other positive feedback. With virtual technologies, four studies combined feedback systems with music, sounds, and visual or tactile components (Merians et al., 2006; Adamovich et al., 2009; Baur et al., 2018; Heyse et al., 2022). In rehabilitation, correctly timed (internal and external) feedback is essential to improve unsatisfactory physical performance, like a range of movement or corrections of planes and axes (Sciascia and Cromwell, 2012; Torp et al., 2019). Further, gamification and exergames have been found to be effective because of the motivating effects of scores, competition, levels, and immediate feedback (Matallaoui et al., 2017). This sets several demands for practitioners in the physical rehabilitation context: they need to understand the kinetic chain as a part of biomechanics but also have knowledge of the feedback timing system. In addition, more research is needed on the psychological effects of music on enjoyment and exercise adherence.
Audiovisual elements have been found to shift attention from an internal stimulus, such as physical sensations, to external cues, such as music or movies (Barwood et al., 2009; Hutchinson et al., 2015). One study used the possibility of shifting attention (Buche et al., 2021), where the idea was to listen to music during a scar massage. It was hypothesized that audiovisual elements might have been more effective than music alone, but the effects were partly situational (Barwood et al., 2009; Hutchinson et al., 2015). Furthermore, it was also unknown what was the ideal dose of music for each person or situation, or the most effective way to use music (Ukkola-Vuoti, 2019). To this end, more research is needed and that should be focused on user-based studies and collection of the experience from practitioners and patients in clinical settings.
Finally, the effects of music were unfortunately not adequately reported, and several meaningful aspects, such as assessment of pain, rhythmic stimulation, and music principles, should be reported in more detail and accuracy. Thus, for further research, it would be important to clearly define what is expected while using music and adequately explain how it is used.
4.4 Summary of studies combining virtual technologies and music for rehabilitation
Major of the studies in the current review focused on motor rehabilitation (Merians et al., 2006; Adamovich et al., 2009; Trobia et al., 2011; Chang et al., 2019; Tunur et al., 2020; Segura et al., 2021; Heyse et al., 2022). The other studies focused on motivation, psychological and cognitive factors in rehabilitation (Trobia et al., 2011; Corrêa et al., 2017; Baur et al., 2018; Tunur et al., 2020; Buche et al., 2021; Lai et al., 2021), and the usability and feasibility of technologies (Trobia et al., 2011; Corrêa et al., 2017; Baur et al., 2018; Tamplin et al., 2020; Tunur et al., 2020; Segura et al., 2021; Heyse et al., 2022).
These studies showed that different virtual technologies, such as immersive and non-immersive VR, could be used with music in rehabilitation. However, there were several inconsistencies that need attention. After analyzing the studies and the methods used, we can state that there were quite different technologies, applications, and methods, and, therefore, it was very difficult to compare the methods used in studies with each other. Further, the studies in this review concluded that motor rehabilitation after stroke showed a clinical improvement in hand functions, specifically fractionation. In addition, different areas, including motivation, adherence, mental health, etc., supported the idea that VR technologies with music have the potential to promote motivation, increase positive emotions, and decrease anxiety. Furthermore, studies in user experience and feasibility presented technologies combined with music to be safe and acceptable in rehabilitation, and participants were highly motivated and had a high adherence rate. However, the number of participants and external quality of studies did not allow the results to be generalized to a larger population.
Based on these studies, we can assume that virtual technologies with music offer promising insights to future researchers to study this more in rehabilitation. However, we cannot conclude that using VR/AR/MR/XR and music together in rehabilitation would be significantly more effective than traditional rehabilitation. Additionally, further research is needed to explore the long-term effects, optimal implementation strategies, and potential benefits for different patient populations using virtual technologies and music in rehabilitation.
To this end, when designing policies or research, there should be equal involvement of ICT professionals who develop systems and technologies, music and health professionals responsible for rehabilitation, patients, and other user groups who use the technologies, so that the usability of the technologies meets accessibility and user-friendliness criteria for adherence and effectiveness of rehabilitation.
4.5 Strengths and limitations
The main strength of the current systematic review is a comprehensive search strategy covering multiple sources of information, including full reports, summaries, and other types of reports in English. We also searched for reviews, protocols, and ongoing data but identified only published data. The use of two independent review authors minimized bias at the review level. We used the quality assessment by Hoy et al. (2012), including the external and internal qualities approach to assessing the methodological rigor of studies (Hoy et al., 2012).
Unfortunately, significant methodological limitations and heterogeneity exist within the current literature. Methods were weakly comparable, as the equipment used, assessment metrics, virtual environment, and training intensity varied from study to study, and the stability of the results had not been studied sufficiently. In addition, patient selection and VR/AR/MR/XR intervention types varied greatly between studies.
It should be noted that most of the studies were pilot studies, and only 160 (ranging from 2 to 52) participants in total were involved in the analyzed studies. Given the small sample sizes, future studies should aim to recruit adequate samples based on estimated outcome-specific effect sizes or minimally clinically significant differences. In addition, existing studies on VR/AR/MR/XR and music-based rehabilitation lacked standardization in equipment set-up and outcome measures. The studies were further limited by the study population’s heterogeneity and the short follow-up length. Thus, the results of this systematic review cannot be directly transferred to a larger population.
5 Conclusion
This systematic review summarized studies of where and how virtual technologies, including VR, AR, MR, and XR, and music combined, could be used and how they influenced the rehabilitation progress.
Some confusion was obtained related to definitions of technologies and managing terms in the included studies in this systematic review. However, based on the qualitative analysis of the studies included, it becomes evident that variations in equipment, diverse applications, assessment metrics, training environments, and methodologies made it challenging to directly compare the findings across studies. Further, it is important to note that the limited number of studies and participants, the heterogeneity among participants, and the overall quality of the studies restrict the generalizability of these results to a larger population.
The main number of studies on motor rehabilitation after stroke showed a clinical improvement in hand functions, specifically fractionation. Further, studies that included motivation, adherence, and mental health, slightly supported the idea that VR technologies with music have the potential to promote motivation and exercise adherence, increase positive emotions, and decrease anxiety. In addition, user experience and feasibility studies presented technologies combined with music to be safe and acceptable in rehabilitation. However, the reviewed material did not offer any evidence of the added value of VR technology over traditional music rehabilitation methods.
In light of these findings, it can be inferred that virtual technologies with music offer promising avenues for future rehabilitation research. Thus, there is also a need for future research to study VR and music rehabilitation methods, separately and to establish a more robust understanding of these combined approaches’ effectiveness and broader applicability, further studies with larger sample sizes, improved study designs, and rigorous methodologies are needed. Future researchers should delve deeper into this area to uncover the potential benefits and clarify the specific mechanisms through which virtual technologies with music can positively impact rehabilitation outcomes.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
PT: Writing–original draft, Writing–review and editing. LS: Writing–original draft, Writing–review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This review was financially supported by the Ministry of Education and Culture in Finland. Diary number of the project: OKM/113/523/2020.
Acknowledgments
We thank librarian Taina Peltonen from TUNI Library for her support and help.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adamovich, S. V., Fluet, G. G., Mathai, A., Qiu, Q., Lewis, J., and Merians, A. S. (2009). Design of a complex virtual reality simulation to train finger motion for persons with hemiparesis: a proof of concept study. J. Neuroeng Rehabil. 6, 28. doi:10.1186/1743-0003-6-28
Alves-Pinto, A., Turova, V., Blumenstein, T., and Lampe, R. (2016). The case for musical instrument training in cerebral Palsy for neurorehabilitation. Neural Plast. 2016, 1–9. doi:10.1155/2016/1072301
Amaral, C. P., Simões, M. A., Mouga, S., Andrade, J., and Castelo-Branco, M. (2017). A novel Brain Computer Interface for classification of social joint attention in autism and comparison of 3 experimental setups: a feasibility study. J. Neurosci. Methods 290, 105–115. doi:10.1016/j.jneumeth.2017.07.029
Ang, K., Maddocks, M., Xu, H., and Higginson, I. J. (2017). The effectiveness of singing or playing a wind instrument in improving respiratory function in patients with long-term neurological conditions: a systematic review. J. Music Ther. 54 (1), 108–131. doi:10.1093/jmt/thx001
Arksey, H., and O Malley, L. (2005). Scoping studies: towards a methodological framework. Int. J. Soc. Res. Methodol. 8 (1), 19–32. doi:10.1080/1364557032000119616
Barnish, J., Atkinson, R. A., Barran, S. M., and Barnish, M. S. (2016). Potential benefit of singing for people with Parkinson's disease: a systematic review. J. Parkinson's Dis. 6 (3), 473–484. doi:10.3233/jpd-160837
Barnish, M. S., and Barran, S. M. (2020). A systematic review of active group-based dance, singing, music therapy and theatrical interventions for quality of life, functional communication, speech, motor function and cognitive status in people with Parkinson’s disease. BMC Neurol. 20 (1), 371. doi:10.1186/s12883-020-01938-3
Barwood, M. J., Weston, N. J. V., Thelwell, R., and Page, J. (2009). A motivational music and video intervention improves high-intensity exercise performance. J. Sports Sci. Med. 8 (3), 435–442.
Baur, K., Speth, F., Nagle, A., Riener, R., and Klamroth-Marganska, V. (2018). Music meets robotics: a prospective randomized study on motivation during robot aided therapy. J. Neuroeng Rehabil. 15 (1), 79. doi:10.1186/s12984-018-0413-8
Benham, S., Kang, M., and Grampurohit, N. (2019). Immersive virtual reality for the management of pain in community-dwelling older adults. OTJR Occup. Ther. J. Res. 39 (2), 90–96. doi:10.1177/1539449218817291
Buche, H., Michel, A., Piccoli, C., and Blanc, N. (2021). Contemplating or acting? Which immersive modes should Be favored in virtual reality during physiotherapy for breast cancer rehabilitation. Front. Psychol. 12, 631186. doi:10.3389/fpsyg.2021.631186
Burdea, G. C. (2003). Virtual rehabilitation--benefits and challenges. Methods Inf. Med. 42 (5), 519–523. doi:10.1055/s-0038-1634378
Cerdán de las Heras, J., Tulppo, M., Kiviniemi, A. M., Hilberg, O., Løkke, A., Ekholm, S., et al. (2022). Augmented reality glasses as a new tele-rehabilitation tool for home use: patients’ perception and expectations. Assist. Technol. 17 (4), 480–486. doi:10.1080/17483107.2020.1800111
Chang, W.-C., Ko, L.-W., Yu, K.-H., Ho, Y., Chen, C., Jong, Y., et al. (2019). EEG analysis of mixed-reality music rehabilitation system for post-stroke lower limb therapy. J. Soc. Inf. Disp. 27, 372–380. doi:10.1002/jsid.787
Clark, I. N., Baker, F. A., and Taylor, N. F. (2016). The modulating effects of music listening on health-related exercise and physical activity in adults: a systematic review and narrative synthesis. Nordic J. Music Ther. 25 (1), 76–104. doi:10.1080/08098131.2015.1008558
Corrêa, A. G. D., de Assis, G. A., do Nascimento, M., and de Deus Lopes, R. (2017). Perceptions of clinical utility of an Augmented Reality musical software among health care professionals. Disabil. Rehabil. Assist. Technol. 12 (3), 205–216. doi:10.3109/17483107.2015.1089328
Fang, X., Qiao, Z., Yu, X., Tian, R., Liu, K., and Han, W. (2022). Effect of singing on symptoms in stable COPD: a systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 17, 2893–2904. doi:10.2147/copd.s382037
Freeman, D., Reeve, S., Robinson, A., Ehlers, A., Clark, D., Spanlang, B., et al. (2017). Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 47 (14), 2393–2400. doi:10.1017/S003329171700040X
Garcia-Agundez, A., Folkerts, A. K., Konrad, R., Caserman, P., Tregel, T., Goosses, M., et al. (2019). Recent advances in rehabilitation for Parkinson's disease with exergames: a systematic review. J. Neuroeng Rehabil. 16 (1), 17. doi:10.1186/s12984-019-0492-1
Gerber, S. M., Jeitziner, M. M., Wyss, P., Chesham, A., Urwyler, P., Müri, R. M., et al. (2017). Visuo-acoustic stimulation that helps you to relax: a virtual reality setup for patients in the intensive care unit. Sci. Rep. 7 (1), 13228. doi:10.1038/s41598-017-13153-1
Gibbs, J. K., Gillies, M., and Pan, X. A. (2022). A comparison of the effects of haptic and visual feedback on presence in virtual reality. Int. J. Human-Computer Stud. 157, 102717. doi:10.1016/j.ijhcs.2021.102717
Gorman, C., and Gustafsson, L. (2020). The use of augmented reality for rehabilitation after stroke: a narrative review. Disabil. rehabilitation Assistive Technol. 17 (4), 409–417. doi:10.1080/17483107.2020.1791264
Hao, J., Pu, Y., Chen, Z., and Siu, K. C. (2023). Effects of virtual reality-based telerehabilitation for stroke patients: a systematic review and meta-analysis of randomized controlled trials. J. stroke Cerebrovasc. Dis. official J. Natl. Stroke Assoc. 32 (3), 106960. doi:10.1016/j.jstrokecerebrovasdis.2022.106960
Heyse, J., Carlier, S., Verhelst, E., Vander Linden, C., De Backere, F., and De Turck, F. (2022). From patient to musician: a multi-sensory virtual reality rehabilitation tool for spatial neglect. Appl. Sci. 12 (3), 1242. doi:10.3390/app12031242
Higgins, J. P., Altman, D. G., Gøtzsche, P. C., Jüni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343, d5928. doi:10.1136/bmj.d5928
Hoy, D., Brooks, P., Woolf, A., Blyth, F., March, L., Bain, C., et al. (2012). Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J. Clin. Epidemiol. 65 (9), 934–939. doi:10.1016/j.jclinepi.2011.11.014
Hutchinson, J. C., Karageorghis, C. I., and Jones, L. (2015). See Hear: psychological effects of music and music-video during treadmill running. Ann. Behav. Med. 49 (2), 199–211. doi:10.1007/s12160-014-9647-2
Ioannou, A., Papastavrou, E., Avraamides, M. N., and Charalambous, A. (2020). Virtual reality and symptoms management of anxiety, depression, fatigue, and pain: a systematic review. SAGE Open Nurs. 6, 237796082093616. doi:10.1177/2377960820936163
Karageorghis, C. I. (2016). “How music can help exercisers and athletes,” in Applying music in exercise and sport. Editor C. I. Karageorghis (London, UK: Human Kinetics), 99, 1–76.
Karageorghis, C. I., and Priest, D. L. (2012). Music in the exercise domain: a review and synthesis (Part I). Int. Rev. Sport Exerc. Psychol. 5 (1), 44–66. doi:10.1080/1750984x.2011.631026
Karageorghis, C. I., Terry, P. C., and Lane, A. M. (1999). Development and initial validation of an instrument to assess the motivational qualities of music in exercise and sport: the Brunel Music Rating Inventory. J. Sports Sci. 17 (9), 713–724. doi:10.1080/026404199365579
Lai, B., Powell, M., Clement, A. G., Davis, D., Swanson-Kimani, E., and Hayes, L. (2021). Examining the feasibility of early mobilization with virtual reality gaming using head-mounted display and adaptive software with adolescents in the pediatric intensive care unit: case report. JMIR Rehabil. Assist. Technol. 8 (2), e28210. doi:10.2196/28210
Lange, B., Flynn, S. M., and Rizzo, A. A. (2009). Game-based telerehabilitation. Eur. J. Phys. Rehabil. Med. 45 (1), 143–151.
Lopes, J., and Keppers, I. I. (2021). Music-based therapy in rehabilitation of people with multiple sclerosis: a systematic review of clinical trials. Arq. Neuropsiquiatr. 79 (6), 527–535. doi:10.1590/0004-282X-ANP-2020-0374
Matallaoui, A., Koivisto, J., Hamari, J., and Zarnekow, R. (2017). “How effective is “exergamification”? A systematic review on the effectiveness of gamification features in exergames,” in Proceedings of the 50th Hawaii International Conference on System Sciences, Hawaii, USA, January, 2017.
McIntyre, A., Brar, J., and Cotoi, A. (2016). The efficacy of playing musical instruments for upper limb rehabilitation among individuals with stroke: a systematic review. Archives Phys. Med. rehabilitation 97 (10), e143. doi:10.1016/j.apmr.2016.08.446
McNamara, R. J., Epsley, C., Coren, E., and McKeough, Z. J. (2017). Singing for adults with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst. Rev. 12, CD012296. doi:10.1002/14651858.CD012296.pub2
Merians, A. S., Poizner, H., Boian, R., Burdea, G., and Adamovich, S. (2006). Sensorimotor training in a virtual reality environment: does it improve functional recovery poststroke? Neurorehabil Neural Repair 20 (2), 252–267. doi:10.1177/1545968306286914
Morie, J. F., and Chance, E. (2011). Extending the reach of health care for obesity and diabetes using virtual worlds. J. Diabetes Sci. Technol. 5, 272–276. doi:10.1177/193229681100500211
Mubin, O., Alnajjar, F., Jishtu, N., Alsinglawi, B., and Al Mahmud, A. (2019). Exoskeletons with virtual reality, augmented reality, and gamification for stroke patients’ rehabilitation: systematic review. JMIR Rehabil. Assist. Technol. 6 (2), e12010. doi:10.2196/12010
Murrock, C. J., and Higgins, P. A. (2009). The theory of music, mood and movement to improve health outcomes. J. Adv. Nurs. 65 (10), 2249–2257. doi:10.1111/j.1365-2648.2009.05108.x
Naef, A. C., Jeitziner, M.-M., Knobel, S., Exl, M. T., Müri, R., Jakob, S., et al. (2022). Investigating the role of auditory and visual sensory inputs for inducing relaxation during virtual reality stimulation. Sci. Rep. 12, 17073. doi:10.1038/s41598-022-21575-9
Nuara, A., Fabbri-Destro, M., Scalona, E., Lenzi, S. E., Rizzolatti, G., and Avanzini, P. (2022). Telerehabilitation in response to constrained physical distance: an opportunity to rethink neurorehabilitative routines. J. neurology 269 (2), 627–638. doi:10.1007/s00415-021-10397-w
Ortiz-Catalan, M., Guðmundsdóttir, R. A., Kristoffersen, M. B., Zepeda-Echavarria, A., Caine-Winterberger, K., Kulbacka-Ortiz, K., et al. (2016). Phantom motor execution facilitated by machine learning and augmented reality as treatment for phantom limb pain: a single group, clinical trial in patients with chronic intractable phantom limb pain. Lancet 388 (10062), 2885–2894. doi:10.1016/S0140-6736(16)31598-7
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71. doi:10.1136/bmj.n71
Pareto, L., Sharkey, P., and Merrick, J. (2016). Using virtual reality technologies to support everyday rehabilitation. J. Pain Manag. 9 (3), 197–198.
Pereira, A. P., Marinho, V., Gupta, D., Magalhães, F., Ayres, C., and Teixeira, S. (2019). Music therapy and dance as gait rehabilitation in patients with Parkinson disease: a review of evidence. J. Geriatric Psychiatry Neurology 32 (1), 49–56. doi:10.1177/0891988718819858
Peretti, A., Amenta, F., Tayebati, S. K., Nittari, G., and Mahdi, S. S. (2017). Telerehabilitation: review of the state-of-the-art and areas of application. Technol 4 (2), e7. doi:10.2196/rehab.7511
Pollock, D., Davies, E. L., Peters, M. D. J., Tricco, A. C., Alexander, L., McInerney, P., et al. (2021). Undertaking a scoping review: a practical guide for nursing and midwifery students, clinicians, researchers, and academics. J. Adv. Nurs. 77 (4), 2102–2113. doi:10.1111/jan.14743
Priest, D., and Karageorghis, C. I. (2008). A qualitative investigation into the characteristics and effects of music accompanying exercise. Eur. Phys. Educ. Rev. 14 (3), 347–366. doi:10.1177/1356336x08095670
Rauschnabel, P. A., Felix, R., Hinsch, C., Shahab, H., and Alt, F. (2022). What is XR? Towards a framework for augmented and virtual reality. Comput. Hum. Behav. 133, 107289. doi:10.1016/j.chb.2022.107289
Rodríguez-Hernández, M., Criado-Álvarez, J. J., Corregidor-Sánchez, A. I., MartínConty, J. L., Mohedano-Moriano, A., and Polonio-López, B. (2021). Effects of virtual reality-based therapy on quality of life of patients with subacute stroke: a three-month follow-up randomized controlled trial. Int. J. Environ. Res. Public Health 18, 2810. doi:10.3390/ijerph18062810
Ruivo, J. A. (2014). Exergames and cardiac rehabilitation, a review. J. Cardiopulm. Rehabilitation Prev. 34, 2–20. doi:10.1097/hcr.0000000000000037
Saposnik, G., and Levin, M. (2011). Virtual reality in stroke rehabilitation: a meta-analysis and implications for clinicians. Stroke 42 (5), 1380–1386. doi:10.1161/strokeaha.110.605451
Särkämö, T. (2018). Music for the ageing brain: cognitive, emotional, social, and neural benefits of musical leisure activities in stroke and dementia. Dementia. Special Issue Arts Dementia 17 (6), 670–685. doi:10.1177/1471301217729237
Sciascia, A., and Cromwell, R. (2012). Kinetic chain rehabilitation: a theoretical framework. Rehabilitation Res. Pract. 2012, 1–9. doi:10.1155/2012/853037
Segura, E., Grau-Sánchez, J., Sanchez-Pinsach, D., De la Cruz, M., Duarte, E., Arcos, J. L., et al. (2021). Designing an app for home-based enriched Music-supported Therapy in the rehabilitation of patients with chronic stroke: a pilot feasibility study. Brain Inj. 35 (12-13), 1585–1597. doi:10.1080/02699052.2021.1975819
Sihvonen, A. J., Särkämö, T., Leo, V., Tervaniemi, M., Altenmüller, E., and Soinila, S. (2017). Music-based interventions in neurological rehabilitation. Lancet Neurol. 16, 648–660. doi:10.1016/S1474-4422(17)30168-0
Slater, M., and Sanchez-Vives, M. V. (2016). Enhancing our lives with immersive virtual reality. Front. Robotics AI 3, 74. doi:10.3389/frobt.2016.00074
Snoswell, A. J., and Snoswell, C. L. (2019). Immersive virtual reality in health care: systematic review of technology and disease states. JMIR Biomed. Eng. 4 (1), e15025. doi:10.2196/15025
Swinnen, N., Vandenbulcke, M., and Vancampfort, D. (2022). Exergames in people with major neurocognitive disorder: a systematic review. Disabil. Rehabil. Assist. Technol. 17 (4), 376–389. doi:10.1080/17483107.2020.1785566
Tamplin, J., Loveridge, B., Clarke, K., Li, Y., and J Berlowitz, D. (2020). Development and feasibility testing of an online virtual reality platform for delivering therapeutic group singing interventions for people living with spinal cord injury. J. Telemed. Telecare 26 (6), 365–375. doi:10.1177/1357633X19828463
Terry, P., and Karageorghis, C. (2006). Psychophysical effects of music in sport and exercise: an update on theory, research, and application. Aust. J. Psychol. 58, 197–198.
Terry, P. C., Karageorghis, C. I., Curran, M. L., Martin, O. V., and Parsons-Smith, R. (2019). Effects of music in exercise and sport: a meta-analytic review. Psychol. Bull. 146 (2), 91–117. doi:10.1037/bul0000216
Torp, D. M., Thomas, A. C., and Donovan, L. (2019). External feedback during walking improves measures of plantar pressure in individuals with chronic ankle instability. Gait Posture 67, 236–241. doi:10.1016/j.gaitpost.2018.10.023
Triberti, S., and Chirico, A. (2016). Healthy avatars, healthy people: care engagement through. Transform. Healthc. Pract. through Patient Engagem., 247–275. doi:10.4018/978-1-5225-0663-8.ch010
Trobia, J., Gaggioli, A., and Antonietti, A. (2011). Combined use of music and virtual reality to support mental practice in stroke rehabilitation. J. CyberTherapy Rehabilitation 4 (1), 57.
Tunur, T., DeBlois, A., Yates-Horton, E., Rickford, K., and Columna, L. A. (2020). Augmented reality-based dance intervention for individuals with Parkinson's disease: a pilot study. Disabil. Health J. 13 (2), 100848. doi:10.1016/j.dhjo.2019.100848
Ukkola-Vuoti, L. (2019). Miten musiikki vaikuttaa terveyteen.Music impacts on health. The article is published in Finnish. Suom. Laakaril. 74 (21), 1348–1353.
Ventura, S., Brivio, E., Riva, G., and Baños, R. M. (2019). Immersive versus non-immersive experience: exploring the feasibility of memory assessment through 360° technology. Front. Psychol. 10, 2509. doi:10.3389/fpsyg.2019.02509
Vourvopoulos, A., Pardo, O. M., Lefebvre, S., Neureither, M., Saldana, D., Jahng, E., et al. (2019). Effects of a brain-computer interface with virtual reality (VR) neurofeedback: a pilot study in chronic stroke patients. Front. Hum. Neurosci. 13, 210. doi:10.3389/fnhum.2019.00210
Weller, C. M., and Baker, F. A. (2011). The role of music therapy in physical rehabilitation: a systematic literature review. Nordic J. Music Ther. 20 (1), 43–61. doi:10.1080/08098131.2010.485785
Wong, K., Yee, H. M., Xavier, B. A., and Grillone, G. A. (2018). Applications of augmented reality in otolaryngology: a systematic review. Otolaryngol. Head. Neck Surg. 158 (6), 956–967. doi:10.1177/0194599818796476
Xie, M., Zhou, K., Patro, N., Chan, T., Levin, M., Gupta, M., et al. (2021). Virtual reality for vestibular rehabilitation: a systematic review. Otology Neurotol. 42 (7), 967–977. doi:10.1097/MAO.0000000000003155
Xiong, J., Hsiang, E. L., He, Z., Zhan, T., and Wu, S. T. (2021). Augmented reality and virtual reality displays: emerging technologies and future perspectives. Light Sci. Appl. 10, 216. doi:10.1038/s41377-021-00658-8
Yang, Z. Q., Du, D., Wei, X. Y., and Tong, R. K. Y. (2022). Augmented reality for stroke rehabilitation during COVID-19. J. Neuro Eng. Rehabil. 19, 136. doi:10.1186/s12984-022-01100-9
Young, R., Camic, P. M., and Tischler, V. (2016). The impact of community-based arts and health interventions on cognition in people with dementia: a systematic literature review. Aging and Ment. Health 20 (4), 337–351. doi:10.1080/13607863.2015.1011080
Zhu, Y., Wang, C., Li, J., Zeng, L., and Zhang, P. (2023). Effect of different modalities of artificial intelligence rehabilitation techniques on patients with upper limb dysfunction after stroke -A network meta-analysis of randomized controlled trials. Front. Neurol. 14, 1125172. doi:10.3389/fneur.2023.1125172
Keywords: virtual reality, augmented reality, mixed reality, extended reality, listening to music, playing, singing
Citation: Tuominen PPA and Saarni LA (2024) The use of virtual technologies with music in rehabilitation: a scoping systematic review. Front. Virtual Real. 5:1290396. doi: 10.3389/frvir.2024.1290396
Received: 07 September 2023; Accepted: 06 May 2024;
Published: 15 May 2024.
Edited by:
Marientina Gotsis, University of Southern California, United StatesReviewed by:
Tomasz Kupka, Polish Dental Association, PolandMarta Matamala-Gomez, University of Barcelona, Spain
Copyright © 2024 Tuominen and Saarni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pipsa P. A. Tuominen, pipsa.tuominen@tuni.fi
†ORCID: Pipsa P. A. Tuominen, orcid.org/0000-0001-8480-6412; Lea A. Saarni, orcid.org/0000-0002-8357-547X