Case report: Endovascular stent-graft repair of aortic penetrating trauma, literature review, and case report
 Juan Gabriel Bayona1
Juan Gabriel Bayona1  Carlos Eduardo Rey Chaves2*
Carlos Eduardo Rey Chaves2*  Oscar Geovanny Hernández Rodríguez3 Vladimir Barón3 Ernesto Fajardo3 Eduardo Posada2
Oscar Geovanny Hernández Rodríguez3 Vladimir Barón3 Ernesto Fajardo3 Eduardo Posada2
- 1Cirujano General, Pontificia Universidad Javeriana, Bogotá, Colombia
- 2Estudiante de Posgrado Cirugía General, Pontificia Universidad Javeriana, Facultad de Medicina, Bogotá, Colombia
- 3Cirugía Vascular Periférica, Pontificia Universidad Javeriana, Facultad de Medicina, Hospital Universitario San Ignacio, Bogotá, Colombia
Penetrating aortic injuries are infrequent. Its incidence is unknown because most patients die of hemorrhage even before they receive adequate treatment. Aortic wounds generally require conventional thoracotomy/laparotomy repair and are related to high mortality rates. Recently with the advent of endovascular techniques, most authors prefer endovascular management when feasible due to better (still poor) outcomes. The short- and mid-term results of immediate endovascular repair of traumatic aortic injuries are promising, especially when compared with open surgical treatment, indicating that endovascular therapy is preferable in patients with multi-trauma and traumatic ruptures of the thoracic aorta. Here we present the diagnosis and treatment of a 30 years-old male patient with multiple traumatic stab wounds, including anterior aortic laceration with a grade II aortic lesion successfully managed with an endovascular stent graft.
Introduction
Penetrating aortic injuries are uncommon. Its incidence is unknown because most patients die even before they receive adequate treatment due to massive hemorrhage (1, 2). Aortic wounds generally require a conventional open surgical approach (thoracotomy or laparotomy) this open approach has been associated, among many other complications, with a 28% mortality rate and 16% paraplegia rate (3, 4). Endovascular aortic repair (EVAR) is a rapidly developing technique that involves placing an endovascular stent graft in the abdominal or thoracic aorta, avoiding the morbidity of open surgery, cardiopulmonary bypass, and aortic cross-clamping (5–7). However, despite recent improvements in resuscitation and emergency operative techniques, penetrating aortic trauma outcomes are still associated with high mortality (5–11). Therefore, we present the diagnosis and treatment of a patient with multiple traumatic stab wounds, including anterior aortic laceration with a grade II aortic lesion (10) successfully managed with an endovascular stent graft Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Case report
After ethical and institutional approval, previous informed consent was filled, following SCARE guidelines (11). We present a 30-year-old man who was found unconscious in a public pathway and transported to the emergency room with multiple thoracic and abdominal stab wounds. At the emergency room, patient presented with tachycardia (Heart rate 116), with an arterial pressure of 90/60 mmHg; initial management was performed with 1l of Ringer lactate. Preoperative blood transfusion was not required. Immediately after initial treatment due to the localization of external wounds and chest x-ray images, the vascular surgery team was called for evaluation. Four knife wounds were found on physical examination. A left supraclavicular entry orifice in zone 1 of the neck was evident without an exit wound, a right paramedian subscapular superficial wound was also evident, a left subxiphoid penetrating wound, and another penetrating wound on the right flank. The patient was hemodynamically unstable at initial hospital admission but responded to initial reanimation strategies with crystalloids. Based on the suspicion of large vessel trauma, Angio tomographic images were ordered and reviewed under multiplanar and 3D analysis (Figure 1). A descendent thoracic periaortic hematoma compromising the whole circumference with a flap-type injury at the diaphragm level was noted (Figure 1). This hematoma involved Ishimaru zones 3 and 4 and started 140 mm from the origin of the left subclavian artery and ended distally at 38 mm from the origin of the celiac trunk. There was no evidence of injuries to the abdominal aorta or other major vascular structures. These findings were later confirmed by contrast aortography.
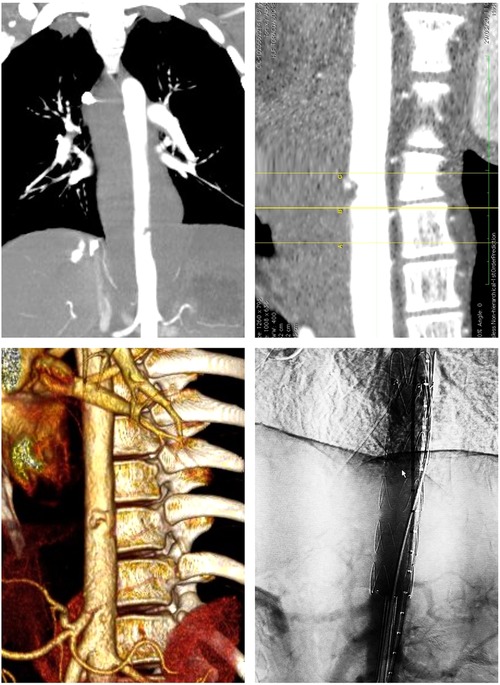
Figure 1. Angiogram showing the location of the aortic lesion, the measured distance from the aortic transection to celiac trunk and the aortic 3d reconstruction.
Emergency endovascular stenting was the best treatment option considering the area compromised because of its proximity to the crura (accessing the supradiaphragmatic aorta is likely to be challenging via open techniques), also due to the least invasive approach given the patient's young age, stable retroperitoneal and thoracic supporting connective tissue/hematoma, and a relatively low, stable blood pressure despite his critical state and the imminent risk of rupture and death. Preoperative measurement of the aorta, with an oversize of 20% was performed to select the endograft size (Figures 2, 3).

Figure 2. CT preoperative planification, measurement of the aorta.
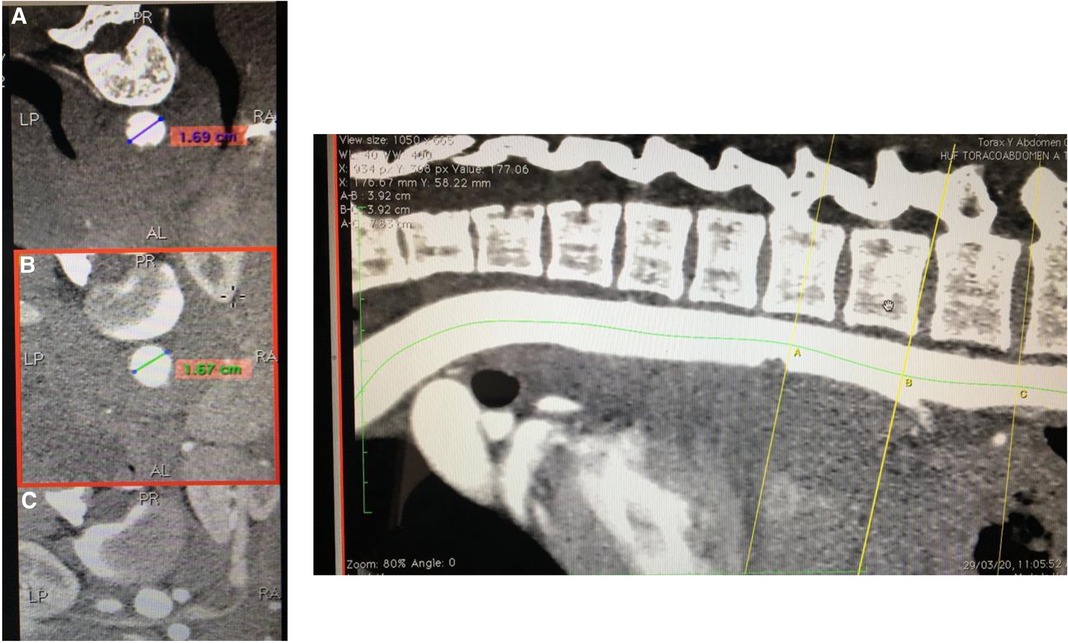
Figure 3. CT angiography measurement of the aorta, distance to the ostium of the celiac trunk.
Under local anesthesia, both femoral arteries were percutaneously punctured guided by ultrasound. After heparinization, the right and then left common femoral arteries were punctured, an 8 Fr right Pinnacle sheath (Terumo, Somerset NJ). Two ProGlide arterial closure systems were placed on each arterial access.
A hydrophilic 0.035 × 260 mm GlideWire (Terumo, Somerset NJ) wire was advanced into the aortic arch via the right femoral Pinnacle sheath, followed by a multipurpose catheter. The hydrophilic wire was posteriorly exchanged for a high support 0.035 × 260 mm Lunderquist (cook Medical INC., Bloomington, In) wire. A Lunderquist guidewire 0.035 × 260 mm (cook Medical INC., Bloomington, In) was advanced into the aortic arch via the left femoral Pinnacle sheath, followed by a pigtail centimeter marked catheter. The celiac trunk was marked. The right femoral Pinnacle sheath was removed, and the endoprosthesis was inserted (cook zenith® Alpha 16 fr) (cook Medical INC., Bloomington, In). The aortic stent was deployed, preserving the celiac trunk (Figure 1). After confirmation of adequate celiac trunk flow, the free flow was released. A completion aortogram via the left pigtail catheter demonstrated the lesion's satisfactory exclusion, showing a well-placed endoprosthesis in the abdominal aorta with no evidence of active bleeding or contrast leakage and adequate patency of the celiac trunk (Figure 1). The catheters were removed, the femoral punctures were repaired using Proglide systems, and the groins closed.
Immediately after the repair of the aortic lesion, a diagnostic laparotomy was performed under general anesthesia with better vital signs. Findings of this second procedure were 2,500 cc of hemoperitoneum, a grade II injury of segment II of the liver, a grade I injury of the upper pole of the spleen, a pinpoint injury of proximal ileum at 130 cms from the ligament of Treitz, and a grade I injury of ascending colon. Blood was drained, lesions to the colon and ileum were managed with primary suture repair and lesions to the liver and spleen with manual compression. After the procedure, there were no visible bleeding spots.
The patient had an adequate recovery without complications. The patient's discharge was made after six days of medical observation. At 6-weeks follow up the patient had no device, access site, or systemic complications. Contrast Tomography (CT) follow-up is planned at regular intervals.
Discussion
Aortic penetrating trauma is uncommon and usually a lethal condition. It occurs in less than 2% of all patients with penetrating trauma and has an approximate mortality of 80%, reaching 87% when a gunshot is the mechanism of trauma (9, 10, 12). In the United States, blunt trauma is the leading cause of aortic injury, for which endovascular repair is a well-defined and increasing practice with evidence of decreased mortality and post-operatory complications (13) In contrast, penetrating vascular trauma due to gunshots or stab wounds in developing countries such as Colombia is still more prevalent than blunt trauma (14, 15) Nevertheless, the experience with penetrating aortic trauma is limited because of its high mortality.
Now, the literature concerning cases of successful endovascular therapy is scarce. Nevertheless, according to the actual evidence endovascular approach should be the first option for treatment for this traumatic condition according to Rimbau et al. (16) in the European Society of Vascular Surgery guidelines (16). Multiple studies compare the open approach vs. Thoracic endovascular aortic repair (TEVAR) in traumatic conditions and show a reduction in mortality (9.7% vs. 27.7%) with statistically significant value, and a lesser rate of neurologic complications such as paralysis and stroke rate (0.4% vs. 2.9% and 0.4% vs. 2.3) (6, 17, 18). As well, Hoffer et al. Hoffer et al. found a reduction in mortality from 20.2% to 8.4% (p = 0.001, n = 638) and a reduction in Paralysis from 5.7% to 0.83% (p = 0.001, n = 638) (18) These results are consistent with the ones reviewed by Karmy–Jones et al. in 2011 (6). For that reason, actual recommendations suggest that for patients with suitable anatomy endovascular approach should be considered first than the open approach (10, 16–19).
Penetrating aortic trauma frequently affects adjacent tissues and organs such as the esophagus, diaphragm, and heart, also, in most cases patients die before reaching hospital facilities (20). In a large proportion of cases, the patients enter the emergency room with hemodynamic instability; in these conditions, any imaging method should be performed, and the surgical approach should not be delayed (16, 20). If the rupture has a contained hematoma, as reported in this patient, endovascular repair may be deferred until the associated life-threatening trauma is treated. In this case, the priority was the aortic wound and the evaluation of additional abdominal or thoracic diaphragm wounds was postponed. The short and mid-term results of immediate endovascular repair of traumatic aortic injuries are promising, especially when compared with open surgical treatment, indicating that endovascular therapy is preferable in patients with multi-trauma and traumatic ruptures of the thoracic aorta (6, 8, 13).
There is scarce literature regarding a long-term follow-up for patients treated with the endovascular approach, nevertheless, according to the data published by Cheng et al. (21), there is a lesser rate of reintervention after 1 and 5 years for patients treated with the TEVAR approach compared with open techniques (0% vs. 2.6%), as well, neurologic complications were lesser in TEVAR approach (21) however, further prospective studies are needed in order to evaluate long-term outcomes for this patients.
This case exhibits a patient hemodynamically stable after initial reanimation with crystalloids with a penetrating aortic injury, an intramural hematoma, and active bleeding successfully treated with TEVAR. A less invasive procedure was made without the necessity of aortic clamping and the morbidity associated with a thoracotomy or a sternotomy.
Conclusions
In conclusion, in patients with multi-trauma and traumatic rupture of the thoracic aorta, performing endovascular therapy is promising for the short- and mid-term results compared with conventional thoracotomy repair. With the increasing use by vascular surgeons of endovascular techniques for traumatic and nontraumatic aortic urgencies, these interventions will likely play an essential role in the future. However, most penetrating aortic trauma is presented in young patients with substantial life expectancy. Subsequent clinical studies evaluating the use of long-term aortic endograft must be performed.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Facultad de Medicina Pontificia Universidad Javeriana/Hospital Universitario San Ignacio. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
JB: Conceptualization, Writing – original draft, Writing – review & editing. CC: Conceptualization, Writing – original draft, Writing – review & editing. OH: Conceptualization, Supervision, Validation, Writing – review & editing. VB: Supervision, Validation, Writing – review & editing. EF: Supervision, Validation, Writing – review & editing. EP: Conceptualization, Data curation, Project administration, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Parmley LF, Mattingly TW, Manion WC. Penetrating wounds of the heart and aorta. Circulation. (1958) 17(5):953–73. doi: 10.1161/01.CIR.17.5.953
2. Demetriades D, Theodorou D, Murray J, Asensio JA, Cornwell EE 3rd, Velmahos G, et al. Mortality and prognostic factors in penetrating injuries of the aorta. J Trauma Acute Care Surg. (1996) 40(5). doi: 10.1097/00005373-199605000-00013
3. Chiba K, Abe H, Kitanaka Y, Miyairi T, Makuuchi H. Conventional surgical repair of traumatic rupture of the thoracic aorta. Gen Thorac Cardiovasc Surg. (2014) 62(12):713–9. doi: 10.1007/s11748-014-0422-x
4. Canaud L, Alric P, Branchereau P, Joyeux F, Hireche K, Berthet JP, et al. Open versus endovascular repair for patients with acute traumatic rupture of the thoracic aorta. J Thorac Cardiovasc Surg. (2011) 142(5):1032–7. doi: 10.1016/j.jtcvs.2010.11.051
5. Urgnani F, Lerut P, Da Rocha M, Adriani D, Leon F, Riambau V. Endovascular treatment of acute traumatic thoracic aortic injuries: a retrospective analysis of 20 cases. J Thorac Cardiovasc Surg. (2009) 138(5):1129–38. doi: 10.1016/j.jtcvs.2008.10.057
6. Karmy-Jones R, Ferrigno L, Teso D, Long WB 3rd, Shackford S. Endovascular repair compared with operative repair of traumatic rupture of the thoracic aorta: a nonsystematic review and a plea for trauma-specific reporting guidelines. J Trauma Acute Care Surg. (2011) 71(4). doi: 10.1097/TA.0b013e3182288783
7. Kolbeck KJ, Kaufman JA. Endovascular stent grafts in urgent blunt and penetrating thoracic aortic trauma. Semin Intervent Radiol. (2011) 28(1):98–106. doi: 10.1055/s-0031-1273944
8. Neuhauser B, Czermak B, Jaschke W, Waldenberger P, Fraedrich G, Perkmann R. Stent-graft repair for acute traumatic thoracic aortic rupture. Am Surg. (2004) 70(12):1039–44. doi: 10.1177/000313480407001202
9. Orlas CP, Herrera-Escobar JP, Zogg CK, Serna JJ, Meléndez JJ, Gómez A, et al. Chest trauma outcomes: public versus private level I trauma centers. World J Surg. (2020) 44(6):1824–34. doi: 10.1007/s00268-020-05400-w
10. Lee WA, Matsumura JS, Mitchell RS, Farber MA, Greenberg RK, Azizzadeh A, et al. Endovascular repair of traumatic thoracic aortic injury: clinical practice guidelines of the society for vascular surgery. J Vasc Surg. (2011) 53(1):187–92. doi: 10.1016/j.jvs.2010.08.027
11. Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A, SCARE Group. The SCARE 2020 guideline: updating consensus surgical CAse REport (SCARE) guidelines. Int J Surg. (2020) 84:226–30. doi: 10.1016/j.ijsu.2020.10.034
12. Eckert KL. Penetrating and blunt abdominal trauma. Crit Care Nurs Q. (2005) 28(1). doi: 10.1097/00002727-200501000-00005
13. Xenos ES, Abedi NN, Davenport DL, Minion DJ, Hamdallah O, Sorial EE, et al. Meta-analysis of endovascular vs open repair for traumatic descending thoracic aortic rupture. J Vasc Surg. (2008) 48(5):1343–51. doi: 10.1016/j.jvs.2008.04.060
14. Ordoñez CA, Manzano-Nunez R, Naranjo MP, et al. Casualties of peace: an analysis of casualties admitted to the intensive care unit during the negotiation of the comprehensive Colombian process of peace. World J Emerg Surg. (2018) 13(1):2. doi: 10.1186/s13017-017-0161-2
15. Svensson LG, Kouchoukos NT, Miller DC, Bavaria JE, Coselli JS, Curi MA, et al. Expert consensus document on the treatment of descending thoracic aortic disease using endovascular stent-grafts. Ann Thorac Surg. (2008) 85(1):S1–S41. doi: 10.1016/j.athoracsur.2007.10.099
16. Riambau V, Böckler D, Brunkwall J, Cao P, Chiesa R, Coppi G, et al. Editor’s choice management of descending thoracic aorta diseases: clinical practice guidelines of the European society for vascular surgery (ESVS). Eur J Vasc Endovasc Surg. (2017) 53(1):4–52. doi: 10.1016/j.ejvs.2016.06.005
17. Steuer J, Björck M, Sonesson B, Resch T, Dias N, Hultgren R, et al. Editor’s choice – durability of endovascular repair in blunt traumatic thoracic aortic injury: long-term outcome from four tertiary referral centers. Eur J Vasc Endovasc Surg. (2015) 50(4):460–5. doi: 10.1016/j.ejvs.2015.05.012
18. Hoffer EK, Forauer AR, Silas AM, Gemery JM. Endovascular stent-graft or open surgical repair for blunt thoracic aortic trauma: systematic review. J Vasc Interv Radiol. (2008) 19(8):1153–64. doi: 10.1016/j.jvir.2008.05.012
19. Ding X, Jiang J, Su Q, Hu S. Endovascular stent graft repair of a penetrating aortic injury. Ann Thorac Surg. (2010) 90(2):632–4. doi: 10.1016/j.athoracsur.2010.01.079
20. Slocum C, Chiba H, Emigh B, Tam B, Schellenberg M, Inaba K, et al. Nationwide analysis of penetrating thoracic aortic injury: injury patterns, management, and outcomes. J Surg Res. (2023) 284:290–5. doi: 10.1016/j.jss.2022.11.077
Keywords: aortic pseudoaneurysm, penetrating trauma, endovascular repair, vascular injury, outcomes
Citation: Bayona JG, Rey Chaves CE, Hernández Rodríguez OG, Barón V, Fajardo E and Posada E (2023) Case report: Endovascular stent-graft repair of aortic penetrating trauma, literature review, and case report. Front. Surg. 10:1264558. doi: 10.3389/fsurg.2023.1264558
Received: 21 July 2023; Accepted: 26 September 2023;
Published: 11 October 2023.
Edited by:
Dimitrios Liakopoulos, General Hospital Nice Piraeus Saint Panteleimon, GreeceReviewed by:
Aikaterini Kotzadimitriou, National and Kapodistrian University of Athens, GreeceDonagh Healy, Royal Victoria Hospital, United Kingdom
© 2023 Bayona, Rey Chaves, Hernández Rodríguez, Barón, Fajardo and Posada. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Eduardo Rey Chaves carlosrey991@gmail.com
Abbreviations EVAR, endovascular aortic repair; SCARE, surgical case report guidelines; CT, contrast tomography; TEVAR, thoracic endovascular aortic repair.