Anterior pushing technique for a broken scalpel blade in lumbar discectomy: a case report
 Dejan Čeleš
Dejan Čeleš Mladen Gasparini2
Mladen Gasparini2 - 1Department of Spine Surgery, Valdoltra Orthopaedic Hospital, Ankaran, Slovenia
- 2Department of Surgery, General Hospital Izola, Izola, Slovenia
- 3Chair of Orthopaedics, Faculty of Medicine, University of Ljubljana, Ljubljana, Slovenia
The presence of broken surgical blades or other surgically uncontrolled sharp and pointed objects in the disc space is a rare but potentially severe complication of posterior lumbar spine procedures. Herein, we report the case of a 59-year-old female patient with a history of lumbar decompression and interspinous process device implantation who underwent an instrumented revision of the lumbosacral junction. During the L5–S1 discectomy, the scalpel blade broke, and the broken fragment could not be retrieved through the posterior approach. With regard to the vascular anatomy, we partially pushed the fragment through the anterior annulus into the retroperitoneal space. In addition, pedicle screws were locked to ensure the stability of the construct. The fractured blade fragment was eventually removed by laparoscopy 1 week after the initial procedure. This experience suggests that the anterior pushing technique with fluoroscopy is an option in rare cases where a broken scalpel blade cannot be reached through the posterior approach. In such cases, computed tomography angiography is recommended.
1. Introduction
Vascular injuries during lumbar spine surgery are rare, accounting for only 1–5 cases per 10,000 lumbar disc surgeries (1), and studies on managing broken blades are scarce. Furthermore, to the best of our knowledge, a management algorithm for the adverse event of anterior migration of a fractured scalpel blade has not yet been published. In the present report, we describe the case management of a broken scalpel on the L5–S1 disc in a 59-year-old female patient who underwent a laminotomy and an implantation of an interspinous process device at the L4–L5 motion segment 7 years before the L3–S1 decompression and instrumented fusion were planned as treatment. The patient was subsequently scheduled for revision surgery due to degenerative lateral spinal canal stenosis, worsening leg pain, and chronic mechanical back pain.
2. Case presentation
In the present case, while performing a continuous-motion oval-shaped incision of the posterior disc annulus during L5–S1 discectomy and transforaminal interbody cage implantation, the No. 15 scalpel blade broke. An attempt was made to retrieve the broken segment through the posterior disc space using a microscope under fluoroscopic control. However, visual confirmation of the fractured fragment was impossible as it was covered with disc material.
3. Case timeline
Figure 1 shows the management timeline of the presented case.
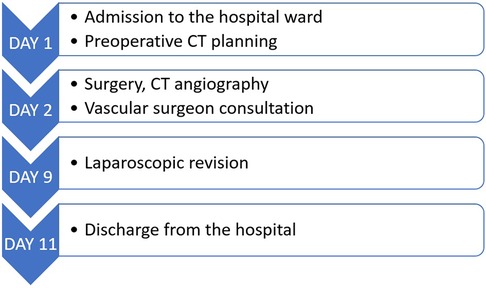
Figure 1. Case management timeline.
4. Diagnostic assessment
Intraoperatively, we reviewed the vascular anatomy of the patient using magnetic resonance (MR) imaging and preoperative computed tomography (CT). In addition, we performed an intraoperative 3D C-arm CT scan to visualize the position of the broken blade.
5. Therapeutic intervention
Removal using a pituitary rongeur was unsuccessful, resulting in the partial anterior migration of the broken scalpel blade. When the broken blade piece was in the anterior third of the disc space, we tried to remove it using a nerve hook, which was again unsuccessful. Afterward, we reevaluated the vascular anatomy using preoperative MR and CT scans. We partially pushed the broken blade piece through the anterior annulus using the nerve hook already in the disc space, guided by serial X-ray imaging (Figure 2). After the pushing maneuver, pedicle screws were locked to the rod to ensure the stability of the construct. The patient was mobilized and resumed regular ambulation as per the standard practice.
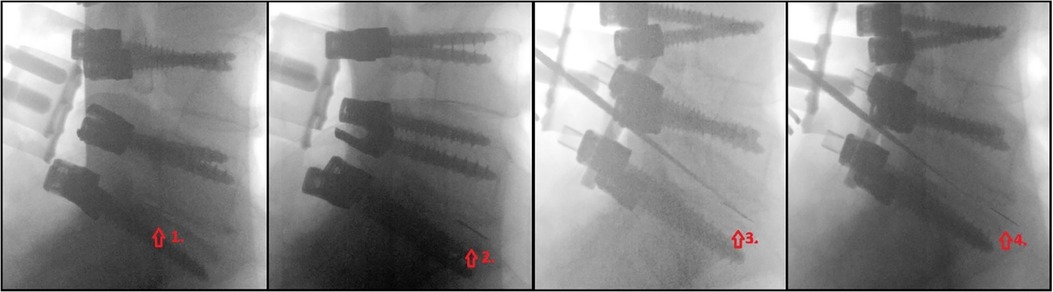
Figure 2. Sequential x-ray images of the anterior blade pushing technique.
Furthermore, CT angiography was conducted before the patient was referred to a vascular surgeon (Figure 3), and laparoscopic revision was performed a week later. This procedure revealed that the omentum majus was detached from the anterior abdominal wall, and the L5 vertebral body was accessed from the medial side of the mesosigmoid colon. After applying cranial traction to the sigmoid colon, the mesocolon of the rectosigmoid became tense, and a peritoneal incision was made. Furthermore, the right iliac artery, ureter, and sacral promontory were identified. The presacral structures were then lifted using a meticulous technique, allowing for the successful removal of the broken blade piece from where it was lodged in the anterior disc annulus.
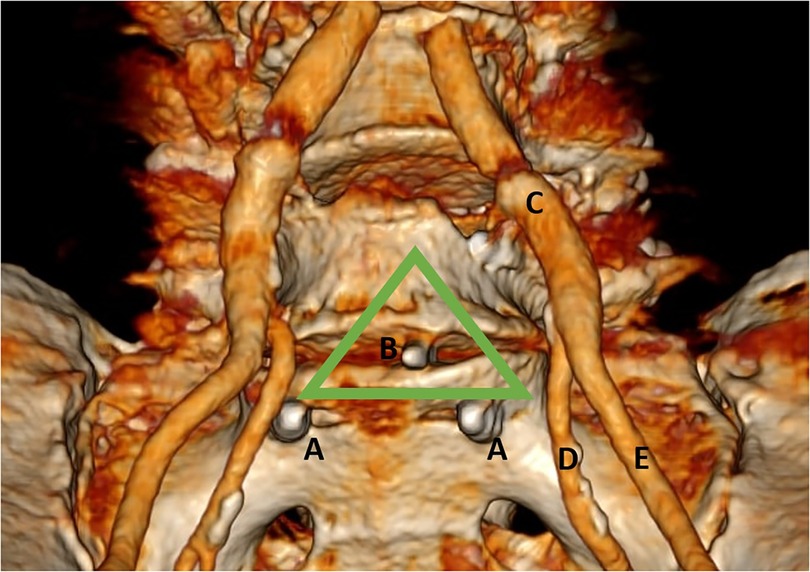
Figure 3. Computed tomography angiography image following three-dimensional reconstruction, demonstrating the (A) tip of the pedicle screw, (B) broken scalpel blade piece in the disc space, (C) common iliac artery, (D) internal iliac artery, and (E) external iliac artery. The green triangle indicates the proposed safe triangular corridor.
6. Follow-up and outcomes
The postoperative course of the patient was uneventful. At the 6-month follow-up, she was pain-free, with a stable L3–S1 fusion construct.
7. Discussion
In terms of anatomy, injury to the iliac artery and its branches is more likely to occur caudal to the L4 midbody. In contrast, the iliac vein and its branches may be damaged caudal to the L4–L5 disc space. Furthermore, the right internal iliac artery and vein are susceptible to injury at the L5–S1 disc level. Aortic and caval injuries most commonly occur at the L1–L4 vertebral levels (1). In addition, the right and left common iliac arteries are the most commonly injured (43% and 29%, respectively) during lumbar discectomy, whereas the right common iliac vein is the least commonly affected vessel (2).
Complications that may arise from protrusion or extrusion of a sharp object anterior to the lumbar disc space include arteriovenous fistula; pseudoaneurysm; vascular, urethral, or bowel laceration; foreign body granuloma; and intravascular migration of a foreign body (1, 3–8). The risk factors for scalpel blade fracture during discectomy include the use of No. 15 blades with a narrow junction, the presence of a calcified posterior longitudinal ligament and annulus, the application of the scalpel blade stabbing-and-turning technique, and encountering a narrowed disc space (9, 10). An anterior annulus ligament defect also increases the risk of anterior protrusion of the blade (11).
We considered laparoscopy (with or without a robotic aid) a minimally invasive, safe, and optimal method to visualize critical anatomical structures. In addition, robot-assisted procedures offer enhanced dexterity, allowing greater precision when dissecting (12–14). In the present study, we proposed a safe triangular corridor for avoiding vascular lesions (Figure 3). Depending on the vascular anatomy of a patient, a pushing maneuver is recommended for scalpel blade pieces retained at specific L5–S1 levels, as higher lumbar levels have a higher risk of vessel laceration. By employing the pushing technique, a minimally invasive anterior approach was possible for retrieving the broken scalpel blade lodged in the anterior disc annulus.
Relevant medical literature on such complications is scarce. Transforaminal, anterior-laparoscopic, posterior-endoscopic, and lateral approaches were used to retrieve broken scalpel blade fragments (3, 10, 12, 15). The limitation of this study is that case reports are rare, making each case unique.
8. Conclusions
Retained and extruded sharp objects within and anterior to the disc space in the lumbosacral spine are potentially life-threatening complications. These can be difficult to treat and may require an interdisciplinary approach to treatment. Vascular injury can manifest in different forms and may initially present as asymptomatic. We suggest using a stabbing technique instead of a continuous stabbing-and-turning excision of the posterior annulus to avoid breaking the scalpel blade. A safe triangular corridor should be considered for the anterior pushing technique. We suggest considering a robot-assisted laparoscopy as the preferred method for retrieving anteriorly extruded objects.
9. Patient perspective and informed consent
During the follow-up, the patient reported being free from pain and expressed satisfaction with our treatment. She had provided informed consent for the publication of this case. All personal information has been anonymized.
Data availability statement
The original contributions presented in the study are included in the article; further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
Author contributions
DČ: Conceptualization, Data curation, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. MG: Supervision, Writing – review & editing. JM: Methodology, Supervision, Writing – original draft, Writing – review & editing.
Funding
The authors declare that financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors thank Tomaž Jakomin for helping manage the reported case. The authors also thank Editage (www.editage.com) for editing the English language.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Papadoulas S, Konstantinou D, Kourea HP, Kritikos N, Haftouras N, Tsolakis JA. Vascular injury complicating lumbar disc surgery. A systematic review. Eur J Vasc Endovasc Surg. (2002) 24:189–95. doi: 10.1053/ejvs.2002.1682
2. Skippage P, Raja J, McFarland R, Belli AM. Endovascular repair of iliac artery injury complicating lumbar disc surgery. Eur Spine J. (2008) 17(Suppl 2):S228–31. doi: 10.1007/s00586-007-0470-3
3. Rahimizadeh A, Ghorbani E, Rahimizadeh S. Transforaminal retrieval of intradiscal retained broken surgical knife blade. Spine (2013) 38:E1278–81. doi: 10.1097/BRS.0b013e31829ef4d7
4. Aras AB, Ozkan OF, Alar T, Ozkan A, Arik MK, Kosar S, et al. A wandering intravascular scalpel fragment after lumbar discectomy: a case report. Turk Neurosurg (2014) 24:774–7. doi: 10.5137/1019-5149.JTN.9233-13.0
5. De Praetere H, Vanden Eycken C, Meuris B, Herijgers P. Migration of a broken scalpel into the heart after spine surgery. Interact Cardiovasc Thorac Surg (2014) 18:527–9. doi: 10.1093/icvts/ivt553
6. Krone A, Heller V, Osterhage HR. Ureteral injury in lumbar disc surgery. Acta Neurochir (1985) 78:108–12. doi: 10.1007/BF01808688
7. Garg N, Panwar P, Devana SK, Ravi Mohan SM, Mandal AK. Ureteric injury after lumbosacral microdiscectomy: a case report and review of literature. Urol Ann (2017) 9:200–3. doi: 10.4103/0974-7796.204191
8. Siasios I, Vakharia K, Khan A, Meyers JE, Yavorek S, Pollina J, et al. Bowel injury in lumbar spine surgery: a review of the literature. J Spine Surg (2018) 4:130–7. doi: 10.21037/jss.2018.03.10
9. Amirjamshidi A, Mehrazin M, Abbassioun K, Ketabtchi E. Retained broken knife blades within the disc space. Spine (1994) 19:981–4. doi: 10.1097/00007632-199404150-00018
10. Zheng GB, Wang Z. Removal of the deeply located intradiskal broken knife blade with arthroscopic assistance: case report and literature review. World Neurosurg (2020) 137:272–5. doi: 10.1016/j.wneu.2020.01.221
11. Leavens ME, Bradford FK. Ruptured intervertebral disc; report of a case with a defect in the anterior annulus fibrosus. J Neurosurg (1953) 10:544–6. doi: 10.3171/jns.1953.10.5.0544
12. Limbachia D, Gandhi P. Laparoscopic retrieval of a foreign body (broken surgical knife) from retroperitoneal space: an interesting case. Gynecol Minim Invasive Ther (2017) 6:193–4. doi: 10.1016/j.gmit.2016.10.003
13. Koutserimpas C, Ioannidis A, Konstantinidis M, Athanasopoulos P, Antonakopoulos F, Konstantinidis K. Robot-assisted removal of a broken scalpel blade following discectomy. Case Rep Surg. (2019) 2019:8609246. doi: 10.1155/2019/8609246
14. Namdarian B, Dasgupta P. What robot for tomorrow and what improvement can we expect? Curr Opin Urol (2018) 28:143–52. doi: 10.1097/MOU.0000000000000474
Keywords: broken scalpel blade, discectomy, retroperitoneal space, CT angiography, laparoscopy, anterior pushing technique
Citation: Čeleš D, Gasparini M and Mohar J (2023) Anterior pushing technique for a broken scalpel blade in lumbar discectomy: a case report. Front. Surg. 10:1266102. doi: 10.3389/fsurg.2023.1266102
Received: 24 July 2023; Accepted: 1 September 2023;
Published: 27 September 2023.
Edited by:
Panagiotis Korovessis, Olympion Medical Center, GreeceReviewed by:
Altay Sencer, Istanbul University, TürkiyeIoannis Siasios, Papageorgiou General Hospital, Greece
© 2023 Čeleš, Gasparini and Mohar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dejan Čeleš dejan.celes@ob-valdoltra.si