 Patrick Téoule
Patrick Téoule Emrullah Birgin
Emrullah Birgin Benjamin ZaltenbachGeorg KählerTorsten J. WilhelmPeter Kienle†
Benjamin ZaltenbachGeorg KählerTorsten J. WilhelmPeter Kienle† Felix Rückert*†
Felix Rückert*†
- Department of Surgery, Medical Faculty Mannheim, University Medical Centre Mannheim, Heidelberg University, Mannheim, Germany
Background: In contrast to the diverticulosis of the colon, jejunal diverticulosis is a rare condition. The incidence is 0.06–5% in large autopsy series. Complicated diverticulosis jejuni (CDJ) often presents with unspecific symptoms. Therefore, diagnosis is often a challenging process and due to the clinical rarity generally valid recommendation of perioperative management does not exist.
Patients and methods: We considered only patients who were operated in our center between April 2007 and August 2014. Patients were identified by data bank search via International Statistical Classification of Diseases and Related Health Problems diagnosis code K57.10. Data were manually screened, and patients with Meckel’s and duodenal diverticula were excluded from this study. Eleven consecutive patients with CDJ were finally included in this study. We analyzed symptoms, diagnostic procedures, surgical treatment, and postoperative morbidity and mortality.
Results: The median age of our patients was 76 years (range: 34–87). CDJ presented most frequently as intestinal bleeding or as diverticulitis. Clinical symptoms were unspecific abdominal pain, hematemesis or melena, ileus, nausea, and emesis as well as patients with acute abdomen. Esophagogastroduodenoscopies confirmed CDJ in two of the three patients. An abdominal computed tomography scan only helped to diagnose CDJ in two of the 10 patients. Eight (72.7%) patients received an open segmental resection with primary anastomosis. In three (27.3%) cases, a reoperation was necessary. Overall morbidity rate was 45.5%, and perioperative mortality was 9.1%.
Conclusion: Due to the acute character of the disease, patients with CDJ are seriously ill. To diagnose patients with CDJ remains challenging as diagnostic investigations are usually not helpful in confirming the diagnosis. Still, diagnosis of CDJ is most frequently confirmed intraoperatively.
Introduction
In contrast to the diverticulosis of the colon, jejunal diverticulosis is a rare disease. Incidence ranges from 0.06 to –5% in large autopsy series (1, 2). Most of the patients with jejunal diverticulosis are asymptomatic throughout their live. Some of the patients with diverticulitis might present with unspecific problems as intermittent abdominal pain, emesis, constipation, and diarrhea (3). Other patients will experience complications like bleeding or perforation, as in diverticulosis of the colon. The complicated diverticulosis jejuni (CDJ) is a very rare disease. Only 10–30% of the patients show such complications (4). In contrast to the diverticulosis of the colon that can often be diagnosed by its typical clinical presentation and symptoms, the CDJ displays unspecific symptoms. This is due to the relatively variable anatomic location of the small bowel. Previous studies could not identify typical symptoms in these patients that might result in further specific diagnostic and therapy (5, 6). However, such early diagnostic might be favorable as perforation or bleeding can result in severe patients’ condition. Such a complication can result in a mortality rate in previously published articles that ranges between 24 and 40% (7–9). The aim of this retrospective study was to retrospectively evaluate a cohort of patients with CDJ in a single center for colorectal surgery. The typical symptoms and findings of medical imaging were analyzed. By this, we hope to improve the perioperative management in the sense of evidence-based medicine. A secondary aim was to analyze and discuss the operative strategies and short-term results in patients with CDJ.
Patients and Methods
Patients
Medical and operative reports of all patients treated for CDJ at the department of Surgery, University Medical Centre Mannheim, Medical Faculty Mannheim, Heidelberg University, during the period from April 2007 to August 2014 were analyzed retrospectively. CDJ was defined as inflamed diverticula ante perforationem, free or sealed perforation, and bleeding diverticula requiring surgery. Meckel’s and duodenal diverticula were excluded. All included patients underwent surgery. Ethical approval for the retrospective analysis was obtained from the local ethics committee. The study was registered at www.researchregistry.com (UIN researchregistry573) and approved by the local ethics committee. All patients finally received end-to-end jejunojejunostomy after resection of the affected jejunal part. A single-layer anastomosis was created with running suture using PDS 4/0.
Data Collection and Statistics
Demographic characteristics, such as gender and age, American Society of Anaesthesiologists (ASA) status, and comorbidities as well as body mass index (BMI) were analyzed. We focused on the preoperative symptoms and the non-clinical diagnostics with respective to their predictive value, operative strategies, postoperative events and outcomes, as well as in-hospital mortality. The predictive value in percentage for a given diagnostic tool was defined as number of congruent preoperative and intraoperative finding divided by the number of all performed examinations. Postoperative complications were graded according to the Clavien–Dindo classification (10). Patient’s characteristics and parameters used for statistical analysis are listed in the Supplementary Material. After resection, patients were routinely observed at an intermediate care unit (IMC). Statistical analysis was performed by SPSS 15.0 (SPSS, Inc., Chicago, IL, USA) statistical software. All clinical and pathological characteristics were stratified to build categorical or nominal variables.
Results
Demographics and Clinical Data
Eleven patients with CDJ, four men (36.4%) and seven women (63.6%), were treated and underwent surgery at our department over a 7-year period. Median age of these patients was 76 (range: 34–87; Table 1).
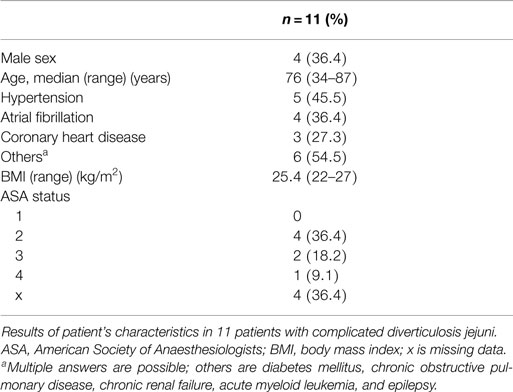
Table 1. Patient cohort demographic and clinical data.
Symptoms and Diagnostic Procedures
The most frequent and leading clinical manifestation of our patient cohort of eleven patients was abdominal pain in eight cases (72.7%). Four of these patients (50.0%) presented in the sense of acute abdomen (patient Nos. 2, 6, 7, and 10). Less frequent symptoms were gastrointestinal hemorrhage in three cases (27.3%; Nos. 4, 7, and 8), ileus in two cases (18.2%; Nos. 5 and 11), and nausea and emesis in two cases (18.2%; Nos. 3 and 9). Abdominal ultrasound was performed in nine (81.8%) patients, esophagogastroduodenoscopy (EGD) was performed in three (27.3%) patients, and colonoscopy was performed in two (18.2%) patients. An abdominal computed tomography (CT) was performed in 10 (90.9%) patients. Table 2 summarizes the duration of complaints (acute or subclinical), the kind of performed examination, and their results. In Table 3, the predictive value of the non-clinical diagnostics is indicated. Two (66.7%) out of three performed EGD helped in medical decision making. In one patient, a diverticula bleeding could initially be clipped successfully (no. 8). The endoscopy of the other patient showed blood distal from the ligament of Treitz (No. 4). Eight of the 10 (80%) patients performed abdominal CT scans and showed unspecific findings that were not helpful in the diagnosis of CDJ. In two patients, the CT findings were conclusive. In the first patients, CT finding listed a sealed perforation from the small bowel (No. 6) and in the second a bleeding after endoscopic clipping (No. 8; Tables 2 and 3).
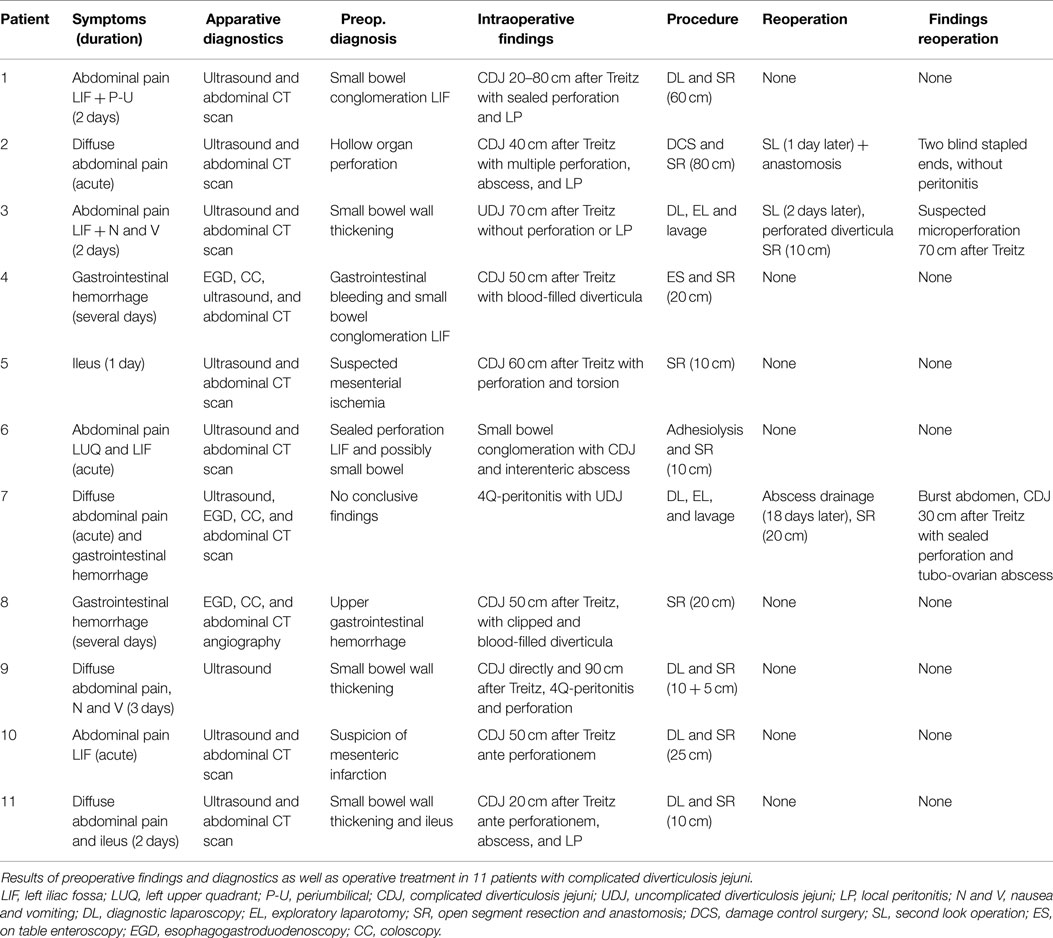
Table 2. Preoperative findings and diagnostics.
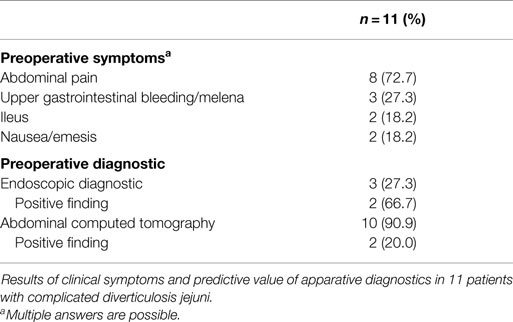
Table 3. Preoperative symptoms and predictive value of apparative diagnostics.
Intraoperative Findings and Operative Treatment
Perforated CDJ (Nos. 2, 5, and 9) and sealed perforation (Nos. 1, 6, and 7) were observed each in three (27.3%) patients. One (9.1%) microperforation was noted (No. 3). Bleeding diverticula (Nos. 4 and 8) and inflamed diverticula ante perforationem (Nos. 10 and 11) were found each in two (18.2%) cases.
Median of operative time was 125 min (range: 78–255), and median blood loss was 100 ml (range: 50–500). The surgical approach was individual and dependent on the intraoperative finding. Eight (72.7%) patients received an open segment resection with primary anastomosis (Nos. 4–6 and 8). One of the patients (9.1%) received an initial damage control surgery with discontinuity resection and lavage. This was due to the patients’ instable condition after chemotherapy for acute lymphatic leukemia. The first operation was followed by a second look operation on the next day with reanastomosis (No. 2; Figure 1). Patient number 3 had an explorative laparotomy. Intraoperatively an uncomplicated diverticulosis jejuni with no sign of perforation was found. After 2 days, a second look operation was performed due to clinical aggravation. During this second operation, a perforated diverticula was diagnosed (Figure 2). In patient number 7, a purulent peritonitis of unknown cause was seen during diagnostic laparoscopy; UJD was noticed. After conversion laparotomy, the operation was terminated with extensive lavage. Initially, the patient recovered well. However, after 18 days a reoperation had to be performed due to a burst abdomen and clinical aggravation. A CDJ 30 cm after the ligament of Treitz was found with a sealed perforation along with a tubo-ovarian abscess as secondary finding. In both of the abovementioned cases (patient Nos. 3 and 7), a resection of the affected jejunal part, reanastomosis, extensive lavage, and drainage was performed. Table 2 summarizes the intraoperative finding, especially the location of the resected jejunal section and the length of resected small bowel, as well as the operative strategies.
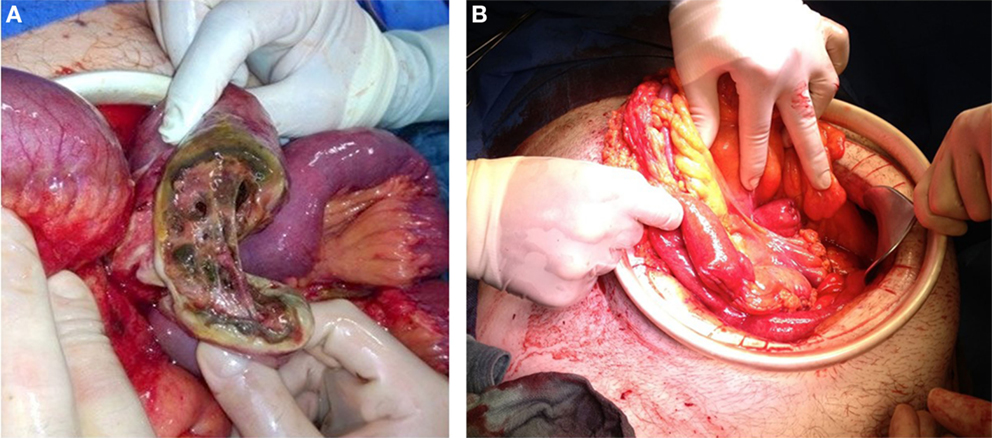
Figure 1. Two pictures after laparotomy of one patient with perforated diverticulosis jejuni and acute myeloid leukemia. [(A) before resection and (B) after damage control surgery with two blind stapled ends].
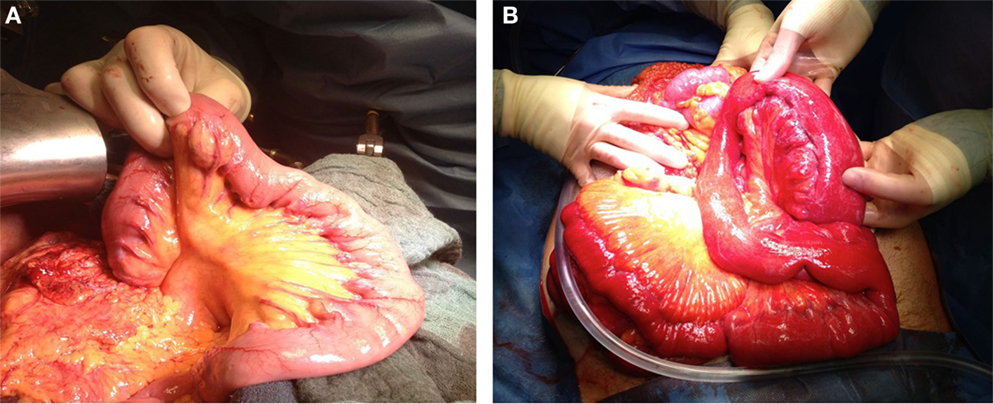
Figure 2. Two pictures after laparotomy of two patients with jejunal diverticulosis [(A) uncomplicated diverticulosis jejuni and (B) complicated diverticulosis jejuni].
Morbidity and Mortality
Postoperative complications occurred in five (45.5%) patients. Three (27.3%) of our patients had only one complication, one patient (9.1%) developed two complications, and one patient (9.1%) had four complications. In declining order, wound infections (three cases, 27.3%; Nos. 2, 5, and 9), urinary retention (one case, 9.1%; No. 3), and multiorgan failure due to sepsis (one case, 9.1%; No. 7) could be observed (Table 4).
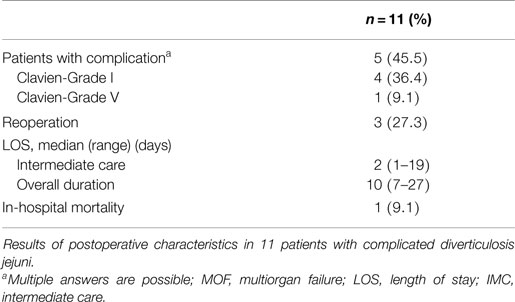
Table 4. Morbidity and mortality.
A reoperation was required in three cases (27.3%): two of the three patients received a planned relaparotomy (Nos. 2 and 3) and one patient was reoperated due to a burst abdomen and clinical aggravation, as mentioned earlier (No. 7). One (9.1%) of our 11 patients died within the postoperative course due to multiorgan failure caused by sepsis (No. 7). This patient was a 76-year-old multimorbid woman. The patient had a preexisting chronic obstructive pulmonary disease, chronic renal failure, and history of myocardial infarction. The median of postoperative length of stay in our patient cohort was 10 days (range: 7–27), whereas the median of length of stay on Intermediate Care (IMC) was 2 days (range: 1–19).
Discussion
Complicated diverticulosis jejuni is a very rare disease. The first reports of jejunal diverticulosis were in 1794 by Somerling et al. and in 1807 by Cooper et al. (11). In 1906, Gordinier and Sampson described the first patient who underwent an operation due to jejunal diverticulosis (12). Jejunal diverticulosis is usually a silent disorder, with unspecific symptoms, until it presents with acute complications. Complications requiring a surgical intervention occur in up to 30% of patients (13). These include gastrointestinal obstruction and hemorrhage as well as perforation (6, 8, 14–17). Pain is an important symptom for perforation or abscess in patients with CDJ (18). In our patient cohort, this symptom was observed in seven (63.6%) patients with peritonitis or intra-abdominal abscess. Additional one patient with severe inflammation had abdominal pain. Therefore, pain indeed seems to be an important finding in CDJ. However, the character of the pain was mostly unspecific. Additional, as a result of the varying location of jejunal diverticula, there is no characteristic localization of pain in patients with CDJ. In comparison to other intra-abdominal acute conditions such as appendicitis, cholecystitis, or colonic diverticulitis, there are no typical clinical findings that might confirm the presence of CDJ. These facts relativize the clinical importance. Clinicians should be aware that a less severe form of CDJ with only mild pain might remain undetected. Therefore, CDJ should be kept in mind as rare differential diagnosis in patient with abdominal pain. Three of our patients (27.3%) presented with hemorrhage, another manifestation of CDJ (17). It is difficult to compare this number with previous reports, as these differ widely in the observed patient cohorts. As endoscopy of the small bowel is not easy to perform, this symptom is difficult to assess.
In our opinion, pains as well as hemorrhage seem to be too unspecific to help in the early diagnosis of CDJ. However, CDJ should be kept in mind as differential diagnosis in patient presenting with these symptoms.
Non-clinical diagnostics such as abdominal CT, which usually detects or confirms a suspected preoperative diagnosis in other clinical pictures, can only reveal unspecific findings in CDJ. These findings include entrapped air or imbibition of fat tissue within the small bowel (19). In our series, only two out of 10 performed abdominal computed tomographies (20%) were helpful in the diagnosis of CDJ. Although previous studies showed that a CT scan might be helpful, our data do not support this. However, it is an important tool to rule out other differential diagnoses. In our cohort, explorative laparoscopy was the definitive diagnostic procedure in confirming CDJ. The treatment of most of our patients was determined based on the findings during laparoscopy. In synopsis, CDJ is a very rare disease with varying locations and symptoms. Today, clinical examination and anamnesis still remain the critical factor in setting the indication for surgical exploration. However, due to its rareness, CDJ is still a diagnosis by exclusion. If the diagnosis is fixed, the choice of operative method should be based on the principles of septic surgery implying immediate decontamination and healthy wound edges. Surgical resection of the involved jejunal section and primary anastomosis is the treatment of choice (7, 17, 20–22). In our patient cohort, eight (72.7%) patients had an open segment resection with primary anastomosis. One (9.1%) patient in critical condition underwent an initial damage control surgery with an open segment resection and extensive lavage, followed by a second look operation on the next day with reanastomosis.
As with most other acute diseases, the postoperative course is strongly influenced by previous medical conditions, as well as the extent of intraoperative findings (23). The incidence of CDJ increases with age, with the peak occurring in the sixth and seventh decades of life (6, 8, 20). Elderly patients have more frequently preexisting health problems and are in higher danger of complications (24). In our patient cohort, the median age was 76 years. One patient who died postoperatively was indeed of advanced age with a poor preoperatively health condition.
Out study shows that CDJ still presents formidable challenges in diagnosis and treatment. When therapy is delayed, further complications can lead to life-threatening consequences. Therefore, the emergency surgeon should always consider this differential diagnosis in acute abdomen.
Conclusion
As a result of its rarity and diffuse symptoms, diagnosis of CDJ remains a challenging process. Despite extensive preoperative diagnostics, definitive diagnosis of CDJ can often only be made intraoperatively. Due to the acute character of the disease, patients are often seriously ill and this should be considered in the perioperative management, especially as this disease is frequent in elderly patients.
Ethics Statement
This study was approved by the Ethikkomission Mannheim II; the decision included the permission to retrospectively evaluate patients data. Due to the setting of the study, it was stated that written consent was not necessary for the evaluation.
Authors Contribution
PT, PK, and FR participated in the conception and design of the study. PT and FR performed the research, analyzed the data, and drafted the manuscript. EB and BZ performed data collection. GK and TW performed data evaluation. BZ, GK, and TW participated in the revision of the manuscript. All authors have read and approved the final manuscript.
Conflict of Interest Statement
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
Funding
There was no funding for this article.
Supplementary Material
The Supplementary Material for this article can be found online at http://journal.frontiersin.org/article/10.3389/fsurg.2015.00057
References
1. Wilcox RD, Shatney CH. Surgical implications of jejunal diverticula. South Med J (1988) 81:1386–91. doi: 10.1097/00007611-198811000-00013
2. Fisher JK, Fortin D. Partial small bowel obstruction secondary to ileal diverticulitis. Radiology (1977) 122:321–2. doi:10.1148/122.2.321
3. Lee RE, Finby N. Jejunal and ileal diverticulosis. AMA Arch Intern Med (1958) 102:97–102. doi:10.1001/archinte.1958.00260190099011
5. Peters R, Grust A, Gerharz CD, Dumon C, Fürst G. Perforated jejunal diverticulitis as a rare cause of acute abdomen. Eur Radiol (1999) 9:1426–8. doi:10.1007/s003300050862
6. Ross CB, Richards WO, Sharp KW, Bertram PD, Schaper PW. Diverticular disease of the jejunum and its complications. Am Surg (1990) 56:319–24.
7. Chendrasekhar A, Timberlake GA. Perforated jejunal diverticula: an analysis of reported cases. Am Surg (1995) 61:984–8.
8. De Bree E, Grammatikakis J, Christodoulakis M, Tsiftsis D. The clinical significance of acquired jejunoileal diverticula. Am J Gastroenterol (1998) 93:2523–8. doi:10.1111/j.1572-0241.1998.00605.x
9. Fronticelli CM, Bellora P, Ferrero A, Anselmetti GC, Passarino G, Burlo P. Complicated jejunal diverticulosis: report of a case. Surg Today (1996) 26:192–5. doi:10.1007/BF00311506
10. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg (2009) 250:187–96. doi:10.1097/SLA.0b013e3181b13ca2
11. Woods K, Williams E, Melvin W, Sharp K. Acquired jejunoileal diverticulosis and its complications: a review of the literature. Am Surg (2008) 74(9):849–54.
12. Gordinier HC, Sampson JA. DIverticulitis (not meckel’s) causing intestinal obstruction.multiple mesenteric (acquired) diverticula of the small intestine. JAMA (1906) XLVI:1585–90. doi:10.1001/jama.1906.62510480013001c
13. Wilcox RD, Shatney CH. Surgical significance of acquired ileal diverticulosis. Am Surg (1990) 56:222–5.
14. Fingerhut A, Eugène C, Pourcher J, Bergue A, Terville JP, Ronat R. [Acquired diverticula of the small intestine. Presentation of a case of diverticulitis of the ileum (author’s transl)]. Gastroenterol Clin Biol (1978) 2:299–303.
15. Sales JP, Berger A, Barbier JP, Cugnenc PH. [Jejuno-ileal diverticula (Meckel excluded). Apropos of 10 cases]. J Chir (Paris) (1992) 129:73–7.
16. Altemeier WA, Bryant LR, Wulsin JH. The surgical significance of jejunal diverticulosis. Arch Surg (1963) 86:732–45. doi:10.1001/archsurg.1963.01310110042007
17. Longo WE, Vernava AM. Clinical implications of jejunoileal diverticular disease. Dis Colon Rectum (1992) 35:381–8. doi:10.1007/BF02048119
18. Staszewicz W, Christodoulou M, Proietti S, Demartines N. Acute ulcerative jejunal diverticulitis: case report of an uncommon entity. World J Gastroenterol (2008) 14:6265–7. doi:10.3748/wjg.14.6265
19. Macari M, Faust M, Liang H, Pachter HL. CT of jejunal diverticulitis: imaging findings, differential diagnosis, and clinical management. Clin Radiol (2007) 62:73–7. doi:10.1016/j.crad.2006.09.014
20. Kawamura S, Nishijima M, Yamamoto T, Sakai KI, Hirai H, Imano M, et al. Massive bleeding from multiple jejunal diverticula associated with an angiodysplasia: report of a case. Surg Today (2000) 30:750–3. doi:10.1007/s005950070091
21. El-Haddawi F, Civil ID. Acquired jejuno-ileal diverticular disease: a diagnostic and management challenge. ANZ J Surg (2003) 73:584–9. doi:10.1046/j.1445-2197.2003.02709.x
22. Papa V, Pacelli F, Gasbarrini G, Doglietto GB. Solitary jejunal diverticulum. Am J Surg (2002) 184:179–80. doi:10.1016/S0002-9610(02)00904-2
Keywords: complicated jejunal diverticulitis, perioperative management, acute abdomen, visceral surgery, rare disease
Citation: Téoule P, Birgin E, Zaltenbach B, Kähler G, Wilhelm TJ, Kienle P and Rückert F (2015) A Retrospective, Unicentric Evaluation of Complicated Diverticulosis Jejuni: Symptoms, Treatment, and Postoperative Course. Front. Surg. 2:57. doi: 10.3389/fsurg.2015.00057
Received: 03 September 2015; Accepted: 26 October 2015;
Published: 13 November 2015
Edited by:
Cihangir Akyol, Ankara University, TurkeyReviewed by:
Jose M. Ramia, SESCAM Regional Public Health System of Castilla La Mancha, SpainBassem Soliman Hegab, University of Menoufiya, Egypt
Copyright: © 2015 Téoule, Birgin, Zaltenbach, Kähler, Wilhelm, Kienle and Rückert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Felix Rückert, ZmVsaXgucnVlY2tlcnRAdW1tLmRl
†Peter Kienle and Felix Rückert have contributed equally to this work.