Editorial
05 September 2022
Antoniya Georgieva
, Patrice Abry
, Ines Nunes
and
Martin G. Frasch

Objective: The role of cardiotocography (CTG) in fetal risk assessment around the beginning of term labor is controversial. We used routinely collected clinical data in a large tertiary hospital to investigate whether infants with “severe compromise” at birth exhibited fetal heart rate abnormalities in their first-hour CTGs and/or other clinical risks, recorded as per routine care.
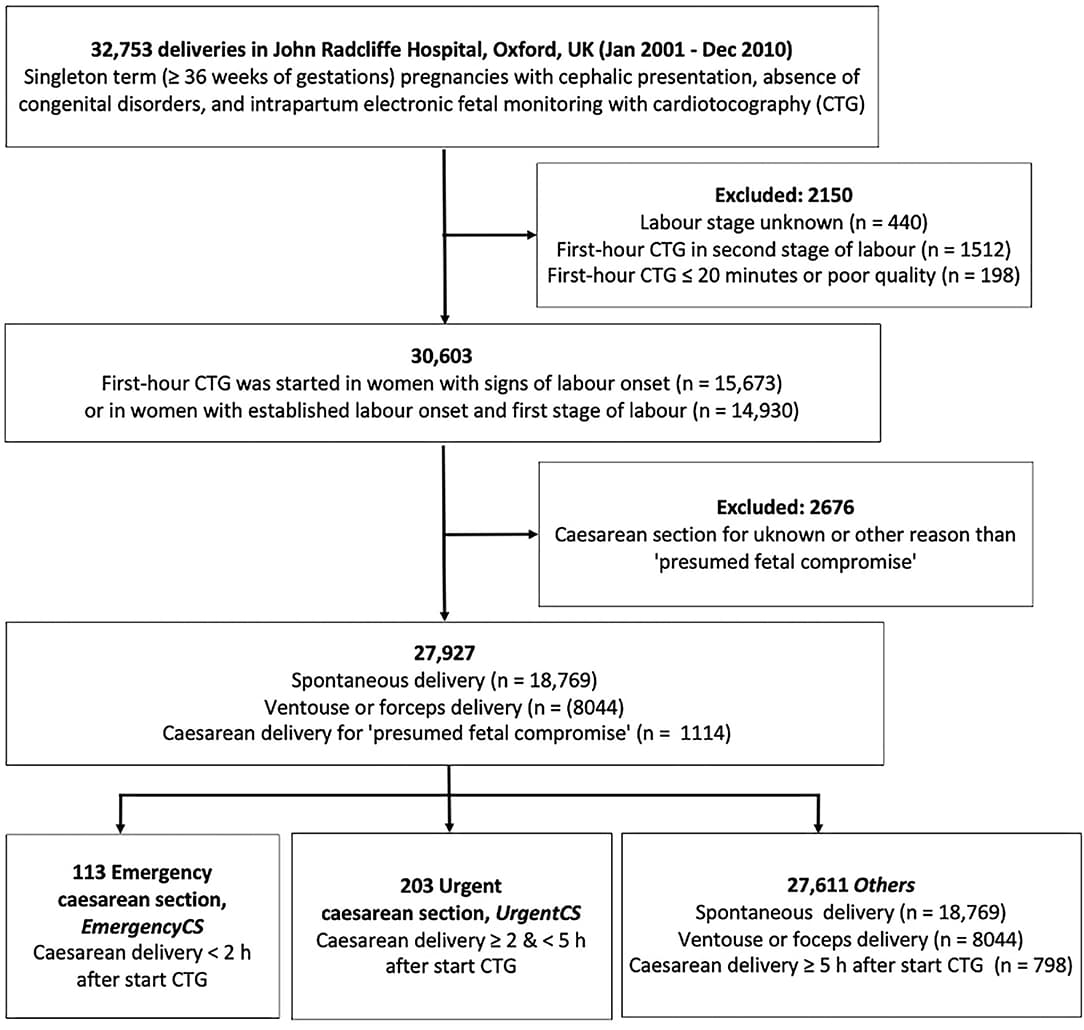
Materials and Methods: Retrospective data from 27,927 parturitions (single UK tertiary site, 2001–2010) were analyzed. Cases were included if the pregnancy was singleton, ≥36 weeks' gestation, cephalic presentation, and if they had routine intrapartum CTG as per clinical care. Cases with congenital abnormalities, planned cesarean section (CS), or CS for reasons other than “presumed fetal compromise” were excluded. We analyzed first-hour intrapartum CTG recordings, using intrapartum Oxford System (OxSys) computer-based algorithms. To reflect the effect of routine clinical care, the data was stratified into three exclusive groups: infants delivered by CS for “presumed fetal compromise” within 2 h of starting the CTG (Emergency CS, n = 113); between 2 and 5 h of starting the CTG (Urgent CS, n = 203); and the rest of deliveries (Others, n = 27,611). First-hour CTG and clinical characteristics were compared between the groups, sub-divided to those with and without severe compromise: a composite outcome of stillbirth, neonatal death, neonatal seizures, encephalopathy, resuscitation followed by ≥48 h in neonatal intensive care unit. Two-sample t-test, X2 test, and Fisher's exact test were used for analysis.
Results: Compared to babies without severe compromise, those with compromise had significantly higher proportion of cases with baseline fetal heart rate ≥150 bpm; non-reactive trace; reduced long-term and short-term variability; decelerative capacity; and no accelerations in the first-hour CTG across all groups. Prolonged decelerations(≥3 min) were also more common. Thick meconium and small for gestational age were consistently more common in compromised infants across all groups. There was more often thick meconium, maternal fever ≥38 C, sentinel events, and other clinical risk factors in the Emergency CS and Urgent CS compared to the Others group.
Conclusion: A proportion of infants born with severe compromise had significantly different first-hour CTG features and clinical risk factors.
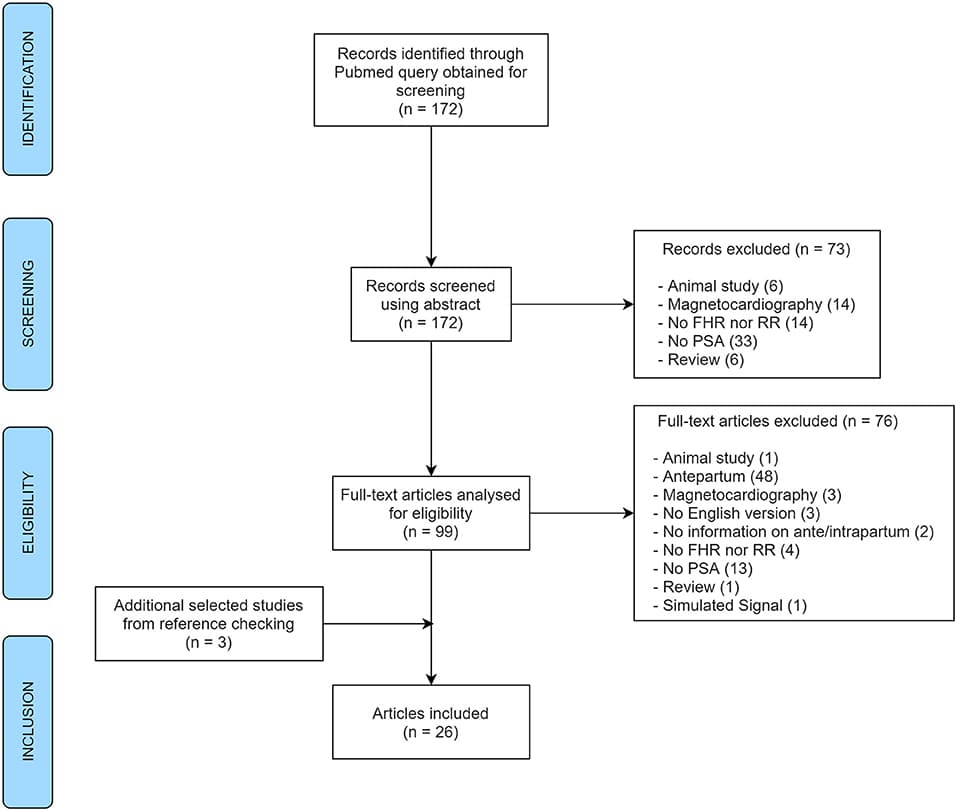
The analysis of fetal heart rate variability has served as a scientific and diagnostic tool to quantify cardiac activity fluctuations, being good indicators of fetal well-being. Many mathematical analyses were proposed to evaluate fetal heart rate variability. We focused on non-linear analysis based on concepts of chaos, fractality, and complexity: entropies, compression, fractal analysis, and wavelets. These methods have been successfully applied in the signal processing phase and increase knowledge about cardiovascular dynamics in healthy and pathological fetuses. This review summarizes those methods and investigates how non-linear measures are related to each paper's research objectives. Of the 388 articles obtained in the PubMed/Medline database and of the 421 articles in the Web of Science database, 270 articles were included in the review after all exclusion criteria were applied. While approximate entropy is the most used method in classification papers, in signal processing, the most used non-linear method was Daubechies wavelets. The top five primary research objectives covered by the selected papers were detection of signal processing, hypoxia, maturation or gestational age, intrauterine growth restriction, and fetal distress. This review shows that non-linear indices can be used to assess numerous prenatal conditions. However, they are not yet applied in clinical practice due to some critical concerns. Some studies show that the combination of several linear and non-linear indices would be ideal for improving the analysis of the fetus's well-being. Future studies should narrow the research question so a meta-analysis could be performed, probing the indices' performance.
Background: CTG remains the only non-invasive tool available to the maternity team for continuous monitoring of fetal well-being during labour. Despite widespread use and investment in staff training, difficulty with CTG interpretation continues to be identified as a problem in cases of fetal hypoxia, which often results in permanent brain injury. Given the recent advances in AI, it is hoped that its application to CTG will offer a better, less subjective and more reliable method of CTG interpretation.
Objectives: This mini-review examines the literature and discusses the impediments to the success of AI application to CTG thus far. Prior randomised control trials (RCTs) of CTG decision support systems are reviewed from technical and clinical perspectives. A selection of novel engineering approaches, not yet validated in RCTs, are also reviewed. The review presents the key challenges that need to be addressed in order to develop a robust AI tool to identify fetal distress in a timely manner so that appropriate intervention can be made.
Results: The decision support systems used in three RCTs were reviewed, summarising the algorithms, the outcomes of the trials and the limitations. Preliminary work suggests that the inclusion of clinical data can improve the performance of AI-assisted CTG. Combined with newer approaches to the classification of traces, this offers promise for rewarding future development.
Background: When exposed to repetitive umbilical cord occlusions (UCO) with worsening acidemia, fetuses eventually develop cardiovascular decompensation manifesting as pathological hypotensive arterial blood pressure (ABP) responses to fetal heart rate (FHR) decelerations. Failure to maintain cardiac output during labor is a key event leading up to brain injury. We reported that the timing of the event when a fetus begins to exhibit this cardiovascular phenotype is highly individual and was impossible to predict.
Objective: We hypothesized that this phenotype would be reflected in the individual behavior of heart rate variability (HRV) as measured by root mean square of successive differences of R-R intervals (RMSSD), a measure of vagal modulation of HRV, which is known to increase with worsening acidemia. This is clinically relevant because HRV can be computed in real-time intrapartum. Consequently, we aimed to predict the individual timing of the event when a hypotensive ABP pattern would emerge in a fetus from a series of continuous RMSSD data.
Study Design: Fourteen near-term fetal sheep were chronically instrumented with vascular catheters to record fetal arterial blood pressure, umbilical cord occluder to mimic uterine contractions occurring during human labor and ECG electrodes to compute the ECG-derived HRV measure RMSSD. All animals were studied over a ~6 h period. After a 1–2 h baseline control period, the animals underwent mild, moderate, and severe series of repetitive UCO. We applied the recently developed machine learning algorithm to detect physiologically meaningful changes in RMSSD dynamics with worsening acidemia and hypotensive responses to FHR decelerations. To mimic clinical scenarios using an ultrasound-based 4 Hz FHR sampling rate, we recomputed RMSSD from FHR sampled at 4 Hz and compared the performance of our algorithm under both conditions (1,000 Hz vs. 4 Hz).
Results: The RMSSD values were highly non-stationary, with four different regimes and three regime changes, corresponding to a baseline period followed by mild, moderate, and severe UCO series. Each time series was characterized by seemingly randomly occurring (in terms of timing of the individual onset) increase in RMSSD values at different time points during the moderate UCO series and at the start of the severe UCO series. This event manifested as an increasing trend in RMSSD values, which counter-intuitively emerged as a period of relative stationarity for the time series. Our algorithm identified these change points as the individual time points of cardiovascular decompensation with 92% sensitivity, 86% accuracy and 92% precision which corresponded to 14 ± 21 min before the visual identification. In the 4 Hz RMSSD time series, the algorithm detected the event with 3 times earlier detection times than at 1,000 Hz, i.e., producing false positive alarms with 50% sensitivity, 21% accuracy, and 27% precision. We identified the overestimation of baseline FHR variability by RMSSD at a 4 Hz sampling rate to be the cause of this phenomenon.
Conclusions: The key finding is demonstration of FHR monitoring to detect fetal cardiovascular decompensation during labor. This validates the hypothesis that our HRV-based algorithm identifies individual time points of ABP responses to UCO with worsening acidemia by extracting change point information from the physiologically related fluctuations in the RMSSD signal. This performance depends on the acquisition accuracy of beat to beat fluctuations achieved in trans-abdominal ECG devices and fails at the sampling rate used clinically in ultrasound-based systems. This has implications for implementing such an approach in clinical practice.
Late intrauterine growth restriction (IUGR) is a fetal pathological condition characterized by chronic hypoxia secondary to placental insufficiency, resulting in an abnormal rate of fetal growth. This pathology has been associated with increased fetal and neonatal morbidity and mortality. In standard clinical practice, late IUGR diagnosis can only be suspected in the third trimester and ultimately confirmed at birth. This study presents a radial basis function support vector machine (RBF-SVM) classification based on quantitative features extracted from fetal heart rate (FHR) signals acquired using routine cardiotocography (CTG) in a population of 160 healthy and 102 late IUGR fetuses. First, the individual performance of each time, frequency, and nonlinear feature was tested. To improve the unsatisfactory results of univariate analysis we firstly adopted a Recursive Feature Elimination approach to select the best subset of FHR-based parameters contributing to the discrimination of healthy vs. late IUGR fetuses. A fine tuning of the RBF-SVM model parameters resulted in a satisfactory classification performance in the training set (accuracy 0.93, sensitivity 0.93, specificity 0.84). Comparable results were obtained when applying the model on a totally independent testing set. This investigation supports the use of a multivariate approach for the in utero identification of late IUGR condition based on quantitative FHR features encompassing different domains. The proposed model allows describing the relationships among features beyond the traditional linear approaches, thus improving the classification performance. This framework has the potential to be proposed as a screening tool for the identification of late IUGR fetuses.
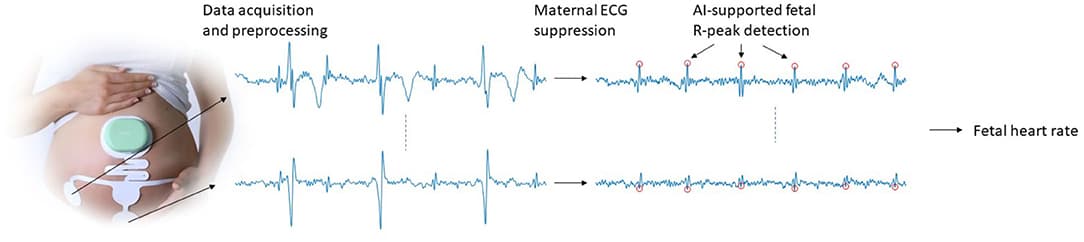


Non-invasive fetal electrocardiography represents a valuable alternative continuous fetal monitoring method that has recently received considerable attention in assessing fetal health. However, the non-invasive fetal electrocardiogram (ECG) is typically severely contaminated by a considerable amount of various noise sources, rendering fetal ECG denoising a very challenging task. This work employs a deep learning approach for removing the residual noise from multi-channel fetal ECG after the maternal ECG has been suppressed. We propose a deep convolutional encoder-decoder network with symmetric skip-layer connections, learning end-to-end mappings from noise-corrupted fetal ECG signals to clean ones. Experiments on simulated data show an average signal-to-noise ratio (SNR) improvement of 9.5 dB for fetal ECG signals with input SNR ranging between −20 and 20 dB. The method is additionally evaluated on a large set of real signals, demonstrating that it can provide significant quality improvement of the noisy fetal ECG signals. We further show that employment of multi-channel signal information by the network provides superior and more reliable performance as opposed to its single-channel network counterpart. The presented method is able to preserve beat-to-beat morphological variations and does not require any prior information on the power spectra of the noise or the pulse location.



