 Feng Tong
Feng Tong ChengLin Yu1
ChengLin Yu1 Iris Chi
Iris Chi Fang Fu
Fang Fu- 1School of International Law and Sociology, Sichuan International Studies University, Chongqing, China
- 2School of Humanities and Management, Southwest Medical University, Sichuan, China
- 3Suzanne Dworak-Peck School of Social Work, University of Southern California, Los Angeles, CA, United States
- 4School of Social Development and Public Policy, Fudan University, Shanghai, China
Background: The social isolation of older people is a growing public health concern. The proportion of older people in society has increased in recent decades, and it is estimated that ~40% of the population will be aged 50 or above within the next few decades. This systematic review aims to summarize and renew knowledge of the effectiveness of existing interventions for alleviating social isolation of older adults.
Methods: Relevant electronic databases, including Cochrane Library, CINAHL, SCOPUS, and Web of Science, were searched by a systematic evaluation method. Eligible randomized controlled trial (RCT) studies were published between 1978 and 2021 in English or Chinese. The primary and secondary outcomes were social isolation and loneliness. The quality of the included RCTs was scored by the Cochrane risk-of-bias tool to assess their quality. Two independent reviewers extracted data, using a standardized form. Narrative synthesis and vote-counting methods were used to summarize and interpret study data.
Results: Twenty-four RCTs were finally included in this review. There was evidence of substantial heterogeneity in the interventions delivered. The overall quality of included studies indicated a low-to-medium risk of bias. Eighteen of 24 RCTs showed at least one dimension effect on reducing social isolation. The interventions with accurate targeting of clients in social and public places had more obvious effect. The interventions in which older people are active participants also appeared more likely to be effective. In addition, group intervention activities and individual intervention interviews were effective in improving structural social support; mixed intervention, and group intervention on training support significantly improved functional social support.
Conclusions: This study suggests that group and mixed intervention targeting of older adults could be helpful for alleviating social isolation problems. The use of modern technology for remote services could also present good results. More well-conducted RCTs of the effectiveness of social interventions for alleviating social isolation are needed to improve the evidence base. Especially as the debating results of remote interventions, further research in this field should be conducted.
Background
Social isolation is a major threat to the health of older adults. There are many risk factors in social isolation in old age, including the lack of family members, rare or no daily communication with friends, depression, and a solitary lifestyle (Iliffe et al., 2007). Studies have indicated that social isolation and loneliness are common negative emotions, and social states among older adults that could lead, without timely intervention, to even more serious situations (Laursen and Hartl, 2013). Subsequently, research has indicated that 40% of adults over the age of 50 often felt lonely (Ferreiraalves et al., 2014). Although “loneliness” is often co-emergent and mutually influential with “social isolation,” they are two different concepts (Grenade and Boldy, 2008). Loneliness relates specifically to negative feelings of one about a situation. It may reflect social isolation or a sense of abandonment, resulting from an excessive gap between expectations and reality (Petersen et al., 2020) and increase with age (Li and Zhou, 2002), while the definitions of social isolation incorporate “structural” and “functional” social support (Lu et al., 2013). Social isolation is, therefore, multidimensional and includes the lack of structural and functional social support (Lubben and Gironda, 2003; Victor et al., 2010). In this research, social isolation was divided into two dimensions: “structural social support” and “functional social support.” Structural social support is an objective evaluation of the scale or frequency of social support participation (Lubben and Gironda, 2003; Victor et al., 2010); and functional social support is a subjective judgment on the quality of social support, including feelings, tools, and information provided by the perceived responses of others (Hall et al., 2019). According to this definition, social isolation is a multidimensional concept, which results from the lack of quality and quantity of social support (Petersen et al., 2020). The current study adopted this definition as the basis for research.
Social isolation is an essential threat to the health of older adults, and many scholars have provided evidence for methods of alleviating this problem. A meta-analysis conducted in 2010 (n = 308, mean age = 64 years; Lunstad et al., 2010) indicated that social isolation of people with strong social relationships might decrease by 50%. The compound variables used to calculate “strong social relationships” included loneliness and social isolation. Specific studies assessing the relationship between social isolation and health have reached different conclusions. For example, social isolation can lead to increased mortality, worse self-rated health (Cornwell and Waite, 2009), more susceptibility to Alzheimer's disease (Fratiglioni et al., 2000), and an increased rate of disability in older adults (Lund et al., 2010). A recent study suggested that social isolation was negatively correlated with health-related quality of life and health status of older adults (Hawton et al., 2010). Much evidence has accumulated to indicate that social isolation can affect the health of an individual. Therefore, it is an important public health problem. Moreover, the results of interventions for social isolation must be scientifically evaluated to reduce its negative impact.
There are several systematic reviews of this topic. For example, one study summarized interventions for loneliness. However, it does not fully address the effectiveness of interventions for social isolation (Masi et al., 2011). In this article, data were integrated from heterogeneous samples and included out-of-school children, homeless teenagers, and older adults. Moreover, the interventions included online chat rooms, exercise, social events, and training support. Although there is a debate about the appropriateness of meta-analysis of heterogeneous data, this kind of systematic evaluation of outcome research has seldom been reported. Recently, two systematic reviews have been conducted that included studies before 2016 (Stojanovic et al., 2016; Poscia et al., 2018). However, in these two systematic reviews, there was no quality evaluation process, and RCTs were not included. Moreover, they did not search the three main databases of PsycINFO, PubMed, and Proquest. Since then, many changes have taken place in the social environment. Remote services have been widely adopted, especially with the rapid development of information technology. Remote and other new-tech intervention RCTs targeting social isolation in older adults have been published until 2021, which necessitates updating of current knowledge.
Outcomes regarding structural social support and functional social support are important indicators of effect in the multidimensional definition of social isolation used in our review. In addition, reporting on loneliness may also contribute to the understanding of intervention effects. Therefore, this systematic review was designed to summarize and update the current knowledge about the efficacy of existing interventions for alleviating social isolation and loneliness among older adults.
Methods
Search Strategy
The literature published from January 1978 to January 2021 was systematically retrieved, using ENDNOTE X6, to manage the literature. Electronic database retrieval included PsycINFO, PubMed, Proquest, Cochrane Library, Applied Social Sciences Index and Abstracts (ASSIA), CINAHL databases, SCOPUS, Web of science, China National Knowledge Infrastructure (CNKI), and Wanfang Data Knowledge Service Platform (WANGFANG). Another search retrieved social isolation and/or loneliness in the review and has been included in the study of the reference literature; retrieval from the University of Southern California Social Work Institute database, evidence-based medicine research center of Lanzhou University, and Population Research Institute of Southwestern University of Finance and Economics. Contacts were made with scholars within the network of the authors to obtain information about ongoing studies. Search words used were as follows: older/elder/senior/aged/geriatric, isolation/isolate/isolated, lone/loneliness/alone/solitude/solitary, social support/network/relations, psychosocial intervention, treatment/therapy, clinical trial, explanatory trial, pragmatic trial, and randomized controlled trial. Search terms used were as follows: (isolation/isolate/isolated) or (lone/loneliness/alone/solitude/solitary) or (social support/network/relations) and (older/elder/senior/aged/geriatric) and (intervention/therapy/clinical trial/explanatory trial) or (explanatory trial/pragmatic trial/randomized controlled trial). The search terms in different databases were slightly different. Therefore, we also searched through the reference lists of systematic review articles on social isolation.
Review Strategy
According to the research topic and summary, two researchers (FT and CLY) made a preliminary identification of study criteria. The third researcher (FF) read the abstract of the indeterminate literature and determined the specific discussion about the disagreement. A pair of independent raters selected abstracts for full review based on inclusion/exclusion criteria. Two independent reviewers extracted data, using a standardized form. Due to the heterogeneity of different outcome indicators (e.g., family ties increased, feeling of social support, social relationship), meta-analysis is not suitable for use. According to the analysis method of the three previous evaluations (Díaz and García, 2016; Canedo-García et al., 2017; Li et al., 2018), narrative synthesis and vote-counting methods were used to summarize and interpret study data. The current review was reported in accordance with the latest PRISMA guidance (Page et al., 2021).
Inclusion and Exclusion Criteria
The primary and secondary outcomes are social isolation and loneliness. All papers selected for final inclusion met the following criteria: (i) older adults over 50 years of age with no mental illness or cognitive impairment; (ii) the purpose of the intervention was to alleviate social isolation or loneliness; (iii) the results of social isolation intervention were reported; (iv) there were randomized controlled trials but no drug trials; and (v) the paper was written in Chinese or English. Exclusion criteria for the study: (i) study samples aged younger than 50 years; (ii) not used a randomized controlled trial (RCT); (iii) drug intervention was used; and (iv) outcomes reporting only on loneliness but no social isolation.
The Quality Evaluation of the Research
Because of the heterogeneity of the intervention types and results of the trial, quantitative analysis of data was not used in the review, so the method of narrative synthesis was applied to analyze the effect of interventions. In the quality evaluation of open randomized controlled trials, we chose not to use the Jadad standard (Berger, 2006) as this is focused on blind and random sequences; therefore, the Cochrane risk-of-bias tool was deemed more appropriate (Ma et al., 2012). In this paper, based on the Cochrane risk of bias, the quality of the randomized control trial and the bias risk level were identified, and the grading principle of JADAD was used to evaluate the overall research quality. The Cochrane bias-risk tool evaluation principle involves six aspects: selection bias, implementation bias, measurement bias, data bias, publication bias, and other bias (Higgins et al., 2011). The system evaluation report is based on the PRISMA (preferred reporting items for systematic reviews and meta-analyses) standard (Page et al., 2021).
Results
About 746 items were found in the related research, with 452 duplicates removed, 268 of the studies excluded as they did not meet the selection criteria. Two studies were excluded because of high-bias risk. Twenty-four studies were eventually included (Figure 1).
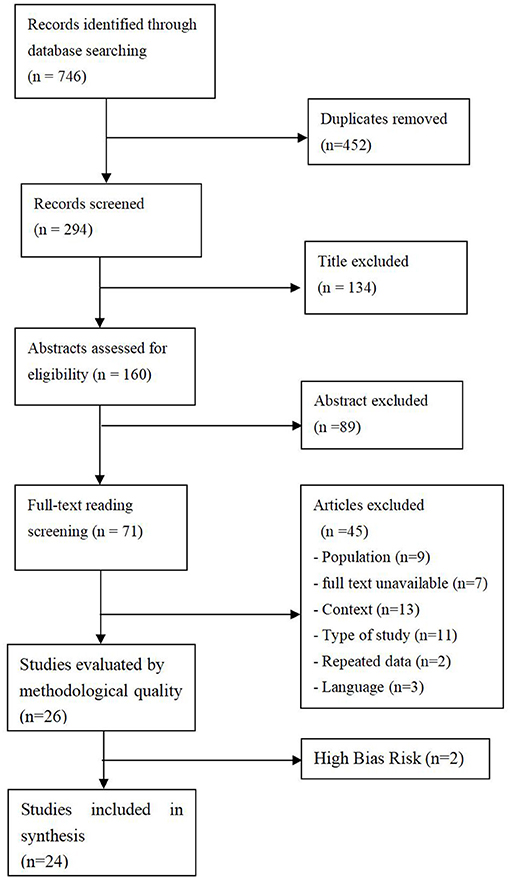
Figure 1. Eligibility and screening of studies considered for the systematic review.
Inclusion of the Study
A total of 24 randomized controlled trial studies were included with a total of 4,078 subjects, each involving 26–708 cases. Table 1 (including two high-bias risks) introduces the characteristics of these studies in accordance with the principle of PICOS, including: population, intervention, comparison, outcomes, and study type (Methley et al., 2014).
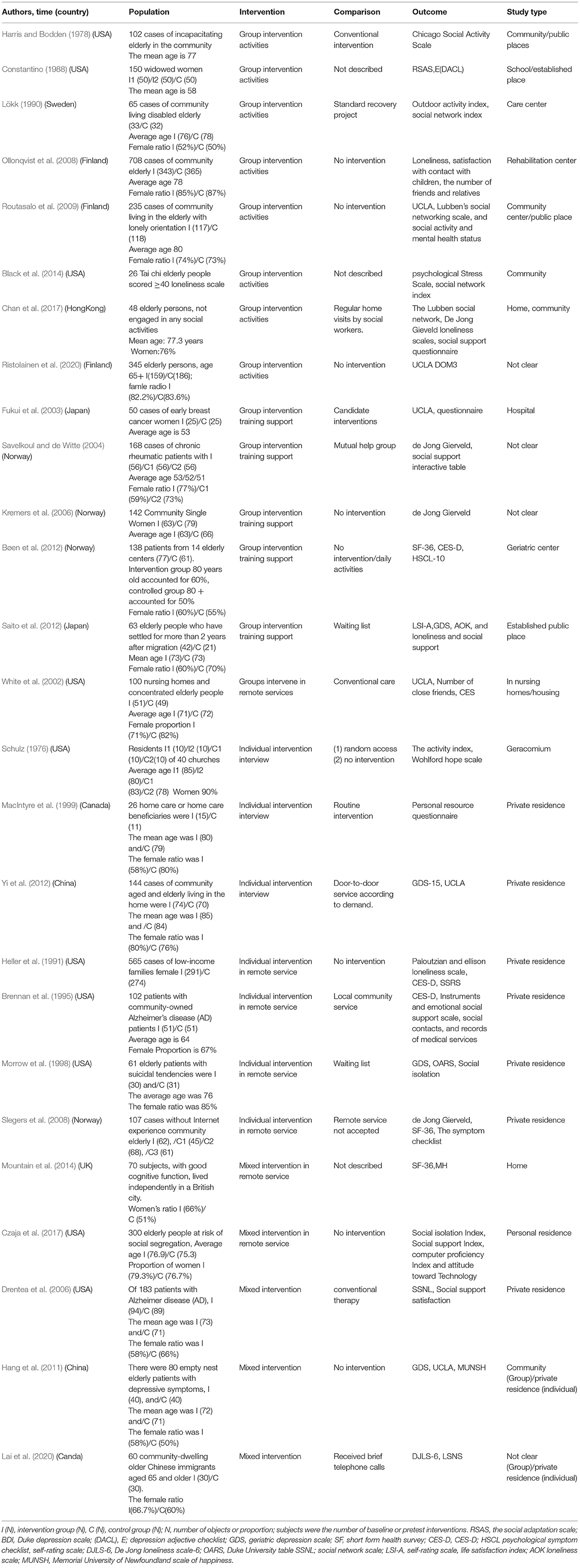
Table 1. Characteristics of studies stratified by PICOS.
Of all the studies, there were only two studies from mainland China (Hang et al., 2011; Yi et al., 2012), and one of them belonged to high risk of bias. The rest of the studies were from Hong Kong, Europe, and other developed countries. The United States occupied 10 studies, while the low-risk bias research was mostly from Finland (Ollonqvist et al., 2008; Routasalo et al., 2009).
In terms of the intervention forms, there were three main categories: group intervention, individual intervention, and mixed intervention. Fourteen studies were conducted using group interaction interventions (e.g., Harris and Bodden, 1978; Constantino, 1988; Lökk, 1990; Ollonqvist et al., 2008; Routasalo et al., 2009), seven studies used individual interventions (e.g., Schulz, 1976; Heller et al., 1991; Brennan et al., 1995; MacIntyre et al., 1999; Yi et al., 2012), and five studies combined the above two approaches (Drentea et al., 2006; Hang et al., 2011). The three intervention types could be subclassified into seven subtypes: intervention activities provided, group intervention training support, group intervention in remote service, face-to-face individual intervention, individual interventions in remote service, mixed interventions in remote service, and mixed interview intervention. Among them, seven items were group intervention activities-provided studies (e.g., Harris and Bodden, 1978; Constantino, 1988; Lökk, 1990; Ollonqvist et al., 2008; Routasalo et al., 2009), eight items were group intervention training support studies (Fukui et al., 2003; Savelkoul and de Witte, 2004; Kremers et al., 2006; Bøen et al., 2012; Saito et al., 2012), one item was a group intervention in remote service study (White et al., 2002), three items were face-to-face individual intervention studies (Schulz, 1976; MacIntyre et al., 1999; Yi et al., 2012), four items were individual interventions in remote service studies, two items were mixed interventions in remote service studies (Mountain et al., 2014; Czaja et al., 2017), two items were mixed interventions in remote service studies (Drentea et al., 2006; Hang et al., 2011), and three items were mixed interview intervention studies.
With regard to the time and frequency of intervention, most of the intervention frequency was regular, one time or two times per week. Most interventions lasted from 6 weeks to 1 year, and there was one study that lasted 5 years (Drentea et al., 2006); one study did not elaborate on the intervention frequency information (Heller et al., 1991). Among them, the primary recipient of the intervention included caregivers, disabled people, family members, older adults, and older adults living alone in the community. Only 50% (13/26) of the studies were specifically focused on social isolation or isolation (e.g., Harris and Bodden, 1978; Savelkoul and de Witte, 2004; Routasalo et al., 2009; Black et al., 2014; Chan et al., 2017), while the rest of the studies were secondary or indirect observations of variables. Intervention practitioners were health commissioners or professional social workers (e.g., Lökk, 1990; Savelkoul and de Witte, 2004; Ollonqvist et al., 2008; Routasalo et al., 2009; Saito et al., 2012), teachers (White et al., 2002; Czaja et al., 2017), students (Schulz, 1976; Constantino, 1988; MacIntyre et al., 1999), or experts. One study involved all of the above staff (Bøen et al., 2012), and one study did not specify the identity of the intervention practitioner (Harris and Bodden, 1978).
In studies that featured control conditions, the control or comparison intervention included setting the control group (e.g., Constantino, 1988; Kremers et al., 2006; Ollonqvist et al., 2008; Routasalo et al., 2009; Black et al., 2014), conventional care, and waiting-list control; four studies used a variety of cross interventions (Schulz, 1976; Savelkoul and de Witte, 2004; Slegers et al., 2008; Mountain et al., 2014); and six studies conducted remote interventions (e.g., Heller et al., 1991; Brennan et al., 1995; Morrow-Howel et al., 1998; Slegers et al., 2008; Mountain et al., 2014). In addition, between 6 months and 3 years after the baseline review, seven studies conducted only one follow-up (e.g., Schulz, 1976; Harris and Bodden, 1978; MacIntyre et al., 1999; Ollonqvist et al., 2008; Black et al., 2014). Thirteen studies included two to four follow-up visits in 2 years after the intervention (e.g., Constantino, 1988; Lökk, 1990; Routasalo et al., 2009; Chan et al., 2017). One of the studies collected follow-up data 11 times during the 5 years of the study (Drentea et al., 2006).
Methodological Quality
In order to evaluate study quality and risk of bias, the Cochrane risk-of-bias tool was applied (see Table 2). Seven studies were classified as low risk of bias (e.g., Savelkoul and de Witte, 2004; Ollonqvist et al., 2008; Routasalo et al., 2009; Bøen et al., 2012; Chan et al., 2017), two studies were classified as high risk of bias (Schulz, 1976; Hang et al., 2011), and the rest of the 17 studies were rated as moderate risk of bias. Two studies with high-bias risk will not be discussed further. The remaining 24 studies will be discussed in the following.
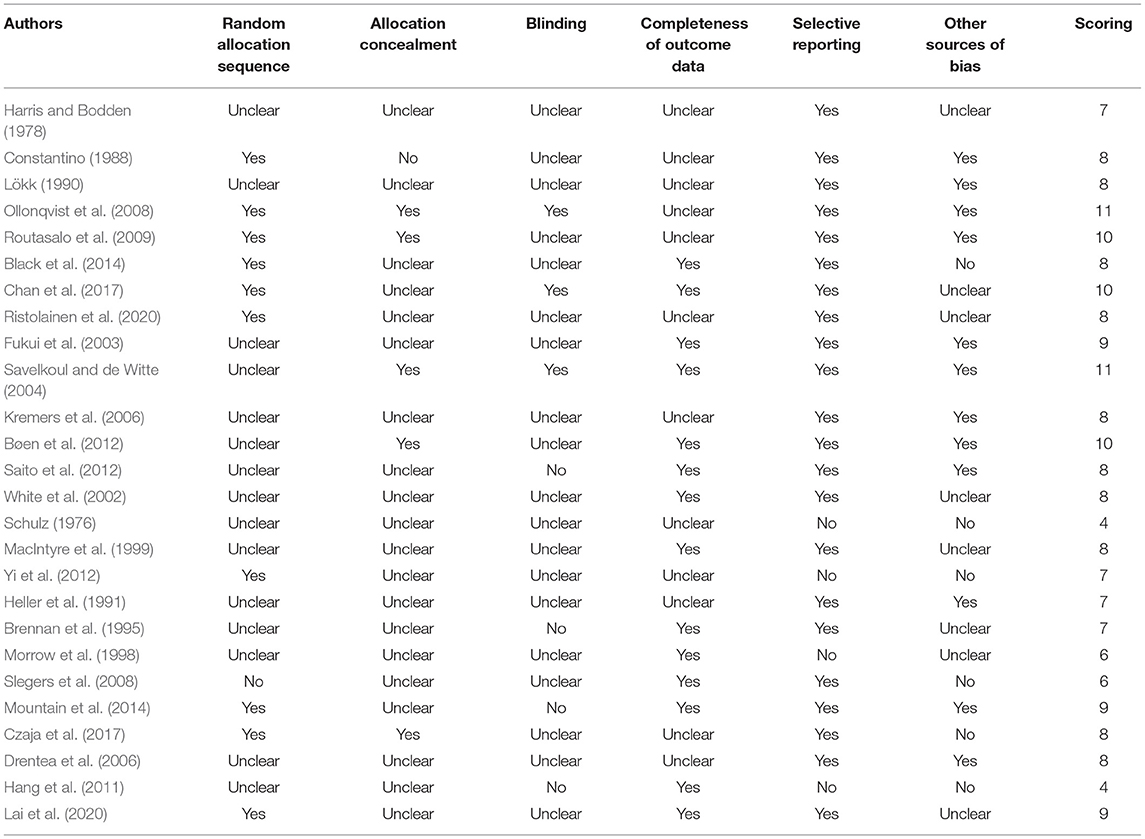
Table 2. Quality of RCT studies included in the systematic review.
The overall quality of the study continued to improve over time. Seven out of the eight intervention studies before 2000 (e.g., Schulz, 1976; Harris and Bodden, 1978; Constantino, 1988; Lökk, 1990; MacIntyre et al., 1999) were rated as moderate risks. Since 2000, 10 of the 18 studies were moderate bias risk; among which, seven were low bias risk.
Intervention Characteristics and Effects
Overall, outcomes labeled with “Y” means the intervention had significant effect on this variable, while “N” indicates no significant effect. Nineteen of the 24 intervention studies showed improvement in social isolation in at least one dimension (e.g., Harris and Bodden, 1978; Constantino, 1988; Lökk, 1990; Routasalo et al., 2009; Black et al., 2014). There was a diversity of definitions and methods of measuring social isolation where it was unclear on how best to categorize all outcomes that were grouped as “social isolation.” Where there was sufficient information about type of a social isolation outcome being measured, studies were categorized as structural social support (such as emotional or psychological support) or functional social support (such as instrumental support) (Table 3).
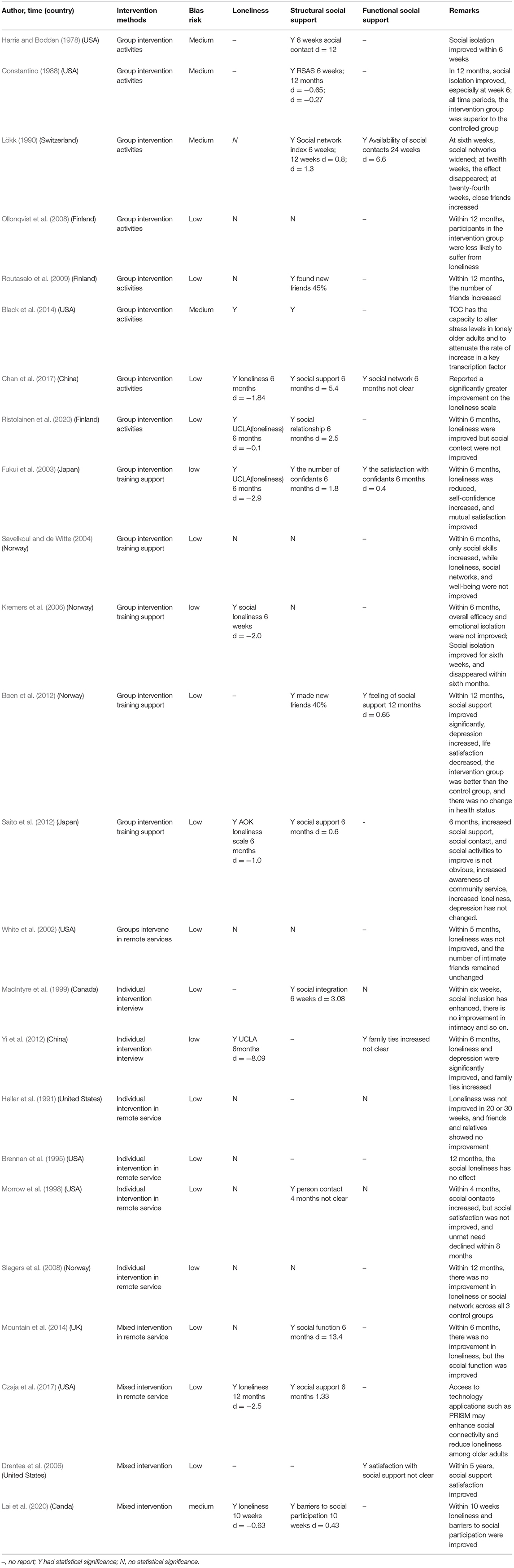
Table 3. Study results for outcomes of loneliness, structural social support, and functional social support.
Intervention Effects According to Intervention Methods
Generally, according to the classification of different intervention methods, there are 14 group interventions, 8 of them were group activities, 5 of them focus on social support training, and 1 was conducted in a remote manner. Moreover, there are six individual interventions; two of them are interviews, and the rest of four are remote service. In addition, there are four mixed interventions, and two of them are remote service.
As to intervention methods, six of the eight group intervention activities improved structural social support (Harris and Bodden, 1978; Constantino, 1988; Lökk, 1990; Routasalo et al., 2009; Black et al., 2014; Lai et al., 2020), while various forms of outcome measures were conducted. For instance, one low-risk physical exercise study showed no obvious improvement in loneliness and structural social support (Ollonqvist et al., 2008), while Taiji physical exercise showed great effect (Black et al., 2014; Chan et al., 2017). Three group interventions focused on functional social support reported significant improvements (Fukui et al., 2003; Bøen et al., 2012; Saito et al., 2012). Four structural social support studies (Fukui et al., 2003; Savelkoul and de Witte, 2004; Kremers et al., 2006; Saito et al., 2012) reported that two out of four patients had no improvement effect or the effect disappeared over time, while a few studies reported significant effects (Fukui et al., 2003; Saito et al., 2012). A moderate risk bias group intervention conducted earlier with remote services found no improvement (White et al., 2002), while another mixed remote service intervention had effects on structural social support (Mountain et al., 2014). Two individual studies that involved face-to-face interviews showed significant improvement in structural social support (MacIntyre et al., 1999; Yi et al., 2012). One of the four older (before 2010) individuals involved in a remote service study (Heller et al., 1991; Brennan et al., 1995; Morrow-Howel et al., 1998; Slegers et al., 2008) showed improvement effects on structural social support, but the follow-up effect was very short (Morrow-Howel et al., 1998). Two studies with moderate risk bias conducted by mixed intervention showed improvement in functional social support (Czaja et al., 2017; Lai et al., 2020).
Intervention Effects According to Intervention Environment
The external environment of intervention, such as the intervention practitioner, the place of intervention, and the client, was also an important factor in the effect of intervention. Five of the six interventions provided by experts showed improved outcomes (Heller et al., 1991; Fukui et al., 2003; Kremers et al., 2006; Mountain et al., 2014; Czaja et al., 2017). Seven of the 10 interventions provided by health or social workers were also effective (Lökk, 1990; Ollonqvist et al., 2008; Saito et al., 2012; Black et al., 2014; Chan et al., 2017; Lai et al., 2020; Ristolainen et al., 2020). Four interventions provided by teachers or students of the education community presented improved results (Constantino, 1988; MacIntyre et al., 1999; White et al., 2002; Slegers et al., 2008). In addition, one study multiple types of intervention practitioners (Bøen et al., 2012), another study didn't specifically described the information of intervention providers (Harris and Bodden, 1978).
As for the field of intervention, five studies took place in schools or public places (Harris and Bodden, 1978; Constantino, 1988; Routasalo et al., 2009; Black et al., 2014; Chan et al., 2017), and 1~2 dimensions were improved. Five studies were professional treatment interventions (e.g., senior center, rehabilitation center, and hospital) (Lökk, 1990; Ollonqvist et al., 2008; Routasalo et al., 2009; Bøen et al., 2012; Black et al., 2014), and all of these showed improvements in 1~3 dimensions. In six individual studies of private residences (Heller et al., 1991; Brennan et al., 1995; Morrow-Howel et al., 1998; MacIntyre et al., 1999; Yi et al., 2012; Lai et al., 2020), only two intervention studies presented no improved effects, even any dimension (Heller et al., 1991, Brennan et al., 1995). The other three studies did not provide evidence of the implementation environment (Savelkoul and de Witte, 2004; Kremers et al., 2006; Ristolainen et al., 2020). In addition, studies precisely targeting clients with social isolation or loneliness problems had better effects on all dimensions (e.g., Harris and Bodden, 1978; Savelkoul and de Witte, 2004; Routasalo et al., 2009; Bøen et al., 2012; Saito et al., 2012). By contrast, the studies without specific targets showed a worsened effect (Savelkoul and de Witte, 2004).
Intervention Effects According to Duration of Effect
Among the 14 studies reporting structural social support effect, three of them used social support as the outcome (Saito et al., 2012; Chan et al., 2017; Czaja et al., 2017), two studies observed the change of new friend number as an outcome (Routasalo et al., 2009; Bøen et al., 2012). One study showed that 45% of the participants made new friends in 1 year (Routasalo et al., 2009), while another showed that 40% of the participants made new friends in 1 year (Bøen et al., 2012), two studies reported using social contact as an outcome (Harris and Bodden, 1978; Morrow et al., 1998). And all studies reporting functional social support effect took completely different indicators during 6–12 months.
Discussion
This study found substantial heterogeneity in the interventions delivered, and the overall quality of included studies indicated a low to medium risk of bias. Also, group intervention activities and individual intervention were effective in improving structural social support; mixed intervention and group intervention on training support significantly improved functional social support. We found that the interventions with accurate targeting of clients in social and public places had more obvious effect. Interventions in which older people were active participants also appeared more likely to be effective. In addition, professionals were better than teachers and students in conducting intervention. The findings provide a tentative indication of the potential benefits of specific types of intervention for improving loneliness/social isolation, advancing theory-informed development of interventions and improving design of evaluation studies. The remote service interventions were debatable, as the recent studies have showed improvement in structural social support, but no effect on older studies. Because of the contradictory results, more research is needed to examine the complexity of “remote interventions” from the perspective of process evaluation. Interventions conducted in social and public places had better effects, and interventions with accurate targeting of clients had more obvious effects. Studies evaluating interventions delivered by professional practitioners appeared to yield better outcomes than those where the intervention was delivered by non-professionals. Effective intervention for older adults in isolation not only improved structural social support, functional social support, and mitigation of loneliness but also promoted the health of older adults.
In the experimental studies, there were a variety of interventions on social isolation. Although experimental design is not always feasible or accepted by participants, this kind of study can provide a scientific and normative reference for the implementation process and assessment report, promote the utilization of randomized control trials, improve the design level, standardize the research process, improve the quality of evidence, and provide a reference for policy-making. We advocate professionals to provide face-to-face intervention in the field of daily life rather than in the home environment and recommend that more efficient remote interventions within smart terminals be developed to achieve better results.
In real life, the environment preference of older adults has an obvious effect on their social interaction. Older adults who enjoy being alone are more likely to be socially isolated. The incidence of social isolation among older adults in different living conditions was also different, with those who were widowed, had low income, and in poor health, more likely to feel lonely and socially isolated. In addition, as age increases, older adults can be more dissociated from social interaction and prefer to be isolated (Lu et al., 2013). Therefore, when we design social isolation interventions, it is essential to consider personal preference, living status, and physiological characteristics of older adults and adjust measures accordingly so as to promote the effectiveness of the intervention. In addition, well-designed remote intervention system, such as personal reminder information and social management (PRISM) system, has the potential to change attitudes toward technology and increase technology self-efficacy.
At the policy level, the establishment of social support systems is imminent (Liu and Ni, 2002). With the advancement of family planning policy, such as China, the aging of the population is becoming more and more serious, and the “4-2-1” or “4-2-2” family pattern (4-grandparent, 2-parent, and 2- or 1-child) has gradually formed (Nan and Dong, 2019). Family support functions have greatly weakened, and, especially, the needs for social interaction and spiritual comfort are not satisfied. Therefore, we must establish a community-based pension support service platform, develop professional social work vigorously, cooperate with research institutes to obtain scientific evidence in order to address the problem of social isolation of older adults, improve their physical and mental health, as well as quality of life, and promote the healthy aging of the population.
Limitations and Future Research Directions
In this study, the inclusion literature was defined as older adults over age 50, who have been in isolation or loneliness. However, the relevant research on the concept of social isolation does not use a standardized and unified definition, so inclusion bias may have been incorporated. Although the inclusion criteria were designed to reduce social isolation or loneliness, only 14/24 studies specifically addressed the problem (e.g., Constantino, 1988; Li and Zhou, 2002; Savelkoul and de Witte, 2004; Kremers et al., 2006; Chan et al., 2017). The study may also have the potential risk that the assessment of social isolation or loneliness was due to other characteristics of the target client (Liu and Ni, 2002). Restricting the study language to English and Chinese may have increased the inclusion bias. The quality and expression of the research in the historical period also limited the quality of this study. Some studies conducted a qualitative report rather than quantitative data. It is not appropriate to use quantitative methods as well as meta-analysis due to the heterogeneity of the study subjects.
At the same time, we found that most pieces of randomized controlled trial research in this field were from developed countries. Future research not only needs to enrich the original evidence from all over the world but especially from developing countries. In addition, most of the pieces of research from Finland, Norway, the United States, and other developed countries were different from developing countries due to legal or volunteer service organizations; thus, the applicability and the effectiveness of the evidence are worth discussing further. Moreover, more refined subgroups of systematic review can be done in the near future; for example, systematic review could be used to quantify the effect of intervention on a certain type of intervention.
Conclusion
The findings provide a tentative indication of the potential benefits of specific types of intervention for improving loneliness/social isolation, advancing theory-informed development of interventions, and improving design of evaluation studies.
Firstly, this study suggests that group and mixed intervention targeting of older adults could be helpful for alleviating social isolation problems. The use of modern technology for remote services could also present good results. Moreover, our systematic review has identified a need for well-conducted studies to improve the evidence base regarding the effectiveness of social interventions for alleviating social isolation. However, more well-conducted RCTs of the effectiveness of social interventions for alleviating social isolation are needed to improve the evidence base.
Because of the debating results, further research is needed to examine the effect of remote interventions from the perspective of process evaluation.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
FT is responsible for analyzing data and writing the draft of the results. CLY is responsible for analyzing the data. FF is responsible for revising the manuscript and submitting the paper. LSW is responsible for writing the literature review. IC is responsible for providing suggestions for revising the paper. All authors contributed to the article and approved the submitted version.
Funding
2019 National Social Science Fund (19BSH173): The Evidence Reorganization, Conversion, and Enlightenment Research of Evidence-based Social Work Intervention on Long-term Care of older adult.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Berger, V. W. (2006). Is the Jadad score the proper evaluation of trials? J. Rheumatol. 33, 1711–1712.
Black, D. S., Irwin, M. R., Olmstead, R. E., Ji, E., Breen, E. C., and Motivala, S. (2014). Tai chi meditation effects on nuclear factor-κB signaling in lonely older adults: a randomized controlled trial. Psychother. Psychosomat. 83, 315–317. doi: 10.1159/000359956
Bøen, H., Dalgard, O. S., Johansen, R., and Nord, E. (2012). A randomized controlled trial of a senior centre group programme for increasing social support and preventing depression in elderly people living at home in Norway. BMC Geriat. 12:20. doi: 10.1186/1471-2318-12-20
Brennan, P. F., Moore, S. M., and Smyth, K. A. (1995). The effects of a special computer network on caregivers of persons with Alzheimer's disease. Nurs. Res. 44, 166–172. doi: 10.1097/00006199-199505000-00007
Canedo-García, A., García-Sánchez, J. N., and Pacheco-Sanz, D. I. (2017). A systematic review of the effectiveness of intergenerational programs. Front. Psychol. 8:1882. doi: 10.3389/fpsyg.2017.01882
Chan, A., Yu, D., and Kai, C. (2017). Effects of tai chi qigong on psychosocial well-being among hidden elderly, using elderly neighborhood volunteer approach: a pilot randomized controlled trial. Clin. Intervent. Aging 12, 85–96. doi: 10.2147/CIA.S124604
Constantino, R. E. (1988). Comparison of two group interventions for the bereaved. J. Nurs. Scholar. 20, 83–87. doi: 10.1111/j.1547-5069.1988.tb00036.x
Cornwell, E. Y., and Waite, L. J. (2009). Social disconnectedness, perceived isolation, and health among elder adults. J. Health Soc. Behav. 50, 31–48. doi: 10.1177/002214650905000103
Czaja, S. J., Boot, W. R., Charness, N., Rogers, W. A., and Sharit, J. (2017). Improving social support for older adults through technology: findings from the PRISM randomized controlled trial. Gerontologist 58, 1–11. doi: 10.1093/geront/gnw249
Díaz, C., and García, J. N. (2016). Identification of relevant elements for promoting effective interventions in old age. Revista de Psicodidáctica, 21, 1–17. doi: 10.1387/RevPsicodidact.13854
Drentea, P., Clay, O. J., Roth, D. L., and Mittelman, M. S. (2006). Predictors of improvement in social support: five-year effects of a structured intervention for caregivers of spouses with Alzheimer's disease. Soc. Sci. Med. 63, 957–967. doi: 10.1016/j.socscimed.2006.02.020
Ferreiraalves, J., Magalhães, P., Viola, L., and Simões, R. (2014). Loneliness in middle and old age. Arch. Gerontol. Geriatr. 59, 613–623. doi: 10.1016/j.archger.2014.06.010
Fratiglioni, L., Wang, H. X., Ericsson, K., Maytan, M., and Winbiad, B. (2000). Influence of social network on occurrence of dementia: a community-based longitudinal study. Lancet 355, 1315–1319. doi: 10.1016/S0140-6736(00)02113-9
Fukui, S., Koike, M., Ooba, A., and Uchitomi, Y. (2003). The effect of a psychosocial group intervention on loneliness and social support for Japanese women with primary breast cancer. Oncol. Nurs. Forum 30, 823–830. doi: 10.1188/03.ONF.823-830
Grenade, L., and Boldy, D. (2008). Social isolation and loneliness among elder people: issues and future challenges in community and residential settings. Austral. Health Rev. 32, 468–478. doi: 10.1071/AH080468
Hall, R. K., Davenport, C. A., Sims, M., Colón-Emeric, C., Washington, T., Russell, J., et al. (2019). Association of functional and structural social support with chronic kidney disease among African Americans: the Jackson Heart study. BMC Nephrol. 20:262. doi: 10.1186/s12882-019-1432-9
Hang, R. H., Liu, X. M., Feng, L. P., and Xing, J. (2011). The effects of psychological intervention on the community Empty Nester the symptoms of depression, loneliness and happiness. China J. Gerontol. 31, 2723–2725. doi: 10.3969/j.issn.1005-9202.2011.14.054
Harris, J. E., and Bodden, J. L. (1978). An activity group experience for disengaged elderly persons. J. Counsel. Psychol. 25, 325–330. doi: 10.1037/0022-0167.25.4.325
Hawton, A., Green, C., Dickens, A. P., Richards, S. H., Taylor, R. S., Greaves, C. J., et al. (2010). The impact of social isolation on the health status and health-related quality of life of elder people. Qual. Life Res. 20, 57–67. doi: 10.1007/s11136-010-9717-2
Heller, K., Thompson, M. G., Trueba, P. E., Hogg, J. R., and Vlachos-Weber, I. (1991). Peer support telephone dyads for elderly women: was this the wrong intervention? Am. J. Community Psychol. 19, 53–74. doi: 10.1007/BF00942253
Higgins, J. P., Altman, D. G., Getzsche, P. C., Juni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 343:d5928. doi: 10.1136/bmj.d5928
Iliffe, S., Kharicha, K., Harari, D., Swift, C., Gillmann, G., and Stuck, A. E. (2007). Health risk appraisal in older people 2: the implications for clinicians and commissioners of social isolation risk in older people. Br. J. General Practice 57, 277–282. doi: 10.1016/S0212-6567(07)70882-X
Kremers, I. P., Steverink, N., Albersnagel, F. A., and Slaets, J. P. (2006). Improved self-management ability and well-being in older women after a short group intervention. Aging Mental Health 10, 476–484. doi: 10.1080/13607860600841206
Lai, D. W., Li, J., Ou, X., and Li, C. Y. (2020). Effectiveness of a peer-based intervention on loneliness and social isolation of older Chinese immigrants in Canada: a randomized controlled trial. BMC Geriat. 20:356. doi: 10.1186/s12877-020-01756-9
Laursen, B., and Hartl, A. C. (2013). Understanding loneliness during adolescence: developmental changes that increase the risk of perceived social isolation. J. Adolesc. 36, 1261–1268. doi: 10.1016/j.adolescence.2013.06.003
Li, J., Ye, H., Tang, Y., Zhou, Z., and Hu, X. (2018). What are the effects of self-regulation phases and strategies for chinese students? A meta-analysis of two decades research of the association between self-regulation and academic performance. Front. Psychol. 9:2434. doi: 10.3389/fpsyg.2018.02434
Li, Z., and Zhou, L. (2002). Epidemiological study on the loneliness of old age. Chinese J. Mental Health 26, 658–662. doi: 10.3969/j.issn.1000-6729.2012.09.004
Liu, Z. R., and Ni, J. (2002). Relevant factors and countermeasures of loneliness among urban elderly. J. Anhui J. Prevent. Med. 8, 326–328. doi: 10.3969/j.issn.1672-6634.2001.02.030
Lökk, J. (1990). Emotional and social effects of a controlled intervention study in a day-care unit for elderly patients. Scand. J. Primary Health Care 8, 165–172. doi: 10.3109/02813439008994951
Lu, R. M., Lin, M. X., and Liu, Y. Z. (2013). On the social isolation and loneliness of the elderly in the urban community, a case study of Yantai city of Shandong province. J. North China Univ. (social science edition) 14, 132–136. doi: 10.3969/j.issn.1009-5101.2013.02.029
Lubben, J., and Gironda, M. (2003). “Centrality of social ties to the health and well-being of older adults,” in Social work and health care in an aging world, eds, B. Berkman and L. Harooytan (New York, NY: Springer), 319–350.
Lund, R., Nilsson, C. J., and Avlund, K. (2010). Can the higher risk of disability onset among elder people who live alone be alleviated by strong social relations? A longitudinal study of non-disabled men and women. Age Ageing 39, 319–326. doi: 10.1093/ageing/afq020
Lunstad, J., Smith, T. B., and Layton, J. B. (2010). Social relationships and mortality risk: a meta-analytic review. PLoS Med. 7:e1000316. doi: 10.1371/journal.pmed.1000316
Ma, J., Liu, Y., Zhong, L. P., Zhang, C. P., and Zhang, Z. Y. (2012). Comparison of Jadad scale and Cochrane bias risk assessment tool in quality evaluation of randomized controlled trials. China J. Oral Maxillofacial Surg. 10, 417–422. Available online at: http://en.cnki.com.cn/Article_en/CJFDTOTAL-ZGKQ201205026.htm.
MacIntyre, I., Corradetti, P., Roberts, J., Browne, G., Watt, S., and Lane, A. (1999). Pilot study of a visitor volunteer programme for community elderly people receiving home health care. Health Soc. Care Commun. 7, 225–232. doi: 10.1046/j.1365-2524.1999.00178.x
Masi, C. M., Chen, H. Y., Hawkley, L. C., and Cacioppo, J. T. (2011). A meta-analysis of interventions to reduce loneliness. Personal. Soc. Psychol. Rev. 15, 219–266. doi: 10.1177/1088868310377394
Methley, A. M., Campbell, S., Chew-Graham, C., Mcnally, R., and Cheraghi-Sohi, S. (2014). Pico, picos and spider: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 14:579. doi: 10.1186/s12913-014-0579-0
Morrow, D. A., Rifai, N., Antman, E. M., Weiner, D. L., and Braunwald, E. (1998). C-reactive protein is a potent predictor of mortality independently of and in combination with troponin t in acute coronary syndromes: a timi 11a substudy. thrombolysis in myocardial infarction. J. Amer. Cardiol., 31, 1460–1465.
Morrow-Howel, N., Becker-Kemppainen, S., and Judy, L. (1998). Evaluating an intervention for the elderly at increased risk of suicide. Res. Soc. Work Practice 8, 28–46. doi: 10.1177/104973159800800104
Mountain, G., Hind, D., Gossage-Worrall, R., Walter, S. J., Duncan, R., Newbould, L., et al. (2014). ‘Putting Life in Years’ (PLINY) telephone friendship groups research study: pilot randomised controlled trial. Trails 15:141. doi: 10.1186/1745-6215-15-141
Nan, J. J., and Dong, B. (2019). Research on the pension problem of rural one-child family from the perspective of social work – taking a village in Shandong Province as an example. Aging Res. 6, 31–36. doi: 10.12677/AR.2019.63005
Ollonqvist, K., Palkeinen, H., Aaltonen, T., Pohjolainen, T., Puukka, P., and Hinkka, K. (2008). Alleviating loneliness among frail elder people–findings from a randomised controlled trial. Int. J. Mental Health Promot. 10, 26–34. doi: 10.1080/14623730.2008.9721760
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst. Rev. 1:89. doi: 10.1186/s13643-021-01626-4
Petersen, N., Knig, H. H., and Hajek, A. (2020). The link between falls, social isolation and loneliness: a systematic review. Arch. Gerontol. Geriatrics 88:104020. doi: 10.1016/j.archger.2020.104020
Poscia, A., Stojanovic, J., La Milia, D., Duplaga, M., Grysztar, M., Moscato, U., et al. (2018). Interventions targeting loneliness and social isolation among the older people: an update systematic review. Exp. Gerontol. 102, 133–144. doi: 10.1016/j.exger.2017.11.017
Ristolainen, H., Kannasoja, S., Tiilikainen, E., Hakala, M., Närhi, K., and Rissanen, S. (2020). Effects of participatory group-based care managementon well-being of older people living alone: A randomized controlled trial. Arch. Gerontol. Geriatr. 89:104095. doi: 10.1016/j.archger.2020.104095
Routasalo, P. E., Tilvis, R. S., and Kautiainen, H. (2009). Effects of psychosocial group rehabilitation on social functioning, loneliness and well-being of lonely, elder people: randomized controlled trial. J. Adv. Nurs. 65, 297–305. doi: 10.1111/j.1365-2648.2008.04837.x
Saito, T., Kai, I., and Takizawa, A. (2012). Effects of a program to prevent social isolation on loneliness, depression, and subjective well-being of elder adults: a randomized trial among elder migrants in Japan. Arch. Gerontol. Geriatr. 55, 539–547. doi: 10.1016/j.archger.2012.04.002
Savelkoul, M., and de Witte, L. P. (2004). Mutual support groups in rheumatic diseases: effects and participants' perceptions. Arthritis Rheum. 51, 605–608. doi: 10.1002/art.20538
Schulz, R. (1976). Effects of control and predictability on the physical and psychological well-being of the institutionalized aged. J. Personal. Soc. Psychol. 33, 563–573. doi: 10.1037/0022-3514.33.5.563
Slegers, K., van Boxtel, M. P. J., and Jolles, J. (2008). Effects of computer training and Internet usage on the well-being and quality of life of elder adults: a randomized, controlled study. J. Gerontol. Series B Psychol. Sci. Soc. Sci. 63, 176–184. doi: 10.1007/BF03324898
Stojanovic, J., Collamati, A., La Milia, D., Borghini, A., Duplaga, M., Rodzinka, M., et al. (2016). Targeting loneliness and social isolation among the elderly: an update systematic review. Europ. J. Public Health 26(suppl_1), 10–11. doi: 10.1093/eurpub/ckw164.010
Victor, C., Scambler, S., Bond, J., and Bowling, A. (2010). Being alone in later life: loneliness, social isolation and living alone. Rev. Clin. Gerontol. 10, 407–417. doi: 10.1017/S0959259800104101
White, H., McConnell, E., Clipp, E., Branch, L. G., Sloane, R., Pieper, C., et al. (2002). A randomized controlled trial of the psychosocial impact of providing internet training and access to elder adults. Aging and Mental Health 6, 213–221. doi: 10.1080/13607860220142422
Keywords: social isolation, loneliness, older adults, health, systematic review, intervention
Citation: Tong F, Yu C, Wang L, Chi I and Fu F (2021) Systematic Review of Efficacy of Interventions for Social Isolation of Older Adults. Front. Psychol. 12:554145. doi: 10.3389/fpsyg.2021.554145
Received: 21 April 2020; Accepted: 06 July 2021;
Published: 07 September 2021.
Edited by:
Fergus Gracey, University of East Anglia, United KingdomReviewed by:
Cristina Queiros, University of Porto, PortugalJesús-Nicasio García-Sánchez, Universidad de León, Spain
Copyright © 2021 Tong, Yu, Wang, Chi and Fu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fang Fu, fufang812@163.com