 Diego Gaddi1
Diego Gaddi1 Angelo Mosca2
Angelo Mosca2 Massimiliano Piatti1Daniele Munegato1Marcello Catalano2Giorgia Di Lorenzo2
Massimiliano Piatti1Daniele Munegato1Marcello Catalano2Giorgia Di Lorenzo2 Marco Turati1,2,3,4,5*
Marco Turati1,2,3,4,5* Nicolò Zanchi1
Nicolò Zanchi1 Daniele Piscitelli2,6,7Kevin Chui8Giovanni Zatti1,2,4,5Marco Bigoni1,2,4,5
Daniele Piscitelli2,6,7Kevin Chui8Giovanni Zatti1,2,4,5Marco Bigoni1,2,4,5- 1Orthopedic Department, San Gerardo Hospital, University of Milano-Bicocca, Monza, Italy
- 2Department of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy
- 3Department of Paediatric Orthopedic Surgery, University Hospital Grenoble-Alpes, University Grenoble-Alpes, Grenoble, France
- 4Transalpine Center of Pediatric Sports Medicine and Surgery, University of Milano-Bicocca, Monza, Italy
- 5Hospital Couple Enfant, Grenoble, France
- 6School of Physical and Occupational Therapy, McGill University, Montréal, QC, Canada
- 7Department of Kinesiology, University of Connecticut, Storrs, CT, United States
- 8Department of Physical Therapy, Waldron College of Health and Human Services, Radford University, Roanoke, VA, United States
Even though ankle sprains are among the most frequent musculoskeletal injuries seen in emergency departments, management of these injuries continues to lack standardization. Our objective was to carry out an umbrella review of systematic reviews to collect the most effective evidence-based treatments and to point out the state-of-the-art management for this injury. PubMed, Scopus, Web of Science, and the Cochrane library were searched from January 2000 to September 2020. After removing duplicates and applying the eligibility criteria, based on titles and abstracts, 32 studies were screened. At the end of the process, 24 articles were included in this umbrella review with a mean score of 7.7/11 on the AMSTAR quality assessment tool. We found evidence supporting the effectiveness of non-surgical treatment in managing acute ankle sprain; moreover, functional treatment seems to be preferable to immobilization. We also found evidence supporting the use of paracetamol or opioids as effective alternatives to non-steroidal anti-inflammatory drugs to reduce pain. Furthermore, we found evidence supporting the effectiveness of manipulative and supervised exercise therapy to prevent re-injury and restore ankle dorsiflexion.
Introduction
During sports activities, especially indoor sports (1) (e.g., volleyball, basketball, and dance), acute ankle sprains are very common, with considerable diagnostical and treatment costs for healthcare systems and high socioeconomic impact due to absenteeism from work (2). Epidemiological data have shown that ~80% of individuals will suffer an ankle sprain during their lifetime (3, 4). This injury is more frequent in women than in men; likewise, children are more affected than adolescents and adults: the progressive development of coordination patterns and neuromuscular control plays a protective role (5–8).
Less than 15% of acute ankle sprains are coupled with a fracture of the ankle or foot, suggesting that the damage mainly concerns soft tissues. Recently, Romero-Morales et al. (9) showed a decreased thickness of the plantar fascia in individuals with lateral ankle sprain when compared with healthy subjects. X-rays are required in 77–99% of cases (10, 11). Based on the anatomical classification, we can identify three types of ankle sprain patterns, namely, lateral, syndesmotic, and medial. Ankle sprains involve the lateral ligament group (~85%), because it is less resistant to load, so it is easier to injure compared with the others ligament groups (12). The lateral ankle ligament is composed of the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL) (10). The ATFL is the weakest and when it is damaged it causes an antero-posterior instability, while the involvement of the CFL turns into an inversion instability. In emergency departments, a clinical classification is more valuable. We can divide acute ankle sprain into three different grades (Table 1): grade I injuries ligaments are only stretched without macroscopic tearing; grade II injuries show partial tear of ligaments, frequently with a complete tear of the ATFL and an additional partial tear of the CFL; and finally grade III injuries are associated with complete tear of ligaments with disruption of both the ATFL and CFL, capsular tear could be associated.

Table 1. Classification of lateral ankle sprain based on increasing ligamentous damage and morbidity.
Although several studies on acute ankle sprain are available, there is a considerable variety of classifications, follow-up times, treatments, outcome measures, and endpoints. Ankle sprain treatment ranges from physical therapy [e.g., orthoses, functional exercise, strength, and endurance (13)] to pharmacology support and orthopedic surgery. Thus, it is difficult to propose a standard algorithm to manage and treat an acute ankle sprain when it occurs in the emergency department. Moreover, a systematic review of published clinical practice guidelines for the treatment of acute lateral ankle sprains revealed that their quality was poor (14). Therefore, this study reviews literature on the different treatments proposed for acute ankle sprain. Specifically, by means of an umbrella review of systematic reviews, we analyze and describe the state-of-the-art management of this injury.
Materials and Methods
Focused Question Based
This study is an umbrella review of systematic reviews. Following the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) (15) guidelines, we developed a specific foreground question that focused on the management of ankle sprains. The following PICO was formulated: Population: adults with acute ankle sprain; Intervention and Comparison: conservative and surgical treatments; Outcomes: pain, swelling, range of motion, instability, function, reinjury rate, and return to sport (see Section Search Strategy and Study Selection for additional details).
Eligibility Criteria
We only considered articles that satisfy the following eligibility criteria: (i) the study must be a systematic review, with or without a meta-analysis; (ii) it must assess the suitability of an intervention for the treatment or prevention of ankle sprains; and (iii) the population examined must not include chronic ankle instability. We have excluded studies dealing exclusively with epidemiology, etiopathogenesis, and diagnosis of ankle sprains. We have also excluded studies concerning pediatric patients. We have included all types of treatments.
Search Strategy and Study Selection
We conducted a comprehensive literature search on PubMed, Scopus, Web of Science, and the Cochrane library from 2000 up to September 2020. We included only systematic reviews and meta-analyses in order to analyze the highest level of evidence and to increase the external validity of the present study.
We developed our research using the following keywords: (a) “ankle” AND “sprain”; (b) “ankle sprain” AND “management”; (c) “ankle sprain” AND “treatment”. No fields in the search engines were specified in order to expand the research (e.g., in PubMed the word “treatment” was translated by the search engine as “therapeutics” [MH] OR “therapeutics” [All Fields] OR “treatments” [All Fields] OR “therapy” [Subheading] OR “therapy” [All Fields] OR “treatment” [All Fields] OR “treatment's” [All Fields]). As a result, we found 3,500 citations. Different authors screened all the articles found, first removing duplicates, and then applying the eligibility criteria based on titles and abstracts; the 32 remaining studies were checked a second time by reading them and applying eligibility criteria to identify a list of relevant articles. Any disagreement was resolved by discussion among all the authors (Figure 1). Another eight studies were then removed, leaving a total of 24 articles for this umbrella review.
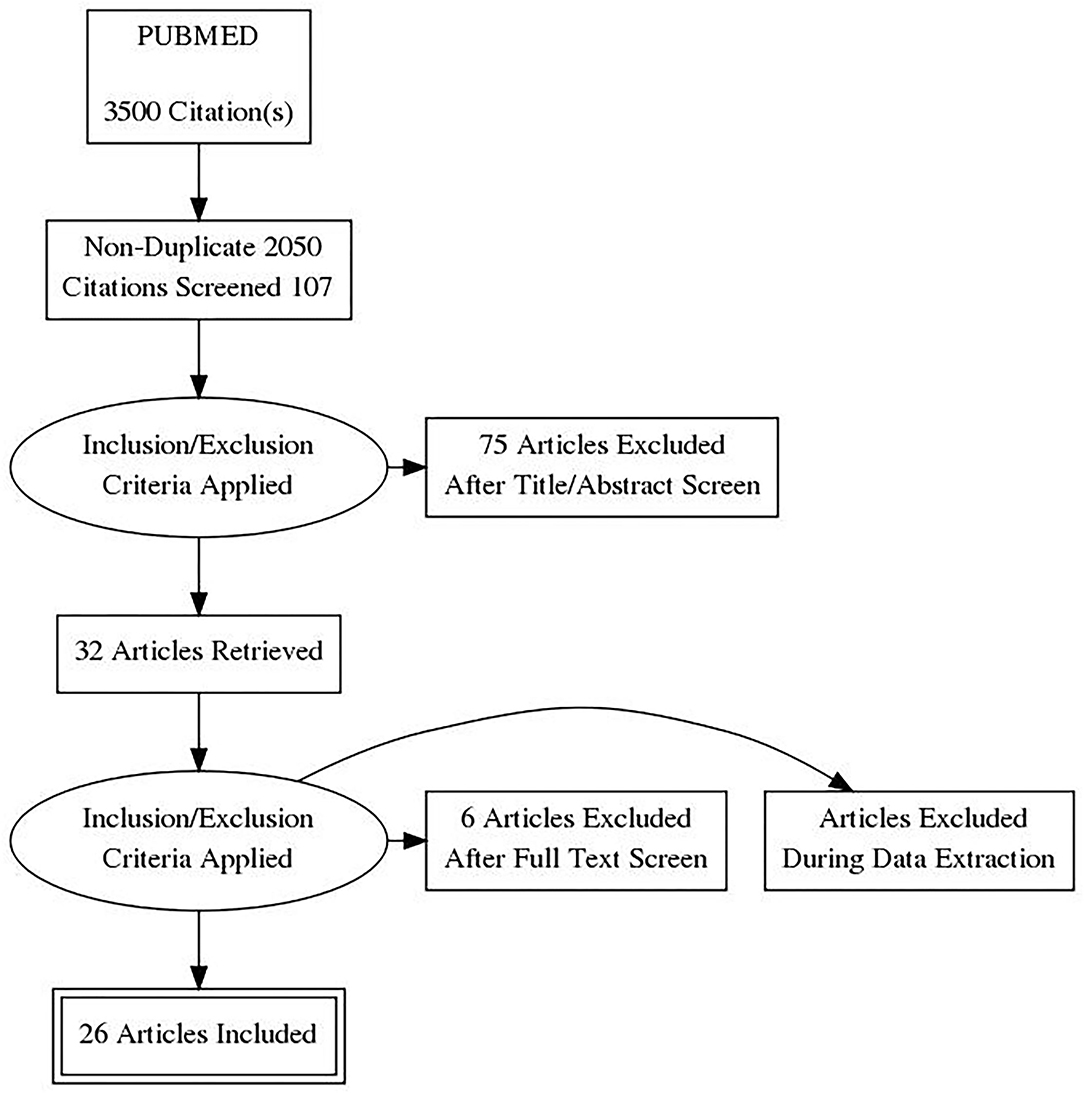
Figure 1. PRISMA flow diagram.
Regarding treatments, we considered both conservative and surgical strategies. Among non-surgical interventions, we reported acute treatment [e.g., RICE (rest, ice, compression, elevation) therapy, immobilization, taping, and bracing], drugs [including NSAIDs (non-steroidal anti-inflammatory drugs) and other medications], rehabilitation and manual therapy (e.g., proprioceptive, coordination and strength training, supervised exercises, and manipulative therapy), and complementary therapies (e.g., acupuncture and electrical stimulation). We selected these categories according to a literature review. Different outcomes have been assessed, including pain, swelling, range of motion, instability, function, and reinjury rate. In our study, we also focused on return to sport.
Methodological Study Quality Assessment
Two authors (DG and MC) independently assessed the quality of the systematic reviews using the AMSTAR tool (16). Any disagreement was resolved by group discussion and consensus.
Consistent with the methods used by Doherty et al., we decided to assess the review as “high” or “low” quality, based on a score of 7/11 on the AMSTAR quality rating. This quality threshold was used to conduct the best evidence synthesis of reviews (17).
Results
Study Selection
We performed our research following PRISMA guidelines (15), as shown in Figure 1. In the beginning, we collected 3,500 studies. At the end of the process, only 24 systematic reviews met the eligibility criteria and were therefore included, with a mean AMSTAR score of 7.7/11 (Table 2 shows the quality of the selected articles, first author, and year of publication).
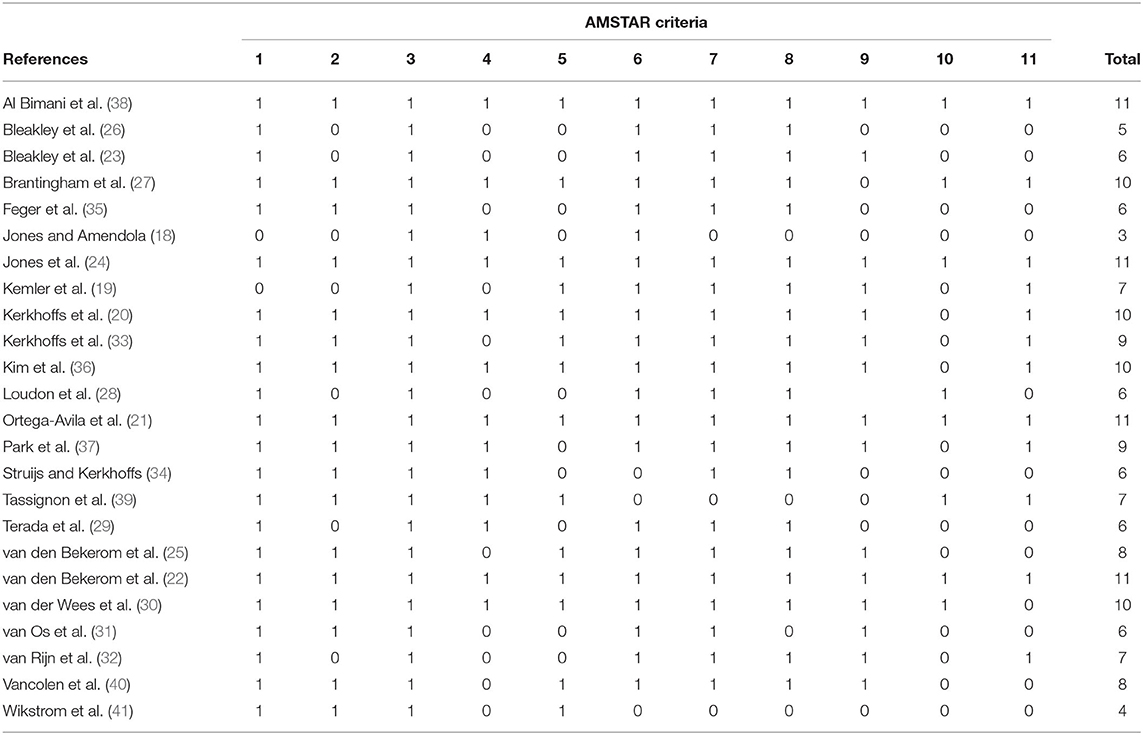
Table 2. Quality assessment of the included studies according to the AMSTAR scale.
All the studies considered investigated treatment strategies for acute ankle sprains. Six reviews investigated specifically acute treatment (18–23) (AMSTAR range 3–11). Two reviews evaluated drug therapy (24, 25) (AMSTAR range 8–11). Seven reviews evaluated rehabilitation and manual therapy (26–32) (AMSTAR range 5–10). Two reviews evaluated surgical treatment (33, 34) (AMSTAR range 6–9). Three reviews analyzed other treatments (35–37) (AMSTAR range 6–10). Finally, four reviews considered return to sport (38–41) (AMSTAR range 4–11). Table 3 summarizes the results and conclusions of included studies, grouped based on the intervention type. While several studies could have been assigned to more than one strategy, each review was noted once in Table 3, and the assignment was based on the primary focus of the review.
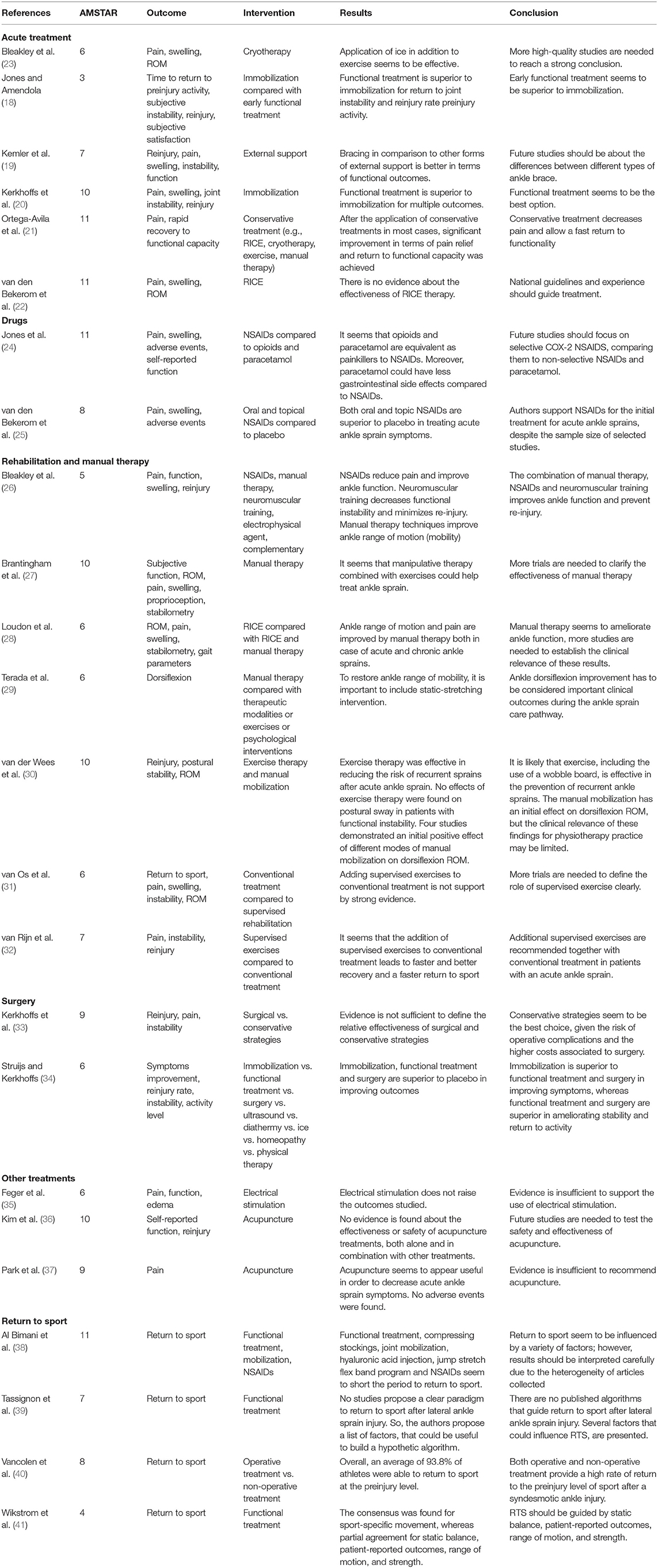
Table 3. Results of the best evidence synthesis from the reviews.
Acute Treatment
Bleakley et al. (23) (AMSTAR 6) included 22 studies involving 1,469 participants to analyze the effectiveness of cryotherapy to manage acute soft-tissue damage. Concerning acute ankle sprain, there is marginal evidence that cryotherapy is effective if it is added to exercises during the management of the early stages of this injury. They do not find consensus about cryotherapy duration and the method with which ice should be used (23).
Jones and Amendola (18) (AMSTAR 3) included 9 studies involving 920 subjects to compare immobilization to early functional treatment. They reported that functional treatment allows earlier return to sport and to work, while there is no substantial difference concerning instability and re-injury rate, although studies seem to favor early functional treatment.
Kemler et al. (19) (AMSTAR 7) included nine studies involving 1,250 patients to compare braces to other functional treatment types. They found no differences concerning time to return to pre-injury activities, time to reduce symptoms, re-injury, and joint instability rates, but it seems that braces have better functional outcomes using the Foot and Ankle Outcome Score and Karlsson scoring scale.
Kerkhoffs et al. (20) (AMSTAR 10) included 22 studies involving 2,157 participants to analyze immobilization as a treatment for acute ankle sprains. They found that functional treatment has better results considering time to return to pre-injury activities, swelling reduction, joint stiffness, and subjective and objective joint instability. They did not find any differences for recurrence or pain.
Ortega-Avila et al. (21) (AMSTAR 11) included 20 studies, involving 2,236 subjects, to demonstrate that conservative treatment (e.g., RICE, cryotherapy, exercise, and manual therapy) effectively manages pain and functional recovery.
van den Bekerom et al. (22) (AMSTAR 11) included 11 studies, involving 868 patients to examine the evidence about RICE therapy during the management of acute ankle sprain. Even if it seems that early post-traumatic immobilization is beneficial, they do not find sufficient evidence to support the effectiveness of RICE therapy.
Drugs
Jones et al. (24) (AMSTAR 11) included 20 studies involving 3,305 subjects to compare the ability of paracetamol, opioids, and NSAIDs to reduce acute ankle sprain symptoms (e.g., pain, loss of function, and swelling) and side effects. The most important finding is that NSAIDs and paracetamol are equivalent in reducing pain at a 3-day follow-up; they also found no statistically significant differences in pain relief between NSAIDs and opioids. They concluded with a high grade of uncertainty that NSAIDs seem to reduce swelling and allow a faster return to normal activities than paracetamol and opioids, but more studies are needed to confirm these results. Opioids cause more gastrointestinal and neurological side effects than NSAIDs, while NSAIDs induce more gastrointestinal side effects than paracetamol.
van den Bekerom et al. (25) (AMSTAR 8) included 28 studies involving 3,447 patients to analyze the effectiveness of oral and topical NSAIDs to treat acute ankle sprains. No trials compared the effectiveness of oral and topical routes of delivery. The most important finding is that independent of the pharmaceutical form, NSAIDs effectively decrease pain and swelling at least on short-term follow-up.
Rehabilitation and Manual Therapy
Bleakley et al. (26) (AMSTAR 5) included 23 studies, involving 3,027 patients to analyze if the combination of conservative strategies in addition to supervised exercises with external support could increase functional outcomes after acute ankle sprains. The most important finding is that independent of the pharmaceutical form, the NSAIDs effectively decrease pain and swelling on short-term follow-up. Moreover, manual therapy seems to improve ankle range of motion if applied in the early phases of an acute ankle sprain; finally, supervised neuromuscular training appears to decrease the re-injury rate.
Brantingham et al. (27) (AMSTAR 10) included 19 studies, involving 2,363 patients, to examine the state-of-the-art supporting manipulative therapy of the lower limb. According to these authors, manipulative therapy and supervised exercises are effective for short-term treatment of acute ankle sprain.
Loudon et al. (28) (AMSTAR 6) included 8 studies, involving 244 patients to determine the effectiveness of manipulative therapy in cases of lateral ankle sprains. According to these authors, manual therapy seems to improve ankle range of motion and decrease pain.
Terada et al. (29) (AMSTAR 6) included 9 studies, involving 196 patients to estimate the effectiveness of treatments to restore dorsiflexion after an acute, recurrent, and chronic ankle sprain. According to these authors, static-stretching for triceps surae included in a standardized rehabilitation program may improve ankle dorsiflexion after an acute sprain.
van der Wees et al. (30) (AMSTAR 10) included 17 studies involving 2,376 patients to analyze supervised exercises and manipulative therapy outcomes in patients with acute ankle sprain or instability. The most important finding is that exercise therapy helps to prevent recurrent ankle sprains. Moreover, manual mobilization seems to positively effect restoring ankle range of motion.
van Os et al. (31) (AMSTAR 6) included 7 studies, involving 436 patients, to compare supervised rehabilitation training to conventional treatment to manage acute lateral ankle sprains. It seems that supervised rehabilitation training added to conventional treatment may have better outcomes when compared to conventional treatment alone.
van Rijn et al. (32) (AMSTAR 7) included 11 studies involving 776 patients to determine the effectiveness of supervised rehabilitation training added to conventional treatment compared with conventional treatment alone. The authors reported that supervised rehabilitation training may produce a shorter recovery period and an earlier return to sports activities.
Surgery
Kerkhoffs et al. (33) (AMSTAR 9) included 20 studies involving 2,562 patients to compare conservative treatment to surgical treatment in acute lateral ankle sprain injury. The evidence reviewed was insufficient to determine the relative effectiveness of surgical and conservative strategies for managing acute lateral ankle sprains.
Struijs and Kerkhoffs (34) (AMSTAR 6) included 38 studies involving 9,976 patients to analyze ankle sprain treatments. They found that surgery was able to decrease the number of patients who did not return to sports and who develop clinical instability.
Other Treatments
Feger et al. (35) (AMSTAR 6) included 4 studies involving 162 participants, but they do not find any statistically significant results to support the effectiveness of electrical stimulation in reducing symptoms or improving functional outcomes.
Kim et al. (36) (AMSTAR 10) included 20 studies involving 2,012 subjects. When comparing acupuncture vs. no acupuncture, and acupuncture vs. another non-surgical intervention, they do not find any statistically significant results.
Park et al. (37) (AMSTAR 9) included 17 studies involving 1,820 patients to examine the effectiveness of acupuncture to reduce patients' global symptoms and pain, especially as an add-on treatment. However, they do not recommend using this practice due to the limited number of studies and insufficient high-quality evidence.
Return to Sport
Al Bimani et al. (38) (AMSTAR 11) included 14 studies involving 1,142 patients to find a consensus about influencing factors for return to play after an acute ankle sprain is treated conservatively. According to these authors, many factors should be considered as influential factors in return to play.
Tassignon et al. (39) (AMSTAR 7) failed to find studies that establish algorithms to define the process to return to sport (RTS) for patients with a lateral ankle sprain, so they proposed variables that could be used for criteria-based RTS decision paradigm.
Vancolen et al. (40) (AMSTAR 8) included 10 studies, involving 333 patients to evaluate the rate of RTS after a syndesmotic ankle injury. According to the authors, most patients can return to sport at the preinjury level in both non-operative and operative treatment groups.
AMSTAR 4 included 11 studies to find consensus among expert opinions about items that have to be considered to develop an RTS criterion for the management of lateral ankle sprain. They found several important criteria, including sport-specific movement, static balance, patient-reported outcomes, range of motion, and strength.
Discussion
Despite the fact that acute ankle sprains are among the most commonly seen injuries in the emergency department, a standardized protocol for its management has not been established. Furthermore, the heterogeneity of interventions and outcomes examined in this revision, and the range in quality of these studies make it difficult to propose a standard algorithm for acute ankle sprain management. Based on this umbrella review, non-surgical treatment is effective to manage acute ankle sprains, and functional treatment seems to be superior when compared to immobilization. Moreover, paracetamol and opioids are as effective as NSAIDs in reducing pain, thus they represent an alternative treatment option. Manipulative and exercise therapy could be also recommended, especially during the initial recovery phase, to prevent reinjury, and to restore dorsiflexion.
Acute Treatment
After an acute ankle sprain, during the first few days (48–72 h), the most used treatment protocol is RICE therapy, which consists of a combination of rest, ice, compression, and elevation. Rest reduces the metabolic tissue demand, decreasing the amount of blood circulating in the damaged area. Ice induces vasoconstriction, it brings down the temperature, diminishing the metabolic rate of cells. It also fights against exudate formation and hemorrhaging, which are responsible for the swelling. Finally, ice has an analgesic role, which is also used in the rehabilitation phase in order to facilitate exercises. Compression limits the swelling and stops hemorrhaging, while elevation improves lymph drainage and venous circulation (22, 23). Although several guidelines promote this approach, there are few studies that demonstrate the effectiveness of this therapy, in part due to several difficulties that exist when researchers try to create a study protocol (22). For example, most patients apply ice before going to the hospital and there are many different ways to use cryotherapy, including mode, duration, and frequency of application (23).
After the acute medical care, various treatments exist to manage the acute ankle sprain. Nevertheless, they can be classified into three main groups, namely, (1) conservative or conventional, which includes immobilization with cast or splint, (2) functional, which consists of early mobilization added to external supports, such as tapes, elastic bandages, and braces, in order to protect the joint from the risk of re-injury, as well as coordination training, and (3) surgery (20).
According to our revision, functional treatment represents a better choice than conservative treatment: fewer patients suffer from swelling, ROM limitations, joint stiffness, and joint instability. Moreover, patients are more satisfied, and they return earlier to their pre-injury work and sports activities; thus, the associated social costs could also be reduced (18–21). As far as recommending a functional treatment as the first choice to manage an acute ankle sprain, there are few studies that compare different types of external supports, even if it seems that some types of braces could be superior based on patient outcomes (19). We, therefore, recommend that more studies are needed to understand which types of external support to use with functional treatment.
Drugs
To reduce swelling, reduce pain, and decrease the time to return to work, NSAIDs are the most commonly used medications in the treatment of ankle sprains, as they have both analgesic and anti-inflammatory effects. Swelling and pain are mediated by the inflammation process, which is also a part of healing; NSAIDs, however, can impair this process. The most common side effect is gastrointestinal bleeding, but they can cause other problems such as bronchospasm or renal failure. The advent of COX-2 selective NSAIDs has recently decreased gastrointestinal side effects at the cost of higher cardiovascular risk (24). NSAIDs are usually prescribed in an oral or topical form, which are both more effective than a placebo. However, we have not found studies comparing the two different formulations (25). Other drugs, customarily used, are paracetamol and opioids, alone or combined with each other, which does not have an anti-inflammatory effect. Opioids act centrally and peripherally on their specific receptors, while the mechanism of paracetamol is not fully clear, although it seems to involve several central pathways, including prostaglandin, serotonergic, nitric oxide, and cannabinoid ones. Paracetamol is hepatotoxic, while opioids are known to cause nausea, respiratory depression, sedation, vomiting, constipation, and dysphoria. Regarding pain, there is no evidence of a difference between paracetamol and NSAIDs; however, paracetamol seems to have fewer gastrointestinal side effects. Considering pain, NSAIDs and opioids would be equivalent, but NSAIDs would have fewer gastrointestinal and neurological side effects. NSAIDs seem to reduce swelling and help regain function better than paracetamol and opioids, but according to our review, we need more studies to confirm these results with a higher grade of certainty (24). We recommend the use of paracetamol or opioids as effective alternatives to NSAIDs for pain reduction. More studies are needed that focus on the impact of COX-2 selective NSAIDs and different pharmaceutical formulations of these drugs.
Rehabilitation and Manual Therapy
Several ankle sprain rehabilitation programs are available with different methods and exercises, practiced alone or in combination with other specific treatments. Functional treatment is the combination of an external device that supports the ankle with a rehabilitation program, which includes early joint mobilization. Many functional treatment programs exist, but it is not clear which program produces the best outcomes including preventing reinjury, and whether supervised exercises are superior to conventional treatment. Conventional treatment includes all types of external support, which allow at most partial joint mobility, combined with standard non-supervised exercises, application of ice, and partial weight-bearing (30). Instead, this conventional treatment could be combined with rehabilitation supervised by a physical therapist that usually begins within 2 weeks from the injury, and emphasizes balance training and coordination exercises. According to our review, no strong evidence was found demonstrating the superiority of supervised exercises to conventional treatment, especially if we consider outcome measures at short-term follow-up (27, 32).
Restoring the ankle dorsiflexion of the ankle and preventing joint stiffness are key goals of rehabilitation programs because the loss of range of motion is a risk factor for recurrent sprains and chronic joint instability. Different interventions and rehabilitation programs are proposed, including proprioceptive training, coordination training, strength training, functional exercises, and manual mobilization. However, the most effective method of ensuring such a restoration is yet to be determined (30).
According to our review, the effectiveness of manual therapy to improve ankle dorsiflexion seems to be limited to the early stages of rehabilitation (30). Its effects have to be linked to increasing triceps surae flexibility with static-stretching exercises, which could also be performed at home, decreasing the need for treatment in terms of time (29).
However, at the same time, it is important to keep in mind that many factors contribute to limitations in ankle range of motion, such as pain, muscle spasm, and swelling, so analgesics, myorelaxants, and anti-oedema drugs, as well as manipulative therapy and lymphatic drainage may also help to restore ankle dorsiflexion. Therefore, a multimodal approach is needed to establish which factors are reducing the range of motion in order to select the most appropriate interventions (28, 29).
Motor control plays a key role in walking and feed forward postural mechanisms (8, 42, 43); however, following an ankle sprain, lower limb muscle activation patterns may be altered (44), thus another popular intervention is neuromuscular training, particularly using the wobble balance board in the sub-acute phase, to improve proprioception that seems to prevent re-injury (26).
Surgery
Surgical treatment of acute ankle sprain generally consists of primary repair of torn ligaments with suturing. Kerkhoffs et al. (33) analyzed trials comparing surgical interventions with conservative management and most of the evidence found was not sufficient to demonstrate effectiveness. However, they found some evidence that may demonstrate the superiority of surgery to improve stability as objectively measured by a positive talar tilt or positive anterior drawer sign on stress radiographs; nevertheless, the clinical relevance of these differences remains unclear. Moreover, surgery is associated with an increased risk of stiffness and limitations in ankle mobility, higher costs, and additional complications associated with surgery itself, including infection and deep vein thrombosis. It should be noted that ankle and foot surgery showed growing interest over the last decade (45, 46).
Struijs and Kerkhoffs (34) found that surgery is superior to immobilization with respect to RTS and objectively decreasing instability. At the same time, however, they did not find relevant differences in clinical and functional outcome measures. Similarly, no differences were found when surgery was compared with functional treatment.
Due to the inconclusive and conflicting data about the efficacy and safety of surgical intervention, in our opinion, more studies are needed before recommending surgery as the first option of treatment; however, we think that surgery should be considered when patients with persistent symptoms such as chronic ankle joint instability are non-responsive to other treatments.
Other Treatments
Alternative medicine practices such as acupuncture and electrical stimulation have also been used to treat acute ankle sprains.
Electrical stimulation is an electrical current produced from an external device that is applied to the body using an electrode. The electrical current can depolarize sensory or motor nerve fibers, curb the formation of edema, and facilitate tissue healing. In theory, different types of electrical stimulation could be used, such as high-voltage pulsed electrical stimulation and neuromuscular electrical stimulation. High-voltage pulsed electrical stimulation is used to suppress edema development by modifying cell permeability. In contrast, neuromuscular electrical stimulation is used to facilitate muscle contractions, which in turn improves venous and lymphatic return and decreases edema. According to our revision, no evidence exists to support the effectiveness of electrical stimulation in the management of acute ankle sprains (35).
Concerning acupuncture, some studies would advocate its effectiveness, especially as an add-on treatment during pain management in grade I and II ankle sprains; moreover, it seems to be more effective than a placebo. Nevertheless, these results are based on subjective parameters such as patient-reported global symptom improvement or patient-reported functional assessment and studies with a few patients, so results can be overestimated. Furthermore, no study demonstrates a statistically significant result when acupuncture was compared with NSAIDs as a single treatment or add-on treatment. Moreover, almost all studies are conducted in China, where acupuncture is an ancient medical technique that is widely integrated into their culture and healthcare system, so further research is needed to establish the acceptance of this practice in other countries (36, 37).
Acupuncture may represent another pain management option to reduce the use of medications; therefore, more clinical trials are required to examine the effectiveness of acupuncture to treat acute musculoskeletal injuries, especially as an add-on treatment, and to test the acceptance of this practice in cultures outside of China. Moreover, in our opinion, it will be important to analyze the efficacy of acupuncture using objective parameters and performance-based functional scores.
Return to Sport
Many athletes develop long-term symptoms, defined as chronic ankle instability, and it is still debated whether early RTS plays a role in this. The key concerns with chronic ankle instability are the increased risk of reinjury and its sequelae such as post-traumatic osteoarthritis, instability, stiffness, muscle hypotonicity, pain, swelling, and functional loss and disability (47, 48). The range of time to RTS is often based on the severity of the injury. A typical grade I lateral ankle sprain may take 2–6 weeks to RTS and a more severe syndesmotic injury takes an average of 46.4 days to RTS (40).
According to our review, many studies separately investigate influencing factors for RTS, but they failed to determine a paradigm (38). The decision about RTS should include balance, proprioception, strength, range of motion, agility tests, and psychological stress. It is important to evaluate both intrinsic modifiable risk factors, such as balance, endurance, muscle strength, range of motion, and extrinsic risk factors, such as the playing surface or environmental conditions (39). An opinion shared by many experts is that a crucial element when determining an athlete's readiness for RTS is the need to assess sport-specific movements, and consequently, each practitioner is encouraged to establish an objective scale to standardize lateral ankle sprain RTS decisions (41). The idea that the time since the injury (trauma) is the primary criterion for determining RTS readiness has been overcome.
In the same way, the grading of injuries based on physical exam findings (e.g., special tests) or the histological damage seen on diagnostic images is of limited value when determining RTS, especially considering the inherent difference between these injuries and the different types of treatment athletes receive. A definition that unifies these criticalities considers the RTS as a dynamic decision-making model, organized in three consecutive phases, which are based on the recovery of each individual athlete. These three phases are identified as (49).
- “return to participation,” in which the athlete is allowed to train but not perform.
- “return to sport,” in which the athlete performs but not at the levels desired before trauma.
- “return to performance,” in which an athlete returns to their pre-injury level and which is considered the goal condition.
Future studies should investigate the different variables that could influence RTS and develop a decision paradigm based on objective criteria and thresholds, possibly introducing a different paradigm based on the specific sport examined. Moreover, in adults older than 40 years who could suffer from osteoarthritis, strategies for reducing central pain mechanisms should be considered (50), taking into account that validated questionaries are available to clinicians to measure several personal factors [e.g., fear avoidance beliefs (51) and pain catastrophizing (52)].
Limitations
Our review has some potential limitations such as articles not identified due to publication bias or bad indexing. According to the eligibility criteria, clinical practice guidelines were not included, thus we may have not included nested systematic reviews developed during the clinical guideline process. We have not considered articles written in languages, which are not English. The risk of bias of the included systematic reviews and meta-analyses has been performed using the AMSTAR tool; other instruments, e.g., the ROBIS tool (53), could be used for this purpose. We decided to administer the AMSTAR tool for its feasibility, reliability, and validity (16).
Conclusion
There is an abundance of literature that examines ankle sprains, but results are often inconclusive and difficult to compare and contrast. In this article, we evaluated the most common treatments for acute ankle injuries and assessed the level of evidence for each systematic review.
There is high-quality evidence about the effectiveness of non-surgical treatment in managing acute ankle sprain. We also recommend functional treatment rather than immobilization.
Paracetamol or opioids are effective for reducing pain in this population and could be used as an alternative to NSAIDs. Manipulative and exercise therapy should be advised to prevent re-injury and restore dorsiflexion, especially if they are begun early during the initial phase of ankle sprain management.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
Study conception: DG, DM, MP, MC, MB, GZ, and MT. Design of the study: DG, MC, MT, AM, DP, MP, DM, MB, GZ, and NZ. Literature search and data analysis: DG, MP, DM, MC, AM, GD, MT, DP, and NZ. Analysis of the results and drafting the manuscript: DG, MP, DM, MC, AM, GD, DP, MT, MB, GZ, NZ, and KC. Manuscript final revision: MT, AM, DP, MB, GZ, and KC. All authors of this article have read and approved the final version submitted.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
This study was planned and performed due to the close collaboration of several institutions and departments, including the Orthopedic Department, San Gerardo Hospital, University of Milano-Bicocca; Department of Medicine and Surgery, University of Milano-Bicocca, Monza, Italy; Department of Pediatric Orthopedic Surgery, University Hospital Grenoble-Alpes, University Grenoble-Alpes, Grenoble, France; Transalpine Center of Pediatric Sports Medicine and Surgery, University of Milano-Bicocca, Monza, Italy; Hospital Couple Enfant, Grenoble, France; School of Physical and Occupational Therapy, McGill University, Montréal, Canada; Department of Physical Therapy, Radford University, Roanoke, VA.
Abbreviations
ATFL, anterior talofibular ligament; CFL, calcaneofibular ligament; PTFL, posterior talofibular ligament; PRISMA, Preferred Reporting Items for Systematic Review and Meta-analysis; RICE, rest, ice, compression, elevation; NSAIDs, non-steroidal anti-inflammatory drugs; RTS, return to sport; ROM, range of mobility.
References
1. Pellicciari L, Piscitelli D, De Vita M, D'Ingianna L, Bacciu S, Perno G, et al. Injuries among Italian dancesport athletes: a questionnaire survey. Med Probl Perform Art. (2016) 31:13–7. doi: 10.21091/mppa.2016.1003
2. Doherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med. (2014) 44:123–40. doi: 10.1007/s40279-013-0102-5
3. Smith RW, Reischl SF. Treatment of ankle sprains in young athletes. Am J Sports Med. (1986) 14:465–71. doi: 10.1177/036354658601400606
4. Holmer P, Sondergaard L, Konradsen L, Nielsen PT, Jorgensen LN. Epidemiology of sprains in the lateral ankle and foot. Foot Ankle Int. (1994) 15:72–4. doi: 10.1177/107110079401500204
5. Davids K, Glazier P. Deconstructing neurobiological coordination: the role of the biomechanics-motor control nexus. Exerc Sport Sci Rev. (2010) 38:86–90. doi: 10.1097/JES.0b013e3181d4968b
6. Turati M, Boerci L, Piatti M, Zanchi N, Zatti G, Accadbled F, et al. What's new about etiopathogenesis of musculoskeletal injuries in adolescent athletes? Minerva Pediatr. (2020). doi: 10.23736/S0026-4946.20.05944-7. [Epub ahead of print].
7. Bigoni M, Turati M, Gandolla M, Augusti CA, Pedrocchi A, La Torre A, et al. Balance in young male soccer players: dominant versus non-dominant leg. Sport Sci Health. (2017) 13:253–8. doi: 10.1007/s11332-016-0319-4
8. Piscitelli D, Falaki A, Solnik S, Latash ML. Anticipatory postural adjustments and anticipatory synergy adjustments: preparing to a postural perturbation with predictable and unpredictable direction. Exp Brain Res. (2017) 235:713–30. doi: 10.1007/s00221-016-4835-x
9. Romero-Morales C, Lopez-Lopez S, Bravo-Aguilar M, Cerezo-Tellez E, Benito-de Pedro M, Lopez Lopez D, et al. Ultrasonography comparison of the plantar fascia and tibialis anterior in people with and without lateral ankle sprain: a case-control study. J Manipulative Physiol Therap. (2020) 43:799–805. doi: 10.1016/j.jmpt.2019.11.004
10. Polzer H, Kanz KG, Prall WC, Haasters F, Ockert B, Mutschler W, et al. Diagnosis and treatment of acute ankle injuries: development of an evidence-based algorithm. Orthop Rev. (2012) 4:e5. doi: 10.4081/or.2012.e5
11. Turati M, Leone G, Zanchi N, Omeljaniuk RJ, Brahim L, Zatti G, et al. Clinical presentation and surgical treatment of distal fibular non-union with talus chondral lesions in a pediatric patient: a case report. BMC Surg. (2020) 20:125. doi: 10.1186/s12893-020-00782-z
12. Ferran NA, Maffulli N. Epidemiology of sprains of the lateral ankle ligament complex. Foot Ankle Clin. (2006) 11:659–62. doi: 10.1016/j.fcl.2006.07.002
13. Vuurberg G, Hoorntje A, Wink LM, van der Doelen BFW, van den Bekerom MP, Dekker R, et al. Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline. Br J Sports Med. (2018) 52:956. doi: 10.1136/bjsports-2017-098106
14. Green T, Willson G, Martin D, Fallon K. What is the quality of clinical practice guidelines for the treatment of acute lateral ankle ligament sprains in adults? A systematic review. BMC Musculoskelet Disord. (2019) 20:394. doi: 10.1186/s12891-019-2750-6
15. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the prisma statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
16. Shea BJ, Hamel C, Wells GA, Bouter LM, Kristjansson E, Grimshaw J, et al. Amstar is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. J Clin Epidemiol. (2009) 62:1013–20. doi: 10.1016/j.jclinepi.2008.10.009
17. Doherty C, Bleakley C, Delahunt E, Holden S. Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med. (2017) 51:113–25. doi: 10.1136/bjsports-2016-096178
18. Jones MH, Amendola AS. Acute treatment of inversion ankle sprains: immobilization versus functional treatment. Clin Orthop Relat Res. (2007) 455:169–72. doi: 10.1097/BLO.0b013e31802f5468
19. Kemler E, van de Port I, Backx F, van Dijk CN. A systematic review on the treatment of acute ankle sprain: brace versus other functional treatment types. Sports Med. (2011) 41:185–97. doi: 10.2165/11584370-000000000-00000
20. Kerkhoffs GM, Rowe BH, Assendelft WJ, Kelly KD, Struijs PA, van Dijk CN. Immobilisation for acute ankle sprain. A systematic review. Arch Orthop Trauma Surg. (2001) 121:462–71. doi: 10.1007/s004020100283
21. Ortega-Avila AB, Cervera-Garvi P, Marchena-Rodriguez A, Chicharro-Luna E, Nester CJ, Starbuck C, et al. Conservative treatment for acute ankle sprain: a systematic review. J Clin Med. (2020) 9:128. doi: 10.3390/jcm9103128
22. van den Bekerom MP, Struijs PA, Blankevoort L, Welling L, van Dijk CN, Kerkhoffs GM. What is the evidence for rest, ice, compression, and elevation therapy in the treatment of ankle sprains in adults? J Athl Train. (2012) 47:435–43. doi: 10.4085/1062-6050-47.4.14
23. Bleakley C, McDonough S, MacAuley D. The use of ice in the treatment of acute soft-tissue injury: a systematic review of randomized controlled trials. Am J Sports Med. (2004) 32:251–61. doi: 10.1177/0363546503260757
24. Jones P, Lamdin R, Dalziel SR. Oral non-steroidal anti-inflammatory drugs versus other oral analgesic agents for acute soft tissue injury. Cochrane Datab Syst Rev. (2020) 8:CD007789. doi: 10.1002/14651858.CD007789.pub3
25. van den Bekerom MPJ, Sjer A, Somford MP, Bulstra GH, Struijs PAA, Kerkhoffs G. Non-steroidal anti-inflammatory drugs (Nsaids) for treating acute ankle sprains in adults: benefits outweigh adverse events. Knee Surg Sports Traumatol Arthrosc. (2015) 23:2390–9. doi: 10.1007/s00167-014-2851-6
26. Bleakley CM, McDonough SM, MacAuley DC. Some conservative strategies are effective when added to controlled mobilisation with external support after acute ankle sprain: a systematic review. Aust J Physiother. (2008) 54:7–20. doi: 10.1016/S0004-9514(08)70061-8
27. Brantingham JW, Bonnefin D, Perle SM, Cassa TK, Globe G, Pribicevic M, et al. Manipulative therapy for lower extremity conditions: update of a literature review. J Manipulative Physiol Ther. (2012) 35:127–66. doi: 10.1016/j.jmpt.2012.01.001
28. Loudon JK, Reiman MP, Sylvain J. The efficacy of manual joint mobilisation/manipulation in treatment of lateral ankle sprains: a systematic review. Br J Sports Med. (2014) 48:365–70. doi: 10.1136/bjsports-2013-092763
29. Terada M, Pietrosimone BG, Gribble PA. Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: a systematic review. J Athl Train. (2013) 48:696–709. doi: 10.4085/1062-6050-48.4.11
30. van der Wees PJ, Lenssen AF, Hendriks EJ, Stomp DJ, Dekker J, de Bie RA. Effectiveness of exercise therapy and manual mobilisation in ankle sprain and functional instability: a systematic review. Aust J Physiother. (2006) 52:27–37. doi: 10.1016/S0004-9514(06)70059-9
31. van Os AG, Bierma-Zeinstra SM, Verhagen AP, de Bie RA, Luijsterburg PA, Koes BW. Comparison of conventional treatment and supervised rehabilitation for treatment of acute lateral ankle sprains: a systematic review of the literature. J Orthop Sports Phys Ther. (2005) 35:95–105. doi: 10.2519/jospt.2005.35.2.95
32. van Rijn RM, van Ochten J, Luijsterburg PA, van Middelkoop M, Koes BW, Bierma-Zeinstra SM. Effectiveness of additional supervised exercises compared with conventional treatment alone in patients with acute lateral ankle sprains: systematic review. BMJ. (2010) 341:c5688. doi: 10.1136/bmj.c5688
33. Kerkhoffs GM, Handoll HH, de Bie R, Rowe BH, Struijs PA. Surgical versus conservative treatment for acute injuries of the lateral ligament complex of the ankle in adults. Cochrane Datab Syst Rev. (2007) 2:CD000380. doi: 10.1002/14651858.CD000380.pub2
35. Feger MA, Goetschius J, Love H, Saliba SA, Hertel J. Electrical stimulation as a treatment intervention to improve function, edema or pain following acute lateral ankle sprains: a systematic review. Phys Ther Sport. (2015) 16:361–9. doi: 10.1016/j.ptsp.2015.01.001
36. Kim TH, Lee MS, Kim KH, Kang JW, Choi TY, Ernst E. Acupuncture for treating acute ankle sprains in adults. Cochrane Datab Syst Rev. (2014) 6:CD009065. doi: 10.1002/14651858.CD009065.pub2
37. Park J, Hahn S, Park JY, Park HJ, Lee H. Acupuncture for ankle sprain: systematic review and meta-analysis. BMC Complement Altern Med. (2013) 13:55. doi: 10.1186/1472-6882-13-55
38. Al Bimani SA, Gates LS, Warner M, Bowen C. Factors influencing return to play following conservatively treated ankle sprain: a systematic review. Phys Sportsmed. (2019) 47:31–46. doi: 10.1080/00913847.2018.1533392
39. Tassignon B, Verschueren J, Delahunt E, Smith M, Vicenzino B, Verhagen E, et al. Criteria-based return to sport decision-making following lateral ankle sprain injury: a systematic review and narrative synthesis. Sports Med. (2019) 49:601–19. doi: 10.1007/s40279-019-01071-3
40. Vancolen SY, Nadeem I, Horner NS, Johal H, Alolabi B, Khan M. Return to sport after ankle syndesmotic injury: a systematic review. Sports Health. (2019) 11:116–22. doi: 10.1177/1941738118816282
41. Wikstrom EA, Mueller C, Cain MS. Lack of consensus on return-to-sport criteria following lateral ankle sprain: a systematic review of expert opinions. J Sport Rehabil. (2020) 29:231–7. doi: 10.1123/jsr.2019-0038
42. Feldman AG, Levin MF, Garofolini A, Piscitelli D, Zhang L. Central pattern generator and human locomotion in the context of referent control of motor actions. Clin Neurophysiol. (2021) 132:2870–89. doi: 10.1016/j.clinph.2021.08.016
43. Furmanek MP, Solnik S, Piscitelli D, Rasouli O, Falaki A, Latash ML. Synergies and motor equivalence in voluntary sway tasks: the effects of visual and mechanical constraints. J Mot Behav. (2018) 50:492–509. doi: 10.1080/00222895.2017.1367642
44. Kazemi K, Arab AM, Abdollahi I, Lopez-Lopez D, Calvo-Lobo C. Electromiography comparison of distal and proximal lower limb muscle activity patterns during external perturbation in subjects with and without functional ankle instability. Hum Mov Sci. (2017) 55:211–20. doi: 10.1016/j.humov.2017.08.013
45. D'Ambrosi R, Villafane JH, Indino C, Liuni FM, Berjano P, Usuelli FG. Return to sport after arthroscopic autologous matrix-induced chondrogenesis for patients with osteochondral lesion of the talus. Clin J Sport Med. (2019) 29:470–5. doi: 10.1097/JSM.0000000000000560
46. Ieropoli G, Villafane JH, Zompi SC, Morozzo U, D'Ambrosi R, Usuelli FG, et al. Successful treatment of infected wound dehiscence after minimally invasive locking-plate osteosynthesis of tibial pilon and calcaneal fractures by plate preservation, surgical debridement and antibiotics. Foot. (2017) 33:44–7. doi: 10.1016/j.foot.2017.10.001
47. Delahunt E, Coughlan GF, Caulfield B, Nightingale EJ, Lin CW, Hiller CE. Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med Sci Sports Exerc. (2010) 42:2106–21. doi: 10.1249/MSS.0b013e3181de7a8a
48. Hiller CE, Kilbreath SL, Refshauge KM. Chronic ankle instability: evolution of the model. J Athl Train. (2011) 46:133–41. doi: 10.4085/1062-6050-46.2.133
49. Ardern CL, Glasgow P, Schneiders A, Witvrouw E, Clarsen B, Cools A, et al. 2016 Consensus statement on return to sport from the first world congress in sports physical therapy, Bern. Br J Sports Med. (2016) 50:853–64. doi: 10.1136/bjsports-2016-096278
50. Villafane JH, Valdes K, Pedersini P, Berjano P. Osteoarthritis: a call for research on central pain mechanism and personalized prevention strategies. Clin Rheumatol. (2019) 38:583–4. doi: 10.1007/s10067-018-4270-4
51. Meroni R, Piscitelli D, Bonetti F, Zambaldi M, Guccione AA, Pillastrini P. Rasch analysis of the Italian version of fear avoidance beliefs questionnaire (Fabq-I). Disabil Rehabil. (2015) 37:151–7. doi: 10.3109/09638288.2014.909890
52. Meroni R, Piscitelli D, Bonetti F, Zambaldi M, Cerri CG, Guccione AA, et al. Rasch analysis of the Italian version of pain catastrophizing scale (Pcs-I). J Back Musculoskelet Rehabil. (2015) 28:661–73. doi: 10.3233/BMR-140564
Keywords: rehabilitation, treatment, management, acute, ankle, sprain, injury
Citation: Gaddi D, Mosca A, Piatti M, Munegato D, Catalano M, Di Lorenzo G, Turati M, Zanchi N, Piscitelli D, Chui K, Zatti G and Bigoni M (2022) Acute Ankle Sprain Management: An Umbrella Review of Systematic Reviews. Front. Med. 9:868474. doi: 10.3389/fmed.2022.868474
Received: 02 February 2022; Accepted: 27 May 2022;
Published: 07 July 2022.
Edited by:
Daniel López-López, Universidade da Coruña, SpainReviewed by:
Santiago Navarro-Ledesma, Universidad de Granada, SpainJorge Hugo Villafañe, Fondazione Don Carlo Gnocchi Onlus (IRCCS), Italy
Yinghui Hua, Huashan Hospital Affiliated to Fudan University, China
Copyright © 2022 Gaddi, Mosca, Piatti, Munegato, Catalano, Di Lorenzo, Turati, Zanchi, Piscitelli, Chui, Zatti and Bigoni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marco Turati, bWFyY28udHVyYXRpQHVuaW1pYi5pdA==