 Cristina Ruiz-Rull1,2†
Cristina Ruiz-Rull1,2† María José Jaén-Moreno1,3*†Gloria Isabel del Pozo1,4Cristina Gómez1,5Francisco Javier Montiel1,5Montserrat Alcántara1,4Laura Carrión1,6Geli Marie Chauca1,6Nuria Feu7Ipek Guler8Fernando Rico-Villademoros9
María José Jaén-Moreno1,3*†Gloria Isabel del Pozo1,4Cristina Gómez1,5Francisco Javier Montiel1,5Montserrat Alcántara1,4Laura Carrión1,6Geli Marie Chauca1,6Nuria Feu7Ipek Guler8Fernando Rico-Villademoros9 Cristina Camacho-Rodríguez1
Cristina Camacho-Rodríguez1 Luis Gutierrez-Rojas9,10David Mannino11Fernando Sarramea1,3,4,12
Luis Gutierrez-Rojas9,10David Mannino11Fernando Sarramea1,3,4,12- 1Instituto Maimónides de Investigación Biomédica de Córdoba (IMIBIC), Córdoba, Spain
- 2Centro de Salud Cruz de Caravaca, Almería, Spain
- 3Departamento de Ciencias Morfológicas y Sociosanitarias, Universidad de Córdoba, Córdoba, Spain
- 4Unidad de Gestión Clínica de Salud Mental, Hospital Universitario Reina Sofía, Córdoba, Spain
- 5Unidad de Gestión Clínica de Salud Mental, Complejo Hospitalario de Jaén, Jaen, Spain
- 6Unidad de Gestión Clínica de Salud Mental, Hospital Infanta Margarita, Cabra, Spain
- 7Unidad de Gestión Clínica de Neumología, Hospital Universitario Reina Sofía, Córdoba, Spain
- 8Instituto Maimónides de Investigación Biomédica de Córdoba (IMIBIC), Área de Gestión de la Investigación, Córdoba, Spain
- 9Instituto de Neurociencias, Universidad de Granada, Granada, Spain
- 10Departamento de Psiquiatria, Universidad de Granada, Granada, Spain
- 11University of Kentucky, Chief Medical Officer, COPD Foundation, Lexington, KY, United States
- 12Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Oviedo, Spain
Introduction: People with serious mental illness (SMI), such as schizophrenia and bipolar disorder, have a higher risk of premature morbidity and mortality. In the general population, impaired lung function is associated with increased morbidity and mortality. We compared lung function between people with and without serious mental illnesses using a cross-sectional study in 9 community mental health units.
Methods: Subjects aged 40–70 years with a diagnosis of schizophrenia or bipolar disorder were recruited consecutively. The controls had no psychiatric diagnosis and were not receiving any psychotropics. Spirometry was performed by a trained nurse. We used the 2021 American Thoracic Society/European Respiratory Society standards for the interpretation of the spirometry results.
Results: We studied 287 subjects. People with SMI (n = 169) had lower spirometry values than those without a psychiatric diagnosis (n = 118). An abnormal spirometry pattern (36.1% vs 16.9%, p < 0.001), possible restriction or non-specific (Preserved Ratio Impaired Spirometry [PRISm]) pattern (17.8% vs 7.6%, p = 0.014), and pattern of airflow obstruction or possible mixed disorder (18.3% vs 9.3%, p = 0.033) were more frequent in people with SMI. Multivariate analyses showed that the PRISm pattern was associated with abdominal circumference (odds ratio [OR] 1.05, 95%CI 1.03–1.08) and that the pattern of airflow obstruction or possible mixed disorder was associated with smoking behavior (OR 5.15, 95%CI 2.06–15.7).
Conclusion: People with SMI have impaired lung function, with up to one-third of them showing an abnormal spirometry pattern. This suggests that regular monitoring of lung function and addressing modifiable risk factors, such as tobacco use and obesity, in this population is of paramount importance.
1 Introduction
People with serious mental illness (SMI), such as schizophrenia and bipolar disorder, have a higher risk of premature morbidity and mortality compared to the general population. It has been observed that their life expectancy may be reduced by 12–15 years in people with schizophrenia (Crump et al., 2013a) and approximately 9 years in people with bipolar disorder (Crump et al., 2013b). This is a major public health issue that requires intervention (Liu et al., 2017; Fiorillo and Sartorius, 2021) and improved knowledge of the risk factors. In relative terms, unnatural causes of death, such as suicide, are associated with the highest excess mortality in people with SMI (Saha et al., 2007; Hayes et al., 2015). Among natural causes, chronic obstructive pulmonary disease (COPD) is one of the highest causes of excess mortality in people with schizophrenia or bipolar disorder, even higher than that of cardiovascular diseases (Saha et al., 2007; Hayes et al., 2015; Olfson et al., 2015; Correll et al., 2022). In the general population, both COPD and spirometrically determined impaired lung function are associated with increased morbidity and mortality (Sin et al., 2005; Guerra et al., 2010; Agusti et al., 2017; Honda et al., 2017; Cuttica et al., 2018; Collaro et al., 2021; Guo et al., 2021; Shah et al., 2021; Kaaks et al., 2022; Ramalho et al., 2022; Sarycheva et al., 2022; Dharmage et al., 2023).
Spirometry is a noninvasive, reproducible and readily available test for evaluating lung function (Global Initiative for Chronic Obstructive Lung Disease, 2022) and has been shown to be a key tool in diagnosing lung disease and monitoring patients (Lamb et al., 2022). To date, four studies have evaluated lung function using spirometry in patients with SMI (Filik et al., 2006; Vancampfort et al., 2014a; Vancampfort et al., 2014b; Partti et al., 2015; Jaen-Moreno et al., 2021). Filik et al. (2006) and Vancampfort et al. (2014a); Vancampfort et al. (2014b) reported that people with schizophrenia had lower lung function as evaluated by spirometry, reporting a lower forced expiratory volume in 1 s (FEV1) and lower forced vital capacity (FVC); however, these studies did not report the frequency of obstructive and restrictive patterns. Using baseline data from a randomized controlled trial in active smokers, Jaen-Moreno et al. (2021) secondarily reported that 27 (23.9%) of 113 patients with SMI met the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria for COPD, and among 86 patients who did not meet COPD criteria, 23 (26.7%) showed an FEV1 less than 80% of the predicted value, which is consistent with a restrictive pattern. Finally, Partti et al. (2015), in a population-based study, showed that people with schizophrenia and other nonaffective psychiatric disorders (e.g., schizophreniform disorder) had impaired lung function and a higher likelihood of a restrictive pattern than people with no psychiatric disorder, and people with schizophrenia also had a higher likelihood of an obstructive pattern. Data on lung function in people with bipolar disorder are lacking.
Our study aimed to evaluate lung function and the prevalence of abnormal spirometry patterns, and explore the factors associated with them in people with SMI (schizophrenia or bipolar disorder) in a community-based mental healthcare sample and compare it to that of people without a psychiatric diagnosis.
2 Materials and methods
This was an observational cross-sectional study conducted in 9 community mental health units in Andalucía (southern Spain). A control group was used to increase the internal validity of the study and support the causal inference. The study was approved by the Ethics Committee of Reina Sofía Hospital (Córdoba, Spain), and written informed consent was obtained from all subjects.
2.1 Selection criteria
We recruited consecutive subjects attending scheduled follow-up visits at their mental health outpatient service. The subjects had to be 40–70 years of age. We included subjects aged 40 years or older because the harmful effects of tobacco occur from that age (Górecka et al., 2003) and excluded subjects over 70 years old because, due to shortened life expectancy, it is difficult to find people with SMI who are attending a psychiatric outpatient clinic. In the clinical sample (i.e., patients with a psychiatric diagnosis), additional inclusion criteria were a DSM-IV diagnosis of schizophrenia or bipolar disorder and clinical stability, which was defined as a score lower than 14 points on the Hamilton Depression Rating Scale (HDRS) and a score lower than six points on the Young Mania Rating Scale (YMRS) in people with bipolar disorder or a score lower than 40 points on the Positive and Negative Syndrome Scale (PANSS) in people with schizophrenia. Subjects without a psychiatric diagnosis (controls) were recruited from those accompanying the person with a psychiatric diagnosis and from those visiting the primary care center for administrative purposes; they were excluded if they had any current or past diagnosis of a psychiatric disorder or were receiving any psychotropic.
In both samples, with or without psychiatric diagnosis, subjects were excluded if they exhibited a clinical condition that made it advisable not to perform spirometry (recent pneumothorax, recent thoracic or abdominal surgery, aortic aneurysm, unstable angulation, retinal detachment, facial hemiparesis or oral/dental problems), had an intellectual disability or a clinical status that, in the investigator’s judgment, made the subject unable to properly understand the instructions for forced spirometry or if they had history of respiratory diseases.
2.2 Assessments
We recorded sociodemographic data, anthropometric data including abdominal circumference, and vital signs (i.e., heart rate and blood pressure). We included abdominal circumference because it is considered that body mass index alone is not sufficient to properly assess the cardiometabolic risk associated with increased adiposity and, therefore, it is recommended as a routine vital sign measurement (Ross et al., 2020). In addition, some studies suggest that abdominal circumference is inversely associated with FEV1 (Wehrmeister et al., 2012). In people with a psychiatric diagnosis, we administered the HDRS, YMRS and PANSS, whereas in controls, the lack of psychiatric diagnosis and lack of history of psychiatric treatment/follow-up were confirmed. The following medical comorbidities were searched from the medical charts and recorded: hypertension, diabetes, dyslipidemia, peripheral vascular disease, heart disease and oncological disease. The evaluation of smoking habit included the history of consumption, current consumption confirmed by CO-oximetry, and dependence on nicotine as evaluated with the Fagerström Test for Nicotine Dependence (Becoña and Vázquez, 1998) (FTND), a standard instrument for assessing the intensity of physical addiction to nicotine which categorizes dependence as mild (0–3), moderate (Saha et al., 2007; Hayes et al., 2015; Liu et al., 2017; Correll et al., 2022) and severe (Olfson et al., 2015; Agusti et al., 2017; Collaro et al., 2021). Physical activity was estimated using the Spanish validated version of the International Physical Activity Questionnaire (IPAQ) (Roman et al., 2006), which allows the calculation of energy expenditure as metabolic equivalents of task (METs) and the total expenditure as METs-minute/week as well as a sedentary index as the total time in minutes seated in a week.
Spirometry was performed at each participant site using a DATOSPIR Touch Easy D+ spirometer (Sibelmed®, Barcelona, Spain). To validate the equipment used and check its characteristics, the test and criteria for quality control was used for acceptability and repeatability of the results; the standardization criteria set down by the American Thoracic Society and the European Respiratory Society (ATS/ERS) (Miller et al., 2005). They were performed by a nurse trained by the pulmonology service of the Reina Sofía Hospital (Córdoba, Spain) on calibration, preparing patients, performing maneuvers, bronchodilatation and repetition of spirometry. A maximum of eight efforts could be made to achieve a minimum of three acceptable blows. The system automatically selected the two best curves with repeatability criteria, that is, the two highest FVC values and the two highest FEV1 values, with a difference of less than 0.15 L. The reversibility test required the repetition of three acceptable efforts 15 min after the inhalation of a bronchodilator (salbutamol 400 µg). Curves and volumes were centrally assessed by a single blinded researcher, the head of the functional test unit of the pulmonology service of the Reina Sofía Hospital (Córdoba, Spain), and the highest readings of FVC and FEV1 were recorded and used in the analysis. Following the 2021 American Thoracic Society (ATS) and European Respiratory Society (ERS) standards (Stanojevic et al., 2022), z-scores were calculated using GLI reference equations, and FEV1/FVC ratio <fifth percentile (z-score < -1.645) and FVC >fifth percentile (z-score > -1.645) were considered indicative of airflow obstruction; FEV1/FVC ratio <fifth percentile (z-score < -1.645) and FVC <fifth percentile (z-score < -1.645) were considered indicative of a possible mixed disorder; and a FEV1/FVC ratio >fifth percentile (z-score > -1.645) and a FVC <fifth percentile (z-score < -1.645) were indicative of a possible restriction or non-specific pattern (Preserved Ratio Impaired Spirometry [PRISm]). The severity of lung function (for all measures using the z-score) was considered mild (−1.65 to −2.5), moderate (−2.51 to −4.0) or severe (<-4.1). According to the 2021 ERS/ATS standards, the response to bronchodilation was considered positive when the difference between pre-bronchodilation and post-bronchodilation was greater than 10% of predicted value in FEV1 or FVC. In addition, predicted values were calculated as a percentage of the reference values from the Spanish Society of Pneumology and Thoracic Surgery (Sociedad Española de Neumología y Cirugía Torácica [SEPAR]), enabling comparison with the existing literature for this particular population group.
2.3 Statistical analysis
Continuous variables were expressed as the mean and standard deviation or the median and range and compared using the Wilcoxon test. Cohen’s d effect size was calculated as the quotient between the difference in means and pooled standard deviation of the two groups. To interpret the relative magnitude of the difference, we considered effect sizes of 0.20 as small, 0.50 as moderate and 0.80 or greater as large. Categorical variables were expressed as absolute and relative frequencies and compared using the chi-squared test. Due to the sample size of the subgroups and consistent with the protocol, all comparisons were limited to those between the overall group of people with SMI vs the control group; however, descriptive data are also presented for the subgroups of people with schizophrenia and people with bipolar disorder.
To evaluate the potential factors associated with spirometry patterns, multivariate logistic regression models were independently fitted for each ATS/ERS spirometry pattern categorized as airflow obstruction or possible mixed disorder (hereafter referred to obstructive component pattern) and possible restriction or non-specific pattern (PRISm). Additionally, we considered an abnormal pattern that combined the two previous patterns. Variable selection was performed using the Akaike Information Criterion (AIC) with backward stepwise elimination in a multivariate model setting using the variables suggested in the literature as risk factors.
The results are expressed as odds ratios (ORs), 95% confidence intervals (CIs) and p values.
All statistical analyses were performed using R software, version 4.0.3.
3 Results
3.1 Patient disposition and characteristics
From July 2018 to February 2020, we recruited 287 participants: 169 with SMI (111 with schizophrenia and 58 with bipolar disorder) and 118 controls. Compared to controls, those with SMI were younger, had a greater waist circumference, body mass index, and sedentary index, had a higher proportion of smokers, were heavier smokers and showed greater nicotine dependence, as shown by the FTND score (Table 1). People with SMI also had a higher frequency of diabetes (14.4% vs 6.1%, p = 0.049) and a lower frequency of hypertension (10.7% vs 25.4%, p = 0.002) (Table 1).
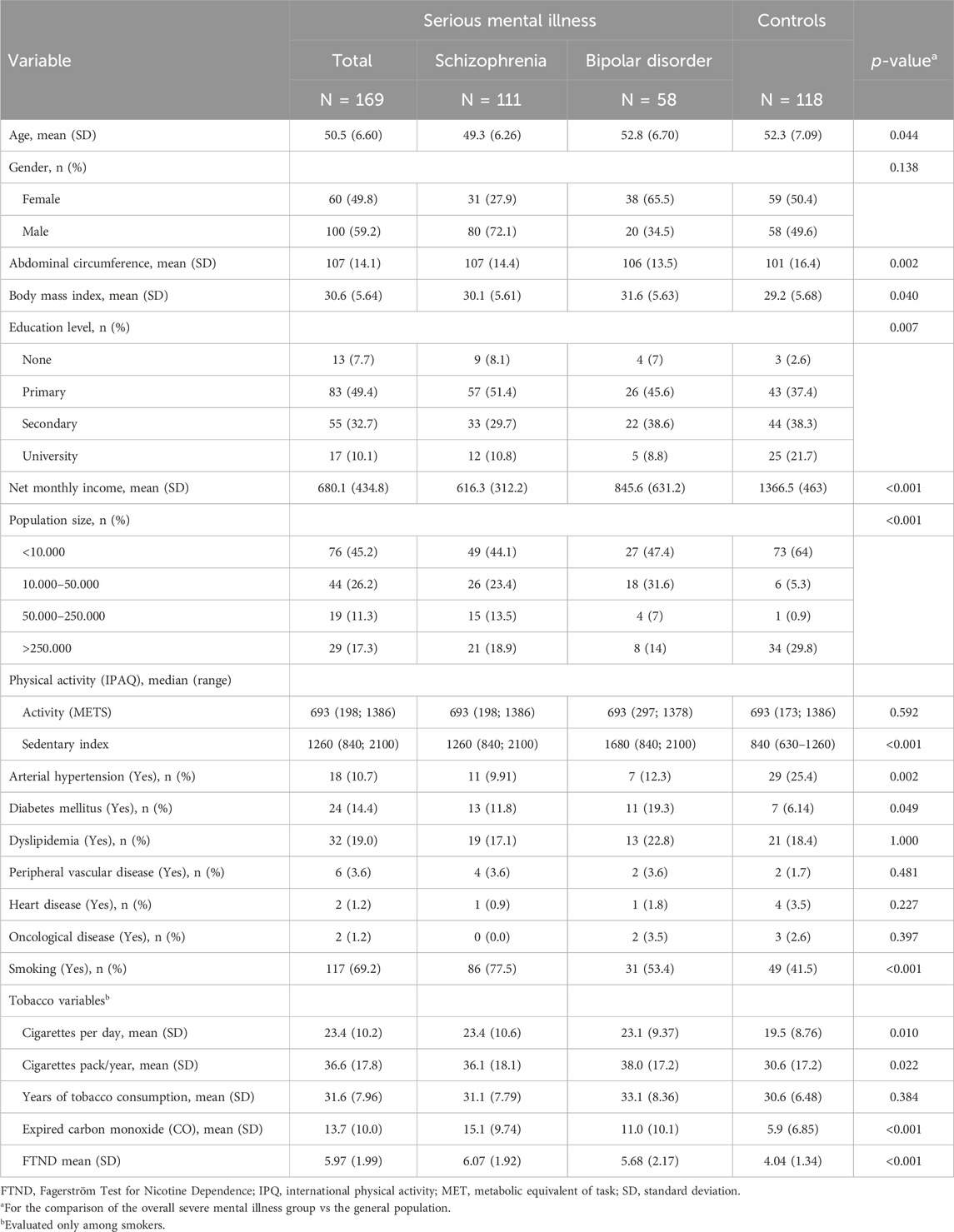
Table 1. Demographic and clinical characteristics.
3.2 Spirometry results
People with SMI had significantly lower FEV1 z-score, FVC z-score, and FEV1/FVC ratio z-score than controls; effect sizes as evaluated with Cohen’s d were moderate for the differences in the FEV1 and FVC z-scores, and small for the difference in FEV1/FVC z-score (Table 2). When evaluated with FEV1 z-score, 24 (14.2%) subjects with SMI showed a moderate lung function impairment and 1 (0.6%) had a severe impairment, while there were no cases of severe impairment and there was one case of moderate lung function impairment among controls (Table 2). Except for the effect sizes, % predicted values showed similar results (Table 2; Supplementary Table S1).
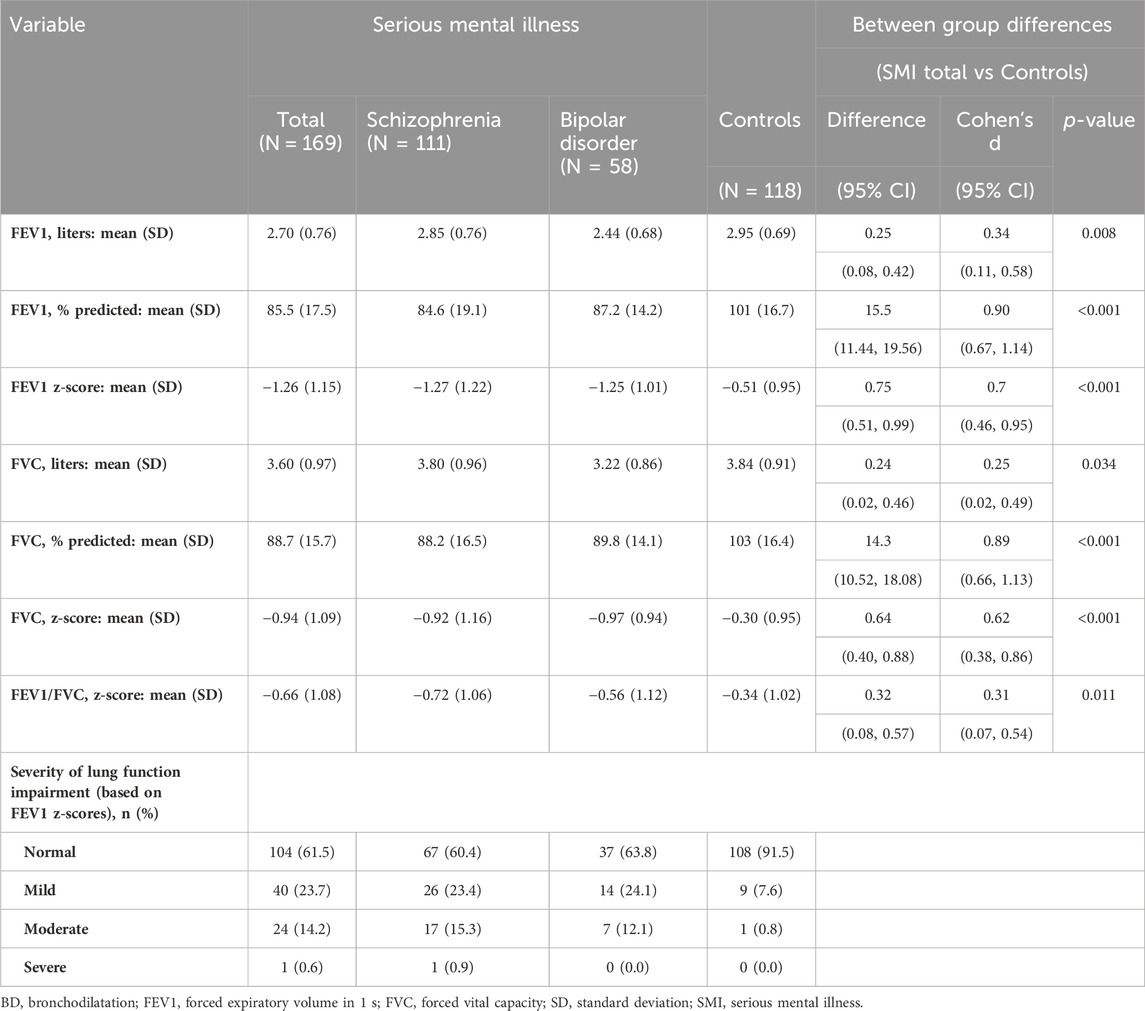
Table 2. Spirometry results.
Overall, 61 (36.1%) of the people with SMI had an abnormal spirometry pattern compared to 20 (16.9%) of controls (p < 0.001). The PRISm pattern was significantly more frequent in people with SMI than controls (17.8% vs 7.6%, p = 0.014), and the proportion of subjects showing an obstructive component pattern was also significantly higher among people with SMI (18.3% vs 9.3%, p = 0.033) (Figure 1). Of the 31 subjects with SMI and obstructive component pattern, 1 (3.2%) responded to bronchodilators; 4 (36.4%) of 11 controls with an obstructive component pattern responded to bronchodilators Spirometry patterns according to the GOLD criteria are shown in Supplementary Figure S1.

Figure 1. Spirometric patterns. p-values refer to the comparison between serious mental illness and the general population.
3.3 Multivariate analyses
The factors associated with a greater likelihood of presenting an abnormal spirometry pattern were having a SMI (odds ratio [OR] 2.29, 95% CI 1.26 to 4.28; p = 0.008) and smoking (OR 2.19, 95% CI 1.20–4.07) (Table 3). Smoking was significantly associated with an obstructive component pattern (OR 5.15, 95% CI 2.06–15.7) and the abdominal perimeter was significantly associated with a PRISm pattern (OR 1.05, 95% CI 1.03–1.08) (Table 3).
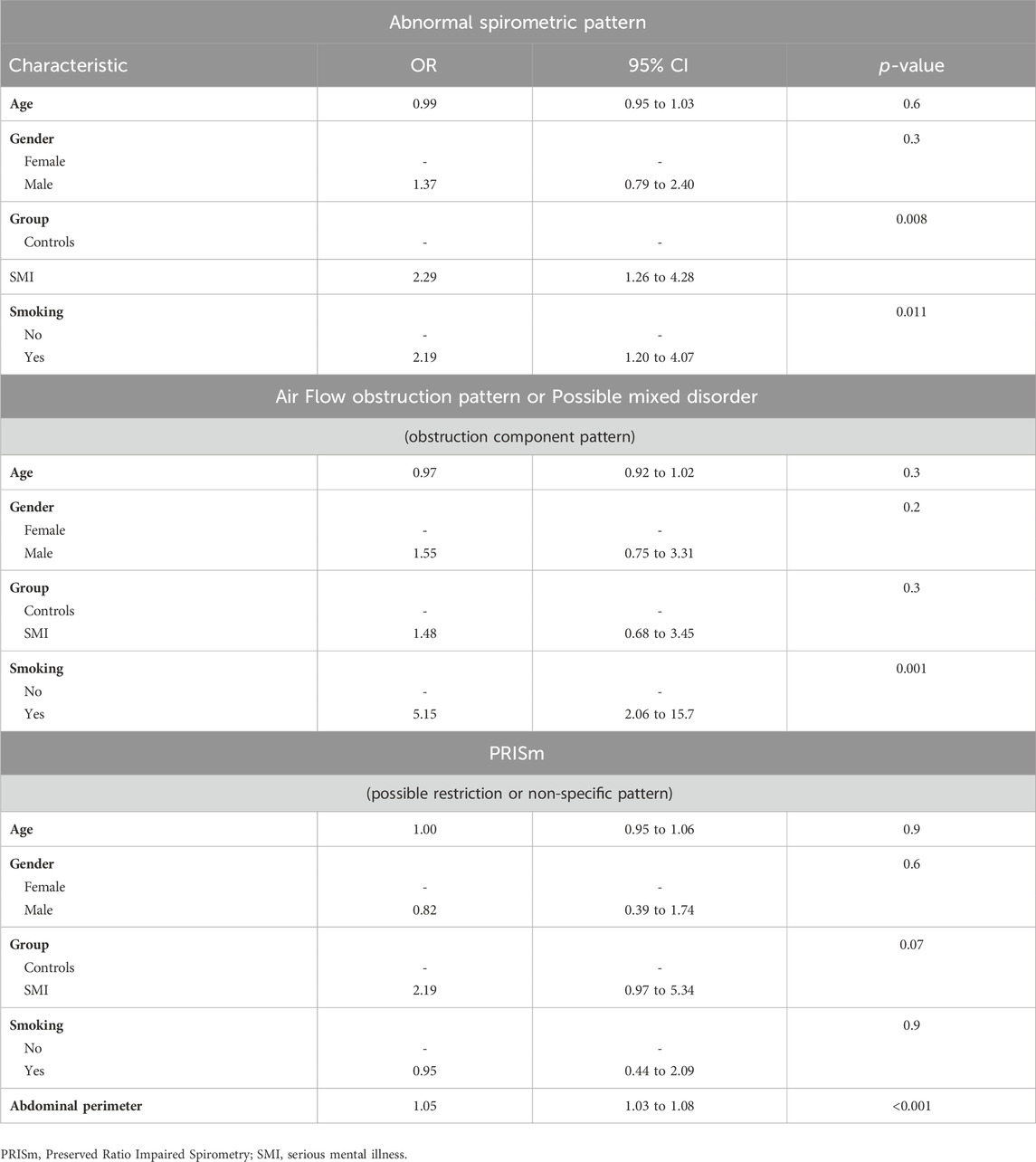
Table 3. Multivariate analyses.
4 Discussion
We found that people with SMI showed a significant reduction in all spirometric values and had an increased frequency of an abnormal spirometry pattern, with significantly higher frequency of obstructive component and PRISm patterns than those without a psychiatric diagnosis. Among modifiable risk factors, while smoking was the main risk factor for an obstructive component pattern, abdominal obesity was the main factor associated with the presence of the PRISm pattern.
People with SMI showed a significant impairment of lung function as evaluated by FEV1 and FVC z-scores, and substantial proportion of subjects (15%) showed at least moderate impairment compared to almost no cases (1%) among controls. None of the previously published studies on lung function in people with SMI used the new ATS/ERS standards for the analyses of spirometry; therefore, in some instances to put our results into perspective we will use % predicted values and the GOLD criteria for obstructive and restrictive patterns. When using classical spirometry parameters, our results are consistent with those reported by Partti et al. and Vancampfort et al. (2014a) in patients with schizophrenia. To the best of our knowledge, there are no previous reports on lung function in people with bipolar disorders.
We found that an obstructive component pattern was more frequent among subjects with SMI than among those without a psychiatric disorder. Our results are consistent with those reported by Partti et al. (2015) for the subgroup of patients with schizophrenia using the GOLD criteria. Furthermore, they are also consistent with the high rates of tobacco consumption in this population who show earlier age of smoking, and greater intensity and frequency of smoking (Dickerson et al., 2018).
The prevalence of the PRISm pattern in subjects with SMI was higher than that in controls. These results were consistent with those reported in a recent cross-sectional study conducted in people who were diagnosed with first-episode psychosis 10-year earlier, which found that the prevalence of PRISm was higher among people with psychosis compared to healthy controls (10.4% vs 1.4%) (Viejo Casas et al., 2024). The absolute difference between people with SMI and controls in our study for a PRISm pattern (17.8% vs 7.6%) was similar to that reported in this latter study; the higher frequency of PRISm in our study could be partially explained by the fact that the subjects included in our study were older (mean age 50.5 vs 41.7 years) and our definition of PRISm was based on z-scores. In our multivariate analysis, abdominal circumference was significantly associated with a higher likelihood of presenting a PRISm pattern. Our results are supported by the strong association found between obesity with the presence of PRISm in the general population (Wan et al., 2021; Higbee et al., 2022). It is also possible that antipsychotic treatment plays a role on the impairment of lung function. Although evidence is weak, some studies suggest that antipsychotics may be associated with an increased risk of acute respiratory failure (Wilson and Ridley, 2007; Wang et al., 2017). More importantly, several antipsychotics are associated with an increased risk of weight gain and other metabolic disorders (Pillinger et al., 2020; Bernardo et al., 2021); thus, they may contribute to the increased risk of PRISm in this population.
Several longitudinal studies have shown an association between reduced lung volume or abnormal spirometry patterns and increased morbidity and mortality. Reduced FEV1 has been associated with an increased risk of occurrence of respiratory disease (Agusti et al., 2017; Shah et al., 2021) and metabolic abnormalities, including diabetes (Agusti et al., 2017; Shah et al., 2021), heart failure (Ramalho et al., 2022) and cardiovascular events (Agusti et al., 2017; Cuttica et al., 2018), and an increased risk of cardiovascular (Sin et al., 2005) and all-cause mortality (Agusti et al., 2017; Sarycheva et al., 2022). COPD or a reduced FEV1/FVC ratio has been associated with an increased risk of lung cancer (Kaaks et al., 2022) and all-cause mortality (Collaro et al., 2021; Guo et al., 2021; Kaaks et al., 2022). Importantly, some of these studies have also shown the presence of a gradient in the relationship between reduced FEV1 (Sarycheva et al., 2022) or COPD (Guo et al., 2021; Kaaks et al., 2022) and all-cause mortality. A restrictive pattern has been associated with an increased risk of cardiovascular events (Guerra et al., 2010; Dharmage et al., 2023), hypertension (Dharmage et al., 2023), diabetes (Guerra et al., 2010; Dharmage et al., 2023) and cardiovascular and all-cause mortality (Guerra et al., 2010; Honda et al., 2017; Guo et al., 2021). PRISm has been also associated with an increased risk of all-cause mortality (Yang et al., 2023).
Our study has several limitations that should be considered. First, we performed a cross-sectional analysis, and thus, we cannot infer causality. Using data from a national health survey in the United States, Goodwin et al. (Goodwin et al., 2007) found an association between the presence of an obstructive and restrictive spirometry pattern and an impairment of mental health as evaluated by the General Wellbeing scale; after controlling for differences in demographic factors, there was an association between a spirometry restrictive pattern and lower scores in general health, vitality and self-control and higher scores for depression. Although we cannot rule out a bidirectional relationship between SMI and lung function impairment, there is evidence from longitudinal studies supporting the association of SMI with the occurrence of COPD and other respiratory diseases (Jaén-Moreno et al., 2023). Second, we used convenience sampling for the selection of the control group, based on the people accompanying the person with a psychiatric diagnosis or those visiting the primary care center for administrative purposes. Having a family member or a friend who is a smoker is a risk factor for being a smoker (Karadogan et al., 2018), which could explain why the prevalence of smokers in our control group was higher than in the general population (19.7% in 2019) (Eurostat, 2023). This could have biased the results against a potential association between SMI and lung function impairment. Third, in addition to a sedentary lifestyle, several medical comorbidities, such as hypertension, dyslipidemia and diabetes, have been associated with a spirometric restrictive pattern both in the general population (Backman et al., 2016; Sperandio et al., 2016) and in subjects with SMI (Partti et al., 2015). These medical comorbidities in our study were elicited through clinical charts and may be underdiagnosed in patients with SMI (Teixeira et al., 2022), thus limiting our multivariate analyses. Importantly, all these studies showing the association between medical comorbidities and impaired lung function were cross-sectional; therefore, we cannot be sure of the direction of the relationship. In a recent longitudinal study, the Tasmanian Longitudinal Health Study (Australia), subjects with a lifetime spirometry restrictive pattern were at increased risk of medical multimorbidity by middle age, including angina/myocardial infarction, hypertension, diabetes and sleep apnea (Dharmage et al., 2023). It is possible that lung function impairment and all medical comorbidities in patients with SMI share a common pathophysiological pathway (Teixeira et al., 2022). In the Tasmanian Longitudinal Health Study, subjects with a spirometry restrictive pattern showed the highest levels of C-reactive protein in middle age (Dharmage et al., 2023). Therefore, it is possible SMI will be associated with lung function impairment through intermediate variables such a smoking and abdominal obesity, direct mechanism such as a hyperinflammatory state, or a complex interplay of several factors. Fourth, information on exposure to inhaled toxicants in the workplace or related to traffic is unavailable. Finally, the age selection criterion could impact the generalizability of the results.
In our view, our study has some strengths. In contrast to Partti et al. (2015) and similar to Vancampfort et al. (2014a) we used a clinical sample and therefore were more representative of clinical practice. In addition, we used the new ATS/ERS standards for the analysis, and, although it was not the primary objective of our study, to our knowledge, we provide for the first time data on lung function in people with bipolar disorder.
Overall, consistent with what has been reported previously in a population-based study (Partti et al., 2015), our results show that people with SMI seen in mental health outpatient services have a significant and clinically relevant reduction in FEV1 and FVC, and suggest that up to one-third of people with SMI have an abnormal spirometry pattern, which in the case of the obstructive component pattern is associated with smoking and in the PRISm pattern with abdominal obesity. Although it has been infrequently studied in patients with SMI, the potentially severe consequences of an abnormal spirometry pattern suggest that patients with SMI should undergo regular monitoring of lung function to detect these alterations. This policy would be consistent with GOLD’s proposal for active COPD case finding (Global Initiative for Chronic Obstructive Lung Disease, 2022), bearing in mind that having an SMI—in addition to being a smoker—is a risk factor for lung function impairment. In a recent review of physical health guidelines for people with SMI, none of the 15 guidelines reviewed included recommendations for evaluating lung function (Friend et al., 2020). In addition to monitoring lung function, addressing modifiable risk factors for lung function impairment, such as tobacco use and obesity, which are also risk factors for other important and frequent comorbidities in people with SMI, is of paramount importance.
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Reina Sofía Hospital (Córdoba, Spain). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
CR–R: Conceptualization, Data curation, Investigation, Methodology, Writing–original draft, Writing–review and editing. MJ–M: Conceptualization, Data curation, Formal Analysis, Methodology, Supervision, Visualization, Writing–original draft, Writing–review and editing. GP: Data curation, Writing–review and editing, Investigation. CG: Data curation, Writing–review and editing. FM: Data curation, Writing–review and editing. MA: Data curation, Writing–review and editing. LC: Data curation, Writing–review and editing. GC: Data curation, Writing–review and editing. NF: Data curation, Writing–review and editing, Validation. IG: Data curation, Writing–review and editing, Formal Analysis. FR-V: Writing–review and editing, Writing–original draft. CC–R: Data curation, Writing–review and editing, Formal Analysis. LG-R: Writing–review and editing. DM: Writing–review and editing. FS: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Methodology, Visualization, Writing–original draft, Writing–review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Project “PI20/01657”, funded by Instituto de Salud Carlos III (ISCIII) and co-funded by the European Union via the European Regional Development Fund (ERDF), “Una manera de hacer Europa”.
Acknowledgments
The authors would like to thank the altruistic and generous participation of all the patients in that project.
Conflict of interest
FS during the last 5 years has been speaker for Rovi and Janssen-Cilag. DM is a consultant to GlaxoSmithKline, AstraZeneca, and Up to Date and is an expert witness on behalf of people suing the tobacco industry. LG-R during the last 5 years has been speaker and advisory board member for Janssen-Cilag, Astra-Zeneca, Rovi, Lundbeck, Otsuka, GSK and Pfizer.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2024.1335798/full#supplementary-material
Abbreviations
AIC, Akaike Information Criterion; CI, confidence intervals; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; FTND, Fagerström Test for Nicotine Dependence; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HDRS, Hamilton Depression Rating Scale; IPAQ, International Physical Activity Questionnaire; METs, metabolic equivalents of task; OR, odds ratio; PANSS, Positive and Negative Syndrome Scale; SMI, serious mental illness; YMRS, Young Mania Rating Scale.
References
Agusti A., Noell G., Brugada J., Faner R. (2017). Lung function in early adulthood and health in later life: a transgenerational cohort analysis. Lancet Respir. Med. 5, 935–945. doi:10.1016/S2213-2600(17)30434-4
Backman H., Eriksson B., Hedman L., Stridsman C., Jansson S. A., Sovijarvi A., et al. (2016). Restrictive spirometric pattern in the general adult population: methods of defining the condition and consequences on prevalence. Respir. Med. 120, 116–123. doi:10.1016/j.rmed.2016.10.005
Becoña E., Vázquez F. L. (1998). The Fagerström test for nicotine dependence in a Spanish sample. Psychol. Rep. 83, 1455–1458. doi:10.2466/pr0.1998.83.3f.1455
Bernardo M., Rico-Villademoros F., García-Rizo C., Rojo R., Gómez-Huelgas R. (2021). Real-world data on the adverse metabolic effects of second-generation antipsychotics and their potential determinants in adult patients: a systematic review of population-based studies. Adv. Ther. 38, 2491–2512. doi:10.1007/s12325-021-01689-8
Collaro A. J., Chang A. B., Marchant J. M., Chatfield M. D., Dent A., Blake T., et al. (2021). Associations between lung function and future cardiovascular morbidity and overall mortality in a predominantly First Nations population: a cohort study. Lancet Reg. Health West Pac 13, 100188. doi:10.1016/j.lanwpc.2021.100188
Correll C. U., Solmi M., Croatto G., Schneider L. K., Rohani-Montez S. C., Fairley L., et al. (2022). Mortality in people with schizophrenia: a systematic review and meta-analysis of relative risk and aggravating or attenuating factors. World Psychiatry 21, 248–271. doi:10.1002/wps.20994
Crump C., Sundquist K., Winkleby M. A., Sundquist J. (2013b). Comorbidities and mortality in bipolar disorder: a Swedish national cohort study. JAMA Psychiatry 70, 931–939. doi:10.1001/jamapsychiatry.2013.1394
Crump C., Winkleby M. A., Sundquist K., Sundquist J. (2013a). Comorbidities and mortality in persons with schizophrenia: a Swedish national cohort study. Am. J. Psychiatry 170, 324–333. doi:10.1176/appi.ajp.2012.12050599
Cuttica M. J., Colangelo L. A., Dransfield M. T., Bhatt S. P., Rana J. S., Jacobs D. R., et al. (2018). Lung function in young adults and risk of cardiovascular events over 29 years: the CARDIA study. J. Am. Heart Assoc. 7, e010672. doi:10.1161/JAHA.118.010672
Dharmage S. C., Bui D. S., Walters E. H., Lowe A. J., Thompson B., Bowatte G., et al. (2023). Lifetime spirometry patterns of obstruction and restriction, and their risk factors and outcomes: a prospective cohort study. Lancet Respir. Med. 11, 273–282. doi:10.1016/S2213-2600(22)00364-2
Dickerson F., Schroeder J., Katsafanas E., Khushalani S., Origoni A. E., Savage C., et al. (2018). Cigarette smoking by patients with serious mental illness, 1999-2016: an increasing disparity. Psychiatr. Serv. 69, 147–153. doi:10.1176/appi.ps.201700118
Eurostat (2023). Tobacco consumption statistics. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Tobacco_consumption_statistics#Daily_smokers_of_cigarettes (Accessed April 14, 2023).
Filik R., Sipos A., Kehoe P. G., Burns T., Cooper S. J., Stevens H., et al. (2006). The cardiovascular and respiratory health of people with schizophrenia. Acta Psychiatr. Scand. 113, 298–305. doi:10.1111/j.1600-0447.2006.00768.x
Fiorillo A., Sartorius N. (2021). Mortality gap and physical comorbidity of people with severe mental disorders: the public health scandal. Ann. Gen. Psychiatry 20, 52. doi:10.1186/s12991-021-00374-y
Friend N., Hughes J., Kisely S., Kumar R., Siskind D. (2020). Appraisal of physical health guidelines for severe mental illness. Aust. Health Rev. 44, 904–915. doi:10.1071/ah20080
Global Initiative for Chronic Obstructive Lung Disease (2022). Global strategy for prevention, diagnosis and management of COPD: 2023 report. Deer Park, USA: Global Initiative for Chronic Obstructive Lung Disease.
Goodwin R. D., Chuang S., Simuro N., Davies M., Pine D. S. (2007). Association between lung function and mental health problems among adults in the United States: findings from the First National Health and Nutrition Examination Survey. Am. J. Epidemiol. 165, 383–388. doi:10.1093/aje/kwk026
Górecka D., Bednarek M., Nowiński A., Puścińska E., Goljan-Geremek A., Zieliński J. (2003). Diagnosis of airflow limitation combined with smoking cessation advice increases stop-smoking rate. Chest 123, 1916–1923. doi:10.1378/chest.123.6.1916
Guerra S., Sherrill D. L., Venker C., Ceccato C. M., Halonen M., Martinez F. D. (2010). Morbidity and mortality associated with the restrictive spirometric pattern: a longitudinal study. Thorax 65, 499–504. doi:10.1136/thx.2009.126052
Guo C., Yu T., Chang L. Y., Bo Y., Yu Z., Wong M. C. S., et al. (2021). Mortality risk attributable to classification of chronic obstructive pulmonary disease and reduced lung function: a 21-year longitudinal cohort study. Respir. Med. 184, 106471. doi:10.1016/j.rmed.2021.106471
Hayes J. F., Miles J., Walters K., King M., Osborn D. P. (2015). A systematic review and meta-analysis of premature mortality in bipolar affective disorder. Acta Psychiatr. Scand. 131, 417–425. doi:10.1111/acps.12408
Higbee D. H., Granell R., Davey Smith G., Dodd J. W. (2022). Prevalence, risk factors, and clinical implications of preserved ratio impaired spirometry: a UK Biobank cohort analysis. Lancet Respir. Med. 10, 149–157. doi:10.1016/s2213-2600(21)00369-6
Honda Y., Watanabe T., Shibata Y., Otaki Y., Kadowaki S., Narumi T., et al. (2017). Impact of restrictive lung disorder on cardiovascular mortality in a general population: the Yamagata (Takahata) study. Int. J. Cardiol. 241, 395–400. doi:10.1016/j.ijcard.2017.04.049
Jaen-Moreno M. J., Feu N., Del Pozo G. I., Gómez C., Carrión L., Chauca G. M., et al. (2021). Chronic obstructive pulmonary disease in severe mental illness: a timely diagnosis to advance the process of quitting smoking. Eur. Psychiatry 64, e22. doi:10.1192/j.eurpsy.2021.12
Jaén-Moreno M. J., Rico-Villademoros F., Ruiz-Rull C., Laguna-Muñoz D., Del Pozo G. I., Sarramea F. (2023). A systematic review on the association between schizophrenia and bipolar disorder with chronic obstructive pulmonary disease. Copd 20, 31–43. doi:10.1080/15412555.2022.2154646
Kaaks R., Christodoulou E., Motsch E., Katzke V., Wielpütz M. O., Kauczor H. U., et al. (2022). Lung function impairment in the German Lung Cancer Screening Intervention Study (LUSI): prevalence, symptoms, and associations with lung cancer risk, tumor histology and all-cause mortality. Transl. Lung Cancer Res. 11, 1896–1911. doi:10.21037/tlcr-22-63
Karadogan D., Onal O., Kanbay Y. (2018). Prevalence and determinants of smoking status among university students: artvin coruh university sample. PLoS One 13, e0200671. doi:10.1371/journal.pone.0200671
Lamb K., Theodore D., Bhutta B. S. (2022). “Spirometry,” in StatPearls. Treasure island (FL): StatPearls publishing copyright © 2022 (Petersburg, Florida, United States: StatPearls Publishing LLC).
Liu N. H., Daumit G. L., Dua T., Aquila R., Charlson F., Cuijpers P., et al. (2017). Excess mortality in persons with severe mental disorders: a multilevel intervention framework and priorities for clinical practice, policy and research agendas. World Psychiatry 16, 30–40. doi:10.1002/wps.20384
Miller M. R., Hankinson J., Brusasco V., Burgos F., Casaburi R., Coates A., et al. (2005). Standardisation of spirometry. Eur. Respir. J. 26, 319–338. doi:10.1183/09031936.05.00034805
Olfson M., Gerhard T., Huang C., Crystal S., Stroup T. S. (2015). Premature mortality among adults with schizophrenia in the United States. JAMA Psychiatry 72, 1172–1181. doi:10.1001/jamapsychiatry.2015.1737
Partti K., Vasankari T., Kanervisto M., Perala J., Saarni S. I., Jousilahti P., et al. (2015). Lung function and respiratory diseases in people with psychosis: population-based study. Br. J. Psychiatry 207, 37–45. doi:10.1192/bjp.bp.113.141937
Pillinger T., McCutcheon R. A., Vano L., Mizuno Y., Arumuham A., Hindley G., et al. (2020). Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis. Lancet Psychiatry 7, 64–77. doi:10.1016/s2215-0366(19)30416-x
Ramalho S. H. R., Claggett B. L., Washko G. R., Estepar R. S. J., Chang P. P., Kitzman D. W., et al. (2022). Association of pulmonary function with late-life cardiac function and heart failure risk: the ARIC study. J. Am. Heart Assoc. 11, e023990. doi:10.1161/JAHA.121.023990
Roman B., Majem L. S., Hagströmer M., Ramon J. M., Ribas L., Sjöström M. (2006). International physical activity questionnaire: reliability and validity in Spain. Med. Sci. Sports Exerc 38, S563. doi:10.1249/00005768-200605001-03214
Ross R., Neeland I. J., Yamashita S., Shai I., Seidell J., Magni P., et al. (2020). Waist circumference as a vital sign in clinical practice: a consensus statement from the IAS and ICCR working group on visceral obesity. Nat. Rev. Endocrinol. 16, 177–189. doi:10.1038/s41574-019-0310-7
Saha S., Chant D., McGrath J. (2007). A systematic review of mortality in schizophrenia: is the differential mortality gap worsening over time? Arch. Gen. Psychiatry 64, 1123–1131. doi:10.1001/archpsyc.64.10.1123
Sarycheva T., Capkova N., Pająk A., Malyutina S., Simonova G., Tamosiunas A., et al. (2022). Impaired lung function and mortality in Eastern Europe: results from multi-centre cohort study. Respir. Res. 23, 140. doi:10.1186/s12931-022-02057-y
Shah C. H., Reed R. M., Liang Y., Zafari Z. (2021). Association between lung function and future risks of diabetes, asthma, myocardial infarction, hypertension and all-cause mortality. ERJ Open Res. 7, 00178–02021. doi:10.1183/23120541.00178-2021
Sin D. D., Wu L., Man S. F. (2005). The relationship between reduced lung function and cardiovascular mortality: a population-based study and a systematic review of the literature. Chest 127, 1952–1959. doi:10.1378/chest.127.6.1952
Sperandio E. F., Arantes R. L., Matheus A. C., Silva R. P., Lauria V. T., Romiti M., et al. (2016). Restrictive pattern on spirometry: association with cardiovascular risk and level of physical activity in asymptomatic adults. J. Bras. Pneumol. 42, 22–28. doi:10.1590/s1806-37562016000000030
Stanojevic S., Kaminsky D. A., Miller M. R., Thompson B., Aliverti A., Barjaktarevic I., et al. (2022). ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur. Respir. J. 60, 2101499. doi:10.1183/13993003.01499-2021
Teixeira A. L., Martins L. B., Berk M., Bauer M. E. (2022). Severe psychiatric disorders and general medical comorbidities: inflammation-related mechanisms and therapeutic opportunities. Clin. Sci. (Lond) 136, 1257–1280. doi:10.1042/cs20211106
Vancampfort D., Probst M., Stubbs B., Soundy A., De Herdt A., De Hert M. (2014a). Associations between expiratory spirometry parameters and limitations in daily life activities in patients with schizophrenia. Gen. Hosp. Psychiatry 36, 172–176. doi:10.1016/j.genhosppsych.2013.11.001
Vancampfort D., Probst M., Stubbs B., Soundy A., De Herdt A., De Hert M. (2014b). Metabolic syndrome and lung function in schizophrenia: a pilot study. Psychiatry Res. 220, 58–62. doi:10.1016/j.psychres.2014.06.008
Viejo Casas A., Amado Diago C., Agüero Calvo J., Gómez-Revuelta M., Ruiz Núñez M., Juncal-Ruiz M., et al. (2024). Individuals with psychosis present a reduced lung diffusion capacity and early spirometry alterations: results from a cross-sectional study. J. Psychosom. Res. 176, 111554. doi:10.1016/j.jpsychores.2023.111554
Wan E. S., Balte P., Schwartz J. E., Bhatt S. P., Cassano P. A., Couper D., et al. (2021). Association between preserved ratio impaired spirometry and clinical outcomes in US adults. Jama 326, 2287–2298. doi:10.1001/jama.2021.20939
Wang M. T., Tsai C. L., Lin C. W., Yeh C. B., Wang Y. H., Lin H. L. (2017). Association between antipsychotic agents and risk of acute respiratory failure in patients with chronic obstructive pulmonary disease. JAMA Psychiatry 74, 252–260. doi:10.1001/jamapsychiatry.2016.3793
Wehrmeister F. C., Menezes A. M., Muniz L. C., Martínez-Mesa J., Domingues M. R., Horta B. L. (2012). Waist circumference and pulmonary function: a systematic review and meta-analysis. Syst. Rev. 1, 55. doi:10.1186/2046-4053-1-55
Wilson H., Ridley S. (2007). Antipsychotic drugs and the acute respiratory distress syndrome. Br. J. Anaesth. 99, 301–302. doi:10.1093/bja/aem195
Keywords: serious mental illness, schizophrenia, bipolar disorder, spirometry, obstructive, restrictive, preserved ratio impaired spirometry
Citation: Ruiz-Rull C, Jaén-Moreno MJ, del Pozo GI, Gómez C, Montiel FJ, Alcántara M, Carrión L, Chauca GM, Feu N, Guler I, Rico-Villademoros F, Camacho-Rodríguez C, Gutierrez-Rojas L, Mannino D and Sarramea F (2024) Low lung function in Bipolar Disorder and Schizophrenia: a hidden risk. Front. Physiol. 15:1335798. doi: 10.3389/fphys.2024.1335798
Received: 20 November 2023; Accepted: 15 March 2024;
Published: 25 April 2024.
Edited by:
Christophe Delclaux, Hôpital Robert Debré, FranceCopyright © 2024 Ruiz-Rull, Jaén-Moreno, del Pozo, Gómez, Montiel, Alcántara, Carrión, Chauca, Feu, Guler, Rico-Villademoros, Camacho-Rodríguez, Gutierrez-Rojas, Mannino and Sarramea. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María José Jaén-Moreno, mjjaen@uco.es
†These authors have contributed equally to this work