 Inés Rivero Belenchón1,2*†
Inés Rivero Belenchón1,2*† Juan Gómez Rivas2,3†
Juan Gómez Rivas2,3† Rafael Antonio Medina López1
Rafael Antonio Medina López1 Enrico Checcucci2,4,5
Enrico Checcucci2,4,5 Mark Taratkin2,6
Mark Taratkin2,6 Stefano Puliatti2,7
Stefano Puliatti2,7 Karl-Friedrich Kowalewski2,8
Karl-Friedrich Kowalewski2,8 Giovanni Cacciamani2,9Carmen Belén Congregado Ruíz1
Giovanni Cacciamani2,9Carmen Belén Congregado Ruíz1 Cristina Castro10
Cristina Castro10 Dmitry Enikeev6
Dmitry Enikeev6 Pablo Abad-Lopez3
Pablo Abad-Lopez3 Fivos Panetsos10,11,12Jesús Moreno-Sierra3
Fivos Panetsos10,11,12Jesús Moreno-Sierra3- 1Urology and Nephrology Department, University Hospital Virgen del Rocío, Biomedical Institute of Seville (IBiS)/University Hospital Virgen del Rocío/CSIC/University of Seville, Seville, Spain
- 2Young Academic Urologist-Urotechnology Working Party (ESUT-YAU), European Association of Urology, Arnhem, Netherlands
- 3Urology Department, Hospital Clínico San Carlos, Madrid, Spain
- 4Department of Urology, San Luigi Gonzaga Hospital, University of Turin, Turin, Italy
- 5Department of Surgery, Candiolo Cancer Institute, FPO-IRCCS, Turin, Italy
- 6Institute for Urology and Reproductive Health, Sechenov University, Moscow, Russia
- 7Department of Urology, University of Modena and Reggio Emilia, Modena, Italy
- 8Department of Urology, University Medical Center Mannheim, University of Heidelberg, Mannheim, Germany
- 9Catherine and Joseph Aresty Department of Urology, USC Institute of Urology, University of Southern California, Los Angeles, CA, United States
- 10Neurocomputing and Neurorobotics Research Group, Complutense University of Madrid (UCM), Madrid, Spain
- 11Institute of Health Research, San Carlos Clinical Hospital (IdISSC), Madrid, Spain
- 12Silk Biomed SL, Madrid, Spain
Prostate cancer is the most common cancer amongst men, and one of its treatments in the localized stage is radical prostatectomy (RP). This technique achieves a high success rate regarding oncological results, but one of its main drawbacks are sexual disorders, especially erectile dysfunction, ranging from 14-90% of the cases. Therefore, surgery advancements in the last decade have been focused on minimizing the impact on patient’s functioning. Now is time for a step forward in the recovery of functional outcomes after RP. Bioengineering solutions such as stem-cell therapy and tissue engineering hold great opportunities for the treatment of all tissues and organs dysfunctions, which may help in neuroprotection and neuro-regeneration. Specifically, the use of Dehydrated human amnion/chorion membrane (dHACM) allografts and chitosan membranes (ChiMe) aims at reconstructing damaged neurovascular plexuses of the urogenital system to support erectile function recovery. Some research is being done on this topic, and promising results are emerging.
Introduction
Prostate cancer (PCa) is one of the most common malignant tumors in the world, the second leading cause of cancer deaths in the United States, where the number of new cases and deaths in 2022 is estimated at 268,490 and 34500, respectively (1). According to the guidelines, radical prostatectomy (RP) in patients with localized PCa is one of the most recommended therapeutic approaches (2, 3). Despite the high success rate regarding oncological results, and even though nerve-sparing is performed, postoperative erectile dysfunction (ED) is one of its most common adverse effects (4). It ranges 14-90% of the cases, depending on the surgical approach and experience: 70.4% after robot-assisted laparoscopic prostatectomy and 74.7% after retropubic RP (adjusted OR 0.81; 95%CI 0.66-0.98) in a prospective, controlled, nonrandomized trial (5).
Post-radical prostatectomy erectile dysfunction (post-RP ED) can have a devastating effect on men’s quality of life due to the feelings of lost self-esteem, manliness, and negative change to self-image (6). The conjunction of the negative psychological aspect, with the increasing proportion of young men undergoing RP thanks to the higher detection rate of PCa, has focused the attention on the importance of postoperative erectile recovery. Nowadays, recovery of erectile function can occur only through a rehabilitation process that prevents fibrosis and end-organ damage while the nerves and vasculature attempt to recover. However, clear guidelines for penile rehabilitation after RP are not easily provided based on current randomized clinical trials (7). In addition, while approaches for peripheral nerve repair have improved over the last few decades, functional recovery is usually incomplete. As a result, much attention has been given by researchers and clinicians to cell-based therapies and tissue engineering (8–11).
Our objective is to perform a narrative review about the current status of tissue engineering for neurovascular bundles (NVB) regeneration after RP.
Evidence acquisition
In February 2022 a computerized literature search of papers published up to February 2022 was performed on different electronic databases including PubMed, the Cochrane Library, Embase, and Web of Science to identify original articles and reviews. Although it was a narrative review, the literature search and the study selection were performed according to the Preferred reporting items for Systematic reviews and Meta-analyses (PriSMa) criteria and the Population, intervention, comparator, outcomes (PICO) methodology (12, 13). Population consisted of patients with ED after RP (P). Treatments of interest were both stem-cell therapy and tissue engineering (I). We considered eligible single or multiple arms studies, so no comparator was mandatory (C). Main outcomes of interest were the erectile function recovery after RP with new therapies, Stem-Cell and Tissue Engineering (O).
Studies identification
2328 articles using the terms “erectile dysfunction” AND “prostatectomy” were found. Out of them, 522 were reviews and systematic reviews. With the terms “neurovascular regeneration” AND “erectile dysfunction” AND “prostatectomy” 34 articles were found, 29 original articles and 5 reviews. The consistency of this revision is affected by the inherent lack of robust evidence in urology.
Screening
After duplicates were removed, 1745 articles were screened by title and abstract. Out of them, 158 full-text articles were assessed for eligibility.
Eligibility
The selection criteria were a) Reviews and original articles, b) Studies about NV regeneration for ED after RP. Exclusion criteria were a) Non-English/Spanish literature, b) Preclinical studies, editorials, comments, letters, c) Studies about non-post RP ED and tissue engineering not applied after RP, d) Studies published before 2000 as they were not enough updated to our purpose.
Study analysis
After applying the above eligibility criteria, 27 studies about erectile dysfunction and prostatectomy were selected and 11 regarding neurovascular regeneration and erectile dysfunction after radical prostatectomy. In total, 38 articles with the highest level of relevance to the discussed topics were selected with the consensus of the authors. A narrative review from the selected studies was conducted. Figure 1 shows the PRISMA flow diagram used for the screening process.
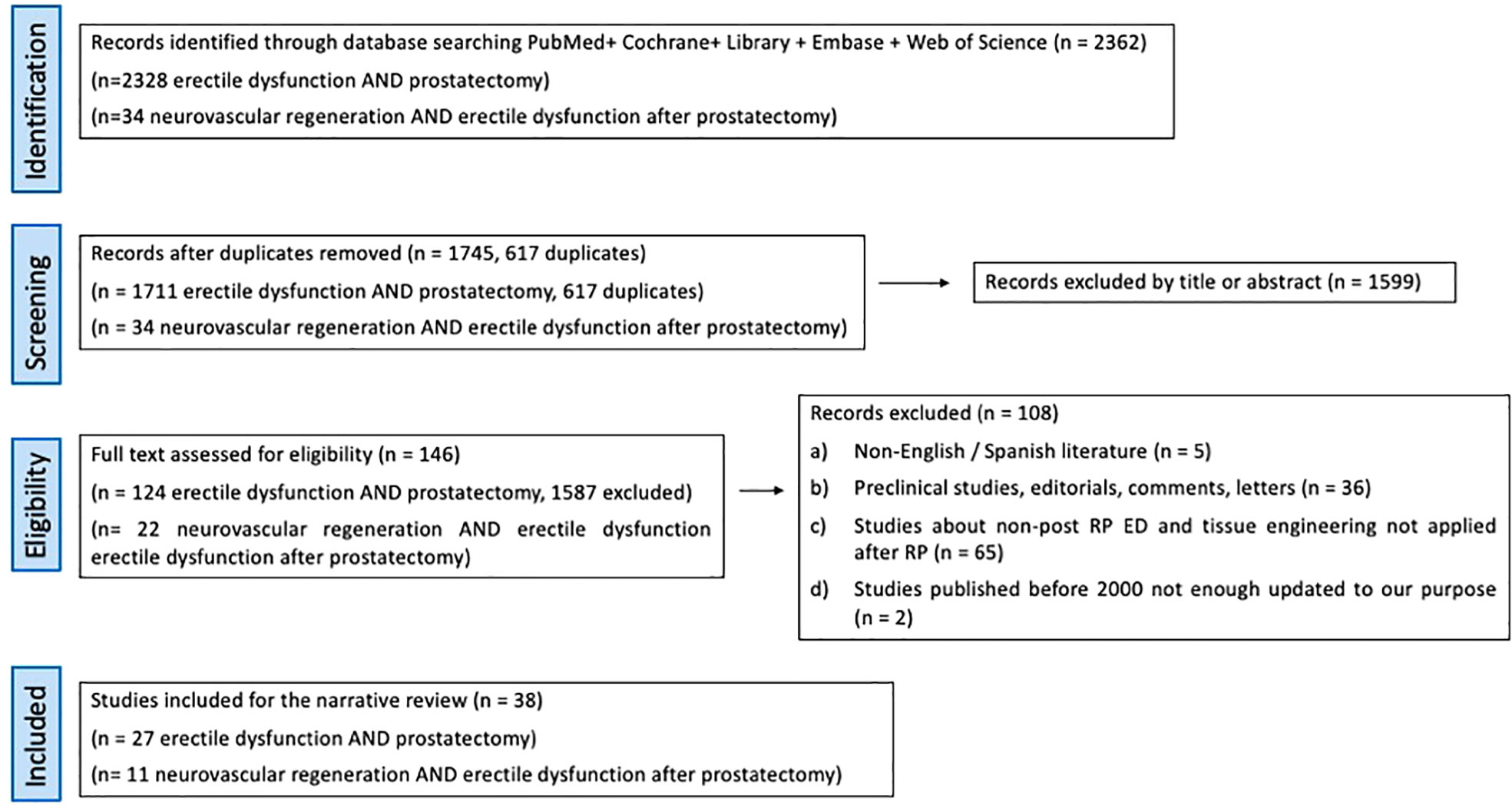
Figure 1 PRISMA flow diagram of the screening process.
Erectile dysfunction management after radical prostatectomy
Over recent decades, knowledge of peri-prostatic anatomical structures has increased in unison with the development of the RP surgical technique. Nevertheless, even in the case of meticulous preservation of the peri-prostatic NVBs, a period of convalescence characterized by unrecovered potency remains (5). Such a delay in potency recovery is probably due to the surgical trauma to the anatomical structures and inflammatory responses from the traction of the NVBs (4).
Still knowing the inherent ED problem related to RP, there is no consensus about its best management. Current therapeutic approaches include:
Oral medications
Type-5 phosphodiesterase (PDE5) inhibitors have been tested in managing ED and has been proven that its mechanism of action is related to the potency dysfunction etiology. After RP, neurologic injury occurs, and penile hypoxia and fibrosis lead to the absence of spontaneous nocturnal erections, which decreases the release of nitric oxide (14, 15), which leads to a drop in the amount of available cyclic guanosine monophosphate (cGMP) (16, 17). PDE5 inhibitors inhibit the mentioned enzyme, which metabolizes cGMP, and this results in an increase in cGMP levels (16), which coupled with nitric oxide induces corporal smooth muscle relaxation, and this leads to subsequent erection by allowing blood flow to the penis (18).
Intracavernosal medications and intraurethral suppositories
Medications such as prostaglandin E1 (PGE1) are a reasonable first-line ED therapy administered through penile corpora or urethra. Compared to the intraurethral mode, the intracavernosal administration has demonstrated to be more effective in restoring penile blood flow and erectile function. However, the side effects such as penile pain along with the risk of urethral infections and hematoma reduce the acceptance of therapy and lead to high discontinuation rates (19). In contrast, the available data for intraurethral suppositories point to its positive effects through be regularly used after nerve-sparing RP (NSRP) (20).
Vacuum erection devices (VEDs)
A manually created negative pressure gradient draws blood into the corporal bodies to provoke an erection. However, many clinicians dismiss this option, since it has been shown that the erection provoked by VEDs consists of 5% arterial blood and 42% venous blood with a SaO2 of 76% which makes it questionable whether this erection will provide sufficient oxygen saturation of the corporal tissue to prevent future fibrosis (21).
Penile prosthesis implantation
This is an invasive surgical approach, limited for patients with end-stage ED following RP (22). According to studies, although patients and partners are usually satisfied with the device, only 54% of them would recommend surgical treatment with no reservations (23).
Low-intensity extracorporeal shock wave therapy (Li-ESWT)
It is still considered investigational (24) and has been mainly studied in vasculogenic ED (25). After RP there is little evidence supporting its use. In 2021 a randomized clinical trial was published demonstrating a slight increase in mean IIEF-5 in men treated with Li-ESWT vs. placebo, but with a doubtful impact on sexual effect (26).
Despite the advancements in the surgical technique and ED management after RP, we do not observe a significant change in sexual function recovery (27). Consequently, additional strategies are required to improve sexual potency outcomes (28).
Stem-cell therapy FOR neurogenic regeneration after radical prostatectomy
Stem cells could promote the regeneration of the nerve axons either directly, through the local action of the neurotrophic and neurotropic biomolecules of their secretome, or indirectly, by stimulating the systemic secretion of neuroregenerative factors. Furthermore, stem cells have a strong modulatory action on the inflammatory processes, moderating pro-inflammatory and intensifying anti-inflammatory cytokines, for example, by decreasing lymphotoxin TNF-α, interferon gamma INF-γ and interleukin IL-12, while increasing interleukins IL-4 and IL-10. In this context, stem cell therapy (SCT) has shown a positive effect on ED in both animal and human studies. However, the numbers of clinical trials investigating SCT on humans with ED after RP are minimal (29, 30).
Haahr et al. (31) performed a 6-month follow-up phase I study assessing treatment with autologous adipose-derived regenerative cells (ADRCs) administered by an intracavernous injection in 17 men with post-RP ED. Eight of them reported erectile response adequate for sexual intercourse. The same authors reported a 12-month follow-up study (32), showing no serious adverse effects after 12 months, IIEF-5 scores increased at 6 months, and this was sustained after 12 months. This improvement was observed in patients who had a normal pre-operative erectile function and were continent at inclusion (32). Yiou et al., reported the safety and effect of bone marrow-derived mononuclear cells (BM-MNCs) in 12 post-RP patients with vasculogenic ED (33). Significant improvements in intercourse satisfaction and erectile function domains of IIEF-15 and EHS were noted at 6 months follow-up, and clinical benefit was sustained after one year. Furthermore, the same authors collected a longer-term follow-up (mean, 62.1 months) data set showed a lack of adverse events and slightly decreased erectile function score compared with data acquired at the 12-month time point (34). Table 1 summarizes the results of these studies.
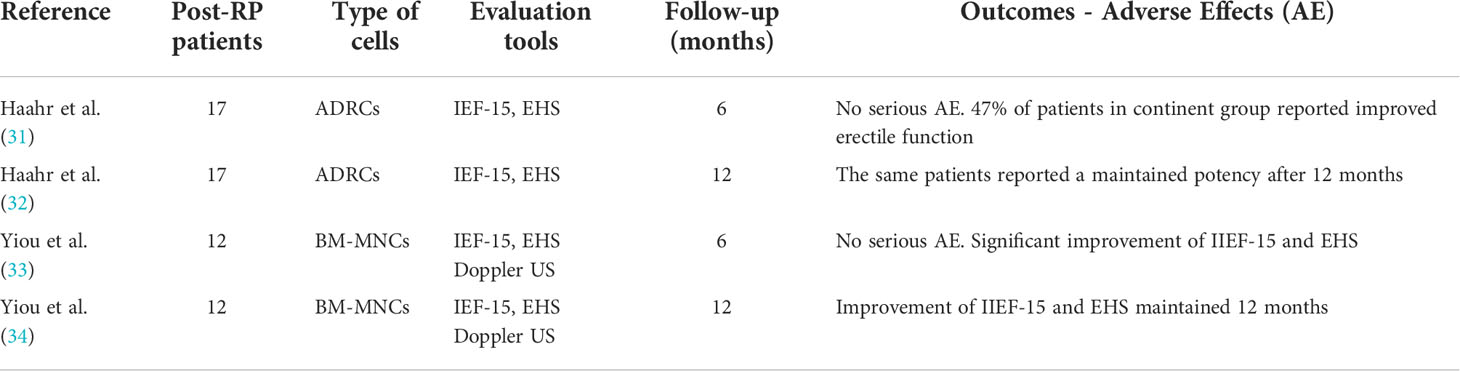
Table 1 Results of clinical trials of intracavernous injection of stem cells in patients with post-radical prostatectomy erectile dysfunction.
Tissue engineering for neurovascular bundles regeneration after radical prostatectomy
In the last few years, the attention on ED management after RP has been redirected from cell-based therapies applied on men with ED not responding to standard therapies, to tissue engineering applied during the surgery to help regenerate the neurovascular plexus with the intention of accelerating potency recovery and preventing the appearance of an established post-RP ED.
Tissue Engineering holds excellent opportunities for the treatment of all tissues and organs dysfunctions, including acute injuries, heart failure, stroke, diabetes, cancer, and neurodegenerative diseases (35–39). Bioprinting technologies are opening the way to obtain additional biomaterial formats and tissue architectures (40).
Reconstructing damaged neurovascular plexuses of the urogenital system is a complex biological process, which implies the combined regeneration of neural and vascular tissue (37). This investigational field is still in an early stage and needs time to develop. However, there is already evidence supporting the use of different biomaterials to promote neurovascular regeneration after RP. All of them have in common the use of tissue engineering scaffolds that are biocompatible, non-toxic, biodegradable, permeable, and noninflammatory (41). In addition, they all should prevent fibrous scar tissue invasion but allow local revascularization to improve nutrient and oxygen supply (42), meaning that an appropriate biomaterial selection is fundamental to a positive clinical outcome. Promising approaches consider the development of structured biomimetic devices mimicking the physical, biological and biomolecular characteristics of the nerves, with differentiated biomolecular environments, each dedicated to a specific modality of nerve fibers (43–45).
Dehydrated human amnion/chorion membrane (dHACM) allografts and chitosan membranes (ChiMe) have been employed in several studies:
Patel et al. (46) conducted a propensity score–matched analysis on 58 patients aimed to evaluate if the use of a dHACM allograft wrapped around the NVBs during robot-assisted RP (RARP) can accelerate the return to normal functioning. All the patients were preoperatively potent and underwent a full NSRP. After a minimum follow-up of 8 weeks, the authors concluded that the application of dHACM in patients accelerates the recovery of potency and continence without an increase on operative time or blood loss compared to patients who did not receive the membranes. No post-RARP rehabilitation protocol is described in this study. A couple of years later, this group also stated that this faster return to potency occurs regardless of the degree of the NVBs preservation after a penile rehabilitation program, and those younger patients (<55 years of age) had the highest overall advantage if they received the graft. Furthermore, they also showed that dHACM placement at the prostatic NVB did not increase the risk of biochemical recurrence (47). Finally, they have recently published the medium-term outcomes with a minimum follow up of 12 months (48), and although patients were selected following different inclusion and exclusion criteria, they showed that dHACM allowed for the return of potency at an average time of 3 months, with an overall shorter period for continence recovery and 10% of biochemical recurrence, similar to the early oncological results reported in the literature (49). In this case, no specific post-RARP rehabilitation protocol is described. Similarly, Razdan et al. (50) matched 1400 patients undergoing full bilateral NSRP by a single surgeon, wherein 700 patients had dHACM allograft wrapped around the NVB, and 700 did not, with a retrospective follow-up of 1 year. Patients were initiated on a penile rehabilitation program, wherein they received a PDE-5 inhibitor every night (Tadalafil 5 mg) starting 3 weeks after surgery and a vacuum erection device or alprostadil injection/urethral suppository twice a week starting 4 weeks after surgery for the duration of the study. Patients with dHACM were 3.86 times (95% CI 2.43–6.13) more likely to achieve potency in the same period when compared with the control group. Recently, Barski et al. (51) published the protocol of a randomized clinical trial (NCT03864939) that is on recruitment phase, to study the efficacy and safety of dHACM placed around the NVB and vesicourethral anastomosis during RP in combination with a rehabilitation training program.
ChiMe has been widely used in a variety of biomedical applications, including peripheral nerve repair, due to its excellent biocompatibility, biodegradability, ready availability, and antibacterial properties (52). Porpiglia et al. conducted a preliminary phase II study with 140 patients to apply ChiMe on the NVBs after NS robot-assisted RP (NS-RARP) showing the feasibility and safety of applying ChiMe on the NVBs. In this case, all patients received a PDE5-inhibitor (Tadalafil 20 mg twice/week) for 3 months after NS-RARP and, subsequently, PDE5-i was continued if required. Authors found a trend towards a faster recovery of erectile function after 6 months of follow-up (53). Moreover, the advantage of ChiMe in terms of potency recovery was maintained during a 12-month follow-up period without compromising the length, the difficulty, or the complication rate of the ‘standard’ procedure and without compromising the short-term oncological efficacy of RP (54). This indicates that the application of ChiMe after NS-RARP may serve as a valuable adjunct approach to support functional recovery of the periprostatic NVB and its target tissue.
Table 2 summarizes the above detailed studies.
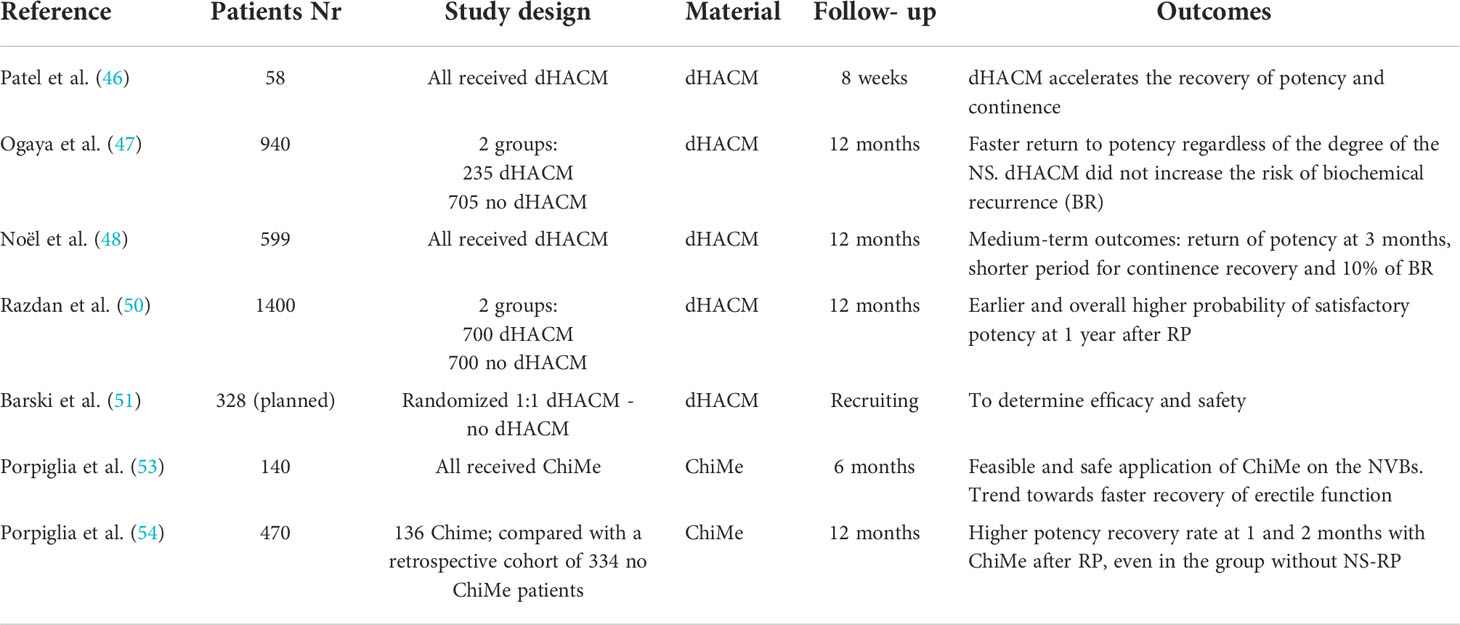
Table 2 Results of clinical trials of dehydrated human amnion/chorion membrane (dHACM) allografts and chitosan membranes (ChiMe) wrapped around the NVBs during robot-assisted RP.
A future insight
Some groups have done recent research showing promising results on new ways of nerve restoring. Yonesi et al. (55) showed the properties of silk fibroin successfully used for nerve restoration in a variety of applications, including neurodegenerative diseases, strokes, and damaged peripheral nerves. Its flexible and adaptable biomaterial, low or null immune response, lack of cell toxicity, inertness, and inflammatory response lower than other biomaterials makes it one of the most appropriate for neural scaffolding. Currently, part of this group is trying to apply silk fibroin-based fibers, and graphene as supporting material for NVBs regeneration after RP.
Other study groups have shown encouraging results on different approaches to ED in animals that might be seen in human clinical trials in the next few years. Gu et al. (56) used Human Placental Stem Cells in a pelvic neurovascular injury rat model showing that this therapy effectively restores the erectile tissue and function in this animal model. Ghatak K et al. (57) demonstrated that Dickkopf2, which is a secreted protein that acts enhancing endothelial cell migration, is reported to promote mature and stable blood vessel formation, rescues erectile function by enhancing neurovascular regeneration in mouse model of cavernous nerve injury. Recently, the same group experimented with Pericyte-Derived Extracellular Vesicle-Mimetic nanovesicles in rats with cavernous nerve injury proving significantly improved erectile function by enhancing neurovascular regeneration (58).
Good outcomes when proving some new substances in vitro have been described. Weyne et al. (59) demonstrated that Galanin administration partially restores erectile function after cavernous nerve injury in vitro. The authors affirmed that endogenous neurotrophins such as galanin could be used as a strategy to improve EF for patients after radical prostatectomy.
Discussion
Over the last two decades, many steps have been taken towards a better understanding of prostatic anatomy and the surgical technique of RP. With specific regard to potency recovery, the preservation of the neurovascular periprostatic network is a crucial step to restore postoperative erectile function (4). However, as stated in the review performed by Marchioni et al. (22) advances in surgery do not seem to rebound on functional outcomes, making it necessary to apply different treatments to recover potency after RP. In that sense, PDE5- inhibitors used after RP have shown some benefit on erectile function (60, 61), leading to a faster potency recovery when associated with vacuum devices (62).
However, it should also be considered that ED after prostatic surgery is multifactorial, deriving from both vasculogenic and neurogenic causes. Nowadays, it is known that inflammation, traction, and diathermy of the NVBs during RP provokes an injury in the pelvic autonomic nerves that can range from neuropraxia, axonotmesis and neurotmesis, as well as muscle degeneration that can delay potency recovery (53)
Recently, the innovations made in this field have transcended the mere technical aspects of NS surgery, focusing on the study of biological alterations of the prostatic NVBs due to neuropraxia induced by surgical dissection. Stem cell therapy administered by intracavernous injections has been proved to enhance potency after stablished post-RP ED (31–34).
Various bioengineering neuro-regenerative materials, such as dHACM and ChiMe, have been developed to be used intraoperatively to prevent and precociously treat post-surgical ED. Those materials help hemostasis regulation, inflammation remodeling, and leukocytes, platelets, fibroblasts, and vascular smooth muscle cells recruiting. In addition, they have a pro-regenerative effect on somatic neuronal ganglia and autonomic neuronal ganglia proved on in-vitro and animal models (63). Altogether have shown positive effects to shorten erectile function recovery after both NSRP (46, 48–53) and non-NSRP (47, 54).
Some encouraging results regarding functional outcomes have been demonstrated in this field. dHACM have been used after RP in large clinical studies demonstrating earlier recovery of potency and continence without a higher biochemical recurrence rate (10%). Currently, the first clinical trial in this field is recruiting patients trying to demonstrate the efficacy and safety of this material. Another group recently used ChiMe for the same purpose and showed a higher potency recovery at 1 and 2 months after RP.
Nonetheless, though positive functional outcomes have been published, a long-term oncological investigation on the use of these materials during RP is warranted due to the absence of published literature in this area. In addition, in the coming years, we will probably see an explosion of clinical studies on this field with the use of different materials, such as placental stem cells and Galanin, to earlier restore erectile function after RP.
Conclusion
Concluding, ED after RP is an important issue that deeply affects men’s quality of life and self-esteem. In the last years, efforts have been focused on enhancing function recovery after RP and preventing the appearance of an established ED. Despite the limitations of this narrative review to properly sum up all the available evidence, it seems that tissue engineering applied during the surgery is showing promising results. However, this is an investigational field that is beginning but with a long way to go.
Author contributions
Conception and Design: IRB and JGR; Definition of Search strategy: EC, SP, and CC; Screening title and abstract and full text: RML and CBCR; Manuscript draft: IRB, JGR, FP, MT, and DE; Critical Review: GC, PA-L, K-FK, and JM-S. All authors contributed to the article and approved the submitted version.
Acknowledgments
We gratefully acknowledge financial support received from the Spanish Ministerio de Economía y Competitividad through grant MAT2015-66666-C3-3-R (FP), Comunidad de Madrid, Spain through grant Neurocentro-B2017/BrMD-3760 (FP), Centro de Desarrollo Tecnológico e Industrial - CDTI through grant 00123395/SNEO-20191263 (FP); predoctoral FPU grant from the Banco Santander - Universidad Complutense de Madrid (CCD).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics. Cancer J Clin (2022) 72:7–33. doi: 10.3322/caac.21708
2. Mottet N, Cornford P, et al. EAU guidelines on prostate cancer (2022). Available at: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-EANM-ESTRO-ESUR-ISUP_SIOG-Guidelines-on-Prostate-Cancer-2022.pdf.
3. Shaeffer E, Srinivas S. Clinical practice guidelines in oncology: prostate cancer (2021). Available at: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf.
4. Walsh PC. The discovery of the cavernous nerves and development of nerve-sparing radical retropubic prostatectomy. J Urol (2007) 177(5):1632–5. doi: 10.1016/j.juro.2007.01.012
5. Haglind E, Carlsson S, Stranne J, Wallerstedt A, Wilderäng U, Thorsteinsdottir T, et al. Urinary incontinence and erectile dysfunction after robotic versus open radical prostatectomy: A prospective, controlled, nonrandomised trial. Eur Urol (2015) 68(2):216–25. doi: 10.1016/j.eururo.2015.02.029
6. Wennick A, Joünsson AK, Bratt O, Stenzelius K. Everyday life after a radical prostatectomy: A qualitative study of men under 65 years of age. Eur J Oncol Nurs (2017) 30:107–12. doi: 10.1016/j.ejon.2017.08.008
7. Salonia A, Burnett AL, Graefen M, Hatzimouratidis K, Montorsi F, Mulhall JP, et al. Prevention and management of postprostatectomy sexual dysfunctions part 2: recovery and preservation of erectile function, sexual desire, and orgasmic function. Eur Urol (2012) 62(2):273–86. doi: 10.1016/j.eururo.2012.04.047
8. Samii M, Carvalho GA, Nikkhah G, Penkert G. Surgical reconstruction of the musculocutaneous nerve in traumatic brachial plexus injuries. J Neurosurg (1997) 87(6):881–6. doi: 10.3171/jns.1997.87.6.0881
9. Lundbord G. Enhancing posttraumatic nerve regeneration. J Peripheral Nervous System (2002) 7:139–40. doi: 10.1046/j.1529-8027.2002.02019.x
10. Geuna S, Papalia I, Tos P. End-to-side (terminolateral) nerve regeneration: A challenge for neuroscientists coming from an intriguing nerve repair concept. Brain Res Rev (2006) 52(2):381–8. doi: 10.1016/j.brainresrev.2006.05.002
11. Höke A. Mechanisms of disease: what factors limit the success of peripheral nerve regeneration in humans? Nat Clin Pract Neurol (2006) 2:448–54. doi: 10.1038/ncpneuro0262
12. Moher D, liberati A, Tetzlaff J, Altman Dg, PriSMa group. Preferred reporting items for systematic reviews and me- ta-analyses: The PriSMa statement. Int J Surg (2010) 8:336–41. doi: 10.1016/j.ijsu.2010.02.007
13. Shamseer l, Moher D, Clarke M,ghersi D, liberati A, Pet- ticrew M, PriSMa-P group. Preferred reporting items for systematic review and meta-analysis protocols (PriSMa-p) 2015: elaboration and explanation. BMJ (2015) 350:g7647–7647. doi: 10.1136/bmj.g7647
14. Zippe CD, Pahlajani G. Penile rehabilitation following radical prostatectomy: role of early intervention and chronic therapy. Urol Clin North Am (2007) 34:601–18. doi: 10.1016/j.ucl.2007.08.012
15. Defade BP, Carson CC, Kennelly MJ. Postprostatectomy erectile dysfunction: the role of penile rehabilitation. Rev Urol (2011) 13:6–13.
16. Raina R, Lakin MM, Agarwal A, Sharma R, Goyal KK, Montague DK, et al. Long-term effect of sildenafil citrate on erectile dysfunction after radical prostatectomy: 3-year follow-up. Urology (2003) 62:110–5. doi: 10.1016/S0090-4295(03)00157-2
17. Padma-Nathan H, McCullough AR, Levine LA, Lipshultz LI, Siegel R, Montorsi F, et al. Randomized, double-blind, placebo-controlled study of postoperative nightly sildenafil citrate for the prevention of erectile dysfunction after bilateral nerve-sparing radical prostatectomy. Int J Impot Res (2008) 20:479–86. doi: 10.1038/ijir.2008.33
18. Lagoda G, Jin L, Lehrfeld TJ, Liu T, Burnett AL. FK506 and sildenafil promote erectile function recovery after cavernous nerve injury through antioxidative mechanisms. J Sex Med (2007) 4:908–16. doi: 10.1111/j.1743-6109.2007.00519.x
19. Montorsi F, Guazzoni G, Strambi LF, Da Pozzo LF, Nava L, Barbieri L, et al. Recovery of spontaneous erectile function after nerve-sparing radical retropubic prostatectomy with and without early intracavernous injections of alprostadil: Results of a prospective, randomised trial. J Urol (1997) 158:1408–10. doi: 10.1016/S0022-5347(01)64227-7
20. McCullough AR, Hellstrom WG, Wang R, Lepor H, Wagner KR, Engel JD. Recovery of erectile function after nerve sparing radical prostatectomy and penile rehabilitation with nightly intraurethral alprostadil versus sildenafil citrate. J Urol (2010) 183:2451–6. doi: 10.1016/j.juro.2010.01.062
21. Saleh A, Abboudi H, Ghazal-Aswad Mb, Mayer Ek, Vale JA. Management of erectile dysfunction post-radical prostatectomy. Res Rep Urol (2015) 7:19–33. doi: 10.2147/RRU.S58974
22. Marchioni M, De Francesco P, Castellucci R, Papalia R, Sarikaya S, Gomez Rivas J, et al. Management of erectile dysfunction following robot-assisted radical prostatectomy: a systematic review. Minerva (2020) 72(5):543–54. doi: 10.23736/S0393-2249.20.03780-7
23. Pillay B, Moon D, Love C, Meyer D, Ferguson E, Crowe H, et al. Quality of life, psychological functioning, and treatment satisfaction of men who have undergone penile pros- thesis surgery following robot-assisted radical prostatectomy. J Sex Med (2017) 14:1612–20. doi: 10.1016/j.jsxm.2017.10.001
24. Ortac M, Özmez A, Can Cilesiz N, Demirelli E, Kadioglu A. The impact of extracorporeal shock wave therapy for the treatment of young patients with vasculogenic mild erectile dysfunction: A prospective randomised single-blind, sham controlled study. Andrology (2021) 9(5):1571–8. doi: 10.1111/andr.13007
25. Dong L, Chang D, Zhang X, Li J, Yang F, Tan K. Effect of low intensity extracorporeal shock wave on the treatment of erectile dysfunction: A systematic review and meta-analysis. Am J Mens Health (2019) 13(2):1–14. doi: 10.1177/1557988319846749
26. Juul Ladegaard PB, Mortensen J, Skov-Jeppesen SM, Lund L. Erectile dysfunction a prospective randomized placebo-controlled study evaluating the effect of low-intensity extracorporeal shockwave therapy (LI-ESWT) in men with erectile dysfunction following radical prostatectomy. Sex Med (2021) 9(3):100338. doi: 10.1016/j.esxm.2021.100338
27. Holmberg L, Bill-Axelson A, Helgesen F, Salo JO, Folmerz P, Häggmann M. A randomised trial comparing radical prostatectomy with watchful waiting in early prostate cancer. N Engl J Med (2002) 347(11):781–9. doi: 10.1056/NEJMoa012794
28. Capogrosso P, Vertosick EA, Benfante NE, Eastham JA, Scardino PJ, Vickers AJ, et al. Are we improving erectile function recovery after radical prostatectomy? analysis of patients treated over the last decade. Eur Urol (2019) 75(2):221–8. doi: 10.1016/j.eururo.2018.08.039
29. Liu MC, Chang ML, Wang YC, Chen WH, Wu CC, Yeh SD. Revisiting the regenerative therapeutic advances towards erectile dysfunction. Cells (2020) 9(5):1250. doi: 10.3390/cells9051250
30. Adamowick J, Kluth LA, Pokrywczynska M, Drewa T. Tissue engineering and its potential to reduce prostate cancer treatment sequelae-narrative review. Front Surg (2021) 8:644057. doi: 10.3389/fsurg.2021.644057
31. Haahr MK, Jensen CH, Toyserkani NM, Andersen DC, Damkier P, Sorensen JA, et al. Safety and potential effect of a single intracavernous injection of autologous adipose-derived regenerative cells in patients with erectile dysfunction following radical prostatectomy: An open-label phase I clinical trial. EBioMedicine (2016) 5:204–10. doi: 10.1016/j.ebiom.2016.01.024
32. Haahr MK, Harken Jensen C, Toyserkani NM, Andersen DC, Damkier P, Sorensen JA, et al. A 12-month follow-up after a single intracavernous injection of autologous adipose-derived regenerative cells in patients with erectile dysfunction following radical prostatectomy: an open-label phase I clinical trial. Urology (2018) 121:203.e6–13. doi: 10.1016/j.urology.2018.06.018
33. Yiou R, Hamidou L, Birebent B, Bitari D, Lecorvoisier P, Contremoulins I, et al. Safety of intracavernous bone marrowmononuclear cells for postradical prostatectomy erectile dysfunction: An open dose-escalation pilot study. Eur Urol (2016) 69:988–91. doi: 10.1016/j.eururo.2015.09.026
34. Yiou R, Hamidou L, Birebent B, Bitari D, Le Corvoisier P, Contremoulins I, et al. Intracavernous injections of bone marrow mononucleated cells for postradical prostatectomy erectile dysfunction: Final results of the INSTIN clinical trial. Eur Urol Focus (2017) 3:643–5. doi: 10.1016/j.euf.2017.06.009
35. Madl CM, Heilshorn SC, Blau HM. Bioengineering strategies to accelerate stem cell therapeutics. Nature (2018) 557:335–42. doi: 10.1038/s41586-018-0089-z
36. Fernández-García L, Perez-Rigueiro J, Martinez-Murillo R, Panetsos F, Ramos M, Guinea GV, Gonzalez Nieto D, et al. Cortical reshaping and functional recovery induced by silk fibroin hydrogels-encapsulated stem cells implanted in stroke animals. Front Cell Neurosci (2018) 12. doi: 10.3389/fncel.2018.00296
37. Shulteiss D. Regenerative medicine in andrology: Tissue engineering and gene therapy as potential treatment options for penile deformations and erectile dysfunction. Eur Urol (2004) 46:162–9. doi: 10.1016/j.eururo.2004.02.001
38. Nokoorani YD, Shamloo A, Bahadoran M, Moravvej H. Fabrication and characterization of scaffolds containing different amounts of allantoin for skin tissue engineering. Sci Rep (2021) 11(1):16164. doi: 10.1038/s41598-021-95763-4
39. Roohani-Esfahani S-I, Newman P, Zreiqat H. Design and fabrication of 3D printed scaffolds with a mechanical strength comparable to cortical bone to repair Large bone defects. Sci Rep (2016) 6(1):19468. doi: 10.1038/srep19468
40. Derakhshanfar S, Mbeleck R, Xu K, Zhang X, Zhong W, Xing M. 3D bioprinting for biomedical devices and tissue engineering: A review of recent trends and advances. Bioactive Materials (2018) 3:144–56. doi: 10.1016/j.bioactmat.2017.11.008
41. Schmidt CE, Leach JB. Neural tissue engineering: Strategies for repair and regeneration. Annu Rev Biomed Eng (2003) 5:293–347. doi: 10.1146/annurev.bioeng.5.011303.120731
42. Huang YC, Huang YY. Biomaterials and strategies for nerve regeneration. Artif Organs (2006) 30(7):514–22. doi: 10.1111/j.1525-1594.2006.00253.x
43. Anand S, Desai V, Alsmadi N, Kanneganti A, Huyen-Tram Nguyen D, Tran M, et al. Asymmetric sensory-motor regeneration of transected peripheral nerves using molecular guidance cues. Sci Rep (2017) 7:14323. doi: 10.1038/s41598-017-14331-x
44. Guedan-Duran A, Jemni-Damer N, Orueta-Zenarruzabeitia I, Guinea GV, Perez-Rigueiro J, Gonzalez-Nieto D, et al. Biomimetic approaches for separated regeneration of sensory and motor fibers in amputee people: Necessary conditions for functional integration of sensory-motor prostheses with the peripheral nerves. Front Bioeng Biotechnol (2020) 8:584823. doi: 10.3389/fbioe.2020.584823
45. Aijie C, Xuan L, Huimin L, Yanli Z, yiyuan K, Yuqing L, et al. Nanoscaffolds in promoting regeneration of the peripheral nervous system. Nanomedicine (2018) 13(9):1067–85. doi: 10.2217/nnm-2017-0389
46. Patel VR, Samavedi S, Bates AS, Kumar A, Coelho R, Rocco B. Dehydrated human amnion/chorion membrane allograft nerve wrap around the prostatic neurovascular bundle accelerates early return to continence and potency following robot-assisted radical prostatectomy: propensity score-matched analysis. Eur Urol (2015) 67:977–80. doi: 10.1016/j.eururo.2015.01.012
47. Ogaya Pinnies G, Palayapalam Ganapathi H, Rogers T, Hernandez Cardona E, Rocco B, Coelho RF, et al. Can dehydrated human amnion/chorion membrane accelerate the return to potency after a nerve-sparing robotic-assisted radical prostatectomy? propensity score-matched analysis. J Robotic Surg (2018) 12:235–43. doi: 10.1007/s11701-017-0719-8
48. Noël J, Mascarenhas A, Patel E, Reddy S, Sandri M, Bhat S, et al. Nerve spare robot assisted laparoscopic prostatectomy with amniotic membranes: medium term outcomes. J Robot Surg (2022), 16(5):1219–1224. doi: 10.1007/s11701-022-01370-4
49. Moris L, Gandaglia G, Vilaseca A, Van den Broeck T, Briers E, De Santis M. Evaluation of oncological outcomes and data quality in studies assessing nerve-sparing versus non-nerve-sparing radical prostatectomy in nonmetastatic prostate cancer: A systematic review. Eur Urol Focus (2021) 16:2405–4569. doi: 10.1016/j.euf.2021.05.009
50. Razdan S, Bajpai RR, Sanchez MA. A matched and controlled longitudinal cohort study of dehydrated human amniotic membrane allograft sheet used as a wraparound nerve bundles in robotic-assisted laparoscopic radical prostatectomy: a puissant adjunct for enhanced potency outcomes. J Robot Surg (2019) 13(3):475–81. doi: 10.1007/s11701-018-0873-7
51. Barski D, Gerullis H, Ecke T, Boros M, Brune J, Beutner U, et al. Application of dried human amnion graft to improve post-prostatectomy incontinence and potency: A randomised exploration study protocol. Adv Ther (2020) 37:592–602. doi: 10.1007/s12325-019-01158-3
52. Haastert-Talini K, Geuna S, Dahlin LB, Meyer C, Stenberg L, Freier T, et al. Chitosan tubes of varying degrees of acetylation for bridging peripheral nerve defects. Biomaterials (2013) 34:9886–904. doi: 10.1016/j.biomaterials.2013.08.074
53. Porpiglia F, Bertolo R, Fiori C, Manfredi M, De Cillis S, Geuna S. Chitosan membranes applied on the prostatic neurovascular bundles after nerve-sparing robot-assisted radical prostatectomy: A phase II study. BJU Int (2017) 121:472–8. doi: 10.1111/bju.13959
54. Porpiglia F, Manfredi M, Checcucci E, Garrou D, De Cillis S, Amparore D. Use of chitosan membranes after nerve-sparing radical prostatectomy improves early recovery of sexual potency: Results of a comparative study. BJU Int (2019) 123:465–73. doi: 10.1111/bju.14583
55. Yonesi M, Garcia Nieto M, Guinea GV, Panetsos F, Perez Rigueiro J, Gonzalez Nieto D. Silk fibroin: An ancient material for repairing the injured nervous system. Pharmaceutics (2021) 13(3):429. doi: 10.3390/pharmaceutics13030429
56. Gu X, Parth U, Thakker U, Matz Terlecki E RP, Marini FC, et al. Dynamic changes in erectile function and histological architecture after intracorporal injection of human placental stem cells in a pelvic neurovascular injury rat model. J Sex Med (2020) 17(3):400–11. doi: 10.1016/j.jsxm.2019.12.002
57. Ghatak K, Yin GN, Choi MJ, Limanjaya A, Minh NN, Ock J, et al. Dickkopf2 rescues erectile function by enhancing penile neurovascular regeneration in a mouse model of cavernous nerve injury. Sci Rep (2017) 7(1):17819. doi: 10.1038/s41598-017-17862-5
58. Yin GN, Park SH, Ock J, Limanjaya A, Ghatak A, Song KM, et al. Pericyte-derived extracellular vesicle-mimetic nanovesicles restore erectile function by enhancing neurovascular regeneration in a mouse model of cavernous nerve injury. J Sex Med (2020) 17(11):2118–28. doi: 10.1016/j.jsxm.2020.07.083
59. Weyne E, Hannan JL, Gevaert T, Soebadi MA, Matsui H, Castiglione F, et al. Galanin administration partially restores erectile function after cavernous nerve injury and mediates endogenous nitrergic nerve outgrowth in vitro. J Sex Med (2018) 15(4):480–91. doi: 10.1016/j.jsxm.2018.02.013
60. Seo YE, Kim SD, Kim TH, Sung GT. The efficacy and safety of tadalafil 5 mg once daily in the treatment of erectile dysfunction after robot-assisted laparoscopic radical pros- tatectomy: 1-year follow-up. Korean J Urol (2014) 55:112–9. doi: 10.4111/kju.2014.55.2.112
61. Kim S, Sung GT. Efficacy and Safety of Tadalafil 5 mg Once Daily for the Treatment of Erectile Dysfunction After Robot-Assisted Laparoscopic Radical Prostatectomy: A 2-Year Follow-Up. Sex Med. (2018) 6(2):108–114. doi: 10.1016/j.esxm.2017.12.005
62. Basal S, Wambi C, Acikel C, Gupta M, Badani K. Opti- mal strategy for penile rehabilitation after robot-assisted radical prostatectomy based on preoperative erectile function. BJU Int (2013) 111:658–65. doi: 10.1111/j.1464-410X.2012.11487.x
Keywords: erectile dysfunction, sexual potency, radical prostatectomy, neurovascular regeneration, tissue engineering, stem cell therapy
Citation: Rivero Belenchón I, Gómez Rivas J, Medina López RA, Checcucci E, Taratkin M, Puliatti S, Kowalewski K-F, Cacciamani G, Congregado Ruíz CB, Castro C, Enikeev D, Abad-Lopez P, Panetsos F and Moreno-Sierra J (2022) New therapies for neurovascular bundles regeneration after radical prostatectomy: A narrative review on clinical studies. Front. Urol. 2:923064. doi: 10.3389/fruro.2022.923064
Received: 18 April 2022; Accepted: 23 September 2022;
Published: 10 October 2022.
Edited by:
Gian Maria Busetto, University of Foggia, ItalyReviewed by:
Marco Capece, University of Naples Federico II, ItalyMichele Marchioni, University of Studies G. d’Annunzio Chieti and Pescara, Italy
Copyright © 2022 Rivero Belenchón, Gómez Rivas, Medina López, Checcucci, Taratkin, Puliatti, Kowalewski, Cacciamani, Congregado Ruíz, Castro, Enikeev, Abad-Lopez, Panetsos and Moreno-Sierra. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Inés Rivero Belenchón, ines.rivero.belenchon@gmail.com
†These authors share first authorship