 Pablo F. Belaunzarán-Zamudio1,2*
Pablo F. Belaunzarán-Zamudio1,2* Ana M. Ortega-Villa3
Ana M. Ortega-Villa3 Alberto J. Mimenza-Alvarado4,5
Alberto J. Mimenza-Alvarado4,5 Paola Del Carmen Guerra-De-Blas6
Paola Del Carmen Guerra-De-Blas6 Sara G. Aguilar-Navarro4
Sara G. Aguilar-Navarro4 Jesús Sepúlveda-Delgado7Sally Hunsberger3
Jesús Sepúlveda-Delgado7Sally Hunsberger3 Raydel Valdés Salgado8
Raydel Valdés Salgado8 José Ramos-Castañeda1,9
José Ramos-Castañeda1,9 Héctor Armando Rincón León10
Héctor Armando Rincón León10 Paul Rodríguez de La Rosa11José Gabriel Nájera Cancino7John Beigel2Sandra Caballero Sosa12Emilia Ruiz Hernández13
Paul Rodríguez de La Rosa11José Gabriel Nájera Cancino7John Beigel2Sandra Caballero Sosa12Emilia Ruiz Hernández13 John H. Powers III14
John H. Powers III14 Guillermo M. Ruiz-Palacios1
Guillermo M. Ruiz-Palacios1 Clifford Lane2 on behalf of the Mexican Emerging Infectious Diseases Clinical Research Network (LaRed)6
Clifford Lane2 on behalf of the Mexican Emerging Infectious Diseases Clinical Research Network (LaRed)6- 1Departamento de Infectología, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
- 2National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD, United States
- 3Biostatistics Research Branch, Division of Clinical Research, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD, United States
- 4Department of Geriatric Medicine, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
- 5Geriatrics & Neurology Fellowship, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
- 6The Mexican Emerging Infectious Diseases Clinical Research Network (LaRed), Mexico City, Mexico
- 7Directorate of Research, Hospital Regional de Alta Especialidad Ciudad Salud, Tapachula & Medical Science Research, Hospital General de Zona 1, Instituto Mexicano del Seguro Social, Mexico City, Mexico
- 8Westat, Rockville, MD, United States
- 9Departamento de Inmunidad, Instituto Nacional de Salud Pública, Cuernavaca, Mexico
- 10Instituto Mexicano del Seguro Social, Delegación Estatal, Tapachula, Mexico
- 11Directorate of Neurology, Hospital Regional de Alta Especialidad Ciudad Salud, Tapachula, Mexico
- 12Clínica Hospital Dr. Roberto Nettel Flores, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado, Tapachula, Mexico
- 13Departamento de Urgencias, Hospital General de Tapachula, Tapachula, Mexico
- 14Clinical Research Directorate, Frederick National Laboratory for Cancer Research, Frederick, MD, United States
Zika has been associated with a variety of severe neurologic manifestations including meningitis and encephalitis. We hypothesized that it may also cause mild to subclinical neurocognitive alterations during acute infection or over the long term. In this observational cohort study, we explored whether Zika cause subclinical or mild neurocognitive alterations, estimate its frequency and duration, and compare it to other acute illnesses in a cohort of people with suspected Zika infection, in the region of Tapachula in Chiapas, Mexico during 2016–2018. We enrolled patients who were at least 12 years old with suspected Zika virus infection and followed them up for 6 months. During each visit participants underwent a complete clinical exam, including a screening test for neurocognitive dysfunction (Montreal Cognitive Assessment score). We enrolled 406 patients [37 with Zika, 73 with dengue and 296 with other acute illnesses of unidentified origin (AIUO)]. We observed a mild and transient impact over cognitive functions in patients with Zika, dengue and with other AIUO. The probability of having an abnormal MoCA score (<26 points) was significantly higher in patients with Zika and AIUO than in those with dengue. Patients with Zika and AIUO had lower memory scores than patients with dengue (Zika vs. Dengue: −0.378, 95% CI−0.678 to −0.078; p = 0.014: Zika vs. AIUO 0.264, 95% CI 0.059, 0.469; p = 0.012). The low memory performance in patients with Zika and AIUO accounts for most of the differences in the overall MoCA score when compared with patients with dengue. Our results show a decrease in cognitive function during acute illness and provides no evidence to support the hypothesis that Zika might cause neurocognitive alterations longer than the period of acute infection or different to other infectious diseases. While effects on memory or perhaps other cognitive functions over the long term are possible, larger studies using more refined tools for neurocognitive functioning assessment are needed to identify these.
Trial Registration: NCT02831699.
Introduction
Zika virus (ZIKV) infection has been associated with severe neurological disease in adults (1). The most frequently identified neurological manifestation is Guillain-Barre syndrome (GBS), which has been estimated to occur in 0.31 to 9.35 per 100,000 people during Zika outbreaks in Latin America and the Caribbean (2). Zika-associated GBS appears to have unique pathophysiological and clinical characteristics, such as the predominance of axonal demyelinating disease and a higher frequency of atypical varieties such as Miller-Fisher syndrome and descending paralysis patterns (3, 4). Along with GBS, ZIKV infection has been associated with other central and peripheral nervous system disorders including meningitis, encephalitis, meningoencephalitis, traverse myelitis, radiculitis, chronic inflammatory demyelinating polyneuropathy, and acute demyelinating encephalomyelitis, optical neuritis, acute hearing loss and other cranial, and peripheral nerve neuropathies (3, 5). ZIKV infect dorsal root ganglion neurons, gastrointestinal tract neurons, and CNS neural progenitors; induce apoptosis and downregulates nucleosome-associated genes, thus decreases cell viability, and enables viral replication (6), which explains neural tube defects, most notably microcephaly, in children of women infected during the first trimester of pregnancy (7).
Although experimental models and human studies have shown that ZIKV has an exquisite affinity for human neural progenitor cells that might explain pre-natal neural damage (8), the mechanisms that induce neuronal damage and explains other neurological manifestations in adults are not clearly understood. Further, severe manifestations in adults and infants have received considerable attention given its conspicuousness and ramifications but it is reasonable to hypothesize that ZIKV infection may cause subclinical or mild disease, which might include neurocognitive impairment during acute infection or over the long term (9–11). In this study, we aimed to explore whether ZIKV infection may cause subclinical or mild neurocognitive alterations, estimate its frequency and duration, and to compare it to other acute illnesses in a cohort of people with suspected Zika infection in Mexico.
Methods
Study Design, Study Population and Settings
We analyzed data from the ZIk01 study (https://www.redmexei.mx/) which was a prospective, observational cohort that enrolled patients with probable ZIKV infection and followed them up for 6 months. The study procedures has been described previously (12, 13). Briefly, participants were assessed at enrollment and 3, 7, 28, and 180 days later. During each visit participants underwent a complete clinical exam, including a screening test for neurocognitive dysfunction, a disability assessment, and complete blood count and clinical chemistry. Blood and urine samples for viral nucleic acid identification were also drawn. Participants had their first sample within 7 days after symptoms onset as recommended by the CDC guidance for Zika (14).
Patients were accrued in four clinical care centers in the city of Tapachula in the State of Chiapas, in Southern Mexico from June 2016 to July 2018. We decided to enroll up to 600 participants across three different cohorts (symptomatic people seeking care for symptoms compatible with Zika, patients with Guillain-Barre Syndrome, and asymptomatic household contacts of symptomatic participants) based on convenience and feasibility given the uncertainty of the number of people that would be infected when we planned the study. The protocol specified that separate analyses would be performed for each cohort. This paper analyses data from the cohort of symptomatic participants. In this analysis, we included patients who were at least 12 years old with any two of the following symptoms with onset in the previous 7 days: rash, elevated body temperature (>37.2°C), arthralgia, myalgia, non-purulent conjunctivitis, conjunctival hyperemia, headache, or malaise; not explained by other medical diagnosis, based on a modified version of the Pan American Health Organization case definition (15).
Study Definitions and Procedures
We classified participants as having confirmed ZIKV, or dengue virus infection if viral RNA was detected in serum or urine samples at enrollment or anytime at 3, 7, or 28 days later. Real-time RT-PCR assays for ZIKV (16), dengue (17), chikungunya (18), and panflavivirus (19) were performed in blood and urine samples from baseline visits and 3,7, and 28 days later. We extracted total nucleic acids from 500 μl of serum and urine using the NucliSENS® easyMAG® system (bioMerieux®, Netherlands) and eluted in 55 μl, according to manufacturer instructions. The amplification of the human RNaseP (RP) gene was carried out for each sample as an internal control to demonstrate the presence of RNA and the validation of the extraction process. The amplification of the NS5 gene was also carried out for the generic detection of Flavivirus as another control of ZIKV and Dengue, and to determine the possible presence of other flaviviruses in the sample. Amplifications were performed in singleplex (each virus detected in a separate reaction) by one-step RT-PCR reaction in 25 μl with SuperScript III Platinum One-Step quantitative RT-PCR System (Invitrogen®, ThermoFisher Scientific®, Waltham, MA, USA) and 5 μl of sample. Cycle sequencing was: retrotranscription at 50°C for 30 min, initial PCR denaturation at 94°C for 2 min followed by 45 cycles of denaturation at 94°C for 15 s and annealing and extension at 60°C for 1 min in the Applied Biosystems 7,500 Fast Real Time PCR System (Applied Biosystems, ThermoFisher Scientific®, Waltham, MA, USA).
Patients with no detectable viral RNA were classified as having an acute illness of unidentified origin (AIUO). We excluded from the analysis 39 participants who had missing data on at least two follow up visits and did not have detectable viral RNA in the available urine or blood samples. We also excluded one participant with confirmed chikungunya virus infection.
We used the Montreal Cognitive Assessment (MoCA) screening tool to assess neurocognitive functions. The MoCA is a one-page test that can be administered in 10 min. The test assesses five domains: (1) memory, (2) visuospatial abilities and executive functions, (3) attention, (4) language, and (5) orientation in time and space (20). Each domain is scored and added for a total score ranging from 0 to 30 points. The Spanish version of the test has been validated in Mexico (21) and showed a sensitivity of 80% and specificity of 75% [Area under the Curve 0,886 (IC95%, 0,826-0,947)] for mild cognitive impairment using a cutoff of <26 points for abnormal performance (21). For the secondary analysis, we explored each domain separately. The MoCA test was originally developed as a brief tool for primary care physicians to identify elderly patients which might suffer cognitive impairment but perform within the normal range of dementia screening tools (20). Still, it has been used in research settings as a screening tool in younger adults with sleep disorders (22), heart failure (23), Parkinson's Disease (24), Vascular Cognitive Impairment (25), and Systemic Lupus Erythematosus (26). Moreover, since the MoCA tests evaluates different domains in cognitive functions, it has also been used to assess specific areas of dysfunction. In recent studies, it has been observed that a neuroanatomical correlation between MoCA scores sub-specific domains and cortical volumes, particularly in hippocampal area (27).
We assessed disability using the World Health Organization Disability Assessment Schedule 2.0 (WHODAS 2). The WHODAS 2 is an instrument designed to provide a cross-cultural standardized method for measuring activity limitations and participation restrictions irrespective of the individual's medical diagnosis (28).
Ethical Considerations
Study protocol was evaluated and approved by the Institutional Review Board in all Mexican participating institutions. Participation was voluntary and documented through a written informed consent procedure. Participants younger than 18 years were requested their assent and parents or legal tutors authorized their participation. This study was carried out in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Statistical Analysis
We modeled the longitudinal behavior of education-adjusted MoCA scores across study visits, and compared these results between disease groups (Zika, dengue, and AIUO), using a regression model and generalized estimable equations (GEE) to account for intrasubject correlation using the geepack package (29) in R (30). We modeled the MoCA score as function of the indicators for disease group, study visits, education status, sex and age; allowing for interactions between visit and disease group, and then dropped non-significant interactions from the final model. We used contrasts to determine whether there were differences in MoCA scores at each study visit across disease groups. In a secondary analysis, the MoCA score was dichotomized into normal or abnormal (≤ 26 points), and fitted a similar model using logistic regression with GEE. We used the same approach of the continuous MoCA to test time and group difference for five MoCA domain scores that make up the total MoCA score. The longitudinal model assumes data is missing at random. We performed analyses to assess missingness, and a sensitivity analysis using the last rank carried forward (LRCF) method (31), to determine the potential impact of missing data in our final results.
Results
Characteristics of the Study Population
We analyzed information from 406 patients of which 73 had confirmed dengue, 37 Zika, and 296 had an acute illnesses of unidentified origin (AIUO). The demographic characteristics of these patients are summarized in Table 1. Overall, patients with dengue were younger and predominantly placed in the lower educations groups (70% with twelve years of school or lower). A brief description of the main clinical characteristics is shown in Table 2. Overall, patients with dengue virus infection and AIUO more frequently presented fever, arthralgia, headache, malaise, behavior alterations, and disability at baseline than patients with ZIKV; while rash was more frequent in ZIKV and dengue virus infection patients compared with those with AIUO.
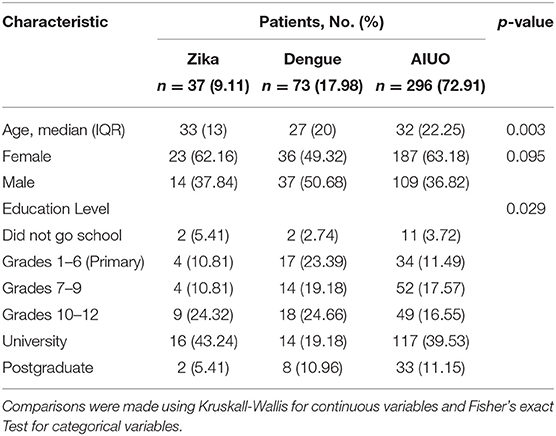
Table 1. Demographic characteristics of participants at baseline visit by disease group (N = 406).
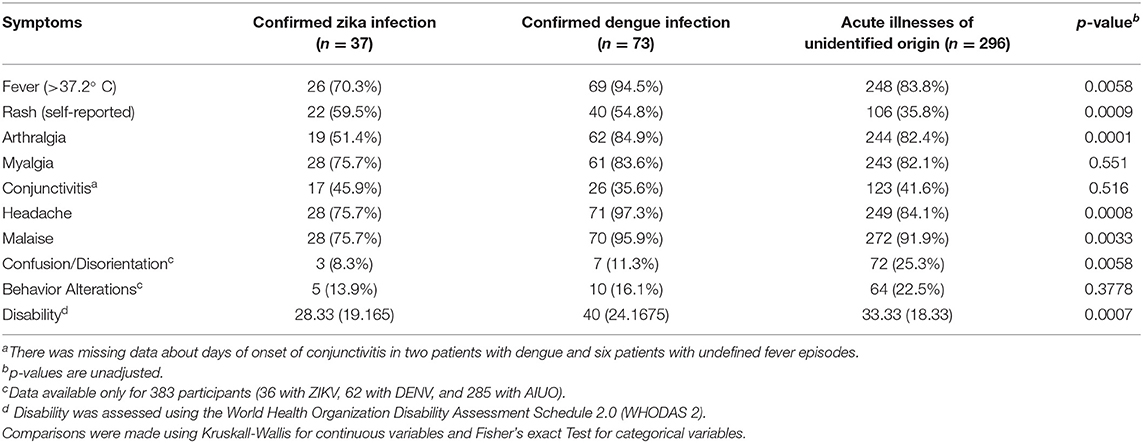
Table 2. Distribution and characteristics of baseline, self-reported signs, and symptoms of patients 12 years and older seeking care within 7 days of onset due to acute episodes of fever and/or rash (N = 406).
MoCA Score
When analyzing the MoCA score as a continuous endpoint we observed that all disease groups (Zika, dengue and AIUO) followed similar trajectories. While patients with dengue tended to have higher mean MoCA scores than patients with Zika and AIUO, these differences were not statistically significant neither in general nor at any timepoint (see Figure 1). This slightly higher MoCA score in patients with dengue could be attributed to better performance in the Memory subdomain for this group (see below). Overall, there were no significant changes in the mean MoCA score from baseline to visit at day 7 (−0.06, 95% CI: −0.35, 0.22 p = 0.68). There was a significant improvement in the mean MoCA scores between day 7 and 28 (1.10 0.83 1.36, p < 0.001), but no further improvement was observed between day 28 and 180 (0.01 −0.31 0.32, p = 0.96). Patients with AIUO as a group, but not those with Zika or dengue, had a non-statistically significant increase in the mean MoCA scores from day 28 to day 180, as illustrated in Figure 1. These findings are consistent with the analysis of the MoCA scores used as a binary variable, where we estimated the probabilities of having an abnormal MoCA score (score <26) during follow up. In all groups, the probability of an abnormal MoCA score decreased at days 28 and 180 in comparison to measurements at baseline and day 7 (see Supplementary Table 1). Also, both the Zika and AIUO groups had increased odds of an abnormal MoCA scores in comparison with the dengue group (see Table 3).
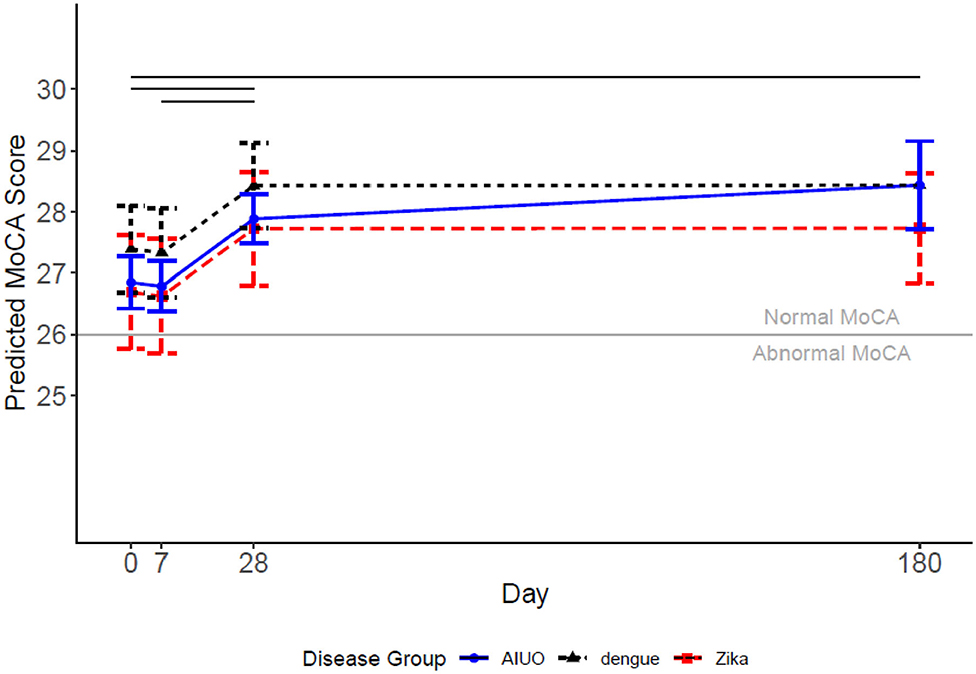
Figure 1. Predicted MoCA scores for each disease group and 95% confidence intervals. Covariates set to 33-year-old female with university education for each disease group. Levels of the adjustment variables were selected to be the most common when categorical and average when continuous. The solid horizonal lines represent significant changes in the level of the score for time comparisons.
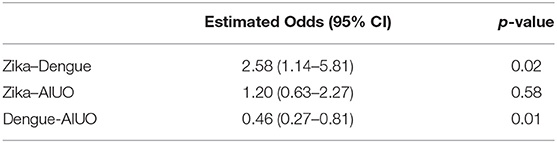
Table 3. Comparisons of the probabilities of having and abnormal MoCA Score and p-values for the group comparisons using the binary MoCA score (abnormal < = 26 points).
MoCA Subdomains
When we analyzed and compared separately the MoCA test subdomains, we observed no overall differences in orientation, attention, language, and visuospatial and executive functions across disease groups (Figure 2). During follow-up, the orientation subdomain score did not change across time (Figure 2A). The Visuospatial and Executive domain score increased at each follow up time point up to day 28: baseline to day 7 [0.192, (0.073, 0.310), p = 0.001], day 7 to day 28 [0.261, (0.116, 0.360), p < 0.001], and slightly decreased afterwards: day 28 to 180 [0.277, (0.142, 0.411) p ≤ 0.001], but not to the level present at baseline [0.279, (0.136, 0.421, p < 0.001)] (Figure 2B). The attention subdomain score did not significantly change between baseline and day 7 [0.06, (−0.05, 0.18) P = 0.26], increased from day 7 to day 28 [0.145, (0.04, 0.250), p = 0.007], and remained stable from day 28 to day 180 [0.10 (−0.01, 0.22); P = 0.08] (Figure 2C). There was an earlier decrease in the language domain score (baseline to day 7 [−0.409, (−0.514, −0.304), p < 0.001]) and subsequent recuperation from day 7 to 28 [0.460, (0.355, 0.565), p < 0.001], and plateaued from day 28 to 180 [0.037, (−0.079, 0.153), p = 0.533] ending at a similar mean score at the end of follow-up than at enrollment (Figure 2D). In contrast, patients with Zika had a lower memory score than patients with dengue (−0.378, 95% CI = −0.678 to −0.078; p = 0.014); and patients with dengue had a higher memory score than patients with AIUO [0.264, (0.059, 0.469); p = 0.012] (Supplementary Table 2). We observed no differences between the Zika and AIUO groups [−0.114, (−0.369, 0.144); p = 0.383]. The difference in the memory subdomain accounted for most of the magnitude of the difference between dengue and Zika or AIUO in the overall MoCA score (Figure 3).
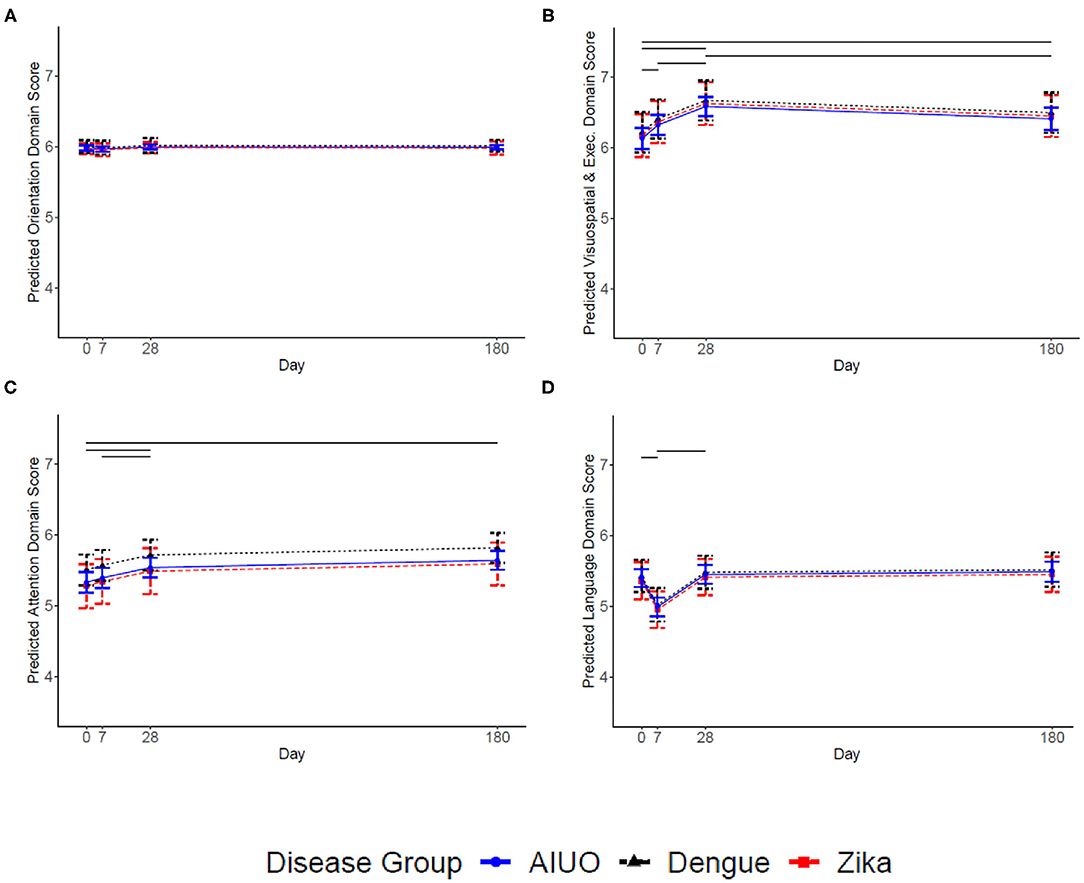
Figure 2. Predicted MoCA Domain scores for each disease group and 95% confidence intervals. Covariates set to 33 year-old female with university education for each disease group. The solid horizonal lines represent significant changes in the level of the domain score between time points. (A) Presents Orientation, (B) Visuospatial and Executive, (C) Attention, and (D) Language. The solid horizonal lines represent significant changes (p ≤ 0.05) in the score between time-points.
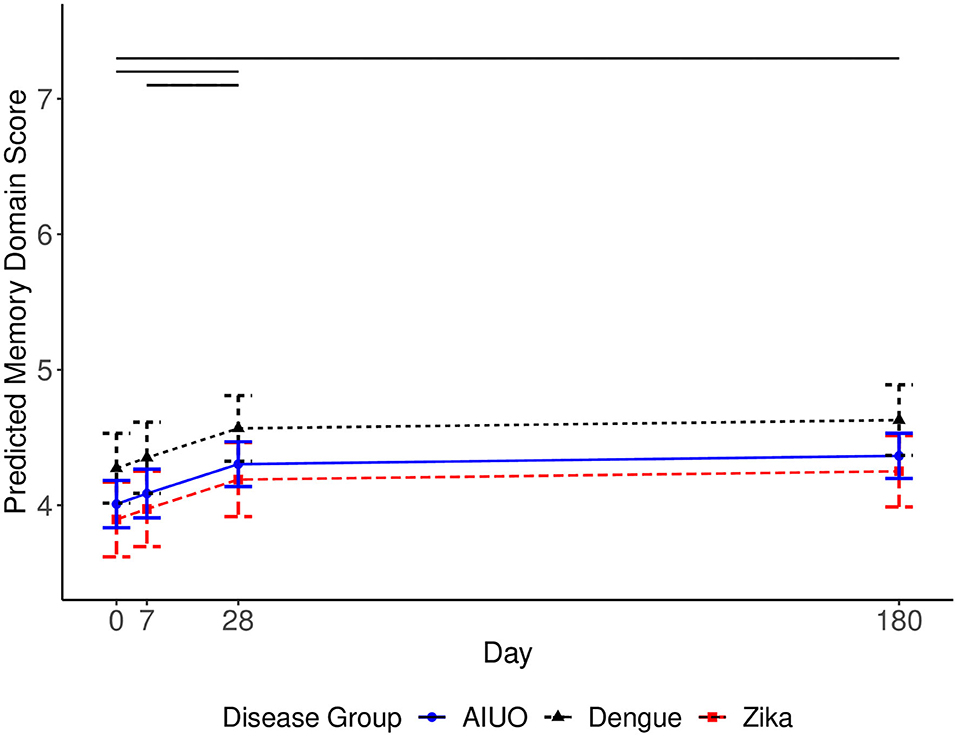
Figure 3. Predicted MoCA Memory Domain scores for each disease group and 95% confidence intervals. Covariates set to 33-year-old female with university education for each disease group. The solid horizonal lines represent significant changes in the level of the domain score between time points. The solid horizonal lines represent significant changes (p ≤ 0.05) in the score between time-points.
Finally, we observed low memory subdomain mean scores at baseline with no significant changes during the first 7 days. The memory subdomain score increased from day 7 to day 28 [0.217, (0.07, 0.364), p = 0.004], and maintained from day 28 to day 180 (Figure 3).
We analyzed missing data patterns among disease groups, which is described in detail in Supplementary Figure 1. Although there is significantly more missing data in the AIUO and dengue groups, there does not appear to be a systematic missingness pattern with respect to baseline MoCA score and disease group. So, it is reasonable to accept the assumption that this information is missing at random.
Discussion
In this study we present a longitudinal assessment of neurocognitive function, using the MoCA score and its subdomains, of a group of patients with Zika and compared them with patients with dengue and acute illnesses of unidentified origin (AIUO) in the region of Tapachula in Chiapas, Mexico during 2016-2018. We documented a transient deficit in cognitive functions in adults infected with Zika, dengue or AIUO during the first days and up to 28 days after infection with recovery at 6 months of follow-up. While all groups experienced this pattern, patients with Zika and AIUO tended to have a lower overall MoCA score during acute infection and early after that than patients with dengue, although these differences did not reach statistical significance. The probability of having an abnormal MoCA score (<26 points) was significantly higher in patients with Zika and AIUO than in those with dengue. The low memory performance in patients with Zika and AIUO accounts for most of the differences in the overall MoCA score when compared with patients with dengue. The sixth month measurements were higher in patients with AIUO and dengue than in patients with Zika, after adjusting for sex, age and educational status, but again these differences were not statistically significant.
Flaviviruses can cause a wide variety of neurological manifestations (1) including alterations in sensitivity, cognitive impairment, seizures and personality disorders such as mania, depression, emotional lability, anxiety, psychosis and agoraphobia in dengue (32) and encephalitis, myelitis, confusion and paresthesia in patients with Zika (5). We observed transient alterations in attention, visuospatial and memory functions as assessed by the MoCA test in all groups of patients, suggesting a possible common mechanism of neural damage instead of specific to each disease. Considering the known mechanisms of neural damage by flaviviruses, our findings could be explained by direct viral replication in brain tissue with subsequent neuronal destruction, immune complex formation or both (32, 33). It also has been demonstrated that neural damage may result from the preexistence of cross-reactive antibodies against flavivirus during ZIKV infection (34–36). Interestingly, patients with Zika and AIUO had a lower memory score than patients with dengue during acute infection and this difference persisted over the 6 months of observation. Animal models showing Zika virus infection and viral replication in the frontal cortex and hippocampus associated with synapse damage leading to memory alterations (37), as well as the presence of ZIKV in CSF in patients with overt encephalopathy (38) are consistent with direct damage by ZIKV to adult neurons (39).
Our study has several drawbacks which might limit the validity of our results. First, it comprises a relatively small group of people with Zika and dengue with most participants in the AIUO group. The latter might include an heterogenous group of infections, which limits our ability to have a comparison group clearly differentiated from Zika, dengue and other flaviviruses. We reasonably excluded the possibility of a potential confounding effect of differentiated patterns of missing data due to loss of follow-up associated with cognitive dysfunction or disease group, and adjusted for the potential confounding effects of sex, age and educational status in our model.
While the MoCA screening test is a convenient, widely used, validated instrument to assess cognitive functions, it was developed to identify mild cognitive impairment in elderly patients performing within the normal range of dementia screening tools. Thus, it might still be poorly sensitive to milder or subclinical cognitive dysfunction in younger people, for whom tools to properly assess cognitive functioning might have been needed. The advantage of the MoCA score is that despite its limitations, its widespread use in research settings facilitates comparisons across studies. Finally, the lack of cerebral neuroimaging studies and cerebrospinal fluid testing, make it difficult to propose a mechanism for the observed changes in memory, visuospatial and attention cognitive domains in all groups. Even so, our study is one of the first to explore the impact of Zika on cognitive functions. Our results show a decrease in cognitive function during acute illness, it would be interesting to follow up on this finding with a larger sample size and more refined tools to identify cognitive impairment.
In conclusion, while Zika is a neurotropic virus that can produce a constellation of severe neurological manifestations, few studies have explored its short- and long-term impact in cognitive function in adult humans. We observed a transient impact on cognitive functions in patients with Zika, dengue and with other undefined acute illnesses, particularly in memory, visuospatial and attention domains. Patients with Zika tended to have lower MoCA scores at 6 months of follow-up than patients with AIUO and dengue but this finding has uncertain clinical significance. Our study provides no clinical evidence to support the hypothesis that Zika or dengue might cause neurocognitive alterations persisting longer than the period of acute infection. While effects on memory or perhaps other cognitive functions over the long term are possible, larger studies using more refined tools for neurocognitive functioning assessment are needed to identify these.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité de Ética en Investigación (Comittee on Ethics in Research) and the Comité de Investigación (Research Comittee) at the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INF-2636-18-19-1. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
PB-Z performed the literature search, was part of the study design team, collected data, wrote sections of the paper, and contributed to data analysis an interpretation. AO-V produced the figures, performed the data analysis and interpretation, and edited the paper. AM-A participated in data analysis and interpretation, wrote sections of the paper and edition. PG-D-B performed the literature search, contributed to data interpretation and the writing and editing of the manuscript. SA-N provided contributed to data analysis and interpretation, wrote sections of the paper and edition. JS-D performed the literature search, wrote sections of the paper, and provided data interpretation. SH wrote sections of the paper, was part of the study design team, and performed the data analysis and interpretation. RV and JR-C participated in data interpretation and edited the paper. HR, JN, SC, and ER was part of the study design team and collected data. PR was part of the study design team and provided data interpretation. JB was part of the study design team and provided supervision. JP provided data interpretation and edited the paper. GR-P and CL was part of the design team, obtained funding and provided supervision. All co-authors critically reviewed the manuscript and approved the final version.
Funding
This work was supported by The Mexican Emerging Infectious Diseases Clinical Research Network (LaRed). LaRed is funded by the Mexico Ministry of Health and the U.S. National Institute of Allergy and Infectious Diseases. This study was supported in part by Consejo Nacional de Ciencia y Tecnología [FONSEC SSA/IMSS/ISSSTE Projects No. 71260 and No. 127088]; National Institute of Allergy and Infectious Diseases, National Institutes of Health, through its Intramural Research Programs and a contract with Westat, Inc., Contract Number: HHSN2722009000031, Task Order Number: HHSN27200002; and in part with federal funds from the National Cancer Institute, National Institutes of Health, under Contract No. HHSN261200800001E and Contract No. 75N91019D00024, Task Order No. 75N91019F00130. The content of this publication does not necessarily reflect the views or policies of the Department of Health and Human Services, or Westat, nor does mention of trade names, commercial products, or organizations imply endorsement by the US Government. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The members for the Mexico Emerging Infectious Diseases Clinical Research Network (LaRed) are Justino Regalado Pineda (LaRed Director), HR and Karla R Navarro-Fuentes (Unidad de Medicina Familiar No.11, Instituto Mexicano del Seguro Social, Tapachula, Chiapas, Mexico), SC, Francisco Camas-Durán and Zoyla Priego-Smith (Clínica Hospital Dr. Roberto Nettel Flores, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado, Tapachula, Chiapas, Mexico), Emilia Ruiz (Hospital General de Tapachula, Tapachula, Chiapas, Mexico), JN, PR, JS-D, Alfredo Vera Maloof, Karina Trujillo, Alexander López-Roblero (Hospital Regional de Alta Especialidad Ciudad Salud, Tapachula, Chiapas, Mexico), RS, Yolanda Bertucci, Isabel Trejos, Luis Diego Villalobos (Westat, Inc., Rockville, MD, USA), PB-Z, Pilar Ramos, Fernando J. Arteaga-Cabello, Lourdes Guerrero, GR-P (Departamento de Infectología, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico), Luis Mendoza-Garcés, Samira Toledo Roy, PG-D-B, Peter Quidgley, Edgar García Romero, Eli Becerril, Laura Macedo, Abelardo Montenegro Liendo (LaRed Coordinating Center, Mexico City), JP (Leidos Biomedical Research, Inc., Frederick National Laboratory for Cancer Research, Frederick, Maryland, USA), JB, SH (National Institute of Allergy and Infectious Diseases, Bethesda, MD, USA).
References
1. Azevedo MB, Coutinho MSC, Silva MAD, Arduini DB, Lima JDV, Monteiro R. Neurologic manifestations in emerging arboviral diseases in Rio de Janeiro City, Brazil, 2015-2016. Rev Soc Bras Med Trop. (2018) 51:347–51. doi: 10.1590/0037-8682-0327-2017
2. Capasso A, Ompad DC, Vieira DL, Wilder-Smith A, Tozan Y. Incidence of Guillain-Barré Syndrome (GBS) in Latin America and the Caribbean before and during the 2015-2016 Zika virus epidemic: a systematic review and meta-analysis. PLoS Negl Trop Dis. (2019) 13:e0007622. doi: 10.1371/journal.pntd.0007622
3. da Silva IRF, Frontera JA, Bispo de Filippis AM, Nascimento OJMD, RIO-GBS-ZIKV Research Group. Neurologic Complications Associated With the Zika Virus in Brazilian Adults. JAMA Neurol. (2017) 74:1190–8. doi: 10.1001/jamaneurol.2017.1703
4. Rivera-Correa J, de Siqueira IC, Mota S, do Rosário MS, Pereira de Jesus PA, Alcantara LCJ, et al. Anti-ganglioside antibodies in patients with Zika virus infection-associated Guillain-Barré Syndrome in Brazil. PLoS Negl Trop Dis. (2019) 13:e0007695. doi: 10.1371/journal.pntd.0007695
5. Mehta R, Soares CN, Medialdea-Carrera R, Ellul M, da Silva MTT, Rosala-Hallas A. The spectrum of neurological disease associated with Zika and chikungunya viruses in adults in Rio de Janeiro, Brazil: a case series. PLoS Negl Trop Dis. (2018) 12:e0006212. doi: 10.1371/journal.pntd.0006212
6. Khan TA, Paşca SP. The Zika threat to the periphery. Nat Neurosci. (2017) 20:1191–2. doi: 10.1038/nn.4633
7. Lebov JF, Brown LM, MacDonald PDM, Robertson K, Bowman NM, Hooper SR, et al. Review: evidence of neurological sequelae in children with acquired zika virus infection. Pediatr Neurol. (2018) 85:16–20. doi: 10.1016/j.pediatrneurol.2018.03.001
8. El Ghouzzi V, Bianchi FT, Molineris I, Mounce BC, Berto GE, Rak M, et al. ZIKA virus elicits P53 activation and genotoxic stress in human neural progenitors similar to mutations involved in severe forms of genetic microcephal. Cell Death Dis. (2016) 7:e2440. doi: 10.1038/cddis.2016.266
9. Chang AY, Lynch R, Martins K, Encinales L, Cadena Bonfanti AÁ, Pacheco N, et al. Long-term clinical outcomes of Zika-associated Guillain-Barré syndrome. Emerg Microbes Infect. (2018) 7:148. doi: 10.1038/s41426-018-0151-9
10. Lannuzel A, Fergé JL, Lobjois Q, Signate A, Rozé B, Tressières B, et al. Long-term outcome in neuroZika: When biological diagnosis matters. Neurology. (2019) 92:e2406–20. doi: 10.1212/WNL.0000000000007536
11. Souza INO, Barros-Aragão FGQ, Frost PS, Figueiredo CP, Clarke JR. Late neurological consequences of zika virus infection: risk factors and pharmaceutical approaches. Pharmaceuticals (Basel). (2019) 12:60. doi: 10.3390/ph12020060
12. Hunsberger S, Ortega-Villa AM, Powers JH 3rd, Rincón León HA, Caballero Sosa S, Ruiz Hernández E, et al. Patterns of signs, symptoms, and laboratory values associated with Zika, dengue, and undefined acute illnesses in a dengue endemic region: secondary analysis of a prospective cohort study in southern Mexico. Int J Infect Dis. (2020) 98:241–9. doi: 10.1016/j.ijid.2020.06.071
13. Belaunzarán-Zamudio PF, Mateja A, Guerra-de-Blas PDC, Rincón-León HA, Navarro-Fuentes K, Ruiz-Hernández E, et al. Comparison of clinical characteristics of Zika and dengue symptomatic infections and other acute illnesses of unidentified origin in Mexico. PLoS Negl Trop Dis. (2021) 15:e0009133. doi: 10.1371/journal.pntd.0009133
14. CDC. Guidance for US Laboratories Testing for Zika Virus Infection. Available online at: https://www.cdc.gov/zika/laboratories/lab-guidance.html (accessed July 24, 2017).
15. Pan American Health Organization. Zika Resources: Case Definitions. Washington, DC: Regional Office for the Americas of the World Health Organization (2016). Available online at: http://www.paho.org/hq/index.php?option=com_content&view=article&id=11117&Itemid=41532&lang=en2016 (accessed June 21, 2020).
16. Lanciotti RS, Kosoy OL, Laven JJ, Velez JO, Lambert AJ, Johnson AJ, et al. Genetic and serologic properties of Zika virus associated with an epidemic, Yap State, Micronesia. Emerg Infect Dis. (2007) 14:1232–9. doi: 10.3201/eid1408.080287
17. Waggoner JJ, Abeynayake J, Sahoo MK, Gresh L, Tellez Y, Gonzalez K, et al. Development of an internally controlled real-time reverse transcriptase PCR assay for pan-dengue virus detection and comparison of four molecular dengue virus detection assays. J Clin Microbiol. (2013) 51:2172–81. doi: 10.1128/JCM.00548-13
18. Carletti F, Bordi L, Chiappini R, Ippolito G, Sciarrone MR, Capobianchi MR, et al. Rapid detection and quantification of Chikungunya virus by a one-step reverse transcription polymerase chain reaction real-time assay. Am J Trop Med Hyg. (2007) 521–4. doi: 10.4269/ajtmh.2007.77.521
19. Patel P, Landt O, Kaiser M, Faye O, Koppe T, Lass U, et al. Development of one-step quantitative reverse transcription PCR for the rapid detection of flaviviruses. Virol J. (2013) 10:58. doi: 10.1186/1743-422X-10-58
20. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. (2005) 53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x
21. Aguilar-Navarro SG, Mimenza-Alvarado AJ, Palacios-García AA, Samudio-Cruz A, Gutiérrez-Gutiérrez LA, Ávila-Funes JA. Validity and Reliability of the Spanish Version of the Montreal Cognitive Assessment (MoCA) for the Detection of Cognitive Impairment in Mexico. Rev Colomb Psiquiatr. (2018) 47:237–43. doi: 10.1016/j.rcp.2017.05.003
22. Wen X, Wang N, Liu J, Yan Z, Xin Z. Detection of cognitive impairment in patients with obstructive sleep apnea hypopnea syndrome using mismatch negativity. Neural Regen Res. (2012) 7:1591–8. doi: 10.3969/j.issn.1673-5374.2012.20.010
23. Hawkins MA, Gathright EC, Gunstad J, Dolansky MA, Redle JD, Josephson R, et al. The MoCA and MMSE as screeners for cognitive impairment in a heart failure population: a study with comprehensive neuropsychological testing. Heart Lung. (2014) 43:462–8. doi: 10.1016/j.hrtlng.2014.05.011
24. Vásquez KA, Valverde EM, Aguilar DV, Gabarain HH. Montreal cognitive assessment scale in patients with Parkinson disease with normal scores in the mini-mental state examination. Dement Neuropsychol. (2019) 13:78–81. doi: 10.1590/1980-57642018dn13-010008
25. Brookes RL, Hollocks MJ, Tan RY, Morris RG, Markus HS. Brief screening of vascular cognitive impairment in patients with cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy without dementia. Stroke. (2016) 47:2482–7. doi: 10.1161/STROKEAHA.116.013761
26. Paez-Venegas N, Jordan-Estrada B, Chavarria-Avila E, Perez-Vazquez F, Gómez-Bañuelos E, Medina-Dávalos R, et al. The montreal cognitive assessment test: a useful tool in screening of cognitive impairment in patients with systemic lupus erythematosus. J Clin Rheumatol. (2019) 25:325–8. doi: 10.1097/RHU.0000000000000876
27. Ritter A, Hawley N, Banks SJ, Miller JB. The association between montreal cognitive assessment memory scores and hippocampal volume in a neurodegenerative disease sample. J Alzheimers Dis. (2017) 58:695–9. doi: 10.3233/JAD-161241
28. Ustün TB, Chatterji S, Kostanjsek N, Rehm J, Kennedy C, Epping-Jordan J, et al. Developing the world health organization disability assessment schedule 2.0. Bull World Health Organ. (2010) 88:815–23. doi: 10.2471/BLT.09.067231
30. R Core Team (2018). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available online at: https://www.R-project.org/
31. O'Brien PC Zhang D Bailey KSemi-parametric R and non-parametric methods for clinical trials with incomplete data. Stat Med. (2005) 24:341–58. doi: 10.1002/sim.1963
32. Li GH, Ning ZJ, Liu YM, Li XH. Neurological Manifestations of Dengue Infection. Front Cell Infect Microbiol. (2017) 7:449. doi: 10.3389/fcimb.2017.00449
33. Galliez RM, Spitz M, Rafful PP, Cagy M, Escosteguy C, Germano CS, et al. Zika Virus Causing Encephalomyelitis Associated With Immunoactivation. Open Forum Infect Dis. (2016) 3:ofw203. doi: 10.1093/ofid/ofw203
34. Pierson TC, Fremont DH, Kuhn RJ, Diamond MS. Structural insights into the mechanisms of antibody-mediated neutralization of flavivirus infection: implications for vaccine development. Cell Host Microbe. (2008) 4:229–38. doi: 10.1016/j.chom.2008.08.004
35. Halstead SB. Dengue antibody-dependent enhancement: knowns and unknowns. Microbiol Spectr. (2014) 2:AID-0022-2014. doi: 10.1128/9781555817411.ch15
36. Wen J, Shresta S. Antigenic cross-reactivity between Zika and dengue viruses: is it time to develop a universal vaccine?. Curr Opin Immunol. (2019) 59:1–8. doi: 10.1016/j.coi.2019.02.001
37. Figueiredo CP, Barros-Aragão FGQ, Neris RLS, Frost PS, Soares C, Souza INO, et al. Zika virus replicates in adult human brain tissue and impairs synapses and memory in mice. Nat Commun. (2019) 10:3890. doi: 10.1038/s41467-019-11866-7
38. Rozé B, Najioullah F, Signate A, Apetse K, Brouste Y, Gourgoudou S, et al. Zika virus detection in cerebrospinal fluid from two patients with encephalopathy, Martinique, February 2016. Euro Surveill. (2016) 21:30205. doi: 10.2807/1560-7917.ES.2016.21.16.30205
Keywords: humans, mental status and dementia tests, communicable diseases, dengue virus infection, memory, cognition, montreal cognitive assessment, zika virus infection
Citation: Belaunzarán-Zamudio PF, Ortega-Villa AM, Mimenza-Alvarado AJ, Guerra-De-Blas PDC, Aguilar-Navarro SG, Sepúlveda-Delgado J, Hunsberger S, Valdés Salgado R, Ramos-Castañeda J, Rincón León HA, Rodríguez de La Rosa P, Nájera Cancino JG, Beigel J, Caballero Sosa S, Ruiz Hernández E, Powers JH III, Ruiz-Palacios GM and Lane C (2021) Comparison of the Impact of Zika and Dengue Virus Infection, and Other Acute Illnesses of Unidentified Origin on Cognitive Functions in a Prospective Cohort in Chiapas Mexico. Front. Neurol. 12:631801. doi: 10.3389/fneur.2021.631801
Received: 21 November 2020; Accepted: 22 February 2021;
Published: 22 March 2021.
Edited by:
Avindra Nath, National Institute of Neurological Disorders and Stroke (NINDS), United StatesReviewed by:
Tory P. Johnson, Johns Hopkins University, United StatesAna Terzian, Oswaldo Cruz Foundation (Fiocruz), Brazil
Copyright © 2021 Belaunzarán-Zamudio, Ortega-Villa, Mimenza-Alvarado, Guerra-De-Blas, Aguilar-Navarro, Sepúlveda-Delgado, Hunsberger, Salgado, Ramos-Castañeda, Rincón León, Rodríguez de La Rosa, Nájera Cancino, Beigel, Caballero Sosa, Ruiz Hernández, Powers, Ruiz-Palacios and Lane. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo F. Belaunzarán-Zamudio, cC5iZWxhdW56QGluZmVjdG8ubXg=