 Heather R. Altier1*
Heather R. Altier1* Jameson K. Hirsch2
Jameson K. Hirsch2 Annemarie Weber3
Annemarie Weber3 Niko Kohls4
Niko Kohls4 Jörg Schelling5*
Jörg Schelling5* Loren L. Toussaint6
Loren L. Toussaint6 Fuschia M. Sirois7
Fuschia M. Sirois7 Martin Offenbächer8,9
Martin Offenbächer8,9- 1Department of Psychiatry and Behavioral Sciences, Johns Hopkins University School of Medicine, Baltimore, MD, United States
- 2Department of Psychiatry and Behavioral Sciences, Quillen College of Medicine, East Tennessee State University, Johnson City, TN, United States
- 3Ärzte der Welt e.V. [Doctors of the World], Munich, Germany
- 4Division of Health Promotion, Faculty for Applied Natural Sciences and Health, Coburg University of Applied Sciences and Arts, Coburg, Germany
- 5Institute of General Practice and Family Medicine, Faculty of Medicine, Ludwig Maximilian University of Munich, Munich, Germany
- 6Department of Psychology, Luther College, Decorah, IA, United States
- 7Department of Psychology, Durham University, Durham, United Kingdom
- 8Gasteiner Heilstollen, Böckstein, Austria
- 9Institute of Ecomedicine, Paracelsus Medical University, Salzburg, Austria
Introduction: Sleep disturbances are prevalent among primary care patients, and psychological dysfunction, including stress, anxiety, and depression, are robust contributors to poor sleep health. Yet, the presence of potential protective characteristics, such as health self-efficacy and engaging in adaptive health behaviors, may mitigate such outcomes. Gratitude (i.e., recognition and appreciation of experiences, relationships, and surroundings), a positive psychological cognitive-emotional characteristic, may serve as a catalyst of these beneficial downstream effects, given its association with improved health functioning and sleep.
Methods: In a sample of primary care patients (N = 869, M age = 53; 60.7% female) from 50 urban and 30 rural practices in Germany, health self-efficacy (i.e., belief in ability to perform necessary actions to manage health) and constructive health behaviors (i.e., actions taken to modify health positively), separately and together as parallel first-order mediators, and stress, anxiety, and depression, as parallel second-order mediators, were investigated as potential serial mediators of the association between gratitude and sleep disturbances. Participants completed self-report measures in person and online.
Results: Significant serial mediation was observed across models, although effects varied. In the first model, gratitude was associated with greater health self-efficacy and, in turn, to less stress (a1d21b4 = −0.019, 95% CI [−0.039, −0.002], SE = 0.010), anxiety (a1d31b5 = −0.026, 95% CI [−0.045, −0.008], SE = 0.009), and depression (a1d41b6 = −0.020, 95% CI [−0.040, −0.003], SE = 0.009), and fewer consequent sleep disturbances. In the second model, health behaviors, and anxiety (a1d31b5 = −0.009, 95% CI [−0.019, −0.002], SE = 0.004) and depression (a1d41b6 = −0.007, 95% CI [−0.016, −0.001], SE = 0.004), were serial mediators, but health behaviors and stress were not. In a final combined model, serial mediation occurred on two pathways, health self-efficacy and anxiety (a1d41b6 = −0.026, 95% CI [−0.046, −0.009], SE = 0.009), and health self-efficacy and depression (a1d51b7 = −0.019, 95% CI [−0.037, −0.003], SE = 0.009), and a specific indirect effect was found for health behaviors (a2b4= −0.086, 95% CI [−0.140, −0.030], SE = 0.026), but not self-efficacy.
Discussion: Overall, gratitude was associated with reduced sleep disturbances through positive health behavior engagement, and via the serial mediation effects of greater health self-efficacy and lower psychological distress. Clinical interventions that enhance gratitude (e.g., gratitude listing or diaries), self-efficacy (e.g., disease self-management programs), or health behavior engagement (e.g., weight management programs) may promote favorable downstream effects on psychological distress and sleep disturbances among primary care patients.
1 Introduction
Sleep disturbances are prevalent worldwide, with 44% of adults reporting difficulty falling asleep and 35% indicating difficulty maintaining sleep (Aernout et al., 2021). Forty percent of primary care visits address sleep-related complaints (Arroll et al., 2012). In the United States, the number of outpatient ambulatory visits with sleep disturbance listed as the chief complaint increased 29% in a decade (Ford et al., 2014). Problems initiating and maintaining sleep are the defining criteria of the most prevalent sleep disorder, insomnia, which afflicts 22% of the global population and is more common (1.6:1) in females than males (Zeng et al., 2020). Insomnia symptoms occur in approximately one-third of primary care patients and difficulty maintaining sleep is the most prevalent characteristic, present in 80% of primary care patients with insomnia (Léger et al., 2010). Both oversleeping and undersleeping are associated with musculoskeletal, endocrine, respiratory, and neurological disorders, inflammation, higher cardiometabolic risk, and mortality (Åkerstedt et al., 2017; Irwin et al., 2016; Kanagasabai and Chaput, 2017; Ohayon et al., 2013; Shorofsky et al., 2019).
Given the deleterious impact of sleep disturbance on health, detection and intervention are imperative (Chattu et al., 2018). Individual-level cognitive-emotional factors are often more amenable to clinical intervention than fixed biological contributors (Hale et al., 2020). Gratitude is one such factor, and has been linked to improvements in health functioning, including sleep (Jackowska et al., 2016; Ng and Wong, 2013). Gratitude is an affective trait or emotion that encompasses appreciation for benefits received, including thankfulness for the present moment, nature, beauty, and life circumstances (McCullough et al., 2002; Wood et al., 2008). Several studies have demonstrated that gratitude can improve sleep. A systematic review of randomized controlled trials revealed that gratitude interventions (e.g., gratitude diaries, daily gratitude lists) improved subjective sleep quality in five samples, including individuals diagnosed with anxiety and depression, patients with neuromuscular disease, community adults, and college students (Boggiss et al., 2020). In these and other studies, the influence of gratitude on sleep disturbances is rarely explored without evaluating cognitive-emotional mechanisms or psychopathology. For example, in an RCT among German community members, a gratitude intervention improved gratitude and reduced worry, anxiety, depression, and insomnia symptoms post-intervention and at 3- and 6- month follow-ups (Heckendorf et al., 2019). In another RCT, individuals endorsing anxiety and depression diagnoses reported reduced stress, anxiety, depression, and sleep difficulties after completing a 3-week gratitude diary and, at 3-week follow-up, stress scores were maintained and anxiety scores had significantly improved (Southwell and Gould, 2017). Finally, among young adults, depressive symptoms explained the effect of gratitude on longer sleep duration and higher daytime energy (Alkozei et al., 2019), and among Austrian patients with rheumatic and musculoskeletal disease, gratitude was associated with less stress, anxiety, and depressive symptoms and, in turn, to better sleep quality and less functional impairment (Hirsch et al., 2021).
Extant research provides support for a beneficial effect of gratitude on amelioration of stress, anxiety, and depression, and sleep disturbances, both directly and indirectly. Yet, the mechanisms responsible for this protective influence have remained largely unexplored. In our theoretical model (see Figure 1), we propose that health self-efficacy, or belief in ability to perform health-supporting behaviors (Sirois, 2007), and engagement in wellness activities, are two potential explanatory linkages (Cousin et al., 2021). Drawing from the broaden-and-build theory (Fredrickson, 2004), gratitude may promote wellbeing by broadening one's awareness, thoughts, and behaviors over time, thereby promoting the development of resources (e.g., health, relationships, skills) that can be utilized to cope with stress (Fredrickson, 2004; Wood et al., 2010). Additionally, the coping hypothesis suggests that gratitude encourages adaptive coping strategies, such as planning and social support, which protect against stress and other adverse mental health outcomes (Wood et al., 2007). Finally, according to the positive affect hypothesis, gratitude, as a pleasant emotion, may produce additional constructive emotions that promote wellbeing and life satisfaction (Wood et al., 2010).
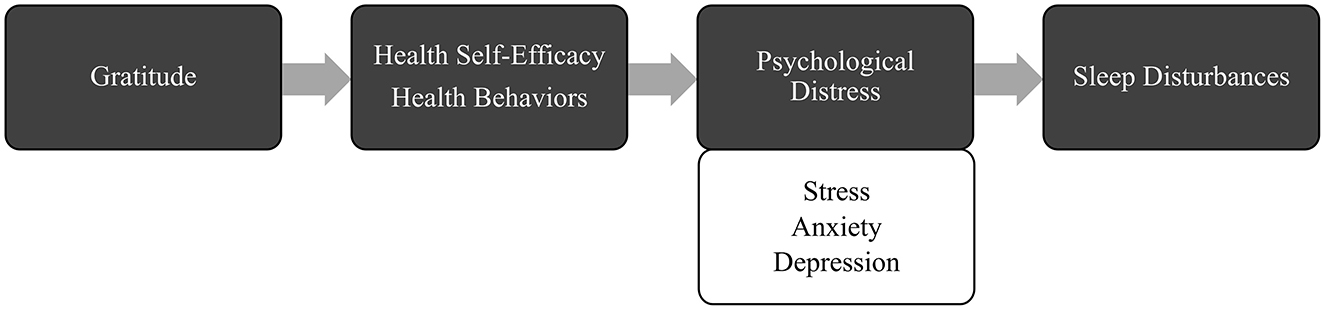
Figure 1. Illustration of theoretical model depicting hypothesized multiple mediation effects of gratitude on sleep disturbances via health self-efficacy, health behaviors, and psychological distress.
Consistent with these theories, prior studies independently link gratitude to health-promoting beliefs (e.g., health self-efficacy), behaviors (e.g., exercise, diet), and reduced psychological distress (DuBois et al., 2016; Grant and Gino, 2010). For example, among patients with heart failure, gratitude was associated with improved self-efficacy to maintain physical functioning and, in turn, to better medication adherence (Cousin et al., 2020), and with greater self-efficacy to preserve heart function, less depression, better sleep, and lower levels of inflammatory markers (Mills et al., 2015). Further, gratitude for one's health predicted heightened physical activity, as assessed via accelerometer, and gratitude for one's life predicted medical adherence after 6 months, among acute coronary syndrome patients (Legler et al., 2019). In primary care samples, the roles of health self-efficacy and health behavior engagement in promoting psychological and sleep health is well-established (Alfaris et al., 2015; Bluestein et al., 2010). However, no studies have integrated these pathways into a unified model, nor clarified the distinct and shared roles of cognitive-emotional and behavioral mediators in the gratitude-sleep relationship.
Given that nearly 70% of primary care visits involve psychological complaints, including depression and anxiety (Hunter and American Psychological Association, 2009), significant comorbidity exists between psychological and physical conditions (Gili et al., 2010), and emerging conditions are most often identified and treated in primary care settings (Schoen et al., 2008), it is important to identify risk and protective factors that can be targeted for clinical intervention in primary care. Gratitude is one such clinically malleable factor (Heckendorf et al., 2019; Yuan et al., 2021), with robust linkages to adaptive health outcomes.
In the current study, we examined the potential serial mediation effects of health self-efficacy and health behaviors, and stress, anxiety, and depression, on the relation between gratitude and sleep disturbances. As perceived stress, anxiety, and depression frequently co-occur and interact and, in conjunction, exacerbate sleep disturbance (Demyttenaere and Heirman, 2020; Kalmbach et al., 2018; Karing, 2021) due to shared cognitive-emotional and biological mechanisms (Boggero et al., 2017; Packard et al., 2016; Thorsteinsson et al., 2019), we examined them as parallel, rather than serial or separate, mediators in our models. We hypothesized that health self-efficacy and health behaviors, separately and together as parallel first-order mediators, and stress, anxiety, and depression, as parallel second-order mediators, would serially mediate the association between gratitude and sleep disturbances, such that greater gratitude would be associated with higher levels of health self-efficacy and/or health behaviors and, in turn, to less stress, anxiety and depressive symptoms, and sleep disturbances.
2 Materials and methods
Over a period of 2 months, patients from 50 urban primary care practices in the Munich area and 30 rural primary care practices in the Upper Franconia region of Germany were recruited in person by clinic staff and providers, and via informational posters, to complete a questionnaire battery. Paper surveys could be returned to the practice in person or to either study center at Coburg University of Applied Sciences or the University of Munich via postal mail, and questionnaires could also be completed online. The original study was approved by the Ethics Commission of the Faculty of Medicine at the Ludwig Maximilian University of Munich, and participation was voluntary. To ensure privacy, the Institutional Review Board waived consent requirements and no written informed consent was obtained. To participate, respondents were required to be age 18 or older, to have sufficient knowledge of German, and to possess a willingness to participate. Participants under age 18 and with severe psychiatric disorders were excluded.
2.1 Participants
Participants (N = 869) were 39.1% male (n = 343) and 60.7% female (n = 533), ranging from 20 to 92 years of age (M = 53.00, SD = 11.96). Race and ethnicity data were not collected, as legal restrictions and sociopolitical pressures enjoin researchers from collecting ethnoracial data in Germany and much of Western Europe (Roig, 2017; Simon, 2012). Regarding education, most participants reported having an intermediate school certificate (n = 287; 32.7%), followed by a high school diploma (n = 252; 28.7%), some high school completed (n = 196; 22.3%), university entrance qualification (n = 75; 8.5%), and other certificate (n = 48; 5.5%). Most participants reported one chronic medical condition (n = 305; 34.7%), followed by zero (n = 206; 23.5%), two (n = 182; 20.7%), three (n = 97; 11.0%), four (n = 46; 5.2%), and five or more (n = 41; 4.6%).
2.2 Measures
In addition to measures assessing this study's variables, participants responded to demographic questions (e.g., age, family composition, zip code, marital status, height/weight), meant for characterizing the sample and to serve as covariates.
2.2.1 Sleep disturbances
Frequency of sleep disturbances was assessed using Item 3 from the Patient Health Questionnaire-9, which was developed to detect depressive symptoms among primary care patients (Kroenke et al., 2001). Item 3 was extracted from the German translation of the PHQ-9, developed by Gräfe et al. (2004) using internationally accepted translation methods and available on Pfizer's Patient Health Questionnaire website. Participants indicated, on a scale from 0 (not at all) to 3 (nearly every day), the frequency with which they experience “Trouble falling or staying asleep, or sleeping too much”, and a higher score indicates greater sleep difficulty. This item is considered a valid measure of sleep disturbances that can be used as a substitute for longer instruments. For example, in a study aiming to evaluate the item's utility for screening for sleep disturbances in primary care patients, the PHQ item 3 demonstrated convergent validity (r = 0.75, p < 0.001) with the Insomnia Severity Index (ISI; Morin, 1993), and a cutoff score of 1, which indicates sleep problems were present several days over the past 2 weeks, yielded the optimal balance of sensitivity (82.5%) and specificity (84.5%; MacGregor et al., 2012). Further, among German cancer patients, this item was strongly correlated with the ISI (r = 0.72, p < 0.001) and performed similarly to the ISI; the ISI and Item 3 exhibited similar correlations with the Patient Health Questionnaire-2 (PHQ-2; Kroenke et al., 2003; r = 0.45, 0.42), Generalized Anxiety Disorder 2-item scale (GAD-2; Kroenke et al., 2007; r = 0.45, 0.39), and had comparable magnitudes and patterns of association with sex, age, and tumor type (Schulte et al., 2021).
2.2.2 Perceived stress
The Perceived Stress Scale–4 (PSS-4; Cohen and Williamson, 1988), German version (Stächele and Volz, 2013), was used to evaluate stress. On a Likert scale, ranging from 0 (never) to 4 (very often), respondents indicated the degree of appraised stress over the past month via statements such as, “In the last month, how often have you felt that you were unable to control the important things in your life?” and “In the last month, how often have you felt that things were going your way?” After recoding two items to indicate greater perceived stress, items are summed to generate a total score between 0 and 16. The four items comprising the scale were extracted from the original scale, the PSS-14 (Cohen et al., 1983). In the current sample, the PSS-4 demonstrated acceptable reliability (Cronbach's α = 0.73; McDonald's ω = 0.74), and acceptable (α = 0.74) to good (α = 0.84) reliability in prior health samples (Vallejo et al., 2018; Wu and Amtmann, 2013).
2.2.3 Anxiety
The Generalized Anxiety Disorder 2-item scale (GAD-2; Kroenke et al., 2007) measures anxiety on a Likert scale ranging from 0 (not at all) to 3 (nearly every day), via items representing core anxiety symptoms from the Generalized Anxiety Disorder 7-item scale (GAD-7; Spitzer et al., 2006). The two items utilized were from the German translation of the GAD-7, developed by Löwe et al. (2008) using internationally accepted translation methods and downloaded from Pfizer's Patient Health Questionnaire website. Participants indicate how often over the last 2 weeks they were bothered by “Feeling nervous, anxious or on edge” and “Not being able to stop or control worrying”. The total score, which ranges from 0 to 6, is obtained by summation of item scores. Higher scores denote greater anxiety symptoms, with a cutoff of 3 providing good sensitivity and specificity to detect clinically significant anxiety symptoms (Kroenke et al., 2007), which was supported in a systematic review (N = 5,223) of validation studies (Plummer et al., 2016). Internal consistency reliability was good in the current sample (α = 0.80; ω = 0.82). The GAD-2 exhibited acceptable reliability and strong correlations with the GAD-7 in samples of community-dwelling adults in Germany (α = 0.72; r = 0.87; Hinz et al., 2017) and multiple sclerosis patients (α = 0.77; r = 0.94; Hughes et al., 2018).
2.2.4 Depression
The Patient Health Questionnaire-2 (PHQ-2; Kroenke et al., 2003), comprised of the first two items of the original measure, the Patient Health Questionnaire-9 (Kroenke et al., 2001), was used to assess depressive symptoms over the past 2 weeks. The two items were taken from Gräfe et al.'s (2004) German translation of the PHQ-9. Respondents indicated how often they were bothered by “Little interest or pleasure in doing things” and “Feeling down, depressed, or hopeless”, on a scale ranging from 0 (not at all) to 3 (nearly every day). Responses were summed for a total score ranging from 0 to 6, with higher scores indicating greater depressive symptoms. A score of 3 is considered the cutoff for detecting clinically significant depression (Staples et al., 2019), although some research suggests a more modest cutoff of 2 (Manea et al., 2016). In the current study, reliability of the PHQ-2 was good (α = 0.79; ω = 0.83), and in a sample of German COPD inpatients, composite reliability was good (CR = 0.89; Schuler et al., 2018). Among 1,619 German primary care outpatients, the PHQ-2 was strongly correlated with the PHQ-9 (r = 0.87; Löwe et al., 2005).
2.2.5 Gratitude
Gratitude was measured using the Gratitude Questionnaire-Six Item Form (GQ-6; McCullough et al., 2002), German translation (Personality and Assessment Group, Department of Psychology, University of Zurich, n.d.), which includes six statements (e.g., “I am grateful to a wide variety of people”; “If I had to list everything that I felt grateful for, it would be a very long list”) assessing appreciation. Responses are rated on a scale ranging from 1 (strongly disagree) to 7 (strongly agree) and are summed to compute a total score between 6 and 42, after reverse scoring two items so that higher scores denote higher gratitude levels. In the current sample, internal consistency reliability was acceptable (α = 0.77; ω = 0.77). In a meta-analysis, internal consistency reliability was acceptable in European studies (α = 0.75), and good when averaging all 74 studies (α = 0.82; Card, 2019).
2.2.6 Health self-efficacy
Health self-efficacy, or the degree of confidence one possesses in their ability to engage in the necessary actions to control their health, was assessed using six items from the 8-item Health Self-Efficacy/Mastery Beliefs subscale of the Control Beliefs Inventory (HSE-CBI; Sirois, 2003a), a 26-item measure of perceived control. Two items assessing aspects of health self-efficacy incorporated in the remaining items with alternative wording were excluded to reduce participant burden. As one item is reverse scored, the omission is not expected to significantly affect internal consistency. The original measure was translated from English into German, and then back-translated to English by a panel comprising members of the research team who are bilingual native German speakers fluent in English. Inconsistencies were reconciled between the researchers. Respondents indicate on a scale ranging from 1 (strongly disagree) to 6 (strongly agree) the degree to which they agree with statements such as “I am confident that I can successfully look after my health” and “I am able to meet the challenge of following a healthy routine”. After reverse scoring two negatively worded items, the average of the six items is computed to calculate an HSE-CBI total score between 1 and 6, with a higher score indicating a greater degree of health self-efficacy. In the current study, the HSE-CBI has acceptable reliability (α = 0.77; ω = 0.73), and good reliability (α = 0.84) in two samples of community adults (Sirois, 2004). The HSE-CBI demonstrated convergent validity with the General Perceived Self-Efficacy Scale (Schwarzer and Jerusalem, 1995) among community adults (Sirois, 2003b).
2.2.7 Health behaviors
Participants completed the Wellness Behaviors Inventory (WBI), a measure that assesses the frequency of engagement in health-promoting behaviors, such as exercising, relaxation, and healthy eating (Sirois, 2001). The WBI was translated into German using the same procedure as the HSE-CBI. Responses to items such as “I eat breakfast” and “I exercise for 20 continuous minutes or more, to the point of perspiration” are provided on a 5-point Likert scale ranging from 1 (less than once a week or never) to 5 (every day of the week). Although the WBI consists of 12 items, only the 10 items utilized to compute the total score were included in this study. The two excluded items refer to vitamin and supplement use and form a separate optional index of health behaviors (Sirois, 2001). Two items are reverse scored before calculating the total mean score, which ranges from 1 to 5, with higher scores denoting greater engagement in health behaviors. In the current primary care sample, the WBI had questionable internal consistency reliability (α = 0.63; ω = 0.64), consistent with prior research; in a meta-analysis of 15 undergraduate and community adult samples, reliability ranged from questionable to acceptable (α = 0.64–74; Sirois et al., 2015), likely due to its checklist status.
2.3 Statistical analyses
2.3.1 Bivariate analyses
All analyses were conducted in R Version 2022.07.1 (R Core Team, 2022). To establish the presence of bivariate relationships before testing mediation effects, Pearson's product-moment and Spearman's rank-order correlation coefficients were calculated to assess the associations among gratitude, health self-efficacy, health behaviors, stress, anxiety, and depression, and the correlations between each of these variables and sleep disturbances were evaluated with Spearman's rank-order correlation coefficients, using the R package psych (Revelle, 2022). A multicollinearity cutoff of r > 0.80 between study variables was used, as associations exceeding this threshold may indicate lack of independence and would be interpreted with caution (Field, 2013).
2.3.2 Serial multivariate mediation analyses
Prior to conducting the mediation analyses, skewness, kurtosis, and heteroscedasticity of the data were evaluated using base R functions, to ensure the assumptions of linear regression were met (R Core Team, 2022). All predictors were standardized (i.e., converted to z-scores) because they have no natural or common metric, allowing the relative influence of each predictor to be meaningfully compared in models containing both linear and ordinal logistic regression analyses (Agresti, 1996; Menard, 2004). Sleep disturbances, being an ordered polytomous variable, was not standardized.
Three serial mediation path analyses were conducted. In the first model, the relation between gratitude and sleep disturbances, via the potential mediating effects of health self-efficacy as a first-order mediator, and stress, anxiety, and depression, as second-order parallel mediators, was assessed. In the second model, health self-efficacy was replaced with health behaviors as the first-order mediator. Finally, in the third model, health self-efficacy and health behaviors were evaluated as parallel first-order mediators. Age, sex, education level, and number of chronic diseases were included as covariates in each model.
2.3.2.1 Analytic procedure
As the outcome variable, sleep disturbances, is not continuous and, instead, was measured using one item with four levels, the final regression equation of the serial mediation model (i.e., sleep disturbances regressed on gratitude and all mediators and covariates) was calculated using cumulative odds ordinal logistic regression with the VGAM package (Yee, 2015). All other pathways of the serial mediation model were analyzed using ordinary least squares linear regression, via the stats package (R Core Team, 2022).
For the ordinary least squares regression steps of each model, a change of one standard deviation in the predictor is associated with a change of β standard deviations in the endogenous variable. Regarding the ordinal logistic regression step of each model, a one standard deviation difference in the predictor is associated with a β-unit difference in ordered logits of sleep disturbance frequency (Menard, 2004). To simplify interpretation of the ordinal logistic regression results, the standardized coefficients were converted to odds ratios (OR), so that for each one standard deviation increase in the predictor, the odds of being more likely to endorse a higher frequency of sleep disturbances is multiplied OR times, holding constant all other variables.
Regarding the final step of each model, ordinal logistic and multinomial logistic regression models were compared, using the likelihood ratio test, to determine which type of model fit the data better, via the VGAM package (Yee, 2015). Next, the proportional odds assumption of ordinal logistic regression (i.e., stating each predictor has an equivalent effect, or parallel slopes, across all levels of the outcome variable; McCullagh, 1980) was evaluated, using likelihood ratio tests in the ordinal package (Christensen, 2019). If the assumption was violated, a partial proportional odds model was fit, which relaxes the proportional odds assumption and allows multiple regression coefficients only for predictors that have differential effects on the levels of the outcome variable (Peterson and Harrell, 1990).
Subsequently, non-significant covariates were removed from the linear and ordinal logistic regression analyses in a backward stepwise manner to preserve power, unless their inclusion improved overall model fit (Faraway, 2015). Finally, a function was written to calculate all mediation effects for each model, by multiplying coefficients for each path (e.g., the serial mediation effect of gratitude on sleep through health self-efficacy and stress is calculated as a1d31b5). As each model used standardized regression coefficients and continuous mediators, the mediated effect may be obtained by multiplying coefficients (i.e., using the product of coefficients method) from both ordinary least squares and ordinal logistic regression pathways and bootstrapping the confidence intervals (MacKinnon et al., 2007). Bootstrapping using 10,000 simulated samples and 95% confidence intervals, per the percentile method, was utilized in each model, to estimate the sampling distribution of the mediation effects. All p-values for the regression coefficients were adjusted using the p.adjust function in the stats package (R Core Team, 2022), applying the False Discovery Rate (FDR) method (Benjamini and Hochberg, 1995) to control for multiple comparisons across models. Pathways were considered statistically significant if the FDR-adjusted p-values were below the conventional threshold of 0.05. To correct the confidence intervals for the mediation effects, the False Coverage Rate (FCR) method was applied at a threshold of 0.97, which was calculated using the proportion of ratio of null effects to total effects across models. This method controls for false coverage in the estimation of CIs, reducing the risk of obtaining misleading conclusions about significance (Benjamini and Yekutieli, 2005). Mediation effects were considered statistically significant if the corrected 97% CIs did not include zero. Finally, multicollinearity for all predictors in each model was assessed by calculating the variance inflation factor (VIF) with the R package car (Fox and Weisberg, 2019). The VIF of each coefficient should be < 5 (Hair et al., 2019), and ideally around 1 (Akinwande et al., 2015).
Of note, path analysis was determined to be a more appropriate statistical approach than structural equation modeling (SEM) because we were interested in the relationships between variables and the mediation pathways, rather than any latent constructs or the measurement properties of the scales, and our one-item outcome variable precludes the use of comprehensive latent SEM. Further, the robust estimators available in R (maximum likelihood, weighted least squares mean and variance), cannot be used with bootstrapping for models with ordinal outcome variables, limiting methods for confidence interval estimation, and cannot be modeled to allow multiple slopes for a predictor when the proportional odds assumption is violated (Rosseel, 2012). However, as a supplementary analysis, we conducted SEM to obtain overall fit statistics for each model, dichotomizing the outcome variable and specifying psychological distress as a latent variable comprised of stress, anxiety, and depression. More details regarding the procedure and results can be found in the Supplementary material.
3 Results
3.1 Bivariate analyses
Pearson's bivariate and Spearman's rank-order correlation analyses indicated that gratitude was positively correlated with health self-efficacy (r = 0.27, p < 0.001) and health behaviors (r = 0.09, p < 0.01), and negatively related to stress (r = −0.17, p < 0.001), anxiety (r = −0.12, p < 0.001), depression (r = −0.15, p < 0.001), and sleep disturbances (r = −0.10, p < 0.01). Similarly, health self-efficacy and health behaviors were positively related to each other (r = 0.30, p < 0.001) and negatively related to stress, anxiety, depression, and sleep disturbances (all p < 0.001). Bivariate correlations between all continuous and ordinal study variables are provided in Table 1. No correlations approached or exceeded the multicollinearity cutoff of r > 0.80.
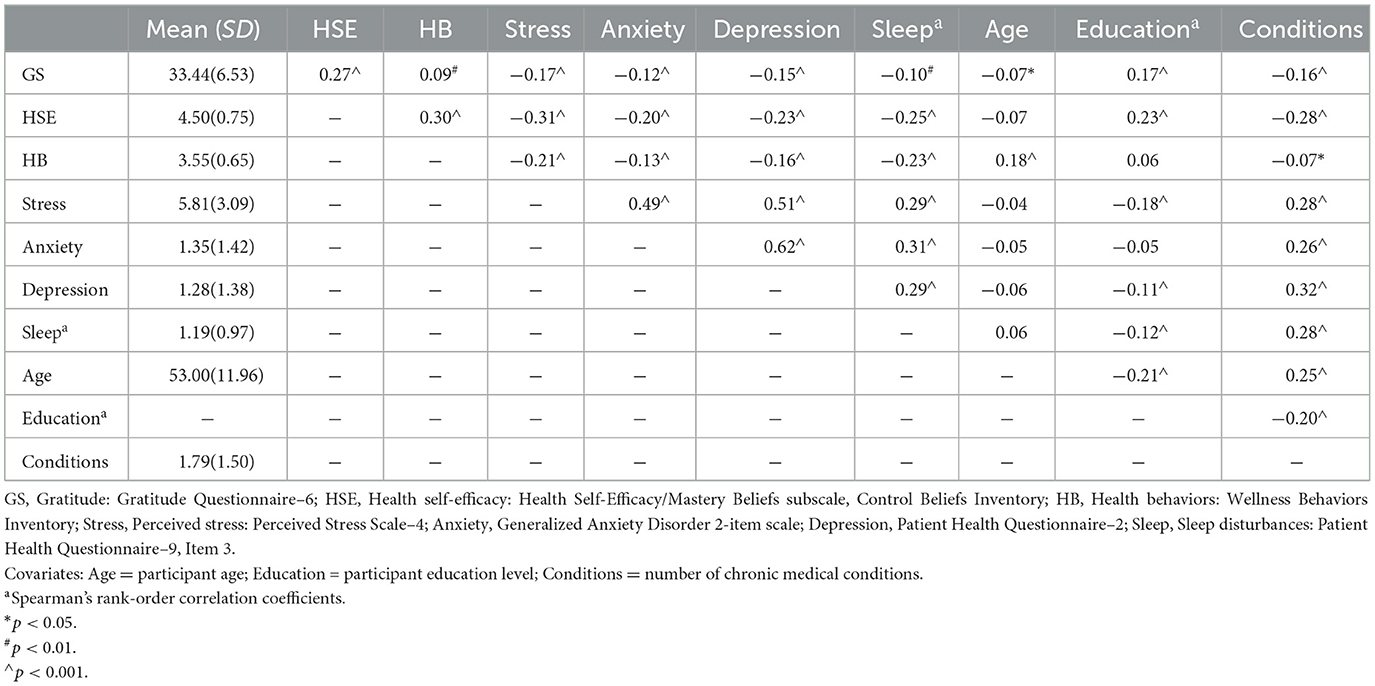
Table 1. Means, standard deviations, and bivariate correlations of study variables.
3.2 Serial multivariate mediation analyses
Examination of skewness, kurtosis, and heteroscedasticity indicated the assumptions of linear regression were met. Table 2 shows the frequencies of the ordinal outcome variable, sleep disturbances, by response category, and normality data for the item.
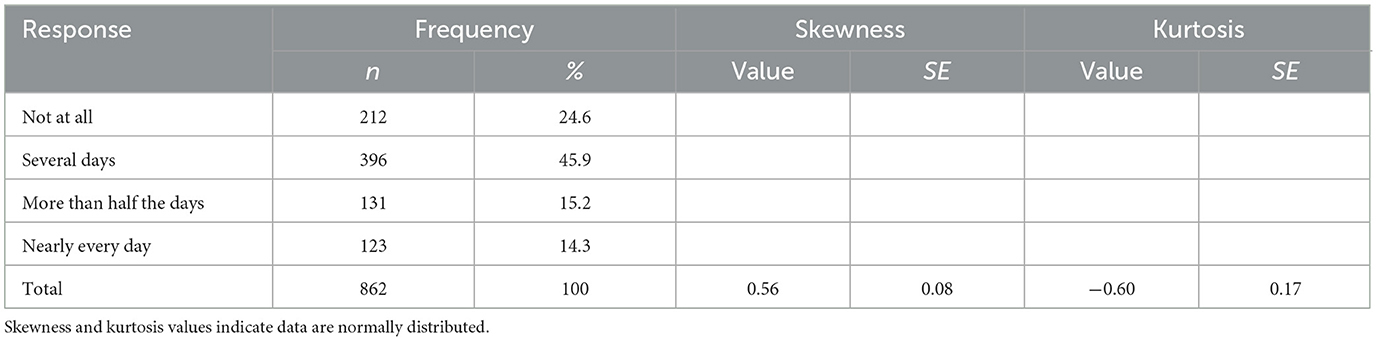
Table 2. Frequencies, skewness, and kurtosis for sleep disturbances.
3.2.1 Model 1
Regarding model 1, the ordinal logistic regression model fit the data significantly better than the multinomial model ( = 538.92, p ≤ 0.001) and was more parsimonious (i.e., contained the fewest regression coefficients). However, the proportional odds assumption was violated for health self-efficacy ( = 7.312, p = 0.026). Therefore, a partial proportional odds model incorporating three regression coefficients for health self-efficacy was used.
Linear and ordinal logistic regression results and fit statistics for each pathway, including significant covariates identified through backward stepwise selection, are provided in Table 3. Variance inflation factors are also provided in Table 3, and no predictors exceed the multicollinearity cutoff. Regression results excluding covariate effects are illustrated in Figure 2. Gratitude was related to higher health self-efficacy (β = 0.273, 95% CI [0.209, 0.337], SE = 0.032, t = 8.412, padjusted < 0.001) which was, in turn, related to lower stress (β = −0.320, 95% CI [−0.387, −0.253], SE = 0.034, t = −9.413, padjusted < 0.001), anxiety (β = −0.218, 95% CI [−0.288, −0.147], SE = 0.036, t = −6.078, padjusted < 0.001), and depression (β = −0.255, 95% CI [−0.322, −0.189], SE = 0.034, t = −7.530, padjusted < 0.001). A one standard deviation increase in stress was associated with a 24% greater likelihood of endorsing a higher frequency of sleep disturbances (OR = 1.242, 95% CI [1.091, 1.414], padjusted = 0.002), while equivalent increases in anxiety (OR = 1.553, 95% CI [1.357, 1.778], padjusted < 0.001) and depression (OR = 1.337, 95% CI [1.162, 1.540], padjusted < 0.001) were associated with 55% and 34% greater likelihood of sleep problem frequency, respectively.
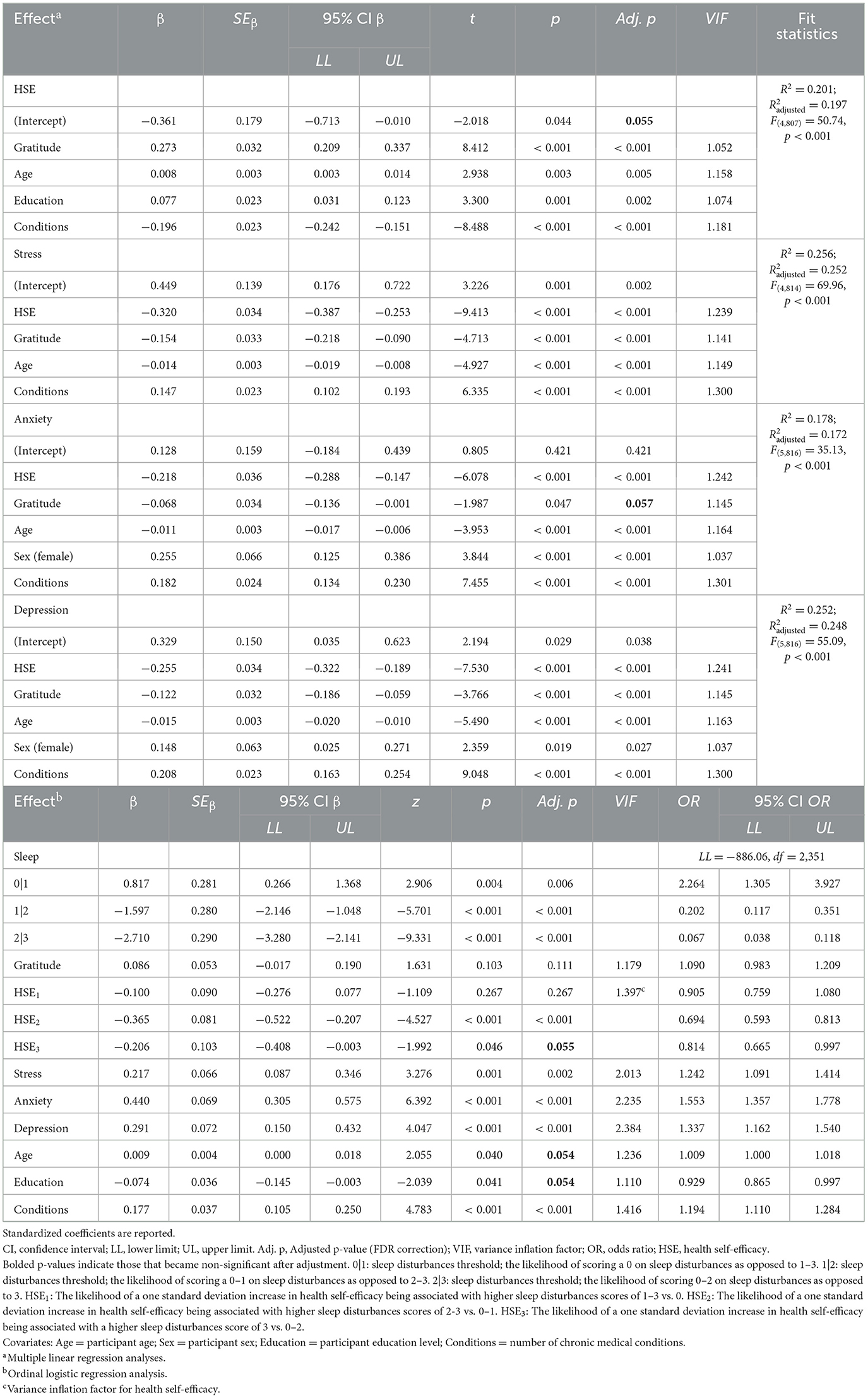
Table 3. Regression coefficients of serial indirect effects Model 1 for gratitude, health self-efficacy, psychological distress, and sleep disturbances, with covariates.
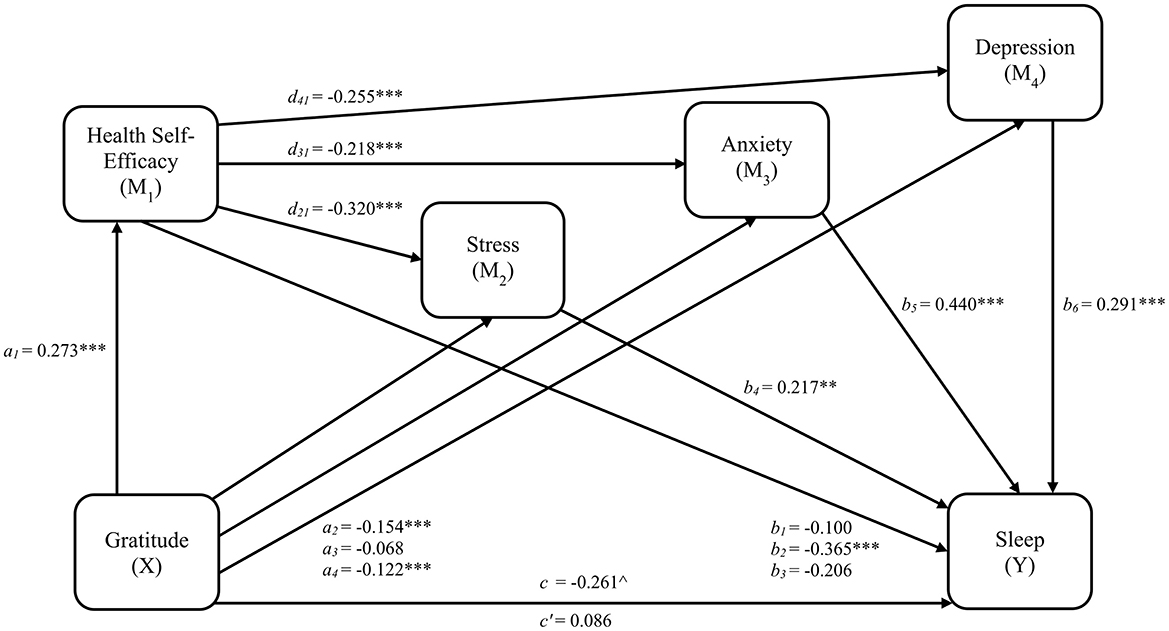
Figure 2. Serial indirect effects Model 1 for gratitude, health self-efficacy, psychological distress, and sleep disturbances. a1, a2, a3, a4 = regression coefficients for gratitude to health self-efficacy, stress, anxiety, and depression, respectively. b1, b2, b3 = regression coefficients for health self-efficacy to each threshold of sleep disturbances scores (0|1, 1|2, and 2|3, respectively). b4, b5, b6 = regression coefficients for stress, anxiety, and depression, respectively, to sleep disturbances. d21, d31, d41 = regression coefficients for health self-efficacy to stress, anxiety, and depression, respectively; c = total effect (gratitude related to sleep disturbances); c' = direct effect (gratitude related to sleep disturbances accounting for health self-efficacy and psychological distress). **p < 0.01; ***p < 0.001. p-values are FDR-adjusted. ∧Significance indicated by 95% CI that does not cross zero.
Mediation effect results for model 1 are provided in Table 4. As hypothesized, health self-efficacy as a first-order mediator, and stress (a1d21b4= −0.019, 95% CI [−0.039, −0.002], SE = 0.010), anxiety (a1d31b5 = −0.026, 95% CI [−0.045, −0.008], SE = 0.009), and depression (a1d41b6 = −0.020, 95% CI [−0.040, −0.003], SE = 0.009) as parallel second-order mediators, serially mediated the relation between gratitude and sleep disturbances. Additionally, specific indirect effects linking gratitude and sleep disturbances were observed for one of the three health self-efficacy pathways, HSE2 (a1b2 = −0.099, 95% CI [−0.166, −0.043], SE = 0.031), and stress (a2b4 = −0.033, 95% CI [−0.072, −0.003], SE = 0.018) and depression (a4b6 = −0.036, 95% CI [−0.078, −0.004], SE = 0.019). Overall, the total indirect effect (β = −0.347, 95% CI [−0.530, −0.066], SE = 0.105) and the total effect of gratitude on sleep disturbances (c = −0.261, 95% CI [−0.478, −0.030], SE = 0.112) were significant, while the direct effect was non-significant (c' = 0.086, 95% CI [−0.066, 0.235], SE = 0.078), indicating mediation. After adjusting the confidence intervals to 0.97 to account for false coverage rate correction, the conclusions regarding all indirect effects remained consistent.
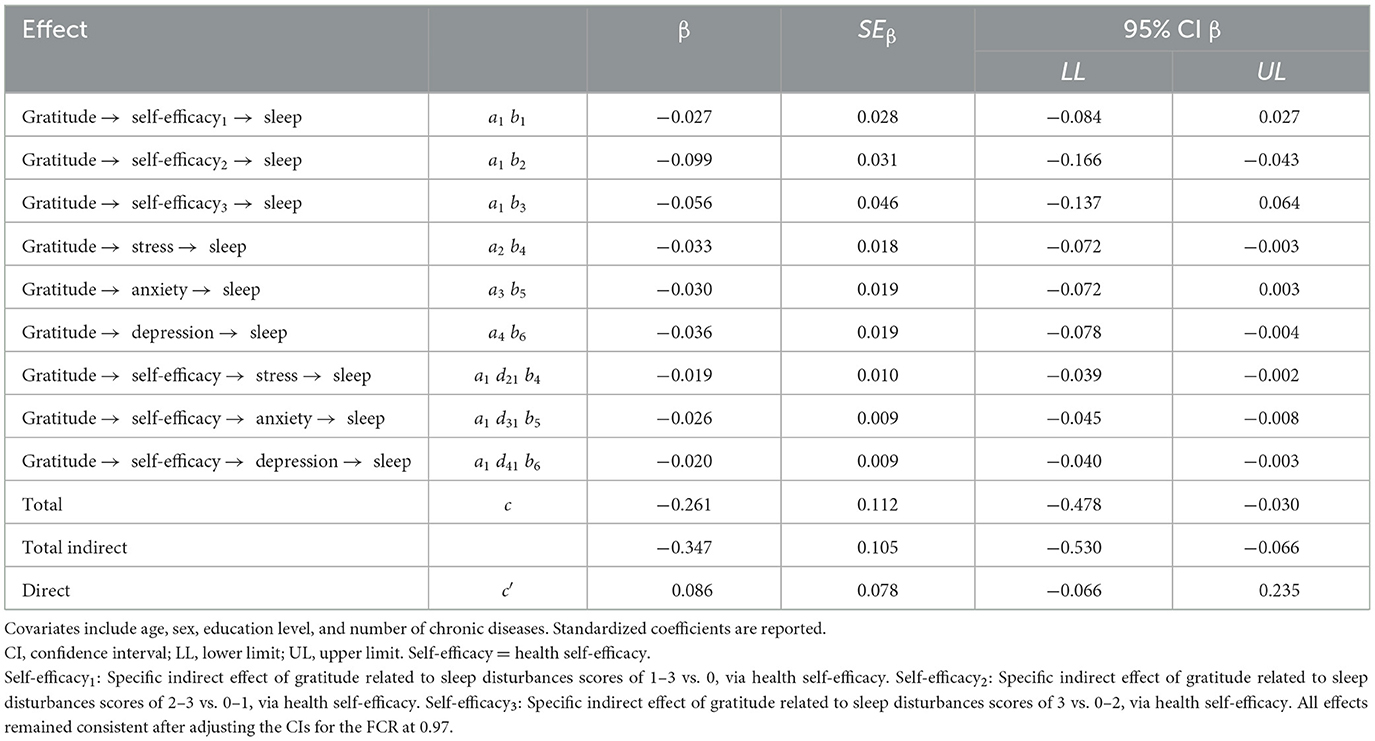
Table 4. Indirect effects of health self-efficacy and psychological distress on the relation between gratitude and sleep disturbances (Model 1).
3.2.2 Model 2
Regarding model 2, the ordinal logistic regression model fit the data significantly better than the multinomial model ( = 98.897, p ≤ 0.001) and was more parsimonious. However, the proportional odds assumption was violated for health behaviors ( = 6.558, p = 0.038). Therefore, a partial proportional odds model including three regression coefficients for health behaviors was used.
Linear and ordinal logistic regression results and fit statistics for each pathway, including significant covariates identified through backward stepwise selection, are provided in Table 5. Variance inflation factors are also provided in Table 5, and no predictors exceed the multicollinearity cutoff. Regression results excluding covariate effects are illustrated in Figure 3. Gratitude was related to better health behavior engagement (β = 0.173, 95% CI [0.106, 0.239], SE = 0.034, t = 5.081, padjusted < 0.001) which was, in turn, related to lower stress (β = −0.209, 95% CI [−0.274, −0.144], SE = 0.033, t = −6.290, padjusted < 0.001), anxiety (β = −0.113, 95% CI [−0.180, −0.046], SE = 0.034, t = −3.314, padjusted = 0.002), and depression (β = −0.143, 95% CI [−0.207, −0.079], SE = 0.033, t = −4.393, padjusted < 0.001). A one standard deviation increase in stress was associated with a 17% greater likelihood of endorsing a higher frequency of sleep disturbances (OR = 1.168, 95% CI [1.026, 1.330], padjusted = 0.024), while equivalent increases in anxiety (OR = 1.602, 95% CI [1.394, 1.840], padjusted < 0.001) and depression (OR = 1.344, 95% CI [1.166, 1.549], padjusted < 0.001) were associated with 60% and 34% greater likelihood of sleep problem frequency, respectively.
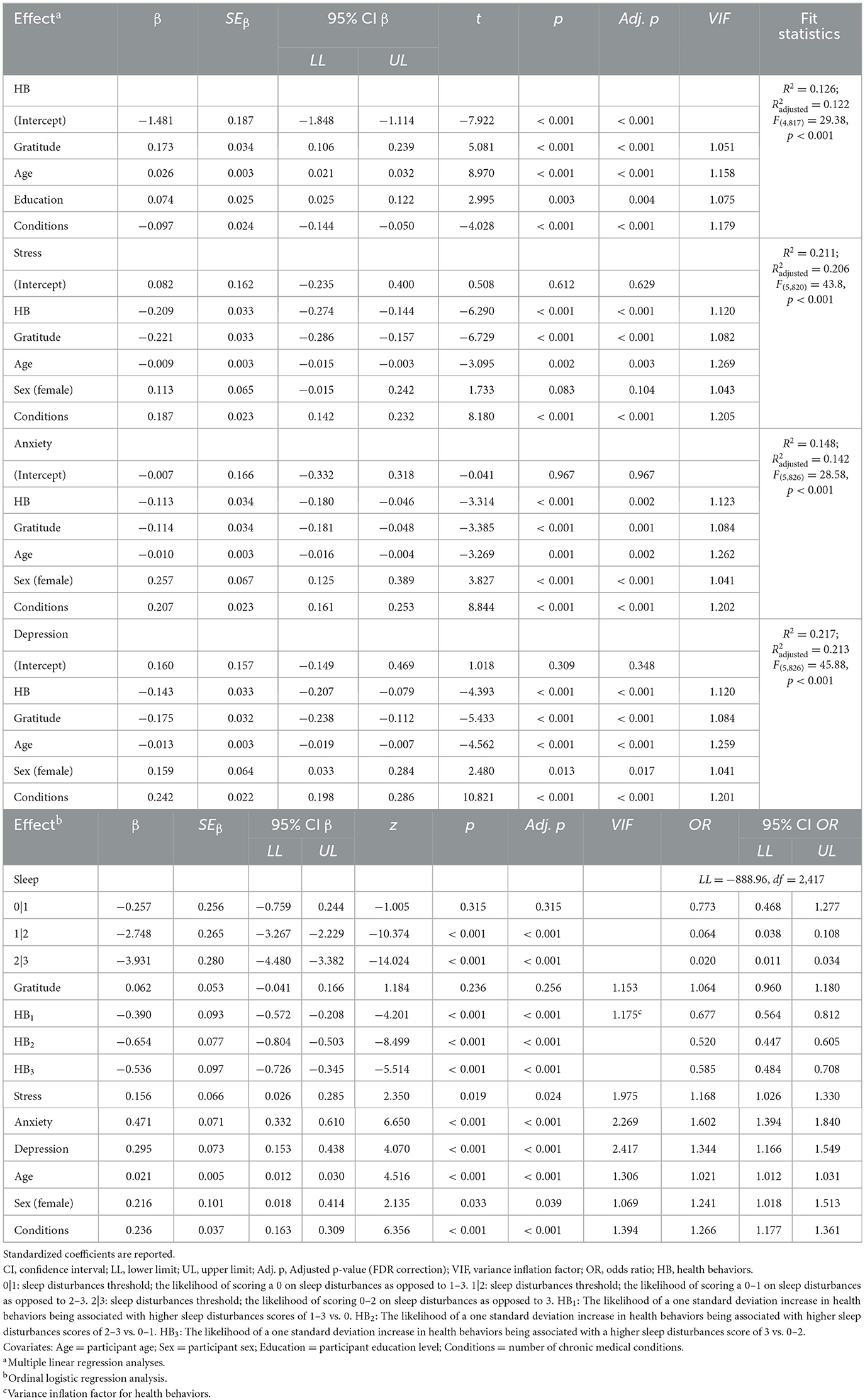
Table 5. Regression coefficients of serial indirect effects Model 2 for gratitude, health behaviors, psychological distress, and sleep disturbances, with covariates.
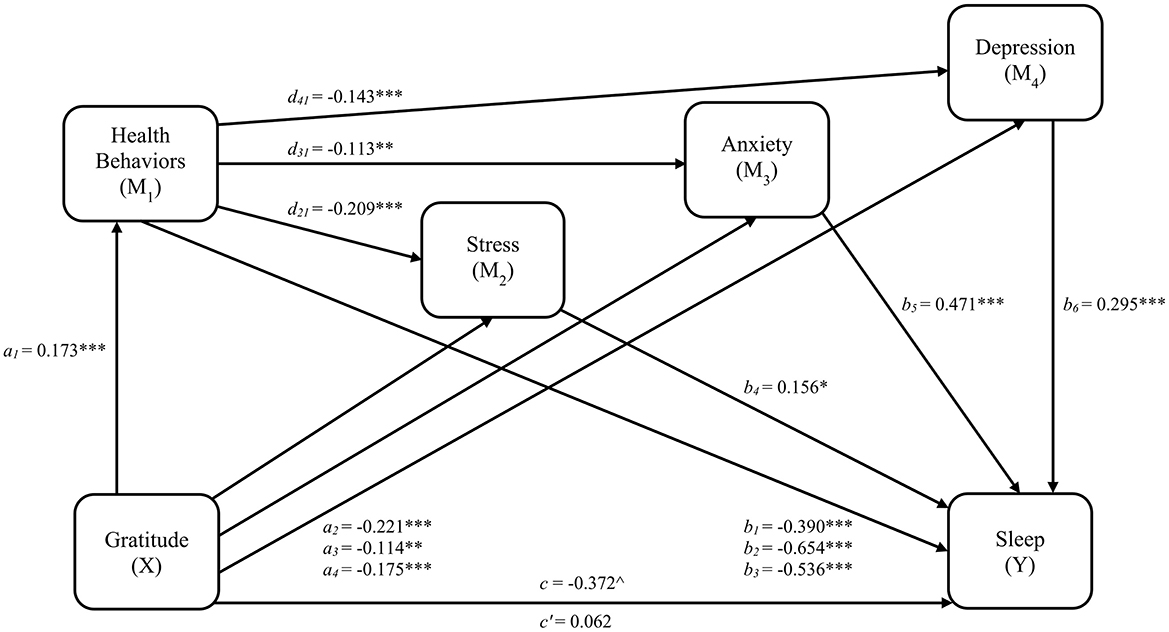
Figure 3. Serial indirect effects Model 2 for gratitude, health behaviors, psychological distress, and sleep disturbances. a1, a2, a3, a4 = regression coefficients for gratitude to health behaviors, stress, anxiety, and depression, respectively. b1, b2, b3 = regression coefficients for health behaviors to each threshold of sleep disturbances scores (0|1, 1|2, and 2|3, respectively). b4, b5, b6 = regression coefficients for stress, anxiety, and depression, respectively, to sleep disturbances. d21, d31, d41 = regression coefficients for health behaviors to stress, anxiety, and depression, respectively; c = total effect (gratitude related to sleep disturbances); c' = direct effect (gratitude related to sleep disturbances accounting for health behaviors and psychological distress). *p < 0.05; **p < 0.01; ***p < 0.001. p-values are FDR-adjusted. ∧Significance indicated by 95% CI that does not cross zero.
Mediation effect results for model 2 are provided in Table 6. Despite significant regression results, the multivariate hypothesis for model 2 was only partially supported. Serial mediation was observed through health behaviors as a first-order mediator, and anxiety (a1d31b5= −0.009, 95% CI [−0.019, −0.002], SE = 0.004) and depression (a1d41b6= −0.007, 95% CI [−0.016, −0.001], SE = 0.004), but not stress, as parallel second-order mediators. Additionally, specific indirect effects linking gratitude and sleep disturbances were observed for all three health behavior pathways, health behaviors1 (a1b1= −0.067, 95% CI [−0.120, −0.026], SE = 0.024), health behaviors2 (a1b2= −0.113, 95% CI [−0.180, −0.059], SE = 0.030), health behaviors3 (a1b3= −0.092, 95% CI [−0.158, −0.040], SE = 0.032), as well as anxiety (a3b5= −0.054, 95% CI [−0.104, −0.015], SE = 0.022) and depression (a4b6= −0.052, 95% CI [−0.103, −0.011], SE = 0.024). Overall, the total indirect effect (β = −0.435, 95% CI [−0.624, −0.268], SE = 0.093) and the total effect of gratitude on sleep disturbances (c = −0.372, 95% CI [−0.607, −0.146], SE = 0.115) were significant, while the direct effect was non-significant (c' = 0.062, 95% CI [−0.090, 0.209], SE = 0.076), indicating mediation. After adjusting the confidence intervals to 0.97 to account for false coverage rate correction, the conclusions regarding all indirect effects remained consistent.
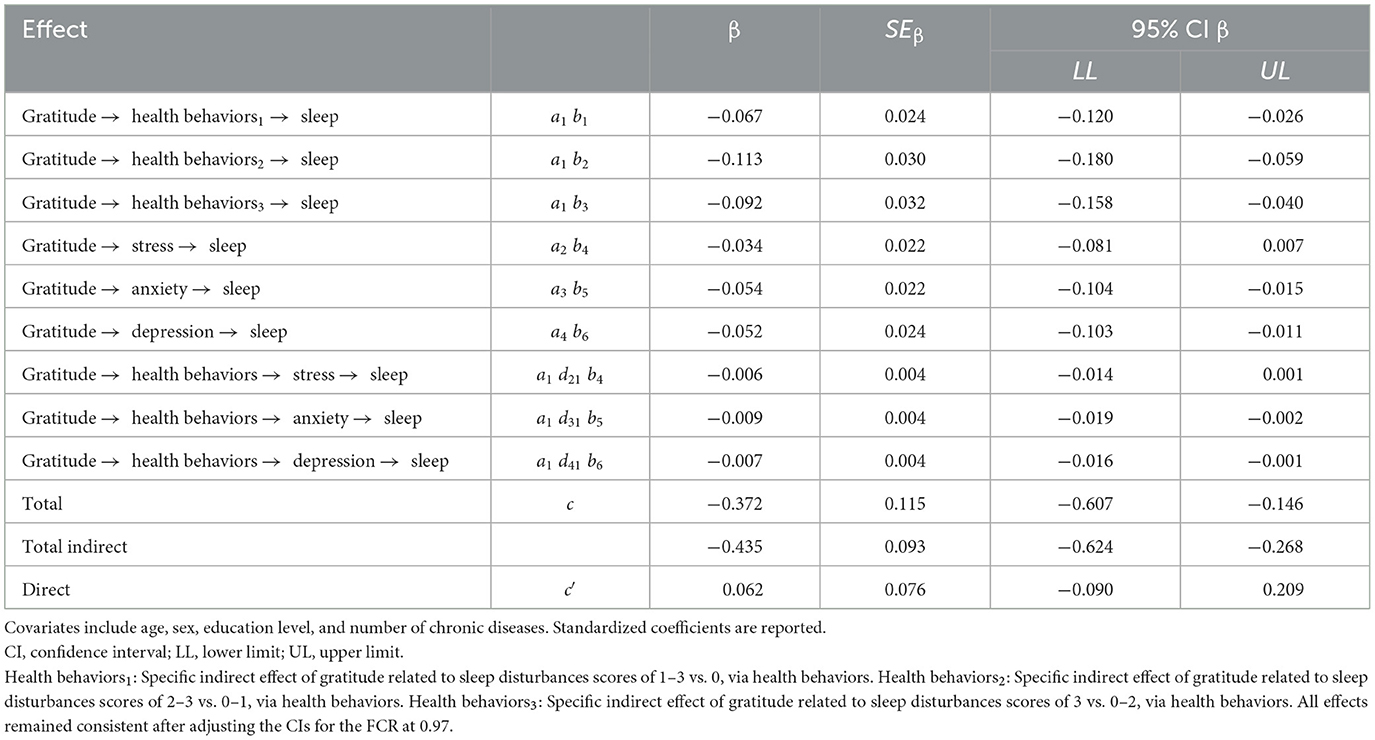
Table 6. Indirect effects of health behaviors and psychological distress on the relation between gratitude and sleep disturbances (Model 2).
3.2.3 Model 3
Regarding model 3, the ordinal logistic regression model fit the data significantly better than the multinomial model ( = 549.04, p ≤ 0.001) and was more parsimonious. However, the proportional odds assumption was violated for both health self-efficacy and health behaviors (HSE: = 6.990, p = 0.030; health behaviors: = 6.712, p = 0.035; both: = 10.397, p = 0.034). As all three models fit significantly better than the parallel model, the partial proportional odds model containing multiple slopes for both health self-efficacy and health behaviors was then compared to models containing multiple slopes for either health self-efficacy or health behaviors, to determine the most parsimonious model. The model including multiple slopes for both health self-efficacy and health behaviors did not fit the data significantly better than the health self-efficacy-only ( = 3.407, p = 0.182) or health behaviors-only ( = 3.685, p = 0.158) models. Next, the health self-efficacy-only and health behaviors-only models were compared. The health self-efficacy-only model fit better than the health behaviors-only model ( = 0.278, p < 0.001); thus, the health self-efficacy-only partial proportional odds model was used.
Linear and ordinal logistic regression results and fit statistics for each pathway, including significant covariates identified through backward stepwise selection, are provided in Table 7. Variance inflation factors are also provided in Table 7, and no predictors exceed the multicollinearity cutoff. Regression results excluding covariate effects are illustrated in Figure 4. Gratitude was related to better health self-efficacy (β = 0.273, 95% CI [0.209, 0.337], SE = 0.032, t = 8.412, padjusted < 0.001) which was, in turn, related to lower stress (β = −0.276, 95% CI [−0.350, −0.203], SE = 0.038, t = −7.352, padjusted < 0.001), anxiety (β = −0.202, 95% CI [−0.280, −0.123], SE = 0.040, t = −5.064, padjusted < 0.001), and depression (β = −0.230, 95% CI [−0.303, −0.157], SE = 0.037, t = −6.169, padjusted < 0.001). Gratitude was also related to better health behavior engagement (β = 0.173, 95% CI [0.106, 0.239], SE = 0.034, t = 5.081, padjusted < 0.001) which was, in turn, related to lower stress (β = −0.107, 95% CI [−0.177, −0.037], SE = 0.036, t = −3.001, padjusted = 0.005), but not anxiety and depression. A one standard deviation increase in stress was associated with a 17% greater likelihood of endorsing a higher frequency of sleep disturbances (OR = 1.168, 95% CI [1.023, 1.333], padjusted = 0.038), while equivalent increases in anxiety (OR = 1.602, 95% CI [1.394, 1.840], padjusted < 0.001) and depression (OR = 1.343, 95% CI [1.163, 1.551], padjusted < 0.001) were associated with 60% and 34% greater likelihood of sleep problem frequency, respectively.
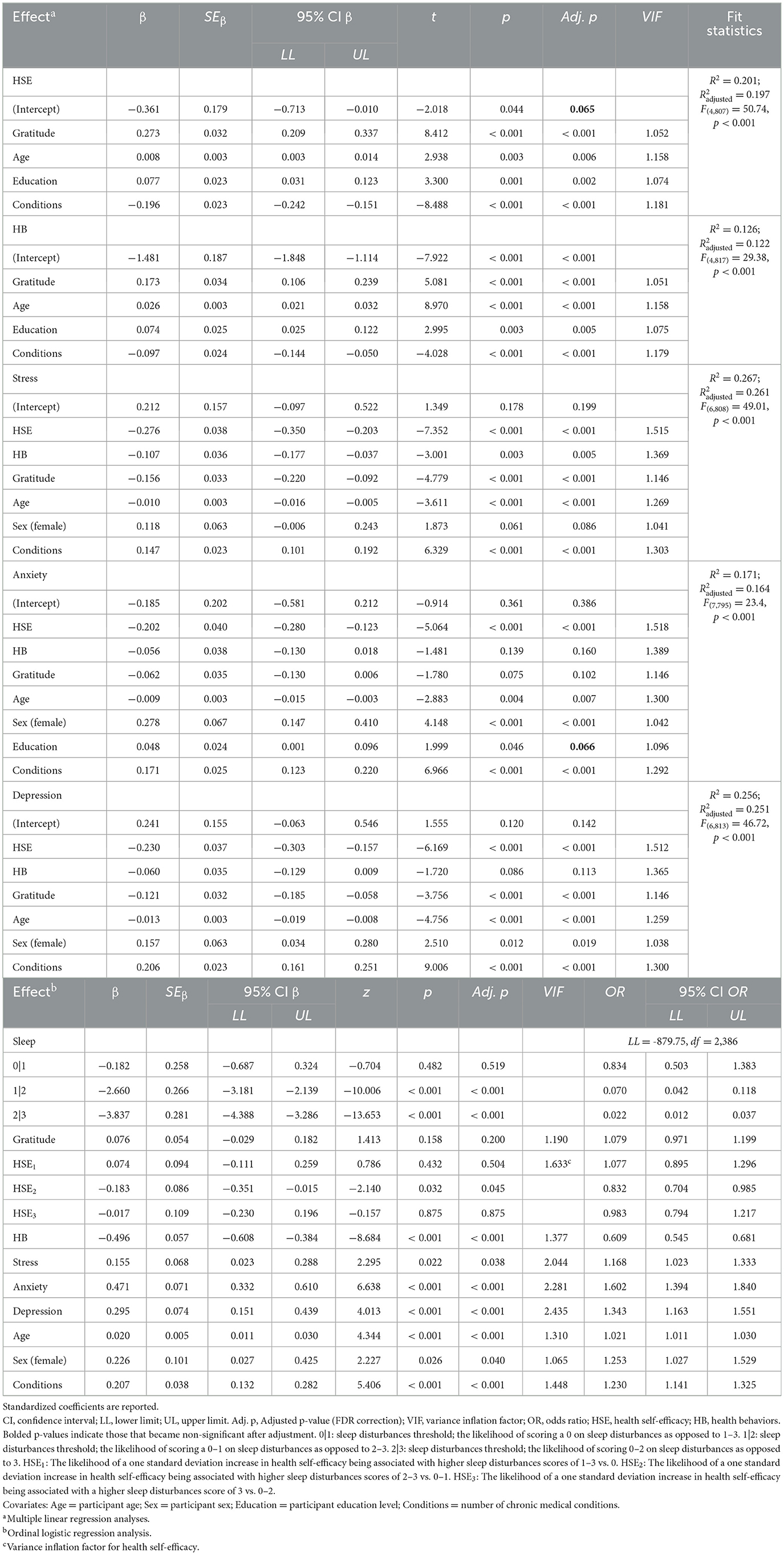
Table 7. Regression coefficients of serial indirect effects Model 3 for gratitude, health self-efficacy, health behaviors, psychological distress, and sleep disturbances, with covariates.

Figure 4. Serial indirect effects Model 3 for gratitude, health self-efficacy, health behaviors, psychological distress, and sleep disturbances. a1, a2, a3, a4, a5 = regression coefficients for gratitude to health self-efficacy, health behaviors, stress, anxiety, and depression, respectively. b1, b2, b3 = regression coefficients for health self-efficacy to each threshold of sleep disturbances scores (0|1, 1|2, and 2|3, respectively). b4, b5, b6, b7 = regression coefficients for health behaviors, stress, anxiety, and depression, respectively, to sleep disturbances. d31, d41, d51 = regression coefficients for health self-efficacy to stress, anxiety, and depression, respectively; d32, d42, d52 = regression coefficients for health behaviors to stress, anxiety, and depression, respectively; c = total effect (gratitude related to sleep disturbances); c' = direct effect (gratitude related to sleep disturbances accounting for health self-efficacy, health behaviors, and psychological distress).*p < 0.05; **p < 0.01; ***p < 0.001. p-values are FDR-adjusted. ∧Significance indicated by 95% CI that does not cross zero. #Indicates effect became non-significant after adjusting confidence interval to 97%.
Mediation effects results for model 3 are provided in Table 8. The multivariate hypothesis for model 3 was only partially supported. No serial mediation was found when health behaviors was included as a first-order mediator and, as a result, health self-efficacy and health behaviors did not function as parallel first-order mediators. Only health self-efficacy and anxiety (a1d41b6 = −0.026, 95% CI [−0.046, −0.009], SE = 0.009), and health self-efficacy and depression (a1d51b7 = −0.019, 95% CI [−0.037, −0.003], SE = 0.009), serially mediated the relation between gratitude and sleep disturbances. Specific indirect effects linking gratitude and sleep disturbances were observed for health behaviors (a2b4 = −0.086, 95% CI [−0.140, −0.030], SE = 0.026) and depression (a5b7= −0.036, 95% CI [−0.079, −0.005], SE = 0.019). Despite serial mediation occurring in only two of six potential paths, the sum of all indirect effects of gratitude on sleep disturbances via health self-efficacy, health behaviors, and psychological distress was significant (β = −0.276, 95% CI [−0.451, −0.053], SE = 0.093), as was the total effect (c = −0.200, 95% CI [−0.412, −0.001], SE = 0.105). The direct effect was non-significant (c' = 0.076, 95% CI [−0.078, 0.227], SE = 0.079), indicating mediation. After adjusting the confidence intervals to 0.97 to account for false coverage rate correction, the conclusions regarding all indirect effects remained consistent. However, the total effect of gratitude on sleep became non-significant after adjustment, indicating a suppression effect in which the positive direct and negative indirect effects cancel each other out (MacKinnon, 2000), and likely reflecting the lack of serial indirect effects for health behaviors.
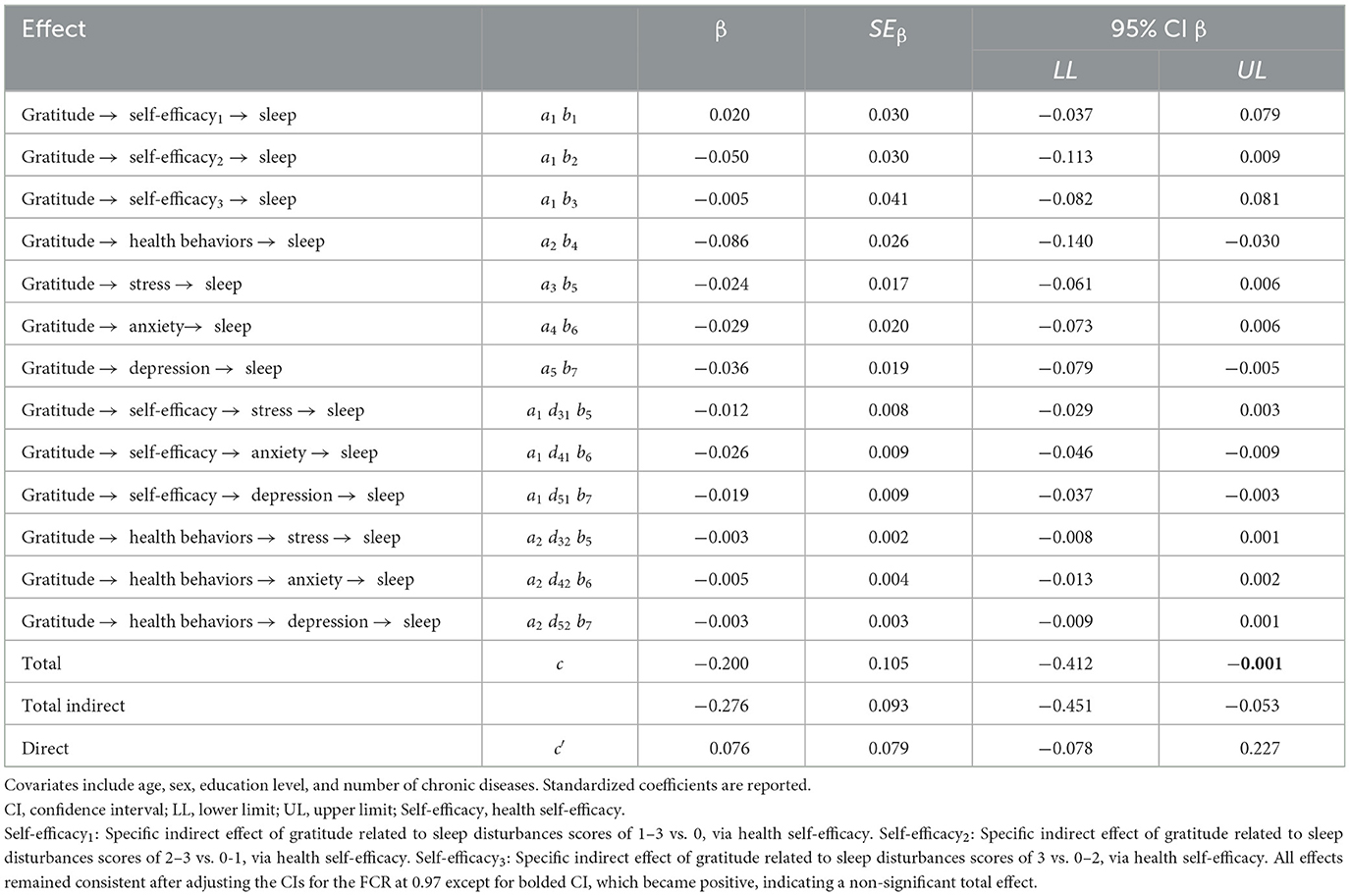
Table 8. Indirect effects of health self-efficacy, health behaviors, and psychological distress on the relation between gratitude and sleep disturbances (Model 3).
Finally, the results of our secondary SEM analyses provided additional support for our models, with modified models (i.e., dichotomized outcome, creation of psychological distress latent variable) exhibiting good fit and comparable patterns of direct and indirect effects. Please refer to Supplementary material for detailed results.
4 Discussion
In a sample of German primary care patients, we examined the potential serial mediating effects of health self-efficacy (HSE) and health behaviors as first-order mediators, and stress, anxiety, and depression as second-order mediators, on the relation between gratitude and sleep disturbances. Consistent with our theoretical model, in model 1, the serial mediation hypothesis was supported; gratitude was related to greater health self-efficacy and, in turn, to less stress, anxiety, and depression in parallel, with subsequent diminished sleep disturbances. However, in model 2, although gratitude was related to health behaviors, and health behaviors were related to stress, anxiety, and depression, the hypothesis was only partially supported, in that serial mediation was observed via health behaviors and anxiety and depression, but not via health behaviors and stress. In model 3, health self-efficacy and health behaviors did not function as parallel first-order mediators as hypothesized. Instead, serial mediation emerged in only two of six potential paths, through health self-efficacy and anxiety, and health self-efficacy and depression.
Support for our theoretical model arises from existing research outlining the benefits of gratitude for health self-efficacy and health behaviors. Gratitude is a pleasant emotion that, when evoked, facilitates the development of additional positive emotions (i.e., positive affect hypothesis; Wood et al., 2010), and the building of resources to be called upon during stressful times (i.e., broaden-and-build theory, Fredrickson, 2004; Wood et al., 2010), thereby contributing to health and wellbeing. Grateful individuals employ health-promoting behaviors as a positive coping strategy and are less likely to engage in maladaptive health behaviors, such as substance use, according to the coping hypothesis (Wood et al., 2007). Further, according to the cognitive framework, gratitude stimulates a positive perception of one's abilities, strengths, and circumstances, engagement in adaptive emotion regulation strategies, and a tendency to focus on and recall encouraging experiences which, in turn, enhances resilience against stress and improves psychological and physical wellbeing (Alkozei et al., 2018). Bandura's (1989) social cognitive theory describes self-efficacy as the belief in one's ability to control life circumstances, and health self-efficacy specifically refers to belief in ability to perform necessary behaviors to attain health goals (Sirois, 2007). Self-efficacy influences health behaviors through goals, perceptions of barriers and facilitators, and outcome expectations (Bandura, 2004). Experience with prior successes helps bolster belief in capability to exert control despite setbacks (Bandura, 1977, 2004); thus, gratitude's tendency to promote a positive perspective of capabilities and experiences may improve sense of control over health (Swain et al., 2020).
Gratitude can foster self-efficacy and mitigate psychological distress and sleep problems, consistent with the significant serial indirect effects findings of models 1 and 3. For example, among first-year U.S. undergraduates with high, but not low, gratitude levels, self-efficacy for COVID-19 safety predicted less depression after 2 months (Ang et al., 2022). Further, gratitude interventions increased self-efficacy and reduced perceptions of stress in German young adults (Lorenz et al., 2022), improved pain self-efficacy and pain-related anxiety in individuals with arthritis (Swain et al., 2020), and improved environmental mastery (i.e., perceived ability to effectively change surrounding circumstances and events; Ryff and Keyes, 1995), perceived stress, anxiety, depression, and insomnia in adults (Czyżowska and Gurba, 2022). Finally, in patients with asymptomatic heart failure, gratitude was related to greater self-efficacy to preserve heart function, less depression, better sleep, and lower levels of inflammatory markers (Mills et al., 2015).
Additionally, consistent with model 2's findings, engagement in adaptive health behaviors can positively impact psychological health and sleep (Su et al., 2021), and numerous studies offer support for gratitude's salubrious influence on these associations. In a global ecological momentary assessment study of adults (N = 4,825), greater gratitude was associated with increased exercise, lower blood pressure, heart rate, and stress, more daily positive expectations and reflections, and better sleep quality (Newman et al., 2021). Similarly, after a gratitude diary intervention, women reporting emotional distress and moderate sleep disturbances experienced more positive emotions, reduced blood pressure, and better sleep quality (Jackowska et al., 2016). In a large online survey of 59,985 respondents from ~160 countries, gratitude was associated with increased likelihood of engaging in healthy eating, social activities, self-care, and exercise, and reduced risk for smoking, depression, anxiety, poor physical health, and insufficient sleep (Weziak-Bialowolska et al., 2023). Finally, in a large multinational online survey of pregnant women, participants endorsing greater gratitude reported less detrimental impact of COVID-19 on diet, fitness, and sleep, and did not have anxiety or depression (Choi et al., 2022).
Importantly, it may be necessary to improve self-efficacy to affect positive changes in health behaviors, and health self-efficacy should be investigated as an antecedent to health behaviors in our model, rather than a parallel mechanism. There is some precedent for this assertion, which could explain the lack of parallel and serial indirect effects for health behaviors and substantiation of serial indirect effects for health self-efficacy in model 3. Rosenstock et al. (1988) revised the health belief model to incorporate self-efficacy, along with perceived benefits and barriers, perceived vulnerability to a severe health threat, and sufficient motivation or health concern, as important explanatory factors in predicting health-related behavior among individuals with chronic illnesses (Rosenstock, 1966). As an example, in a sample of Ukrainian primary care patients with both chronic kidney disease and hypertension, self-efficacy accounted for 76% of the variance in quality of life associated with health behaviors (i.e., physical activity, diet, stress management, smoking, medication adherence, blood pressure control; Korzh et al., 2022). Further, in German primary care patients with heart failure, low self-efficacy predicted both poor lifestyle and medication adherence (Eisele et al., 2020).
Given that affective traits are known to influence health behaviors, the self-regulation resource model posits that affective (i.e., high positive and low negative affect) and social-cognitive variables (i.e., self-efficacy) work in conjunction to bolster the self-regulation capacity needed to perform health-promoting behaviors (Sirois, 2015). Gratitude is one possible positive affective trait that can be drawn upon, alongside health self-efficacy, to facilitate behavior change (Klibert et al., 2019; Wood et al., 2010). Self-efficacy mediated the effect of gratitude on medication adherence in heart failure patients (Cousin et al., 2020), and, in a systematic review, gratitude for the medical team and patient's donor, and self-efficacy, emerged as the primary factors contributing to medical self-management among kidney transplant recipients (Jamieson et al., 2016).
Multiple patterns emerged across models that warrant further discussion. In model 2, health behaviors were an independent mediator at all severity levels of sleep disturbances whereas, in model 3, health behaviors were not a significant mediator in serial pathways but emerged as an independent mediator of the relation between gratitude and sleep disturbances. This pattern of findings indicates that there is a strong independent influence of health behaviors on sleep. Engagement in both positive and negative health behaviors can have direct effects on sleep. For example, caffeine use can increase arousal and disrupt sleep onset, duration, and efficiency, and quality of slow-wave sleep (Clark and Landolt, 2017). Similarly, cocaine and nicotine intoxication can impair REM sleep, sleep onset time, and sleep duration (Garcia and Salloum, 2015). On the other hand, physical exercise and weight control can directly improve sleep quality, efficiency, duration, and onset latency (Alfaris et al., 2015; Rogers et al., 2017). Other health behaviors, such as a healthy diet, can help to regulate circadian rhythms through nutrients that affect the release of hormones, such as melatonin, growth hormone, and serotonin (Vernia et al., 2021).
The final notable finding, across models, was that, although gratitude and the first-order mediators (i.e., M1; health self-efficacy and/or health behaviors) predicted greater reductions in stress than anxiety and depression, the effect of stress on sleep disturbances was weaker than the effects of anxiety and depression. As well, serial mediation for the stress pathway occurred only in model 1, which was focused on health self-efficacy. Thus, although the broaden-and-build theory (Fredrickson, 2004) indicates that gratitude, health self-efficacy, and health behavior engagement may lead to stress reduction, these salubrious effects are not transmitted to sleep, as with anxiety and depression, unless health behaviors are excluded from the model and only health self-efficacy is considered. Because biological stress is considered a significant contributor to the development of anxiety and depression (Ross et al., 2017), physiological stress and, as a result, perceived stress, may exacerbate anxiety and depression, rather than escalating concurrently.
Overall, our findings indicate that gratitude has a greater effect on psychological distress through health self-efficacy than through health behaviors, and that health self-efficacy is the primary mechanism through which gratitude predicts reductions in psychological distress and downstream sleep problems.
4.1 Limitations and directions for future research
It is important that our findings are interpreted within the context of several study limitations. To begin, this study's cross-sectional design precludes determinations of causality (O'Laughlin et al., 2018) and, thus, bidirectionality of variables is a possibility. First, sleep disturbances and depression are known to have a bidirectional association in primary care patients (Bouwmans et al., 2017). This may occur because, in the context of a maladaptive stress response, a persistent feedback loop of anxiety and depressive symptoms, and sleep problems, can manifest (Gold, 2015). Additionally, sleep is considered a health behavior that, independently and through its impact on other health behaviors, such as diet and exercise, contributes to the development and progression of depression (Dzierzewski et al., 2014; Lopresti et al., 2013).
In adults, anxiety and depressive disorders predict unfavorable health behaviors, such as smoking, low physical activity, and poor diet (Difrancesco et al., 2022; Gall et al., 2016; Walsh et al., 2023), and self-efficacy and smoking behavior may be bidirectional (Clyde et al., 2019). In sum, given the current study's cross-sectional, survey-based design, future randomized controlled trials in which study variables are manipulated and prospective, longitudinal studies may help to elucidate these linkages.
Further, the use of self-report measures may limit external validity, as responses are affected by participants' understanding of the items, level of personal insight, and potential social desirability and response biases (Demetriou et al., 2015). Future studies should employ objective or physiological assessments, such as medical record reviews, actigraphy, polysomnography, and ecological momentary assessment, to improve validity (Jackson et al., 2018; Prince et al., 2020; Scarlett et al., 2021). Relatedly, the outcome variable of sleep disturbances was measured using only one item, item 3 of the PHQ-9, which precludes estimates of internal consistency and may not adequately capture a construct as multifaceted as sleep disturbances (Allen et al., 2022). However, this item has been validated in primary care patients as a brief screening tool for sleep disturbances (MacGregor et al., 2012). In future studies, utilizing a multidimensional measure, such as the Pittsburgh Sleep Quality Index (Buysse et al., 1989), may enhance reliability and validity and allow for the use of SEM or ordinary least squares regression at each stage of the model, simplifying interpretation of the regression results and potentially reducing measurement error.
Notably, as most participants (58%) reported zero or one medical condition, the results may not fully capture the experiences of individuals with multimorbidity. Nearly 40% of German adults experience multimorbidity (i.e., have two or more chronic medical conditions simultaneously), including half of adults between 50 and 59 years old, and 47% of adults between 40 and 49 years of age with low education levels (Puth et al., 2017). More chronic conditions predict development of stress, anxiety, and depression in representative population-based samples (Hajek and König, 2020; Liu et al., 2021), and sleep disturbances in primary care patients (Ullmann et al., 2022). Number of chronic diseases was covaried in all analyses and emerged as a significant predictor on almost all pathways of every model.
Finally, race and ethnicity statistics are not collected in German studies due to legal prohibitions and political factors, thus precluding inferences of generalizability for these demographic factors. Yet, it is likely that disparities exist, based on immigration research findings indicating that first-generation migrants in Germany have significantly higher rates of depression and generalized anxiety (Beutel et al., 2016). Future research conducted with additional demographic groups, chronic disease populations (e.g., cardiovascular, rheumatological, neurodegenerative), and sleep disorder populations (e.g., insomnia, sleep apnea, narcolepsy) is needed to improve generalizability and substantiate our findings across diverse groups.
4.2 Implications
Despite limitations, this study's novel findings may help to inform the selection of targeted clinical interventions to improve sleep in primary care patients. To begin, self-management interventions are effective for improving gratitude, health behaviors, self-efficacy, psychological distress, and sleep, including in individuals living with cancer (Martin et al., 2020), sedentary European adults with insomnia (Hartescu et al., 2015), and primary care patients from 10 practices in Germany (Zimmermann et al., 2016) and enrolled in a global cardiovascular risk reduction program (Prince et al., 2017). Importantly, according to a systematic review, to promote health self-efficacy, successful self-management programs in primary care should be tailored to meet individual needs, and should include independent symptom monitoring with self-treatment, regular communication with one's provider, stress management and coping strategies for addressing psychological distress, and promotion of responsibility for health behavior choices (Dineen-Griffin et al., 2019).
Further, systematic reviews and meta-analyses indicate beneficial effects of gratitude interventions for self-efficacy (Grant and Gino, 2010), stress, anxiety, and depression (Carr et al., 2021; Cregg and Cheavens, 2021), and subjective sleep quality (Boggiss et al., 2020). In a systematic review of positive psychological interventions (PPIs) in which 16 of 27 studies included gratitude-specific exercises, PPIs were responsible for favorable effects on health behaviors (Feig et al., 2022). Additional evidence-based interventions that may improve self-efficacy, health behaviors, psychological distress, and sleep disturbance include cognitive behavioral therapy (e.g., changing maladaptive thoughts to alter emotional responses) and acceptance and commitment therapy (e.g., fostering present-moment awareness, acceptance, and values-driven behavior), which can be efficaciously implemented in primary care settings (Arnold et al., 2022; Benninghoven et al., 2022; Hopko et al., 2009; Jonkers et al., 2012; Siengsukon et al., 2020). Behavioral activation for depression (i.e., identifying and intentionally scheduling enjoyable activities), a component of cognitive behavioral therapy, is particularly well-suited to cultivating engagement in salubrious behaviors, such as reducing problem drinking, facilitating smoking cessation, and improving physical activity and depression (May et al., 2024). In sum, as psychological distress and sleep disturbances are most often identified in primary care populations, providers have an opportunity to facilitate the initial catalyst of advantageous downstream effects that begins with promotion of gratitude.
4.3 Conclusion
In a sample of German primary care patients, health self-efficacy as a first-order mediator, and stress, anxiety, and depression, as parallel second-order mediators, serially mediated the relation between gratitude and sleep disturbances. In addition, health behaviors, and anxiety and depressive symptoms, functioned as serial mediators of the gratitude-sleep linkage. Finally, we found that health self-efficacy and health behaviors were not parallel first-order mediators, and only health self-efficacy and anxiety, and health self-efficacy and depression, serially mediated the relation between gratitude and sleep disturbances. Future prospective research utilizing objective assessments and across diverse samples is needed to substantiate these findings. However, despite limitations, this study provides preliminary support for the role of gratitude as a catalyst for health self-efficacy and health behaviors and, in turn, for its beneficial influence on psychological distress and sleep disturbances.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Commission of the Faculty of Medicine at the Ludwig Maximilian University of Munich. The studies were conducted in accordance with the local legislation and institutional requirements. The Ethics Committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin because participation was voluntary and, to ensure privacy, no personally identifiable information was obtained.
Author contributions
HA: Conceptualization, Data curation, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. JH: Conceptualization, Data curation, Methodology, Supervision, Validation, Writing – review & editing. AW: Conceptualization, Investigation, Project administration, Writing – review & editing, Data curation. NK: Conceptualization, Investigation, Project administration, Resources, Supervision, Writing – review & editing, Methodology. JS: Conceptualization, Investigation, Project administration, Resources, Supervision, Writing – review & editing. LT: Conceptualization, Methodology, Writing – review & editing. FS: Conceptualization, Methodology, Writing – review & editing. MO: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frsle.2025.1459854/full#supplementary-material
References
Åkerstedt, T., Narusyte, J., Alexanderson, K., and Svedberg, P. (2017). Sleep duration, mortality, and heredity—A prospective twin study. Sleep. 40:zsx135. doi: 10.1093/sleep/zsx135
Aernout, E., Benradia, I., Hazo, J.-B., Sy, A., Askevis-Leherpeux, F., Sebbane, D., et al. (2021). International study of the prevalence and factors associated with insomnia in the general population. Sleep Med. 82, 186–192. doi: 10.1016/j.sleep.2021.03.028
Akinwande, M. O., Dikko, H. G., and Samson, A. (2015). Variance inflation factor: As a condition for the inclusion of suppressor variable(s) in regression analysis. OJS 5, 754–767. doi: 10.4236/ojs.2015.57075
Alfaris, N., Wadden, T. A., Sarwer, D. B., Diwald, L., Volger, S., Hong, P., et al. (2015). Effects of a 2-year behavioral weight loss intervention on sleep and mood in obese individuals treated in primary care practice. Obesity 23, 558–564. doi: 10.1002/oby.20996
Alkozei, A., Smith, R., and Killgore, W. D. S. (2018). Gratitude and subjective wellbeing: a proposal of two causal frameworks. J. Happiness Stud. 19, 1519–1542. doi: 10.1007/s10902-017-9870-1
Alkozei, A., Smith, R., Kotzin, M. D., Waugaman, D. L., and Killgore, W. D. S. (2019). The association between trait gratitude and self-reported sleep quality is mediated by depressive mood state. Behav. Sleep Med. 17, 41–48. doi: 10.1080/15402002.2016.1276017
Allen, M. S., Iliescu, D., and Greiff, S. (2022). Single item measures in psychological science: a call to action. Eur. J. Psychol. Assess. 38, 1–5. doi: 10.1027/1015-5759/a000699
Ang, J. Y.-Z., Monte, V., and Tsai, W. (2022). First-year college students' adjustment during the COVID-19 pandemic: the protective roles of hope and gratitude. Transl. Issues Psychol. Sci. 8, 375–388. doi: 10.1037/tps0000320
Arnold, T., Haubrick, K. K., Klasko-Foster, L. B., Rogers, B. G., Barnett, A., Ramirez- Sanchez, N. A., et al. (2022). Acceptance and commitment therapy informed behavioral health interventions delivered by non-mental health professionals: a systematic review. J. Context. Behav. Sci. 24, 185–196. doi: 10.1016/j.jcbs.2022.05.005
Arroll, B., Fernando, A., Falloon, K., Goodyear-Smith, F., Samaranayake, C., and Warman, G. (2012). Prevalence of causes of insomnia in primary care: a cross-sectional study. Br. J. Gen. Pract. 62, e99–e103. doi: 10.3399/bjgp12X625157
Bandura, A. (1977). Self-efficacy: toward a unifying theory of behavioral change. Psychol. Rev. 84, 191–215. doi: 10.1037//0033-295X.84.2.191
Bandura, A. (1989). “Social cognitive theory,” in Annals of Child Development, ed. R. Vasta (Greenwich, CT: JAI Press), 1–60.
Bandura, A. (2004). Health promotion by social cognitive means. Health Educ. Behav. 31, 143–164. doi: 10.1177/1090198104263660
Benjamini, Y., and Hochberg, Y. (1995). Controlling the false discovery rate: a practical and powerful approach to multiple testing. J. R. Stat. Soc. Series B Stat. Methodol. 57, 289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x
Benjamini, Y., and Yekutieli, D. (2005). False discovery rate–adjusted multiple confidence intervals for selected parameters. J. Am. Stat. Assoc. 100, 71–81. doi: 10.1198/016214504000001907
Benninghoven, D., Menke, E., China, C., Schroeder, F., and Bethge, M. (2022). Implementation of a behavioral medicine-oriented concept in cardiological rehabilitation. Psychother. Psychosom. Med. Psychol. 72, 429–437. doi: 10.1055/a-1749-6379
Beutel, M. E., Jünger, C., Klein, E. M., Wild, P., Lackner, K. J., Blettner, M., et al. (2016). Depression, anxiety and suicidal ideation among 1st and 2nd generation migrants – Results from the Gutenberg health study. BMC Psychiatry 16:288. doi: 10.1186/s12888-016-0995-2
Bluestein, D., Rutledge, C. M., and Healey, A. C. (2010). Psychosocial correlates of insomnia severity in primary care. J. Am. Board Fam. Med. 23, 204–211. doi: 10.3122/jabfm.2010.02.090179
Boggero, I. A., Hostinar, C. E., Haak, E. A., Murphy, M. L. M., and Segerstrom, S. C. (2017). Psychosocial functioning and the cortisol awakening response: meta-analysis, P-curve analysis, and evaluation of the evidential value in existing studies. Biol. Psychol. 129, 207–230. doi: 10.1016/j.biopsycho.2017.08.058
Boggiss, A. L., Consedine, N. S., Brenton-Peters, J. M., Hofman, P. L., and Serlachius, A. S. (2020). A systematic review of gratitude interventions: effects on physical health and health behaviors. J. Psychosom. Res. 135:110165. doi: 10.1016/j.jpsychores.2020.110165
Bouwmans, M. E. J., Conradi, H. J., Bos, E. H., Oldehinkel, A. J., and De Jonge, P. (2017). Bidirectionality between sleep symptoms and core depressive symptoms and their long-term course in major depression. Psychosom. Med. 79, 336–344. doi: 10.1097/PSY.0000000000000407
Buysse, D. J., Reynolds, C. F., Monk, T. H., Berman, S. R., and Kupfer, D. J. (1989). The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 28, 193–213. doi: 10.1016/0165-1781(89)90047-4
Card, N. A. (2019). Meta-analyses of the reliabilities of four measures of gratitude. J. Posit. Psychol. 14, 576–586. doi: 10.1080/17439760.2018.1497690
Carr, A., Cullen, K., Keeney, C., Canning, C., Mooney, O., Chinseallaigh, E., et al. (2021). Effectiveness of positive psychology interventions: a systematic review and meta-analysis. J. Posit. Psychol. 16, 749–769. doi: 10.1080/17439760.2020.1818807
Chattu, V. K., Md Manzar, D., Kumary, S., Burman, D., Spence, D. W., and Pandi-Perumal, S. R. (2018). The global problem of insufficient sleep and its serious public health implications. Healthcare 7:1. doi: 10.3390/healthcare7010001
Choi, K. W., Kim, H. H., Basu, A., Kwong, A. S. F., Hernandez-Diaz, S., Wyszynski, D. F., et al. (2022). COVID-19 perceived impacts on sleep, fitness, and diet and associations with mental health during pregnancy: a cross-national study. J. Affect. Disord. Rep. 7:100288. doi: 10.1016/j.jadr.2021.100288
Clark, I., and Landolt, H. P. (2017). Coffee, caffeine, and sleep: a systematic review of epidemiological studies and randomized controlled trials. Sleep Med. Rev. 31, 70–78. doi: 10.1016/j.smrv.2016.01.006
Clyde, M., Pipe, A., Reid, R., Els, C., and Tulloch, H. (2019). A bidirectional path analysis model of smoking cessation self-efficacy and concurrent smoking status: impact on abstinence outcomes. Addict. Biol. 24, 1034–1043. doi: 10.1111/adb.12647
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. Health Soc. Behav. 24:385. doi: 10.2307/2136404
Cohen, S., and Williamson, G. (1988). “Perceived stress in a probability sample of the United States,” in The Social Psychology of Health, eds. S. Spacapan and S. Oskamp (Newbury Park, CA: Sage Publications, Inc.), 31–67.
Cousin, L., Buck, H., Benitez, B., Mills, P., and Redwine, L. (2020). A structural equation model of gratitude, self-efficacy, and medication adherence in patients with stage B heart failure. J. Cardiovasc. Nurs. 35, E18–E24. doi: 10.1097/JCN.0000000000000721
Cousin, L., Redwine, L., Bricker, C., Kip, K., and Buck, H. (2021). Effect of gratitude on cardiovascular health outcomes: a state-of-the-science review. J. Posit. Psychol. 16, 348–355. doi: 10.1080/17439760.2020.1716054
Cregg, D. R., and Cheavens, J. S. (2021). Gratitude interventions: effective self-help? A meta-analysis of the impact on symptoms of depression and anxiety. J. Happiness Stud. 22, 413–445. doi: 10.1007/s10902-020-00236-6
Czyżowska, N., and Gurba, E. (2022). Enhancing meaning in life and psychological well-being among a European cohort of young adults via a gratitude intervention. Front. Psychol. 12:751081. doi: 10.3389/fpsyg.2021.751081
Demetriou, C., Ozer, B. U., and Essau, C. A. (2015). “Self-report questionnaires,” in The Encyclopedia of Clinical Psychology, eds. R. L. Cautin and S. O. Lilienfeld (Wiley), 1–6. doi: 10.1002/9781118625392.wbecp507
Demyttenaere, K., and Heirman, E. (2020). The blurred line between anxiety and depression: hesitations on comorbidity, thresholds and hierarchy. Int. Rev. Psychiatry 32, 455–465. doi: 10.1080/09540261.2020.1764509
Difrancesco, S., Penninx, B. W. J. H., Merikangas, K. R., Van Hemert, A. M., Riese, H., and Lamers, F. (2022). Within-day bidirectional associations between physical activity and affect: a real-time ambulatory study in persons with and without depressive and anxiety disorders. Depres. Anxiety 39, 922–931. doi: 10.1002/da.23298
Dineen-Griffin, S., Garcia-Cardenas, V., Williams, K., and Benrimoj, S. I. (2019). Helping patients help themselves: a systematic review of self-management support strategies in primary health care practice. PLoS ONE 14:e0220116. doi: 10.1371/journal.pone.0220116
DuBois, C. M., Millstein, R. A., Celano, C. M., Wexler, D. J., and Huffman, J. C. (2016). Feasibility and acceptability of a positive psychological intervention for patients with type 2 diabetes. Prim. Care Companion CNS Disord. 18:10.4088/PCC.15m01902. doi: 10.4088/PCC.15m01902
Dzierzewski, J. M., Buman, M. P., Giacobbi, P. R., Roberts, B. L., Aiken-Morgan, A. T., Marsiske, M., et al. (2014). Exercise and sleep in community-dwelling older adults: evidence for a reciprocal relationship. J. Sleep Res. 23, 61–68. doi: 10.1111/jsr.12078
Eisele, M., Harder, M., Rakebrandt, A., Boczor, S., Marx, G., Blozik, E., et al. (2020). Association of depression and anxiety with adherence in primary care patients with heart failure—cross-sectional results of the observational RECODE-HF cohort study. Fam. Pract. 37, 695–702. doi: 10.1093/fampra/cmaa042
Feig, E. H., Madva, E. N., Millstein, R. A., Zambrano, J., Amonoo, H. L., Longley, R. M., et al. (2022). Can positive psychological interventions improve health behaviors? A systematic review of the literature. Prev. Med. 163:107214. doi: 10.1016/j.ypmed.2022.107214
Ford, E. S., Wheaton, A. G., Cunningham, T. J., Giles, W. H., Chapman, D. P., and Croft, J. B. (2014). Trends in outpatient visits for insomnia, sleep apnea, and prescriptions for sleep medications among US adults: findings from the National Ambulatory Medical Care Survey 1999-2010. Sleep 37, 1283–1293. doi: 10.5665/sleep.3914
Fox, J., and Weisberg, S. (2019). An R Companion to Applied Regression. 3rd Edn. Thousand Oaks, CA: Sage.
Fredrickson, B. L. (2004). “Gratitude, like other positive emotions, broadens and builds,” in The Psychology of Gratitude, eds. R. A. Emmons and M. E. McCullough (New York, NY: Oxford University Press), 144–166.
Gall, S. L., Sanderson, K., Smith, K. J., Patton, G., Dwyer, T., and Venn, A. (2016). Bi-directional associations between healthy lifestyles and mood disorders in young adults: The Childhood Determinants of Adult Health Study. Psychol. Med. 46, 2535–2548. doi: 10.1017/S0033291716000738
Garcia, A. N., and Salloum, I. M. (2015). Polysomnographic sleep disturbances in nicotine, caffeine, alcohol, cocaine, opioid, and cannabis use: a focused review. Am. J. Addict. 24, 590–598. doi: 10.1111/ajad.12291
Gili, M., Comas, A., García-García, M., Monzón, S., Antoni, S.-B., and Roca, M. (2010). Comorbidity between common mental disorders and chronic somatic diseases in primary care patients. Gen. Hosp. Psychiatry 32, 240–245. doi: 10.1016/j.genhosppsych.2010.01.013
Gold, P. W. (2015). The organization of the stress system and its dysregulation in depressive illness. Mol. Psychiatry 20, 32–47. doi: 10.1038/mp.2014.163
Gräfe, K., Zipfel, S., Herzog, W., and Löwe, B. (2004). Screening psychischer Störungen mit dem “Gesundheitsfragebogen für patienten (PHQ-D)”. Diagnostica 50, 171–181. doi: 10.1026/0012-1924.50.4.171
Grant, A. M., and Gino, F. (2010). A little thanks goes a long way: explaining why gratitude expressions motivate prosocial behavior. J. Pers. Soc. Psychol. 98, 946–955. doi: 10.1037/a0017935
Hair, J. F., Risher, J. J., Sarstedt, M., and Ringle, C. M. (2019). When to use and how to report the results of PLS-SEM. EBR 31, 2–24. doi: 10.1108/EBR-11-2018-0203
Hajek, A., and König, H.-H. (2020). Prevalence and correlates of individuals screening positive for depression and anxiety on the PHQ-4 in the German general population: Findings from the nationally representative German Socio-Economic Panel (GSOEP). IJERPH 17:7865. doi: 10.3390/ijerph17217865
Hale, L., Troxel, W., and Buysse, D. J. (2020). Sleep health: an opportunity for public health to address health equity. Annu. Rev. Public Health 41, 81–99. doi: 10.1146/annurev-publhealth-040119-094412
Hartescu, I., Morgan, K., and Stevinson, C. D. (2015). Increased physical activity improves sleep and mood outcomes in inactive people with insomnia: a randomized controlled trial. J. Sleep Res. 24, 526–534. doi: 10.1111/jsr.12297
Heckendorf, H., Lehr, D., Ebert, D. D., and Freund, H. (2019). Efficacy of an internet and app-based gratitude intervention in reducing repetitive negative thinking and mechanisms of change in the intervention's effect on anxiety and depression: results from a randomized controlled trial. Behav. Res. Ther. 119:103415. doi: 10.1016/j.brat.2019.103415
Hinz, A., Klein, A. M., Brähler, E., Glaesmer, H., Luck, T., Riedel-Heller, S. G., et al. (2017). Psychometric evaluation of the Generalized Anxiety Disorder Screener GAD-7, based on a large German general population sample. J. Affect. Disord. 210, 338–344. doi: 10.1016/j.jad.2016.12.012
Hirsch, J. K., Altier, H. R., Offenbächer, M., Toussaint, L., Kohls, N., and Sirois, F. M. (2021). Positive psychological factors and impairment in rheumatic and musculoskeletal disease: do psychopathology and sleep quality explain the linkage? Arthr. Care Res. 73, 55–64. doi: 10.1002/acr.24440
Hopko, D. R., Robertson, S. M. C., and Carvalho, J. P. (2009). Sudden gains in depressed cancer patients treated with behavioral activation therapy. Behav. Ther. 40, 346–356. doi: 10.1016/j.beth.2008.09.001
Hughes, A. J., Dunn, K. M., Chaffee, T., Bhattarai, J., and Beier, M. (2018). Diagnostic and clinical utility of the GAD-2 for screening anxiety symptoms in individuals with multiple sclerosis. Arch. Phys. Med. Rehabil. 99, 2045–2049. doi: 10.1016/j.apmr.2018.05.029
Hunter, C. L., and American Psychological Association, eds. (2009). Integrated Behavioral Health in Primary Care: Step-By-Step Guidance for Assessment and Intervention, 1st Ed. Washington, DC: American Psychological Association.
Irwin, M. R., Olmstead, R., and Carroll, J. E. (2016). Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Bio. Psychiatry 80, 40–52. doi: 10.1016/j.biopsych.2015.05.014
Jackowska, M., Brown, J., Ronaldson, A., and Steptoe, A. (2016). The impact of a brief gratitude intervention on subjective well-being, biology and sleep. J. Health Psychol. 21, 2207–2217. doi: 10.1177/1359105315572455
Jackson, C. L., Patel, S. R., Jackson, W. B., Lutsey, P. L., and Redline, S. (2018). Agreement between self-reported and objectively measured sleep duration among white, black, Hispanic, and Chinese adults in the United States: multi-ethnic study of atherosclerosis. Sleep 41:zsy057. doi: 10.1093/sleep/zsy057
Jamieson, N. J., Hanson, C. S., Josephson, M. A., Gordon, E. J., Craig, J. C., Halleck, F., et al. (2016). Motivations, challenges, and attitudes to self-management in kidney transplant recipients: a systematic review of qualitative studies. Am. J. Kid. Dis. 67, 461–478. doi: 10.1053/j.ajkd.2015.07.030
Jonkers, C. C. M., Lamers, F., Bosma, H., Metsemakers, J. F. M., and Van Eijk, J. Th. M. (2012). The effectiveness of a minimal psychological intervention on self-management beliefs and behaviors in depressed chronically ill elderly persons: a randomized trial. Int. Psychogeriatr. 24, 288–297. doi: 10.1017/S1041610211001748
Kalmbach, D. A., Anderson, J. R., and Drake, C. L. (2018). The impact of stress on sleep: pathogenic sleep reactivity as a vulnerability to insomnia and circadian disorders. J. Sleep Res. 27:e12710. doi: 10.1111/jsr.12710
Kanagasabai, T., and Chaput, J.-P. (2017). Sleep duration and the associated cardiometabolic risk scores in adults. Sleep Health 3, 195–203. doi: 10.1016/j.sleh.2017.03.006
Karing, C. (2021). Prevalence and predictors of anxiety, depression and stress among university students during the period of the first lockdown in Germany. J. Affect. Disord. Rep. 5:100174. doi: 10.1016/j.jadr.2021.100174
Klibert, J., Rochani, H., Samawi, H., Leleux-LaBarge, K., and Ryan, R. (2019). The impact of an integrated gratitude intervention on positive affect and coping resources. Int. J. Appl. Posit. Psychol. 3, 23–41. doi: 10.1007/s41042-019-00015-6
Korzh, O., Titkova, A., Fylenko, Y., and Lavrova, Y. (2022). Evaluation of health-promoting self-care behaviors in hypertensive patients with concomitant chronic kidney disease in primary care. Prim. Health Care Res. Dev. 23:e48. doi: 10.1017/S1463423622000299
Kroenke, K., Spitzer, R. L., and Williams, J. B. W. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Kroenke, K., Spitzer, R. L., and Williams, J. B. W. (2003). The patient health questionnaire-2: validity of a two-item depression screener. Med. Care 41, 1284–1292. doi: 10.1097/01.MLR.0000093487.78664.3C
Kroenke, K., Spitzer, R. L., Williams, J. B. W., Monahan, P. O., and Löwe, B. (2007). Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann. Intern. Med. 146:317. doi: 10.7326/0003-4819-146-5-200703060-00004
Léger, D., Partinen, M., Hirshkowitz, M., Chokroverty, S., and Hedner, J. (2010). Characteristics of insomnia in a primary care setting: EQUINOX survey of 5293 insomniacs from 10 countries. Sleep Med. 11, 987–998. doi: 10.1016/j.sleep.2010.04.019
Legler, S. R., Beale, E. E., Celano, C. M., Beach, S. R., Healy, B. C., and Huffman, J. C. (2019). State gratitude for one's life and health after an acute coronary syndrome: prospective associations with physical activity, medical adherence and re-hospitalizations. J. Posit. Psychol. 14, 283–291. doi: 10.1080/17439760.2017.1414295
Liu, X., Cao, H., Zhu, H., Zhang, H., Niu, K., Tang, N., et al. (2021). Association of chronic diseases with depression, anxiety and stress in Chinese general population: the CHCN-BTH cohort study. J. Affect. Disord. 282, 1278–1287. doi: 10.1016/j.jad.2021.01.040
Lopresti, A. L., Hood, S. D., and Drummond, P. D. (2013). A review of lifestyle factors that contribute to important pathways associated with major depression: diet, sleep and exercise. J. Affect. Disord. 148, 12–27. doi: 10.1016/j.jad.2013.01.014
Lorenz, T., Algner, M., and Binder, B. (2022). A positive psychology resource for students? Evaluation of the effectiveness of the 6 minutes diary in a randomized control trial. Front. Psychol. 13:896741. doi: 10.3389/fpsyg.2022.896741
Löwe, B., Decker, O., Müller, S., Brähler, E., Schellberg, D., Herzog, W., et al. (2008). Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med. Care 46, 266–274. Available online at: http://www.jstor.org/stable/40221654
Löwe, B., Kroenke, K., and Gräfe, K. (2005). Detecting and monitoring depression with a two-item questionnaire (PHQ-2). J. Psychosom. Res. 58, 163–171. doi: 10.1016/j.jpsychores.2004.09.006
MacGregor, K. L., Funderburk, J. S., Pigeon, W., and Maisto, S. A. (2012). Evaluation of the PHQ-9 item 3 as a screen for sleep disturbance in primary care. J. Gen. Intern. Med. 27, 339–344. doi: 10.1007/s11606-011-1884-5
MacKinnon, D. P. (2000). Equivalence of the mediation, confounding and suppression effect. Prevent. Sci. 1, 173–181. doi: 10.1023/A:1026595011371
MacKinnon, D. P., Fairchild, A. J., and Fritz, M. S. (2007). Mediation analysis. Ann. Rev. Psychol. 58, 593–614. doi: 10.1146/annurev.psych.58.110405.085542
Manea, L., Gilbody, S., Hewitt, C., North, A., Plummer, F., Richardson, R., et al. (2016). Identifying depression with the PHQ-2: a diagnostic meta-analysis. J. Affect. Disord. 203, 382–395. doi: 10.1016/j.jad.2016.06.003
Martin, F., Wright, H., Moody, L., Whiteman, B., McGillion, M., Clyne, W., et al. (2020). Help to overcome problems effectively for cancer survivors: development and evaluation of a digital self-management program. J. Med. Internet Res. 22:e17824. doi: 10.2196/17824
May, D., Litvin, B., and Allegrante, J. (2024). Behavioral activation, depression, and promotion of health behaviors: a scoping review. Health Educ. Behav. 51, 321–331. doi: 10.1177/10901981221090157
McCullagh, P. (1980). Regression models for ordinal data. J. R. Stat. Soc. Series B Statist. Methodol. 42, 109–127. doi: 10.1111/j.2517-6161.1980.tb01109.x
McCullough, M. E., Emmons, R. A., and Tsang, J.-A. (2002). The grateful disposition: a conceptual and empirical topography. J. Person. Soc. Psychol. 82, 112–127. doi: 10.1037//0022-3514.82.1.112
Menard, S. (2004). Six approaches to calculating standardized logistic regression coefficients. Am. Statist. 58, 218–223. doi: 10.1198/000313004X946
Mills, P. J., Redwine, L., Wilson, K., Pung, M. A., Chinh, K., Greenberg, B. H., et al. (2015). The role of gratitude in spiritual well-being in asymptomatic heart failure patients. Spirit. Clin. Pract. 2, 5–17. doi: 10.1037/scp0000050
Morin, C. M. (1993). Insomnia: Psychological Assessment and Management. New York, NY: Guilford Press.
Newman, D. B., Gordon, A. M., and Mendes, W. B. (2021). Comparing daily physiological and psychological benefits of gratitude and optimism using a digital platform. Emotion 21, 1357–1365. doi: 10.1037/emo0001025
Ng, M.-Y., and Wong, W.-S. (2013). The differential effects of gratitude and sleep on psychological distress in patients with chronic pain. J. Health Psychol. 18, 263–271. doi: 10.1177/1359105312439733
Ohayon, M. M., Reynolds, C. F., and Dauvilliers, Y. (2013). Excessive sleep duration and quality of life. Ann. Neurol. 73, 785–794. doi: 10.1002/ana.23818
O'Laughlin, K. D., Martin, M. J., and Ferrer, E. (2018). Cross-sectional analysis of longitudinal mediation processes. Multivar. Behav. Res. 53, 375–402. doi: 10.1080/00273171.2018.1454822
Packard, A. E. B., Egan, A. E., and Ulrich-Lai, Y. M. (2016). HPA axis interactions with behavioral systems. Compr. Physiol. 6, 1897–1934. doi: 10.1002/cphy.c150042
Personality and Assessment Group Department of Psychology, University of Zurich. (n.d.). Gratitude Questionnaire–6, German Translation. Available online at: https://www.michael-mccullough.com/research/measures-and-translations (accessed June 18, 2023).
Peterson, B., and Harrell, F. E. (1990). Partial proportional odds models for ordinal response variables. Appl. Stat. 39:205. doi: 10.2307/2347760
Plummer, F., Manea, L., Trepel, D., and McMillan, D. (2016). Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic meta-analysis. Gen. Hosp. Psychiatry 39, 24–31. doi: 10.1016/j.genhosppsych.2015.11.005
Prince, S. A., Cardilli, L., Reed, J. L., Saunders, T. J., Kite, C., Douillette, K., et al. (2020). A comparison of self-reported and device measured sedentary behaviour in adults: a systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act 17:31. doi: 10.1186/s12966-020-00938-3
Prince, S. A., Reid, R. D., Pipe, A. L., and McDonnell, L. A. (2017). An evaluation of CardioPrevent: a technology-enabled, health-behavior change program for the global reduction of cardiovascular risk. Curr. Opin. Cardiol. 32, 580–589. doi: 10.1097/HCO.0000000000000438
Puth, M.-T., Weckbecker, K., Schmid, M., and Münster, E. (2017). Prevalence of multimorbidity in Germany: Impact of age and educational level in a cross-sectional study on 19,294 adults. BMC Public Health 17:826. doi: 10.1186/s.12889-017-4833-3
R Core Team (2022). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available online at: https://www.R-project.org/
Revelle, W. R. (2022). psych: Procedures for Psychological, Psychometric, and Personality Research. Northwestern University, Evanston, Illinois. Available online at: https://CRAN.R-project.org/package=psych
Rogers, L. Q., Courneya, K. S., Oster, R. A., Anton, P. M., Robbs, R. S., Forero, A., et al. (2017). Physical activity and sleep quality in breast cancer survivors: a randomized trial. Med. Sci. Sports Exer. 49, 2009–2015. doi: 10.1249/MSS.0000000000001327
Roig, E. (2017). “Uttering ‘race' in colorblind France and post-racial Germany,” in Rassismuskritik und Widerstandsformen, eds. K. Fereidooni and M. El (Wiesbaden: Springer Fachmedien Wiesbaden), 613–627.
Rosenstock, I. M. (1966). Why people use health services. Milbank Mem. Fund Quart. 44, 94–127. doi: 10.2307/3348967
Rosenstock, I. M., Strecher, V. J., and Becker, M. H. (1988). Social learning theory and the health belief model. Health Educ. Quart. 15, 175–183. doi: 10.1177/109019818801500203
Ross, R. A., Foster, S. L., and Ionescu, D. F. (2017). The role of chronic stress in anxious depression. Chronic Stress 1:247054701668947. doi: 10.1177/2470547016689472
Rosseel, Y. (2012). lavaan: an R Package for structural equation modeling. J. Stat. Soft. 48. doi: 10.18637/jss.v048.i02
Ryff, C. D., and Keyes, C. L. M. (1995). The structure of psychological well-being revisited. J. Pers. Soc. Psychol. 69, 719–727. doi: 10.1037//0022-3514.69.4.719
Scarlett, S., Nolan, H. N., Kenny, R. A., and O'Connell, M. D. L. (2021). Discrepancies in self-reported and actigraphy-based sleep duration are associated with self-reported insomnia symptoms in community-dwelling older adults. Sleep Health 7, 83–92. doi: 10.1016/j.sleh.2020.06.003
Schoen, C., Osborn, R., How, S. K. H., Doty, M. M., and Peugh, J. (2008). In chronic condition: experiences of patients with complex health care needs, in eight countries, 2008. Health Affairs 27, w1–w16. doi: 10.1377/hlthaff.28.1.w1
Schuler, M., Strohmayer, M., Mühlig, S., Schwaighofer, B., Wittmann, M., Faller, H., et al. (2018). Assessment of depression before and after inpatient rehabilitation in COPD patients: psychometric properties of the German version of the Patient Health Questionnaire (PHQ-9/PHQ-2). J. Affect. Disord. 232, 268–275. doi: 10.1016/j.jad.2018.02.037
Schulte, T., Hofmeister, D., Mehnert-Theuerkauf, A., Hartung, T., and Hinz, A. (2021). Assessment of sleep problems with the Insomnia Severity Index (ISI) and the sleep item of the Patient Health Questionnaire (PHQ-9) in cancer patients. Supp. Care Cancer 29, 7377–7384. doi: 10.1007/s00520-021-06282-x
Schwarzer, R., and Jerusalem, M. (1995). “Generalized self-efficacy scale,” in Measures in Health Psychology: A User's Portfolio, eds. J. Weinman, S. Wright, and M. Johnston (Windsor: NFER-Nelson), 35–37.
Shorofsky, M., Bourbeau, J., Kimoff, J., Jen, R., Malhotra, A., Ayas, N., et al. (2019). Impaired sleep quality in COPD is associated with exacerbations. Chest 156, 852–863. doi: 10.1016/j.chest.2019.04.132
Siengsukon, C. F., Alshehri, M., Williams, C., Drerup, M., and Lynch, S. (2020). Feasibility and treatment effect of cognitive behavioral therapy for insomnia in individuals with multiple sclerosis: a pilot randomized controlled trial. Mult. Scler. Relat. Disord. 40:101958. doi: 10.1016/j.msard.2020.101958
Simon, P. (2012). Collecting ethnic statistics in Europe: a review. Ethnic Racial Stud. 35, 1366–1391. doi: 10.1080/01419870.2011.607507
Sirois, F. M. (2003b). Beyond health locus of control: a multidimensional measure of health-related control beliefs and motivations (PhD diss.). Carleton University, Ottawa, ON, Canada.
Sirois, F. M. (2004). Procrastination and intentions to perform health behaviors: the role of self-efficacy and the consideration of future consequences. Pers. Indiv. Diff. 37, 115–128. doi: 10.1016/j.paid.2003.08.005
Sirois, F. M. (2007). “I'll look after my health, later”: a replication and extension of the procrastination–health model with community-dwelling adults. Pers. Indiv. Diff. 43, 15–26. doi: 10.1016/j.paid.2006.11.003
Sirois, F. M. (2015). A self-regulation resource model of self-compassion and health behavior intentions in emerging adults. Prevent. Med. Rep. 2, 218–222. doi: 10.1016/j.pmedr.2015.03.006
Sirois, F. M., Kitner, R., and Hirsch, J. K. (2015). Self-compassion, affect, and health-promoting behaviors. Health Psychol. 34, 661–669. doi: 10.1037/hea0000158
Southwell, S., and Gould, E. (2017). A randomised wait list-controlled pre–post–follow-up trial of a gratitude diary with a distressed sample. J. Posit. Psychol. 12, 579–593. doi: 10.1080/17439760.2016.1221127
Spitzer, R. L., Kroenke, K., Williams, J. B. W., and Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. 166:1092. doi: 10.1001/archinte.166.10.1092
Stächele, T., and Volz, H.-P. (2013). Taschenatlas Stress [Pocket Atlas of Stress]. Berlin: Aesopus Publishing.
Staples, L. G., Dear, B. F., Gandy, M., Fogliati, V., Fogliati, R., Karin, E., et al. (2019). Psychometric properties and clinical utility of brief measures of depression, anxiety, and general distress: the PHQ-2, GAD-2, and K-6. Gen. Hosp. Psychiatry 56, 13–18. doi: 10.1016/j.genhosppsych.2018.11.003
Su, Y., Wang, S.-B., Zheng, H., Tan, W.-Y., Li, X., Huang, Z.-H., et al. (2021). The role of anxiety and depression in the relationship between physical activity and sleep quality: a serial multiple mediation model. J. Affect. Disord. 290, 219–226. doi: 10.1016/j.jad.2021.04.047
Swain, N., Lennox Thompson, B., Gallagher, S., Paddison, J., and Mercer, S. (2020). Gratitude Enhanced Mindfulness (GEM): a pilot study of an internet-delivered programme for self-management of pain and disability in people with arthritis. J. Posit. Psychol. 15, 420–426. doi: 10.1080/17439760.2019.1627397
Thorsteinsson, E. B., Brown, R. F., and Owens, M. T. (2019). Modeling the effects of stress, anxiety, and depression on rumination, sleep, and fatigue in a nonclinical sample. J. Nerv. Ment. Dis. 207, 355–359. doi: 10.1097/NMD.0000000000000973
Ullmann, S., Strauß, B., Tiesler, F., Schneider, N., Gensichen, J., and Brenk-Franz, K. (2022). Patient characteristics as predictors of sleep disturbances in multimorbid primary care patients—a secondary analysis. J. Psychos. Res. 153:110705. doi: 10.1016/j.jpsychores.2021.110705
Vallejo, M. A., Vallejo-Slocker, L., Fernández-Abascal, E. G., and Mañanes, G. (2018). Determining factors for stress perception assessed with the Perceived Stress Scale (PSS-4) in Spanish and other European samples. Front. Psychol. 9:37. doi: 10.3389/fpsyg.2018.00037
Vernia, F., Di Ruscio, M., Ciccone, A., Viscido, A., Frieri, G., Stefanelli, G., et al. (2021). Sleep disorders related to nutrition and digestive diseases: a neglected clinical condition. Int. J. Med. Sci. 18, 593–603. doi: 10.7150/ijms.45512
Walsh, R. F. L., Smith, L. T., Klugman, J., Titone, M. K., Ng, T. H., Goel, N., et al. (2023). An examination of bidirectional associations between physical activity and mood symptoms among individuals diagnosed and at risk for bipolar spectrum disorders. Behav. Res. Ther. 161:104255. doi: 10.1016/j.brat.2023.104255
Weziak-Bialowolska, D., Bialowolski, P., and Niemiec, R. M. (2023). Character strengths and health-related quality of life in a large international sample: a cross-sectional analysis. J. Res. Pers. 103:104338. doi: 10.1016/j.jrp.2022.104338
Wood, A. M., Froh, J. J., and Geraghty, A. W. A. (2010). Gratitude and well-being: a review and theoretical integration. Clin. Psychol. Rev. 30, 890–905. doi: 10.1016/j.cpr.2010.03.005
Wood, A. M., Joseph, S., and Linley, P. A. (2007). Coping style as a psychological resource of grateful people. J. Soc. Clin. Psychol. 26, 1076–1093. doi: 10.1521/jscp.2007.26.9.1076
Wood, A. M., Maltby, J., Stewart, N., and Joseph, S. (2008). Conceptualizing gratitude and appreciation as a unitary personality trait. Pers. Indiv. Diff. 44, 621–632. doi: 10.1016/j.paid.2007.09.028
Wu, S. M., and Amtmann, D. (2013). Psychometric evaluation of the perceived stress scale in multiple sclerosis. ISRN Rehabil. 2013, 1–9. doi: 10.1155/2013/608356
Yee, T. W. (2015). Vector Generalized Linear and Additive Models: With an Implementation in R. New York, NY: Springer.
Yuan, S. L. K., Couto, L. A., and Marques, A. P. (2021). Effects of a six-week mobile app versus paper book intervention on quality of life, symptoms, and self-care in patients with fibromyalgia: a randomized parallel trial. Braz. J. Phys. Ther. 25, 428–436. doi: 10.1016/j.bjpt.2020.10.003
Zeng, L.-N., Zong, Q.-Q., Yang, Y., Zhang, L., Xiang, Y.-F., Ng, C. H., et al. (2020). Gender difference in the prevalence of insomnia: a meta-analysis of observational studies. Front. Psychiatry 11:577429. doi: 10.3389/fpsyt.2020.577429
Zimmermann, T., Puschmann, E., Van Den Bussche, H., Wiese, B., Ernst, A., Porzelt, S., et al. (2016). Collaborative nurse-led self-management support for primary care patients with anxiety, depressive or somatic symptoms: cluster-randomised controlled trial (findings of the SMADS study). Int. J. Nurs. Stud. 63, 101–111. doi: 10.1016/j.ijnurstu.2016.08.007
Keywords: insomnia, sleep disturbance, health behaviors, health self-efficacy, psychological distress, gratitude, primary care
Citation: Altier HR, Hirsch JK, Weber A, Kohls N, Schelling J, Toussaint LL, Sirois FM and Offenbächer M (2025) Gratitude and sleep disturbance in primary care patients: the mediating roles of health self-efficacy, health behaviors, and psychological distress. Front. Sleep 4:1459854. doi: 10.3389/frsle.2025.1459854
Received: 05 July 2024; Accepted: 19 March 2025;
Published: 17 April 2025.
Edited by:
Kristi E. Pruiksma, The University of Texas Health Science Center at San Antonio, United StatesReviewed by:
Jessica M. Meers, United States Department of Veterans Affairs, United StatesRebecca Campbell, University of Arizona, United States
Copyright © 2025 Altier, Hirsch, Weber, Kohls, Schelling, Toussaint, Sirois and Offenbächer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Heather R. Altier, aGFsdGllcjFAamguZWR1; Jörg Schelling, am9lcmcuc2NoZWxsaW5nQG1lZC51bmktbXVlbmNoZW4uZGU=