 Molly Jacobs1
Molly Jacobs1 Charles Ellis Jr.
Charles Ellis Jr.- 1Department of Health Services Research, Management and Policy, University of Florida, Gainesville, FL, United States
- 2Department of Speech, Language and Hearing Sciences, University of Florida, Gainesville, FL, United States
- 3Communication Equity and Outcomes Laboratory, University of Florida, Gainesville, FL, United States
Introduction: Auditory difficulties (i.e., hearing loss, tinnitus, both) are correlated with unemployment, underemployment, and reduced income, particularly among minority populations, Although hearing loss is more common among Non-Hispanic White individuals, receipt of otologic and hearing healthcare is far less common among Non-Hispanic Black individuals with hearing loss and tinnitus. The objective of this study was to evaluate differences in employment and income among young adults with hearing loss, tinnitus, and both.
Methods: Data from Waves IV (2008) (N = 15,701) and V (2016–18) (N = 11,955) of the National Longitudinal Study of Adolescent to Adult Health (ADD Health) contained self-reported hearing loss for individuals aged 24–43. Logistic and ordinal dependent variable regression evaluated the likelihood of having paid employment and the level of income, respectively, between categories of hearing loss controlling for sample heterogeneity. Findings were validated using a two-part model with racial/ethnic interactions.
Results: Among respondents, 5.81%−8.87% reported tinnitus only, 0.82%−1.39% reported hearing loss only, and 0.54%−1.41% reported both. Regression analysis showed that Black individuals were less likely to have paid employment (OR = 0.72, CI = 0.58, 0.90) and earned lower income (OR = 0.85, CI = 0.82, 0.88) than White individuals. There were no differences in the likelihood of employment/income between those with tinnitus/both conditions and those with no difficulties, but those with hearing loss had lower likelihood of paid employment (OR = 0.88, CI = 0.85, 0.87) and income (OR = 0.95, CI = 0.94, 0.97). Black and Hispanic individuals with hearing loss were less likely to have paid employment (Black individuals OR = 0.02, CI = 0.00, 0.18; Hispanic individuals OR = 0.01, CI = 0.00, 0.15). Black individuals with hearing loss (OR = 0.79, CI = 0.64, 0.95), tinnitus (OR = 0.83, CI = 0.80, 0.88), and other respondents with both (OR = 0.72, CI = 0.68, 0.77) earned lower income.
Conclusion: Results suggest that hearing loss is associated with a reduced likelihood of employment and employment advancement particularly among young Black and Hispanic individuals.
1 Introduction
The World Health Organization (2024) estimates that by 2050, approximately 2.5 billion people will have some degree of hearing loss. Higher rates of hearing loss have been reported among Non-Hispanic White Americans when compared to other racial-ethnic groups (DeAngelis et al., 2024). Currently there are over 28 million working age (20–69 years) Americans who experience some degree of hearing loss (HL) (Lin, 2012). Untreated hearing loss can result in reductions in health, quality of life, and life satisfaction (Kamil and Lin, 2015) by adversely affecting interpersonal relationships as well as relationships in the workplace (Cunningham and Tucci, 2017). Furthermore, hearing-impaired workers experience higher levels of stress, expend increased effort in listening at work, and tend to take more sick days as a result of stress-related complaints (Canlon et al., 2013).
Related to hearing loss is tinnitus or the “ringing or other noises” in one's ears (Biswas et al., 2022). Worldwide estimates suggest 14% of adults experience tinnitus (Jarach et al., 2022) and in the US, 11.2% of the population or ~27 million people) experience tinnitus (Batts and Stankovic, 2024). Tinnitus is the auditory perception of a stimulus in the absence of a stimulus that is commonly associated with acoustic trauma, chronic hearing loss, emotional stressors, or spontaneous occurrence (Piccirillo et al., 2020). Tinnitus has also been associated with lower self-reported health, and higher levels of depression, anxiety, and stress (Stegeman et al., 2021). A reciprocal relationship with stress appears to exist as individuals with tinnitus frequently experience abnormal responses to stress and stress has also been identified as a probable cause of tinnitus (Patil et al., 2023). According to Dalrymple and colleagues (Dalrymple et al., 2021), most cases of tinnitus are benign and idiopathic. Additionally, a standard diagnostic workup emphasizing detailed history and physical examination can result in identifying causes that are treatable.
Racial disparities have been reported in the presence of hearing loss and tinnitus. Studies show that the odds of hearing loss are 91% higher in Non-Hispanic White older adults when compared to Non-Hispanic Black older adults even after adjusting for age, sex, household income, and educational levels (Deng et al., 2021). These same disparities persist among younger adults aged 45–64 (Madans et al., 2021). Similarly, Batts and Stankovic (2024) reported that tinnitus rates were significantly higher among non-Hispanic individuals vs. Hispanic White individuals, Black individuals, or other ethnicity. However, a different trend exists among adults with hearing loss and tinnitus in relationship to their hearing environments and hearing healthcare for their conditions. For example, a recent study utilizing national data demonstrated that Non-Hispanic White individuals reported a significantly better hearing health than other ethnicities (Nadler, 2023). Similarly, non-Hispanic White individuals have better access to hearing healthcare when compared to other racial-ethnic groups (Blazer et al., 2016). Finally, non-Hispanic Black individuals with tinnitus were less likely to receive tinnitus evaluations for tinnitus suggesting they are under-served in the treatment of the disorder (Batts and Stankovic, 2024).
In addition to racial disparities, the presence of hearing loss or tinnitus has significant economic implications. For example, hearing loss has been attributed to unemployment, underemployment, and reduced earnings (Emmett and Francis, 2015; Garcia Morales et al., 2022; Shan et al., 2020). Similarly, the presence of tinnitus has also been associated with higher rates of unemployment, underemployment, and lower income (Emmett and Francis, 2015). However, before considering the long-term economic implications of hearing loss and tinnitus, we must acknowledge that key human investment is made during the teens, twenties, and early thirties through the growth of knowledge, development of positive work habits, gathering of information, accrual of advancement opportunities, establishment of benchmark wages, and determination of one's market value (Quinones et al., 1995). During this time, the accrual of human capital through post-secondary education, early employment, and continuity in employment benefits young adults throughout their working lives (Staff and Mortimer, 2007). Studies show that differences in both the amount and timing of work experience, can explain a substantial portion of individual-level wage differentials (Light and Ureta, 1995).
Most studies of the economic impact of hearing loss and tinnitus have primarily focused on associations among older adults and few studies have included individuals with tinnitus (Haji et al., 2022). To our knowledge, no study has directly examined the longitudinal association between hearing loss, tinnitus, and earned income in a large, nationally representative sample. Benito et al. (2016). examined the “hearing earnings gaps” between individuals who were deaf or hard of hearing and those without a hearing disability, but their small, cross-sectional sample limited their ability to assess causality and account for educational and employment heterogeneity. Therefore, this study explored the relationship between hearing loss, employment, and income examining racial and ethnic differences in these relationships among a nationally representative sample of young adults. Given the importance of early career employment and earnings in subsequent wage growth and job tenure, the identification and explication of potential employment and income differentials is essential amidst the increasing prevalence of both hearing loss (Shargorodsky, 2010) and tinnitus (Mahboubi et al., 2013) among the youth and young adult population.
2 Methods
2.1 Data
Data for this study came from the National Longitudinal Study of Adolescent to Adult Health (ADD Health)—a longitudinal study following a nationally representative sample of adolescents who were in Grades 7–12 during the 1994–1995 school year (Harris and Udry, 2018). ADD Health combines longitudinal survey data on respondents' social, economic, psychological, and physical wellbeing with contextual data on family, neighborhood, community, school, friendships, peer groups, and romantic relationships. Participant responses from the ADD Health survey have been used to study the relationships between labor market outcomes and a variety of characteristics, including education (Rees and Sabia, 2014), health conditions (Norton and Han, 2008), and behaviors (Fletcher, 2009; Rees and Sabia, 2015). However, despite the inclusion of survey items concerning hearing loss few studies have focused on the implications thereof for this study population.
The initial ADD Health cohort consisted of children and adolescents who were followed into young adulthood through five in-home interviews (Waves I–V) occurring in 1994–5, 1996, 2001–02, 2008–09, and 2016–18 when respondents were 12–17, 13–18, 18–26, 24–32, and 33–43 years old, respectively. ADD Health used a school-based design with the primary sampling frame derived from the Quality Education Database (QED) comprised of 26,666 U. S. High Schools. From this frame, a stratified sample of high schools was selected with the probability of selection proportional to school size. Schools were stratified by region, urbanicity, school type (public, private, parochial), ethnic mix, and size. For each high school selected, one of its feeder schools was identified and recruited with probability proportional to its student contribution to the high school. Adolescents were selected with unequal probability from the 1994–1995 enrollment rosters for the schools and those not on rosters that completed the in-school questionnaire. A core sample was derived from this administration by stratifying students in each school by grade and sex and then randomly choosing students from each stratum. For additional information on the ADD Health sampling process, attrition, and data collection, see http://www.cpc.unc.edu/projects/addhealth/design. In Wave I, a parent of each ADD Health respondent was interviewed to gather social, behavioral, and health information. To reflect the changing lives as the respondents age from adolescence to adults, ADD Health changes survey questionnaires with each successive Wave. In Waves III and IV, survey items regarding hearing ability and tinnitus, respectively, were included in the survey for the first time. Therefore, this study utilized Waves IV and V collected when respondents were aged 24–32 and 33–43, respectively, to evaluate the association between income and hearing loss/tinnitus.
2.2 Inclusion and identification criteria
The study sample was limited to individuals who responded to questions related to hearing loss and tinnitus in either Wave IV or V. The first question asked, “Which statement best describes your hearing without a hearing aid or other assistive devices? [Excellent, Good, Fair/A Little Trouble, Poor/Moderate Trouble, Very Poor/A Lot of Trouble, Deaf].” The second question asked, “In the past 12 months have you been bothered by ringing, roaring, or buzzing in your ears or head (tinnitus) that lasts for 5 min or more? [Yes, No].” These criteria resulted in 15,701 respondents in Wave IV (345 excluded) and 11,955 respondents in Wave V (2 excluded).
2.3 Hearing loss/tinnitus identification
Most (Wave IV 15,701, Wave V 11,955) respondents provided valid responses to hearing-related survey items in each wave making them eligible for inclusion in the panel. Given the difficulty in the interpreting results from multinomial models, we collapsed the responses into two groups containing the top three and bottom three categories in each wave (Table 1). In this study, these categories are labeled as hearing loss and no hearing loss. In the panel, 128 (0.82%), 913 (5.81%), and 85 (0.54%%) reported having hearing loss only, tinnitus only, and both conditions in Wave IV while 166 (1.39%), 1,061 (8.87%), and 168 (1.41%) reported these conditions in Wave V. The 14,575 (92.83%) and 10,560 (88.33%) in Waves IV and V, respectively, reported neither difficulty.
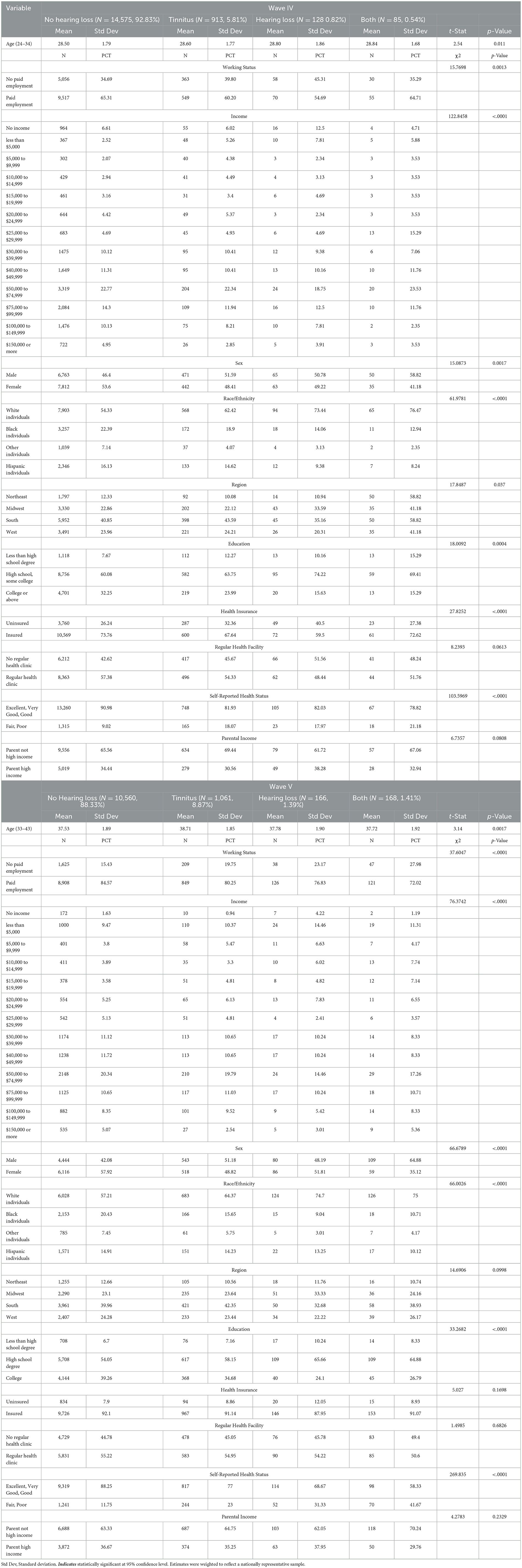
Table 1. Sample characteristics and tests of differences by type of hearing loss.
2.4 Individual characteristics
Demographic, parental, and health-related attributes were included in the analysis (Biswas et al., 2022; Stegeman et al., 2021). Demographic covariates included age, sex, race/ethnicity, region of residence, employment status, and educational attainment. To create a consistent measure of educational attainment across waves, education was coded into three categories: (1) less than a high school degree; (2) high school degree or equivalent, some college, vocational or technical degree; and (3) college degree and beyond. Region included four geographic regions—Northeast, Midwest, South, and West. Respondents were employed if they reported working at least 10 h per week for pay. Both sex (male, female) and race/ethnicity (non-Hispanic White individuals, non-Hispanic Black individuals, Hispanic individuals, non-Hispanic Asian/Pacific Islander individuals, non-Hispanic American Indian/Native American non-Hispanic Other, or Multiracial individuals) were self-identified. Respondents who reported being non-Hispanic Asian/Pacific Islander, non-Hispanic American Indian/Native American non-Hispanic Other, or Multiracial individuals were combined due to small sample sizes.
Since access to resources, education, and care during childhood is associated with individual-level educational attainment, income, and health status later in life (Maness et al., 2016), we included an indicator for Wave I parental income over $60,000 annually—the upper 50% of the distribution. To account for differences in health care access between respondents, an indicator was created for having health insurance. Respondents also reported their general health status as excellent (5), very good (4), good (3), fair (2), or poor (1). Consistent with other studies using ADD Health data (Maness et al., 2016; Hoke and Boen, 2021), responses were collapsed into two groups—excellent/very good/good and fair/poor.
2.5 Employment and income
Respondents indicated whether not they were working for pay. Those working for pay were also asked about their income. Income was reported as the total received from personal earnings before taxes including, wages or salaries, including tips, bonuses, and overtime pay, and income from self-employment. In Wave IV, earned income was reported as one of 12 categories ranging from “less than $5,000” to “$150,000 or more.” In Wave V, earned income was reported as one of 13 income categories ranging from “ <$5,000” to “$200,000 or more.” Therefore, to create a consistent series across waves, the values provided in Waves V were coded into the 12 categories used in Wave IV. The categorical translation is shown in Table 2. Respondents with no earned income who indicated that they were not working, were assigned an income value of zero. Respondents who indicated that they were working but did not report a valid income (Wave IV N = 1,039, Wave V N = 2,216) were not included in the regression analysis.
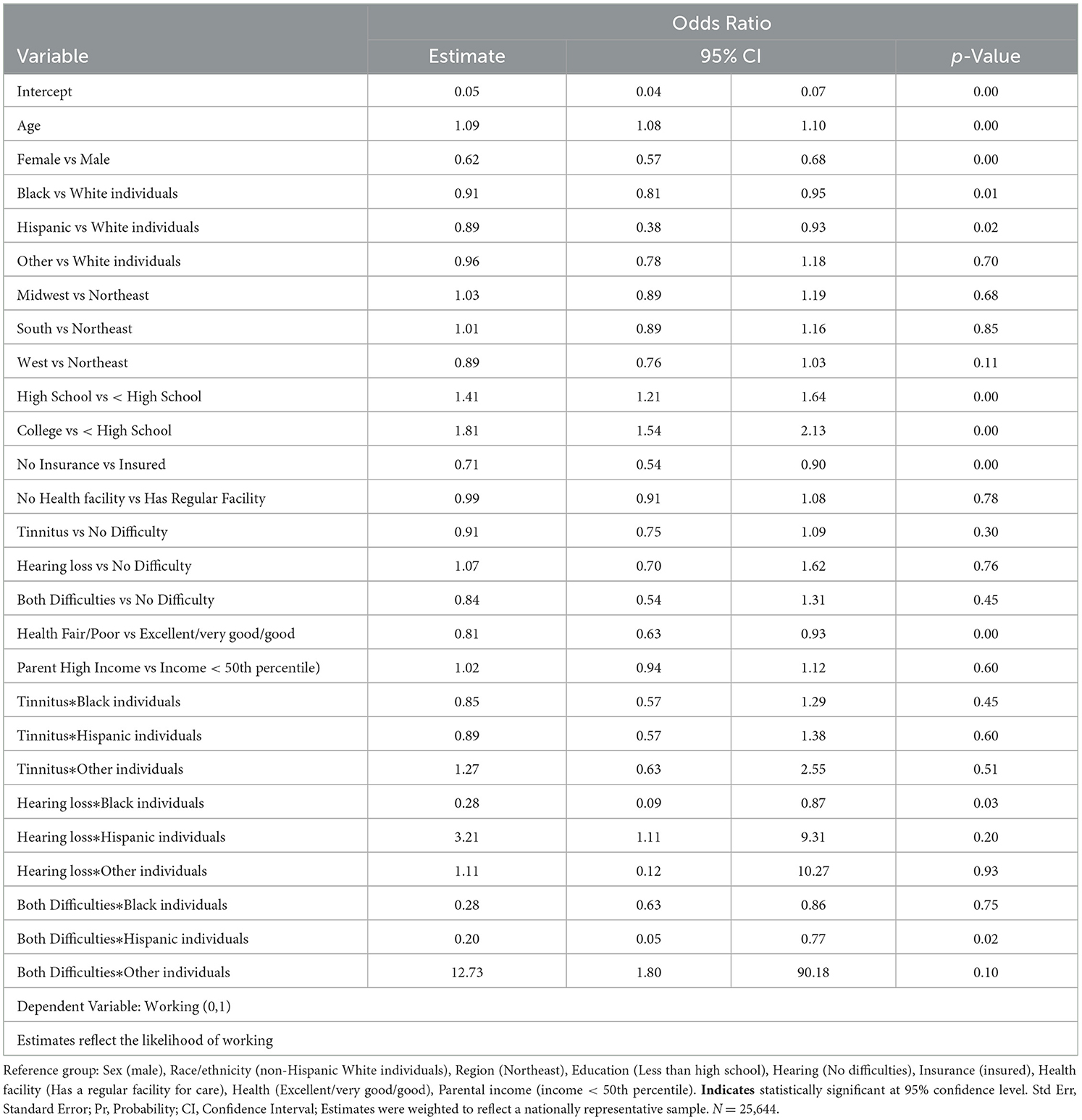
Table 2. Likelihood of working- multilevel logistic estimation.
2.6 Statistical analysis
First, using Wave IV and V longitudinal weights, descriptive statistics for all covariates were calculated for respondents with hearing loss (HL) only, tinnitus (TN) only, both difficulties, and no hearing difficulties. Between group differences in continuous and categorical covariates were tested using t- and chi-square tests, respectively. To adjust for the complex clustered sampling frame of ADD Health and ensure that the results were nationally representative, survey commands and sampling weights were used for all calculations. Statistical analyses accounted for clustering and stratification of the ADD Health sampling design.
Second, multivariable logistic regression analyzed the relationships between covariates and the relative likelihood of paid employment adjusting for age, sex, race/ethnicity, region of residence, education, health insurance, having a regular care facility, hearing loss, health status, and parental income level. Interaction terms between race/ethnicity and hearing loss were included to assess subgroup differences. Since some respondents were present in both Waves IV and V, their responses would be correlated over time. To account for this type of correlation as well as the school-level clustering and regional stratification of the ADD Health sampling design, regression models included random individual-time intercepts that adjusted for the compounded structure of their covariance using multilevel models with time-invariant fixed effects. Significance levels were set at p < 0.05. Adjusted odds ratios (ORs) were calculated for all covariates and interaction effects. The model specification accounted for the repeated individual-level observations in the panel data.
Third, since income was reported as categorical values in Waves IV and V, rather than a discrete or continuous value, the distribution and distributional parameters of income were examined to determine the appropriate distributional specification. Due to the ordered categorical nature of the outcome, an ordinal logistic regression model was specified. The ordinal logistic regression assumes a non-normal distribution in the error term of an integer-based dependent variable and can be employed without any special corrections. Given the proportional odds assumption which was tested and validated using the Brant-Wald test, the coefficients represent the difference in the log odds of a given level and the reference. Odds ratios and associated 95% confidence intervals were also calculated to reflect the magnitude of the expected change in income levels. The model specification accounted for repeated individual-level structure and cross-wave covariance of the panel data through the log of individual-level time exposure.
Although this study utilizes data from Waves IV and V of the National Longitudinal Study of Adolescent to Adult Health (Add Health), it is not a fully longitudinal analysis in the strictest sense, as not all respondents were present in both waves. Therefore, the analytic sample includes both longitudinal respondents (those observed in both waves) and cross-sectional respondents (those observed in either Wave IV or Wave V). While the longitudinal design of Add Health informs the structure and strengths of the dataset, the current analysis is treated as a pooled cross-sectional study. All models account for missingness under the assumption that data are missing at random (MAR), but the primary research question does not rely on within-person changes over time. This design choice reflects the study's goal of estimating population-averaged associations between income and auditory health outcomes, rather than examining within-individual trajectories. Since some Wave IV respondents were not present or had missing response values in Wave V, the missing at random (MAR) assumption was tested by regressing a binary indicator of Wave V missingness on the model covariates. The lack of significance in any covariates suggested that sample attrition did not significantly bias results.
2.7 Sensitivity analysis
To ensure that the inclusion of an interaction term between hearing loss and race enhanced the model fit, a likelihood ratio test was conducted to compare the model with and without the inclusion of these interactions (improvement in model fit at α = 0.05 was larger than critical value 3.84). Finally, we conducted a sensitivity analysis to examine the robustness of findings. A two-part selection regression model was used to validate the findings related to differential earnings likelihoods and levels between respondents with HL only, tinnitus only, both conditions, and no hearing loss. Two-part selection models mitigate any potential selection bias by separating the selection process (i.e., whether a respondent earns income) from the primary relationship of interest (i.e., the association between income level and hearing loss). Since respondents who are not working or are not in the labor force, have no income, they were coded as missing.
Missing data is a common challenge in analyzing longitudinal survey data. If the data are missing at random (MAR), and the parameters governing the missing data process and the model for the outcome are disjoint, then the missing data are ignorable. Most statistical methods used in longitudinal data analysis rely on the MAR assumption and violation of the assumption can result in biased estimates. In a two-part model, the relationship between the risk of the variable being missing and its unseen value is fit for the probability of observing a positive-vs.-non-positive outcome. Then, conditional on a positive outcome, a regression model is fit for the positive outcome. The analysis herein models the risk of a respondent having a missing or non-missing income, then, conditional on having non-missing income, models the association between income level and the covariates. The model specification accounted for repeated individual-level structure of the panel data and cross-wave covariance through the log of individual-time exposure. To ensure that sample attrition did not bias results, the model was also estimated to include those with missing observation in Wave V within the stage 1 analysis sample.
3 Results
Table 1 provides descriptive statistics for all covariates for respondents with no hearing loss, hearing loss, and tinnitus. Chi-square and t-statistics tested for statistically significant differences across groups. Only a small portion of respondents reported tinnitus only (Wave IV 5.81%; Wave V 8.87%), HL only (Wave IV 0.82%; Wave V 1.39%), or both conditions (Wave IV 0.54%; Wave V 1.41%). Most respondents reported no hearing loss (Wave IV 92.83%; Wave V 88.33%). Over half (Wave IV 53.6%; 57.92% Wave V) of those with no hearing loss were female. However, females comprised less than half of those with tinnitus (Wave IV 48.41%; Wave V 48.82%), HL (Wave IV 49.22%; Wave V 51.81%), and both conditions (Wave IV 41.18%; Wave V 35.12%)—a statistically significant difference (Wave IV χ2 = 15.09, p = 0.0017; Wave V χ2 = 66.68, p < 0.0001). Most respondents were White individuals (tinnitus only Wave IV 62.42%; Wave V 64.37%; HL only Wave IV 73.44%; Wave V 74.70%, both conditions Wave IV 76.47%; Wave V 75%). Only a small portion of those with these difficulties were Black and Hispanic individuals. Respondents were distributed throughout the US with the largest representation in the South (Wave IV: TN only 43.59%; HL only 35.16%; 58.82%; Wave V: TN only 42.35%; HL only 32.68%; both conditions 38.93%), but these differences were not statistically significant (Wave IV χ2 = 17.85, p = 0.087; Wave V χ2 = 14.69, p = 0.10).
Significantly differences in educational attainment (Wave IV χ2 = 18.01, p = 0.0004; Wave V χ2 = 33.27, p < 0.0001) were found between the auditory groups with college graduation among those hearing loss only (Wave IV 15.63%; Wave V 24.1%), tinnitus only (Wave IV 23.99%; Wave V 34.68%), and both conditions (Wave IV 15.29%; Wave V 26.79%) lower compared to those with no hearing loss (Wave IV 32.25%; Wave V 39.26%). Between 80 and 90% of all groups had health insurance (Wave IV χ2 = 27.83, p < 0.0001; Wave V χ2= 5.03, p = 0.17) and over half had a regular facility where they received healthcare (Wave IV χ2 = 8.24, p = 0.06; Wave IV χ2 = 1.50, p = 0.68). However, roughly 91% and 88% of those with no hearing loss in Waves IV and V reported being in good, very good, or excellent health. Only 82%, 82%, and 79% in Wave IV and 77%, 68.67%, and 58.33% in Wave V of those with tinnitus only, HL only, and both difficulties (Wave IV χ2 = 103.60, p < 0.0001; Wave V χ2 = 269.84, p < 0.0001) reported good health. Between 30 and 40% of respondents had parents in the top half of the income distribution in Waves IV (No difficulty 34.44%; Tinnitus only 30.56%; HL only 38.28%; Both 32.94) and V (No difficulty 36.67%; Tinnitus only 35.25%; HL only 37.95%; Both 29.76%) and there was no statistically significant difference between groups (Wave IV χ2 = 6.74, p = 0.08; Wave V χ2 = 4.28, p = 0.23).
Figure 1 shows the percent of each auditory group at each income level in Waves IV and V. As indicated in the figures, there were significant differences in the income distribution (Wave IV χ2 = 122.85, p < 0.0001; Wave V χ2 = 76.37, p < 0.0001) with respondents with no difficulty clustered in the upper income ranges and respondents with hearing loss concentrated in the left tail of the distribution. However, the groups also showed significant sex, racial/ethnic, educational, and self-reported health differences. To determine if the association between hearing loss and income level were robust to differences in these characteristics, we performed three regression analyses.
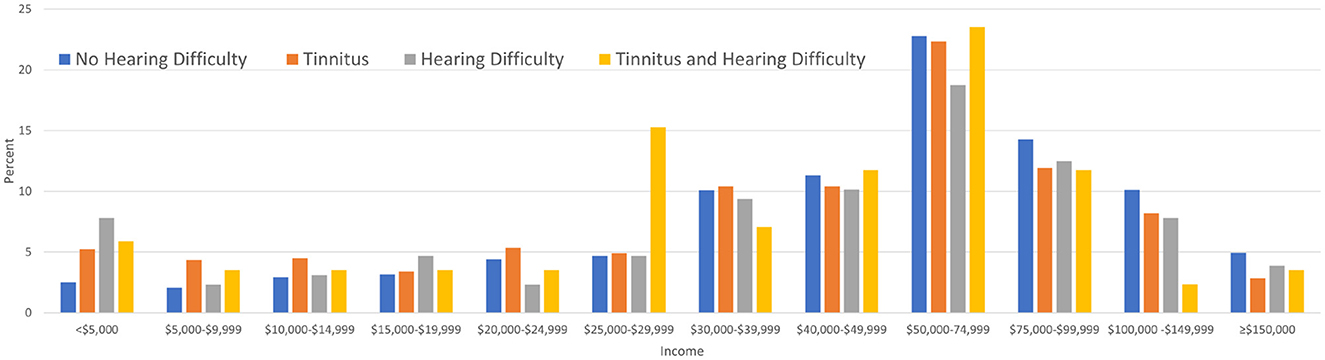
Figure 1. Reported income level by auditory difficulty wave IV.
Multilevel logistic regression (Table 2) estimated the association between the likelihood of engaging in work and age, sex, race/ethnicity, region of residence, education, insurance, regular health facility, parental income, auditory group, and auditory group-race interactions. Results showed that the likelihood of working increased with age (OR = 1.09, CI = 1.08, 1.10). Given the longitudinal nature of the data, this may also suggest that the likelihood increased over the time frame of the panel. Those with a high school (OR = 1.41, CI = 1.21, 1.64) or college (OR = 1.81, CI = 1.54, 2.13) education were also more likely to work compared to the reference group. Compared to males, White respondents, and those in good health, females (OR = 0.62, CI = 0.57, 0.68), Black individuals (OR = 0.91, CI = 0.81, 0.95), Hispanic individuals (OR = 0.89, CI = 0.38, 0.93), and those in poor health (OR = 0.81, CI = 0.63, 0.93) had a lower likelihood of working. Compared to their counterparts without any hearing loss, Black individuals with hearing difficulties (OR = 0.28, CI = 0.09, 0.87) and Black and Hispanic individuals with both difficulties (Black individuals OR = 0.28, CI = 0.63, 0.86; Hispanic individuals OR = 0.20, CI = 0.05, 0.77) had a lower likelihood of working.
Multilevel logistic regression (Table 3) estimated the longitudinal association between the likelihood of being paid for work (a binary variable) and the individual-level covariates, auditory groups, and auditory group-race interactions. Results showed that the likelihood of being paid for work increased with age (OR = 1.14, CI = 1.11, 1.16). All else held constant, respondents in the Midwest (OR = 1.43, CI = 1.11, 1.85) and South (OR = 1.40, CI = 1.10, 1.77) were more likely to be paid for work relative to those in the Northeast. Compared to respondents without a degree, those with a high school diploma (OR = 1.52, CI = 1.18, 1.95) and college degrees (OR = 2.72, CI = 1.97, 3.75) were significantly more likely to be paid for work. However, being uninsured (OR = 0.63, CI = 0.34, 0.99), not having a regular facility for healthcare (OR = 0.35, CI = 0.12, 0.64), and rating individual health as fair or poor (OR = 0.52, CI = 0.180.96) was associated with a lower likelihood of being paid for work. Black individuals (OR = 0.72, CI = 0.58, 0.90), Hispanic individuals (OR = 0.64, CI = 0.43, 0.95), and respondents of Other racial groups (OR = 0.75, CI = 0.56, 1.00) were less likely to be paid for work compared to White individuals. Compared to respondents without any hearing loss, those with HL (OR = 0.88, CI = 0.85, 0.87) were significantly less likely to be paid for work. Relative to their counterparts with no HL, Black individuals (OR = 0.02, CI = 0.00, 0.18) and Hispanic individuals (OR = 0.01, CI = 0.00, 0.15) respondents with HL were less likely to be paid for work.
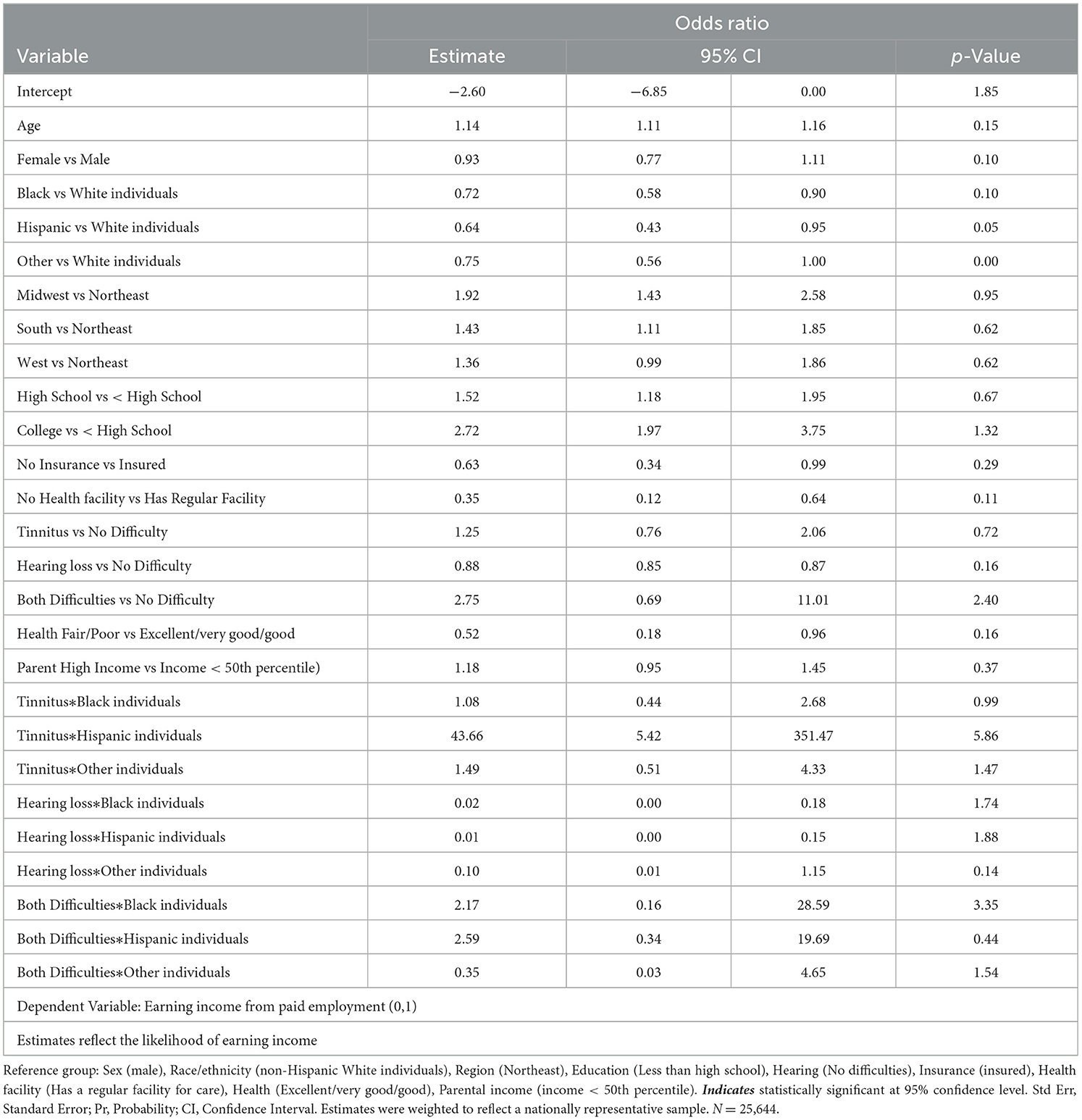
Table 3. Likelihood of being paid for work-multilevel logistic estimation.
Multilevel ordinal logistics regression (Table 4) estimated longitudinal covariate associations with income level among respondents who reported earned income. Since ordinal logistics coefficient values do not have an intuitive interpretation, results were also expressed as odds ratios (ORs). Results indicated that, compared to males, females had significantly lower income levels (OR = 0.53, CI = 0.50, 0.56) levels lower. Income was also lower among older respondents (OR = 0.95, CI = 0.94, 0.96) compared to those at younger ages. Residents of the South (OR = 0.87, CI = 0.79, 0.97) and Midwest (OR = 0.80, CI = 0.72, 0.89) earned comparatively lower income than Northeastern residents. Compared to those with lower educational attainment, respondents with a high school (OR = 1.51, CI = 1.30, 1.75) or college (OR = 3.75, CI = 3.19, 4.42) degree had higher relative earnings. Uninsured respondents (OR = 0.53, CI = 0.48, 0.58) and those without a regularly facility for health care (OR = 0.60, CI = 0.56, 0.65) earned less than their counterparts. Relative to those without hearing loss, respondents with hearing loss (OR = 0.67, CI = 0.45, 0.99) and both HL and tinnitus (RO = 0.82, CI = 0.71, 0.95) had significantly lower earnings. Relative to White individuals, Black individuals (OR = 0.52, CI = 0.48, 0.57) had lower income, but respondents of other races (OR = 1.32, CI = 1.12, 1.57) had comparatively higher income. However, Black individuals with HL (OR = 0.35, CI = 0.19, 0.47) or tinnitus (OR = 0.84, CI = 0.75, 0.97) had lower income than their unimpaired counterparts.
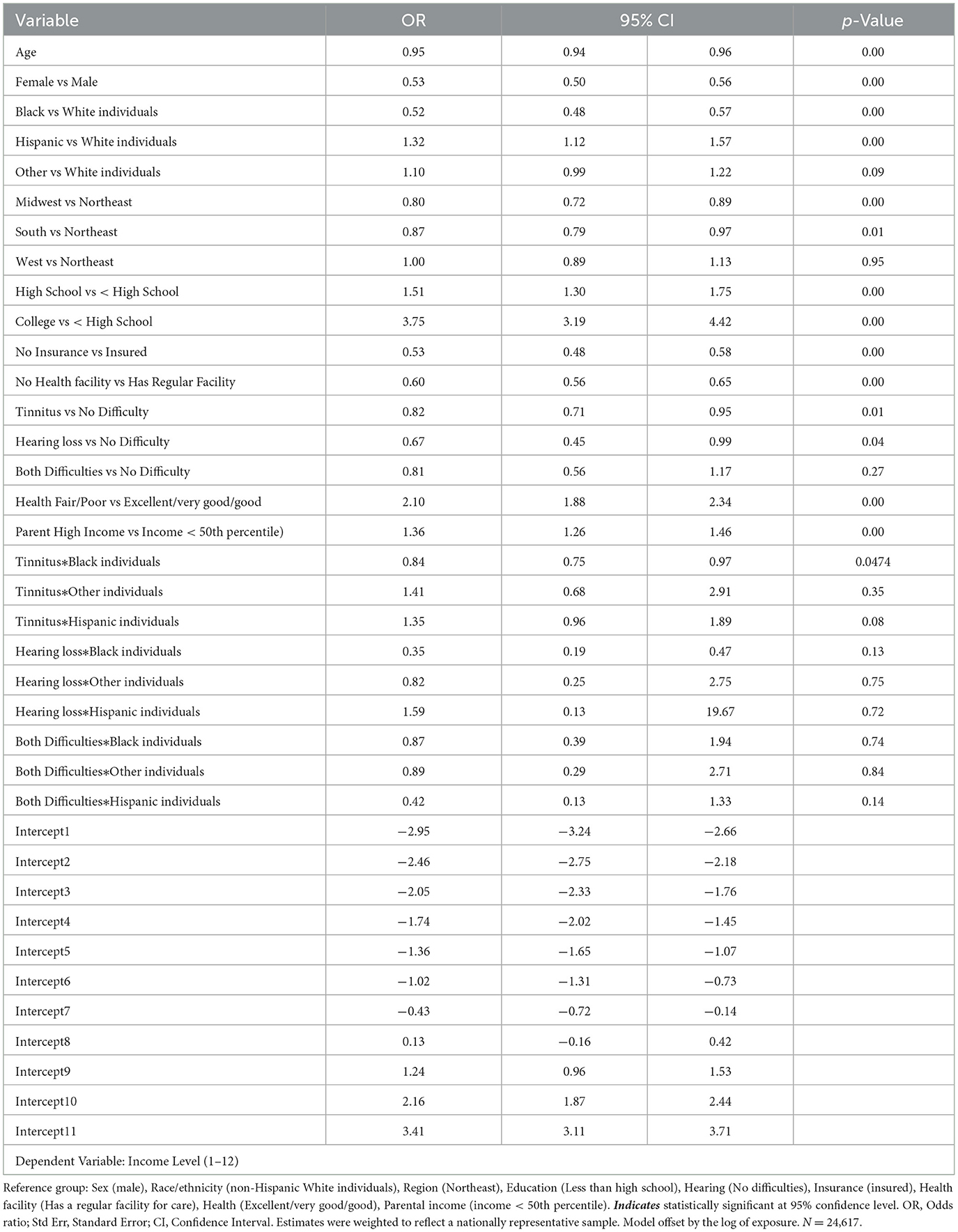
Table 4. Relative level of earnings-multilevel ordinal logistic estimation.
3.1 Sensitivity analysis
While the direction and statistical significance of key covariates remained consistent across both the original and two-part models, the magnitude of several coefficients—particularly for variables such as parental income and health status—was reduced in the two-part model. This attenuation suggests that unobserved selection processes, such as the non-random likelihood of depression may have influenced part of the original associations. The two-part model addresses this by jointly modeling the probability of employment and income, providing more conservative and potentially more accurate effect estimates. Thus, while the original models highlight robust associations, the two-part model adds value by strengthening causal inference and clarifying the extent to which selection bias may influence observed relationships. The coefficient values and magnitudes vary between the two frameworks as a result of the variations in empirical procedures, but the consistency in coefficient significance confirmed the robustness of the logit and ordinal regression estimates showing differences in the likelihood of earning income as well as the income levels of respondents with hearing loss and show differential earnings associations among racial and ethnic minority groups with hearing loss (Table 5).
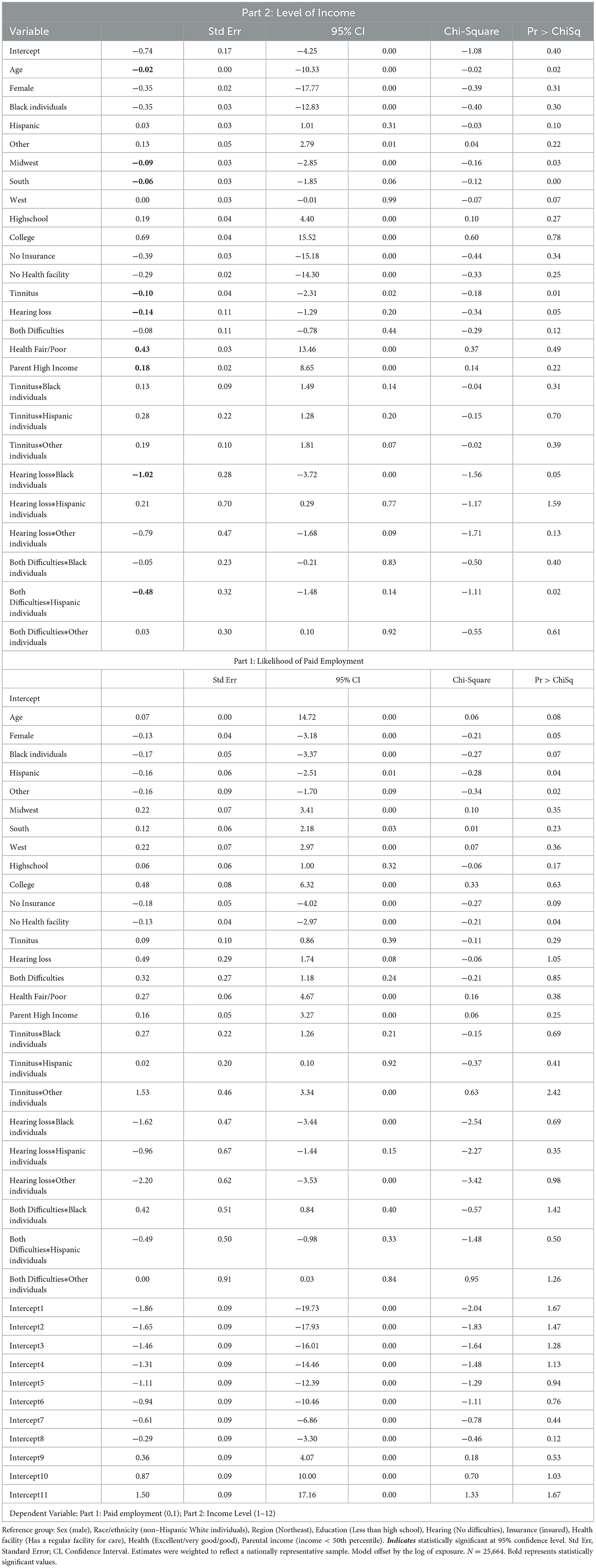
Table 5. Sensitivity analysis-two-part sample selection estimation.
4 Discussion
In those cohort of young adults (ages 22–43) who were initially identified when they were in grades 7–12, this study showed that hearing loss has a detrimental effect on income. Additionally, young adults from minoritized backgrounds with hearing loss earn substantially less than their White counterparts. These findings suggest hearing-related issues have a negative effect on earning beginning in young adulthood. The study also showed that, despite being more prevalent among young adults, the presence of tinnitus was not associated with differential employment likelihood or potential earnings. Reviews of the literature report a high economic cost associated with tinnitus (Daoud et al., 2022), yet a negative impact among young adults in this study did not emerge.
According to the Hearing Health Foundation (Hearing Health Foundation, 2024), individuals with hearing loss typically earn about 25% less than their counterparts without hearing loss. More importantly, individuals with hearing loss are more likely to be unemployed or underemployed, have lower income, and less likely to have access the hearing care (Malcolm et al., 2022). Further, adults with hearing loss frequently retire earlier than adults without hearing loss which translates into greater financial strain long term (Helvik et al., 2013). Garcia Morales et al. (2022) found that individuals with moderate-severe hearing loss were more likely to not be engaged in the labor force. Frequent transitions in and out of the labor market may force individuals to work well-past usual retirement ages to manage later life expenses (Adhikari et al., 2011). However, it is possible that individuals with hearing loss face unexplained barriers to entering and continuously being employed that are not specific to their hearing loss (e.g., poor general health, employment type, etc.) (Garcia Morales et al., 2022).
A second concerning issue is the implication for lifetime earnings. According to Infurna and Wiest (2018) disabilities impact the trajectories of wellbeing. Life satisfaction declines in adults who become disabled in the years following disability. Given evidence that the effects of early work force participation are felt and often exacerbated throughout the course of employment (Helbling et al., 2016), it is tenable that hearing loss among young adults could potentially operate in the same fashion by negatively impacting employment and income over time—analogous to individuals with disabilities (Svinndal et al., 2020).
Workforce participation issues and subsequently lifetime earnings are further complicated by racial-ethnic difficulties that are common among hearing workers. This study showed that compared with White individuals with hearing loss, Black individuals with the same difficulty had lower earnings. Lower earning among individuals with hearing-related issues has been previously reported however the longer-term impact is less clear. Emmett and Francis (2015) found that individuals with hearing loss demonstrated 1.5 times higher odds of having a low income than individuals with normal hearing. Black and Hispanic individuals with hearing loss earned 68% and 75% the income of White individuals with hearing loss highlighting the potential additive effect of hearing loss among Black individuals who traditionally earn less than White individuals (Wilson and Darity, 2022).
Finally, the issues of racial differences in earnings may not be isolated but linked to early decisions about care for individuals with hearing loss and tinnitus. Batts and Stankovic (2024) found that Non-Hispanic Black individuals were less likely to discuss hearing loss and tinnitus with their healthcare providers. Additionally, those Non-Hispanic Black individuals that did discuss their conditions were less likely to be subsequently evaluated for hearing loss or tinnitus. These early hearing healthcare interactions that lack the necessary discussion about hearing loss and tinnitus may contribute to observed otologic healthcare disparities.
The lack of difference between the income of young adults with tinnitus and those without hearing loss may suggest that tinnitus has little impact on employment/income of young adults or that the impact is more likely to occur later in life. Age is a primary risk factor tinnitus even though the specific mechanism that cause tinnitus are less clear (Reisinger et al., 2023). Similarly, it is possible that tinnitus in young adulthood does not impact workforce participations and subsequently income. Studies suggest that young adults with tinnitus are less likely to seek professional services to reduce the debilitating effects (Bhatt, 2018). Young adults are also less likely to have chronic diseases commonly associated with tinnitus which increases their likelihood of continuing to work and earn income (Bhatt, 2018). Research suggests that tinnitus may worsen over time among those exposed to noise in their work environment (Engdahl et al., 2012), but the likelihood of exacerbation varies by nature of the condition (Ralli et al., 2017) suggesting a potential interactions between age, duration of tinnitus, symptomatology, and environment that may influence employment disruption and income. Finally, the impact of disabling conditions such as hearing loss and tinnitus is dynamic and unfolds over time (Shuey and Willson, 2019). Minimally, disabilities are associated with economic insecurity particularly as individuals approach retirement (Shuey and Willson, 2019). Disabilities also have negative implications for income by increasing the likelihood that income is derived from lower paying sources (Ranaldi, 2022)—such as government benefits or pensions which are lower than wages or salaries (Pu and Syu, 2023).
4.1 Limitations
Despite the robustness of these findings, they must be interpreted in the context of the following limitations. First, all data was self-reported and cannot be otherwise verified, validated, or confirmed. Despite self-reported, survey data, is known to suffer from several biases including favorability bias, recall bias, acquiescence bias, and demand bias. Second, we are unable to account for any treatment, care, or mitigation efforts to absolve their hearing loss or tinnitus. While they may have previously or contemporaneously received amelioratory services, this information was not collected. Third, slightly lower percentages of the sample reported hearing loss and tinnitus than is seen in the general population. This likely reflects the difference between self-reported and clinically validated data use. Fourth, we do not account for differences in the severity, frequency, or chronic nature of either hearing loss or tinnitus which was not available in the data but could influence results. The data also does not confirm whether the reported hearing loss was congenital or acquired. Fifth, due to small cell sizes we combined non-Hispanic Asian/Pacific Islander, non-Hispanic American Indian/Native American, non-Hispanic Other, and Multiracial individuals into a single category. This decision, however, obscured the distinct heterogeneity of these groups illustrating the necessity of future studies with larger and more diverse samples. Finally, it is not possible to control for all sources of individual heterogeneity in these data for reasons such as availability within the ADD Health survey, confounding of statistical robustness, and unobservability.
5 Conclusions
Young adults with hearing loss are less likely to earn the same level of income to those absent of hearing loss and performing the same job even after controlling for relevant covariates. These observations are magnified when young adults from racial-ethnic minoritized backgrounds have hearing related issues. Future work is needed to determine the long-term impact for all individuals with hearing loss and to develop policy strategies to ensure equitable workforce participation and subsequently income.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://researchdata.unc.edu/.
Ethics statement
The studies involving humans were approved by the University of Florida Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
MJ: Methodology, Supervision, Visualization, Investigation, Data curation, Formal analysis, Software, Conceptualization, Funding acquisition, Validation, Resources, Writing – original draft, Writing – review & editing, Project administration. ET: Resources, Writing – original draft, Writing – review & editing, Conceptualization, Methodology. CE: Writing – original draft, Project administration, Visualization, Resources, Conceptualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Adhikari, R., Soonthorndhada, K., and Haseen, F. (2011). Labor force participation in later life: evidence from a cross-sectional study in Thailand. BMC Geriatr. 11:15. doi: 10.1186/1471-2318-11-15
Batts, S., and Stankovic, K. M. (2024). Tinnitus prevalence, associated characteristics, and related healthcare use in the United States: a population-level analysis. Lancet Reg. Health Am. 29:100659. doi: 10.1016/j.lana.2023.100659
Benito, S. G., Glassman, T. S., and Hiedemann, B. G. (2016). Disability and labor market earnings. J. Disabil. Policy Stud. 27, 178–188. doi: 10.1177/1044207316658752
Bhatt, I. S. (2018). Prevalence of and risk factors for tinnitus and tinnitus-related handicap in a college-aged population. Ear Hear. 39, 517–526. doi: 10.1097/AUD.0000000000000503
Biswas, R., Genitsaridi, E., Trpchevska, N., Lugo, A., Schlee, W., Cederroth, C. R., et al. (2022). Low evidence for tinnitus risk factors: a systematic review and meta-analysis. J. Assoc. Res. Otolaryngol. 24, 81–94. doi: 10.1007/s10162-022-00874-y
Blazer, D. G., Domnitz, S., and Liverman, C. T. (2016). Committee on Accessible and Affordable Hearing Health Care for Adults, Board on Health Sciences Policy. Health and Medicine Division, National Academies of Sciences, Engineering, and Medicine Hearing Health Care for Adults. Washington, DC: National Academies Press. doi: 10.17226/23446
Canlon, B., Theorell, T., and Hasson, D. (2013). Associations between stress and hearing problems in humans. Hear. Res. 295, 9–15. doi: 10.1016/j.heares.2012.08.015
Cunningham, L. L., and Tucci, D. L. (2017). Hearing loss in adults. New Engl. J. Med. 377, 2465–2473. doi: 10.1056/NEJMra1616601
Dalrymple, S. N., Lewis, S. H., and Philman, S. (2021). Tinnitus: diagnosis and management. Am. Fam. Phys. 103, 663–671.
Daoud, E., Caimino, C., Akeroyd, M. A., Noreña, A. J., and Baguley, D. M. (2022). The utility of economic measures to quantify the burden of tinnitus in affected individuals: a scoping review. Pharmacoecon Open 6, 21–32. doi: 10.1007/s41669-021-00273-8
DeAngelis, R. T., Frizzelle, B. G., Hummer, R. A., and Harris, K. M. (2024). Traces of historical redlining in the contemporary United States: new evidence from the add health cohort. Popul. Res. Policy Rev. 43:61. doi: 10.1007/s11113-024-09906-2
Deng, Z., Agbeyaka, S., and Fuller-Thomson, E. (2021). Black older Americans have lower prevalence of hearing loss than their white peers: findings from two large nationally representative surveys. J. Speech, Lang. Hear. Res. 64, 5014–5021. doi: 10.1044/2021_JSLHR-21-00075
Emmett, S. D., and Francis, H. W. (2015). The socioeconomic impact of hearing loss in U.S. adults. Otol. Neurotol. 36, 545–550. doi: 10.1097/MAO.0000000000000562
Engdahl, B., Krog, N. H., Kvestad, E., Hoffman, H. J., and Tambs, K. (2012). Occupation and the risk of bothersome tinnitus: results from a prospective cohort study (HUNT). BMJ Open 2:e000512. doi: 10.1136/bmjopen-2011-000512
Fletcher, J. (2009). Beauty vs. brains: early labor market outcomes of high school graduates. Econ. Lett. 105, 321–325. doi: 10.1016/j.econlet.2009.09.006
Garcia Morales, E. E., Lin, H., Suen, J. J., Varadaraj, V., Lin, F. R., and Reed, N. S. (2022). Labor force participation and hearing loss among adults in the united states: evidence from the national health and nutrition examination survey. Am. J. Audiol. 31, 604–612. doi: 10.1044/2022_AJA-21-00266
Haji, A. K., Qashar, A. A., Alqahtani, S. H., and Masarit, R. M. (2022). AlSindi TS, Ali-Eldin EM. Prevalence of noise-induced tinnitus in adults aged 15 to 25 years: a cross-sectional study. Cureus 14:e32081. doi: 10.7759/cureus.32081
Harris, K. M., and Udry, J. R. (2018). National longitudinal study of adolescent to adult health (add health), 1994-2008 [Public Use]. Ann Arbor, MI: Carolina Population Center, University of North Carolina-Chapel Hill [distributor], Inter-university Consortium for Political and Social Research [distributor].
Hearing Health Foundation (2024). Workplace Hearing Loss. Available online at: https://hearinghealthfoundation.org/hearing-loss-in-the-workplace#:~:text=Untreatedhearinglosscandecrease,byasmuchas%2430%2C000 (Accessed February 20, 2024).
Helbling, L. A., Imdorf, C., Ayllon, S., and Sacchi, S. (2016). Methodological challenges in the study of scarring effects of early job insecurity. NEGOTIATE working paper.
Helvik, A. S., Krokstad, S., and Tambs, K. (2013). Hearing loss and risk of early retirement. The HUNT study. Eur. J. Public Health 23, 617–622. doi: 10.1093/eurpub/cks118
Hoke, M. K., and Boen, C. E. (2021). The health impacts of eviction: evidence from the national longitudinal study of adolescent to adult health. Soc. Sci. Med. 273:113742. doi: 10.1016/j.socscimed.2021.113742
Infurna, F. J., and Wiest, M. (2018). The effect of disability onset across the adult life span. J. Gerontol. 73, 755–766. doi: 10.1093/geronb/gbw055
Jarach, C. M., Lugo, A., Scala, M., van den Brandt, P. A., Cederroth, C. R., Odone, A., et al. (2022). Global prevalence and incidence of tinnitus: a systematic review and meta-analysis. JAMA Neurol. 79, 888–900. doi: 10.1001/jamaneurol.2022.2189
Kamil, R. J., and Lin, F. R. (2015). The effects of hearing impairment in older adults on communication partners: a systematic review. J. Am. Acad. Audiol. 26, 155–182. doi: 10.3766/jaaa.26.2.6
Light, A., and Ureta, M. (1995). Early-career work experience and gender wage differentials. J. Labor Econ. 13, 121–154. doi: 10.1086/298370
Lin, F. R. (2012). Hearing loss and falls among older adults in the United States. Arch. Intern. Med. 172:369. doi: 10.1001/archinternmed.2011.728
Madans, J. H., Weeks, J. D., and Elgaddal, N. (2021). Hearing difficulties among adults: United States, 2019. NCHS Data Brief. 414, 1–8. doi: 10.15620/cdc:107540
Mahboubi, H., Oliaei, S., Kiumehr, S., Dwabe, S., and Djalilian, H. R. (2013). The prevalence and characteristics of tinnitus in the youth population of the United States. Laryngoscope 123, 2001–2008. doi: 10.1002/lary.24015
Malcolm, K. A., Suen, J. J., and Nieman, C. L. (2022). Socioeconomic position and hearing loss: current understanding and recent advances. Curr. Opin. Otolaryngol. Head Neck Surg. 30, 351–357. doi: 10.1097/MOO.0000000000000831
Maness, S. B., Buhi, E. R., Daley, E. M., Baldwin, J. A., and Kromrey, J. D. (2016). Social determinants of health and adolescent pregnancy: an analysis from the national longitudinal study of adolescent to adult health. J. Adol. Health. 58, 636–643. doi: 10.1016/j.jadohealth.2016.02.006
Nadler, D. (2023). Workforce diversity and occupational hearing health. Safety 9:23. doi: 10.3390/safety9020023
Norton, E. C., and Han, E. (2008). Genetic information, obesity, and labor market outcomes. Health Econ. 17, 1089–1104. doi: 10.1002/hec.1383
Patil, J. D., Alrashid, M. A., Eltabbakh, A., and Fredericks, S. (2023). The association between stress, emotional states, and tinnitus: a mini-review. Front. Aging Neurosci. 15:1131979. doi: 10.3389/fnagi.2023.1131979
Piccirillo, J. F., Rodebaugh, T. L., and Lenze, E. J. (2020). Tinnitus. JAMA 323:1497. doi: 10.1001/jama.2020.0697
Pu, C., and Syu, H. F. (2023). Effects of disability on income and income composition. PLoS ONE 18:e0286462. doi: 10.1371/journal.pone.0286462
Quinones, M. A., Ford, J. K., and Teachout, M. S. (1995). The relationship between work experience and job performance: a conceptual and meta-analytic review. Pers. Psychol. 48, 887–910. doi: 10.1111/j.1744-6570.1995.tb01785.x
Ralli, M., Balla, M. P., Greco, A., Altissimi, G., Ricci, P., Turchetta, R., et al. (2017). Work-related noise exposure in a cohort of patients with chronic tinnitus: analysis of demographic and audiological characteristics. Int. J. Environ. Res. Public Health 14:1035. doi: 10.3390/ijerph14091035
Ranaldi, M. (2022). Income composition inequality. Rev. Income Wealth 68, 139–160. doi: 10.1111/roiw.12503
Rees, D. I., and Sabia, J. J. (2014). The kid's speech: the effect of stuttering on human capital acquisition. Econ. Educ. Rev. 38, 76–88. doi: 10.1016/j.econedurev.2013.07.007
Rees, D. I., and Sabia, J. J. (2015). Migraine headache and labor market outcomes. Health Econ. 24, 659–671. doi: 10.1002/hec.3052
Reisinger, L., Schmidt, F., Benz, K., Vignali, L., Roesch, S., Kronbichler, M., et al. (2023). Ageing as risk factor for tinnitus and its complex interplay with hearing loss—evidence from online and NHANES data. BMC Med. 21:283. doi: 10.1186/s12916-023-02998-1
Shan, A., Ting, J. S., Price, C., Goman, A. M., Willink, A., Reed, N. S., et al. (2020). Hearing loss and employment: a systematic review of the association between hearing loss and employment among adults. J. Laryngol. Otol. 134, 387–397. doi: 10.1017/S0022215120001012
Shargorodsky, J. (2010). Change in prevalence of hearing loss in US adolescents. JAMA 304:772. doi: 10.1001/jama.2010.1124
Shuey, K. M., and Willson, A. E. (2019). Trajectories of work disability and economic insecurity approaching retirement. J. Gerontol. 74, 1200–1210. doi: 10.1093/geronb/gbx096
Staff, J., and Mortimer, J. T. (2007). Educational and work strategies from adolescence to early adulthood: consequences for educational attainment. Soc. Forc. 85, 1169–1194. doi: 10.1353/sof.2007.0057
Stegeman, I., Eikelboom, R. H., Smit, A. L., Baguley, D. M., Bucks, R. S., Stokroos, R. J., et al. (2021). Tinnitus and its associations with general health, mental health and hearing loss. Prog. Brain Res. 262, 431–450. doi: 10.1016/bs.pbr.2021.01.023
Svinndal, E. V., Jensen, C., and Rise, M. B. (2020). Working life trajectories with hearing impairment. Disabil. Rehabil. 42, 190–200. doi: 10.1080/09638288.2018.1495273
Wilson, V., and Darity, W. (2022). Understanding black-white disparities in labor market outcomes requires models that account for persistent discrimination and unequal bargaining power. Economic Policy Institute. Available online at: https://www.epi.org/unequalpower/publications/understanding-black-white-disparities-in-labor-market-outcomes/ (Accessed February 21, 2024).
World Health Organization (2024). Deafness and hearing loss. Available online at: https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss (Accessed April 7, 2025).
Keywords: hearing loss, tinnitus, employment, income, young adult
Citation: Jacobs M, Tobener EN and Ellis C Jr (2025) Hearing loss and tinnitus: association with employment and income among young adults. Front. Audiol. Otol. 3:1595281. doi: 10.3389/fauot.2025.1595281
Received: 17 March 2025; Accepted: 18 June 2025;
Published: 01 August 2025.
Edited by:
Adrian Fuente, Montreal University, CanadaReviewed by:
Brian Richard Earl, University of Cincinnati, United StatesCharlotte Bigras, Montreal University, Canada
Copyright © 2025 Jacobs, Tobener, Ellis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Charles Ellis Jr., ZWxsaXNjaEBwaGhwLnVmbC5lZHU=