 Yonghee Oh1,2*
Yonghee Oh1,2* Chase Sereno2
Chase Sereno2 Phillip Friggle1
Phillip Friggle1 Josephine Kinder1
Josephine Kinder1 Caroline Cuthbertson1
Caroline Cuthbertson1 Hannah Borton1
Hannah Borton1 Lauren Pollock1
Lauren Pollock1 Ingrid Edwards2
Ingrid Edwards2- 1Department of Otolaryngology, HNS and Communicative Disorders, School of Medicine, University of Louisville, Louisville, KY, United States
- 2Heuser Hearing Institute, Hearing & Language Academy, Louisville, KY, United States
Objectives: To explore binaural speech perception patterns in hearing aid (HA) and/or cochlear implant (CI) users through a retrospective observational study.
Design: Monaural and binaural speech perception scores of 82 bilateral HA, 83 bimodal CI+HA, and 89 bilateral CI users were analyzed.
Results: The binaural benefit pattern dominated at 55% in the bilateral HA group, while only 1% of the binaural interference pattern was observed. Both CI groups exhibited lower rates of the binaural benefit pattern (bimodal CI+HA: 37%; bilateral CI: 27%) but higher rates of the binaural interference pattern (bimodal CI+HA: 8%; bilateral CI: 12%), compared to the bilateral HA group.
Conclusions: The presence of binaural interference implies that listening on two devices is not always better than one. Increased understanding of how this binaural disadvantage affects speech perception for hearing-impaired users is clinically essential for future design of training- and device-based rehabilitative strategies to increase the binaural benefits.
Introduction
In recent years, significant advancements in auditory technology have transformed the lives of individuals with hearing loss through various types of hearing devices, such as hearing aids (HAs) and cochlear implants (CIs). Their devices can provide an increased understanding of speech in noisy environments, sound localization ability, and better subjective quality of life for hearing-impaired (HI) listeners (Ching et al., 2004; Culling et al., 2012; Gifford and Stecker, 2020; Litovsky et al., 2006; van Hoesel, 2004; Yawn et al., 2018; Zheng et al., 2022). Those advantages arise mostly from binaural auditory processing, which is the benefit of auditory information from both ears. However, the degree to which binaural advantages are observed can vary greatly depending on various factors, such as the type of hearing device configuration (e.g., bilateral HAs, bilateral CIs, or bimodal stimulation using a CI in one ear and a HA in the other) and the etiology of hearing loss (e.g., age-related, noise-induced, or drug-induced). Therefore, understanding the relative advantages and disadvantages of different binaural hearing device configurations is essential to explore how those factors impact the overall binaural listening experiences.
Bilateral HAs are often the first line of intervention for individuals with mild to severe hearing loss in both ears. Bilateral HAs aim to restore/aid binaural hearing capabilities, improving their access to binaural cues such as interaural timing and level differences for better speech segregation performance (Zheng et al., 2022). Second, CIs offer an alternate option for individuals with a severe to profound hearing loss who do not gain enough benefit from HAs (i.e., amplification). Bimodal stimulation, which combines a CI and a contralateral HA, has been used to leverage the strengths of both CI and HA devices. Sound localization ability can be maintained with this bimodal CI + HA configuration, particularly when the electrical stimulation and natural acoustic sound in the opposite ear are well-matched and balanced across the spectral and temporal domains (Dorman and Gifford, 2010). Lastly, bilateral CIs offer an alternative to bimodal CI + HA for individuals with profound hearing loss in the non-implanted ear of the bimodal CI + HA users, which means that instead of relying on a HA in one ear and a CI in the other, both ears receive a CI. Similar to the bimodal CI + HA users, the majority of bilateral CI recipients demonstrate improved speech recognition and sound localization when auditory input is balanced across both ears. Notably, within-subject comparison studies have shown that individuals tend to exhibit better audiologic outcomes, speech perception, and quality of life with bilateral CIs compared to a bimodal CI + HA configuration (Ching et al., 2004; Potts and Litovsky, 2014; van Hoesel, 2004; Yawn et al., 2018).
However, limitations to the benefits of binaural devices can be seen. For bilateral HA users, several factors, such as the degree of hearing loss and the presence of dead regions in the cochlea, could vary the effectiveness of using two HAs (Cox et al., 2012). For CI users, they can experience difficulties related to asymmetrical hearing, device compatibility, and the integration of different auditory inputs (Anderson et al., 2024). Therefore, the benefits of bilateral devices may be influenced by the ability of how well the inputs from two hearing devices could be integrated during the auditory processing (Oh et al., 2022, 2023; Reiss et al., 2016).
Although most previous studies showed that bilateral hearing devices elicit binaural benefits, there were also some studies showing little benefit or worse performance in listeners' binaural perception when using two devices compared to just one device. This is an indication of the presence of binaural interference. The existence of this binaural interference was first documented from the mid-1990s to the early 2000s by clinical case reports (Jerger et al., 1993; Carter et al., 2001; Chmiel et al., 1997; Holmes, 2003), and a more recent cross-sectional study by Mussoi and Bentler (2017) confirmed the co-occurrence of binaural benefits and binaural interference phenomena in their HA patients. Therefore, there remains significant variability in the benefits/interferences between two HAs, two CIs, and a CI with a contralateral HA. The goal of this study is to investigate different patterns of binaural perception in all three bilateral hearing device users (i.e., bilateral HA, bimodal CI+HA, and bilateral CI users) with a large sample size. Through retrospective data analysis of patients‘ speech recognition records, this study explores several types of binaural advantages and disadvantages, looking to identify where underlying binaural interferences may be present in bilateral HA, bimodal CI+HA, and bilateral CI users.
Materials and methods
Participants
This study retrospectively reviewed electronic medical records for adult HI listeners using HA and/or CI, who underwent audiologic evaluations at two major audiology clinics in Kentucky, USA (University of Louisville Hospital and Heuser Hearing Institute) between September 2008 and October 2024. A total of 578 HI patients (422 CI recipients and 156 HA users) were initially assessed for their eligibility, and 254 patients (172 CI recipients and 82 HA users) were selected according to the following inclusion/exclusion criteria: documented history of bilateral device use with at least 1 year of experience with their CI and/or HA devices, post-lingual onset of hearing loss, age between 19 and 100 (age of 19 years or older at the time of implantation), pure-tone audiometric thresholds for each ear, and two monaural (i.e., unilateral device) and binaural (i.e., bilateral devices) speech perception scores in quiet. Patients with other pathologic histories, such as Meniere's disease, labyrinthitis, and vestibular neuronitis, were excluded from the study to rule out inconsistent hearing test results. Finally, subjects were divided into three groups: those who used two HAs (82 bilateral HA users), those who used two CIs (89 bilateral CI users), and those who used bimodal stimulation (a CI with a contralateral HA: 83 bimodal CI+HA users). The guidelines for the protection of human subjects were reviewed and approved by the Institutional Review Board (IRB) of the University of Louisville.
Data acquisition
Subject's demographic information (age and sex), audiometric thresholds (aided thresholds for the non-implanted ear), and their two monaural and binaural speech recognition scores in quiet (AzBio Quiet scores; Spahr et al., 2012) were all obtained. Table 1 shows a summary of the demographic data for the subjects who were selected via the inclusion/exclusion criteria described above. It should be noted that all audiologic measurements were conducted in a calibrated sound-treated booth with a traditional sound field setup used in the United States, where the participants were positioned 1 meter away from the loudspeaker. The free-field laaudiometric thresholds were calculated as a pure-tone average (PTA, mean threshold across 250, 500, 1,000, 2,000, 4,000, and 6,000 Hz), and the speech recognition ability was measured using the AzBio sentence corpus, one of the most common test batteries in the United States for the clinical evaluation for adult HI listeners, especially for adult CI users, for both pre- and post-implant assessment of speech recognition performance. Each patient was examined using one randomly selected list of AzBio sentences (20 sentences per list), and the percentage of words that were correctly repeated was calculated to score each list. The measurements were conducted in quiet (AzBio Quiet) at the fixed presentation level of 60 dB sound pressure level (SPL) using a loudspeaker, and the AzBio Quiet scores were measured separately for each ear with the non-test ear's hearing device off (and the non-implanted ear plugged and muffled) and both ears (binaurally). In addition, all subjects' data were collected based on the most recent patient visit records saved in the database.
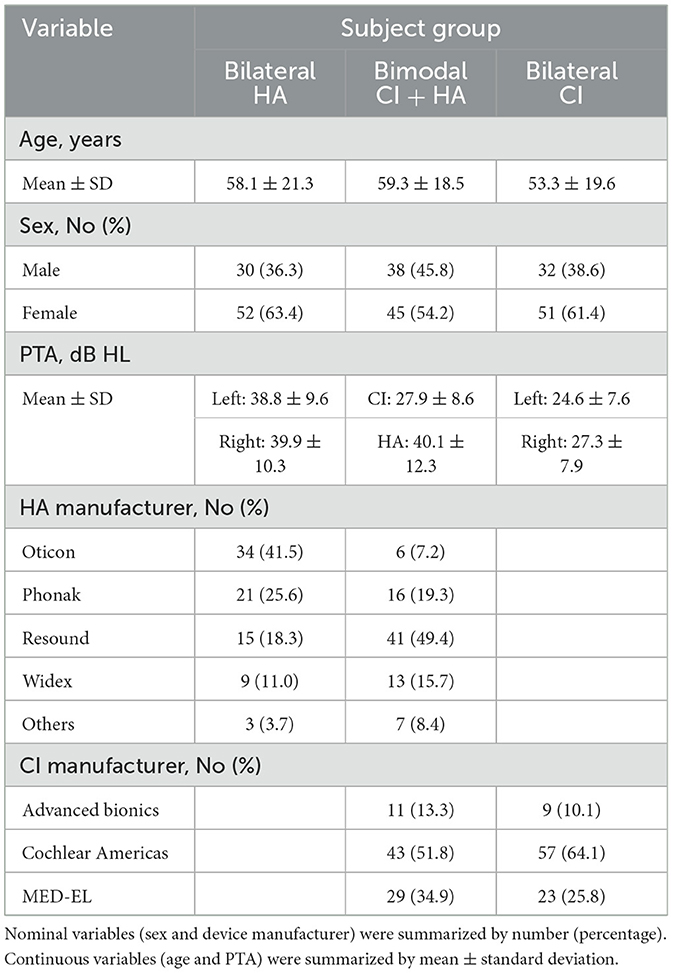
Table 1. Participant demographics for 82 bilateral HA, 83 bimodal CI+HA, and 89 bilateral CI users, including age, sex, pure-tone average (PTA), and HA/CI manufacturer.
Statistical analysis
Descriptive analysis based on frequency and percent distribution was performed for all demographic data (nominal variables: sex and manufacturer; continuous variables: age and pure-tone threshold). A univariate analysis of variance (ANOVA) was conducted to compare the age across three listener groups and the mean pure tone thresholds between the two ears within each listener group. For the speech recognition test, categorical analysis, using a “discretize” function in MATLAB (version R2025a, MathWorks, Natick, Massachusetts, USA) was used to organize the binaural speech recognition (AzBio Quiet) scores into four distinct patterns (Described the details in the Results Section), and statistical analyses were performed to assess the difference in the AzBio Quiet scores between monaural and bilateral listening conditions. All statistical analyses were conducted in SPSS (version 25, IBM, New York, USA).
Results
Demographic results
A total of 254 adult HI patients (82 bilateral HA users, 83 bimodal CI+HA users, and 89 bilateral CI users) were involved in this retrospective observational study. Bilateral HA users ranged in age from 21 to 96 (mean ± std = 58.1 ± 21.3 years; 63.4% females), bimodal CI+HA users ranged in age from 21 to 98 (mean ± std = 59.3 ± 18.5 years; 54.2% females), and bilateral CI users ranged in age from 20 to 90 (mean ± std = 53.3 ± 19.6 years; 61.4% females). A one-way ANOVA test showed that there were no significant age differences between the three listener groups (F2,166 = 2.290, p = 0.104). Note that the participants' ages were collected at their most recent visits for both pure-tone and speech audiometry measurements, and all 254 participants reported regularly using their bilateral devices (i.e., full-time bilateral device usage).
Pure-tone average (PTA) results
The PTA mean ± standard deviation of the aided thresholds for bilateral HA users was 38.8 ± 9.6 dB for the left ear and 39.9 ± 10.3 dB for the right ear. For bimodal CI + HA users, the mean PTA was 27.9 ± 8.6 dB HL in the implanted ear and 40.1 ± 12.3 dB HL in the non-implanted ear. The mean PTAs for the left and right ears of bilateral CI users were 24.6 ± 7.6 and 27.3 ± 7.9 dB HL, respectively. The statistical analysis results using a one-way ANOVA within each listener group demonstrated no significant differences in PTAs between the two ears for the two bilateral device user groups (Bilateral HA: F1,161 = 0.506, p = 0.478; Bilateral CI: F1,176 = 1.44, p = 0.232); however, for the bimodal CI+HA user group, there was a significant PTA difference in PTAs between CI and HA ears (F1,146 = 54.0, p < 0.001).
Speech recognition (AzBio quiet) results
Figure 1 shows individual and average AzBio scores for two monaural and binaural listening conditions. The results revealed four distinct binaural speech recognition patterns across all three listener groups: (1) binaural benefit, where two ears exhibit better speech recognition performance than a single ear alone; (2) better-ear dominance, where the ear with better speech recognition performance plays a more dominant role in binaural speech recognition; (3) binaural averaging, where binaural speech recognition is averaged between two monaural performances; (4) binaural interference, where speech recognition is poorer when listening with two ears than with each ear alone.

Figure 1. Individual and average AzBio speech perception scores for four different binaural perception patterns: binaural benefit, better-ear dominance, binaural averaging, and binaural interference. Error bars represent standard deviation of the mean (*p < 0.05; **p < 0.01; ***p < 0.001). The right column shows percentage distribution of the four binaural speech recognition patterns for each subject group (the percentages were rounded to the nearest whole number).
Within the bilateral HA group, the binaural benefit pattern was the most dominant at 55% (N = 45 out of 82), the better ear pattern was 27% (N = 22 out of 82), the binaural averaging pattern was 17% (N = 14 out of 82), and only 1% of subjects (N = 1 out of 82) exhibited binaural interference patterns. Within the bimodal CI group, the binaural benefit and better ear patterns were similar at 37% (N = 31 out of 83) and 34% (N = 28 out of 83), respectively, the binaural averaging pattern was 17% (N = 17 out of 83), and an increased binaural interference pattern (8%; N = 7 out of 83) was observed. Within the bilateral CI group, the better ear pattern was relatively dominant (40%; N = 36 out of 89), and 27% binaural benefit (N = 24 out of 89), 20% binaural averaging (N = 18 out of 89), and 12% binaural interference (N = 11 out of 89) patterns were observed. Multiple one-way ANOVAs were performed for each binaural speech recognition pattern with the speech perception score as a dependent variable and the listening condition (i.e., two monaural and binaural) as a grouping variable, and the analyses were repeated for each listener group. The results showed significant effects of the listening condition on all four speech recognition patterns in each listener group (p < 0.007, see details in Table 2). Post hoc pairwise comparison results (using Bonferroni correction) demonstrated that the binaural listening condition was significantly different than either monaural listening condition (p < 0.05 for all cases, except for the better-binaural listening condition pairs in the better ear patterns). Please see Table 3 for the detailed pairwise comparison results. Note that the statistical analysis was not performed for the binaural interference in the bilateral HA user group due to the low sample size (N = 1).

Table 2. One-way ANOVA results for the effects of listening conditions on four different binaural speech recognition patterns in three listener groups.
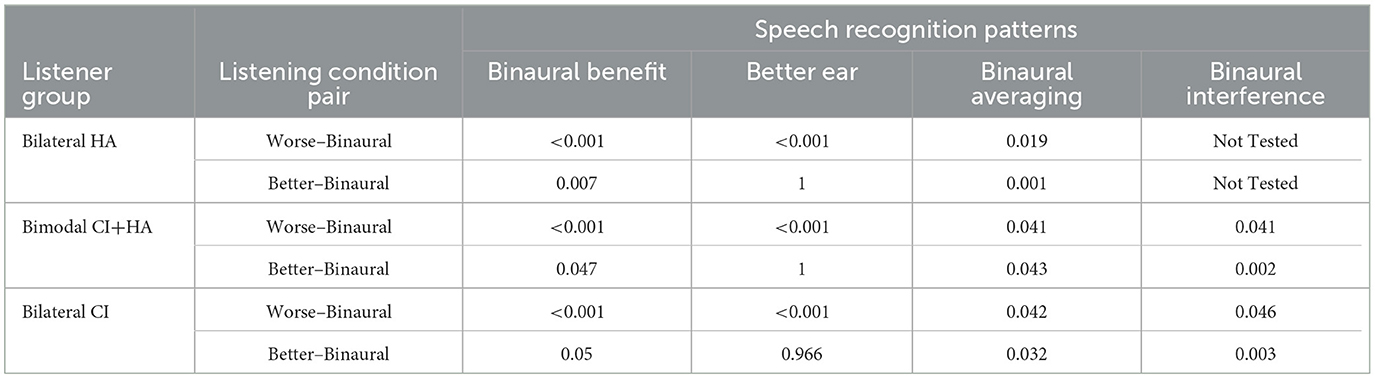
Table 3. Post hoc pairwise comparison results (i.e., p-values) for the listening effects on binaural speech recognition patterns described in Table 2.
Discussion
The results of the current retrospective observational study estimate four distinct patterns of binaural speech recognition in quiet among HA and/or CI users. All three listener groups showed the following four patterns: (1) binaural benefit; (2) better-ear dominance; (3) binaural averaging; and (4) binaural interferences. Here, the binaural benefit and binaural interference are indicative of the existence of binaural advantages and disadvantages in speech recognition performance, respectively. The findings in this study demonstrate that the binaural benefit dominated in the bilateral HA group (55%), while a small chance of binaural interference (1%) occurred. In addition, the findings also show that, in comparison to the bilateral HA group, both CI groups showed less of the binaural benefit pattern (bimodal CI+HA: 37%; bilateral CI: 27%) and more of the binaural interference pattern (bimodal CI+HA: 8%; bilateral CI: 12%).
The binaural advantages (or benefits) have been reported in many previous studies for bilateral hearing device users (Gifford and Dorman, 2019; Litovsky et al., 2006; van Hoesel, 2004). For example, studies have shown that bilateral HA users demonstrate a 3–5 dB improvement in speech recognition thresholds (SRT) in noisy environments compared to unilateral users (Litovsky et al., 2006). Similarly, both bimodal CI + HA and bilateral CI users exhibited bilateral benefits in their word recognition in quiet (bimodal CI + HA: up to 26%; bilateral CI: up to 20%) and in their AzBio sentence recognition in both quiet (bimodal CI+HA: up to 24%; bilateral CI: up to 15%) and noisy (bimodal CI + HA: up to 52%; bilateral CI: up to 25%) conditions (Gifford and Dorman, 2019). In addition to speech perception ability, localization accuracy—the ability to identify source locations—can also improve with binaural hearing. Bilateral CI users show a 30–50% improvement in angular resolution compared to unilateral CI users (van Hoesel, 2004).
Although many studies have reported binaural benefits, a few studies have reported the phenomenon of binaural interference in speech perception for HI listeners, especially for HA users in speech-in-noise configurations (Allen et al., 2000; Henkin et al., 2007; McArdle et al's., 2012; Walden and Walden, 2005); however, their results of the proportion of binaural interference cases are mixed. The studies by Henkin et al. (2007) and Walden and Walden (2005) reported that 70 to 80% of HA device users exhibited poor speech (word or phoneme) recognition performance while using bilateral amplification compared to unilateral amplification (i.e., binaural interference). On the contrary, only 20 to 30% of binaural interference cases were observed in other studies (McArdle et al's., 2012; Mussoi and Bentler, 2017). It should be noted that the binaural interference in the context of all previous studies refers to the situation wherein performance with two ears is poorer than with the better ear alone, which includes both binaural averaging and binaural interference, as distinguished in the present study. For the bilateral HA users in our study, the proportion of those binaural disadvantage cases was 18% (17% binaural averaging + 1% binaural interference), which is shown to be similar to the findings in the studies by McArdle et al's. (2012) and Mussoi and Bentler (2017).
In the study with CI device users, the proportion of binaural interference wasn't directly measured like in the studies with HA users; however, binaural interference was often represented as negative values of binaural benefit. For example, the study by Gifford and Dorman (2019) reported that binaural benefit for AzBio sentence recognition in quiet (AzBio Quiet) ranged from −18 to 100% for the bimodal CI+HA users and −57 to 100% for the bilateral CI users. The study by (Litovsky et al. 2006) also reported that 10% to 23% of their bilateral CI users have a negative performance with their two CI devices compared to one CI. Here, the negative values mean that AzBio Quiet scores in the use of bilateral devices are worse than those in the better ear alone, which is compatible with the combined proportion of binaural averaging (bimodal CI+HA: 20%; bilateral CI: 20%) and binaural interference (bimodal CI+HA: 8%; bilateral CI: 12%) found in the present study.
While this study provided investigators with evidence that there are advantages and disadvantages for speech recognition performance using bilateral hearing devices, it also raised another question: what factors might account for the binaural disadvantages? Several potential factors include: (1) aging, (2) asymmetric hearing performance, and (3) non-optimized device parameters. First, as observed in the previous studies (Allen et al., 2000; Henkin et al., 2007; Mussoi and Bentler, 2017), the binaural interference phenomenon mostly occurred in the elderly population, and their studies suggested that age-related hearing loss (presbycusis) could cause more experience in binaural disadvantages compared to young listeners. Second, the asymmetric hearing performance could cause differences in loudness growth and dynamic range between ears, which are associated with poor sensitivity to access interaural timing and level cues (Litovsky et al., 2006). The results of Litovsky et al.'s (2006) study showed that bilateral CI users could exhibit both bilateral averaging (6 out of 10) and bilateral interference (4 out of 10) in their study participants (N = 10) who had asymmetrical unilateral CI performances. Additional data analysis was conducted to check if the four distinct patterns found in the current study could be explained by either demographic information (age) or hearing asymmetry (PTA difference between two ears). The results using a one-way ANOVA demonstrated that neither age nor PTA differences are significant factors to explain those binaural speech perception patterns within subject groups (Age: F3,78.9 = 1.62, p = 0.191; PTA difference: F3,71.6 = 0.657, p = 0.581).
The last possibility is that binaural interference could occur with non-optimal device parameters, which causes a mismatch in the timing or processing of auditory information between the two devices. In the clinic, CI mapping procedures typically require more time than HA fittings due to the complexity of electrically stimulated hearing, such as the need for electrode-specific adjustments (e.g., electrode impedance check, threshold/comfort level settings) and the iterative process due to the progressive adaptation required for optimal outcomes. This could be more challenging in bilateral device setup (bimodal CI+HA and bilateral CI) because clinicians should consider more factors such as loudness matching between two ears, increased subjective feedback demands, and interaction between devices. Future studies should include those possibilities to better understand the relationships between parameter optimization and bilateral device performance.
The findings in the present study provide insightful information; however, it is important to acknowledge certain limitations that may have influenced our results and their interpretation. In this study, the patients' medical records were collected over a sixteen-year duration for the retrospective period (between 2008 and 2024). Thus, the binaural speech perception patterns seen in the current study could not equally reflect the development of new technologies applied to the participants' hearing devices. For example, bilaterally synchronized signal processing between two CI devices could improve functional spatial hearing performance and reduce bilateral stimulation artifacts (Dennison et al., 2021). For the bimodal CI+HA users, new clinically available functions to program a mismatch in the processing delay between CI and the contralateral HA could also improve listeners' spatial hearing performance (Richter et al., 2024). Additionally, a recent development of anatomy-based fitting (such as OTOPLAN®, MED-EL, Innsbruck, Austria) could decrease the frequency-to-place mismatch caused by different tonotopic characteristics between two CIs (e.g., different insertion depths), and thereby improve speech perception performance in bilateral CI users (Kurz et al., 2023). It is also noted that the current data set (i.e., audiometric thresholds and speech perception scores) was collected only in the two audiology clinics in Kentucky, USA (University of Louisville Hospital and Heuser Hearing Institute), and the variability of repeated tests was not considered in this study, which could lead to limited generalizability and might not be able to generalize to broader populations. While it may not be possible to completely eliminate the inherent systematic errors of observational retrospective studies, a better understanding of binaural speech perception patterns in bilateral hearing device users could be provided by incorporating a rigorous study design, including accounting for confounding variables and acknowledging the limitations of the data.
In summary, to our knowledge, this is the first study to estimate binaural speech recognition patterns with a large sample size, including adult listeners with HA and/or CI devices. The results from this retrospective observational study have strong clinical implications for the management of cochlear implantation, especially for transitioning from bilateral HA to bimodal CI+HA and from bimodal CI+HA to bilateral CIs. The presence of both binaural averaging and binaural interference patterns implies that listening on two devices is not always better than one. Increased understanding of how those binaural disadvantages affect speech perception for hearing-impaired listeners is clinically essential for the future design of training- and device-based rehabilitative strategies to increase the benefits of binaural processing for speech perception in both quiet and noise. In addition, delving into the intricacies of individual binaural benefits is crucial for refining treatment strategies and tailoring services to the unique needs of each recipient, consequently bolstering speech perception and spatial hearing abilities. Such insights hold promise for addressing suboptimal outcomes, notably in mitigating instances of binaural interference.
Data availability statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Institutional Review Board (IRB) of the University of Louisville. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin because retrospective observational study.
Author contributions
YO: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. CS: Investigation, Writing – review & editing. PF: Investigation, Writing – review & editing. JK: Investigation, Writing – review & editing. CC: Investigation, Writing – review & editing. HB: Investigation, Writing – review & editing. LP: Investigation, Writing – review & editing. IE: Investigation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the American Speech-Language-Hearing Foundation and an internal funding source from the University of Louisville School of Medicine.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Allen, R. L., Schwab, B. M., Cranford, J. L., and Carpenter, M. D. (2000). Investigation of binaural interference in normal-hearing and hearing-impaired adults. J. Am. Acad. Audiol. 11, 494–500. doi: 10.1055/s-0042-1748138
Anderson, S. R., Burg, E., Suveg, L., and Litovsky, R. Y. (2024). Review of binaural processing with asymmetrical hearing outcomes in patients with bilateral cochlear implants. Trends Hear. 28, 1–25. doi: 10.1177/23312165241229880
Carter, A. S., Noe, C. M., and Wilson, R. H. (2001). Listeners who prefer monaural to binaural hearing aids. J. Am. Acad. Audiol. 12, 261–272. doi: 10.1055/s-0042-1745605
Ching, T. Y. C., Incerti, P., and Hill, M. (2004). Binaural benefits for adults who use hearing aids and cochlear implants in opposite ears. Ear Hear. 25, 9–21. doi: 10.1097/01.AUD.0000111261.84611.C8
Chmiel, R., Jerger, J., Murphy, E., Pirozzolo, F., and Tooley-Young, C. (1997). Unsuccessful use of binaural amplification by an elderly person. J. Am. Acad. Audiol. 8, 1–10.
Cox, R. M., Alexander, G. C., Johnson, J., and Rivera, I. (2012). Cochlear dead regions in typical hearing aid candidates: prevalence and implications for use of high-frequency speech cues. Ear Hear. 32, 339–348. doi: 10.1097/AUD.0b013e318202e982
Culling, J. F., Jelfs, S., Talbert, A., Grange, J. A., and Backhouse, S. S. (2012). The benefit of bilateral versus unilateral cochlear implantation to speech intelligibility in noise. Ear Hear. 33, 673–682. doi: 10.1097/AUD.0b013e3182587356
Dennison, S. R., Jones, H. G., Kan, A., and Litovsky, R. Y. (2021). The impact of synchronized cochlear implant sampling and stimulation on free-field spatial hearing outcomes: comparing the ciPDA research processor to clinical processors. Ear Hear. 43, 1262–1272. doi: 10.1097/AUD.0000000000001179
Dorman, M. F., and Gifford, R. H. (2010). Combining acoustic and electric stimulation in the service of speech recognition. Int. J. Audiol. 49, 912–919. doi: 10.3109/14992027.2010.509113
Gifford R. H, and Dorman, M. F. (2019) Bimodal hearing or bilateral cochlear implants? Ask the patient. Ear Hear. 40, 501–516. 10.1097/AUD.0000000000000657.
Gifford, R. H., and Stecker, G. C. (2020). Binaural cue sensitivity in cochlear implant recipients with acoustic hearing preservation. Hear. Res. 390:107929. doi: 10.1016/j.heares.2020.107929
Henkin Y. Waldman A. Kishon-Rabin L. (2007) The benefits of bilateral versus unilateral amplification for the elderly: are two always better than one? J. Basic Clin. Physiol. Pharmacol. 18, 201–216. 10.1515/JBCPP.2007.18.3.201
Holmes, A. E. (2003). Bilateral amplification for the elderly: are two aids better than one? Int. J. Audiol. 42, S63–S67. doi: 10.3109/14992020309074646
Jerger, J., Silman, S., Lew, H. L., and Chmiel, R. (1993). Case studies in binaural interference: converging evidence from behavioral and electrophysiologic measures. J. Am. Acad. Audiol. 4, 122–131.
Kurz, A., Herrmann, D., Hagen, R., and Rak, K. (2023). Using anatomy-based fitting to reduce frequency-to-place mismatch in experienced bilateral cochlear implant users: a promising concept. J. Pers. Med. 13:1109. doi: 10.3390/jpm13071109
Litovsky, R., Parkinson, A., Arcaroli, J., and Sammeth, C. (2006). Simultaneous bilateral cochlear implantation in adults: a multicenter clinical study. Ear Hear. 27, 714–731. doi: 10.1097/01.aud.0000246816.50820.42
McArdle, R. A., Killion, M., Mennite, M. A., and Chisolm, T. H. (2012). Are two ears not better than one? J. Am. Acad. Audiol. 23, 171–181. doi: 10.3766/jaaa.23.3.4
Mussoi B. S. S. Bentler R. A. (2017) Binaural interference the effects of age hearing loss. J. Am. Acad. Audiol. 28, 5–13. 10.3766/jaaa.15011
Oh, Y., Hartling, C. L., Srinivasan, N. K., Diedesch, A. C., Gallun, F. J., Reiss, L. A. J., et al. (2022). Factors underlying masking release by voice-gender differences and spatial separation cues in multi-talker listening environments in listeners with and without hearing loss. Front. Neurosci. 16:1059639. doi: 10.3389/fnins.2022.1059639
Oh, Y., Srinivasan, N. K., Hartling, C. L., Gallun, F. J., and Reiss, L. A. J. (2023). Differential effects of binaural pitch fusion range on the benefits of voice gender differences in a “cocktail party” environment for bimodal and bilateral cochlear implant users. Ear Hear. 44, 318–329. doi: 10.1097/AUD.0000000000001283
Potts, L. G., and Litovsky, R. Y. (2014). Transitioning from bimodal to bilateral cochlear implant listening: speech recognition and localization in four individuals. Am. J. Audiol. 23, 79–92. doi: 10.1044/1059-0889(2013/11-0031)
Reiss, L. A., Eggleston, J. L., Walker, E. P., and Oh, Y. (2016). Two ears are not always better than one: mandatory vowel fusion across spectrally mismatched ears in hearing-impaired listeners. J. Assoc. Res. Otolaryngol. 17, 341–356. doi: 10.1007/s10162-016-0570-z
Richter, M. E., Rooth, M. A., and Dillon, M. T. (2024). Influence of matching the processing delays of cochlear implant and hearing aid devices for bimodal listeners on speech recognition in noise. Am. J. Audiol. 33, 1350–1355. doi: 10.1044/2024_AJA-24-00026
Spahr, A. J., Dorman, M. F., Litvak, L. M., Van Wie, S., Gifford, R. H., Loizou, P. C., et al. (2012). Development and validation of the AzBio sentence lists. Ear Hear. 33, 112–117. doi: 10.1097/AUD.0b013e31822c2549
van Hoesel, R. J. M. (2004). Exploring the benefits of bilateral cochlear implants. Audiol. Neurotol. 9 234–246. doi: 10.1159/000078393
Walden, T. C., and Walden, B. E. (2005) Unilateral versus bilateral amplification for adults with impaired hearing. J. Am. Acad. Audiol. 16, 574–584. doi: 10.3766/jaaa.16.8.6
Yawn, R. J., O'Connell, B. P., Dwyer, R. T., Sunderhaus, L. W., Reynolds, S., Haynes, D. S., et al. (2018). Bilateral cochlear implantation versus bimodal hearing in patients with functional residual hearing: a within-subjects comparison of audiologic performance and quality of life. Otol. Neurotol. 39, 422–427. doi: 10.1097/MAO.0000000000001750
Keywords: binaural benefit, better ear, binaural averaging, binaural interference, cochlear implant, hearing aid, speech perception
Citation: Oh Y, Sereno C, Friggle P, Kinder J, Cuthbertson C, Borton H, Pollock L and Edwards I (2025) Binaural speech perception patterns in adult listeners with hearing aids and/or cochlear implants: a retrospective observational study. Front. Audiol. Otol. 3:1613714. doi: 10.3389/fauot.2025.1613714
Received: 17 April 2025; Accepted: 01 August 2025;
Published: 01 September 2025.
Edited by:
Ilona Anderson, MED-EL, AustriaReviewed by:
Brian Richard Earl, University of Cincinnati, United StatesSasan Dabiri, Northern Ontario School of Medicine University, Canada
Daniel Polterauer, LMU Munich University Hospital, Germany
Copyright © 2025 Oh, Sereno, Friggle, Kinder, Cuthbertson, Borton, Pollock and Edwards. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yonghee Oh, eW9uZ2hlZS5vaEBsb3Vpc3ZpbGxlLmVkdQ==