 Cosima F. Lukas1
Cosima F. Lukas1 Daniela Ivansic1
Daniela Ivansic1 Gerlind Schneider1Christina Lemhöfer2
Gerlind Schneider1Christina Lemhöfer2 Orlando Guntinas-Lichius1
Orlando Guntinas-Lichius1 Christian Dobel1,3*
Christian Dobel1,3*- 1Department of Otorhinolaryngology, Jena University Hospital, Friedrich Schiller University Jena, Jena, Germany
- 2Institute for Physical and Rehabilitative Medicine, Jena University Hospital, Friedrich Schiller University Jena, Jena, Germany
- 3Department of Linguistics and Translation, City University of Hong Kong, Kowloon, Hong Kong SAR, China
Introduction: Tinnitus is a chronic condition that can cause considerable psychological distress. While clinical guidelines recommend interdisciplinary treatment, long-term effects remain underexplored. This study evaluated tinnitus-related distress over a 5-year follow-up period following intensive interdisciplinary treatment in patients experiencing chronic bothersome tinnitus.
Methods: This cohort study analyzed a representative sample of patients with chronic, bothersometinnitus (n = 747) who underwent a 5-day intensive interdisciplinary treatment, including cognitive behavioral therapy, sound enrichment via hearing aids, ENT and medical rehabilitation diagnostics, and physiotherapy. Long-term follow-up assessments were conducted at an average of 5 years post-treatment with a response rate of 48%. Tinnitus-related distress was assessed using the Tinnitus Questionnaire. Data were missing completely at random.
Results: Tinnitus-related distress was significantly reduced post-treatment and remained stable across follow-up measurements (p < 0.001, d = 1.33), regardless of initial symptom severity [F(10, 1, 470) = 5.6, p < 0.001, η2 = 0.02]. Psychosocial factors explained 47% of the variance in tinnitus-related distress at follow-up [F(4, 335) = 75.77, p = 0.000, R2 = 0.47].
Discussion: Sustained improvements in tinnitus-related distress were observed over a 5-year follow-up period after the intervention. These findings show that chronic tinnitus can be sustainably managed within a brief treatment period, emphasizing the need for personalized, interdisciplinary strategies to accommodate patient heterogeneity.
1 Introduction
Subjective tinnitus is described as the perception of sound without any external auditory stimulus and affects a substantial proportion of the general population (Eggermont and Roberts, 2004; Baguley et al., 2013). While inconsistencies in the definition of tinnitus, heterogeneous assessment methods, and geographical biases cause variation in epidemiological studies (Henry et al., 2020), the prevalence of chronic tinnitus is estimated to be approximately 14%, increasing with age (Biswas et al., 2022; Jarach et al., 2022). While tinnitus symptoms are often well-compensated, 1.2 to 2% of the population experiences severe, bothersome tinnitus, which is associated with considerable psychological distress, leading patients to seek treatment (Biswas et al., 2022; Jarach et al., 2022). Severe tinnitus-related distress often occurs with mental health-related comorbidities, such as depression, anxiety, and somatoform disorders (Pinto et al., 2014; Stegeman et al., 2021; Ivansic et al., 2019). Affective responses to chronic tinnitus are reflected pathophysiologically, as tinnitus is considered a consequence of structural alterations, maladaptive neuroplasticity, and alterations in functional connectivity as a reaction to peripheral hearing loss (Kang and Zheng, 2024; Elgoyhen et al., 2015; Weisz et al., 2005). It involves a complex network of interacting brain regions in auditory and non-auditory systems, including frontal regions, the limbic system, and, more specifically, depression and distress-related networks (Paraskevopoulos et al., 2019; Leaver et al., 2016; Salvari et al., 2023; Besteher et al., 2019). Tinnitus, along with hyperacusis—defined as physical discomfort or pain from loud sounds—can occur without clinically relevant hearing loss and may reflect altered auditory processing with desynchronized or hyperactive bottom-up processing, explaining changes in higher-order brain networks (Xie et al., 2025). Although tinnitus generation is pathophysiologically not entirely understood, guidelines for treatment exist and revolve around a multidisciplinary combination of psychotherapeutic interventions, i.e., cognitive behavioral therapy (CBT), counseling, and hearing aids (Mazurek et al., 2022a; Cima et al., 2019). Multiple systematic reviews and meta-analyses provide evidence for the effectiveness of CBT in reducing tinnitus-related distress (Hesser et al., 2011; Landry et al., 2020; Martinez Devesa et al., 2007). Owing to the complexity and heterogeneity in tinnitus perception, etiology, and related comorbidities (Cederroth et al., 2019), multidisciplinary and personalized treatment strategies are indicated (Mazurek et al., 2022b; Taylor et al., 2020). However, treatment responses are characterized by large interindividual variations (Cederroth et al., 2019; Mueller et al., 2024). The heterogeneity in tinnitus has also been hypothesized to hinder attempts at predicting tinnitus-related distress and treatment response (Cederroth et al., 2019; Biswas et al., 2022; Ivansic et al., 2022). Long-term investigations of treatments for tinnitus are rare, with some notable exceptions (Brueggemann et al., 2018).
The Jena Interdisciplinary Treatment for Tinnitus JITT (Ivansic et al., 2017a) represents a specialized interdisciplinary day-clinic approach. The structured program focuses on evidence-based, individualized interventions following the German S3 guidelines for chronic tinnitus (Mazurek et al., 2022a). It integrates psychotherapeutic, medical (otorhinolaryngology, physical medicine and rehabilitation) as well as audiological [hearing aids and Terzo® hearing therapy (Funk et al., 2008)] and physiotherapeutic interventions. For a detailed description of the treatment regimen, see (Ivansic et al., 2017a).
The effectiveness of the JITT has been investigated for up to 6 months after therapy, indicating promising outcomes with significant improvements in tinnitus severity and associated psychological distress (Ivansic et al., 2017a). The current work examines its long-term treatment results by presenting the findings from a 5-year follow-up study of patients treated with the JITT. The study examines whether treatment outcomes are sustained 5 years after treatment and whether treatment success can be observed across all levels of tinnitus-related distress. Additionally, the study aims to identify factors that could account for the variation in therapy success at follow-up.
2 Materials and methods
2.1 Participants and datasets
The study involved patients from a dataset containing demographic, tinnitus-, hearing- and mental health-related data from 747 patients who attended therapy at the JITT between 2013 and 2017. Data were assessed before treatment (t0), at the beginning (t1) and end (t2) of five consecutive treatment days, as well as 2 weeks (t3) and 6 months (t4) after treatment. Patients were between 18 and 81 years old (55.7 ± 11.6 years). At t0, 66.1% (N = 494) presented with decompensated tinnitus. The long-term follow-up questionnaire (t5) was assessed in 2020, with a mean of 5 years (range 3–7 years) post-treatment and a response rate of 48% (N = 361). Descriptive data from both participants and non-participants can be obtained from Table 1.
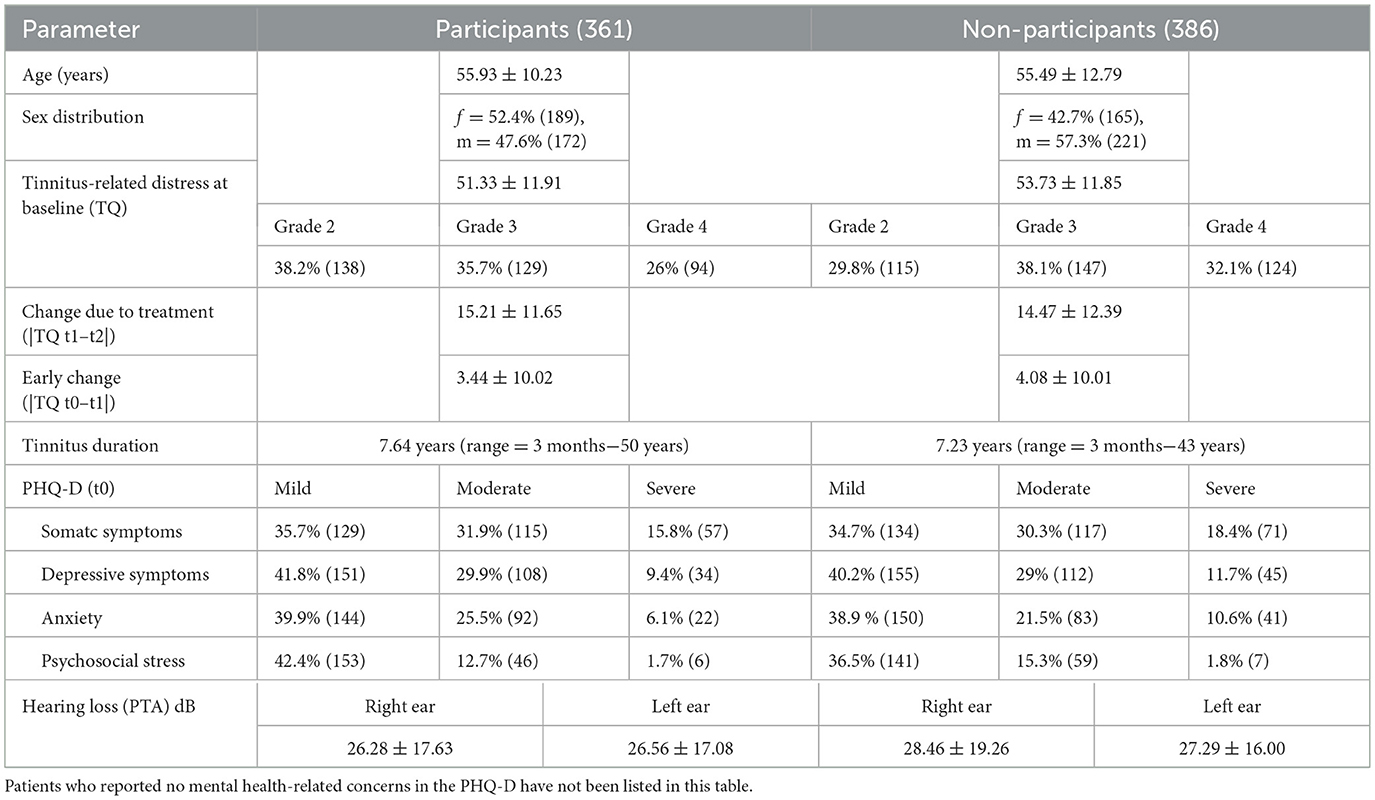
Table 1. Baseline characteristics of patients who completed the 5-year follow-up questionnaire compared with non-participants, M ± SD (N).
This study protocol was reviewed and approved by the Jena University Hospital ethics committee, approval number 4366-03/15. Written informed consent was obtained from all patients to participate in the study. This study was performed in accordance with the Declaration of Helsinki and following the recommendations of the ICH harmonized tripartite guidelines for Good Clinical Practice.
2.2 Missing data mechanism
To determine whether the patient's willingness to respond in the 5-year follow-up investigation depended on the variables in the dataset, Little's (1988) test was conducted on the full dataset (N = 747) with p = 0.102. Therefore, we conclude that the data are missing completely at random. Patients answered the survey questionnaire at t5 independently of their age, sex, initial tinnitus-related distress and therapy success (change due to treatment between t1 and t2), duration of tinnitus awareness, tinnitus lateralization, or initial psychological symptom severity (somatization, depressiveness, anxiety, and psychosocial stress), as assessed with the Patient Health Questionnaire at t0 (PHQ-D) (Spitzer et al., 1999).
2.3 Intervention and inclusion criteria
Patients received interdisciplinary treatment, as described previously (Ivansic et al., 2017a). The JITT approach aims to achieve habituation, improve quality of life, and reduce perceived tinnitus-related distress through comprehensive diagnostics, daily counseling, CBT, mindfulness-based interventions, physiotherapy, and relaxation exercises. The appointment at t0 involves a preliminary screening, excluding potentially pathological or malignant causes of tinnitus, and a short psychoeducational tinnitus counseling. All patients receive individually fitted hearing aids between t1 and t3 using a standardized DSLchild algorithm-based setting (Boecking et al., 2022).
The inclusion criteria for treatment require a clinical diagnosis of chronic tinnitus with a minimum persistence of 3 months, clinically significant tinnitus-related distress as determined by a clinical psychologist in a semi-structured interview, and a TQ score above 30 indicating moderate to severe levels of tinnitus-related distress. Patients with acute suicidality and severe psychiatric conditions that impede their participation in group therapy are not included in treatment. All patients were 18 years of age or older and were proficient in the German language.
2.4 Main outcome measures
To measure treatment-related changes in tinnitus-related distress, the Tinnitus Questionnaire (TQ) (Goebel and Hiller, 1998) is a standard psychometric instrument. It considers multifaceted aspects of tinnitus impairment, including the subscales of emotional and cognitive distress, intrusiveness, hearing problems, sleep disturbances, and somatic complaints, while showing evidence for high test–retest reliability and internal consistency (Goebel and Hiller, 1998). The overall sum score of all 52 items ranges between 0 and 84. A sum score below 30 implies mild tinnitus severity (grade 1), 31–46 moderate tinnitus-related distress (grade 2), 47–59 severe tinnitus-related distress (grade 3), and 60–84 very severe tinnitus-related distress (grade 4). Grades 1 and 2 are considered compensated symptom levels, indicating mild secondary symptoms and bothersome tinnitus under the experience of mental or physiological strain. Grades 3 and 4 denote decompensated symptom levels indicating ongoing tinnitus annoyance and psychological distress from cognitive, emotional, and physiological impairment to severe psychological decompensation. Treatment is indicated beginning with severity grade 2, if patients are at risk of decompensation, based on clinical impression.
The long-term follow-up questionnaire was sent in paper-pencil form to all patients who participated in therapy between 2013 and 2017 and provided informed written consent. Self-reported demographic data, tinnitus- and treatment-related information, self-reported difficulty in speech comprehension (DSC), and perceived noise sensitivity were collected.
Subjective DSC was assessed via a 12-item self-report questionnaire (developed by Terzo©) to investigate perceived impairment and associated listening effort in speech recognition in various (adverse) listening environments (e.g., “I have difficulty engaging in a conversation with one person in a quiet environment.” “It is tiring for me to follow the conversation when there are several people at the table.” “In a noisy environment, I have to concentrate particularly hard to understand my conversation partner.”).
Perceived noise sensitivity was measured via a single-item self-report questionnaire (“Do you find yourself particularly sensitive to noise? For instance, are you bothered by sounds that others do not perceive as too loud?”).
2.5 Statistical analysis
Removing missing cases from the participants' dataset (N = 361) resulted in two different subsets used for the analyses. The first dataset consists of N = 297 complete cases containing TQ scores across all six measurement time points (t0–t5). The second dataset comprised N = 340 patients with full information on the TQ scores at t0, t1, t2, and t5, as well as the variables age, sex, tinnitus-related distress at baseline, improvement due to counseling [“early change” (Ivansic et al., 2017a) improvement in the TQ score between t0 and t1], number of tinnitus-specific treatments before and after the JITT, including the number of new behaviors adopted after treatment, use of hearing aids at t5, baseline mental health-related variables (PHQ-D somatic symptoms, depressiveness, anxiety and psychosocial stress), mean hearing loss at t0 and self-reported DSC and perceived noise sensitivity at t5. The baseline characteristics for both sub-datasets can be obtained from Table 2.
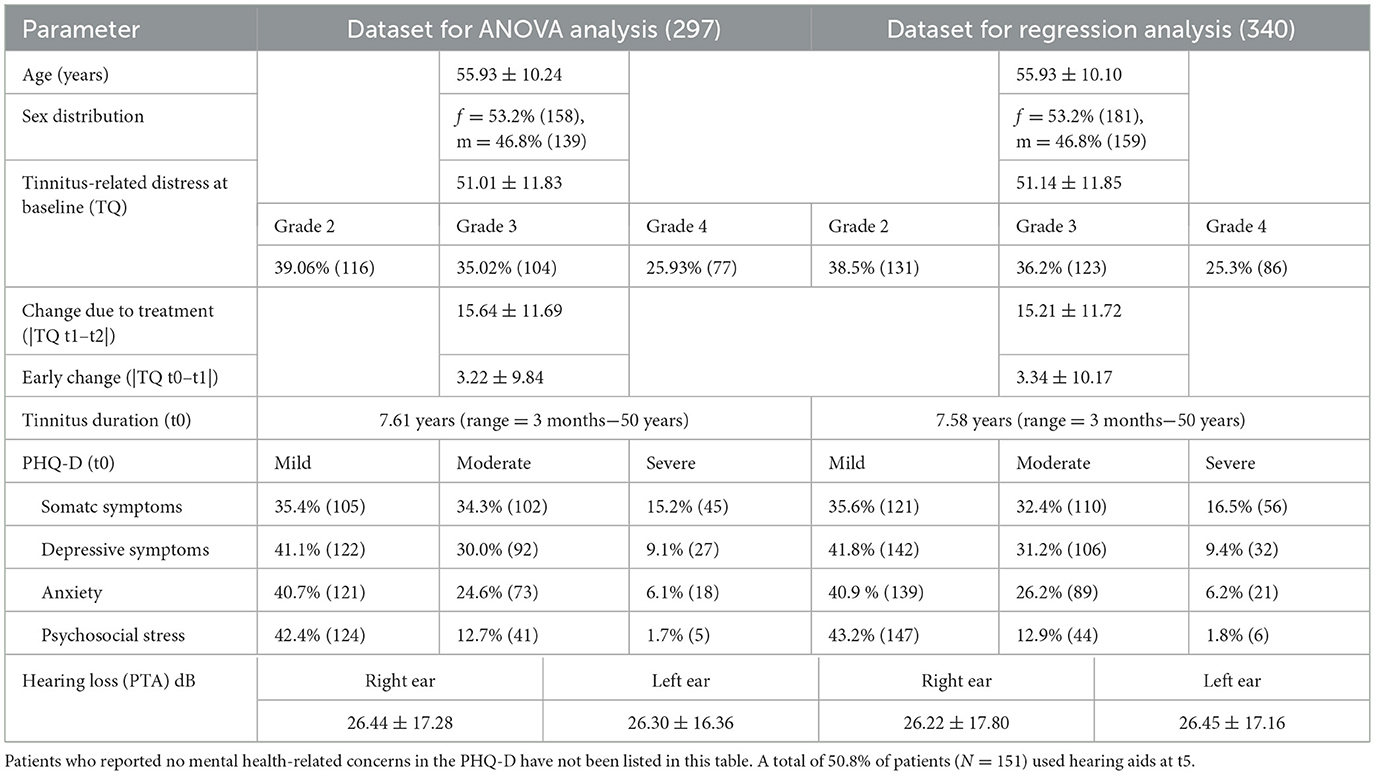
Table 2. Baseline characteristics of patients who completed the 5-year follow-up questionnaire compared between both sub-datasets for analysis, M ± SD (N).
Repeated-measures ANOVA (rmANOVA) was used to investigate the main effect of time across all complete cases (N = 297). This analysis was followed by a mixed ANOVA and Bonferroni-corrected post-hoc tests regarding group differences across time. The sample was categorized into three severity grades based on the TQ score at t0. Additionally, linear regression models with backward selection were calculated on N = 340 cases using the R-packages “caret,” (Kuhn, 2008) “leaps,” (Lumley and Miller, 2020) and “MASS” (Venables and Ripley, 2002) to identify the parsimonious model for explaining variance in tinnitus-related distress at t5, including demographic, tinnitus-, hearing-, and mental health-related indicators. Two independent variables (self-reported DSC and perceived noise sensitivity) were measured at t5. A regression analysis was performed to assess the relationships between these variables and the experienced tinnitus-related distress cross-sectionally. Using a maximum of 15 independent variables, the best model for each number of factors was identified. The average prediction error (RMSE) for each model was calculated via 10-fold cross-validation. The model with the lowest RMSE was then selected as the best and final model.
3 Results
The rmANOVA results revealed a significant main effect of time [F(3.59, 1062.8) = 234.69, p < 0.001, η2 = 0.22]. Differences occurred between t0 and t1, indicating a significant early change with a small to medium effect size (p < 0.001, d = 0.33). A significant treatment-related change occurred between t1 and t2, with a large effect size (p < 0.001, d = 1.33). On average, patients experienced a 19-point improvement on the TQ scale between t0 and t2, which transformed decompensated to compensated symptom levels in most cases (see Table 3). From the first follow-up consultation 2 weeks after treatment (t2), no significant changes occurred up to the 5-year follow-up at t5, suggesting a stable long-term effect.
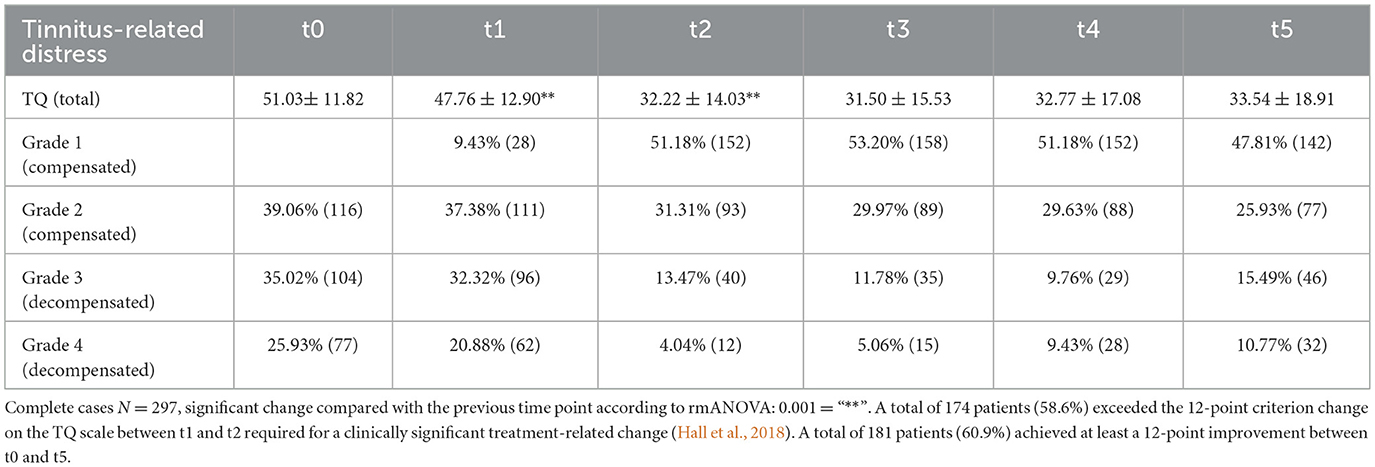
Table 3. Tinnitus-related distress (TQ) and distribution of severity levels among patients (N = 297) across all time points, M ± SD (N).
To investigate differences in change trajectories for patients starting therapy with distinct levels of tinnitus-related distress, a mixed ANOVA was performed for the TQ. For a visual representation of the means and standard deviations in tinnitus-related distress for each group across all time points, refer to Figure 1.
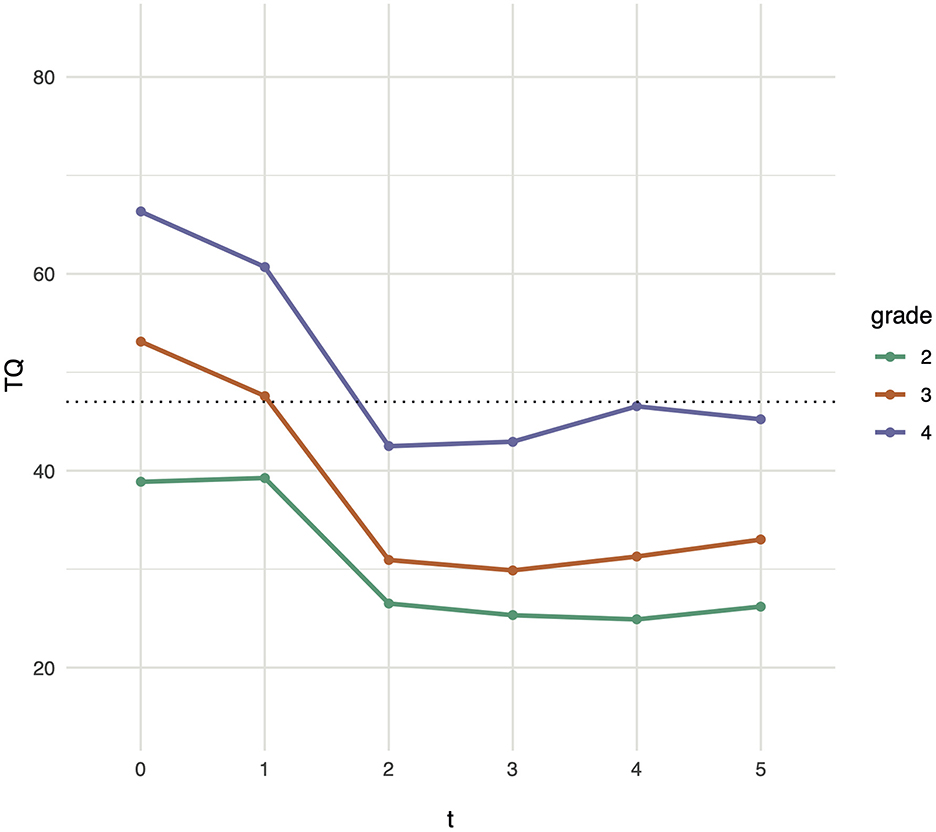
Figure 1. Tinnitus-related distress trajectories. Changes in tinnitus-related distress are depicted for participants beginning treatment with compensated (grade 2) and decompensated (grades 3 and 4) tinnitus, as measured by the TQ at t1. The dotted line indicates the cutoff between compensated and decompensated tinnitus based on the TQ. Assessments were conducted at the initial screening (t0), at the start of treatment (t1, on average 3 months after screening), and immediately following the five-day intervention (t2). Follow-up assessments were completed 3 weeks (t3), 6 months (t4), and on average 5 years (t5) after treatment. Mean values and standard deviations are provided in Table 3.
A comparison of the change in tinnitus-related distress across severity grades revealed a significant interaction effect between time and tinnitus severity [Greenhouse Geisser F(10, 1, 470) = 5.6, p < 0.001, η2 = 0.02]. Bonferroni-corrected pairwise comparisons indicated a highly significant change due to treatment between t1 and t2 at all severity levels [grade 2 (7.54, p < 0.001), grade 3 (9.41, p < 0.001), and grade 4 (8.81, p < 0.001)]. From t2, there was no significant change in any severity grade up to the five-year follow-up. The significant early change between t0 and t1 occurred only for severity grade 3 (3.13, p < 0.05). The group means differ significantly across all time points [t0: grade 2 vs. 3 (−8.23, p < 0.001), grade 2 vs. 4 (−14.5, p < 0.001), grade 3 vs. 4 (−6.86, p < 0.001); t1: grade 2 vs. 3 (−4.81, p < 0.001), grade 2 vs. 4 (−11.4, p < 0.001), grade 3 vs. 4 (−6.81, p < 0.001); t2: grade 2 vs. 3 (−2.55, p < 0.05), grade 2 vs. 4 (−8.46, p < 0.001), grade 3 vs. 4 (−6.01, p < 0.001); t3: grade 2 vs. 3 (−2.63, p < 0.05), grade 2 vs. 4 (−9.33, p < 0.001), grade 3 vs. 4 (−6.79, p < 0.001); t4: grade 2 vs. 3 (−3.69, p < 0.001), grade 2 vs. 4 (−11.5, p < 0.001), grade 3 vs. 4 (−7.93, p < 0.001); t5: grade 2 vs. 3 (−3.93, p < 0.001), grade 2 vs. 4 (−10.1, p < 0.001), grade 3 vs. 4 (−6.34, p < 0.001)], indicating significant treatment-related changes on all severity levels, while the ranking order of tinnitus-severity remains unchanged over time across groups.
The optimal model for explaining variance in tinnitus-related distress at the 5-year follow-up (t5), identified through linear regression models with backward selection, was highly significant, with [F(4, 335) = 75.77, p = 0.000]. The model explained 47% of the variance in tinnitus-related distress at t5 (adjusted R2 = 0.47). The change trajectory in tinnitus-related distress can be predicted using baseline tinnitus-related distress [t(335) = 7.06, p = 0.000] as well as early change [t(335) = 2.89, p < 0.001], indicating that patients who started treatment with high levels of tinnitus-related distress also tended to experience increased distress levels 5 years after treatment, supporting the findings from the mixed ANOVA. Here, higher values in early change indicate less improvement in tinnitus-related distress in the intended direction between t0 and t1, suggesting increased tinnitus-related distress at t5 if patients had a smaller response to counseling. With respect to hearing-related indicators, both perceived noise sensitivity, t(335) = 2.91, p < 0.001, and subjective DSC, t(335) = 9.39, p = 0.000, were identified as significant factors. These findings indicate that tinnitus-related distress tends to increase with more severe levels of perceived noise sensitivity and when more severe DSC is experienced. The remaining factors, such as age, sex, the number of tinnitus-specific treatments before and after treatment with the JITT, the number of new behaviors adopted after treatment, the use of hearing aids at t5, baseline mental health-related variables (PHQ-D somatic symptoms, depressiveness, anxiety and psychosocial stress) as well as the mean hearing loss at t0, were not included in the best prediction model after cross-validation. The variance inflation factor (VIF) scores were < 5 for all factors, indicating no evidence of multicollinearity.
4 Discussion
The present data show a stable long-term reduction in tinnitus-related distress, indicating sustained positive treatment outcomes at the 5-year follow-up This program can facilitate long-lasting transformations, regardless of the initial severity of tinnitus-related distress and despite its short duration.
These findings support the use of interdisciplinary, multimodal interventions that target tinnitus distress alongside psychological and somatic symptoms, as this approach may produce synergistic improvements across tinnitus-related and comorbid symptoms. A previous analysis of two large datasets from two different tinnitus-specific treatment centers revealed a bidirectional relationship between tinnitus-related distress and depression while also highlighting the relevance of somatization and stress-related symptoms (Lukas et al., 2024). This suggests that tinnitus-related and psychological distress are reciprocally interconnected, with changes in one condition influencing the other over the course of treatment. In light of these findings, JITT exemplifies an approach that integrates tinnitus-specific, psychological, and somatic components, thereby fostering improvements across interconnected symptoms.
This biopsychosocial perspective aligns closely with several cognitive and neurophysiological frameworks, which highlight the interaction of auditory, cognitive, and emotional processes (Hallam et al., 1984; Ghodratitoostani et al., 2024, 2016; Jastreboff, 1990). The common denominator of these tinnitus models is the idea that tinnitus becomes a problem not because of the sound itself, but because of neurophysiologically reflected cognitive-emotional appraisal processes. The Conceptual Cognitive Framework (Ghodratitoostani et al., 2024), for instance, emphasizes the role of maladaptive attention and cognitive-emotional appraisal in developing and maintaining tinnitus-related distress. Negative, dysfunctional, or catastrophizing thought patterns provoke arousal and are often associated with emotional distress, depression, anxiety, increased tinnitus-related distress, and lower ratings in quality of life. They drive the maintenance of selective attention, monitoring, and counterproductive safety behaviors whereby the subjective tinnitus loudness perception increases. Dysfunctional cognitive processing thereby hinders habituation to the tinnitus percept (Hallam et al., 1984).
JITT aids in modifying this attentional bias through attentional defocusing and audiological distraction from the tinnitus percept using hearing aids. An improvement in cognitive and emotional appraisal is achieved through CBT, primarily through restructuring negative thought patterns, psychoeducation, and relaxation exercises. JITT explicitly targets dysfunctional coping strategies and uses mindfulness-based interventions to facilitate the process of habituation by focusing on acceptance. Treatment modules focusing on emotion regulation help correct a distorted tinnitus perception, while hearing aids also reduce the subjective loudness or intrusiveness of tinnitus.
The long-term improvements observed in our cohort suggest that addressing these multiple domains simultaneously facilitates long-term reduction of tinnitus-related distress.
Early change refers to the phenomenon in which patients experience a reduction in symptoms early at the beginning of their treatment. It is a well-investigated predictor in psychotherapy and is strongly associated with better and more sustainable treatment outcomes (Haas et al., 2002; Schibbye et al., 2014). The results reported here indicate that patients who experienced early change showed better treatment outcomes at t5. In this context, early change describes the patients' reaction to psychoeducational counseling alone between t0 and t1 and occurs significantly in severity grade 3. The factors contributing to early change are not fully understood, but relevant patient characteristics have been identified, among other hypotheses (Erekson et al., 2018). Patients with more severe symptoms and higher levels of resilience, characterized by an internal locus of control, hope, confidence in their ability to change, and motivation to engage in therapy, appear more likely to experience early change (Erekson et al., 2018). This could explain why the subgroup with moderately severe symptoms experienced a significant early change in this sample.
The present study highlights the association between perceived noise sensitivity and tinnitus-related distress at t5, despite the use of a single-item measure. Noise sensitivity is described as increased reactivity to sounds, leading to considerable discomfort regardless of loudness (Bigras et al., 2024). Patients reporting higher noise sensitivity experienced more severe tinnitus-related distress at t5. Both noise sensitivity and hyperacusis, are conditions associated with decreased sound tolerance (Bigras et al., 2024) and contribute to the heterogeneity of tinnitus outcomes. Research has indicated that 30–50% of tinnitus patients report comorbid hyperacusis, and those with both conditions report higher distress levels than those with tinnitus alone (Cederroth et al., 2020; Refat et al., 2021). Refat et al. (2021) consider hyperacusis to be the main cause of long-term tinnitus-related distress, with their findings suggesting that patients with both tinnitus and hyperacusis experience increased tinnitus loudness over time, whereas those with tinnitus alone report a reduction in tinnitus loudness. Danioth et al. (2020) describe tinnitus to be related to multisensory environmental hypersensitivity, with anxiety as a predictor of this environmental vulnerability. Although hyperacusis and noise sensitivity share a conceptual overlap, they should not be used interchangeably (Bigras et al., 2024). The significance of the presented results should be reinvestigated in the future via validated psychometric instruments to disentangle the specific contributions of noise sensitivity and hyperacusis to long-term tinnitus distress.
Subjective DSC is commonly reported in patients with tinnitus and cannot be exclusively attributed to hearing loss (Ivansic et al., 2017b; Tai and Husain, 2019; Vielsmeier et al., 2016). Cognitive control of attention and emotion is proposed to play a substantial role. The perception of tinnitus consumes attentional capacity, leading to a deficiency in executive attention that can hinder speech recognition in noise (Tai and Husain, 2019). Subjective DSC emerges as an important factor in explaining variance in tinnitus-related distress at t5 and, therefore, influences the overall distress associated with tinnitus, which is evident independently of the level of hearing loss. This is supported by brain imaging studies showing alterations in the attention network in patients with chronic tinnitus. According to a resting-state fMRI study, changes in the connectivity patterns of the default mode and dorsal attention network were correlated with tinnitus severity, supporting a relationship between tinnitus severity, cognitive control, and speech in noise recognition (Schmidt et al., 2017). Furthermore, communication difficulties and perceived social estrangement or isolation might perpetuate the bidirectional relationship between depressive symptoms and tinnitus-related distress, exacerbating symptoms (Lukas et al., 2024). Although hearing aids were not a significant predictor of tinnitus-related distress in this study due to self-selection bias, the findings reiterate the importance of hearing aids and improved speech comprehension in tinnitus management.
The long-term follow-up assessment took place during the COVID-19 pandemic. The simultaneous governmental lockdown in Germany potentially represented an environmental stressor affecting tinnitus-related distress due to increased psychological distress, social isolation, and a lack of distraction from tinnitus noise (Schlee et al., 2020). The pandemic's impact on tinnitus-related distress has been characterized by considerable heterogeneity, depending on individual coping strategies and personality traits (Schlee et al., 2020; Fioretti et al., 2022). Consequently, the COVID-19 pandemic and lockdown may have further influenced the variability in tinnitus-related distress observed at t5.
4.1 Limitations
The absence of repeated PHQ-D assessments limited our observation of the dynamic interactions between tinnitus-related distress and psychological factors over time. Although some psychological measures may have explained variance at t5, they were collected at intervals too far from the follow-up assessment, potentially limiting their predictive power due to state dependency. The absence of repeated psychological assessments also limited our ability to disentangle sustained treatment effects from independent fluctuations in comorbid psychological conditions over the follow-up period. Furthermore, the use of validated psychometric instruments to assess noise sensitivity and hyperacusis would enhance our understanding of their role in tinnitus-related distress in the future. Regarding the risk of non-response bias, Little's MCAR test indicated that missingness was unrelated to baseline factors or treatment response (t1–t2). However, it cannot account for any prospective events or changes that occurred in the intervening years leading up to t5. While additional treatments during the 5-year follow-up may have introduced confounding effects, JITT educates patients to make more informed healthcare choices, enabling continued engagement in effective interventions.
4.2 Conclusions
This study provides evidence for the sustained benefits of an interdisciplinary treatment regimen for chronic, bothersome tinnitus. The highly variable pathways of disorder development emphasize the remarkable heterogeneity in tinnitus patients, highlighting the need for individualized treatment approaches. Active and conscious patient involvement is regarded as a guiding principle in effective tinnitus management, aligning with a patient-centered perspective on systems medicine, viewing individuals as active agents in managing their symptoms rather than passive recipients of treatment. The findings emphasize the role of speech comprehension and noise sensitivity in tinnitus-related distress, illustrating the importance of audiological interventions within an interdisciplinary framework to personalize treatment further.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Friedrich-Schiller-University Jena Faculty of Medicine, Jena University Hospital, Friedrich-Schiller-University Jena, Jena, Germany. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CFL: Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. DI: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. GS: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. CL: Data curation, Writing – original draft, Writing – review & editing. OG-L: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. CD: Conceptualization, Data curation, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the German Research Foundation (DO 711/10-1, 10-3; JU 445/10-3).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Baguley, D., McFerran, D., and Hall, D. (2013). Tinnitus. Lancet 382, 1600–1607. doi: 10.1016/S0140-6736(13)60142-7
Besteher, B., Gaser, C., Ivanšić, D., Guntinas-Lichius, O., Dobel, C., Nenadić, I., et al. (2019). Chronic tinnitus and the limbic system: reappraising brain structural effects of distress and affective symptoms. Neuroimage: Clin. 24:101976. doi: 10.1016/j.nicl.2019.101976
Bigras, C., Theodoroff, S. M., Thielman, E. J., and Hebert, S. (2024). Noise sensitivity or hyperacusis? Comparing the Weinstein and Khalfa questionnaires in a community and a clinical samples. Hear. Res. 445:108992. doi: 10.1016/j.heares.2024.108992
Biswas, R., Lugo, A., Akeroyd, M. A., Schlee, W., Gallus, S., Hall, D. A., et al. (2022). Tinnitus prevalence in Europe: a multi-country cross-sectional population study. Lancet Reg. Health - Eur. 12:100250. doi: 10.1016/j.lanepe.2021.100250
Boecking, B., Rausch, L., Psatha, S., Nyamaa, A., Dettling-Papargyris, J., Funk, C., et al. (2022). DSL(child)-algorithm-based hearing aid fitting can improve speech comprehension in mildly distressed patients with chronic tinnitus and mild-to-moderate hearing loss. J. Clin. Med. 11:5244. doi: 10.3390/jcm11175244
Brueggemann, P., Otto, J., Lorenz, N., Schorsch, S., Szczepek, A. J., Bocking, B., et al. (2018). Long-term changes in multimodal intensive tinnitus therapy: a 5 year follow-up. HNO 66, 34–38. doi: 10.1007/s00106-017-0463-4
Cederroth, C. R., Gallus, S., Hall, D. A., Kleinjung, T., Langguth, B., Maruotti, A., et al. (2019). Towards an Understanding of Tinnitus Heterogeneity. Front. Aging Neurosci. 11:53. doi: 10.3389/fnagi.2019.00053
Cederroth, C. R., Lugo, A., Edvall, N. K., Lazar, A., Lopez-Escamez, J. A., Bulla, J., et al. (2020). Association between hyperacusis and tinnitus. J. Clin. Med. 9:2412. doi: 10.3390/jcm9082412
Cima, R. F. F., Mazurek, B., Haider, H., Kikidis, D., Lapira, A., Norena, A., et al. (2019). A multidisciplinary European guideline for tinnitus: diagnostics, assessment, and treatment. HNO 67, 10–42. doi: 10.1007/s00106-019-0633-7
Danioth, L., Brotschi, G., Croy, I., Friedrich, H., Caversaccio, M. D., Negoias, S., et al. (2020). Multisensory environmental sensitivity in patients with chronic tinnitus. J. Psychosom. Res. 135:110155. doi: 10.1016/j.jpsychores.2020.110155
Eggermont, J. J., and Roberts, L. E. (2004). The neuroscience of tinnitus. Trends Neurosci. 27, 676–682. doi: 10.1016/j.tins.2004.08.010
Elgoyhen, A. B., Langguth, B., De Ridder, D., and Vanneste, S. (2015). Tinnitus: perspectives from human neuroimaging. Nat. Rev. Neurosci. 16, 632–642. doi: 10.1038/nrn4003
Erekson, D. M., Clayson, R., Park, S. Y., and Tass, S. (2018). Therapist effects on early change in psychotherapy in a naturalistic setting. Psychother Res. 30, 68–78. doi: 10.1080/10503307.2018.1556824
Fioretti, A., Natalini, E., Triggianese, G., Eibenstein, R., Angelone, A. M., Lauriello, M., et al. (2022). Impact of the COVID-19 lockdown on patients with chronic tinnitus-preliminary results. Audiol. Res. 12, 327–336. doi: 10.3390/audiolres12030034
Funk, C., Wohlfeil, J., Jauch, E., and Sorg, R. (2008). Manual der Terzo®Gehörtherapie. Unpublished manual.
Ghodratitoostani, I., Vaziri, Z., Miranda Neto, M., de Giacomo Carneiro Barros, C., Delbem, A. C. B., Hyppolito, M. A., et al. (2024). Conceptual framework for tinnitus: a cognitive model in practice. Sci. Rep. 14:7186. doi: 10.1038/s41598-023-48006-7
Ghodratitoostani, I., Zana, Y., Delbem, A. C., Sani, S. S., Ekhtiari, H., Sanchez, T. G., et al. (2016). Theoretical tinnitus framework: a neurofunctional model. Front. Neurosci. 10:370. doi: 10.3389/fnins.2016.00370
Goebel, G., and Hiller, W. (1998). Tinnitus-Fragebogen (TF): ein Instrument zur Erfassung von Belastung und Schweregrad bei Tinnitus. Göttingen: Hogrefe.
Haas, E., Hill, R. D., Lambert, M. J., and Morrell, B. (2002). Do early responders to psychotherapy maintain treatment gains? J. Clin. Psychol. 58, 1157–1172. doi: 10.1002/jclp.10044
Hall, D. A., Mehta, R. L., and Argstatter, H. (2018). Interpreting the Tinnitus Questionnaire (German version): what individual differences are clinically important? Int. J. Audiol. 57, 553–557. doi: 10.1080/14992027.2018.1442591
Hallam, R., Rachmann, S., and Hinchcliffe, R. (1984). “Psychological aspects of tinnitus,” in Contributions to Medical Psychology, Vol 3, ed. S. Rachman (Oxford: Pergamon press), 31–53.
Henry, J. A., Reavis, K. M., Griest, S. E., Thielman, E. J., Theodoroff, S. M., Grush, L. D., et al. (2020). Tinnitus an epidemiologic perspective. Otolaryng Clin. N. Am. 53:481. doi: 10.1016/j.otc.2020.03.002
Hesser, H., Weise, C., Westin, V. Z., and Andersson, G. A. (2011). systematic review and meta-analysis of randomized controlled trials of cognitive-behavioral therapy for tinnitus distress. Clin. Psychol. Rev. 31, 545–553. doi: 10.1016/j.cpr.2010.12.006
Ivansic, D., Besteher, B., Gantner, J., Guntinas-Lichius, O., Pantev, C., Nenadic, I., et al. (2019). Psychometric assessment of mental health in tinnitus patients, depressive and healthy controls. Psychiatry Res. 281:112582. doi: 10.1016/j.psychres.2019.112582
Ivansic, D., Dobel, C., Volk, G. F., Reinhardt, D., Müller, B., Smolenski, U. C., et al. (2017a). Results of an interdisciplinary day care approach for chronic tinnitus treatment: a prospective study introducing the jena interdisciplinary treatment for tinnitus. Front. Aging Neurosci. 9:192. doi: 10.3389/fnagi.2017.00192
Ivansic, D., Guntinas-Lichius, O., Muller, B., Volk, G. F., Schneider, G., Dobel, C., et al. (2017b). Impairments of speech comprehension in patients with tinnitus-a review. Front. Aging Neurosci. 9:224. doi: 10.3389/fnagi.2017.00224
Ivansic, D., Palm, J., Pantev, C., Bruggemann, P., Mazurek, B., Guntinas-Lichius, O., et al. (2022). Prediction of treatment outcome in patients suffering from chronic tinnitus - from individual characteristics to early and long-term change. J. Psychosom. Res. 157:110794. doi: 10.1016/j.jpsychores.2022.110794
Jarach, C. M., Lugo, A., Scala, M., van den Brandt, P. A., Cederroth, C. R., Odone, A., et al. (2022). Global prevalence and incidence of tinnitus: a systematic review and meta-analysis. JAMA Neurol. 79, 888–900. doi: 10.1001/jamaneurol.2022.2189
Jastreboff, P. J. (1990). Phantom auditory perception (tinnitus): mechanisms of generation and perception. Neurosci. Res. 8, 221–254. doi: 10.1016/0168-0102(90)90031-9
Kang, Y. J., and Zheng, Y. (2024). Current understanding of subjective tinnitus in adults. Eur. Arch. Otorhinolaryngol. 281, 4507–4517. doi: 10.1007/s00405-024-08633-w
Kuhn, M. (2008). Building predictive models in R using the caret package. J. Stat. Softw. 28, 1–26. doi: 10.18637/jss.v028.i05
Landry, E. C., Sandoval, X. C. R., Simeone, C. N., Tidball, G., Lea, J., Westerberg, B. D., et al. (2020). Systematic review and network meta-analysis of cognitive and/or behavioral therapies (CBT) for tinnitus. Otol. Neurotol. 41, 153–166. doi: 10.1097/MAO.0000000000002472
Leaver, A. M., Seydell-Greenwald, A., and Rauschecker, J. P. (2016). Auditory-limbic interactions in chronic tinnitus: challenges for neuroimaging research. Hear. Res. 334, 49–57. doi: 10.1016/j.heares.2015.08.005
Little, R. J. A. (1988). A test of missing completely at random for multivariate data with missing values. J. Am. Stat. Assoc. 83, 1198–1202. doi: 10.1080/01621459.1988.10478722
Lukas, C. F., Mazurek, B., Brueggemann, P., Junghofer, M., Guntinas-Lichius, O., Dobel, C. A., et al. (2024). retrospective two-center cohort study of the bidirectional relationship between depression and tinnitus-related distress. Commun. Med. 4:242. doi: 10.1038/s43856-024-00678-6
Lumley, T., and Miller, A. (2020). leaps: Regression Subset Selection. R package version 31. Available online at: https://CRAN.R-project.org/package=leaps (Accessed December 3, 2024).
Martinez Devesa, P., Waddell, A., Perera, R., and Theodoulou, M. (2007). Cognitive behavioural therapy for tinnitus. Cochrane Database Syst. Rev. 2007:CD005233. doi: 10.1002/14651858.CD005233.pub2
Mazurek, B., Hesse, G., Sattel, H., Kratzsch, V., Lahmann, C., Dobel, C., et al. (2022a). S3 Guideline: chronic tinnitus: German society for otorhinolaryngology, head and neck surgery. HNO 70, 795–827. doi: 10.1007/s00106-022-01207-4
Mazurek, B., Rose, M., Schulze, H., and Dobel, C. (2022b). Systems medicine approach for tinnitus with comorbid disorders. Nutrients 14:4320. doi: 10.3390/nu14204320
Mueller, L., Kallogjeri, D., Frumkin, M. R., Dizdar, K., Shin, J., Rodebaugh, T., et al. (2024). Predictors of response to cognitive behavioral therapy in patients with tinnitus. JAMA Otolaryngol. Head Neck Surg. 150, 819–826. doi: 10.1001/jamaoto.2024.2264
Paraskevopoulos, E., Dobel, C., Wollbrink, A., Salvari, V., Bamidis, P. D., Pantev, C., et al. (2019). Maladaptive alterations of resting state cortical network in Tinnitus: a directed functional connectivity analysis of a larger MEG data set. Sci. Rep. 9:15452. doi: 10.1038/s41598-019-51747-z
Pinto, P. C., Marcelos, C. M., Mezzasalma, M. A., Osterne, F. J., de Melo Tavares de Lima, M. A., and Nardi, A. E. (2014). Tinnitus and its association with psychiatric disorders: systematic review. J. Laryngol. Otol. 128, 660–664. doi: 10.1017/S0022215114001030
Refat, F., Wertz, J., Hinrichs, P., Klose, U., Samy, H., Abdelkader, R. M., et al. (2021). Co-occurrence of hyperacusis accelerates with tinnitus burden over time and requires medical care. Front. Neurol. 12:627522. doi: 10.3389/fneur.2021.627522
Salvari, V., Korth, D., Paraskevopoulos, E., Wollbrink, A., Ivansic, D., Guntinas-Lichius, O., et al. (2023). Tinnitus-frequency specific activity and connectivity: a MEG study. Neuroimage Clin. 38:103379. doi: 10.1016/j.nicl.2023.103379
Schibbye, P., Ghaderi, A., Ljotsson, B., Hedman, E., Lindefors, N., Ruck, C., et al. (2014). Using early change to predict outcome in cognitive behaviour therapy: exploring timeframe, calculation method, and differences of disorder-specific versus general measures. PLoS ONE 9:e100614. doi: 10.1371/journal.pone.0100614
Schlee, W., Holleland, S., Bulla, J., Simoes, J., Neff, P., Schoisswohl, S., et al. (2020). The effect of environmental stressors on tinnitus: a prospective longitudinal study on the impact of the COVID-19 pandemic. J. Clin. Med. 9:2756. doi: 10.3390/jcm9092756
Schmidt, S. A., Carpenter-Thompson, J., and Husain, F. T. (2017). Connectivity of precuneus to the default mode and dorsal attention networks: a possible invariant marker of long-term tinnitus. Neuroimage Clin. 16, 196–204. doi: 10.1016/j.nicl.2017.07.015
Spitzer, R. L., Kroenke, K., and Williams, J. B. (1999). Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary care evaluation of mental disorders. Patient health questionnaire. JAMA 282, 1737–1744. doi: 10.1001/jama.282.18.1737
Stegeman, I., Eikelboom, R. H., Smit, A. L., Baguley, D. M., Bucks, R. S., Stokroos, R. J., et al. (2021). Tinnitus and its associations with general health, mental health and hearing loss. Prog. Brain Res. 262, 431–450. doi: 10.1016/bs.pbr.2021.01.023
Tai, Y., and Husain, F. T. (2019). The role of cognitive control in tinnitus and its relation to speech-in-noise performance. J. Audiol. Otol. 23, 1–7. doi: 10.7874/jao.2018.00409
Taylor, J. A., Thompson, D. M., Hall, D. A., Walker, D. M., McMurran, M., Casey, A., et al. (2020). The TinMan study: feasibility trial of a psychologically informed, audiologist-delivered, manualised intervention for tinnitus. Int. J. Audiol. 59, 905–914. doi: 10.1080/14992027.2020.1788730
Venables, W. N., and Ripley, B. D. (2002). Modern Applied Statistics With S, 4th Edn. New York, NY: Springer.
Vielsmeier, V., Kreuzer, P. M., Haubner, F., Steffens, T., Semmler, P. R., Kleinjung, T., et al. (2016). Speech comprehension difficulties in chronic tinnitus and its relation to hyperacusis. Front. Aging Neurosci. 8:293. doi: 10.3389/fnagi.2016.00293
Weisz, N., Wienbruch, C., Dohrmann, K., and Elbert, T. (2005). Neuromagnetic indicators of auditory cortical reorganization of tinnitus. Brain 128(Pt 11), 2722–2731. doi: 10.1093/brain/awh588
Keywords: chronic tinnitus, treatment, follow-up, interdisciplinary, cognitive behavioral therapy
Citation: Lukas CF, Ivansic D, Schneider G, Lemhöfer C, Guntinas-Lichius O and Dobel C (2025) Short and sweet: Sustained reduction in tinnitus-related distress following intensive interdisciplinary treatment—A 5-year follow-up study. Front. Audiol. Otol. 3:1648132. doi: 10.3389/fauot.2025.1648132
Received: 17 June 2025; Accepted: 19 September 2025;
Published: 08 October 2025.
Edited by:
Divya Bharatkumar Adhia, University of Otago, New ZealandReviewed by:
Iman Ghodratitoostani, University of Sao Paulo, BrazilNicolas Gninenko, Swiss Federal Institute of Technology Lausanne, Switzerland
Copyright © 2025 Lukas, Ivansic, Schneider, Lemhöfer, Guntinas-Lichius and Dobel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christian Dobel, Y2hyaXN0aWFuLmRvYmVsQG1lZC51bmktamVuYS5kZQ==