 Guillaume Gersdorff1
Guillaume Gersdorff1 Nicola Ivanovic2
Nicola Ivanovic2 Masoud Zoka Assadi2Peter Nopp2
Masoud Zoka Assadi2Peter Nopp2 Séverine Camby1Philippe Lefèbvre1*
Séverine Camby1Philippe Lefèbvre1*- 1Department of Otorhinolaryngology, Centre Hospitalier Universitaire (CHU), Liège, Belgium
- 2Medel, Innsbruck, Austria
Introduction: Single-sided deafness (SSD) affects the ability to localize sounds and understand speech in noisy environments, significantly impacting the quality of life. Cochlear implants (CIs) have been explored as a solution for SSD, with varying success attributed to different factors, such as onset of deafness (pre- vs. post-lingual), duration of especially pre-lingual deafness, and compliance to rehab protocols, as well as the frequency-to-place mismatch, where the frequency assigned to CI electrodes does not align with the cochlea's natural tonotopy. The objective is to investigate the influence of frequency-to-place mismatch on hearing performance, sound quality, and patient satisfaction in SSD CI recipients by comparing default and anatomical frequency mapping.
Methods: A retrospective study was conducted on 19 SSD patients implanted with MEDEL CIs between 2014 and 2023. Post-activation, high-resolution cone beam computed tomography scans were analyzed using OTOPLAN® (Version V4) to define anatomical frequency mapping. The average frequency mismatch (AFM) between default and anatomical mapping was calculated. Speech intelligibility was assessed using articulation function (AF) scores, and sound quality was evaluated through patient questionnaires.
Results: A significant negative correlation between AFM and AF (R = −0.47, p = 0.042) was observed. Sound quality aspects, including natural sound perception and similarity to the normal ear, inversely correlated with AFM (R2 = 0.281, p = 0.05, and R2 = 0.301, p = 0.043, respectively). Global satisfaction scores were high (3.58 ± 0.77), unaffected by AFM.
Conclusion: Frequency-to-place mismatch impacts speech intelligibility and sound quality in SSD CI patients. Anatomical frequency mapping using tools like OTOPLAN can enhance CI outcomes, highlighting the need for individualized cochlear measurements and electrode assignment.
Introduction
Hearing is a crucial sense that connects us to the surrounding world, enabling communication, fostering relationships, and enriching our overall life experiences. The human auditory system relies on the ability to differentiate between sounds and localize their source. For individuals with single-sided deafness (SSD), this natural ability is compromised, leading to a range of issues in environments where background noise and multiple speakers are prevalent. SSD refers to the condition in which one ear has profound or severe hearing loss while the other ear maintains normal hearing or has a less severe impairment. It affects 3%−6% of the total population (Ross et al., 2010). While this condition may seem manageable in quiet settings, the difficulties become pronounced in noisy situations, making it challenging for individuals with SSD to effectively understand speech in noise and engage in social interactions. This situation requires compensatory mechanisms, and patients' quality of life may be affected by social isolation (Taylor, 2010; Tokita et al., 2014; Kitterick et al., 2015).
In recent years, advancements in auditory technology have paved the way for transformative solutions, and one such breakthrough is the use of cochlear implants (CIs) to address SSD. The first use of a CI for treating SSD was reported in 2008 (Van de Heyning et al., 2008). CIs, originally designed for individuals with bilateral hearing loss, are currently being explored as an innovative option to restore hearing in those with SSD. They can support better-ear listening and provide access to interaural intensity cues. Studies have demonstrated that CIs can improve sound localization and speech understanding in noise (Dillon et al., 2022; Wesarg et al., 2024; Park et al., 2023; Távora-Vieira et al., 2019; Seebacher et al., 2023; Mertens et al., 2017). Evidence from a previous study involving SSD children and adults has shown that CI use significantly improves performance across all three target-to-masker configurations [speech at 0° azimuth, masking noise at 0° azimuth (collocated) (S0N0), p = 0.013; speech front and masker to the CI or left ear (S0Nci/L), p = 0.027; and speech front and masker to the normal hearing or right ear (S0Nnh/R), p < 0.001] (Park et al., 2023). Additionally, significant improvements in Speech Reception Threshold (SRTs) with a CI, compared to the preoperative unaided condition, were found in all spatial configurations (Wesarg et al., 2024).
As we delve into the possibilities and challenges associated with CIs in the context of SSD, it becomes evident that these devices offer newfound hope for a more inclusive and enriched auditory experience. The criteria and predictive factors for recommending implantation have been recently published (Dillon et al., 2022; Park et al., 2023). During CI activation, auditory frequencies are typically assigned in a quasi-logarithmic and identical manner (which is a standard procedure) based on the specific implant model. However, due to limitations in the electrode array's ability to reach the most apical regions of the cochlea, as well as natural variability of cochlear anatomy (Alexiades et al., 2015; Escudé et al., 2006; Spiegel et al., 2022), this frequency assignment may not align with the cochlea's natural tonotopy. As a result, there is a discrepancy between the default frequency assigned to an electrode and the actual frequency of the stimulated neurons. This phenomenon is commonly referred to as the frequency-to-place mismatch. The current challenge in CI fitting lies in incorporating anatomical data (Mertens et al., 2022). A collaborative effort between CASCINATION AG (Switzerland) and MED-EL (Austria) has resulted in the development of OTOPLAN®, a tablet-based software. This innovative tool offers otologists an intuitive and efficient method to evaluate the anatomy of the temporal bone, enabling them to plan personalized cochlear implantation for optimal outcomes. By utilizing computed tomography (CT) scans of the temporal bone, OTOPLAN® accurately identifies crucial structures such as the modiolus, round window, and the tonotopic location of each electrode contact. The software's reliability was confirmed for estimating cochlear canal length and insertion angle depth of the electrodes (Canfarotta et al., 2020). Therefore, this program can provide a tonotopic setting for CI patients.
This retrospective study aims to investigate the influence of frequency-to-place mismatch on the hearing performance, sound quality, and patient satisfaction in individuals with SSD, by comparing anatomical frequency mapping defined by OTOPLAN with the default mapping used at the time of CI activation.
Materials and methods
This retrospective study included patients with post-lingual deafness implanted unilaterally with MEDEL CI from 2014 to 2023 at the University Hospital of Liege, a tertiary care center. The inclusion criteria were age >18 years and unilateral post-lingual hearing loss eligible for CI implantation in the deaf ear with normal hearing in the contralateral ear [Pure Tone Average (PTA) < 20 dB for 500, 1,000, 2,000, 4,000, and 8,000 Hz]. The exclusion criteria were: age < 18 years, abnormal hearing threshold in the contralateral ear (PTA >35 dB at 250, 500, 1,000, 2,000, 4,000, and 8,000 Hz), pre-lingual deafness, cochlear malformations, contraindication to CT imaging, unavailable or poor-resolution scans, or incompatibility with the OTOPLAN program.
All implants were activated and fitted with a processing strategy (FS4) using a standard frequency allocation map (logFS) distributed on active electrode contacts, as prescribed by the manufacturer. All patients underwent a post-operative, high-resolution cone beam CT of the temporal bone, which was analyzed using OTOPLAN (V4; CE-certification number: G1 17 10 95657 003). The software performed automated anatomical landmark assignment without manual intervention (Figure 1). Using the MAESTRO 9.0 anatomy-based fitting tools, an automated formula was used without manual intervention to determine a frequency allocation that followed the natural tonotopic map of the cochlea. In our calculation, we used the logFS bandpass-filter center frequencies.
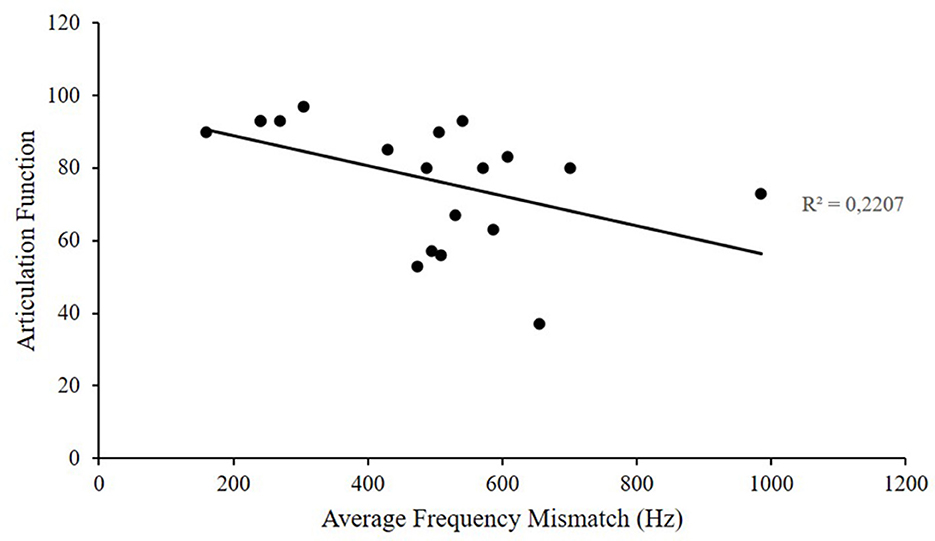
Figure 1. Correlation between average frequency mismatch and articulation function.
The default frequency assigned to each electrode at the time of fitting was compared with the frequency established by OTOPLAN based on the position of the spiral ganglion neurons. The difference between these two values was calculated for each electrode for the frequencies corresponding to the speech spectrum (500–2,000 Hz) and then averaged and presented as “average of frequency mismatch” (AFM).
Finally, the AFM was compared with the hearing results for patients as assessed by speech audiometry. We used the articulation function (AF) as an index of speech intelligibility, defined as the average speech discrimination score obtained at 40, 55, and 70 dB. The speech audiometries were performed in a soundproof booth, with the patient sitting 1 m from the sound source and their normal-hearing ear masked using an earphone. We used the words of Fournier's dissyllabic list in French, pronounced to the patient through a loudspeaker. Measurements were recorded at 40–55 and 70 dB Sound Pressure Level (SPL) to calculate the AF. All tests were conducted in a quiet environment, using the default frequency allocation.
The patients were interviewed to fill out a satisfaction questionnaire composed of five questions on an analog scale ranging from 0 (not at all) to 5 (completely), with one exception for the question on robotic sound quality, which ranged from 0 (completely) to 5 (not at all). The following aspects of satisfaction were evaluated: (1) global satisfaction of the cochlear implant, (2) sound detection (is the implant activated), (3) robotic quality of sound, (4) similarity of the sound to the normal ear, and (5) natural sound sensation.
All data sets are available upon request.
Results
Patients
Nineteen patients were included in this retrospective study. Among the 7 men and 12 women, the mean age of implantation was 60 ± 11.8 (range 44–80 years). All participants were French-speaking. Eight patients were implanted in the right ear and 11 in the left ear. No post-operative complications were observed. Implantation with a round window approach was performed for all patients; a MEDEL FLEX 24 (24-mm) electrode array was used for 13 patients, a FLEX 26 (26-mm) electrode was implanted for 2 patients, and a FLEX 28 (28-mm) electrode was implanted for 4 patients. The normal-hearing ear showed a PTA of 19.6 ± 10.99 dB, and the implanted ear showed a PTA of 93.66 ± 20.09 dB before surgery and of 38.32 ± 4.42 dB with the implant activated.
AFM
The main objective of this retrospective study was to evaluate the outcome of speech intelligibility as a function of the difference between the default frequency mapping for each electrode and the frequency fitted by the OTOPLAN software. All patients (100%) had a frequency mismatch of at least 159.8 Hz and a maximum of 985 Hz, and the average mismatch was 489.09 ± 193.21 Hz.
AF
The relationship between AFM and AF was analyzed (Figure 1). Among implant-activated patients, the AF measured at the plateau reached after implant activation was 77 ± 17.03%. The average frequency mismatch showed a significant inverse correlation (R = −0.47, R2 = 0.22) with speech intelligibility, as measured by the Articulation Function (p = 0.042).
Quality of sound
The increase in the difference between the tonotopic frequency, as defined by OTOPLAN, and the fitted frequency strongly and inversely correlated with the perception of a natural sound (R = −0.476, R2 = 0.281, p = 0.05) and with the similarity of the sound perceived in the normal ear (R = −0.494, R2 = 0.301, p= 0.043), as assessed on an analog scale ranging between 0 and 5 (Figure 2). Robotic sound quality (R = −0.22, R2 = 0.089, p = 0.395) and perception of the presence of the implant ON (R = −0.172, R2 = 0.071, p = 0.52) were not significantly affected by the AFM. However, overall subjective satisfaction remained very good for all patients, with a score of 3.58 ± 0.77 (R = −0.347, R2 = 0.15, p = 0.17), and was not affected by AFM.
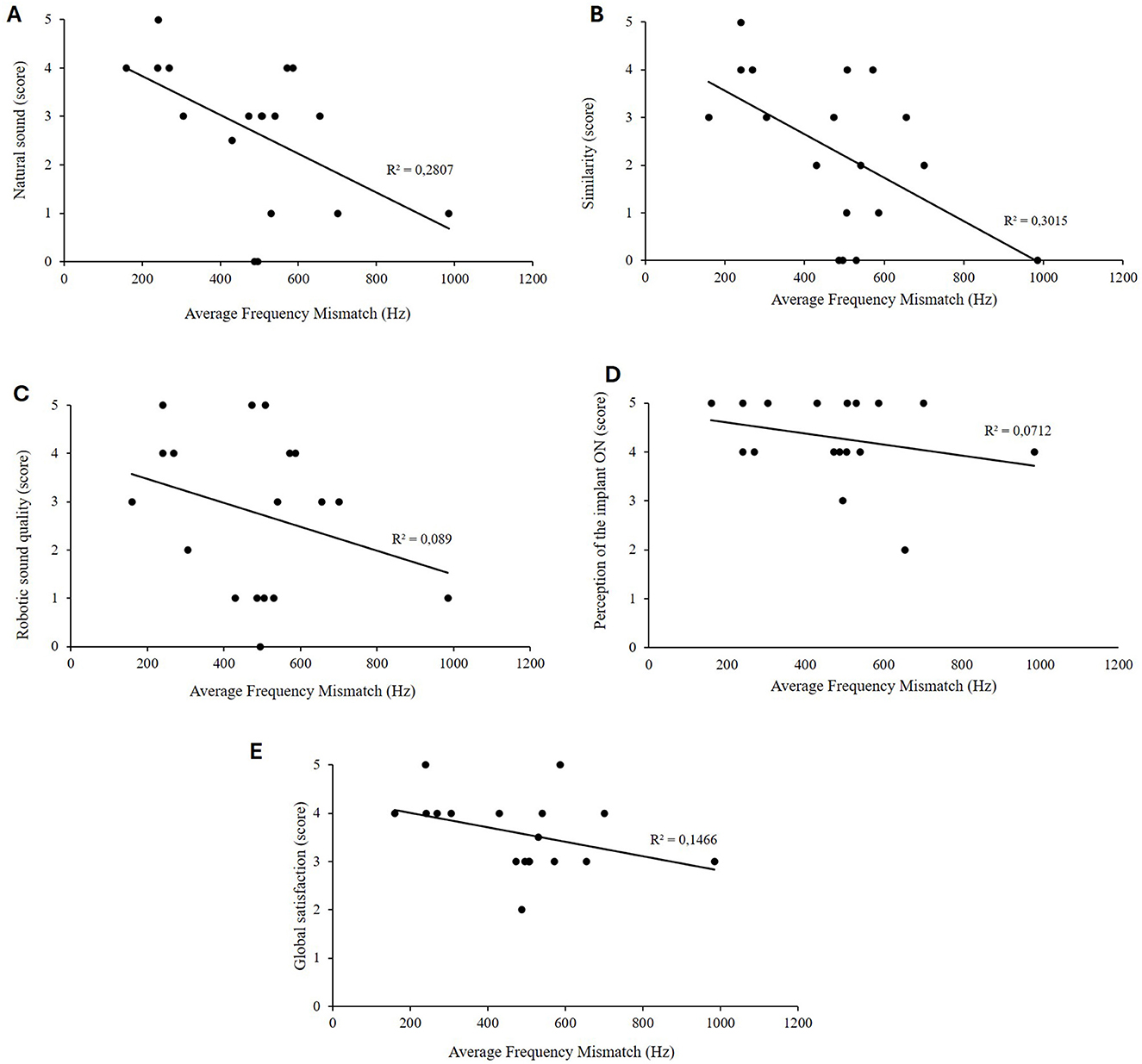
Figure 2. Natural sound (A), similar sound to normal ear (B), robotic sound quality (C), perception of the implant ON (D), and global satisfaction score (E) as a function of the calculated frequency placed mismatch.
Overall, significantly, the closer the match between the adjusted and predicted frequencies, the higher the total score for the five questions on subjective sound quality perception after CI activation (R = −0.562, R2 = 0.316, p = 0.0188).
Discussion
Previous studies on frequency mapping were mainly conducted on patients suffering from bilateral hearing loss. The originality of this retrospective study was to evaluate the outcomes of speech intelligibility, as well as the quality of sound and the global satisfaction of patients presenting a SSD, as a function of the difference between the default frequency mapping for each electrode and the frequency suggested by the software OTOPLAN based on the anatomy of the cochlea. CI implantation in the deaf ear improves binaural function rehabilitation in SSD. Sound localization can be restored, and speech understanding greatly improved after implantation, while the severity of SSD-related tinnitus can be reduced. Moreover, CI confers greater improvement in sound localization than a bone conduction hearing aid or a contralateral routing of signal device, which do not restore meaningful sound localization (Van de Heyning et al., 2008; Wesarg et al., 2024; Arndt et al., 2011; Cabral Junior et al., 2016; Kitterick et al., 2016; Thomas et al., 2016; Hempel et al., 2018).
Criteria and predictive factors for recommended implantation have been recently published (Dillon et al., 2022; Park et al., 2023), suggesting that CI is an appropriate treatment for patients with SSD. Parameters such as age at the time of implantation, duration of hearing loss, preoperative speech intelligibility thresholds, and the patient's cognitive abilities can influence post-implant hearing performance (Blamey et al., 2013). It has been established that CI tends to produce a positive effect in noise for some SSD patients (Firszt et al., 2012; Távora-Vieira et al., 2013; Gersdorff et al., 2024) and that there is a significant positive correlation between contralateral PTA and noise test results under certain conditions (Gersdorff et al., 2024; Dorbeau et al., 2018). Overall, post-operative CI hearing performance can be extremely inconsistent. Therefore, additional unknown factors still remain. Recent studies have shown that several factors could play a role in hearing performance, including the depth of electrode insertion, the percentage of electrodes present in the scala vestibuli, and the amount of fluid and scar tissue surrounding the electrodes (Holden et al., 2014; Van Der Beek et al., 2016; Finley et al., 2008; Buchman et al., 2014). As an additional factor, the variable anatomy and dimensions of the human cochlea suggest that frequency maps could vary considerably. Therefore, the electrode frequency assignment may not align with the cochlea's natural tonotopy and may not be optimal for specific anatomical variations. Partial coverage of electrical stimulation in CI recipients with profound post-lingual deafness could lead to a frequency mismatch. In a previous study, we reported that frequency-to-place mismatch could explain the variability in results for speech intelligibility in bilaterally deaf patients. The same trend could be observed with the length and width of the cochlear base, the total cochlear volume, and the volumes of the separate compartments (Starovoyt et al., 2023). In this study, we confirm that the bigger the AFM is, the lower the intelligibility in SSD patients will be. It has been shown that matching electrodes to cochlear frequency maps is essential for optimal fitting and performance. There is a strong interaction between the optimal frequency–place mapping, electrode insertion depth, and speech recognition (Li et al., 2020; Dhanasingh and Jolly, 2017; Baskent and Shannon, 2005). Understanding and incorporating these factors into research and development efforts are essential for tailoring interventions to individual needs.
The primary outcome of this study was to compare the default frequencies assigned to the electrodes of a CI at the time of fitting with those established based on the anatomical values defined in OTOPLAN. As expected, we demonstrated a systematic mismatch between these frequencies as previously reported in several studies (Mertens et al., 2022; Canfarotta et al., 2020; Venail et al., 2015; Landsberg et al., 2015; Dessard et al., 2024). The average of the mismatch was 489.09 ± 193.21 Hz.
The secondary outcome was to compare this mismatch with the hearing performance of CI users. The maximum speech intelligibility achieved by the patients was measured at 78.95 + 13.87%. AFM showed a strong inverse correlation with speech intelligibility, as measured by the AF. This inverse correlation between the mismatch and speech performance is statistically significant. A linear correlation between frequency-to-place mismatch and hearing performance impairment was described by Mertens et al. (2022). Our results are in line with other studies (Mertens et al., 2022; Canfarotta et al., 2020; Venail et al., 2015; Landsberg et al., 2015; Dessard et al., 2024), highlighting the necessity of reducing this mismatch to improve hearing performance.
The third outcome of this study was to analyze the perception of a natural sound and the similarity of the sound perceived in the normal ear, as assessed on an analog scale ranging from 0 to 5. We showed a statistically significant negative correlation with the AFM. The closer the match between the adjusted and predicted frequencies, the higher the total score on the five questions assessing subjective perception after CI activation. However, overall subjective satisfaction remained very good for all patients, with an average score of more than 3.5. The perception of “natural” sound is inherently subjective and varies among CI users. Therefore, considering an objective measurement of the quality of life as defined by Kitterick et al. (2015) is important. It is particularly relevant for SSD patients who are able to achieve a comparison between both sides. We know that compliance could be an issue for those recipients when they consider no similarity in the perceived sound between both sides. Factors such as age at implantation, duration of deafness, and individual differences in auditory processing contribute to the diversity in user experiences. In our study, we did not take those parameters into account, but they should also be analyzed in further studies.
This study has several limitations. First, it is a retrospective analysis based on data that were not originally collected for research purposes, which may result in missing information or inaccuracies. Stratifying the sample according to potential influencing factors—such as cochlear anatomy, depth of electrode insertion, age, and others—could help with better understanding possible confounding variables. Multivariate models may also be valuable to explore these associations, but they would require a larger sample size.
This study should be considered preliminary. Further prospective research with larger cohorts is needed to confirm these findings and address these limitations.
Conclusion
In this study, we showed that sound quality and patient satisfaction in individuals with SSD are inversely proportional to the difference between the default frequency mapping for each electrode, fitted by MAESTRO 9.0, and the frequency suggested by the OTOPLAN (V4) software. In addition, we have demonstrated a systematic mismatch between the assigned default frequencies and those established based on the anatomical values defined in OTOPLAN®. We also highlighted that, in line with other studies, the average frequency mismatch correlated statistically with speech intelligibility (p = 0.042). CIs, originally designed for individuals with bilateral hearing loss, are currently being explored as an innovative option to address SSD. This study reinforces the hypothesis that CIs are an appropriate treatment for patients with SSD and that incorporating the concept of anatomy-based fitting into clinical practice is valuable for tailoring interventions to individual needs. Frequency-to-place mismatch could explain variability in results for test-in-noise or in localization tests. This should be considered in a further SSD prospective study.
This study encourages further research into the benefits of personalized fitting strategies for SSD patients.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comité d‘Éthique Hospitalo-Facultaire Universitaire de Liège. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin because this retrospective study is not under the law of 07 May 2004.
Author contributions
GG: Writing – original draft, Software, Writing – review & editing, Data curation. NI: Software, Writing – review & editing. MZ: Software, Writing – review & editing. PN: Supervision, Writing – review & editing. SC: Formal analysis, Writing – review & editing. PL: Writing – review & editing, Conceptualization, Investigation.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors thank the audiologist from the Department of Oto-rhinolaryngology for outstanding clinical work.
Conflict of interest
NI, MZ, and PN were employed by Medel.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alexiades, G., Dhanasingh, A., and Jolly, C. (2015). Method to estimate the complete and two-turn cochlear duct length. Otol. Neurotol. 36, 904–907. doi: 10.1097/MAO.0000000000000620
Arndt, S., Aschendorff, A., Laszig, R., Beck, R., Schild, C., Kroeger, S., et al. (2011). Comparison of pseudobinaural hearing to real binaural hearing rehabilitation after cochlear implantation in patients with unilateral deafness and tinnitus. Otol. Neurotol. 32, 39–47. doi: 10.1097/MAO.0b013e3181fcf271
Baskent, D., and Shannon, R. (2005). Interactions between cochlear implant electrode insertion depth and frequency-place mapping. J. Acoust. Soc. Am. 117, 1405–1416. doi: 10.1121/1.1856273
Blamey, P., Artieres, F., Başkent, D., Bergeron, F., Beynon, A., Burke, E., et al. (2013). Factors affecting auditory performance of postlinguistically deaf adults using cochlear implants: an update with 2251 patients. Audiol. Neurotol. 18, 36–47. doi: 10.1159/000343189
Buchman, C. A., Dillon, M. T., King, E. R., Adunka, M. C., Adunka, O., Pillsbury, H. C., et al. (2014). Influence of cochlear implant insertion depth on performance: a prospective randomized trial. Otol. Neurotol. 35, 1773–1779. doi: 10.1097/MAO.0000000000000541
Cabral Junior, F., Pinna, M. H., Alves, R. D., Malerbi, A. F. D. S., and Bento, R. F. (2016). Cochlear implantation and single-sided deafness: a systematic review of the literature. Int Arch Otorhinolaryngol. 20, 69–75. doi: 10.1055/s-0035-1559586
Canfarotta, M. W., Dillon, M. T., Buss, E., Pillsbury, H. C., Brown, K. D., O'Connell, B. P., et al. (2020). Frequency-to-place mismatch: characterizing variability and the influence on speech perception outcomes in cochlear implant recipients. Ear Hear. 41, 1349–1361. doi: 10.1097/AUD.0000000000000864
Dessard, L., Gersdorff, G., Ivanovik, N., Zoca-Assadi, M., Nopp, P., Camby, S., et al. (2024). Cochlear implant: analysis of the frequency-to-place mismatch with the table-based software OTOPLAN® and its influence on hearing performance. Audiol. Neurootol. 29, 239–245. doi: 10.1159/000535693
Dhanasingh, A., and Jolly, C. (2017). An overview of cochlear implant electrode array designs. Hear Res. 356, 93–103. doi: 10.1016/j.heares.2017.10.005
Dillon, M., Rooth, M. A., Canfarotta, M. W., Richter, M., Thompson, N., Brown, K. D., et al. (2022). Sound Source localization by cochlear implant recipients with normal hearing in the contralateral ear: effects of spectral content and duration of listening experience. Audiol. Neurootol. 27, 437–448. doi: 10.1159/000523969
Dorbeau, C., Galvin, J., Fu, Q., Legris, E., Marx, M., Bakhos, D., et al. (2018). Binaural perception in single-sided deaf cochlear implant users with unrestricted or restricted acoustic hearing in the non-implanted ear. Audiol. Neurootol. 23, 187–197. doi: 10.1159/000490879
Escudé, B., James, C., Deguine, O., Cochard, N., Eter, E., Fraysse, B., et al. (2006). The size of the cochlea and predictions of insertion depth angles for cochlear implant electrodes. Audiol. Neurotol. 11(Suppl. 1), 27–33. doi: 10.1159/000095611
Finley, C. C., Holden, T. A., Holden, L. K., Whiting, B. R., Chole, R. A., Neely, G. J., et al. (2008). Role of electrode placement as a contributor to variability in cochlear implant outcomes. Otol. Neurotol. 29, 920–928. doi: 10.1097/MAO.0b013e318184f492
Firszt, J., Holden, L., Reeder, R., Waltzman, S., and Arndt, S. (2012). Auditory abilities after cochlear implantation in adults with unilateral deafness: a pilot study. Otol. Neurotol. 33, 1339–1346. doi: 10.1097/MAO.0b013e318268d52d
Gersdorff, G., Péan, V., Camby, S., Barriat, S., and Lefebvre, P. P. (2024). Factors predictive of binaural hearing restoration by cochlear implant in single-sided deafness. Audiol. Neurootol. 1, 1–11. doi: 10.1159/000540577
Hempel, J., Simon, F., and Müller, J. (2018). Extended applications for cochlear implantation. Adv. Otorhinolaryngol. 81, 74–80. doi: 10.1159/000485546
Holden, L. K., Finley, C. C., Firszt, J. B., Timothy, A., Brenner, C., Potts, L. G., et al. (2014). Factors affecting open-set word recognition in adults with cochlear implants. Ear Hear. 34, 342–360. doi: 10.1097/AUD.0b013e3182741aa7
Kitterick, P. T., Lucas, L., and Smith, S. N. (2015). Improving health-related quality of life in single-sided deafness: a systematic review and meta-analysis. Audiol. Neurotol. 20, 79–86. doi: 10.1159/000380753
Kitterick, P. T., Smith, S. N., and Lucas, L. (2016). Hearing instruments for unilateral severe-to-profound sensorineural hearing loss in adults: a systematic review and meta-analysis. Ear Hear. 37, 495–507. doi: 10.1097/AUD.0000000000000313
Landsberg, D. M., Svrakic, S., Roland, J. T., and Svirsky, M. (2015). The relationship between insertion angles, default frequency allocations, and spiral ganglion place pitch in cochlear implants. Ear Hear. 36, e207–e213. doi: 10.1097/AUD.0000000000000163
Li, H., Schart-Morén, N., Rohani, S. A., Ladak, H. M., Rask-Andersen, H., Agrawal, S., et al. (2020). Synchrotron radiation-based reconstruction of the human spiral ganglion: implications for cochlear implantation. Ear Hear. 41, 173–181. doi: 10.1097/AUD.0000000000000738
Mertens, G., De Bodt, M., and Van de Heyning, P. (2017). Evaluation of long-term cochlear implant use in subjects with acquired unilateral profound hearing loss: focus on binaural auditory outcomes. Ear Hear. 38, 117–125. doi: 10.1097/AUD.0000000000000359
Mertens, G., Van de Heyning, P., Vanderveken, O., Topsakal, V., and Van Rompaey, V. (2022). The smaller the frequency-to-place mismatch the better the hearing outcomes in cochlear implant recipients? Eur. Arch. Oto-Rhino-Laryngol. 279, 1875–1883. doi: 10.1007/s00405-021-06899-y
Park, L. R., Dillon, M. T., Buss, E., and Brown, K. D. (2023). Two-year outcomes of cochlear implant use for children with unilateral hearing loss: benefits and comparison to children with normal hearing. Ear Hear. 44, 955–968. doi: 10.1097/AUD.0000000000001353
Ross, D., Visser, S., Holstrum, W., Qin, T., and Kenneson, A. (2010). Highly variable population-based prevalence rates of unilateral hearing loss after the application of common case definitions. Ear Hear. 31, 126–133. doi: 10.1097/AUD.0b013e3181bb69db
Seebacher, J., Franke-Trieger, A., Weichbold, V., Galvan, O., Schmutzhard, J., Zorowka, P., et al. (2023). Sound localisation of low- and high-frequency sounds in cochlear implant users with single-sided deafness. Int. J. Audiol. 62, 71–78. doi: 10.1080/14992027.2022.2030496
Spiegel, J. L., Polterauer, D., Hempel, J. M., Canis, M., Spiro, J. E., Müller, J., et al. (2022). Variation of the cochlear anatomy and cochlea duct length: analysis with a new tablet-based software. Eur. Arch. Oto-Rhino-Laryngol. 279, 1851–1861. doi: 10.1007/s00405-021-06889-0
Starovoyt, A., Pyka, G., Putzeys, T., Balcaen, T., Wouters, J., Kerckhofs, G., et al. (2023). Human cochlear microstructures at risk of electrode insertion trauma, elucidated in 3D with contrast-enhanced microCT. Sci. Rep. 13:2191. doi: 10.1038/s41598-023-29401-6
Távora-Vieira, D., Marino, R., Krishnaswamy, J., Kuthbutheen, J., and Rajan, G. (2013). Cochlear implantation for unilateral deafness with and without tinnitus: a case series. Laryngoscope 123, 1251–1255. doi: 10.1002/lary.23764
Távora-Vieira, D., Rajan, G., Van de Heyning, P., and Mertens, G. (2019). Evaluating the long-term hearing outcomes of cochlear implant users with single-sided deafness. Otol. Neurotol. 40, e575–e580. doi: 10.1097/MAO.0000000000002235
Taylor, B. (2010). Controlateral routing of signal amplification strategies. Semin. Hear. 31, 378–392. doi: 10.1055/s-0030-1268036
Thomas, R., Buchman, C., Eisenberg, L., Henderson, L., He, S., Firszt, J., et al. (2016). Proceedings of the annual symposium of the american cochlear implant alliance. Cochlear Implants Int. 17, 211–237. doi: 10.1080/14670100.2016.1225348
Tokita, J., Dunn, C., and Hansen, M. (2014). Cochlear implantation and single sided deafness. Curr. Opin. Otolaryngol. Head Neck Surg. 22, 353–358. doi: 10.1097/MOO.0000000000000080
Van de Heyning, P., Vermeire, K., Diebl, M., Nopp, P., Anderson, I., De Ridder, D., et al. (2008). Incapacitating unilateral tinnitus in single-sided deafness treated by cochlear implantation. Ann. Otol. Rhinol. Laryngol. 117, 645–652. doi: 10.1177/000348940811700903
Van Der Beek, F. B., Briaire, J. J., Van Der Marel, K. S., Verbist, B. M., and Frijns, J. H. M. (2016). Intracochlear position of cochlear implants determined using CT scanning versus fitting levels: higher threshold levels at basal turn. Audiol. Neurotol. 21, 54–67. doi: 10.1159/000442513
Venail, F., Mathiolon, C., Menjot De Champfleur, S., Piron, J. P., Sicard, M., Villemus, F., et al. (2015). Effects of electrode array length on frequency-place mismatch and speech perception with cochlear implants. Audiol. Neurotol. 20, 102–111. doi: 10.1159/000369333
Keywords: cochlear implant, hearing quality, frequency allocation, cochlear length, OTOPLAN®
Citation: Gersdorff G, Ivanovic N, Zoka Assadi M, Nopp P, Camby S and Lefèbvre P (2025) The importance of frequency–place mismatch in the quality of sound perceived in single-sided deafness among cochlear implant recipients. Front. Audiol. Otol. 3:1648716. doi: 10.3389/fauot.2025.1648716
Received: 17 June 2025; Accepted: 21 July 2025;
Published: 18 August 2025.
Edited by:
Mehdi Abouzari, University of California, Irvine, United StatesReviewed by:
Sasan Dabiri, Northern Ontario School of Medicine University, CanadaMiriam Smetak, Washington University in St. Louis, United States
Copyright © 2025 Gersdorff, Ivanovic, Zoka Assadi, Nopp, Camby and Lefèbvre. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Philippe Lefèbvre, cHAubGVmZWJ2cmVAdWxpZWdlLmJl