 Hanna Josefsson Dahlgren
Hanna Josefsson Dahlgren Kia Nøhr Iversen
Kia Nøhr Iversen Malou Hultcrantz
Malou Hultcrantz Cecilia Engmér Berglin
Cecilia Engmér Berglin- 1Division of ENT Diseases, Department of Clinical Intervention and Technology, Karolinska Institutet, Stockholm, Sweden
- 2Medical Unit Ear, Nose, Throat and Hearing, Karolinska University Hospital, Stockholm, Sweden
- 3Oticon Medical AB, Askim, Sweden
Introduction: Bone conduction hearing systems is a well-established treatment for patients with conductive or mixed hearing losses, such as conductive hearing loss caused by congenital aural atresia. Percutaneous bone conduction systems consist of a titanium fixture implanted in a temporal bone and a skin penetrating abutment connecting to an external sound processor. Implant design and surgical techniques have developed over time and while one-stage minimally invasive procedures have long been the standard in adult patients, the development has been more cautious in pediatric patients as they have been more prone to complications and implant loss. The purpose of this study was to collect systematic data from a pediatric population receiving a percutaneous bone conduction hearing device, the laser ablated Ponto BHX implant, in a one-stage surgical procedure.
Methods: Prospective, one-armed, observational cohort study of children undergoing surgery for a percutaneous bone conduction device with a laser ablated fixture. Outcomes were assessed at screening, during surgery, 7–10 days after surgery, 6–14 weeks after surgery, and 12 months after surgery. The primary outcome was implant stability over 12 months. Furthermore, implant survival, skin reactions, and audiological performance were evaluated, and implant survival was compared to a retrospective control cohort.
Results: Fifteen study participants with a mean age of 6 years (range 3–12 years) were included. Three were bilaterally implanted, rendering a total of 18 implants. Implant stability showed a 10-point increase in mean implant stability measurements at 12 months, compared to at surgery. Four implants (22%) were lost before the 12-month follow-up, which was comparable to the retrospective cohort where the 12-month implant loss rate was 23%. Across the 12-month period, 8/18 implant sites had a maximum Holgers score of 0, indicating no skin reactions. The remaining implant sites had a maximum Holgers score of 1–3.
Conclusion: In conclusion, this study shows safe and reliable outcomes using laser ablated fixtures for one stage surgery in a pediatric population.
Public trial registration: ClinicalTrials.gov, identifier: NCT03723161.
1 Introduction
Bone conduction devices (BCDs) are used to transmit sound through the bone of the skull to the cochlea when conventional hearing aids are not an option, such as in cases of aural atresia or chronically infected ears. BCDs can be used in passive transcutaneous forms from infancy, worn on a soft headband or a more rigid arc. Titanium fixtures used for dental prosthesis were initially developed by Brånemark in Gothenburg, Sweden and has been used for hearing implants since 1977 (Tjellström et al., 1981). Surgically implanted percutaneous BCDs using titanium implants fixated in the temporal bone, a skin-penetrating abutment and a sound processor attached to the abutment have been the treatment of choice due to their superior sound transmission properties. As the implant is fixed into the bone of the skull, the attenuation of the skin and soft tissues is surpassed, allowing a higher degree of amplification, especially in the higher frequencies (Verstraeten et al., 2009; Reinfeldt et al., 2015). Percutaneous BCDs are generally available from approximately 3 years of age, though practices vary (Kruyt et al., 2020).
Since its invention, the surgical technique for implanting percutaneous BCDs have developed from invasive two-stage procedures with extensive tissue reduction and skin transplants to minimally invasive one-stage procedures supporting tissue preservation (Lagerkvist et al., 2020). Once the implant fixture is placed in the bone, the titanium will osseointegrate into the bone, an immune driven process where new bone will form on the surface if the implant anchoring it more firmly into the implant site. The process of osseointegration is affected by surgical technique, implant surface structure and form, as well as individual factors such as the quality of the surrounding bone, comorbidities, smoking and BMI (Esposito et al., 1998; Lee and Bance, 2019). Children have been found to be more prone to implant loss compared to adults (McDermott et al., 2009; Bezdjian et al., 2018), and also have a larger proportion of skin irritation at the implant site (Kruyt et al., 2020). In the pediatric population, wide implants with a diameter of 4.5 mm have been found to provide a higher implant survival rate than the original 3.75 mm implants (Kruyt et al., 2020). Recent clinical studies on laser ablated implants used for BCDs have shown an implant survival rate of 97% in adults (Kruyt et al., 2018) and 96.6% in children (Osborne et al., 2022). Both the wider diameter and the laser ablated surfaces contributes to a larger bone-implant interface and thereby an improved biomechanical anchorage compared to the traditional machined implants, and thereby improved implant stability (Westerkull and Jinton, 2012; Shah et al., 2016; Lee and Bance, 2019).
The purpose of this study was to evaluate the performance and stability of the laser ablated implant Ponto BHX implant, following a one-stage implantation procedure in a pediatric population. Implant stability quotient (ISQ) 12 months after implantation was the primary endpoint. Implant survival was compared to a retrospective cohort of pediatric study participants from the same clinic.
2 Materials and methods
2.1 Study design
The study was designed as a prospective, single center observational study of pediatric study participants undergoing one-stage surgery for a BCD using a laser ablated Ponto BHX implant (Oticon Medical, Askim, Sweden). For comparison of implant survival, a retrospective control group implanted with the previous Ponto Wide implant was included.
2.2 Study population
Patients between 2.5 and 18 years of age diagnosed with unilateral or bilateral congenital conductive hearing loss, referred for percutaneous BCD surgery and eligible for one-stage surgery, were invited to participate in the study. Furthermore, all study participants used BCD on a softband during a trial period of at least 2 weeks prior to surgery. Before inclusion, parents or legal guardians had to provide informed consent in writing. Individuals not fluent in Swedish (patient or legal guardian) or those who did not wish to participate in follow-up visits were excluded. Participants were withdrawn if they could not undergo one-stage procedure, lost the implant, were unwilling/unable to attend follow-up visits or considered unfit to continue by the responsible physician. Participants were included in the prospective cohort between September 2018 and November 2021.
The retrospective cohort consisted of children aged 2.5–18 years, diagnosed with congenital conductive hearing loss, that had undergone one-stage BCD surgery using the Ponto Wide implant prior to 2018 (actual surgery dates September 2012–November 2017).
2.3 Implants
The implants used in the prospective cohort were the Ponto BHX Implant, while the Ponto Wide implant was used in the retrospective cohort (Oticon Medical, Askim, Sweden). The Ponto Wide and Ponto BHX implants are similar in design, but the Ponto BHX implant has a laser ablated surface (Biohelix™), which has been shown to improve osseointegration (Westerkull and Jinton, 2012; Shah et al., 2016). The implants both have a diameter of 4.5 mm and are available in two different lengths (3 and 4 mm). Both implants are available with a pre-mounted abutment (length 6, 9, 12, or 14 mm), which is suitable for one-stage implantation. Implants without pre-mounted abutments were used as sleeper implants.
2.4 Surgical procedure
Implantation was performed under general anesthesia using a one-stage, single incision technique without skin thinning (Hultcrantz, 2015). The thickness of the skin at the implant site was measured using a needle prior to injection of local anesthesia. Implants were positioned posterior to or at the incision line. The thickness and quality of the bone was noted while drilling was performed, as well as any complications, such as bleeding and exposure of the dura mater. A pre-mounted implant/abutment complex was installed, as well as a separate sleeper implant. The skin was then punched to fit the abutment and threaded over the abutment. The skin incision was sutured, and a healing cap was installed covering the implant site.
2.5 Measurements of implant stability
ISQ was measured using an Ostell ISQ device (Osstell AB, Gothenburg, Sweden). The device uses resonance frequency analysis (RFA) to excite a small rod (SmartPeg, Osstell AB, Gothenburg, Sweden) inserted into the abutment. The vibrations transmitted through the abutment and implant are measured by the device and expressed as ISQ on a scale of 1–100, with a higher value indicating a more stable implant (Sennerby and Meredith, 2008). Two perpendicular measurements were done and the lower of the two (denoted ISQ low) was the primary endpoint, while the higher (denoted ISQ high) was reported as a secondary outcome.
2.6 Follow-up visits
Surgical follow-up was planned at 7–10 days post-surgery, while fitting of the sound processor was scheduled 6–14 weeks after surgery. In addition, the patient visited the clinic for follow-up assessments at 12 and 24 months after surgery. The present study includes data up to the primary endpoint evaluation at 12 months. ISQ values were measured at all follow-up visits. Skin healing was assessed as well as skin reactions according to the Holgers score (Holgers et al., 1988) and the IPS (Inflammation, Pain, Skin height) score (Kruyt et al., 2017). In addition, data was collected at any unplanned visits occurring between the scheduled follow-up visits.
2.7 Sound processor fitting and audiological assessment
Audiological measurements were performed by an experienced pediatric audiologist at the hearing rehabilitation clinic for children, in a soundproof double walled booth according to ISO 8253-1:2010 using a Ponto sound processor (Oticon Medical, Sweden). Pure tone thresholds were obtained at 250, 500, 1,000, 2,000, 4,000, and 6,000 Hz in a free sound field. Pure tone average (PTA4) was calculated as the average of thresholds at 500, 1,000, 2,000, and 4,000 Hz. Prior to surgery, thresholds were obtained with the patient wearing the sound processor on a Softband, while thresholds were obtained with the sound processor on the abutment at the fitting visit and at the 12-month visit. Bone conduction (BC) in situ measurements were conducted as part of the fitting process in the fitting software (Genie Medical, Oticon Medical, Sweden) at all three occasions. In bilateral cases, BC in situ assessments were performed separately for each implant whereas aided thresholds were tested with both sound processors activated. In the case of unilateral implantation, the contralateral ear was blocked during audiological testing using an earplug (3M 1100, Minnesota, USA) and an earmuff (Peltor Optime III, Minnesota, USA).
2.8 Statistical analysis
Due to the observational nature of the study, the analysis consisted of within subject comparisons over time. Conservative, non-parametric Wilcoxon Signed Rank test was used for comparisons of continuous data, due to the relatively small sample size and deviations from normal distribution. Data was analyzed using Microsoft Excel (Microsoft 365, version 2303) and R (version 4.3.1, The R Foundation for Statistical Computing, Vienna, Austria). Missing data was imputed using last observation carried forward for the primary outcome (ISQ low), while secondary outcomes were analyzed using an intention-to-treat approach including all available data without imputation.
Sample size was calculated for the primary endpoint, ISQ low at 12-month follow-up compared to at surgery, to detect a difference of 5 ISQ points. A standard deviation of 5 was assumed, and the significance level was set to 5%, with 80% power, leading to a minimum of 14 study implants needed to be included.
3 Results
3.1 Population
Fifteen individuals were included in the prospective cohort. Three study participants were bilaterally implanted; therefore the total number of implants was 18. During the first 12 months, 4 implants/3 study participants were excluded due to implant loss and 2 study participants/implants were lost to follow up (Figure 1). Both participants who were lost to follow up left the study after fitting. All enrolled study participants were included in the primary analysis population. In the retrospective cohort, 28 individuals were included out of which three were bilaterally implanted, resulting in a total of 31 implants.
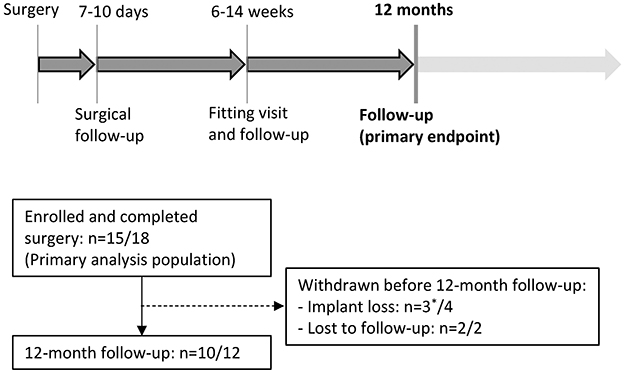
Figure 1. Study design (top) and flow chart of participants enrolled in the prospective cohort (bottom). n denotes study participants/implants. *One patient was bilaterally implanted and was not excluded as the other implant was not lost.
Demographics for the enrolled study participants in both cohorts are presented in Table 1. Mean ± SD age was 5.6 ± 2.8 in the prospective cohort and 6.3 ± 4.1 in the retrospective cohort. In both groups there was a male predominance (11/14 in the prospective cohort and 20/28 in the retrospective cohort). In the prospective cohort 7/15 study participants were < 5 years old at the time of surgery, while the corresponding numbers were 13/28 study participants in the retrospective cohort. All participants in the prospective cohort had congenital conductive hearing loss, all but one having aural atresia. Atresia was present in 26 of the participants in the retrospective cohort. In the prospective cohort, three participants were syndromic as of one in the retrospective group (Table 1).
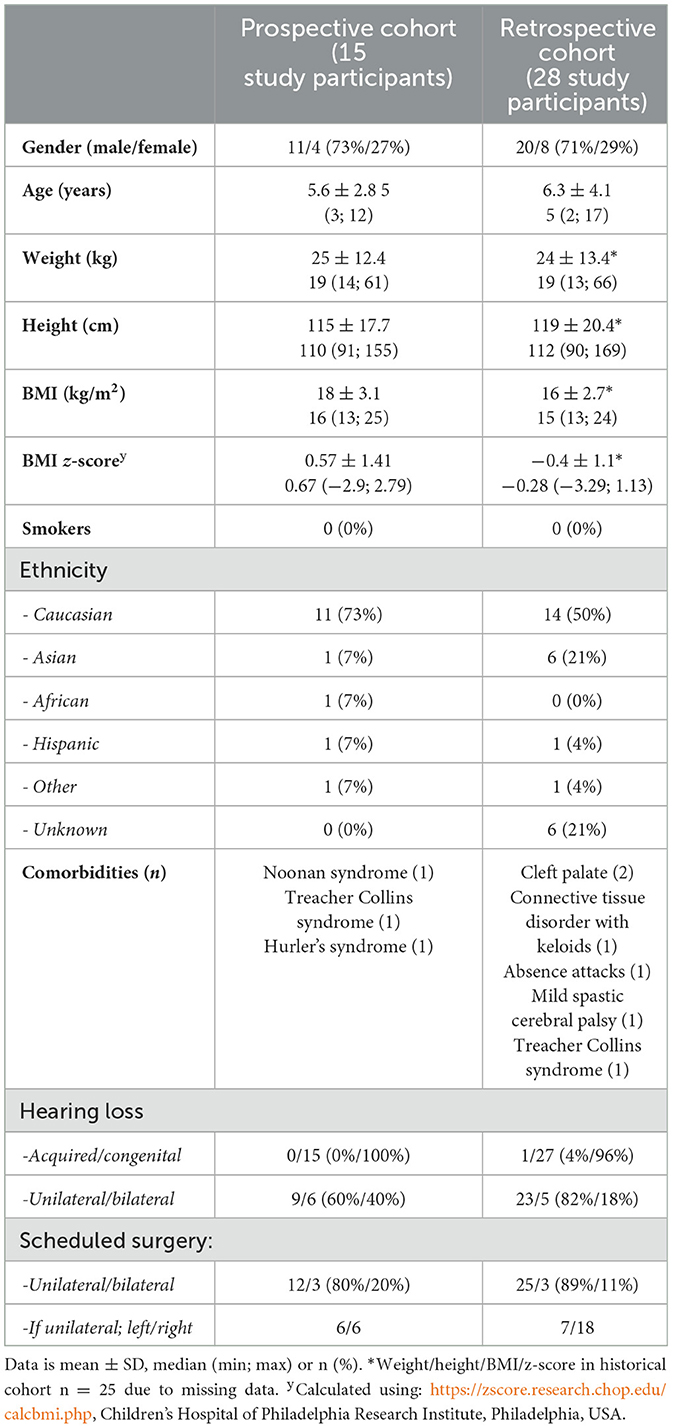
Table 1. Demographic data.
3.2 Surgical data
3.2.1 Prospective cohort
All surgeries were performed under general anesthesia followed by local anesthesia in the surgical field by an experienced surgeon. Linear incision technique was used in 17 cases; in one case the incision was placed in an older semi-circumferent scar. The skin thickness was (mean ± SD) 4.0 ± 1.0 mm, and no reduction of subcutaneous tissue was performed. Of the implants inserted 9 were 4 mm and 9 were 3 mm. All participants also received a sleeper implant (4 mm n = 5, 3 mm n = 13). Reported surgical events were exposure of the dura mater (n = 12), repositioning of the implant (n = 2), angled insertion of implant (n = 1) and revision of skin punch hole (n = 1). Abutment lengths used were 6 mm (n = 9) and 9 mm (n = 9). All implants were fully seated at the end of the procedure.
3.2.2 Retrospective cohort
Study participants were implanted with wide implant; either 4 mm (n = 6) and 3 mm (n = 25) long. All surgeries were performed under general anesthesia and supplemented with local anesthetics in 30/31 implant sites. Skin thickness was measured to (mean ± SD) 4.4 ± 2.0 mm (n = 27, data not available in 4 cases). No reduction of subcutaneous tissue had been performed. Most participants were operated using the linear incision technique (n = 30) whereas one participant underwent Minimally Invasive Ponto Surgery (MIPS; Johansson et al., 2017). The abutment lengths used were 6 mm (n = 25), 9 mm (n = 3), and 12 mm (n = 3). One implant was partially seated whereas 30 were fully seated. In most cases, a wide sleeper implant was installed (4 mm n = 2, 3 mm n = 21, unknown/not used n = 8).
3.3 Implant stability
ISQ was measured at the end of surgery, at 7–10 days postoperatively and at 12 months follow up in the prospective cohort. ISQ high/low was (mean ± SD) 45 ± 9.7/39 ± 10.4 (n = 18) at surgery, 45 ± 9.7/37 ± 11.0 (n = 18) at 7–10 days postoperatively and 54 ± 6.8/49 ± 7.7 (n = 11) at 12 months follow up. When comparing ISQ high/low for the 14 implants still in situ at 12 months follow up data imputed using last observation carried forward for 3 implants with missing data (2 lost to follow up, 1 missed visit), there was a significant improvement in implant stability between surgery and 12 months (p = 0.011; ISQ high) and p = 0.014 (ISQ low; Figure 2).
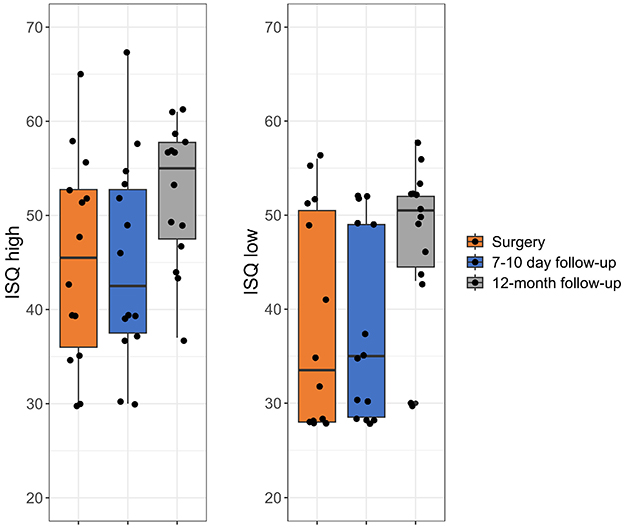
Figure 2. Implant stability quotient (ISQ) high and low at surgery, 7–10-day follow-up and at 12-month follow-up. Data is shown as individual datapoints, as well as summarizing boxplot. Lost implants have been excluded, and missing data has been imputed using last observation carried forward (n = 3 at 12-month follow-up), for primary analysis of the primary endpoint.
3.4 Implant survival
During the first 12 months, 4 of 18 implants in the prospective cohort were lost resulting in an implant survival rate of 78% (3 mm implant n = 3, 4 mm implant n = 1). The traumatic implant loss occurred in a bilaterally implanted 3-year-old patient who suffered a fall 38 days after surgery which led to loss of one implant, while the other was not affected and was in situ at the 12-month follow-up. No skin reactions or other problems were reported prior to the incident, and the site of the lost implant was reported to heal well.
The other three implant losses occurred 87, 258, and 266 days after surgery, in unilaterally implanted patients (aged 4, 6, and 8 years), and were reported to be caused by infections. The loss that occurred 87 days after surgery, was preceded by a 2-month long period of recurring infections leading up to the implant loss, although there were no indication of infections or skin reactions at the 7–10-day visit. The ISQ measured at surgery and 7–10-day follow-up were 41/35 and 44/43 (ISQ high/low), respectively. For the implant losses occurring 266 and 258 days after surgery, there were no reported skin reactions, aside from a single occurrence of inflammation in one of the implants 6 months prior to the implant loss that was treated with topical antibiotics. The ISQ values were as follows: 46/44 (surgery), 41/36 (7–10-day visit) and 46/44 (surgery), 46/12 (7–10-day visit; ISQ high/low).
In the retrospective cohort, 7/31 implants were lost during the first year of follow up resulting in a 77% implant survival rate (3 mm implant n = 6, 4 mm implant n = 1). The implant losses were attributed to traumatic implant losses n = 3 (38–82 days after surgery), spontaneous losses n = 3 (32–79 days after surgery) and infection n = 1 (48 days after surgery). One of the cases with traumatic implant loss had reported some infection at the implant site in the days leading up to a fall that caused the implant loss. The case with implant loss due to infection was treated with antibiotic ointment in the week leading up to the loss of the implant. No skin reactions or other problems were reported for the remaining cases that suffered implant loss.
3.5 Skin reactions
Skin reactions in the prospective cohort were addressed using the Holgers scale as well as the IPS scores at all scheduled follow up visits and at any unplanned visits. At 7–10 days postoperatively, the surgical wound was noted to be healed in all study participants and a Holgers score of 0 as well as an IPS score of 0 observed in all implant sites (Tables 2, 3). At 12-month follow-up, four implants were noted to have a Holgers score or IPS score above 0 (max scores Holgers 2, I2P1S1), however skin reactions were more frequently registered at unscheduled visits (Tables 2, 3). Fifty percentage (n = 9) of the implant sites had an adverse skin reaction (maximum Holgers ≥2) at least once during the time of follow up (Table 2).
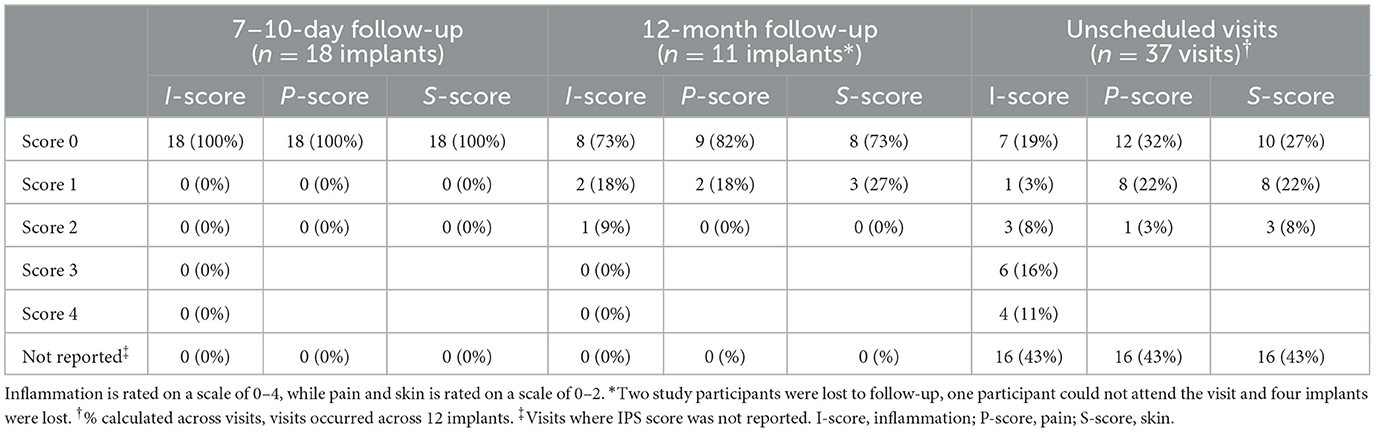
Table 2. Inflammation, pain, and skin (IPS) scores across visits (n = 18 implants in 15 study participants).
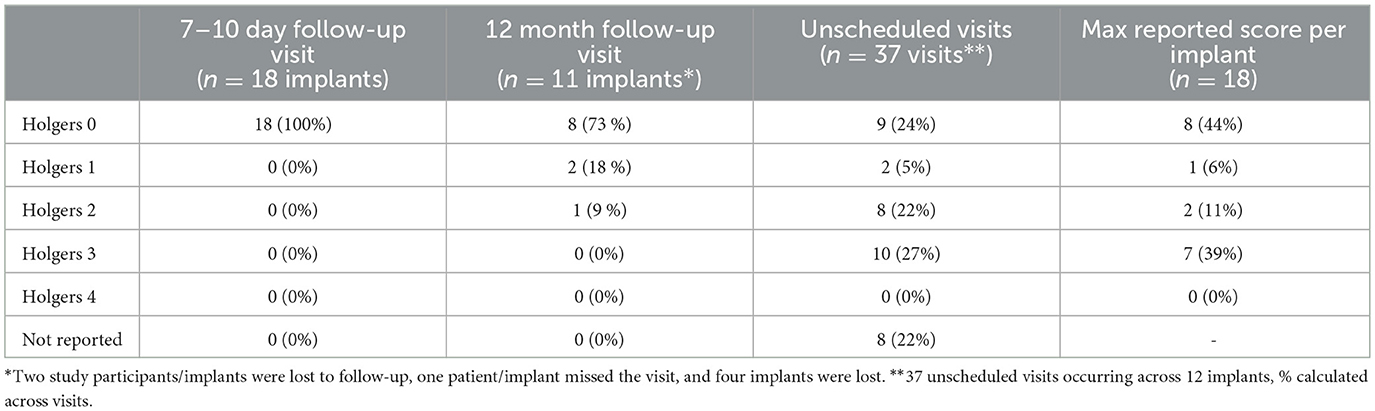
Table 3. Holgers scores across visits and implants (n = 18 implants in 15 study participants).
Of the three implants that were lost due to infection, two were reported to have a maximum Holgers score of 3 and maximum IPS scores of I4P2S2 and I4P1S0. For the third infection-related implant loss, no Holgers or IPS scores were reported aside from the 7–10 follow-up visit where no skin reaction was observed (all scores 0). The last implant loss was a traumatic loss, where no skin reactions were observed prior to the traumatic event that led to the implant loss.
3.6 Audiological performance
On average, study participants were fitted with the sound processor 8 weeks after surgery (range: 4–12 weeks). BC in situ thresholds were lower at fitting when using the abutment, compared to at screening when using the sound processor on a softband, primarily at the higher frequencies (1,000–6,000 Hz; Table 4). A similar pattern was observed for the aided thresholds. PTA4 was lower in the abutment aided conditions at fitting, compared to softband aided conditions at screening (mean difference: −4 ± 4.6 dB, p = 0.028). Generally, the difference in BC in situ and aided thresholds seemed to attenuate over the 12-month follow-up period, however this could be caused by the reduction in sample size, and consequently loss of power, due to fewer study participants completing audiological assessment at 12 months. This is supported by the estimates at 12-month follow-up being similar to those at fitting (Table 4). In 78% of the cases, the audiological assessments were performed using sound processors belonging to the Ponto 3 family (mainly Ponto 3 SuperPower), whereas the remaining were done using Ponto 4, Ponto Pro and Ponto Plus.
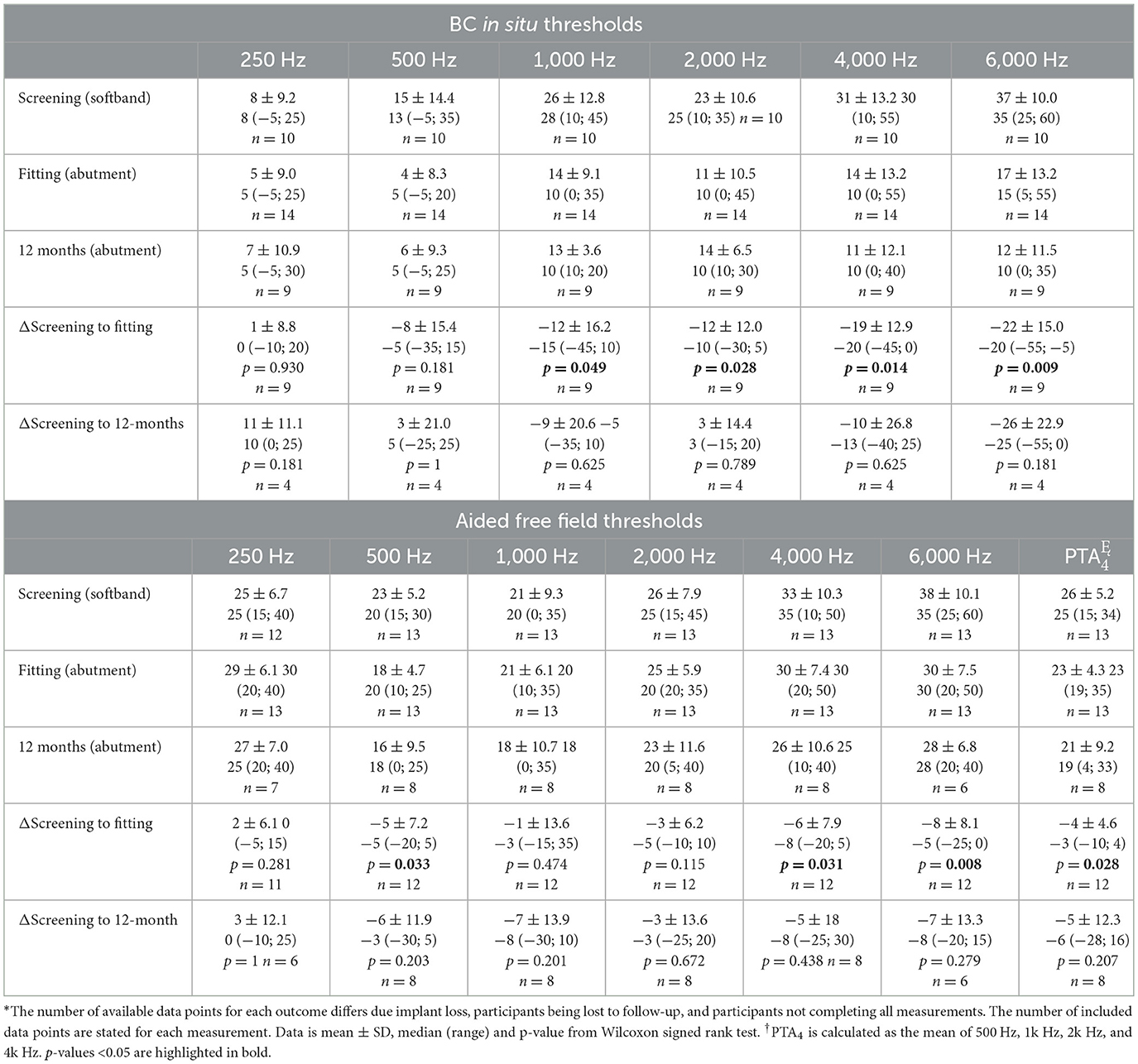
Table 4. BC in-situ (n = 18 implanted ears*) and aided free field thresholds (n = 15 study participants*) evaluated at screening, fitting and 12-month follow-up.
4 Discussion
This study reports 1 year data on a pediatric population, characterized by a relatively low age and prevalence of co-morbidities, undergoing BCD treatment in a one-stage implantation surgery. These patients were implanted with the laser-ablated Ponto BHX implant and implant survival was compared to a retrospective cohort of pediatric patients implanted with the previous generation of implants without laser ablation (Ponto Wide). The two cohorts were similar in their baseline characteristics. Typically, BCD is used when conventional hearing aids are not an option such as in congenital aural atresia, which is known to affect males in a higher degree (Kelley and Scholes, 2007), explaining the male predominance in both groups.
The primary outcome was ISQ, which increased significantly over time, which is indicative of developing osseointegration (McLarnon et al., 2014). The increase was mainly driven by an increase in ISQ score for the implants with the lowest scores at surgery, whereas the implants that already had higher ISQ scores at surgery did not increase substantially over time. The increase in ISQ over time is comparable to the findings of previous publications investigating the same implant (Kruyt et al., 2018; Osborne et al., 2022; Moller et al., 2024). Abutment length has been shown to affect ISQ scores, longer abutments being associated with lower ISQ- values (Høgsbro et al., 2020) and it cannot be ruled out that some of the variation in the ISQ data was influenced by different abutment lengths. However, none of the participants had a change in abutment during the follow-up period and statistical evaluation evaluated intra-individual changes over time, minimizing the influence of inter-individual variation due to differences in abutment length. As there are no established reference values for ISQ of hearing implants, conclusions based on absolute values should be done with care. The values observed in the present study are similar to what has been observed in recent studies (Moller et al., 2024; Teunissen et al., 2025b,a), albeit slightly lower than some older studies (Wazen et al., 2015; Nelissen et al., 2016).
The implant survival rate was 78% in the prospective cohort, which is lower than what is generally expected (Kruyt et al., 2020; Lagerkvist et al., 2020). However, implant losses are more frequent in younger pediatric populations (Kruyt et al., 2020) and in syndromic populations (Salameh et al., 2023). The implant survival rate was similar in the retrospective cohort indicating that the implant survival rate found in this investigation is in line with what can be expected in this specific population (Bezdjian et al., 2018; Salameh et al., 2023; Bradley et al., 2024). Though traumatic implant losses are more common in pediatric patients than in adult patients (Bezdjian et al., 2018), implant losses due to other reasons such as infection or failed osseointegration are frequently reported as a cause of implant losses in children (Salameh et al., 2023; Bradley et al., 2024).
The rough surface of the laser ablated implant possibly allows for a firmer osseointegration in the first months after implantation. Such clinical correlations need to be further investigated but it can be noted that implant losses in the retrospective cohort all occurred within 3 months post-surgery, whereas the implant losses in the prospective cohort occurred more widespread over the 12-month follow-up period. However, conclusions should be drawn carefully as the sample size in the present study is small and the retrospective and prospective method of data collection may not be completely comparable. Generally, the ISQ scores of the lost implants were similar to those of the implants that remained in situ, indicating no association between implant survival and ISQ score. However, ISQ was only measured at surgery and 7–10 days post-surgery in the lost implants, thus it is unknown how the ISQ scores developed up to the time of the implant losses which occurred at 38–266 days after surgery. ISQ was not routinely measured in the retrospective cohort, and no comparison could be made.
There was a relatively high frequency of skin reactions with 50% (9/18) of the implant sites having an adverse skin reaction (Holgers ≥2) at least once during the 12-month follow-up. This was also reflected in the IPS scores, where skin reactions were frequently reported. However, other studies have shown that populations including syndromic pediatric study participants and younger children are more prone to skin reactions, so although the frequency of skin reactions was seemingly high it may be within normal range in this population (Amonoo-Kuofi et al., 2015; Salameh et al., 2023; Bradley et al., 2024). Importantly, skin reactions were not severe enough to warrant abutment removal or revision surgery, indicating that although there was a high frequency of skin reactions, they could be sufficiently managed. During the first years of the study, the organization for managing complications arising in individuals with percutaneous BCDs changed at our hospital, and new staff had to be trained to manage these issues. Furthermore, a large part of the study was conducted during the COVID-19 pandemic, which introduced changes in the routines around surgical procedures and general follow-up in many parts of the healthcare system (Ekman et al., 2021; Melander et al., 2021). These factors might have affected the study participants and thereby the results of the study.
Three of the four implant losses in the prospective cohort were attributed to infections. However, among the implants in situ after 12 months, the prevalence of adverse skin reactions during the 12-month were also 50% (7/14), indicating that the rate of skin reactions was not systematically higher among study participants who suffered implant losses. The last implant loss within the prospective cohort was due to trauma to the implant site approximately 1 month after surgery. This patient was bilaterally implanted and as the other implant was in place at the 12-month follow-up, it is likely that the implant loss was not mediated by poor osseointegration, but merely a traumatic implant loss which children are generally more prone to than adults (McDermott et al., 2009).
An implant loss rate of approximately 15% has been previously described in children (Kruyt et al., 2020). Osborne et al. (2022) reported an implant loss rate of only 3.4% using the wide Ponto BHX implant. The discrepancy to the present study might be partially explained by differences in the base line characteristics of the study participants. The participants in the study by Osborne et al. (2022) were slightly older (8.8 ± 3.5 years of age) and surgery was performed in two stages. There was also a slight female dominance in the study by Osborne, compared to the male dominance in the present study. This could indicate that the underlying indications for the surgery differs between the cohorts, as certain indications, such as atresia, are more common among males than females. It cannot be ruled out that the difference in implant failure might be due to patient selection, the younger children in the present study being more prone to infections and head trauma (McDermott et al., 2009; Amonoo-Kuofi et al., 2015) or due to differences in surgical technique.
Traditionally a two-stage approach has been employed for BCD surgery in children, where the implant with a cover screw is inserted in the skull bone and allowed to osseointegrate, before the skin penetrating abutment is placed in a second surgery (Doshi et al., 2012). Performing the surgery in two stages has mainly been a precaution, as children tend to have thinner skull bones than adults and can be more prone to traumatic injuries to the implant site, leading to implant loss. However, one-stage surgery is standard practice in adult populations today and has been adopted for pediatric populations with good results (Saliba et al., 2012; Kruyt et al., 2020; Moller et al., 2024; Teunissen et al., 2025b,a). As most implantations in children are performed under general anesthesia, the one-stage procedure has an obvious advantage as the child only needs to undergo anesthesia once. Furthermore, as only one procedure is needed, the time between decision to treat and the child being fitted with a sound processor can be shortened substantially (Teunissen et al., 2025a). Even though the implant loss rate in the present study was high, the authors still consider one stage surgery for BCD to be safe and advantageous compared to two stage surgery. If all participants who suffered implant loss in the present study underwent a second surgery to call up the sleeper implant, a second surgery under general anesthesia would still only have had to be performed in 22%, compared to 100% if a two-stage surgery protocol was to be applied.
The audiological data suffered from a high degree of missing data, mainly due to the young age of the study participants, who had difficulties completing the audiological tests. Furthermore, most of the assessments were performed with sound processors belonging to the Ponto 3 family, which has since been surpassed by the Ponto 4 and Ponto 5 families of sound processors. Nonetheless, the PTA4 for aided free-field thresholds and the BC in-situ indicate an improvement in hearing thresholds when switching from a passive transcutaneous to a percutaneous device. The difference was most noticeable in the higher frequencies, which is in line with previous findings (Verstraeten et al., 2009; Pittman, 2019).
4.1 Conclusion
In conclusion, this study shows a positive development in implant stability over a 12-month period using the laser ablated Oticon Ponto BHX implant in a pediatric population having undergone one stage surgery. The complication rate and implant loss rate were higher than what is expected in the general population, but within normal range considering that the population is characterized by young children who are prone to traumatic implant loss and with a prevalence of comorbidities that might be associated with worse outcomes. Audiological data suffered from a high degree of missing data, but nonetheless the available data did indicate a positive change in hearing thresholds when with an implantable BCD compared to the non-surgical solution.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the regional Ethical Committee in Stockholm (Regionala etikprövningsnämnden i Stockholm). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
HJ: Data curation, Investigation, Project administration, Resources, Visualization, Writing – original draft, Writing – review & editing. KI: Data curation, Formal analysis, Project administration, Visualization, Writing – original draft, Writing – review & editing. MH: Conceptualization, Data curation, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing. CE: Data curation, Investigation, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The study was funded by Oticon Medical AB, Askim, Sweden.
Conflict of interest
KI is a paid employee of Oticon Medical AB. HJ has received financial support from Stiftelsen Tysta skolan, Swedish Association for Otorhinolaryngology Head and Neck Surgery (SFOHH), and ACTA otolaryngologica. During the study period CE received financial support from ACTA otolaryngologica and grants from Center for Innovative Medicine (CIMED) Karolinska Institutet and ALF Region Stockholm.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Amonoo-Kuofi, K., Kelly, A., Neeff, M., and Brown, C. R. (2015). Experience of bone-anchored hearing aid implantation in children younger than 5 years of age. Int. J. Pediatr. Otorhinolaryngol. 79, 474–480. doi: 10.1016/j.ijporl.2014.12.033
Bezdjian, A., Smith, R. A., Thomeer, H., Willie, B. M., and Daniel, S. J. (2018). A systematic review on factors associated with percutaneous bone anchored hearing implants loss. Otol. Neurotol. 39, e897–e906. doi: 10.1097/MAO.0000000000002041
Bradley, M., Shields, C., Sabourn, R., Whittle, E., Boyd, R., Bruce, I. A., et al. (2024). Paediatric percutaneous bone anchored hearing aid implant failures: comparing the experience of a tertiary centre with a systematic review of the literature and meta-analysis. Cochlear Implants Int. 25, 1–13. doi: 10.1080/14670100.2024.2332036
Doshi, J., Sheehan, P., and McDermott, A. L. (2012). Bone anchored hearing aids in children: an update. Int. J. Pediatr. Otorhinolaryngol. 76, 618–622. doi: 10.1016/j.ijporl.2012.02.030
Ekman, B., Arvidsson, E., Thulesius, H., Wilkens, J., and Cronberg, O. (2021). Impact of the Covid-19 pandemic on primary care utilization: evidence from Sweden using national register data. BMC Res. Notes 14:424. doi: 10.1186/s13104-021-05839-7
Esposito, M., Hirsch, J. M., Lekholm, U., and Thomsen, P. (1998). Biological factors contributing to failures of osseointegrated oral implants. (II). Etiopathogenesis. Eur. J. Oral. Sci. 106, 721–764. doi: 10.1046/j.0909-8836.t01-6-.x
Høgsbro, M., Agger, A., Johansen, L. V., and Gaihede, M. (2020). In vitro investigation of the dependency between abutment length and implant stability quotient (ISQ) for stability measurements on bone anchored hearing implant systems. Otol. Neurotol. 41, 848–854. doi: 10.1097/MAO.0000000000002620
Holgers, K. M., Tjellstrom, A., Bjursten, L. M., and Erlandsson, B. E. (1988). Soft tissue reactions around percutaneous implants: a clinical study of soft tissue conditions around skin-penetrating titanium implants for bone-anchored hearing aids. Am. J. Otol. 9, 56–59.
Hultcrantz, M. (2015). Stability testing of a wide bone-anchored device after surgery without skin thinning. Biomed. Res. Int. 2015:853072. doi: 10.1155/2015/853072
Johansson, M. L., Stokroos, R. J., Banga, R., Hol, M. K., Mylanus, E. A., Savage Jones, H., et al. (2017). Short-term results from seventy-six patients receiving a bone-anchored hearing implant installed with a novel minimally invasive surgery technique. Clin. Otolaryngol. 42, 1043–1048. doi: 10.1111/coa.12803
Kelley, P. E., and Scholes, M. A. (2007). Microtia and congenital aural atresia. Otolaryngol. Clin. North Am. 40, 61–80, vi. doi: 10.1016/j.otc.2006.10.003
Kruyt, I. J., Bakkum, K. H. E., Caspers, C. J. I., and Hol, M. K. S. (2020). The efficacy of bone-anchored hearing implant surgery in children: a systematic review. Int. J. Pediatr. Otorhinolaryngol. 132:109906. doi: 10.1016/j.ijporl.2020.109906
Kruyt, I. J., Banga, R., Banerjee, A., Mylanus, E. A. M., and Hol, M. K. S. (2018). Clinical evaluation of a new laser-ablated titanium implant for bone-anchored hearing in 34 patients: 1-year experience. Clin. Otolaryngol. 43, 761–764. doi: 10.1111/coa.13060
Kruyt, I. J., Nelissen, R. C., Johansson, M. L., Mylanus, E. A. M., and Hol, M. K. S. (2017). The IPS-scale: a new soft tissue assessment scale for percutaneous and transcutaneous implants for bone conduction devices. Clin. Otolaryngol. 42, 1410–1413. doi: 10.1111/coa.12922
Lagerkvist, H., Carvalho, K., Holmberg, M., Petersson, U., Cremers, C., and Hultcrantz, M. (2020). Ten years of experience with the Ponto bone-anchored hearing system-a systematic literature review. Clin. Otolaryngol. 45, 667–680. doi: 10.1111/coa.13556
Lee, J. W. Y., and Bance, M. L. (2019). Physiology of osseointegration. Otolaryngol. Clin. North Am. 52, 231–242. doi: 10.1016/j.otc.2018.11.004
McDermott, A. L., Williams, J., Kuo, M., Reid, A., and Proops, D. (2009). The birmingham pediatric bone-anchored hearing aid program: a 15-year experience. Otol. Neurotol. 30, 178–183. doi: 10.1097/MAO.0b013e31818b6271
McLarnon, C., Johnson, I., Davison, T., Hill, J., Henderson, B., Leese, D., et al. (2014). Resonance frequency analysis of osseo-integrated implants for bone conduction in a pediatric population - a novel approach for assessing stability for early loading. Int. J. Pediatr. Otorhinolaryngol. 78, 641–644. doi: 10.1016/j.ijporl.2014.01.023
Melander, S., Almström, J., Enlund, G., and Frykholm, P. (2021). The COVID-19 pandemic first wave in Sweden: a national registry study of the effects on pediatric anesthesia and surgery. Paediatr. Anaesth. 31, 846–853. doi: 10.1111/pan.14203
Moller, M. L., Foghsgaard, S., and Hougaard, D. D. (2024). Very early loading of a bone-anchored hearing system is safe. Otol. Neurotol. 45, 556–563. doi: 10.1097/MAO.0000000000004190
Nelissen, R. C., den Besten, C. A., Faber, H. T., Dun, C. A., Mylanus, E. A., and Hol, M. K. (2016). Loading of osseointegrated implants for bone conduction hearing at 3 weeks: 3-year stability, survival, and tolerability. Eur. Arch. Otorhinolaryngol. 273, 1731–1737. doi: 10.1007/s00405-015-3746-y
Osborne, M. S., Child-Hymas, A., Holmberg, M., Thomsen, P., Johansson, M. L., and McDermott, A. L. (2022). Clinical evaluation of a novel laser-ablated titanium implant system for bone anchored hearing systems in a pediatric population and the relationship of resonance frequency analysis with implant survival. Otol. Neurotol. 43, 219–226. doi: 10.1097/MAO.0000000000003435
Pittman, A. L. (2019). Bone conduction amplification in children: stimulation via a percutaneous abutment versus a transcutaneous softband. Ear Hear. 40, 1307–1315. doi: 10.1097/AUD.0000000000000710
Reinfeldt, S., Hakansson, B., Taghavi, H., and Eeg-Olofsson, M. (2015). New developments in bone-conduction hearing implants: a review. Med. Devices 8, 79–93. doi: 10.2147/MDER.S39691
Salameh, S., El-Khoury, S., Bezdjian, A., Roy, C. F., Khneisser, E., Bianchi, M., et al. (2023). Percutaneous bone-anchored hearing implant surgery: do syndromic children have more adverse perioperative outcomes? Otol. Neurotol. 44, e504–e511. doi: 10.1097/MAO.0000000000003922
Saliba, I., Froehlich, P., and Bouhabel, S. (2012). One-stage vs. two-stage BAHA implantation in a pediatric population. Int. J. Pediatr. Otorhinolaryngol. 76, 1814–1818. doi: 10.1016/j.ijporl.2012.09.007
Sennerby, L., and Meredith, N. (2008). Implant stability measurements using resonance frequency analysis: biological and biomechanical aspects and clinical implications. Periodontol 2000 47, 51–66. doi: 10.1111/j.1600-0757.2008.00267.x
Shah, F. A., Johansson, M. L., Omar, O., Simonsson, H., Palmquist, A., and Thomsen, P. (2016). Laser-modified surface enhances osseointegration and biomechanical anchorage of commercially pure titanium implants for bone-anchored hearing systems. PLoS ONE 11:e0157504. doi: 10.1371/journal.pone.0157504
Teunissen, E., Caspers, C., Kruyt, I., Mylanus, E., and Hol, M. (2025b). Long-term clinical outcomes for bone-anchored hearing implants: 3-year comparison between minimally invasive ponto surgery and the linear incision technique with tissue preservation. Otol. Neurotol. 46, 161–169. doi: 10.1097/MAO.0000000000004398
Teunissen, E. M., Aukema, T. W., Caspers, C. J. I., Bakkum, K. H. E., Kruyt, I. J., Cals, F. L. J., et al. (2025a). Single-stage bone-anchored hearing implant surgery in children: a prospective comparative study. Acta Otolaryngol. 145, 1–8. doi: 10.1080/00016489.2025.2476188
Tjellström, A., Lindström, J., Hallen, O., Albrektsson, T., and Brånemark, P. I. (1981). Osseointegrated titanium implants in the temporal bone. A clinical study on bone-anchored hearing aids. Am. J. Otol. 2, 304–310.
Verstraeten, N., Zarowski, A. J., Somers, T., Riff, D., and Offeciers, E. F. (2009). Comparison of the audiologic results obtained with the bone-anchored hearing aid attached to the headband, the testband, and to the “snap” abutment. Otol. Neurotol. 30, 70–75. doi: 10.1097/MAO.0b013e31818be97a
Wazen, J. J., Daugherty, J., Darley, S., and Wycherly, B. (2015). Three week loading for the Baha BI-300(R) implant system. Am. J. Otolaryngol. 36, 195–199. doi: 10.1016/j.amjoto.2014.10.030
Keywords: bone conduction implant, percutaneous bone anchored hearing system, conductive hearing loss, aural atresia, one-stage BCD surgery, audiology, pediatrics
Citation: Josefsson Dahlgren H, Iversen KN, Hultcrantz M and Engmér Berglin C (2025) Evaluation of a percutaneous bone conduction system using the Ponto BHX implant in a pediatric population with congenital conductive hearing loss—a 1 year prospective follow-up study. Front. Audiol. Otol. 3:1677161. doi: 10.3389/fauot.2025.1677161
Received: 31 July 2025; Accepted: 03 October 2025;
Published: 20 October 2025.
Edited by:
William (Bill) E. Hodgetts, University of Alberta, CanadaReviewed by:
Byanka Cagnacci Buzo, Santa Casa of Sao Paulo, BrazilPaul Zwittag, Kepler University Hospital GmbH, Austria
Copyright © 2025 Josefsson Dahlgren, Iversen, Hultcrantz and Engmér Berglin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hanna Josefsson Dahlgren, aGFubmEuam9zZWZzc29uQGtpLnNl