 Johanes Mandowa
Johanes Mandowa Mark Matsa
Mark Matsa Steven Jerie
Steven Jerie- Department of Geography, Environmental Sustainability and Resilience Building, Midlands State University, Gweru, Zimbabwe
Background: Promotion of OSH management systems (OSHMSs) has gained commendable traction worldwide with the developed world taking the lead, however non to suboptimal implementation of OSHMSs is still evident in the least developed and developing countries. The purpose of this study was to evaluate the uptake of OSHMSs in the manufacturing industry of the City of Mutare in Zimbabwe.
Methods: A descriptive cross-sectional study that exploited the pragmatism philosophical approach was utilized. Data collection was done through administration of 312, 30 and 11 questionnaires to worker, top manager and OSH practitioner respondents respectively complimented by interviews and secondary data from respective manufacturing factories. Data was analyzed, presented using pie charts, bar graphs and frequency tables to illustrate trends and then discussed qualitatively in continuous prose.
Results: Results revealed subdued implementation of OSHMSs in manufacturing industry of Mutare as evidenced by a low uptake rate of 26.7%. Results projected lack of leadership and management commitment and lack of human, material, and financial resources for systems sustenance as main reasons for non-implementation of OSHMSs.
Conclusion: Low uptake rate of OSHMSs revealed is a serious bottleneck to the endeavor to attain OSH sustainability for securing the future of work.
1 Introduction
The global Occupational Safety and Health (OSH) performance has been on a negative trajectory over the years (1). According to ILO, an estimated average of 2.78 million workers are dying every year as a result of occupational accidents or work-related diseases in addition to the 374 million non-fatal injuries and illnesses (2–6). This unpleasant global performance is a travesty on the sanctity of human lives and represents enormous ramifications to workers, their families, and the society at large. ILO is convinced that this bad global OSH performance is reflective of rampant failure by many workplaces world-wide to implement OSH management systems (OSHMSs) (1).
Research into OSHM systems uptake has been conducted extensively in many industrial sectors globally (7, 8). A study by Wang et al. (7), observed that OSHMSs uptake rate is generally observed to be higher in manufacturing organizations that support the international market than those that support the local market. A systematic literature review of implementation of occupational safety and health management systems for the period 1970–2020 conducted by Mandowa et al. (9), revealed low implementation levels of OSHMSs in small enterprises as comprehensive OSHMSs are generally considered too complicated to be applied by small enterprises. There is consensus amongst many authors that the extent of implementation of OSH management systems is largely influenced by other compelling factors that are congruent to the environmental context (9, 10).
A plethora of studies have fumigated the factors affecting uptake of OSHMSs globally (11–15). Insights from scholarly studies show that Leadership and Management commitment (16–19), workers awareness (20), worker involvement and participation (9, 21, 22) are key factors promoting uptake of OSHMSs whilst their non-existence has a negative impact on implementation of OSHMSs (23). Njogu et al. (14), and Zwetsloot et al. (24), noted the importance of management commitment and employee involvement in OSH management system implementation as revealed by several studies, however asserted lack of exploration of the causal factors for lack of management commitment and employee involvement in these studies.
Globally, the promotion of a systems approach to OSH management has gained commendable traction with progressive countries in the developed world taking the lead (9, 11, 25, 26). Adoption and implementation of OSH systems has had an inexplicably challenging gestation and a protracted delivery phase globally (27, 28). The birth of OSH management systems strategy therefore became a significant development in the OSH landscape as it represented a paradigm shift from prescriptive traditional OSH strategy that proved to be unsuccessful and inefficient in curtailing occupational injuries and diseases to a goal setting philosophy based on the premise that collectively employers and employees are best placed to identify and control workplace hazards and risks (29).
Despite the widespread promotion of OSH management system (9, 25, 26), Southern African Development Community (SADC) is still generally characterized by limited to non-implementation of OSH management systems (27). On average, over a period of more than a decade from 2008 to 2024, Zimbabwe has been losing 77 lives due to work related deaths every year (30), a statistic that is disproportionately high considering the size of the Zimbabwean economy. The statistic is even more alarming considering that it largely represents what is transpiring in the formal sector and therefore is just a tip of an iceberg considering rampant non-reporting and underreporting of accidents in the informal sector which constitutes approximately 80 percent of the working population in Zimbabwe (31). A study conducted by NSSA in 2020 that reviewed the trends of Occupational Safety and Health Performance in Zimbabwe over a ten-year period from 2008 to 2018 revealed an average Lost Time Injury Frequency Rate (LTIFR) for all the industrial sectors to be above the international standard of 1 over the ten-year period thereby rendering all industrial sectors in the country generally unsafe and unhealthy. The study further revealed that the economic costs of occupational injuries in the manufacturing sector stood at 0.39% of Zimbabwe's GDP thereby making the manufacturing sector the second highest sector coming after mining and quarrying sector whose costs of occupational injuries was highest at 0.43% of the national GDP. Mutetwa (32), identifies the manufacturing sector as one of the major sectors contributing immensely to the Zimbabwe bad OSH landscape. Mutare manufacturing industry is not exempted from a myriad of OSH challenges bedeviling many workplaces in Zimbabwe that are contributing to the bad OSH performance of the country. Dhliwayo (33) bemoaned a poor OSH performance in Mutare attributed to the highly hazardous trait of Mutare manufacturing industry that is dominantly timber based. It's a reality that the quest for Zimbabwe to attain sustainable development goals stands the risk of being set off by costs of occupational injuries and diseases as long as the country continues to entertain such a negative OSH performance trajectory.
Mutetwa (32) is convinced that the chief causal factor to the unpleasant OSH performance in the country is non-implementation of OSHMS at the generality of workplaces as evidenced by a paltry 10% of organisations that had implemented OSH systems up to certification level. A significant extent of OSH management problems in the country are a manifestation of the socio-economic challenges in the country. The de-industrialization and the general economic decline that our country has been experiencing since more than a decade of years ago has created dangerous workplaces characterised by antiquated plant and equipment, acute shortage of necessary skills and competences and dilapidated infrastructure across many industrial sectors.This scenario is worrisome to the Government of Zimbabwe and its social partners as it militates against the National Development Strategy's (NDS1) quest for the transformation of the country to become an Empowered and Prosperous Upper- Middle Income Society by 2030 and the need to attain the decent work and sustainable development agendas.
Pillar number 3 of the ILO's Global Strategy for OSH recognizes the need for accelerated action towards implementation of systems approach to OSH management as key in effectively addressing current and future OSH risks in the field of work (34). With the emergence of new and more volatile OSH risks such as COVID 19 confronting workplace in Zimbabwe, Mutare manufacturing industry included, it has increasingly become more imperative to ensure the attainment of OSH sustainability. Pandey (35) research identified a systems approach to OSH management as one of the five fundamental principles of successful OSH management. As observed by Mandowa et al. (9), literature shows that only a few studies on implementation of OSHMSs in the sub- sahara region of Africa are recorded. An attempt by scholars to explore implementation of OSHMSs in Zimbabwe is evident in literature (36–38), however there is currently no published research that has been conducted specifically to evaluate the uptake of OSH management systems in the Mutare manufacturing industry as a whole, yet it is an industry with a host of occupational risks that are progressively contributing to Zimbabwe's bad OSH national performance owing to the dominance of the highly risky timber processing factories (33, 39, 40). According to Jerie (40), timber processing factories are characterized by unguarded dangerous moving parts of machinery, physical hazards (such as excessive noise, dust and vibration) and ergonomic hazards (such as poor work postures, visual strain, and poor workstation design) that are responsible for the rampant occurrence of occupational accidents and diseases. Vitrano and Micheli (11) acknowledged that in the OSH fraternity, most successful accident prevention initiatives are hinged on implementation of OSHMSs which are designed to foster continual improvement in OSH management at enterprise level. The efficacy of OSHMSs as an OSH improvement strategy emphasizes the significance of OSHMSs as a natural area of research interest.
The few studies (36–39) recorded on implementation of OSHMSs in the sub- sahara region of Africa, particularly in Zimbabwe are bereft of examining the context based problems bedeviling implementation of OSHMSs so as to initiate problem driven solutions to buttress OSHMSs uptake. Limited research on implementation of OSHMSs in developing and least developed countries has largely been based on lessons learnt from developed countries. It can be extrapolated that the inadequacy of research based evidence on the contextual problems affecting implementation of OSHMSs could be a reason why OSHMSs implementation remains subdued in developing and least developed countries as most workplaces tend to shun implementation of OSHMSs as they consider them as an unnecessary cost to business. Mandowa et al. (9), study recommended propagation of further research that will unearth the problems associated with implementation of OSHMSs so as to contextualize OSHMSs implementation taking into consideration other differing environmental factors. Mandowa et al. (9), findings are cemented by Vitrano and Micheli (11), study that argued the need for further research in development of OSHMSs that consider all inherent dynamics of the environment in which they are implemented. Njogu's (14), study on factors that influence implementation of OSHMSs at Public Universities in Kenya suggested the need to consider basic problems in OSH management systems implementation in crafting effective strategies in the promotion of OSHMSs at workplaces. This research based evidence presents a research gap for researchers to explore further studies to establish the contextual problems impeding implementation of OSHMSs as a pathway to establishing problem driven solutions aimed at increasing uptake of OSH management system. Against such a background, this study therefore seeks to analyze the uptake rate of OSH management systems in the manufacturing industry of Mutare, to examine the reasons for non-implementation of OSHMSs in the manufacturing industry of Mutare and to assess opportunities that can be harnessed to increase uptake of OSHMSs in the manufacturing industry of Mutare.
2 Materials and methods
2.1 Study design
Relativism ontological assumption was found appropriate for this study considering that the reality about the challenges associated with uptake of OSH management systems in Mutare manufacturing industry is subjective and vary from person to person and from one organization to another. The qualitative (interpretivist) and quantitative (positivist) paradigms (41, 42) formed the epistemological basis of the methodology. Based on the ontological and epistemological assumptions, a descriptive cross-sectional study that exploited the pragmatism philosophical approach (mixed method design) was utilized (43–46). The methodology was considered ideal for this study as it is credited for its proficiency in extracting divergent multiple viewpoints, opinions, perspectives and standpoints (45, 47) utilizing several research instruments such as questionnaires, interviews, and available documents which is critical in enhancing the veracity of the research findings through data triangulation. The schematic representation of the methodology is depicted in Figure 1.
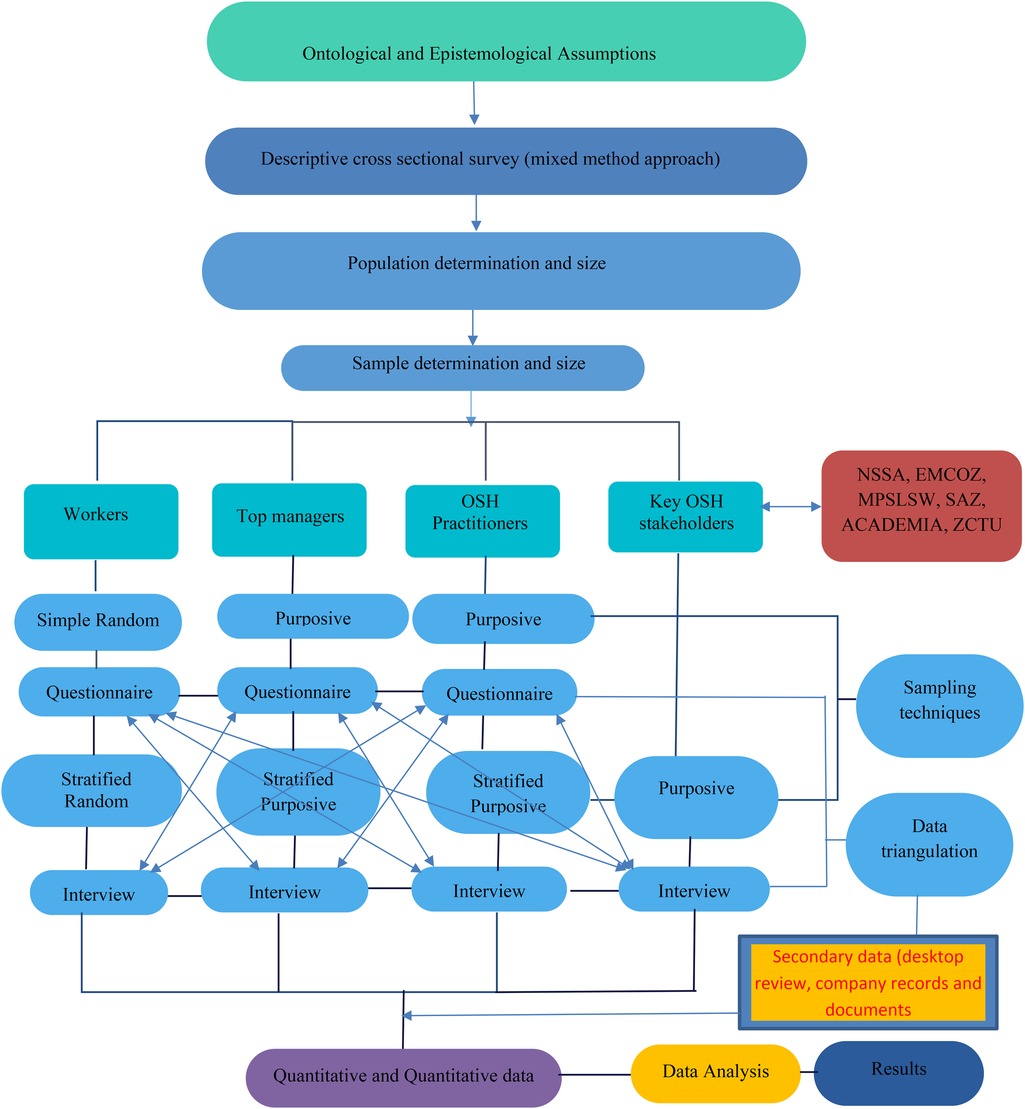
Figure 1. Schematic representation of the methodology.
2.2 Population size
The targeted population was all the 30 manufacturing factories of Mutare that are registered by NSSA and six key OSH stakeholders in the implementation of OSH management systems in Mutare manufacturing industry that included Ministry of Public Service, Labour and Social Welfare (MPSLSW), The Academia (Mutare Polytechnic College), Employers' Confederation of Zimbabwe (EMCOZ), Zimbabwe Congress of Trade Union (ZCTU), Standard Association of Zimbabwe (SAZ) and National Social Security Authority (NSSA). The 30 manufacturing factories of Mutare were made up of the following categories; Timber based manufacturing, food manufacturing, engineering and other manufacturing with the number of factories in each category being 14, 8, 5 and 3 respectively. The selection of the manufacturing factories of Mutare registered by NSSA was chiefly motivated by their known hazardous trait owing to the dominance of the highly hazardous timber processing factories (32, 40, 48). The justification for the selection of the six key OSH stakeholders is as depicted in Table 1.
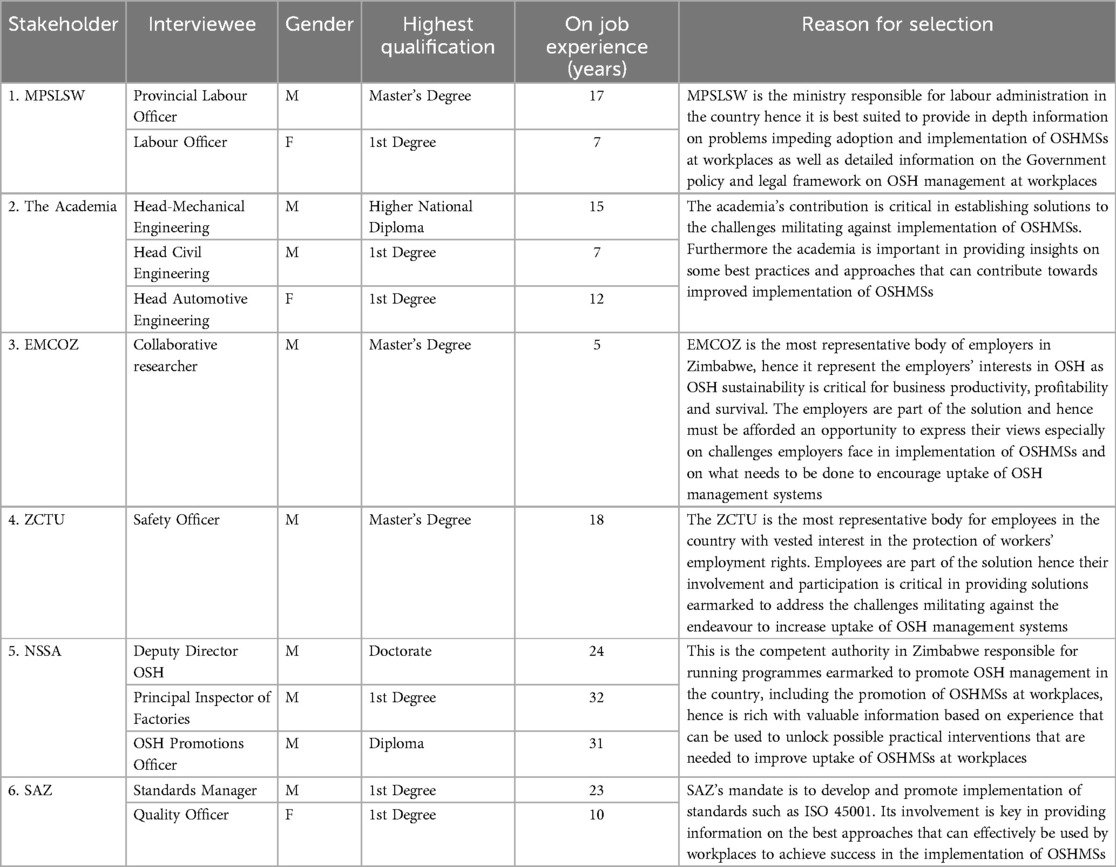
Table 1. Justification for selection of key OSH stakeholders.
2.3 Sampling methods
According to Turner (43) application of appropriate sampling methods enhances the credibility of the research findings. The NSSA factories database makes use of a 3-tier classification system where all registered factories are classified according to their size in terms of the number of employees. According to the NSSA 3 tier factories classification system, factories with a number of employees in the range of 1–50, 51–99 and 100 and above are classified as C (small), B (medium) and A (large) respectively. Taking from the NSSA factories classification systems, a total of 30 manufacturing factories of Mutare with a total employee compliment of 1,356 were stratified according to the nature of manufacturing business they were involved in, as well as according to their size in terms of the number of employees as depicted in Table 2. Fusch and Ness (49) noted the unmatched importance of conducting a census for small populations (200 or less). All the 30 (100%) manufacturing factories of Mutare were sampled so as to boost the representativeness of the sample basing on the assertion by Fusch and Ness (49).
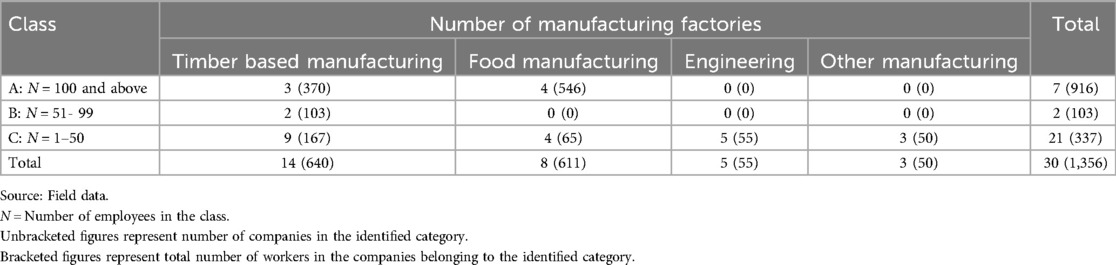
Table 2. Classification of manufacturing industry of Mutare.
2.4 Sample size determination
In line with the ILO conventions 155 (50), 187 (51) and ISO 45001 (52) requirements for employee involvement and participation in successful OSH management, workers were chosen for questionnaire administration. Employee involvement was key in strengthening their commitment to OSH management taking cognizance of the reality of the existence of a strong positive relationship between employee involvement in OSH and employee commitment (53, 54). Slovin's formula was used to determine the sample size capitalizing on its ability to yield a truly representative sample (55–58). In the determination of the sample size, a confidence level of 95% was used as it is generally acceptable in social sciences (59, 60).
A sample size of 309 was determined by applying the Slovin's formula as shown below;
where;
n: sample size
N: proportion of the population
e: margin of error = 0.05
The calculated sample size of a total of 309 employees represented 22.8% of the study population, which was above the 10% threshold that is generally considered sufficient to provide study findings that are a true representation of the population (61, 62). The manufacturing industry of Mutare were given a unique reference code (identifier) that consisted of two distinct letters and a number to ensure that the factory name remains anonymous. The nature of manufacturing business was coded with letters T, F, E and O representing Timber based, Food Manufacturing, Engineering and Other Manufacturing respectively. Letters A, B and C on the code represent the class of the manufacturing factory; A (large ∼100 and above employees), B (medium ∼51–99 employees) and C (small ∼1–50 employees) respectively according to the NSSA factories classification system. The sample size was distributed proportionately to all the 30 manufacturing factories in Mutare according to the formula (61).
where:
n1 = Proportion of sample size in a particular manufacturing factory
Xn = Number of workers in a particular manufacturing factory
N = Total target population in the manufacturing industry of Mutare.
The calculated number of respondents for each manufacturing factory is shown in Table 3.
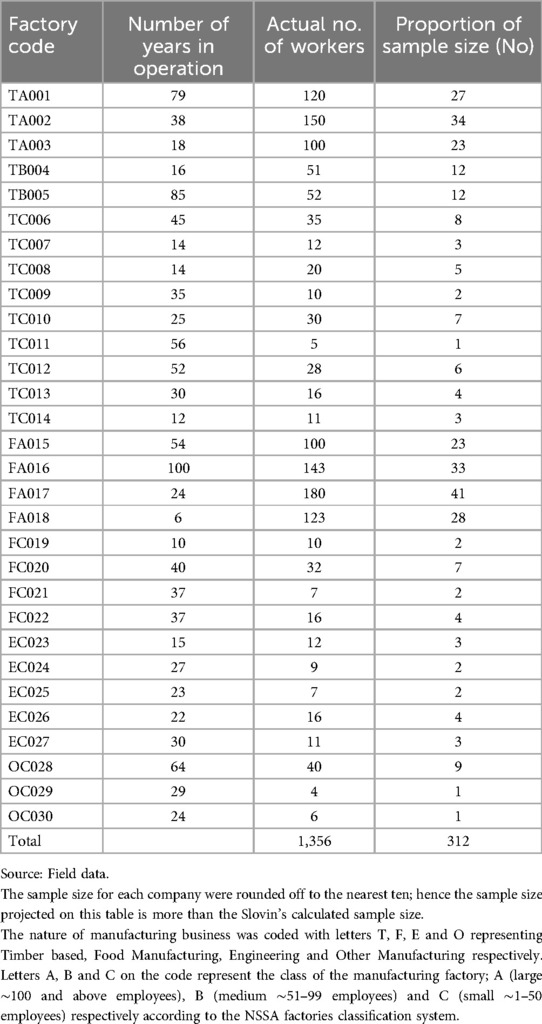
Table 3. Sample respondents selected from each company.
A simple random sampling technique was used to sample the 312 workers (The sample size for each company were rounded off to the nearest ten; hence the sample size projected is more than the Slovin's calculated sample size) for questionnaire administration proportionally distributed as shown in Table 3, exploiting on the technique's ability to ensure that the probability of each worker being selected as a questionnaire respondent (63) is equal for all workers in the manufacturing industry of Mutare.
Questionnaires were also extended to either both an appointed OSH practitioner and a Top manager or just a Top manager in the absence of an OSH practitioner in every manufacturing factory. Data triangulation that was critical in enhancing the authenticity of the research results (63, 64) was achieved through administration of follow up in depth interviews. Follow up interviews were administered to 10% of the worker questionnaire respondents drawn by stratified random sampling technique. Furthermore, purposive sampling technique was applied to purposefully select 2 key interview informants (OSH practitioner or Safety Representative and Top Manager of the factory) for in-depth data elucidation.
Purposive sampling technique was chosen to select the interviewees as it allowed the researchers the leeway to use personal judgment to select key interviewees' that would best answer the research objectives (58, 65–67). The choice of OSH Practitioner was informed by their technical capacity to implement effectively the various elements of an OSHMS owing to their skills and competence in OSH delivery. Studies have proven that without qualified and competent OSH practitioners implementation of OSHMSs becomes difficult (9, 10, 39). Their inclusion in the study was to ensure that they provide in depth information on the challenges impeding OSHMSs implementation and the reasons for non-implementation of OSHMSs and on sound scientific solutions of what needs to be done to increase uptake of OSHMSs. Top management representatives were selected as interviewees' necessitated by the fact that they are decision makers as far as unlocking of resources for effective implementation of OSHMSs is concerned, hence their input was valuable in establishing practical solutions for increased uptake of OSHMSs. Purposive sampling technique was also employed to select one informant each for further in-depth interviews from pivotal identified OSH stakeholders. These identified key OSH stakeholders were handy in the exploration of their perception about uptake of OSH management systems in manufacturing industry of Mutare and their opinions on how to increase uptake of OSH management systems in Mutare manufacturing industry.
2.5 Data collection methods
Both primary and secondary data sources were used in this study in line with Trochim et al. (68), assertion that use of multiple sources of data enhances the confidence about the reliability of the research findings.
2.5.1 Primary data sources
2.5.1.1 Questionnaires and interviews
An anonymous semi-structured questionnaire was self-administered to obtain data from a sample of 312 workers proportionally drawn from the 30 factories under the Mutare manufacturing industry as depicted in Table 4. The semi- structured questionnaire was segmented into four sections (A, B, C, D) aligned to the research objectives. Section A covered socio-economic demographic data of the respondents and sections B, C and D covered questions that answered objectives 1, 2 and 3 respectively. The questionnaire contained a total of 13 Likert scale questions.

Table 4. Distribution of worker questionnaire respondents.
To counter the challenge of a low response rate, the researchers deliberately designed questions with possible answers for respondents to choose from, thereby making it easier and faster for them to complete the questionnaire. Additional questionnaire data was obtained through purposive administration of 30 and 11 semi structured questionnaires to top manager and OSH practitioner respondents respectively making up the manufacturing industry of Mutare as shown in Table 5. Administration of semi structured questionnaire to the OSH practitioner and/or the top manager was necessitated by the need to collect comparable data that would answer the research objectives.
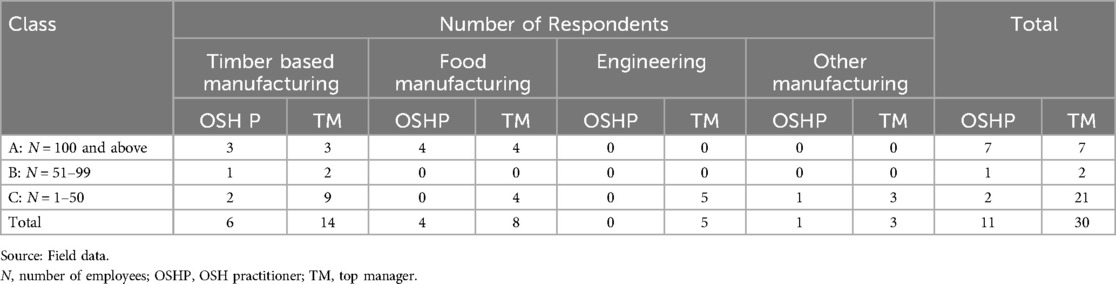
Table 5. Distribution of OSH practitioner and top manager questionnaire respondents.
The questionnaires were subjected to pre-testing to ensure their effectiveness in collecting data that answered the research questions. Pre-testing of the questionnaire was conducted on 30% of the workers randomly drawn by stratified sampling technique from all the three categories of manufacturing industry of Mutare basing on Neuman (65) assertion that 30% sample is advisable to ensure confidence of research results culminating in the final version of the questionnaire that incorporated all the views obtained from the pretesting exercise. Cronbach's Alpha (69) was computed to assess reliability and validity of the questionnaires. The reliability coefficient of 0.85 was found and considered acceptable taking cognizance of an assertion by Jilcha (70) that a reliability coefficient of 0.70 and above is generally regarded as “acceptable” in most research situations.
Semi structured interviews were extended to 10% of the worker questionnaire respondents drawn by stratified random sampling technique as shown in Table 6. Semi structured follow up interviews were also administered to collect in-depth information by stratified purpose sampling technique from 50% of questionnaire respondents from the OSH practitioner category (Table 7) basing on Rea & Parker (71) conviction that at least 50% response is a requisite for small populations of less than 200 subjects to guarantee the validity of the research results. Semi structured follow up interviews were administered to collect in-depth information by stratified purposive sampling technique from 10% of questionnaire respondents from the top manager category (Table 7) basing on Mburu et al. (61), approval of a 10% of the study population as sufficient sample size in a survey. The sample size for top manager interviewees was increased to 23.3% to cater for those eligible respondents who could be unwilling to participate in order to retain the representativeness of the sample.
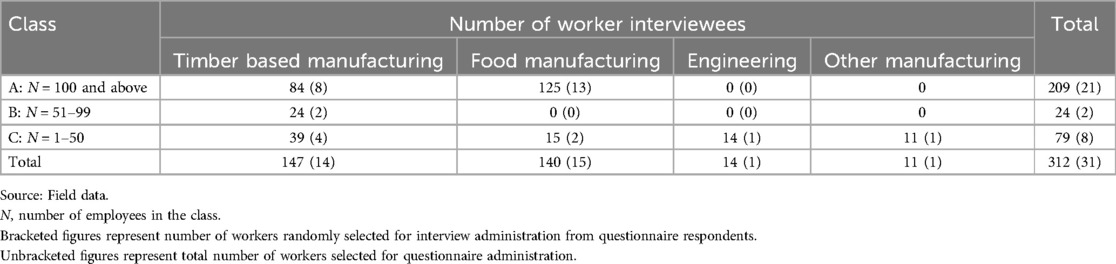
Table 6. Distribution of the worker interviewees.
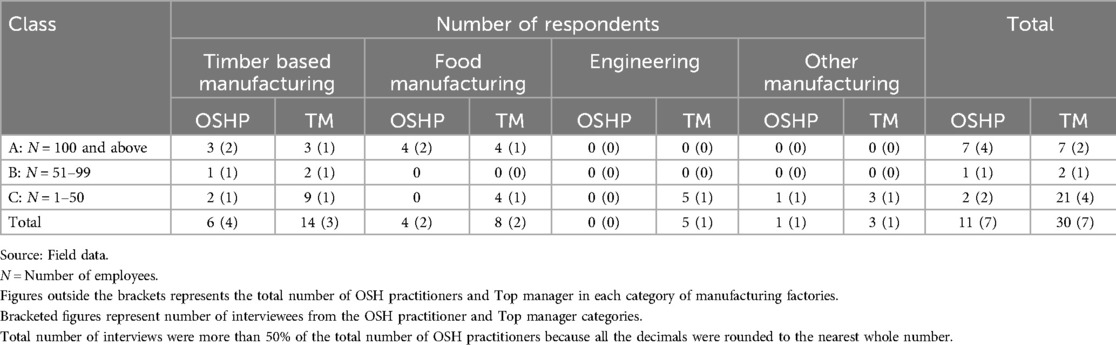
Table 7. Distribution of interview respondents from OSH practitioners and Top managers' categories.
Notes and audio recording were taken during the interviews to ensure the retention of important information during the interview. Semi structured face to face interviews were also extended to 6 key OSH stakeholders drawn by purposive nonprobability sampling technique. The choice of the semi structured face to face interviews was informed by the need to provide the same stimuli to the informants to generate data that could easily be aggregated and to ensure a good response rate that was estimated by Neuman (72) as being around 90%. An interview guide containing questions that answer the research objectives was pretested for its efficacy in data extraction on 30% of the total population of identified interviewees in the manufacturing industry of Mutare drawn by stratified purposive sampling considering Neuman (65) confirmation of a 30% sample ideal for populations less than 1,000.
2.5.1.2 Uptake of elements of an occupational safety and health management system
The underlying philosophy of an Occupational Safety and Health Management System is continual improvement based on the Deming Cycle, which consists of an iterative process of four steps known as “Plan, Do, Check and Act” (PDCA) (73, 74). In Zimbabwe, NSSA established an OSHMS Assessment Matrix which has become a de-facto instrument for gauging uptake of OSHMSs at workplaces in Zimbabwe based on its consistence with the provisions of the OHSAS 18001, ISO 45001 and ILO –OSHMS 2001 guidelines (32).
The NSSA OSHMSs Assessment Matrix was applied to Mutare manufacturing industry to measure the uptake of various elements of OSHMSs. The NSSA's OSHMS Assessment Matrix embraced OSH Management Systems elements namely: Occupational Safety and Health Policy, Visible Leadership and Commitment, OSH Legislation and other requirements, OSH objectives and targets, Hazard/Risk Identification, Competence, awareness, and training, Accident investigation programme, Emergency preparedness and response plan and procedure, Planned preventive maintenance program, Contractor safety and health management, Provision of Personal Protective Equipment, Safety and Health Committee, Accident reporting and recording, Occupational Health Services Provision, Employee wellness policy and programmes, Waste management, Planned safety audits, inspections and surveys and Management review meetings.
2.5.2 Secondary data sources
Secondary data was mainly collected from targeted companies' OSH records and documents, desktop review of OSH information from various OSH websites, and NSSA's OSH records and documents among other sources. Secondary data assisted in exploring knowledge gaps on uptake of OSH management systems at workplaces, conducting comparative evaluations and discussions on uptake of OSH management systems in manufacturing industry of Mutare.
2.6 Data analysis and presentation
The valid questionnaires were coded according to the nature of manufacturing business (T (Timber Based), F (Food manufacturing), E (Engineering based) and O (Other manufacturing) and the class in relation to NSSA factories classification system [A (large ∼100 and above employees), B (Medium ∼51–99 employees) and C (small ∼1–50 employees)] and numbered sequentially. For instance, code TA1 depicted questionnaire number 1 for a respondent in a Timber based manufacturing company that is in class A (100 and above employees). This numbering enabled the analysis of questionnaire data according to the nature of manufacturing business as well as to the factory size. A microsoft excel grid was created to collate data from the questionnaires which was subsequently grouped into defined data sets according to the research objectives and presented using pie charts, frequency tables and bar graphs to illustrate trends and then discussed qualitatively in continuous prose. Data from interviews was extracted from the written notes and audio recordings and compiled according to the research objectives. A comparative analysis was done to synthesize and group the data into defined data sets according to similarities and differences that would have been seen in the respondents' responses. The interview data was presented in a descriptive qualitative manner to augment other data sources. Secondary data was synthesized and described in a qualitative manner in line with the research objectives.
2.7 Ethical considerations
A consent form was administered to both company representatives and respondents of all participating manufacturing factories of Mutare to ensure voluntary participation and unhindered access to both primary and secondary data. Research participants and participating organizations were anonymized to allay fears of irreparable reputational damage to organizations and victimization of research participants which could impact negatively on their willingness to participate in the study.
3 Results
3.1 Response rate for questionnaires
As shown in Figure 2, workers, OSH practitioners and top managers' questionnaire response rates were 81.4%, 100% and 87.1% respectively. All the questionnaire response rates for workers, OSH practitioners and Top Managers were above 70% which is generally considered by many authors as excellent response rate in a survey to ensure reliability of the study results (14, 75, 76).
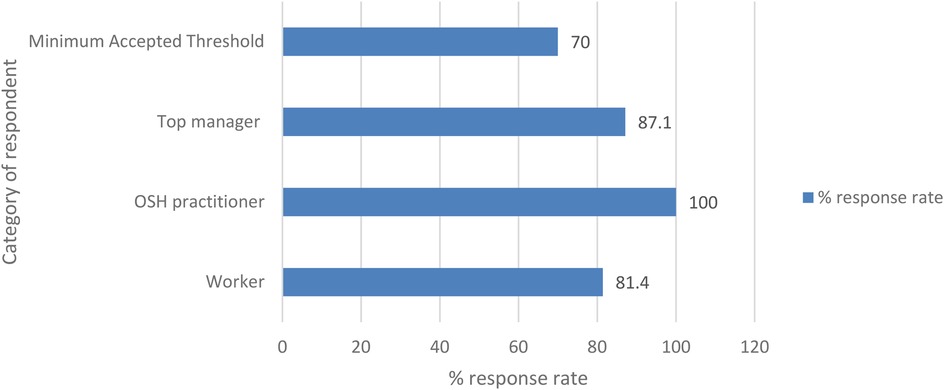
Figure 2. Questionnaire response rates.
3.2 Socio-economic demographic characteristics of the respondents
In terms of gender, the results show the dominance of male respondents (71.1%) over female respondents (28.9%) in the worker category in all the categories of manufacturing factories of Mutare. In the OSH practitioner and Top manager categories male respondents also dominated with 80% and 59.3% respectively. 47.2% of the questionnaire respondents in the worker category had more than 6 years of continuous experience working for their respective companies, with the majority of the workers (52.8%) having worked for less than 5 years.
The highest number of worker respondents (59.4%) were tertiary level graduates whilst 10.6%, 27.8% and 2.2% of the workforce were high, secondary, and primary level graduates respectively. The majority of the worker respondents in all the categories of the manufacturing industry of Mutare [Timber based (37.4%), Food manufacturing (43.4%), Engineering (42.9%) and Other manufacturing (66.7%)] described their remuneration as poor.
Most worker respondents (66.7%) were trained on OSH after joining their respective companies and 33.3% did not receive any training on OSH. Most of the Top managers (90%) interviewed were conscious about the importance of OSH training in curbing occupational injuries and diseases; however lamented high operating cost, low profitability, extreme financial pressure and lack of human resources as challenges impeding execution of OSH trainings. A categorical analysis reveals that training of workers as they are recruited is more pronounced in Timber based (76.9%) and Food manufacturing (61.8%) companies than in Engineering (42.9%) and Other manufacturing (0%) factories.
54.5% of the OSH practitioners were found in the timber-based manufacturing factories with the remaining 36.4% being in the food manufacturing factories and 9.1% in factories classified as Other manufacturing. The results indicated the non-availability of OSH practitioners in Engineering firms. In terms of the markets served by the manufacturing industry of Mutare, most of the factories (66.7%) in the different factory categories purely manufacture product for the local market consumption whilst 33.3% serve both local and international markets. All the key OSH stakeholders (100%) that were interviewed had on job experience of more than 5 years. Furthermore, most of the OSH stakeholders were holders of at least a first degree.
3.3 Analysis of the implementation rate of occupational safety and health management systems in manufacturing industry of Mutare
Approximately twenty seven percent (26.7%) of all the factories in different manufacturing categories making up the manufacturing industry of Mutare implemented an OSH management system whilst 73.3% of the factories did not implement an OSH management system as depicted in Figure 3.
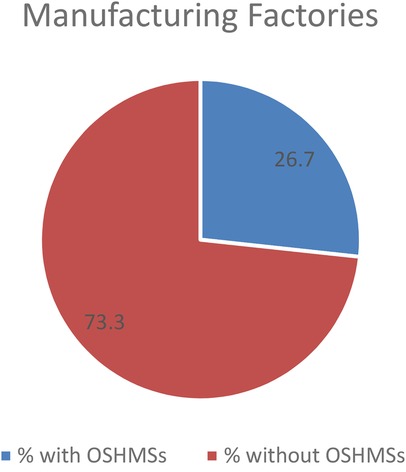
Figure 3. Percentages of manufacturing factories with OSHMSs and manufacturing factories without OSHMSs.
In most factories (87.5%) that implemented an OSH management system, their systems were aligned to an internationally acclaimed ISO 45001 OSH management system with a paltry 12.5% having an industry specific type of an OSH management system. Approximately forty-one (40.5%) of the workers that responded to questionnaires revealed that there were aware of the existence of an OSH management system at their organization whilst 59.5% expressed ignorance on the availability of OSH management system at their organization. Administration of the NSSA OSH Management systems assessment protocol showed that only 26.7% factories had implemented more than 50% of all the envisaged OSH management system elements. One factory (3.3%) out of all manufacturing factories of Mutare was certified to ISO 45001. Table 8 is indicative of OSH management systems implementation landscape of the manufacturing industry of Mutare as assessed by the NSSA OSHMS assessment protocol.
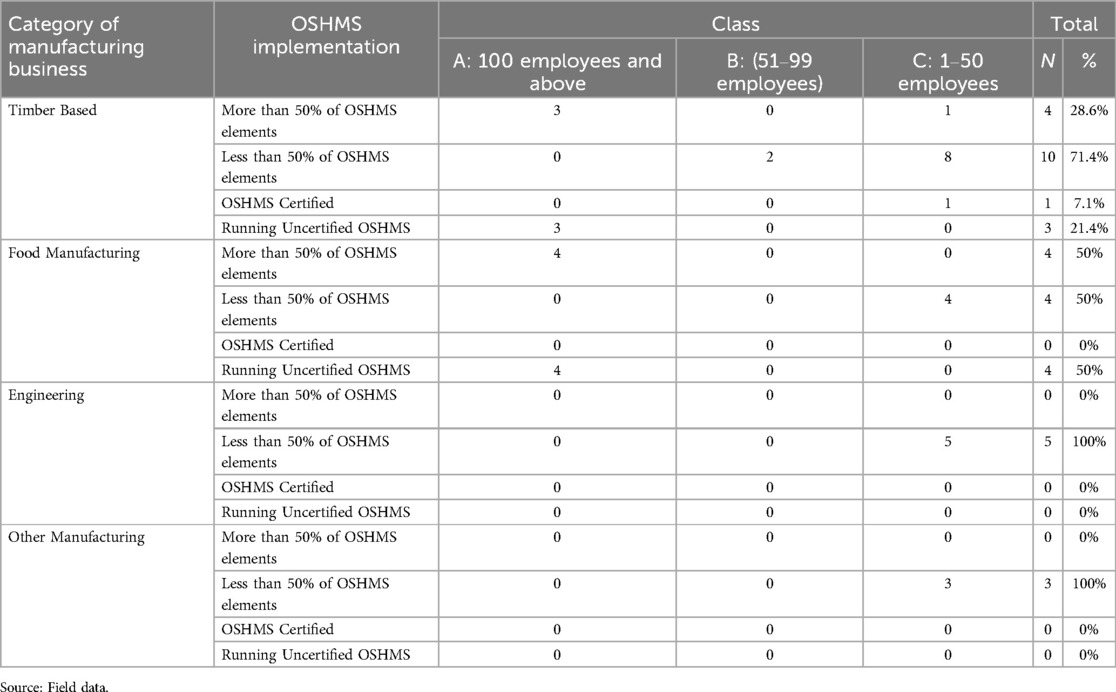
Table 8. Analysis of OSHMS implementation status in different categories of manufacturing business.
An evaluation of each manufacturing category as shown in Table 8 reveals that 28.6% of Timber based manufacturing factories had implemented more than 50% of the required OSHMS elements whilst 71.4% had less than 50% of the elements implemented. Seventy-five percent (75%) of the factories that implemented more than 50% of the required elements were from bigger firms with more than 100 employees and 25% were from firms with less than 50 employees. Twenty percent (20%) of the factories with less than 50% of the OSHMS elements were from factories that had employees in the range 51–99% and 80% were from factories with less than 50 employees. About seven percent (7.1%) of the timber-based factories had a certified OSH management system. Approximately twenty one percent (21.4%) of the timber-based factories had running uncertified OSH management systems. As reflected in Table 8, 50% of the food manufacturing factories had implemented more than 50% of the elements of an OSH management systems as well as 50% of the factories had implemented less than 50% of the elements required. Results show that there was no food manufacturing company that was certified to an OSH management system. Interestingly, in both the engineering and other manufacturing categories, OSH management systems were non-existent. It is interesting to note that most of the factories (66.7%) in the different factory categories making up the Mutare manufacturing industry that did not implement OSH management systems purely manufactured products for the local market consumption whilst 33.3% that served both local and international markets had some resemblance of functional OSH management systems. Most of the Top managers interviewed showed great sense of reluctance to implement OSHMSs citing lack of motivation as the systems are not a requirement for them to do business and furthermore the need to maximum profits by cutting down on operational costs associated with having a functional OSHMSs.
The subdued uptake of a systems approach to OSH management systems is a travesty to NSSA's OSH management system promotional strategy as well as the Standard Association of Zimbabwe's quest to promote the adoption of standards at workplaces. The academia on being interviewed bemoaned lack of a coordinated approach amongst OSH stakeholders in the quest to improve uptake of OSH management systems. Despite the unpleasant uptake of OSH management systems, 55.5% of top managers were convinced NSSA's OSHMS promotional programmes were satisfactory with only 37% and 7.4% describing NSSA's programmes as good and poor respectively. Most of the OSH practitioners (70%) were convinced that NSSA's OSHMS promotional programmes were good. According to ZCTU representative interviewee, the low uptake of OSH management systems was indicative of lack of a robust national systems to promote OSH management systems implementation at workplaces in Zimbabwe. Most OSH practitioners (90%) and top managers (85%) interviewed were persuaded that the approach currently being used by NSSA to promote OSHMSs was not good enough to stimulate increased uptake of OSHMSs as it was majoring on establishing the existence or non-existence of various defined elements of an OSHMS as a basis for awarding organizations for good OSH performance during the Safety, Health at Work conference held annually.
3.3.1 Uptake of various elements of OSH management systems in the manufacturing industry of Mutare
Table 9 is an analysis of the uptake of various elements of an OSH management system by Mutare manufacturing industry. Results in Table 9 reveal the top three OSHMS elements being implemented in the manufacturing industry of Mutare in order of their prominence as provision of personal protective equipment (90%), accident reporting and recording (83.3%) and planned preventive and maintenance program (53.3%). These results projecting provision of PPE as the most implemented element was consistent with the view of the majority of the workers interviewees' who expressed a deep understanding of PPE provision as a control in OSH management. OSH practitioners interviewed identified the insatiable appetite of employers of wanting to address OSH problems with PPE provision as a factor that had commonised PPE in many workplaces as an effective control to OSH hazards and risks ahead of other more effective controls. The element of accident reporting and recording was significantly evident (83.3%) in many workplaces. The majority of workers interviewed cemented the existence of the accident reporting and recording element by expressing their awareness of the availability of accident reporting and recording procedures. The least three implemented elements in the manufacturing industry of Mutare were planned safety audits (13.3%), occupational health services provision (10%) and employee wellness policy and programs (10%). NSSA representative interviewed expressed that lack of qualified and competence OSH practitioners in many manufacturing factories of Mutare was the causal factor contributing to subdued implementation of planned safety audits and occupational health services programmes. Workers interviewed were convinced that employers were reluctant to implement planned safety audits due to absence of a good safety culture that is hinged on pro-activeness rather than reactiveness.
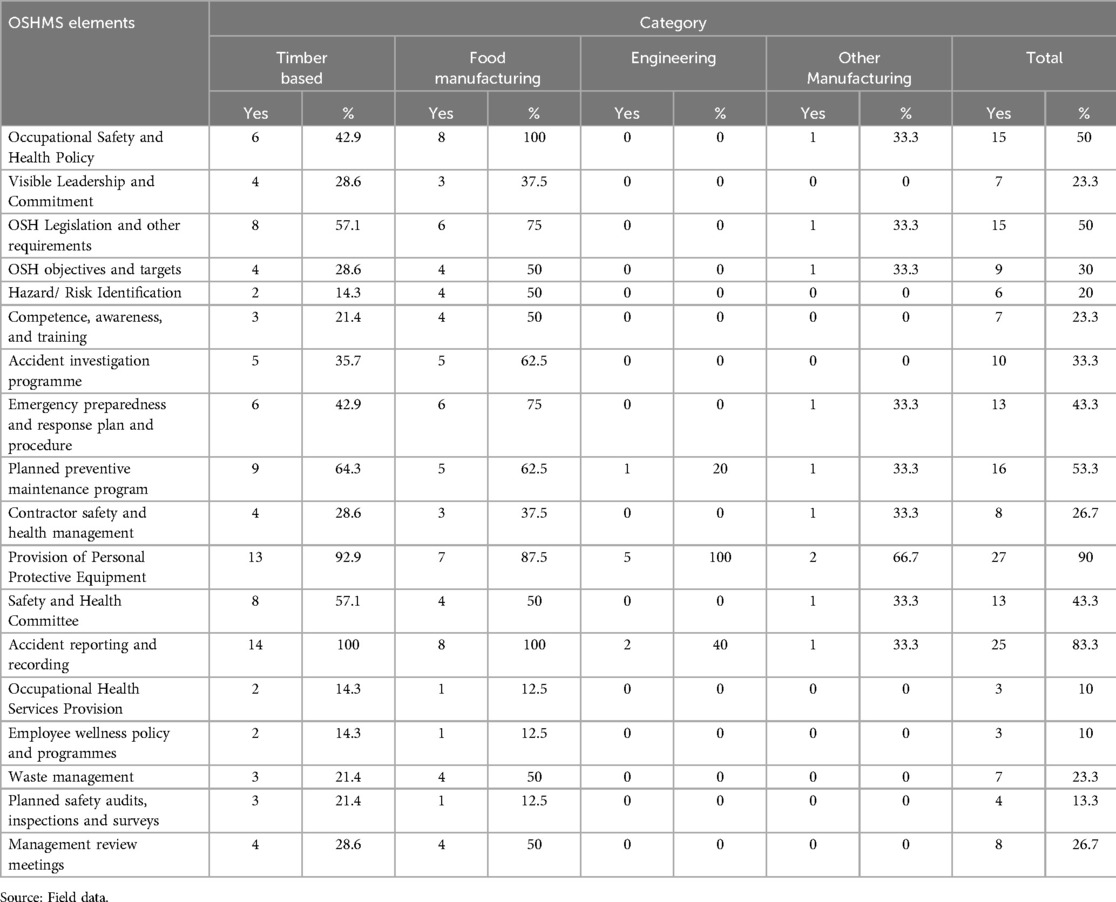
Table 9. Analysis of uptake of various elements of OSH management systems in the manufacturing industry of Mutare.
3.4 Reasons for non-implementation of occupational safety and health management systems by manufacturing industry of Mutare
From a worker's perspective as depicted in Figure 4, the results show that the generality of the workers in the manufacturing industry of Mutare believed that the major reasons for non-implementation of OSH management systems were unavailability of punitive penalties given to organizations for causing accidents (66.1%), management attitude where production is viewed as more important than safety (64.1%), lack of leadership and management commitment (61.5%), no immediate benefits for OSH implementation (60%) and lack of training on the importance of OSHMSs (60%). Workers interviewed were unanimous that the old OSH legal framework currently being administered in the country was a major setback to implementation of OSHMSs as it does not make the OSHMSs compulsory and more so the penalties for non-compliance to OSH standard were not deterrent enough to induce positive change in OSH management. ZCTU interviewees' concurred with workers on the need to reform the old OSH legal framework, however they asserted that it takes more than just a good legislation for compliance to happen but also a cocktail of other influencing factors such as the capacity of the regulator to effectively enforce the OSH laws. NSSA interviewee weighed in to the general view of employees by admitting that the current OSH laws in the country were redundant and there was need to expedite their reformation to ensure that they are responsive, relevant and effective in addressing the current and future of OSH challenges arising out of ever-changing dynamics of the world of work. The general view of workers on the reasons for non-implementation of OSH management systems is generally mirrored in all the four categories making up the manufacturing industry of Mutare. Top managers' view was a divergent from the workers perspective as they projected the major reasons for non-implementation of OSH management systems as lack of adequate human, material and financial resources (63%), high initial investment required to implement an OSHMS and related costs for its sustenance (55.6%) and lack of expertise to spearhead OSHMS implementation (55.6%). It is however, important to note that the same reasons that were given by workers were also significantly highlighted by top managers.
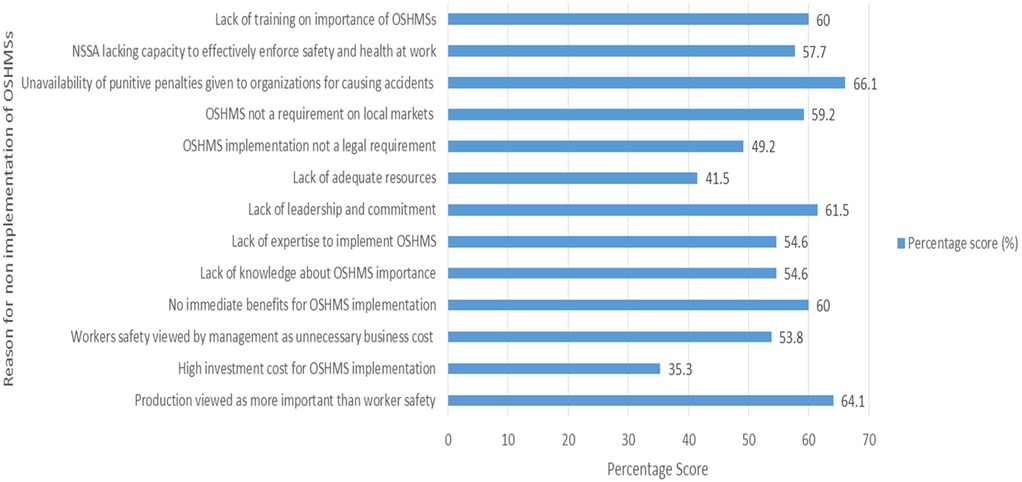
Figure 4. Reasons for non-implementation of OSHMSs in the manufacturing industry of mutare. Source: Field data.
EMCOZ interviewee was supportive of the top managers' view that lack of adequate resources exacerbated by a declining socio-economic environment was militating against accelerated adoption of OSH management systems as many employers were faced with the need to balance competing needs for business survival. However, the employee representative body (ZCTU) dismissed the assertion by EMCOZ that companies lack adequate resources as baseless basing on research-based evidence that generally employers tend to consider OSH management as an unnecessary cost to business (39). In line with the workers' and top managers' general views, OSH practitioners were emphatic on lack of leadership and commitment (66.7%), lack of training on the importance of OSH management system (66.7%), high initial investment required to implement an OSH management system (66.6%) and unavailability of punitive penalties given to organizations for causing accidents as major reasons for non-implementation of OSH management system in the manufacturing industry of Mutare. NSSA confirmed lack of leadership and commitment as the chief driver of all the challenges that militate against effective adoption and implementation of OSH management system basing on noticeable evidence of non-implementation of OSH management systems even in organizations that had sound financial resources.
3.5 Opportunities to improve uptake of OSHMSs by the manufacturing industry of Mutare
Table 10 is a representation of respondents' opinions on opportunities that should be harnessed to improve uptake of OSH management systems in the manufacturing industry of Mutare.
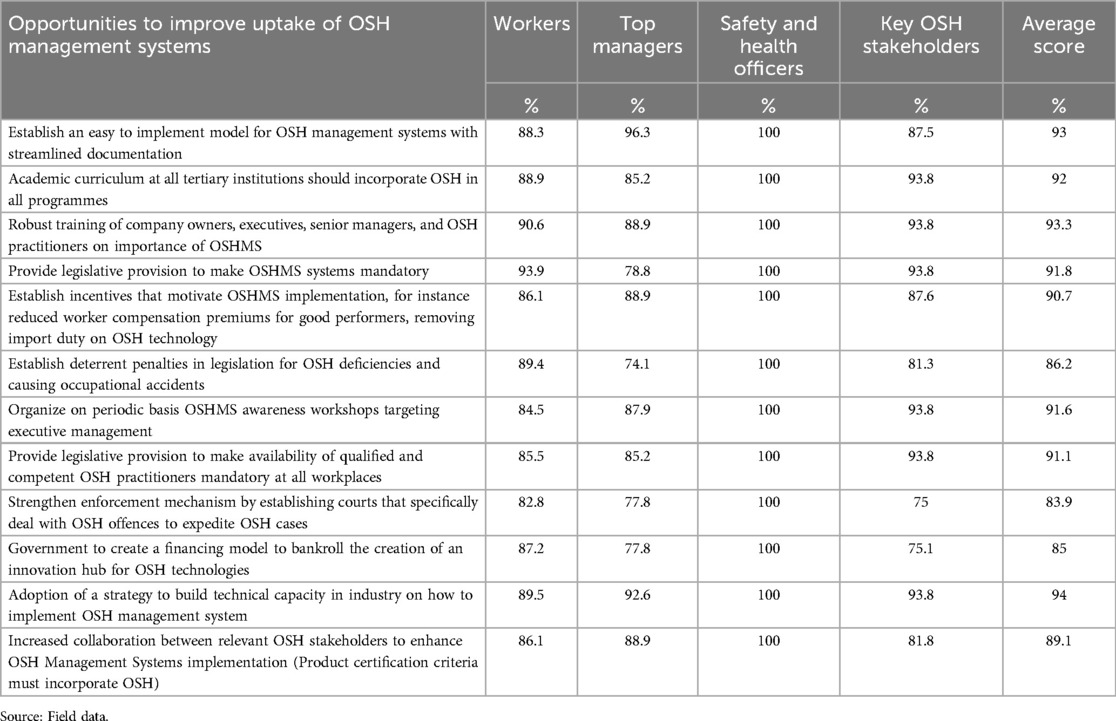
Table 10. Opportunities to improve uptake of OSHMSs in manufacturing industry of Mutare.
Results from various respondents demonstrate the need for a cocktail of interventions to be harnessed to improve the uptake of OSH management systems in the manufacturing industry of Mutare. The top five interventions that emerged were the need for a national strategy to build technical capacity in industry on how to implement OSH management systems (94%), establishment of an easy to implement model for OSH management systems with streamlined documentation (93%), incorporation of OSH in all academic curriculums offered at all tertiary institutions (92%), provision of robust training of company owners, executives, senior managers, and OSH practitioners on importance of OSHMSs (93.3%) and establishment of legislative provision to make OSH management systems mandatory (91.8%). The need to provide legislative provision to make availability of qualified and competent OSH practitioners' mandatory at all workplaces (91.1%) and establishment of incentives that motivate OSHMSs implementation, for instance, reduced workers compensation premiums for good performers and removing import duty on OSH technology (90.7%) also emerged prominently as possible interventions to improve uptake of OSHMSs.
4 Discussion
4.1 Response rate for questionnaire
All the questionnaire response rates for workers (81.4%), OSH practitioners (100%) and Top Managers (87.1%) were above 70% which is generally considered by many authors as excellent response rate in a survey to ensure reliability and validity of the study results (14, 75, 76).
4.2 Socio-economic demographic characteristics of the respondents
Male respondents dominated their female counterparts in all the categories of manufacturing factories of Mutare. The dominance of male respondents could be due to the nature of manufacturing industry which is generally associated with highly arduous and hazardous tasks that makes it highly unattractive to female employees. Conversely, the dominance of male respondents could be indicative of unavailability of gender policies in the manufacturing factories of Mutare that advance the need for gender equity in recruitment of workers in line with ILO's convention 111- Discrimination (Employment and Occupation) Convention, 1958 that promote gender equality in the world of work (77).
The highest number of worker respondents (59.4%) were tertiary level graduates which implies that the generality of worker respondents were knowledgeable enough to comprehend the demands of the questionnaire and interview thereby contributing to the enhancement of the reliability of the research data.
The majority of the worker respondents in all the categories of the manufacturing industry of Mutare [Timber based (37.4%), Food manufacturing (43.4%), Engineering (42.9%) and Other manufacturing (66.7%)] described their remuneration as poor. The poor remuneration that characterizes the manufacturing industry of Mutare is worrisome as it is a psychosocial risk factor that has the propensity to impede the successful implementation of OSHMSs by increasing the vulnerability of employees to occupational safety and health risks. It is a progressive development to realize from the results that most worker respondents (66.7%) in the manufacturing industry of Mutare were trained on OSH after joining their respective companies. This realization is commendable as it resonates with Golden rule number 6 “Improve qualification- develop competences” of the Vision Zero Concept that recognizes training of employees in OSH management as a critical step in ensuring the development of skills and competences necessary for effective implementation of OSH programs (78). From the results, a conclusion can be drawn from the results that availability of an OSH practitioner in an organization has some influence on establishment of OSH training programmes as most of the employees that received OSH training after joining their respective organizations were working in Timber based and Food manufacturing organizations that had an appointed OSH practitioner. This is so because OSH practitioners are technically knowledgeable to appreciate OSH training as a fundamental in the creation of safe and healthy workplaces.
Most of the top managers (70.4%) confessed having received some safety and health training since joining the organization. This confession by top managers provides a firm ground for a presumption to be made that most top managers were well versed with the importance of OSH management at workplaces. This presumption is cemented further by NSSA's OSH management systems promotional strategy that targets top managers and OSH practitioners of enterprises as focal people for OSHMSs promotion thereby becoming a vehicle for enlightenment of top managers on the importance of OSH management systems.
The revelation that the generality (90%) of the manufacturing factories of Mutare were experiencing high operating cost, low profitability and extreme financial pressure owing to difficult economic environment casts doubt on the capacity of the majority of the factories to effectively implement OSH management systems in a sustainable manner. The non-availability of OSH practitioners in Engineering firms as portrayed by the results is indicative of workplaces in this category that are devoid of OSH technical knowhow to implement OSH management systems. This gap in technical expertise in OSHMSs implementation can be a contributory factor to subdued uptake of OSHMSs. Vitrano et al. (10), affirmed the difficulties in OSHMSs implementation when there is lack of technical knowledge.
The fact that most of the OSH practitioners (75%) had attained a first degree in either OSH or OSH related field is a testimony of the commendable strides that the Zimbabwe's education sector is making in ensuring the wide-spread establishment of OSH academic programmes in several tertiary institution in the country. This is supported by ILO convention 155 article 14 that seeks to promote mainstreaming of OSH at all levels of education and training, including higher technical, medical and professional education, in a manner meeting the training needs of all workers.
Most of the companies (66.7%) largely manufacture products for the local market consumption whilst 33.3% serve both local and international markets. Unlike international markets that are now increasingly recognizing the sanctity of human life by progressively demanding their suppliers to demonstrate their moral obligation for the protection of their employees' safety and health as a condition for doing business (9, 79), local markets in Zimbabwe do not demand OSH management systems as a condition of doing business, hence this situation has the capacity to negatively impact the adoption and implementation of OSH management systems by the generality of the manufacturing industry of Mutare.
All the key OSH stakeholders (100%) that were interviewed had on job experience of more than 5 years. It can be presumed from the analysis of working experience of the key OSH stakeholders that all the respondents from the key OSH stakeholder's category have had an adequate exposure to appreciate the importance of OSH management systems. Such an experience was critical in unravelling problem driven solutions that could be harnessed to improve the uptake of OSH management systems in the manufacturing industry of Mutare.
4.3 Analysis of the implementation rate of occupational safety and health management systems in manufacturing industry of Mutare
The low uptake rate of OSHMSs in manufacturing industry of Mutare vindicates the long-held position by NSSA that the bad OSH performance of the country was largely being influenced by non-implementation of OSH management systems in many workplaces across the country (31, 32). ILO (1) attributed limited to no uptake of a systems approach to OSH Management at most workplaces as a catalyst to the unpleasant global OSH performance. It is important to highlight that Zimbabwe has not demonstrated its commitment to ensuring the implementation of OSH systems by its failure to ratify the ILO Convention 187 (51) on the promotional framework for OSH which clearly attests to the need for organizations to embrace OSH management systems as a way of establishing a national preventative safety and health culture. Indeed, as long as this negative OSHMSs implementation trajectory remains untamed, achievement of OSH sustainability to secure the future of work (1) will remain a pipedream and consequently a charade on Zimbabwe's quest to attain the 2030 Sustainable Development Targets, its NDS 1 deliverables and the vision for an upper middle-income economy by 2030. As observed by Stroh (80), this scenario is duplicated in many workplaces in least and developing countries such as in SADC.
The low uptake of OSH management system is a pointer to the inadequacy and ineffectiveness of the current strategies being implemented by NSSA in promoting OSH management systems. Apart from utilizing the ZOSHC assessment protocol chiefly as the barometer of measuring national OSH performance and as a basis for awarding organizations for good OSH performance during the Safety, Health at Work conference held annually, NSSA should revolutionize its OSHMSs promotional strategy to be more oriented towards offering long term technical assistance to organizations on an ongoing basis guided by well-defined objectives and targets taking cognizance of the fact that implementation of OSH management system is a continuous and progressive process that takes substantial amount of time, resources and effort. Additionally, there is a need for NSSA to buttress the current persuasive approach of promoting OSHMSs with legislative provision to compel adoption of safety systems.
Against a plethora of challenges confronting the least developed and developing countries that range from OHS human resource capital deficits, lack of comprehensive national and institutional OSH management framework and the proliferation of the difficult to regulate SMEs and informal economy (27, 39, 81), a conclusion can be made that concerted effort at national and international level is demanded in terms of coming up with tailor made, pragmatic and systematic interventions to scale up adoption and implementation of OSH management systems in least and developing countries taking cognizance of their diverse environmental contexts.
The results show the dominance of the internationally acclaimed ISO 45001 OSH management system in most companies (87.5%) that implemented an OSH management system. The dominance of the ISO 45001 standard (52) is reflective of the new order in the OSH management space where most workplaces are increasingly transiting to the ISO 45001 OSHMS standard of 2018 after the phasing out of the OHSAS 18001 standard which had over several years turned out to be the de-facto international standard in many organizations in Europe, Asia, and Africa (82).
One factory out of all manufacturing factories of Mutare was certified to ISO 45001 (52) despite there being other companies that had running uncertified OSH management systems. This seemingly shocking result of only few manufacturing factories that are certified to an OSH management system is consistent with Zwetsloot (83) observation that several companies globally choose to implement a “certifiable management system” but refrain from certification as they enjoy the benefits of a good and auditable OSH management system whilst avoiding the danger of the certification process becoming a “means to an end”. The certification regimes for OSH management systems have been criticized over time, for example, for increasing the cost to businesses and for becoming an “aim in themselves” (83, 84), for failures in the broader certification regime (85, 86) and in the associated market mechanisms (86) and for problems with the quality of the essential auditing process (87, 88).
Seventy-five percent (75%) of the companies that implemented more than 50% of the required elements were from bigger factories with more than 100 employees and 25% were from factories with less than 50 employees. This differentiation is supported in literature by many sources that it is largely due to the high capital that is demanded in setting up OSH management system (89–91). Frick (90) is of the view that certified safety management systems are only possible for a small number of large worksites, which can implement and benefit from a standard for OSH Management System. Lahm (92) and McKinney (91) opined that OSH Management systems are often perceived as irrelevant in small to medium enterprises (SMEs) as they do not have a huge workforce to guarantee translation of OSH Management System implementation into direct monetary gain for the company and consequently seems unimportant for companies' survival. Tejamaya et al. (93), asserted lack of OSH expertise in small to medium scale enterprises to quantify OSH performance in terms of monetary gain or loss as a compounding factor contributing to the observed unwillingness of SMEs to implement OSHMSs. This finding of disparities in implementation of OSHMSs between large and small to medium enterprises is a confirmation of Mandowa's (39) study that asserted the existence of an association between factory size and implementation of OSHMSs in timber processing factories. As observed by Mandowa (39), large factories often have a large financial resource base that translate to increased capacity to implement OSHMSs. On the contrary, Micheli et al. (17), asserted lack of financial muscle on the part of small to medium businesses as a major contributory factor to the less commitment exhibited by these organizations in establishing OSHMSs. Another school of thought is that generally, small to medium organizational structures tend to normally have simple structures that can only be sustained by few human resources hence every additional head count, for instance, employing a safety practitioner is regarded as generally costly to the organization (9, 39, 94) such that OSH is relegated to being managed by appointed workers without the requisite OSH management competence. Strong arguments have been put forward by researchers that due to the peculiarity of the structural set up in small to medium organizations, its ideal that they be subjected to different simplified, low cost and affordable OSH management systems than those used by large factories in order to ensure that they comply with the safety and health requirements necessary not to at least compromise workers' safety (9, 95, 96).
It is important to highlight that the new thinking world over in the domain of OSH management systems based on empirical evidence seems to suggest lack of leadership and commitment as the underlying factor that trigger the manifestation of other factors thereby becoming a strong determinant of whether an organization is going to implement an OSH management system or not (78). Gilkey et al. (97), noted that there is a mutual relationship between management commitment and availability of resources to spearhead safety systems implementation. This nexus between leadership and commitment and availability of financial resources is confirmed by ISSA's (78) observation that companies that have sound financial resources as evidenced by huge profits they declared failed to adopt safety management systems due to questionable management commitment. A narrative can thus be deduced that even in those manufacturing factories where financial resources are not a major challenge, low uptake of safety systems may continue to persist as long as leadership and management commitment to release the resources is not available. Such a negative trajectory will ultimately impact negatively on productivity and profitability taking into consideration research backed evidence by ISSA that there is $2 dollars return on investment for every dollar invested in safety (78). Based on this revelation, it follows that leadership and commitment should be central in defining OSH management systems both at national and enterprise level. According to Sankar and Anandh (98) there is empirical evidence that demonstrates the existence of a strong association between leadership and safety and health performance. In congruency to Sankar and Anandh (98), assertion, Oswald and Lingard (99) noted that the correlation between safety obligations perceived by workers and their safety performance exhibits greater strength when workers' perception of safety leadership is high, as compared to when it is low.
From the results, it is also interesting to note that the uptake rate is generally observed to be higher in manufacturing factories that are internationally acclaimed and supporting the international market than those that support the local market. Frick (90) and Frick, & Zwetsloot (79) noted that international organizations tend to have an insatiable appetite for OSH management system as part of their corporate social responsibility and the duty of care to prove for their employees' safety as a condition for product's acceptance on the market. These results therefore make it imperative for policy makers in Zimbabwe and beyond to consider mainstreaming OSH into trade policies in order to ensure a competitive market advantage for products that come from workplace where the sanctity of human life is upheld in line with the 1948 UN universal declaration for human rights (100).
4.3.1 Uptake of various elements of OSH management systems in the manufacturing industry of Mutare
The results that revealed the prominent implementation of provision of personal protective equipment may imply that PPE provision is being regarded by most manufacturing factories of Mutare as the ultimate control for exposure to occupational safety and health hazards. This is in tandem with Khoshakhlgh et al. (101), assertion that many workplaces in developing countries tend to view utilization of PPE as a cost reduction strategy as PPE provision is generally considered a cheaper OSH intervention as compare to other intervention such as engineering that require huge capital investment. As observed by NIOSH (102), this general view however violates the principle of the hierarchy of risk control that entail; hazard elimination, substitution, engineering control, administrative control and PPE provision as the last line of defense owing to a plethora of disadvantages associated with PPE utilization chief among them being the fact the PPE does not remove the hazards from the workplace hence its failure implies automatic exposure to the risk. As supported by Sehgal and Milton (103), a conclusion can be drawn that achievement of OSH sustainability in Mutare manufacturing factories will continue to be problematic as long as the hierarchy of risk control is not fully embraced. Education and training on the application of the risk assessment at the design stage of a system, process, and product should be provided to OSH practitioners, top managers, employers and employees in the manufacturing factories of Mutare. This will ensure that most effective and sustainable controls such as elimination of hazards and risks are applied at the design stage of a system, process, and product thereby offsetting the cost of sustaining perpetually risk control measures such as provision of PPE.
The majority of workers interviewed concurred to the existence of the accident reporting and recording element. The availability of accident reporting and recording procedures in most manufacturing factories of Mutare is induced by the fact that it is mandatory under Factories and Works Act Chapter 14:08 for workplaces to have accident registers upon which occupational accidents are recorded. This legal requirement is buttressed by the workers' compensation system of Zimbabwe that penalizes workplaces for non-reporting of occupational accidents within stipulated time frames. The revelation from the questionnaires results that Occupational Health Services is the least implemented element resonates very well with Masekameni et al. (104), and Moyo et al. (81), studies that reveal suboptimal implementation of Occupational Health Services in Southern Africa owing to critical shortage of occupational health practitioners.
There is therefore an urgent need for human resources' capacity development in the field of occupational health. As observed by worker interviewees', the subdued implementation of planned safety audits (13.3%) is indicative of absence of good safety culture that promotes proactiveness rather than reactiveness. This contradicts the Vision Zero concept, a global transformative approach to prevention of occupational accidents and diseases that regards proactiveness as an important value to successful management of OSH (78, 105, 106).
5 Reasons for non-implementation of OSH management systems by manufacturing industry of Mutare
Unavailability of punitive penalties for breaching OSH legislation that emerged as one prominent reason for non-implementation of OSHMSs in the manufacturing industry of Mutare is a bottleneck arising out of availability of outdated OSH laws that are not being reviewed periodically to ensure that they are deterrent enough to prompt organizations to consider failure of OSH as a huge cost to business and a threat to business sustainability. Unavailability of punitive penalties for OSH transgression is worsened by unavailability of labour courts specifically designed to effectively deal and expedite judgements on OSH legal matters. This finding places a demand on the Government of Zimbabwe for the need to reform the current OSH legal framework to ensure its effectiveness in promoting establishment of OSHMSs. Citation of lack of leadership and commitment as one important reason for failure to implement OSH management system is in tandem with the Vision Zero strategy golden rule number one which clearly recognizes visible felt leadership and commitment as the driving force in successful amelioration of occupational safety and health risks (78, 107). The concurrence by the majority of respondents that lack of adequate human, material and financial resources was a hindrance to implementation of OSH management systems was endorsed by Underhill et al. (108), who cited lack of adequate resources as a huge impediment to OSHMS implementation. This implies that without a sound national policies and promotional strategies to counter the burden of adequate human, material and financial resources, most organizations particularly the small to medium enterprise will perpetually remain incapacitated to establish all the critical elements of an effective OSHMS thereby ending up relegating OSH management systems to the bottom of their priority list.
5.1 Opportunities to improve uptake of OSH management systems in the manufacturing industry of Mutare
The results project the need for the regulatory authority (NSSA) to progressively interrogate and review its current OSHMS promotional strategy in order to build technical capacity in industry on how to effectively implement OSH management system. The need to build technical capacity in industry on implementation of OSH management system was corroborated by top managers who bemoaned acute knowledge gap on OSHMS implementation exacerbated by non-availability of qualified and competent OSH practitioners as contributing immensely to low uptake of a systems approach to OSH management in the generality of the manufacturing industry of Mutare. There is therefore a need for NSSA to roll out in a systematic manner deliberate educational programmes to raise OSH management systems awareness in the manufacturing industry of Mutare.
Establishment of an easy to implement model for OSH management systems with streamlined documentation (93%) also emerged prominently from the results. This solidifies observations made by other researchers (9, 89–91) that with changing work dynamics, a “one size fits all” approach to implementation of OSH management system may not be ideal considering the differentiation between large and small to medium enterprises as well as the socio-economic demographic differences. Zwetsloot (83) supports this view by asserting that OSH management systems do not function as independent systems but are rather impacted on by a range of internal and external factors. According to Zwetsloot (83), OSH management systems must be made better to suit the “changing world of work”, where production is increasingly being outsourced and risks are being easily shifted to partners in the supply chain.
Incorporation of OSH in all academic curricula offered at all tertiary institutions also emerged as handy in buttressing the quest for improved uptake of OSH management systems. Article 14 of the ILO Convention 155 on Occupational Safety and Health (50) supports this notion by asserting the need for measures to be taken in promoting the inclusion of questions of occupational safety and health and the working environment at all levels of education and training, including higher technical, medical, and professional education, in a manner meeting the training needs of all workers. Graduates that are eventually churned out of education systems are the future leaders at workplaces, hence should be equipped with the necessary OSH skills and competence to enable them to provide OSH leadership and commitment which is regarded as the nucleus of attainment of zero harm at the workplace according to ISSA (78). Over time, this will ultimately inculcate a national preventative safety and health culture in line with ILO fundamental OSH convention 187 on Promotional Framework for Occupational Safety and Health (51). However, in practice, the degree and level of inclusion of OSH in national education systems and trainings largely depend on the level of development of OSH systems and on specialized personnel available in a particular country (109). It is important to highlight that most initiatives to mainstream OSH in national education systems globally focus on the experience of developed economies and might not be fully applicable/transferable to developing economies, hence mainstreaming of OSH into national education system must be customized taking into considering the environmental context of the country.
The need to ensure that company owners, executives, senior managers, and OSH practitioners are trained on importance of OSHMS was also largely highlighted as an option helpful in aiding the uptake of OSH management systems. The current OSHMSs promotional strategy being championed by NSSA is proving to be falling short catalyzing increased uptake of OSH management systems in the manufacturing industry of Mutare. This compelling reality places a demand on NSSA to embrace a stakeholder approach in reforming its national OSHMSs promotional strategy to ensure increased educational and training support for decision makers such as company owners, executives, senior managers, and OSH practitioners Establishment of legislative provision to make OSHMS systems mandatory was cited as useful in aiding uptake of OSH management system. Use of legislation “command approach” can only be instrumental where there is a robust system of enforcement of the law. However, studies (9, 39) have proven that use of legislation alone cannot guarantee yielding of the desired results owing to several counteracting factors associated with enforcement in least developed and developing countries, such as corruption, nepotism, no punitive penalties, inadequate human, material, and financial resources among others. In line with this thinking, Yangho (110) affirmed OSH management systems strategy driven by self-motivation as a significant paradigm shift from prescriptive traditional OSH strategy (enforcement by law) that over the years proved to be unsuccessful and inefficient in curtailing occupational injuries and diseases. World over, self-compliance has taken center stage ahead of command approach and hence it is therefore paramount that workplaces align to the new paradigm of self-compliance buttressed by a firm understanding of the importance of OSH management systems in curtailing occupational accidents and diseases that negatively impact on business productivity and profitability.
The need to provide legislative provision to make availability of qualified and competent OSH practitioners mandatory at all workplaces was also echoed by majority of the respondents in all categories. Mandowa (39), study explored the association between the availability of an OSH practitioner and OSHMS implementation that demonstrated that availability of a qualified and competent OSH practitioner aided implementation of OSH management systems. This is mainly because a qualified and competent OSH practitioner is vested with OSH knowledge that can be deployed to convince top management to embrace OSH management systems as a business case for sustainable productivity and profitability. Notwithstanding the importance of OSH practitioners in driving the successful implementation of OSHMSs, their effectiveness is only enhanced in workplaces where there is top management commitment as top management's decisions have a bearing in unlocking the required resources to ensure sustainability in the implementation of the OSH management system. Legal and policy reformation to incorporate the need for qualified and competent OSH practitioners at workplaces will be handy in aiding the availability of the required expertise to champion the effective implementation of OSH management systems. To avoid the availability of incompetent OSH practitioners on the market, which is detrimental to OSH delivery in manufacturing industry of Mutare, competence criteria for OSH professions must be defined in policy in tandem with Article 5(c) of Convention No. 155 (50) and Article 11 of Convention No. 161 (111) even though there is no international labour standard that reflects member of States' agreement on the regulation of OSH professionals. As supported by Hale (112), there is a strong push in developed economies to regulate entry to OSH profession by defining exclusive education and training requirements for OSH practitioners to ensure the attainment of necessary knowledge and competence to effectively carry out OSH related functions.
Establishment of incentives that motivate OSHMSs implementation also emerged prominently as possible intervention to improve uptake of OSHMSs in view of the challenge of inadequate material and financial resources highlighted by the majority of Top managers. Taking into consideration the difficult socio-economic environment which is impacting negatively on business profitability in the majority of factories that make up the manufacturing industry of Mutare, there is need for the Government of Zimbabwe to come up with deliberate economic policy interventions, such as reduced import duty on all OSH necessities such as OSH technology, hygiene measuring equipment and personal protective equipment among others thereby making OSHMSs more attractive to all workplaces as this intervention will help to lower significantly high initial investment costs associated with implementation of OSHMSs and related costs associated with sustenance of the OSH management systems.
6 Limitations
This study, while groundbreaking in unravelling contextual insights on the impediments to uptake of OSHMSs, is not without limitations. Although reliability has been secured by providing a clear and structured methodology of data collection, the reproducibility of the results may be compromised owing to inherent limitations of questionnaires and interviews. As noted by Theofanidis et al. (113), most qualitative methodologies, such as interviews cannot be truly replicated (as in controlled experimental conditions) and therefore are unable to be easily verified. The use of Likert scale on the questionnaire presented a limiting factor when asking attitudes or behavioural questions. There was a possibility of having many participants gravitating towards avoiding the selecting of the extreme measures “Strongly Disagree” and “Strongly Agree” and preferring choosing middle measures like “Agree” and “Disagree”; this could lead to masking of the intensity of the real attitudes and behaviours of the participants. The deployment of data triangulation technique was handy in countering the questionnaire and interviews limitations so as to ensure the reliability and validity of the research results.
Another limitation of the study is that the research only concentrated on the manufacturing industry of Mutare thereby excluding many manufacturing industries in other regions of the country. Though the idea to focus on the manufacturing industry of Mutare is likely to affect the generalizability of the research findings across diverse manufacturing contexts, it was however prudent to focus on manufacturing industry of Mutare considering its bad OSH performance trait (32). Similarities in the political, socio-economic environmental context faced by manufacturing industries across the country and in many developing and least developed countries provided a strong case for a possibility of duplication and generalizability of the results beyond the study area. Another limitation of the study was the possibility of encountering restrictions on data access owing to company policy restrictions. This could have a negative impact on the quality of the data obtained thereby affecting reproducibility of the results, however it was countered by seeking prior permission from targeted organization to obtain relevant company information and to administer questionnaires and interviews without restrictions.
7 Conclusion
The study findings revealed the low uptake rate of OSH management systems (26.7%) by the manufacturing industry on Mutare that vindicates ILO's long held observation of non to suboptimal implementation of OSH management systems in the majority of the least developed and developing countries (1). It can be concluded that the low uptake rate revealed by the study is a serious bottleneck to the endeavor for the manufacturing industry of Mutare to secure OSH sustainability in the future of work in line with the ILO's Global Action for Prevention on Occupational Safety and Health (OSH-GAP) (114) which advocates for the development and implementation of sustainable and scalable actions for prevention of occupational injuries and diseases. It can be concluded from the low uptake rate in the manufacturing industry of Mutare that the current national OSHMSs promotional strategy spearheaded by NSSA in Zimbabwe is ineffective and hence require reformation. Results revealed a differentiation between large companies and small to medium companies as reflected by the fact that most of the OSH management systems were evident in large companies as compared to small to medium enterprises. This revelation places a demand for researchers to rethink the current global order where workplaces are expected to implement the same OSHMSs requirement irrespective of the size of the workplace and other underlying counteracting factors such as weak enforcement mechanism, human, material, and financial resources constraints among others.
Main reasons cited for non-implementation of OSH management systems included unavailability of punitive penalties given to organizations for causing accidents, lack of leadership and management commitment, high initial investment demanded in implementing an OSH management system and the cost of OSH management systems' sustenance, lack of human, material and financial resources to effectively implement OSH management systems. The study revealed a cocktail of opportunities that could be harnessed to ensure improved performance in uptake of OSH management systems that included the need to come up at national level with tailor-made awareness training programmes targeting company owners, executives, senior managers, and OSH practitioners., establishing educational and training programmes to build technical capacity in industry on implementation of OSH management system, establishment of an easy to implement model for OSH management systems with streamlined documentation targeting the small to medium enterprise, incorporation of OSH in all academic curriculums offered at all tertiary institutions so as to build a national preventive safety and health culture and the need to reform OSH legislation to make availability of qualified and competent OSH practitioners mandatory at all workplaces among others. Based on the results, a conclusion can be made that the ambition to improve uptake of OSH management systems substantially demands leadership and commitment of management, involvement of workers and the continual adaptation of off the shelf OSH management systems standards to be in sync with the operational economic environment, capacities, and efficiencies in the manufacturing industry of Mutare.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
JM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. MM: Supervision, Writing – review & editing. SJ: Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
Special acknowledgements go to my wife, Natashia Mandowa who assisted me in the collection of questionnaires from workplace as well as in extracting data from the questionnaires.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. ILO. Safety and health at work. (2023). Available at: https://www.ilo.org/global/topics/safety-and-health-at-work/lang–de/index.htm (Accessed December 22, 2023). [Ref list].
3. ILO. A call for safer and healthier working environments. (2023). Available at: https://www.ilo.org/publications/call-safer-and-healthier-working-environments (Accessed October 10, 2024).
4. Hämäläinen P, Takala J, Boon Kiat T. Global Estimates of Occupational Accidents and Work-related Illnesses (XXI World Congress on Safety and Health at Work, Singapore, Workplace Safety and Health Institute) (2017).
5. Mywage. Occupational Health and Safety Worldwide. (2015). Available at: http://m.mywage.org (Accessed September 17, 2015).
6. Takala J, Hämäläinen P, Saarela K, Yun L, Manickam K, Jin T, et al. Global estimates of the burden of injury and illness at work in 2012. J Occup Environ Hyg. (2014) 11(5):326–37. doi: 10.1080/15459624.2013.863131
7. Wang Y, Chen H, Liu B, Yang M, Long Q. A systematic review on the research progress and evolving trends of occupational health and safety management: a bibliometric analysis of mapping knowledge domains. Front Public Health. (2020) 8:81. doi: 10.3389/fpubh.2020.00081
8. Bianchini A, Donini F, Pellegrini M, Saccani C. An innovative methodology for measuring the effective implementation of an occupational health and safety management system in the European union. Saf Sci. (2017) 92:26–33. doi: 10.1016/j.ssci.2016.09.012
9. Mandowa J, Matsa M, Jerie S. A global review of implementation of occupational safety and health management systems for the period 1970–2020. Int J Occup Saf Ergon. (2022) 29(2):821–36. doi: 10.1080/10803548.2022.2083811
10. Vitrano G, Urso D, Micheli GJL, Guglielmi A, De Merich D, Pellicci M. Enabling effective implementation of occupational safety and health interventions. Saf Health Work. (2024) 15(2):213–9. doi: 10.1016/j.shaw.2024.04.003, ISSN 2093-791139035805
11. Vitrano G, Micheli GJL. Effectiveness of occupational safety and health interventions: a long way to go. Front Public Health. (2024) 12:1292692. doi: 10.3389/fpubh.2024.1292692
12. Dyreborg J, Lipscomb HJ, Nielsen K, Törner M, Rasmussen K, Frydendall KB, et al. Safety interventions for the prevention of accidents at work: a systematic review. Campbell Syst Rev. (2022) 18:1–187. doi: 10.1002/cl2.1234
13. Othmani I, Kamil M, Sunindijo RY, Alnsour M, Kineber AF. Critical success factors influencing construction safety program implementation in developing countries. J Phys Conf Ser (2020) 1529:042079. doi: 10.1088/1742-6596/1529/4/042079
14. Njogu PK, Mburu C, Karanja B. Role of safety and health awareness in occupational safety and health performance in public health facilities in Machakos County, Kenya. J Environ Health Res. (2019) 5(1):1–7. doi: 10.11648/j.jher.20190501.11
15. Nordlof H, Hogberg H, Wiitavaara B. A cross sectional study of factors influencing occupational health and safety management practices in companies. Saf Sci. (2017) 5:92–103. doi: 10.1016/j.ssci.2017.02.008
16. Vitrano G, Micheli GJL, Guglielmi A, De Merich D, Pellicci M, Urso D, et al. Sustainable occupational safety and health interventions: a study on the factors for an effective design. Saf Sci. (2023) 166:106249. doi: 10.1016/j.ssci.2023.106249
17. Micheli GJL, Gnoni MG, de Merich D, Sala G, Rosso A, Tornese F, et al. Barriers, drivers and impact of a simplified occupational safety and health management system in micro and small enterprises. In: Arezes P, editor. Advances in Intelligent Systems and Computing. Cham: Springer Verlag (2019). p. 81–90. doi: 10.1007/978-3-319-94589-7_8
18. Ghahramani A. Factors that influence the maintenance and improvement of OHSAS 18001 in adopting companies: a qualitative study. J Clean Prod. (2016) 137:283–90. doi: 10.1016/j.jclepro.2016.07.087
19. Nordlöf H, Wijk K, Westergren K-E. Perceptions of work environment priorities: are there any differences by company size?—an ecological study. Work. (2015) 52(3):697–706. doi: 10.3233/WOR-152123
20. Ismail Z, Doostdar S, Harun Z. Factors influencing the implementation of a safety management system for construction sites. Saf Sci. (2012) 50:418–23. doi: 10.1016/j.ssci.2011.10.001
21. Acakpovi A, Dzamikumah L. An investigation of health and safety measures in a hydroelectric power plant. Saf Health Work. (2016) 7:331–9. doi: 10.1016/j.shaw.2016.04.006
22. Rajaprasad SVS, Chalapathi PV. Factors influencing implementation of OHSAS 18001 in Indian construction organizations: interpretive structural modeling approach. Saf Health Work. (2015) 6:200–5. doi: 10.1016/j.shaw.2015.04.001
23. da Silva SLC, Amaral FG. Critical factors of success and barriers to the implementation of occupational health and safety management systems: a systematic review of literature. Saf Sci. (2019) 117:123–32. doi: 10.1016/j.ssci.2019.03.026
24. Zwetsloot G, Bezemer R, Drupsteen L, Kines P, Ruotsala R. Success factors for the implementation of Zero Accidents Vision. TNO Report, Earth, Life and Social Sciences, Netherlands. (2015). Available at: https://www.dguv.de/medien/ifa/en/netzwerke/zaf/r11506-tno-report-dguv-zav-project-617.0-fp-0352-(nov-2015).pdf (Accessed February 02, 2021).
25. ILO. Building an inclusive future with decent work: towards sustainable development in Asia and the Pacific. Report of the Director- General: 16th Asia and the Pacific Regional Meeting, Bali, Indonesia (2016).
26. ILO. Occupational Safety and Health Management Systems. (2014). Available at: http://ilo.org/safework/areasofwork/occupational-safety-and-health-management-systems/lang–en/index.htm (Accessed January 12, 2015).
27. Moyo D, Zungu M, Kgalamono S, Mwila C. Review of occupational safety and health organization in expanding economies: case of Southern Africa. Ann Glob Health. (2015) 81(4):495–502. doi: 10.1016/j.aogh.2015.07.002
28. ILO. Improving Safety and Health at Work Through the Decent Work Agenda. Geneva: International Labour Organization (2015). Available at: http://www.ilo.org/safework/projects/WCMS_149466/langeen/index.htm. (Accessed May 13, 2021).
29. Mywage. Occupational Health and Safety Worldwide (2014). Available at: http://m.mywage.org (Accessed September 17, 2015).
30. Magada EY. O-357 occupational accidents and diseases in Zimbabwe: the economic burden—2009 to 2018. Occup Med (Chic Ill). (2024) 74(Supplement_1), doi: 10.1093/occmed/kqae023.1317
31. Shava C. Rising occupational fatalities and injuries worry Government. The Sunday News. (2024). Available at: https://www.sundaynews.co.zw/rising-occupational-fatalities-injuries-worry-government/#:∼:text=%E2%80%9CIn%202023%20alone%2C%20Nssa%20reported,reveal%2C%E2%80%9D%20said%20Dr%20Shava (Accessed October 06, 2024).
32. Mutetwa B. A systematic review of trends and patterns in occupational safety and health performance in Zimbabwe. 58th SHAW Conference, Rainbow Towers Hotel, Harare, Zimbabwe (2021).
33. Dhliwayo R. Occupational safety and health performance: January to December 2014: injury frequency rates by NSSA regions. On Guard Mag. (2014) 10(1):5–6.
34. ILO. Global strategy on occupational safety and health. (2024). Available at: https://www.ilo.org/resource/policy/global-strategy-occupational-safety-and-health (Accessed October 09, 2024).
35. Pandey BR. Rethinking occupational health and safety principles—a systems perspective. J R Soc N Z. (2024):1–22. doi: 10.1080/03036758.2024.2333555
36. Shabani T, Jerie S, Shabani T. Overview of quality health safety and environmental management systems implementation in Zimbabwe. Saf Extrem Environ. (2024) 6:29–41. doi: 10.1007/s42797-023-00090-8
37. Shabani T, Jerie S, Shabani T. The impact of occupational safety and health programs on employee productivity and organizational performance in Zimbabwe. Saf Extrem Environ. (2023) 5:293–304. doi: 10.1007/s42797-023-00083-7
38. Musungwa T, Kowe P. Effects of occupational health and safety management systems implementation in accident prevention at a Harare beverage company. Cogent Eng. (2022) 9(1):6–7. doi: 10.1080/23311916.2022.2124638
39. Mandowa J. Evaluation of OSH management systems implementation by mutare urban timber processing sector (Dissertation). Midlands State University, Gweru, Zimbabwe (2015).
40. Jerie S. ‘Occupational health and safety problems among workers in the wood processing industries in Mutare’, journal of emerging trends in economics and management sciences (JETEMS). Sch Res Inst J. (2012) 3(3):278–85. Available at: http://www.jetems.scholarlinkresearch.org.
41. Singh D. Understanding philosophical underpinnings of research with respect to various paradigms: perspective of a research scholar. (2019). Available at: https://www.researchgate.net/publication/333036861 (Accessed May 03, 2024).
42. Kivunja C, Kuyini AB. Understanding and applying research paradigms in educational contexts. Int J High Educ. (2017) 6(5):26–41. doi: 10.5430/ijhe.v6n5p26
43. Turner D. Sampling Methods in Research Design. (2020). Available at: https://headachejournal.onlinelibrary.wiley.com/doi/abs/10.1111/head.13707 (Accessed March 14, 2021).
44. Babbie ER. The Practice of Social Research. 14th ed. Boston, MA: Cengage Learning US (2015). p. 22–7.
45. Gray DE. Doing Research in the Real World, 3rd ed. London: Sage (2014). Available at: https://www.worldcat.org/title/doing-research-in-the-real-world/oclc/858825461 (Accessed July 15, 2021)
46. Bailey LF. The origin and success of qualitative research. Int J Mark Res. (2014) 56:167–84. doi: 10.2501/ijmr-2014-013
47. Landsverk J, Brown H, Chamberlain P, Palinkas LA, Horwitz SM. Design and analysis in dissemination and implementation research. In: Brownson RC, Colditz GA, Proctor EK, editors. Translating Science to Practice. New York: Oxford University Press (2012). p. 225–60.
49. Fusch PI, Ness LR. Are we there yet? Data saturation in qualitative research. Qual Res J. (2015) 20(9):1408–16. doi: 10.46743/2160-3715/2015.2281
50. ILO. C155—Occupational Safety and Health Convention, 1981 (No. 155). (1981). Available at: https://www.ilo.org/dyn/normlex/en/f?p = NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C155 (Accessed October 12, 2022).
51. ILO. C187—Promotional Framework for Occupational Safety and Health Convention, 2006 (No. 187). (2006). Available at: https://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C187 (Accessed October 13, 2022).
52. ISO. ISO 45001:2018 Occupational health and safety management systems — Requirements with guidance for use. (2018). Available at: https://www.iso.org/standard/63787.html (Accessed September 01, 2021).
53. Zwetsloot G. Evidence of the benefits of a culture of prevention. From Risk to Vision Zero- Proceedings of the International Symposium on Culture of Prevention- Future Strategies (2014). p. 30–5
54. Korzynski P. Employee motivation in new working environment. Int J Acad Res. (2013) 5:184–8. doi: 10.7813/2075-4124.2013/5-5/b.28
55. Ellen S. Slovin’s Formula Sampling Technique, (2020). Available at: https://sciencing.com/how-6188297-do-determine-audit-sample-size-.html (Accessed July 26, 2021).
56. Gergen KJ, Josselson R, Freeman M. The promises of qualitative inquiry. Am Psychol J. (2015) 70(1):1–9. doi: 10.1037/a0038597
57. Cronin C. Using case study research as a rigorous form of inquiry. J Nurs Res. (2014) 21(5):19–27. doi: 10.7748/nr.21.5.19.e1240
58. Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. London.UK: Sage publications (2014).
59. Mark S, Philip L, Adrian T. Research Methods for Business Students. 5th ed. Edinburgh Gate, England: Pearson Education Limited (2009).
60. Crawshaw J, Chambers J. Advanced Level Statistics with Worked Examples. 4th ed. United Kingdom: Nelson Thornes Ltd (2001).
61. Mburu C, Karanja B, Njogu KP. Effects of management commitment and Workers’ participation on occupational safety and health performance in public health facilities. J Environ Health Res. (2019) 5(2):54. doi: 10.11648/j.jher.20190502.14
62. Mugenda OM, Mugenda AG. Research Methods: Quantitative and Qualitative Approaches. Revised ed. Nairobi: Act press (2003).
63. von Thiele Schwarz U, Hasson H, Tafvelin S. Leadership training as an occupational health intervention: improved safety and sustained productivity. Saf Sci. (2016) 81:35–45. doi: 10.1016/j.ssci.2015.07.020
64. Hunt N, Tyrrel S. Stratified Sampling. Webpage at Coventry University (2001). Available at: http://ea.wikipedia.org/wiki/Stratified_sampling # cite_ref1 (Accessed December 12, 2014).
65. Neuman WL. Basics of Social Research: Qualitative and Quantitative Approaches. 2nd ed. Boston, MA: Allyn and Bacon (2007).
66. Patton MQ. Qualitative Research & Evaluation Methods. 3rd ed. London: Sage Publications (2002). p. 15–9.
67. Frey LR, Botan CH, Kreps GL. Investigating Communication: An introduction to Research Methods. 2nd ed. Boston: Allyn & Bacon (2000). p. 4–6.
68. Trochim W, Donnelly JP, Kanika A. Research Methods: The Essential Knowledge Base. United Kingdom: CENGAGE Learning (2015). p. 219–20.
69. Cucos L. How to calculate Cronbach’s Alpha in SPSS. (2022). Available at: https://uedufy.com/how-to-calculate-cronbachs-alpha-in-spss/ (Accessed June 27, 2022).
70. Jilcha K. A new integrated system of safety and health model development for manufacturing industries: a case of Ethiopia. J Ergon. (2020) 10:265. doi: 10.35248/2165-7556.20.10.265
71. Rea M, Parker R. Designing and Conducting Survey Research: A Comprehensive Guide: Jossey-Bass Publishers. Hoboken: University of Michigan (1997). p. 20–1.
72. Neuman W. Social Research Methods: Qualitative and Quantitative Approaches. Essex, UK: Pearson (2014).
73. Colden Corporation. Occupational Health and Safety Management Systems (OHSMS). (2022). Available at: https://www.colden.com/occupational-health-and-safety-management-systems-ohsms/ (Accessed February 05, 2022).
74. Lis T, Nowacki K. Modern Trends in Occupational Safety Management. Poland: Silesian University of Technology (2019). Vol 2(2). p. 126–38.
75. Dolinski D, Grzyb T, Kulesza W, Błaszczyk P, Laska D, Liebersbach F, et al. ‘We are looking for people like you’—new technique of social influence as a tool of improving response rate in surveys. Soc Influ. (2024) 19(1):1–14. doi: 10.1080/15534510.2024.2316348
76. Booker QS, Austin JD, Balasubramanian BA. Survey strategies to increase participant response rates in primary care research studies. Fam Pract. (2021) 38(5):699–702. doi: 10.1093/fampra/cmab070
77. ILO. C111—Discrimination (Employment and Occupation) Convention, 1958 (No. 111). (1958). Available at: https://normlex.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C111 (Accessed November 21, 2024).
78. ISSA. Vision Zero. 7 golden Rules- for zero accidents and healthy work: A guide for employers and managers. (2017). Available at: http://visionzero.global/ (Accessed December 01, 2018).
79. Frick K, Zwetsloot G. From safety management to corporate citizenship: an overview of approaches to managing health. In: Johansson U, Ahonen G, Roslender R, editors. Work Health and Management Control. Stockholm: Thomson Fakta (2007). p. 99–134.
80. Stroh DP. Introduction to systems thinking. Proceedings of the how Will the Future of Work Shape the OSH Professional of the Future? A Workshop. Shaping the Future to Ensure Worker Health and Well-Being: Shifting Paradigms for Research, Training and Policy, Houston, TX, USA (2020).
81. Moyo D, Zungu M, Erick P, Tumoyagae T, Mwasa C, Muteti S, et al. Occupational health and safety in the Southern African development community. Occup Med. (2017). doi: 10.1093/occmed/kqx071
82. Awang N, Baharudin MR, Saliluddin SM. Occupational safety and health management system (OSHMS): perception and safety satisfaction among employees in certified organisations in Klang valley. Int J Educ Res. (2019) 7(7):38–44.
83. Zwetsloot G. What are Occupational Safety and Health Management Systems and Why do Companies Implement Them? Hague: Netherlands Organization for Applied Scientific Research (2022). Available at: https://oshwiki.eu/wiki/What_are_occupational_safety_and_health_management_systems_and_why_do_companies_implement_them%3F (Accessed September 23, 2022).
84. Zwetsloot G. Developments and debates on OHSM system standardization and certification. In: Frick K, Quinlan M, Langaa Jensen P, Wilthagen T, editors. Systematic Occupational Safety & Health Management: Perspectives on an International Development. Oxford: Pergamon-Elsevier Science (2000). p. 391–412.
85. Mollo LG, Emuze F, Smallwood J. Using a safety management system to reduce errors and violations. Proc Inst Civ Eng. (2021) 174(3):136–43. doi: 10.1680/jmuen.20.00017
86. Zwetsloot G, Zwanikken S, Hale A. Policy expectations and the use of market mechanisms for regulatory OSH certification and testing regimes. Saf Sci. (2011) 49(7):1007–13. doi: 10.1016/j.ssci.2010.12.006
87. You NSN, Chan DWM, Shan M, Sze NN. Implementation of the safety management system in managing construction projects: benefits and obstacles. Saf Sci. (2019) 117:23–32. doi: 10.1016/j.ssci.2019.03.027
88. Achieng OC. Implementing Occupational Health and Safety Management Systems: An Analysis of Employee Capacity Gaps at a Wind Energy Establishment in Kenya. (2018). Available at: http://erepository.uonbi.ac.ke/bitstream/handle/11295/104757/Cynthia%20Achieng_M.A%20EPM%20Final%20Project%20Report%20%2814.12.2018%29.pdf?sequence=1&isAllowed=y (Accessed February 13, 2022).
89. Surienty L. Management Practices and OSH Implementation in SMES in Malaysia, School of Management. Pulau Pinang. Malaysia: Universiti Sains Malaysia (2012). Available at: http://ilera2012.wharton.upenn.edu/RefereedPapers/SurientyLilisILERA.pdf (Accessed July 17, 2015).
90. Frick K. Occupational Health & Safety Management Systems—when are They Good for Your Health? Mälardalen University, Sweden European Trade Union Institute, aisbl, Sweden (2011).
91. McKinney P. Expanding HSE’s ability to communicate with small firms: A targeted approach (No. 420/2002): Prepared by AEA Technology plc for the Health and Safety Executive), (2002).
92. Lamm F. Small business and occupational health and safety advisors. Saf Sci J. (1997) 25:153–61. doi: 10.1016/S0925-7535(97)00013-1
93. Tejamaya M, Puspoprodjo W, Susetyo H, Modjo R. An analysis of pivotal factors in the implementation of occupational health and safety management systems in micro, small and medium enterprises (MSMEs): literature review. Gac Sanit. (2021) 35(S2):S348–59. doi: 10.1016/j.gaceta.2021.10.050
94. Vassie L, Tomas JM, Oliver A. Health and safety management in UK and Spanish SMEs: a comparative study. J Saf Res. (2000) 31:35–43. doi: 10.1016/S0022-4375(99)00028-6
95. Eakin JM, Lamm F, Limborg HJ. International perspective on the promotion of health and safety in small workplaces. Workshop on Policies for Occupational Health & Safety Management Systems and Workplace Change, 21st-24th September, Amsterdam (1998).
96. Wright M. Factors Motivating Proactive Health and Safety Management, Contact Research Report Prepared for Entec UK Ltd for the Health and Safety Executive. London: HMSO (1998).
97. Gilkey DP, Keefe TJ, Hautaluoma JE, Bigelow PL, Herron RE, Stanley SA. Management commitment to safety and health in residential construction: home safe spending trends 1991–1999. Work. (2003) 20:35–44.12632001
98. Sankar SS, Anandh KS. Navigating leadership styles through qualitative exploration for enhanced safety in the construction sector. Saf Sci. (2024) 175:106495. doi: 10.1016/j.ssci.2024.106495
99. Oswald D, Lingard H. Development of a frontline H&S leadership maturity model in the construction industry. Saf Sci. (2019) 118:674–86. doi: 10.1016/j.ssci.2019.06.005
100. UN. Universal Declaration of Human Rights. (1948). Available at: https://www.un.org/sites/un2.un.org/files/2021/03/udhr.pdf (Accessed November 5, 2021).
101. Khoshakhlgh A, Malakoutikhah M, Park J, Kodnoueieh M, Boroujeni Z, Bahrami M, et al. Assessing personal protective equipment usage and its correlation with knowledge, attitudes, performance, and safety culture among workers in small and medium-sized enterprises. BMC Public Health. (2024) 24:1987. doi: 10.1186/s12889-024-19517-3
102. NIOSH. About Hierarchy of Controls. (2024). Available at: https://www.cdc.gov/niosh/hierarchy-of-controls/about/?CDC_AAref_Val=https://www.cdc.gov/niosh/topics/hierarchy/default.html (Accessed October 23, 2024).
103. Sehgal NJ, Milton DK. Applying the hierarchy of controls: what occupational safety can teach US about safely navigating the next phase of the global COVID-19 pandemic. Front Public Health. (2021) 9:747894. doi: 10.3389/fpubh.2021.747894
104. Masekameni MD, Moyo D, Khoza N, Chamdimba C. Accessing occupational health services in the Southern African development community region. Int J Environ Res Public Health. (2020) 7(18):6767. doi: 10.3390/ijerph17186767
105. Jilcha K. Vision zero for industrial workplace safety innovative model development for metal manufacturing industry. Heliyon. (2023) 9(11). doi: 10.1016/j.heliyon.2023.e21504
106. Alanko T, Ruotsala R. A multi-perspective framework of vision zero: toward collaborative promotion of safety, health and well-being at work. Saf Health Work. (2022) 13(3):372–5. doi: 10.1016/j.shaw.2022.05.001
107. Mandowa J. Vision Zero Seven Golden Rules Paper Presented to SHAW Conference, Harare, Zimbabwe (2019).
108. Underhill E, Worland D, Fitzpatrick M. Self-Employment in the Victorian Construction Industry: An assessment of its impact on individual workers and the industry, (1997). A Report prepared for the Redundancy Payment Central Fund Limited (Incolink), Melbourne.
109. ILO. ILO Training Package on Development of a National Programme of Occupational Safety and Health. Geneva: ILO (2012).
110. Yangho K, Jungsun P, Mijin P. Creating a culture of prevention in occupational safety and health practice. Saf Health Work. (2016) 7(2):89–96. doi: 10.1016/j.shaw.2016.02.002
111. ILO. C161—Occupational Health Services Convention, 1985 (No. 161). (1985). Available at: https://www.ilo.org/dyn/normlex/en/f?p = NORMLEXPUB:55:0:::55:P55_TYPE,P55_LANG,P55_DOCUMENT,P55_NODE:CON,en,C161,/Document (Accessed November 01, 2021).
112. Hale A. Occupational safety and health (OSH) Professions: Who are they and why do we need them? (2019). Available at: https://www.ilo.org/global/topics/safety-and-health-at-work/events-training/events-meetings/world-day-for-safety/33thinkpieces/WCMS_678734/lang–en/index.htm (Accessed October 15, 2022).
113. Theofanidis D, Fountouki A. Limitations and delimitations in the research process. Perioper Nurs. (2019) 7(3):155–62. doi: 10.5281/zenodo.2552022 E-ISSN: 2241-3634.
114. ILO. ILO OSH GAP. Health and Safety at the Workplace. (2017). Available at: https://www.ilo.org/wcmsp5/groups/public/—ed_dialogue/—lab_admin/documents/project documentation/wcms_541545 (Accessed October 09, 2021).
Keywords: occupational safety and health, occupational safety and health management system, decent work, developing countries, OSH sustainability
Citation: Mandowa J, Matsa M and Jerie S (2025) Uptake of occupational safety and health management systems in manufacturing industry of Zimbabwe: case of Mutare manufacturing factories. Front. Environ. Health 4:1565213. doi: 10.3389/fenvh.2025.1565213
Received: 22 January 2025; Accepted: 29 May 2025;
Published: 19 June 2025.
Edited by:
Atul Kumar Singh, Dayananda Sagar College of Engineering, IndiaReviewed by:
Sathvik Sharath Chandra, Dayananda Sagar College of Engineering, IndiaK. S. Anandh, SRM Institute of Science and Technology, India
Copyright: © 2025 Mandowa, Matsa and Jerie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johanes Mandowa, am1hbmRvd2FAZ21haWwuY29t