 Binod Kumar Behera
Binod Kumar Behera Binod Kumar Patro
Binod Kumar Patro Manish Taywade
Manish Taywade Mukunda Chandra Sahoo2
Mukunda Chandra Sahoo2
- 1Department of Community Medicine and Family Medicine, All India Institute of Medical Sciences Bhubaneswar, Bhubaneswar, India
- 2Department of Hospital Administration, All India Institute of Medical Sciences Bhubaneswar, Bhubaneswar, India
Background: Adequate water, sanitation, and hygiene (WASH) are essential to sustain healthy living. Providing WASH in any working facility, like hospitals and educational and non-educational institutions, helps prevent infections and the spread of disease and protects the stakeholders and the community from various infectious diseases. According to the 2030 vision for WASH in Schools agenda for Sustainable Development Goal, governments must work on universal and equitable access to safe and affordable drinking water.
Methods: This cross-sectional study assessed the WASH status of all the Anganwadi centers (AWCs)/Indian preschools and interviewed all the Anganwadi workers working in those centers using a semi-structured pre-tested questionnaire developed by modifying the Swachh Vidyalaya Puraskar assessment questionnaire. It collected data on the availability and gaps in the WASH infrastructure at the Anganwadi centers and the training needs of the Anganwadi workers using the epi-collect-5 digital platform.
Results: In the present survey, 58.3% of the AWCs run in government buildings. A daily cleaning schedule was not followed in 68.2% of the AWCs. An improved source of drinking water was available in 83.7% of the AWCs. In more than 86% of the AWCs, there were either no toilets available or available toilets that were not child-friendly. Over 90% of the AWCs had no handwashing facility for the kids to use after toilet use or before eating the hot cooked food served. More than 70% of the Anganwadi workers need to be sensitized or trained related to WASH.
Conclusion: Infrastructure improvement needs to be done, such as constructing child-friendly toilets or modifying existing toilets into child-friendly ones. Once the department's human resources are sensitized about the importance of WASH through on-job training, they can be asked to supervise the kids' hand hygiene practices. In the long run, all these will lead to a decrease in health-related issues due to lack of sanitation and improve the health and learning ability of the kids.
Highlights
• This research reveals poor WASH infrastructure in a rural Odisha district in Anganwadi centers.
• This research highlights the need for workforce training to create awareness of sanitation and hygiene among kids.
Introduction
Adequate water, sanitation, and hygiene (WASH) are essential to sustain healthy living. Providing WASH in any working facility, like hospitals and educational and non-educational institutions, helps prevent infections and the spread of disease and protects the stakeholders and the community from various infectious diseases (1). WASH facilities broadly refer to the quantity and quality of facilities such as access to safe and wholesome water, access to toilets, proper waste management, a clean environment, and availability of hygiene facilities. Sustainable Development Goal (SDG) number 6 aims to “ensure available and sustainable management of water and sanitation for all.” It includes universal access to all drinking water, sanitation, and hygiene targets by 2030 (6.1 and 6.2). The term “universal” implies all settings, including households, schools, healthcare facilities, workplaces, and public places, and “for all” suggests services suitable for men, women, girls, and boys of all ages, including people with disabilities (2). In most parts of India, preschools or Angan Wadi Centre (AWC) are the first place where the kids playfully learn nonformal education under the integrated child development services scheme (ICDS), besides getting supplementary nutrition (3). According to various reports, attendance in the schools and AWC in India has increased. However, the infrastructure and conditions still need to be improved. Most of the time, the school or teaching curriculum needs more scope for formal teaching and training about hygienic practices (4). Mostly, government-run schools and AWCs are attended by children from low-income families who have never been taught hygienic practices at home. Hence, AWCs are ideal places to make them aware of sanitation and hygienic practices. It has been discussed in larger forums, and there is evidence that one of the main reasons for girls” dropout in Indian schools is the lack of infrastructure and proper WASH facilities (5). There is evidence that diseases related to sanitation and hygiene are the primary reasons for school dropout and school absenteeism in India (6). Improving the WASH facility in the schools and AWCs is more likely to prevent school dropout and absenteeism due to sickness. According to the 2030 vision for WASH in Schools agenda for Sustainable Development Goal, governments must work on universal and equitable access to safe and affordable drinking water (2). In 2019, Globally, 69% of schools had a basic drinking water service, 63% of schools had a basic sanitation service, and 57% of schools had a basic hygiene service; for India, the figures are 67%,64%, and 53% with a lot of rural and urban differences (7).
The government has implemented several nutrition programs for Anganwadi Centres and school children (8–10). The Midday Meal (MDM) scheme is the school meal program that started with the twin objectives of improving the health and education of poor children and improving school children's attendance and retention. In ICDS, the main aim is to provide supplementary nutrition to small kids likely to be deprived of proper nutrition at home. Supplementary nutrition is provided as ready-to-eat food or a hot cooked meal prepared by the Anganwadi worker and the helper. There should be provision for safe and wholesome water to provide cooked Meals under the program and to eat the cooked food (11). The kids at AWC need to wash their hands before eating food or using the toilet. Washing hands can prevent the spread of respiratory and diarrheal infections. An adequate and clean water supply, soap, and a designated hand washing station should be provided for proper hand washing. Improving WASH facilities in schools and preschools alike will prevent waterborne diseases among the kids and prevent school dropout and sickness absenteeism. There is a paucity of literature assessing the WASH at preschools/AWCs of India and Odisha. With this background in mind, the present survey was done to assess the WASH in the AWCs and determine the training needs of the Anganwadi workers (AWW) regarding the WASH in the district so that the district administration can give suggestions to improve them.
Methods
Study setting
Jajpur district is one of the rural districts of Odisha in eastern India. It has 1,781 villages with an 1,826,275 population. The district has 10 Tahsils, 10 Blocks, and 311-g panchayats, which are smaller administrative divisions (in descending order) of districts that are larger administrative divisions of a state (12). Agriculture and mining play a dominant role in the district's economy. In recent years, Jajpur District has taken significant strides in industrial development. The literacy rate of the Jajpur District is 80.44 percent. Jajpur was declared an Open defecation-free District under the Swachha Bharat Mission 2019. According to the Jajpur district's secondary data, 2,724 AWCs run in 10 blocks across the districts.
Study design
The present study adopted a cross-sectional design to know the status of WASH in the Anganwadi centers of this district. The study assessed the WASH status of all the AWCs and interviewed all the Anganwadi workers working in those centers between October 2021 and May 2022 in the Jajpur district.
Data collection
Data was collected using a semi-structured pre-tested questionnaire developed by modifying the Swachh Vidyalaya Puraskar assessment questionnaire (11). The modified questionnaire was translated to Odia (local language) and back-translated to English by another independent translator to see whether the meaning of the question-altering after-translation or remaining the same. The English and Odia questionnaires collected data on the availability and gaps in the WASH infrastructure at the Anganwadi centers. Drinking water from an improved source and water is available at the school at the time of the survey is called a basic drinking water service; improved sanitation facilities at the schools that are single-sex and usable (available, functional, and private) at the time of the survey are called basic sanitation service and Handwashing facilities with water and soap available at the school at the time of the study is called a basic hygiene service as per the Joint Monitoring Program service ladders for global monitoring of WASH in schools (13). It also assessed the awareness of the AWC staff regarding the importance of WASH in life and their training needs. The questionnaire also captured the promotion of the WASH concept among the kids by the Anganwadi workers. The data were collected using the epi-collect-5 digital platform by a team of 11 members with a master's degree in Social work and previous experience in WASH-related projects. They were selected and trained to assess the AWCs by visiting and interacting with the concerned Anganwadi workers and observing the facilities at the AWCs. Consent was obtained from the respondents (Anganwadi workers). The collected data was available in digital format only and could only be assessed by the research team. The Institute Ethics Committee of All India Institute of Medical Sciences, Bhubaneswar, and the State Ethics Committee of Odisha approved the study. The descriptive analysis of the collected data was doen using SPSS Windows version 20.
Results
In the present study, we assessed 2,607 Anganwadi centers in the district. In the district, 58.3% of the AWCs run in government buildings, more than 40% of AWCs run in places like temples or places provided by charitable organizations or under the trees, and around 1.3% of AWCs rent buildings. Daily cleaning schedule was not followed in 68.2% of the AWCs, and it was observed that cleaning agents like floor cleaning solutions were not available in 60.0% of the AWCs. Improved sources of drinking water (13) available in 83.7% of the AWCs, as shown in Table 1.
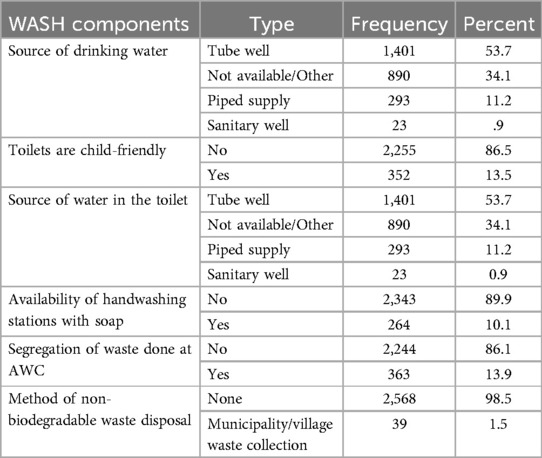
Table 1. Source of drinking water in the AWCs of the district Jajpur (n = 2,607).
In more than 86% of the AWCs, there were either no toilets available or available toilets that were not child-friendly. Besides, there was no running water in the toilets in 90% of the AWCs, as shown in Table 1. Over 90% of the AWCs had no handwashing facility for the kids to use after toilet use or before eating the hot cooked food served. An AWC caters to around 40–45 children as a day-care centre, providing cooked food per the schedule. Household and general cooking waste generation can occur as cooked meals are prepared. Table 1 shows the segregation and disposal of the garbage generated at AWCs. The food waste is being disposed of in compost pits in only 252 (9.7%) AWCs, and kitchen grey water is used for kitchen gardens in 133(5.1%) of the AWCs.
The present survey found that 72.9% of the AWWs are not trained in WASH. Most of the Anganwadi centers do not even paste any WASH-related posters to create awareness about sanitation and hygiene, as shown in Table 2.
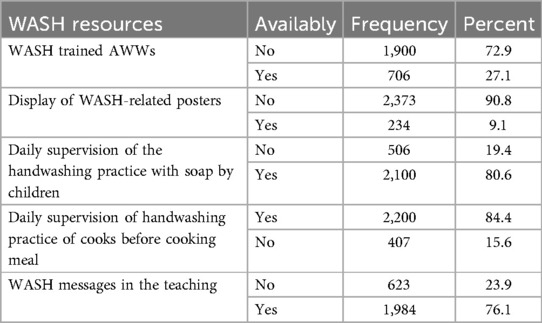
Table 2. Availability of WASH resources and supervision at the AWCS of the district Jajpur.
The data collected and compiled in the Joint monitoring program service ladder for WASH in school, which is being used to compare and monitor services in school, shows that except for the water provision, the other two indicators' performance is inferior in the district's AWCs, as shown in Table 3.
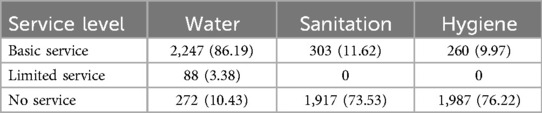
Table 3. Distribution of Anganwadi centers per JMP service ladder for WASH in the district Jajpur.
More than 86% of the AWCs have basic water service on their premises, whereas more than 73% have no sanitation and hygiene service, as shown in Table 3.
Discussion
The present study assessed the WASH infrastructure in the preschools of the rural district of Odisha, India, besides assessing the training needs of the AWWs in WASH and sanitary practices adopted at the AWCs. It is encouraging that this district has more than 58% AWC in the government building. Conference of State Women and Child Development Ministry report says that out of the 2,701 audited AWCS, only 39% were found in government-owned buildings, 29% in rented facilities, and 32% in other premises.
The Anganwadi Helper (AWH) is responsible for cleaning the AWC premises and helping the AWW with other routine work. They must be aware of the importance of hygiene and cleanliness to make the children aware of sanitation. The Village Health Sanitation and Nutrition Committee may resource cleaning agents (14).
Improved sources include piped water, boreholes or tube wells, protected dug wells, protected springs, and packaged or delivered water (13). Over 80% of the AWCs have unimproved sources, including unprotected wells, springs, and surface water. The remaining 34% of the AWCs can be supplied with piped water through rural water schemes or Jal Jeevan missions.
Most AWCs (90%) lack running water facilities in the available toilets and no handwashing station with soap. The children availing of those facilities are at greater risk of developing waterborne diseases, which should be addressed immediately. In this district, 58% of the AWCs are in government buildings. It is expected that those buildings will be WASH compliant, but it was found that 86.5% of such facilities do not have a toilet that is child-friendly. The unavailability of child-friendly toilets makes the available toilets unusable, so child-friendly toilets should be built whenever there is a proposal for constructing the AWC building. With the implementation of solid and liquid waste management at the village level, the kitchen waste generated at the AWCs should be collected by the village waste collection system. This will reduce the haphazard waste disposal in nearby areas and improve the village's overall sanitation.
More than 70% of the Anganwadi workers need to be sensitized or trained related to WASH, leading to poor handwashing supervision. The display of posters or wall paintings improves the community's awareness; the same needs to be improved in most of this district's AWCs (90.8%). The district administration should train all the AWCs and AWHs in WASH to implement and supervise the children attending their AWCs.
Conclusions
To make the AWCS of the district WASH compliant, a lot of infrastructure improvement in terms of construction of child-friendly toilets or modification of existing toilets to child-friendly needs to be done. Once the department's human resources are sensitized about the importance of WASH through on-job training, they will implement and supervise the hygienic and sanitary practices of the children attending their AWCs.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
BB: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. BP: Funding acquisition, Investigation, Methodology, Supervision, Writing – review & editing. MT: Formal analysis, Supervision, Writing – review & editing. MS: Project administration, Resources, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Fund was received for the work from District collector office Jajapur, Odisha.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. CDC. Water, Sanitation, and Hygiene (WASH) in Healthcare Facilities. Global Water, Sanitation, and Hygiene (WASH). (2024). Available at: https://www.cdc.gov/global-water-sanitation-hygiene/prevention/index.html (Accessed March 24, 2025).
2. #Envision2030 Goal 6: Clean Water and Sanitation | United Nations Enable. Available at: https://www.un.org/development/desa/disabilities/envision2030-goal6.html (Accessed August 29, 2022).
3. Untitled Page. Available at: http://icds-wcd.nic.in/icds.aspx (Accessed August 29, 2022).
4. Condition of government schools in India. Our education system. Available at: http://oureducationsystem.weebly.com/condition-of-government-schools-in-india.html (Accessed December 14, 2020).
5. Maithly B, Saxena V. Adolescent’s educational Status and reasons for dropout from the school. Indian J Community Med. (2008) 33(2):127–8. doi: 10.4103/0970-0218.40885
6. Ben Amor Y, Dowden J, Borh KJ, Castro E, Goel N. The chronic absenteeism assessment project: using biometrics to evaluate the magnitude of and reasons for student chronic absenteeism in rural India. Int J Educ Dev. (2020) 72:102140. doi: 10.1016/j.ijedudev.2019.102140
7. WHO. Drinking water, sanitation and hygiene in schools. WHO. Available at: http://www.who.int/water_sanitation_health/publications/jmp-wash-in-schools/en/ (Accessed April 23, 2021).
8. Nutrition and Health Education | Department of Women and Child Development. Available at: https://wcd.odisha.gov.in/ICDS/nutrition-and-health-education (Accessed April 15, 2025).
9. School Education | Government of India, Ministry of Education. Available at: https://www.education.gov.in/mid-day-meal (Accessed April 15, 2025).
10. Supplementary Nutrition Programme | Department of Women and Child Development. Available at: https://wcd.odisha.gov.in/ICDS/supplementary-nutrition-programme (Accessed April 15, 2025).
11. Park K. Park's text Book of Preventive and Social Medicine. 25th ed. Jabalpur, India: Banarsidas Bhanot (2019).
12. India - Census of India 2011 - Administrative Atlas - Odisha - Volume I. Available at: https://censusindia.gov.in/nada/index.php/catalog/41 (Accessed March 25, 2025).
13. jmp-wash-in-schools-en.pdf. Available at: https://www.who.int/water_sanitation_health/publications/jmp-wash-in-schools-en.pdf (Accessed April 26, 2021).
14. Village Health Sanitation & Nutrition Committee: National Health Mission. Available at: https://www.nhm.gov.in/index1.php?lang=1&level=1&sublinkid=149&lid=225 (Accessed August 3, 2023).
Keywords: Anganwadi centers, water, sanitation, hygiene, preschools
Citation: Behera BK, Patro BK, Taywade M and Sahoo MC (2025) WASH improvement challenges in preschools in Eastern India. Front. Environ. Health 4:1573048. doi: 10.3389/fenvh.2025.1573048
Received: 8 February 2025; Accepted: 13 May 2025;
Published: 29 May 2025.
Edited by:
Gabriela Mustata Wilson, University of Louisiana at Lafayette, United StatesReviewed by:
Medani Bhandari, Akamai University, United StatesEthel Mkandawire, University of Zambia, Zambia
Copyright: © 2025 Behera, Patro, Taywade and Sahoo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Binod Kumar Behera, Y21mbV9iaW5vZGJAYWlpbXNiaHViYW5lc3dhci5lZHUuaW4=; Manish Taywade, Y21mbV9tYW5pc2hAYWlpbXNiaHViYW5lc3dhci5lZHUuaW4=