 Almudena Zapatero1Teresa Alonso-Gordoa2Alfredo Rodríguez Antolín3
Almudena Zapatero1Teresa Alonso-Gordoa2Alfredo Rodríguez Antolín3 Felipe Couñago4,5Noelia Sanmamed6Mario Domínguez Esteban7Marta López Valcárcel8Ray Manneh9Ángel Borque-Fernando10
Felipe Couñago4,5Noelia Sanmamed6Mario Domínguez Esteban7Marta López Valcárcel8Ray Manneh9Ángel Borque-Fernando10 Nuria Sala González11
Nuria Sala González11 Pablo Maroto12*
Pablo Maroto12*- 1Radiation Oncology Department, Health Research Institute, Hospital Universitario de La Princesa, Madrid, Spain
- 2Medical Oncology Department, Ramón y Cajal University Hospital, Madrid, Spain
- 3Urology Service, Hospital Universitario 12 de Octubre, Madrid, Spain
- 4GenesisCare Radiation Oncology Department, San Francisco de Asís University Hospital and Vithas La Milagrosa University Hospital, Madrid, Spain
- 5Department of Medicine, Faculty of Medicine, Health and Sport Sciences, Universidad Europea de Madrid, Madrid, Spain
- 6Radiation Oncology Department, Clínico San Carlos Hospital, Madrid, Spain
- 7Urology Service, Marqués de Valdecilla University Hospital, Santander, Spain
- 8Radiation Oncology Department, Puerta de Hierro Majadahonda University Hospital, Madrid, Spain
- 9Society of Oncology and Hematology of Cesar, Valledupar, Colombia
- 10Urology Service, Miguel Servet University Hospital, IIS-Aragón, Zaragoza, Spain
- 11Medical Oncology Service, Catalan Institute of Oncology, Josep Trueta Hospital, Girona, Spain
- 12Medical Oncology Service, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
This article aims to critically evaluate the evidence for triplet therapy consisting of androgen deprivation therapy (ADT), docetaxel and a second-generation androgen receptor pathway inhibitor ([ARPI]; abiraterone, enzalutamide, darolutamide or apalutamide) in patients with metastatic hormone-sensitive prostate cancer (mHSPC), and what this evidence reveals regarding the use of these treatments in clinical practice. A search of PubMed, Medline, Embase, Cochrane, Scopus and Web of Science was conducted in April 2024 to identify relevant prospective and retrospective observational trials, randomized controlled trials (RCTs) and meta-analyses. The search identified 52 relevant articles: six full articles and 31 abstracts based on three RCTs, one observational study and 14 meta-analyses. Abiraterone- or darolutamide-containing triplet therapy was significantly better than ADT + docetaxel for improving overall survival in all study populations, particularly subgroups with high-volume and/or synchronous disease. The tolerability of ADT + docetaxel and triplet therapy were similar with most adverse events related to docetaxel. There were no data comparing triplet therapy with ADT + ARPI doublet therapy. Triplet therapy appears to be the most effective first-line regimen for men with mHSPC, good performance status and high-volume and synchronous metastases. Darolutamide-based triplet therapy may also be of benefit in other patients with high- or low-risk disease. Careful consideration of the risks and benefits are required to determine which patients can be spared from receiving docetaxel and rather be treated with alternative regimens.
1 Introduction
It is estimated that 1.5 million men were diagnosed with prostate cancer in 2022 (1), and the global incidence is estimated to almost double in the next 5 years with changing demographic trends (2). Prostate cancer is the fourth most common cancer and the eighth leading cause of cancer deaths (3). Approximately 10%–15% of men with prostate cancer have metastatic hormone-sensitive prostate cancer (mHSPC) (4).
Over the past 10–15 years, the systemic treatment of mHSPC has been evolving from treatment with androgen deprivation therapy (ADT) alone, to doublet therapy consisting of ADT + docetaxel or ADT + a second-generation androgen receptor pathway inhibitor (ARPI), and more recently to triplet therapy with ADT + second-generation ARPI + docetaxel (5). Both European and American guidelines now include triplet therapy as first-line recommendations for selected patients with mHSPC (6-8).
The aim of the current article is to critically evaluate the evidence for triplet therapy in mHSPC, and what this evidence tells us about how to use triplet therapy in clinical practice, focusing on identifying the optimal patient characteristics for this treatment alternative.
2 Materials and methods
We conducted a literature search of PubMed, Medline, Embase, Cochrane, Scopus and Web of Science on 17 April 2024 to identify potentially relevant studies. The search strategy used a range of MeSH terms designed to identify studies in which ADT, ARPIs and docetaxel were all used in patients with mHSPC (see the Supplementary Material for full details of search strategies). All clinical trial types were considered for inclusion (observational and randomized controlled trials [RCTs]; prospective and retrospective), but only English-language articles were included. Additional articles were identified based on the authors’ experience in the area and a number of articles were added at the suggestion of the peer reviewers. Reviews, editorials, news items, case reports and correspondence were excluded, but bibliographies were reviewed for potentially relevant data. While priority was given to articles published in peer-reviewed journals, conference abstracts were considered for inclusion if they presented information that may help to clarify treatment decisions. No date limits were set, but only conference abstracts published since January 2021 were reviewed for potential inclusion.
3 Results
Our search identified 483 articles, which were investigated for inclusion. Of these, 95 were considered potentially relevant and 52 were considered relevant (Figure 1). Three major RCTs (ARASENS, ENZAMET and PEACE-1) collectively generated seven clinical research articles (9-14), 31 abstracts (15-45) and one congress highlight with abstract (46). We also identified one observational study (47) and 14 meta-analyses (48-61).
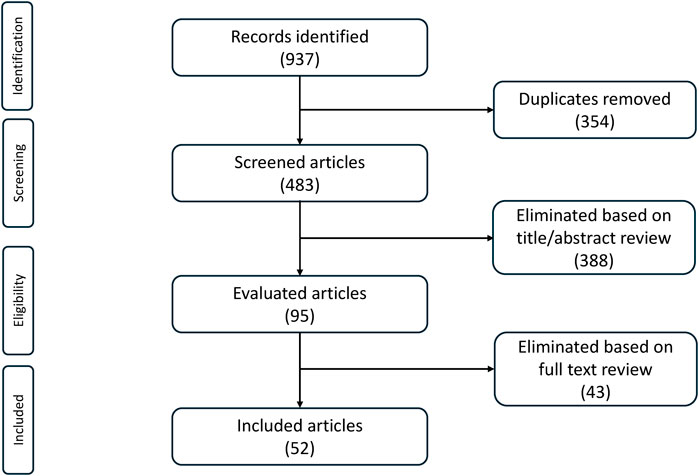
Figure 1. Article identification and inclusion.
3.1 Randomized controlled trials
3.1.1 Design
Of the three RCTs that comprised most of the articles in our search, only the ARASENS study set out to compare triplet therapy and doublet therapy from the start (12). The PEACE-1 and ENZAMET studies began using ADT alone (as the standard of care [SOC]) for background therapy but later included ADT + docetaxel as an option once this combination became the SOC (11, 13, 14).
Patient inclusion/eligibility criteria were similar but the studies had different designs (Table 1). ARASENS had a straightforward randomized, double-blind, placebo-controlled design, with two treatment arms; patients in both the active treatment group and control group received ADT + docetaxel (12), but one received darolutamide and the other placebo, i.e., this was a comparison of doublet therapy with ADT + docetaxel versus triplet therapy.
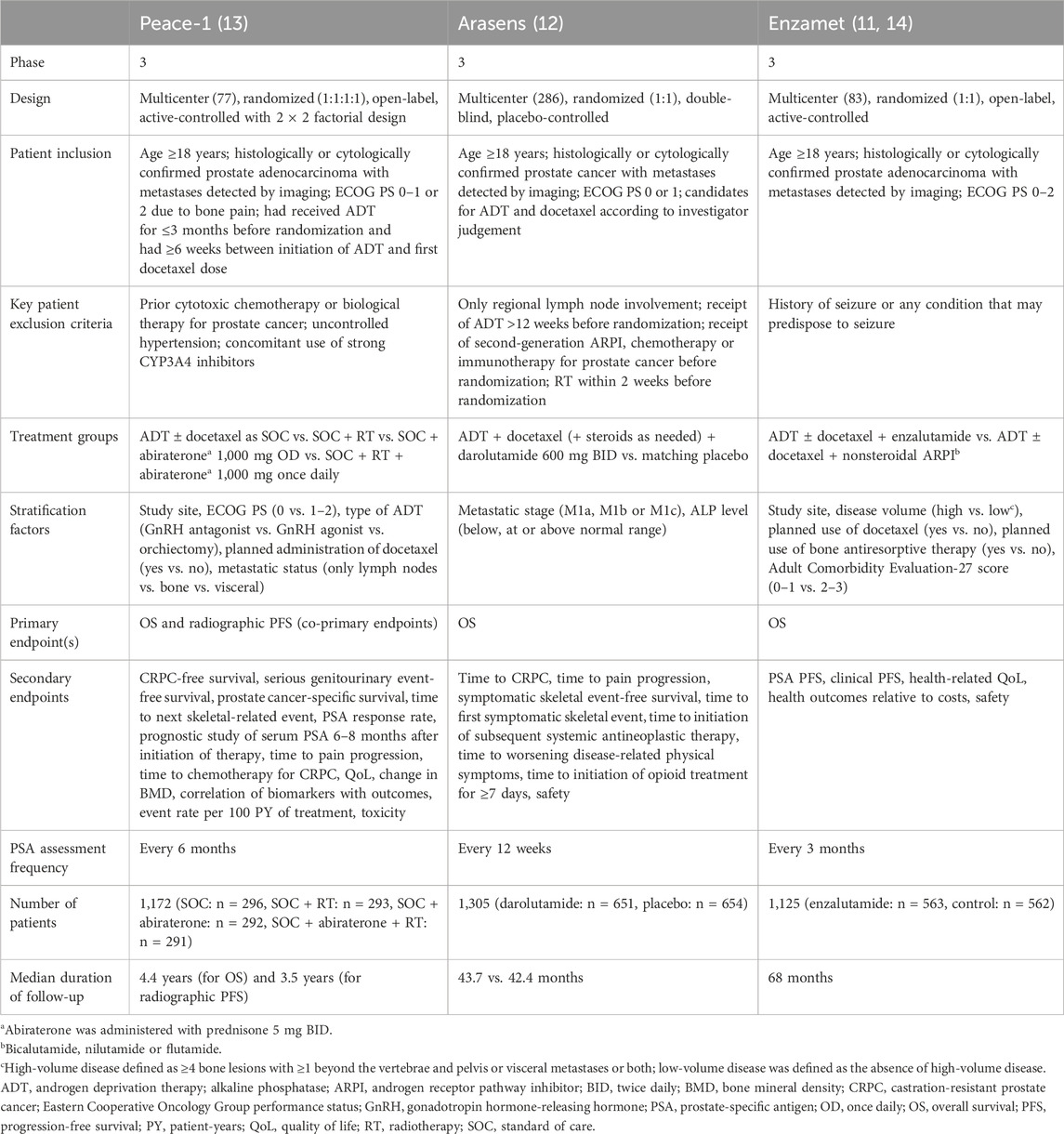
Table 1. Study designs of the PEACE-1, ARASENS and ENZAMET studies.
PEACE-1 was open-label and included four treatment groups using a 2 × 2 factorial design: 1) SOC alone; 2) SOC + radiotherapy; 3) SOC + abiraterone (and prednisone); and 4) SOC + abiraterone + radiotherapy (13). At the start of the study, SOC was ADT, but a protocol modification allowed physicians to start using ADT + docetaxel as SOC. Therefore, not all patients received docetaxel as SOC; of the 583 patients assigned to abiraterone (with or without radiotherapy), 355 (60.9%) received the triplet regimen of ADT + docetaxel + abiraterone.
ENZAMET was also open-label, with patients randomized to SOC + enzalutamide or SOC + a first-generation nonsteroidal ARPI (bicalutamide, flutamide or nilutamide) (11, 14). After enrolment of the first 88 patients, investigators were given the option to add open-label docetaxel to ADT as SOC. As a result, some of the patients (n = 483; 43%) received triplet therapy, of whom 243 received enzalutamide and 240 received a nonsteroidal ARPI. The rest of the patients in this study (n = 642) received doublet therapy with either enzalutamide + SOC or a nonsteroidal ARPI + SOC. Therefore, while patients in the ENZAMET study received doublet or triplet therapy, the study was not designed to compare outcomes in these two groups; rather, it was designed to compare outcomes between patients receiving enzalutamide and those receiving a first-generation ARPI. Moreover, patients receiving doublet therapy in this study received ADT with either enzalutamide or nonsteroidal ARPI; none received ADT + docetaxel.
All three studies had overall survival (OS) as a primary endpoint (11-13), but the PEACE-1 study had a co-primary endpoint of radiographic progression-free survival (PFS) (13).
Regarding patient characteristics, the population of the ARASENS trial had high-risk disease (78.2% Gleason score ≥8, 86.1% synchronous disease and 77.0% high-volume disease) (12, 40). All patients included in the PEACE-1 trial had synchronous disease and 57%–65% also had high-burden disease, so therefore were also at high risk overall (13). In ENZAMET, 60.6% of patients had synchronous disease, 53.5% had high-volume disease and 57%–60% had a Gleason score ≥8; 61% of patients with high-volume disease received docetaxel versus 27% of low-volume disease patients (11).
3.1.2 Results–survival
In all three studies, the treatment groups that included a next-generation ARPI had significantly better OS than the groups without this therapy (11-14).
In ARASENS, the only study specifically designed to compare doublet and triplet therapy as a predefined objective, triplet therapy containing darolutamide reduced the risk of death by 32.5% compared with ADT + docetaxel (hazard ratio [HR] 0.68, 95% confidence interval [CI] 0.57–0.80; p < 0.001; Table 2), even though 76% of patients in the doublet therapy group received subsequent systemic therapies (12). Triplet therapy was also associated with a significantly reduced risk of most secondary endpoints including time to castration-resistant prostate cancer (CRPC; HR 0.36, 95% CI 0.30–0.42; p < 0.001; Table 2), time to pain progression (HR 0.79, 95% CI 0.66–0.95; p = 0.01; Table 2), symptomatic skeletal event-free survival (HR 0.61, 95% CI 0.52–0.72; p < 0.001), time to first symptomatic skeletal event (HR 0.71, 95% CI 0.54–0.94; p = 0.02), and time to initiation of subsequent antineoplastic therapy (HR 0.39, 95% CI 0.33–0.46; p < 0.001). There was no significant difference between triplet and ADT + docetaxel doublet therapy in the time to worsening of disease-related symptoms (12). Median time to initiation of opioid use for ≥7 days was not reached in either group, but there was a trend towards earlier initiation of opioids in the triplet versus the doublet therapy group (HR 0.69, 95% CI 0.52–0.91).
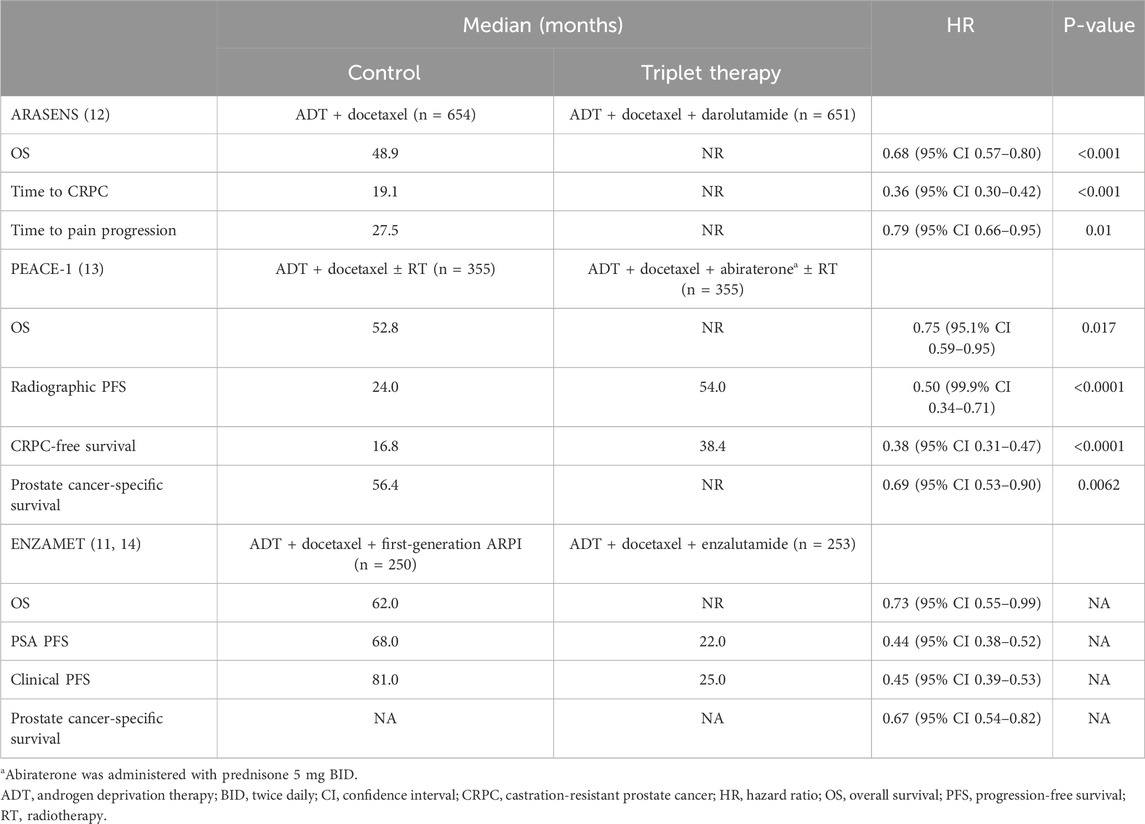
Table 2. Primary and selected secondary endpoint results of the PEACE-1, ARASENS and ENZAMET studies.
ENZAMET, which compared enzalutamide with first-generation ARPIs in combination with ADT ± docetaxel, found that the enzalutamide-containing regimen reduced the risk of death by 30% (HR 0.70, 95% CI 0.58–0.84; p < 0.0001) in the overall study cohort at final analysis (14). Enzalutamide-containing treatment was also associated with a significantly reduced risk of most secondary endpoints including time to prostate-specific antigen (PSA) progression (HR 0.44, 95% CI 0.38–0.52), time to clinical progression (HR 0.45, 95% CI 0.39–0.53), and prostate cancer-specific survival (HR 0.67, 95% CI 0.54–0.82) (14). However, in a pre-specified subgroup analysis of patients with early planned use of docetaxel (the triplet therapy group), the difference in OS between the enzalutamide group and control group did not reach statistical significance (HR 0.82, 95% CI 0.63–1.06). On the one hand, the use of docetaxel was at the investigator’s discretion, and patients who were selected for triplet therapy in this study had worse prognostic features than those who received doublet therapy, specifically a higher proportion of patients receiving triplet therapy had synchronous and/or high-volume disease. On the other hand, in the high-risk subgroup (patients with synchronous high-volume disease), older patients and those with comorbidities were less likely to receive docetaxel (14). A pre-specified subgroup analysis showed that triplet therapy containing enzalutamide significantly improved OS in patients with synchronous metastases compared with triplet therapy containing a first-generation ARPI, but not in those with metachronous disease (Figure 2) (14).
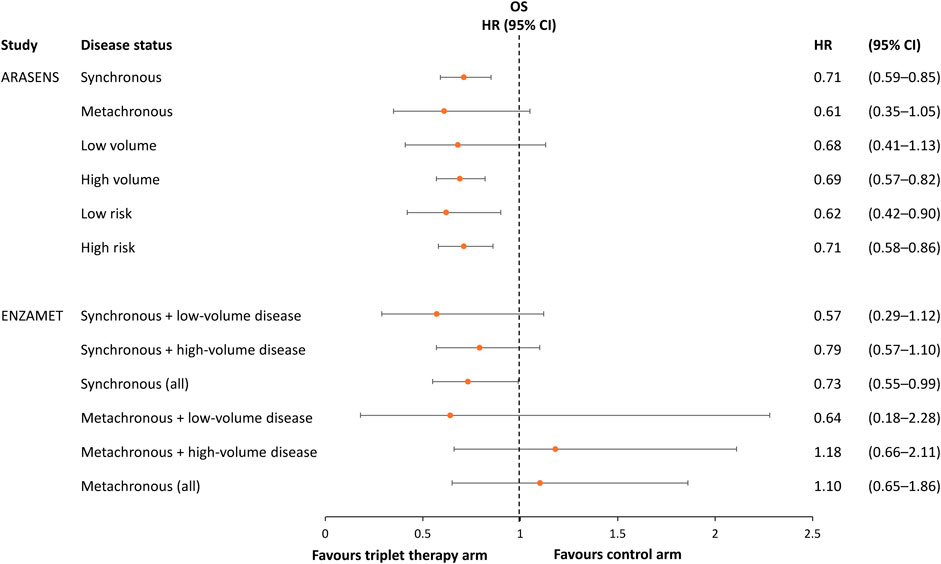
Figure 2. Hazard ratio and 95% confidence intervals for overall survival in subgroups of patients in the ARASENS and ENZAMET studies, stratified by metastatic status/volume and/or disease risk (9, 12, 14).
The subgroup findings from ENZAMET are consistent with results in the ARASENS study, in which the effect of triplet versus ADT + docetaxel doublet therapy on OS remained significant in the group with synchronous metastases but not those with metachronous metastases (9). In ARASENS, triplet therapy significantly improved OS in patients with high-volume disease (using the definition from the CHAARTED study, i.e., visceral metastases and/or ≥4 bone metastases with ≥1 beyond the vertebral column and pelvis (62)) and in patients with low- or high-risk disease (high-risk defined as two of the following criteria: Gleason score ≥8, ≥3 bone metastases and presence of measurable visceral metastasis (63)), but not those with low-volume disease (Figure 2) (9).
In the PEACE-1 study, 60.5% of patients received docetaxel as SOC, so the results in this subgroup allowed a comparison of triplet therapy with ADT + abiraterone + docetaxel (±radiotherapy; n = 355) and doublet therapy with ADT + docetaxel (±radiotherapy; n = 355) (13). Triplet therapy significantly improved the two co-primary endpoints of OS and radiographic PFS compared with ADT + docetaxel. The adjusted HR for OS was 0.75 (95.1% CI 0.59–0.95; p = 0.017) and the adjusted HR for radiographic PFS was 0.50 (99.9% CI 0.34–0.71; p < 0.0001).
Secondary endpoints of CRPC-free survival and prostate cancer-specific survival were also significantly better in the triplet than doublet therapy groups, with median CRPC-free survival of 3.21 versus 1.45 years in the triplet versus ADT + docetaxel doublet therapy groups, respectively (HR 0.38, 95% CI 0.31–0.47; p < 0.0001). Median prostate cancer-specific survival was not reached in the triplet therapy group but was 4.72 years in the doublet therapy group (HR 0.69, 95% CI 0.53–0.90; p = 0.0062) (13).
Consistent with the results of ARASENS, triplet therapy in PEACE-1 was associated with a significant improvement in OS in the subgroup of patients with high-volume metastatic disease but not in those with low-volume disease (Figure 3) (13). However, the other co-primary endpoint of radiographic PFS showed a significant improvement with triplet versus ADT + docetaxel doublet therapy in patients with low- or high-volume metastatic disease, with an HR of 0.58 (99.9% CI 0.29–1.15; p = 0.0061) in the low-volume group and 0.47 (99.9% CI 0.30–0.72; p < 0.0001) in the high-volume group (13).
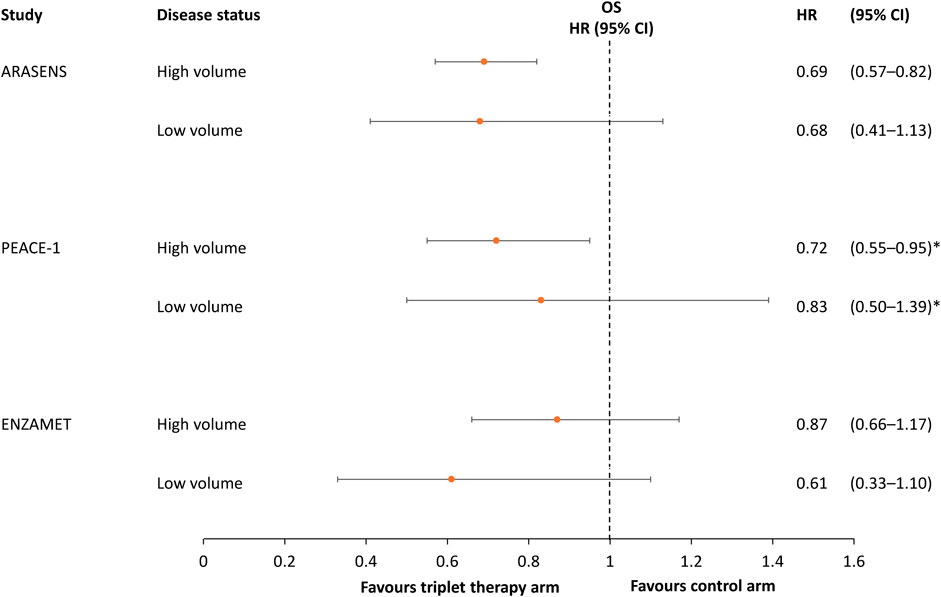
Figure 3. Hazard ratio and 95% confidence intervals for overall survival in the ARASENS, PEACE-1 and ENZAMET studies, stratified by metastatic volume (12, 13, 14). *95.1% CI.
Overall, triplet therapy regimens demonstrated superior survival benefits in the key trials versus doublet therapy in terms of radiographic PFS, time to CRPC, pain progression and remaining free from skeletal events, and the need for subsequent antineoplastic therapy.
3.1.3 Results–demographic subgroups
The preliminary results of a PEACE-1 subanalysis suggested that the magnitude of the benefit of adding abiraterone to SOC decreased with age (44). However, the magnitude of the improvement in radiographic PFS with triplet versus ADT + docetaxel doublet therapy was similar in men aged ≥70 years (HR 0.55, 95% CI 0.29–1.04) and those aged <70 years (HR 0.5, 95% CI 0.33–0.78), whereas younger men tended to derive a greater OS benefit (HR 0.71, 95% CI 0.52–0.95) than men aged ≥70 years (HR 0.80, 95% CI 0.53–1.2) (44). This was not the case in the ENZAMET trial, in which patients aged <70 and ≥70 years both derived a similar benefit from triplet therapy (43). The magnitude of the OS benefit associated with enzalutamide-containing triplet therapy relative to a nonsteroidal antiandrogen-containing triplet therapy in these age subgroups did not reach statistical significance (43). Both the PEACE-1 and ENZAMET analyses in elderly patients have been presented at conferences but data have not yet been published in full.
Subgroup analysis of the ARASENS data showed that the benefits of triplet versus ADT + docetaxel are directionally consistent in all age groups and ethnic/geographic/racial groups (12), including Chinese patients (56), North American patients (20), and Black/African-American patients (20, 21). Ongoing trials such as the PANTHER study are evaluating the effect of the combination of apalutamide + abiraterone + prednisone in clinical efficacy in Black men with mCRPC who are typically under-represented in clinical trials (64). Interim results indicate that Black participants had greater radiographic PFS, time to PSA progression, and overall survival than White participants (64). ARACOG is an ongoing, prospective, randomized, open-label phase II study comparing cognitive outcomes between men with metastatic and non-metastatic CRPC or mHSPC in the United States (65). Patients will be randomized (1:1) to receive treatment with enzalutamide 160 mg orally daily or darolutamide 600 mg orally twice daily, in combination with standard LHRH agonist-based treatment. Cognitive assessments will be to assess cognitive function and impairment (65).
3.1.4 Results–patient-reported outcomes
To date, only the ARASENS study has reported patient-reported outcomes (PROs) data and only as conference abstracts (15, 18). These data suggest that the addition of an ARPI does not negatively impact on patient quality of life, with similar quality of life in the triplet and ARPI + docetaxel doublet therapy arms (15, 18).
3.1.5 Results–toxicity
In the ARASENS study, the overall incidences of adverse events (AEs), serious AEs, grade ≥3 AEs and fatal AEs were similar in patients receiving ADT + docetaxel doublet versus triplet therapy; 98.5% and 99.5% of patients in these groups, respectively, developed any AEs, 42.3% and 44.8% experienced serious AEs, 63.5% and 66.1% had grade 3 or 4 AEs, and 4.0% and 4.1% died as a result of AEs (12). The highest incidence of AEs was seen with docetaxel and the most common AEs were those related to docetaxel in both groups, i.e., alopecia, fatigue, anemia and neutropenia (which included the preferred terms of leukopenia, neutropenia, decreased neutrophil count and decreased white blood cell count). Neutropenia occurred in 38.8% of patients in the doublet therapy arm and 39.3% in the triplet therapy arm, alopecia in 40.6% and 40.5%, respectively, fatigue in 32.9% and 33.1%, respectively, and anemia in 25.1% and 27.8%, respectively. AEs that occurred at a higher incidence in the group receiving darolutamide versus placebo were rash (16.6% vs. 13.5%) and hypertension (13.7% vs. 9.2%), although the rate of these events was similar in the two groups when adjusted for exposure time (rash: 6.2 vs. 7.3 per 100 patient-years [PY], respectively; hypertension: 4.9 per 100 PY in both groups) (12). AEs led to treatment discontinuation in 13.5% of patients in the darolutamide group and 10.6% of patients in the placebo group.
In the PEACE-1 study, 100% of patients receiving abiraterone-containing triplet therapy and 100% receiving ADT + docetaxel doublet therapy developed an AE of any severity, 63% versus 52% of patients who received triplet versus doublet therapy developed at least one grade ≥3 AE, and 2% versus 1%, respectively, developed a fatal AE (13). However, the incidence of severe AEs per 100 PY of treatment was 49 in the group receiving triplet therapy with abiraterone versus 55 in the group receiving doublet therapy. Abiraterone was stopped because of toxicity in 29 patients (21.0%) receiving triplet therapy and in one patient (<1.0%) receiving doublet therapy. AEs occurring at a higher incidence in the triplet versus ADT + docetaxel doublet arms of the PEACE-1 study, respectively, were hypertension (22% vs. 13%) and hepatotoxicity with elevated aminotransferase levels (6% vs. 1%) (13). Grade ≥3 neutropenia occurred at a similar rate in patients receiving triplet therapy and those receiving ADT + docetaxel (10% and 9%, respectively).
In the ENZAMET study, the overall incidence of AEs was similar in patients receiving enzalutamide versus a first-generation ARPI as part of triple therapy, but more patients in the first-generation ARPI group had grade 1–2 AEs (51% vs. 31%) and more patients in the enzalutamide group had grade 3 AEs (58% vs. 37%) (14). The most common grade 3–4 AEs were febrile neutropenia during docetaxel, which developed in 6% of patients in both treatment groups, fatigue (occurring in 1% of the control group vs. 5% of the enzalutamide group) and hypertension (occurring in 6% of the control group vs. 10% of the enzalutamide group) (14). Deaths due to serious AEs occurred in 10 patients (2%) in the control group and 13 patients (2%) in the enzalutamide group; no deaths were considered to be caused by enzalutamide.
It is expected that triplet therapy regimes would precipitate more AEs than doublet regimens. Overall, AE occurrence has been consistent among the three main RCTs and no new safety concerns have been identified.
3.2 Meta-analyses
Of the 14 meta-analyses identified, five compared triplet therapy with doublet therapy based on drug class groupings (48, 50, 56, 58, 59), and 11 used network meta-analysis (NMA) to compare regimens by individual ARPI (49, 51, 52, 53, 54, 55, 56, 57, 59, 60, 61).
3.2.1 Survival outcomes in meta-analyses
The five meta-analyses that compared triplet with ADT + docetaxel doublet therapy reported a consistent overall improvement in OS with triplet therapy of about 25% (Table 3) (48, 50, 56, 58, 59).
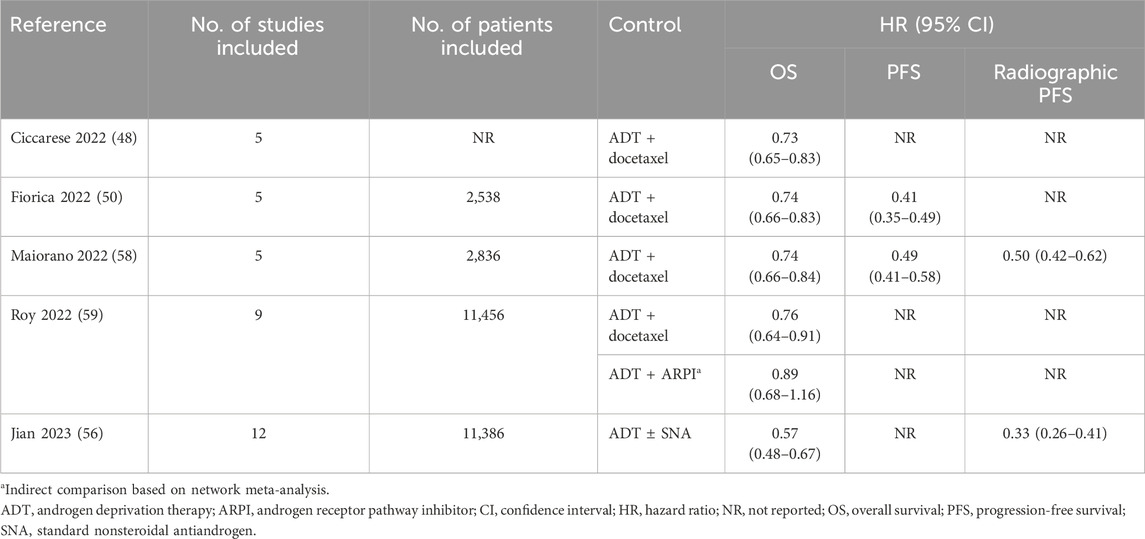
Table 3. Effect of triplet therapy versus control on survival endpoints in meta-analyses.
3.2.2 Survival outcomes in network meta-analyses
The 11 NMAs included between seven and 28 studies of triplet and doublet combinations conducted in between 5,804 and 12,298 patients (49, 51, 52, 53, 54, 55, 56, 57, 59, 60, 61). Because the NMAs included doublet therapy studies, the analyses also included apalutamide, which has not been studied as part of triplet therapy in RCTs. The survival analyses showed that darolutamide triplet therapy was consistently associated with a significant improvement in OS compared with ADT + docetaxel (Supplementary Figure S1A) (49, 52, 54, 55, 60). Abiraterone-containing triplet therapy was associated with a significant improvement in OS compared with ADT + docetaxel in three out of four NMAs analyzing this association (Supplementary Figure S1B) (49, 52, 55, 60), but neither enzalutamide- nor apalutamide-containing triplet regimens were associated with a significant improvement in OS compared with ADT + docetaxel (Supplementary Figures S1C, S1D) (49, 52, 54, 60, 61). The NMAs also evaluated indirect comparisons between triplet therapy and ADT + ARPI doublet therapy. In all cases, triplet therapy was not significantly more effective than ADT + ARPI doublet at improving OS (Supplementary Figures S2A–C) (53, 54, 55, 57, 60, 61), and in one case, abiraterone + ADT doublet therapy was found to be significantly better than abiraterone-based triplet therapy (Supplementary Figure S2C) (53).
The NMA data regarding PFS were generally similar to the OS data, with triplet therapy containing abiraterone or darolutamide being significantly better than SOC (ADT, ADT + ARPI or ADT + docetaxel) in one NMA (Supplementary Table S1) (53). Abiraterone-containing triplet therapy was significantly superior to ADT + docetaxel in two NMAs (55, 60). Enzalutamide-containing triplet therapy was superior to ADT + docetaxel in one NMA (60) but not in another (61). In most comparisons of triplet therapy with ARPI + ADT doublets, there was no significant differences in PFS (Supplementary Table S1), but Wang and colleagues found a significant improvement in PFS with abiraterone- or enzalutamide-containing triplet therapy compared with a doublet regimen of abiraterone + ADT (60). Triplet combinations were significantly superior to ADT + docetaxel for improving radiographic PFS and time to CRPC in an analysis by Jian and colleagues (Supplementary Table S2) (52).
When the data were analyzed by subgroup, none were significant in patients with low-volume disease (Supplementary Table S3), but some of the NMA comparisons of OS were statistically significant in patients with high-volume disease (Supplementary Table S4). With regard to PFS, none of the comparisons of abiraterone triplet therapy with any comparator (ADT alone, ADT + docetaxel or ADT + ARPI) were statistically significant in the low-volume disease groups (Supplementary Table S5) (55), whereas abiraterone was associated with a significant improvement in PFS in patients with high-volume disease compared with ADT alone (51, 54, 55), ADT + docetaxel (55), and ADT + apalutamide (55), but not compared with ADT + enzalutamide (55).
In the subgroup of patients with synchronous disease, significant improvements in OS were seen with triplet therapy compared with ADT alone or ADT + docetaxel, but not with ADT + ARPI (Supplementary Table S6) (55). No significant improvement was seen with triplet therapy vs. any comparator in patients with metachronous disease (Supplementary Table S6) (55).
3.2.3 Toxicity
Eight meta-analyses evaluated the effects of triplet therapy on the incidence of AEs (49, 50, 52, 54, 56, 58, 60, 61), but the comparisons were mostly with ADT alone (54, 60, 61), ADT ± standard nonsteroidal antiandrogen (56) or docetaxel alone (49). The meta-analysis by Jian and colleagues was the only one to specifically compare AE rates during individual triplet regimens (abiraterone + ADT + docetaxel, and darolutamide + ADT + docetaxel) versus doublet therapy (52). In this analysis, both abiraterone- and darolutamide-containing triplet therapy were associated with a higher risk of hypertension compared with ADT + docetaxel, but only abiraterone + ADT + docetaxel was associated with a higher risk of grade ≥3 AEs (Supplementary Figure S3) (52). The risks of neutropenia and febrile neutropenia were similar with triplet regimens and ADT + docetaxel (52).
Menges and colleagues evaluated the net clinical benefit of doublet and triplet regimens, as the number of deaths avoided per 1,000 patients compared with ADT alone, weighted by 0.18 for incident grade 1–2 AEs and by 0.53 for incident grade 3–4 AEs (54). In this analysis, the probability of having a net clinical benefit over 24 months compared with ADT alone was 63.3%–78.7% for ARPI + ADT doublet regimens and 20.0% for darolutamide + ADT + docetaxel, and over 5 years was 66.7%–83.2% with ARPI + ADT doublet regimens and 23.5% for darolutamide + ADT + docetaxel. A sensitivity analysis using lower preference weights for AEs increased the probabilities, but did not change the relative rankings (54). No analysis was conducted comparing the net clinical benefit of triplet therapy with that of ARPI + ADT doublet therapy.
AE results data for the meta-analyses were similar to those obtained for RCTs.
3.3 Observational studies
There is also real-world evidence to support the use of triplet therapy in mHSPC. Our search identified one observational study in patients who received abiraterone (n = 77), darolutamide (n = 17), apalutamide (n = 2) or enzalutamide (n = 1) in combination with docetaxel and ADT (47). All the patients who received triplet therapy experienced a 99% decrease in PSA levels, and a radiologic response or stable disease was confirmed in 88% of those receiving abiraterone-based triplet therapy and 75% of those receiving darolutamide-based triplet therapy. In the abiraterone group, mean time to progression or CRPC was 8.5 months, time to second-line therapy was 8 months and time to death was 14.7 months. Abiraterone and darolutamide were associated with a similar incidence of AEs of any grade (62.3% and 58.8%, respectively) and grade ≥3 (19.5% and 11.8%). The most common AEs occurring during triplet therapy were fatigue, polyneuropathy and dermatologic conditions.
4 Discussion
The available RCT data and meta-analyses indicate that triplet therapy is often associated with better clinical outcomes compared with ADT + docetaxel, particularly for patients with synchronous, high-volume metastatic disease (5). Of note, most of the patients enrolled in ARASENS and PEACE-1 were at higher risk than usual (12, 13). To date, there is no randomized evidence on whether systemic triplet therapy improves outcomes compared with doublet therapy with ADT + an ARPI.
In the RCTs that allowed direct comparison of triplet therapy with ADT + docetaxel doublet therapy (ARASENS and PEACE-1), triplet therapy increased OS in the overall study populations by 32.5% and 25%, respectively (12, 13), and in meta-analyses the increase in OS was about 25%, with the HR ranging from 0.73 to 0.76 (48, 50, 56, 58, 59). It is possible that the magnitude of the OS improvement in the meta-analyses would have been greater if they had not included the ENZAMET study, which did not directly compare triplet therapy with ADT + docetaxel doublet therapy.
Both the timing and volume of metastases are independent prognostic indicators in mHSPC (66), and these parameters influence the magnitude of the benefit of triplet and doublet therapy. The available data indicate that patients with high-volume metastatic burden derive a significant benefit from triplet therapy, particularly those with synchronous mHSPC, but the benefit is less clear in patients with a low metastatic burden. Research has shown that, in patients with low-volume prostate cancer, metachronous disease has a more ADT-responsive transcriptional profile than synchronous disease (67), which may explain the better survival outcomes during ARPI therapy among those with synchronous versus metachronous disease.
The importance of both high-volume and synchronous metastases as determinants of response to triplet therapy is reflected in the latest iterations of major guidelines. The NCCN® guidelines recommend triplet therapy (with abiraterone or darolutamide) or doublet ADT + ARPI therapy (with abiraterone, apalutamide or enzalutamide) as options for patients with high-volume synchronous metastases, high-volume metachronous metastases, or low-volume synchronous metastases, but recommend ADT + ARPI doublet therapy for patients with low-volume metachronous metastases (8). European Society for Medical Oncology (ESMO) guidelines recommend two triplet regimens as first-line therapy for mHSPC: abiraterone + ADT + docetaxel for fit men with synchronous (de novo) mHSPC (especially those with visceral or >3 bone metastases) or darolutamide + ADT + docetaxel for patients with synchronous or metachronous mHSPC (7). Similarly, other international guidelines recommend both triplet therapy (ADT + docetaxel + abiraterone or darolutamide) and doublet therapy (ADT + abiraterone) for patients with mHSPC (6). The only requirement for triplet therapy is that the patient is eligible to receive docetaxel (6). Further data are needed to determine whether triplet therapy may be superior to ADT + ARPI doublet therapy in patients with low-volume disease (e.g., younger patients with aggressive tumors or patients with high-risk disease) (68, 69).
ENZAMET (11) and PEACE-1 (13) did not include triplet therapy as a predefined treatment arm, and not all randomized patients in ENZAMET who received triplet therapy received a next-generation ARPI. Therefore, these studies were probably underpowered to detect significant differences among those who received triplet therapy regimens. Another potential confounder in the PEACE-1 study was that some patients also received radiotherapy to the primary tumor, and the data from the radiotherapy analysis have not yet been published. A preliminary analysis presented at the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting suggested that outcomes were better in men receiving ADT (±docetaxel) + ARPI with radiotherapy compared with those receiving ADT (±docetaxel) alone, but the analysis did not compare outcomes among radiotherapy recipients who did versus did not receive docetaxel, so it is not clear how the use of radiotherapy may affect the outcomes in the triplet therapy arm of this study (16). Adding radiotherapy to ADT (±docetaxel) did not improve outcomes compared with ADT (±docetaxel) alone. Interestingly, prostate radiotherapy was associated with a reduction in serious genitourinary events regardless of metastatic burden.
All patients in the clinical trials of triplet therapy had an Eastern Cooperative Oncology Group performance status (ECOG PS) ≤2 and a median patient age of about 67 years, so there are no data on the use of triplet therapy in patients with more compromised performance status. The ENZAMET and PEACE-1 studies included patients with ECOG PS of 2. In subgroup analyses from these studies, the benefit of triplet therapy with a next-generation ARPI (abiraterone in PEACE-1 or enzalutamide in ENZAMET) on the primary endpoints was similar in patients with ECOG PS 1–2 and those with ECOG PS 0 (13, 14).
Patient fitness is a consideration when making any treatment decision in cancer. Real-world data show that outcomes are maximized in patients who can complete six cycles of docetaxel (70), so patients who develop docetaxel-related toxicity may not derive the optimal benefit of triplet therapy. In the ARASENS study, 87.6% of patients receiving darolutamide and 85.5% of those receiving placebo were able to complete six cycles of docetaxel (12), while in ENZAMET 65% of patients receiving enzalutamide triplet therapy completed six cycle of docetaxel (11). The PEACE-1 study did not report the proportion of patients who completed six cycles of docetaxel as part of an abiraterone-containing triplet regimen, but did note that the median number of cycles completed was six (13). Similarly high rates of docetaxel completion (86.7%) were reported in the real-world observational study of triplet therapy in routine clinical practice (47).
There are limited data on the effects of triplet therapy on PROs. Preliminary PRO data from ARASENS have been presented as a conference abstract, and indicated that HRQoL was similar in the triplet and doublet therapy arms (15, 18).
Finally, it is worth noting that, despite guideline recommendations, intensified therapy appears to be underutilized in the United States and Europe, even among patients who are candidates for these strategies (71). Therefore, many patients who could benefit from triplet therapy may not be receiving it, and the reasons for underutilization are not clearly known. Further, there is a need to individualize treatments considering patient-dependent factors such as age, comorbidities, clinical factors (disease presentation, risk, and volume) and the kinetics of PSA response to therapies; and to develop and validate biomarkers. The authors of the ENZAMET trial noted that the choice of new hormonal therapy will be reliant on its availability and on the patient’s age and comorbidity profile (14).
To date, we do not know which patients benefit most from triplet therapy, nor do we know in whom docetaxel can be omitted, nor whether such triplet therapy is superior to ADT + ARPI (72). Currently, no single triplet regimen can be considered superior to another because they have not been directly compared in a clinical trial. Moreover, a key limitation of the available RCT data is that the comparison doublet therapy was ADT + docetaxel, which was subsequently superseded by ADT + ARPI as the preferred doublet regimen. There have been no direct comparisons of triplet therapy with a doublet regimen comprising ADT + ARPI.
The available NMAs using indirect comparisons suggest that there is a statistically significant benefit with triplet therapy versus ADT + ARPI in patients with high-volume metastases (53, 54, 55, 57, 60, 61). While the NMA results are interesting, it is important to remember that they have their limitations. First, NMAs are subject to heterogeneity and incoherence, depending on the quality and quantity of the data supporting each direct and indirect comparison (73). Indirect comparisons assume transitivity, i.e., that if A = B and B=C then A = C (74). In fact, even when identical treatments are used in different studies, the magnitude of the effect may differ if the study populations are not identical (74). Heterogeneity between studies can lead to incoherence between the direct and indirect comparisons, which can be significant (75). Finally, NMAs are affected by publication bias and potentially by selection bias. Notwithstanding these limitations, in the absence of direct comparisons, NMAs are the only method for undertaking comprehensive comparisons of multiple interventions, overcoming the limitations of pairwise meta-analysis (76). Therefore, they provide valuable comparative effectiveness estimates that can be used for treatment decision-making (76).
5 Conclusion
Based on available data, triplet therapy appears to be the most effective first-line treatment regimen for men with mHSPC who have high-volume metastatic burden, particularly those with synchronous mHSPC. In patients with low-volume metachronous mHSPC, doublet therapy with an ADT + ARPI may be the most appropriate choice. For other patients with high- or low-risk disease, a darolutamide-based triplet therapy regimen may also be of benefit. To date, there are a lack of data to compare triplet therapy with ADT + ARPI doublet therapy. Further evidence is required to identify prognostic and predictive factors, beyond disease volume and metastatic burden, to make therapeutic decisions, and also to identify patients who can be spared docetaxel, without compromising survival outcomes.
Author contributions
AZ: Conceptualization, Writing – review and editing. TA-G: Writing – review and editing, Conceptualization. AR: Conceptualization, Writing – review and editing. FC: Writing – review and editing, Conceptualization. NS: Conceptualization, Writing – review and editing. MD: Writing – review and editing, Conceptualization. ML: Conceptualization, Writing – review and editing. RM: Conceptualization, Writing – review and editing. ÁB-F: Writing – review and editing, Conceptualization. NS: Conceptualization, Writing – review and editing. PM: Supervision, Project administration, Writing – review and editing, Conceptualization, Funding acquisition.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The development of the manuscript and open access publishing fee has been funded by Bayer in accordance with the Good Publication Practice Guidelines (GPP-2022).
Acknowledgments
The authors would like to thank Catherine Rees who assisted in the preparation of the outline and first draft of the manuscript on behalf of Springer Health+. This medical writing assistance was funded by Bayer.
Conflict of interest
AZ has received speaker honoraria from Astellas-Pharma; travel expenses from Ipsen, Recordati, and Janssen; and research grants from Janssen. TA-G has received fees for speaker, consultancy, research and other non-financial support from IPSEN, Eli Lilly, Adacap, Pfizer, EISAI, Bayer, Johnson & Johnson, Astellas-Pharma, Roche and MSD. AR has received honoraria for his participation in training and consultancy sessions from Astellas-Pharma, AstraZeneca, Novartis, Bayer and Janssen. FC has received honoraria for participation in expert committees and conferences from Janssen, Astellas, IPSEN, Recordati, Boston Scientific, AstraZeneca and Bayer. NS has served on an advisory board for Astellas-Pharma, and received speaker honoraria from Astellas-Pharma, Janssen, and Bayer, and travel expenses from Ipsen and Recordati. MD has received honoraria for participation in expert committees and conferences from Janssen, Astellas, IPSEN, Bristol Myers Squibb, AAA, Boston Scientific, Intuitive, AstraZeneca and Bayer. ML has received speaker honoraria from Astellas-Pharma, Janssen, and Bayer. RM has served as a speaker, advisory board member and clinical researcher for Astellas, Amgen, Jannsen, Bayer, Pfizer, Novartis, BMS, MSD, Eli Lilly, Roche, Ipsen, Merck Serono and Adium. ÁB-F has participated in training sessions and has received consultancy fees from Asofarma, Astellas-Pharma, AstraZeneca, Bayer, GP Pharm, HealthMDx, Ipsen, Janssen, Lacer, MSD, Pharmalink and Recordati. NS has received research grants, honoraria, and other non-financial support from IPSEN, Pfizer, Bayer, BMS and MSD. PM has received speaker and consultancy fees, and other support such as logistical assistance from Astellas, Janssen, Bayer, MSD and Novartis.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/or.2025.1599292/full#supplementary-material
Abbreviations
ADT, androgen deprivation therapy (a GnRH agonist or GnRH antagonist or orchiectomy); AEs, adverse events; ALP, alkaline phosphatase; ARPI, androgen receptor pathway inhibitor; ASCO, American Society of Clinical Oncology; BID, twice daily; BMD, bone mineral density; CI, confidence interval; CRPC, castration-resistant prostate cancer; CYP, cytochrome P450; ECOG PS, Eastern Cooperative Oncology Group performance status; ESMO, European Society for Medical Oncology; GnRH, gonadotropin hormone-releasing hormone; HR, hazard ratio; mHSPC, metastatic hormone-sensitive prostate cancer; NA, not available; NMA, network meta-analysis; NR, not reported; OD, once daily; OS, overall survival; PFS, progression-free survival; PROs, patient-reported outcomes; PSA, prostate-specific antigen; PY, patient-year; QoL, quality of life; RCT, randomized controlled trial; RT, radiotherapy; SNA, standard nonsteroidal antiandrogen; SOC, standard of care.
References
1. International Agency for Research on Cancer. Cancer today data: prostate cancer. International Agency for Research on Cancer (2022). Available online at: https://gco.iarc.fr/today/en/dataviz/tables?mode=population&cancers=27 [Accessed February 28, 2024].
2. International Agency for Research on Cancer. Cancer tomorrow data: prostate cancer. Int Agency Res Cancer (2022). Available online at: https://gco.iarc.fr/tomorrow/en/dataviz/tables?cancers=27 [Accessed February 28, 2024].
3. International Agency for Research on Cancer. Global cancer observatory fact sheet. Prostate: Int Agency Res Cancer (2022). Available online at: https://gco.iarc.who.int/media/globocan/factsheets/cancers/27-prostate-fact-sheet.pdf [Accessed February 28, 2024].
4. de Velasco Oria de Rueda, G, Plata Bello, AC, Landeira, M, Mateo, M, Anguita, P, Pranzo, A, et al. Incidence, prevalence, and treatment patterns in metastatic hormone-sensitive prostate cancer in Spain: ECHOS study. Actas Urológicas Españolas (English Edition) (2022) 46(9):557–64. doi:10.1016/j.acuroe.2022.02.009
5. Hamid, AA, Sayegh, N, Tombal, B, Hussain, M, Sweeney, CJ, Graff, JN, et al. Metastatic hormone-sensitive prostate cancer: toward an era of adaptive and personalized treatment. Am Soc Clin Oncol Educ book. Am Soc Clin Oncol Annu Meet (2023) 43:e390166. doi:10.1200/EDBK_390166
6. Cornford, P, Tilki, D, van den Bergh, RCN, Briers, E, Eberli, D, De Meerleer, G, et al. EAU-EANM-ESTRO-ESUR-ISUP-SIOG guidelines on prostate cancer (2024). Available online at: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-EANM-ESTRO-ESUR-ISUP-SIOG-Guidelines-on-Prostate-Cancer-2024.pdf [Accessed May 13, 2024].
7. Fizazi, K, and Gillessen, S, ESMO Guidelines Committee Electronic address clinicalguidelines@esmo org. Updated treatment recommendations for prostate cancer from the ESMO clinical practice guideline considering treatment intensification and use of novel systemic agents. Ann Oncol (2023) 34(6):557–63. doi:10.1016/j.annonc.2023.02.015
8. National Comprehensive Cancer Network® (NCCN®). NCCN® clinical practice guidelines in oncology: prostate cancer. Version 3.2024: NCCN (2024). Available online at: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf [Accessed May 13, 2024].
9. Hussain, M, Tombal, B, Saad, F, Fizazi, K, Sternberg, CN, Crawford, ED, et al. Darolutamide plus androgen-deprivation therapy and docetaxel in metastatic hormone-sensitive prostate cancer by disease volume and risk subgroups in the phase III ARASENS trial. J Clin Oncol (2023) 41(20):3595–607. doi:10.1200/JCO.23.00041
10. Shore, ND, Hussain, M, Saad, F, Fizazi, K, Sternberg, CN, Crawford, D, et al. Efficacy and safety of darolutamide in combination with androgen-deprivation therapy and docetaxel in black patients from the randomized ARASENS trial. The Oncologist (2024) 29(3):235–43. doi:10.1093/oncolo/oyad254
11. Davis, ID, Martin, AJ, Stockler, MR, Begbie, S, Chi, KN, Chowdhury, S, et al. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med (2019) 381(2):121–31. Epub 2019/06/02. doi:10.1056/NEJMoa1903835
12. Smith, MR, Hussain, M, Saad, F, Fizazi, K, Sternberg, CN, Crawford, ED, et al. Darolutamide and survival in metastatic, hormone-sensitive prostate cancer. N Engl J Med (2022) 386(12):1132–42. Epub 2022/02/17. doi:10.1056/NEJMoa2119115
13. Fizazi, K, Foulon, S, Carles, J, Roubaud, G, McDermott, R, Fléchon, A, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. The Lancet (2022) 399(10336):1695–707. Epub 2022/04/08. doi:10.1016/S0140-6736(22)00367-1
14. Sweeney, CJ, Martin, AJ, Stockler, MR, Begbie, S, Cheung, L, Chi, KN, et al. Testosterone suppression plus enzalutamide versus testosterone suppression plus standard antiandrogen therapy for metastatic hormone-sensitive prostate cancer (ENZAMET): an international, open-label, randomised, phase 3 trial. Lancet Oncol (2023) 24(4):323–34. doi:10.1016/S1470-2045(23)00063-3
15. Bernard-Tessier, A, Cancel, M, Tombal, B, Roubaud, G, Carles Galceran, J, Flechon, A, et al. 1421P Effect of Abiraterone-Prednisone in Metastatic Castration-Sensitive Prostate Cancer (mCSPC) with Neuroendocrine and Very High-Risk Features in the PEACE-1 Trial [Congress Abstract]. Ann Oncol (2022) 33(Suppl. 7):S1194–S5. doi:10.1016/j.annonc.2022.07.1907
16. Bossi, A, Foulon, S, Maldonado, X, Sargos, P, McDermott, RS, Flechon, A, et al. Prostate Irradiation in Men with de novo, Low-Volume, Metastatic, Castration-Sensitive Prostate Cancer (mCSPC): results of PEACE-1, a Phase 3 Randomized Trial with a 2x2 Design. J Clin Oncol (2023) 41(17_Suppl. l):LBA5000. doi:10.1200/JCO.2023.41.17_suppl.LBA5000
17. Crawford, ED, Smith, MR, Tombal, B, Fizazi, K, Hussain, M, Sternberg, CN, et al. LBA01-07 OVERALL SAFETY AND INCIDENCES OF ADVERSE EVENTS BY TIME INTERVAL WITH DAROLUTAMIDE PLUS ANDROGEN-DEPRIVATION THERAPY AND DOCETAXEL IN THE PHASE 3 ARASENS TRIAL. J Urol (2022) 207(Suppl. 5):e1038. doi:10.1097/JU.0000000000002669.07
18. Fizazi, K, Bogemann, M, Smith, M, Hussain, M, Saad, F, Sternberg, CN, et al. Quality of Life and Patient-Relevant Endpoints with Darolutamide in the Phase 3 ARASENS Study [Congress Abstract]. Oncol Res Treat (2024) 47(Suppl. 1):79.
19. Francis, P, Matthew, SR, Maha, H, Fred, S, Karim, F, Cora, SN, et al. Overall Survival Following Treatment with Darolutamide Plus Androgen-Deprivation Therapy and Docetaxel for Metastatic Hormone-Sensitive Prostate Cancer: Primary Results from the Phase 3 Placebo-Controlled ARASENS Trial [Congress Abstract]. Asia Pac J Clin Oncol (2022) 18(Suppl. 1):76. doi:10.1111/ajco.13827
20. Hovey, E, Hussain, M, Tombal, B, Saad, F, Fizazi, K, Sternberg, C, et al. Darolutamide in Combination with Androgen-Deprivation Therapy and Docetaxel in Patients with Metastatic Hormone-Sensitive Prostate Cancer by Disease Volume and Risk in the Phase 3 ARASENS Study [Congress Abstract]. Asia Pac J Clin Oncol (2023) 19(Suppl. 2):64.
21. Hussain, M, Bogemann, M, Tombal, B, Saad, F, Fizazi, K, Sternberg, CN, et al. Efficacy and Safety of Darolutamide (DARO) in Combination with Androgen-Deprivation Therapy (ADT) and Docetaxel (DOC) by Disease Volume and Risk in the Phase 3 ARASENS Study [Congress Abstract]. Oncol Res Treat (2024) 47(Suppl. 1):80. doi:10.1159/000535363
22. Morgans, AK, Boegemann, M, Paracha, N, Grossman, J, Rodriguez Santamaria, F, Tyas, E, et al. Rate of hospitalization and length of hospital stay during and post docetaxel for darolutamide in metastatic hormone-sensitive prostate cancer using ARASENS. J Clin Oncol (2024) 42(4_Suppl. l):228. doi:10.1200/jco.2024.42.4_suppl.228
23. Fizazi, K, Smith, MR, Hussain, M, Saad, F, Sternberg, C, Crawford, ED, et al. 1360MO quality of life and patient-relevant endpoints with darolutamide in the phase III ARASENS study. Ann Oncol (2022) 33(Suppl. 7):S1162. doi:10.1016/j.annonc.2022.07.1492
24. Todenhofer, T, Smith, MR, Hussain, M, Saad, F, Fizazi, K, Sternberg, CN, et al. Overall Survival with Darolutamide Versus Placebo in Combination with Androgen-Deprivation Therapy and Docetaxel for Metastatic Hormone-Sensitive Prostate Cancer in the Phase 3 ARASENS Trial [Congress Abstract]. Oncol Res Treat (2022) 45(Suppl. 3):109. doi:10.1159/000521004
25. Fizazi, K, Maldonado, X, Foulon, S, Roubaud, G, McDermott, RS, Flechon, A, et al. A phase 3 trial with a 2x2 factorial design of abiraterone acetate plus prednisone and/or local radiotherapy in men with de novo metastatic castration-sensitive prostate cancer (mCSPC): first results of PEACE-1. J Clin Oncol (2021) 39(15_Suppl. l):5000. doi:10.1200/JCO.2021.39.15_suppl.5000
26. Gravis, MG, Maldonado, X, Roubaud, G, McDermott, RS, Flechon, A, Tombal, B, et al. 1361MO 8-Month PSA Strongly Predicts Outcomes of Men with Metastatic Castration-Sensitive Prostate Cancer in the PEACE-1 Phase III Trial [Congress Abstract]. Ann Oncol (2022) 33(Suppl. 7):S1162–S3. doi:10.1016/j.annonc.2022.07.1493
27. Roubaud, G, Kostine, M, McDermott, RS, Bernard-Tessier, A, Maldonado, X, Silva, M, et al. Bone mineral density in men with de novo metastatic castration-sensitive prostate cancer treated with or without abiraterone plus prednisone in the PEACE-1 phase 3 trial. J Clin Oncol (2022) 40(6_Suppl. l):19. doi:10.1200/JCO.2022.40.6_suppl.019
28. Kalebasty, AR, Hammerer, P, Tombal, B, Hussain, M, Saad, F, Fizazi, K, et al. Dosing, Safety, and Pharmacokinetics (PK) of Combination Therapy with Darolutamide (DARO), Androgen-Deprivation Therapy (ADT), and Docetaxel (DOC) in Patients with Metastatic Hormone-Sensitive Prostate Cancer (mHSPC) in the ARASENS Study [Congress Abstract]. Oncol Res Treat (2024) 47(Suppl. 1):80–1.
29. Parnis, F, Tombal, B, Hussain, M, Saad, F, Fizazi, K, Sternberg, CN, et al. 173P Clinical Outcomes in Stratification Subgroups in the ARASENS Study in Metastatic Hormone-Sensitive Prostate Cancer (mHSPC) [Congress Abstract]. Ann Oncol (2022) 33(Suppl. 9):S1501–S2. doi:10.1016/j.annonc.2022.10.210
30. Rezazadeh, A, Tombal, BF, Hussain, MHA, Saad, F, Fizazi, K, Sternberg, CN, et al. Dosing, safety, and pharmacokinetics (PK) of combination therapy with darolutamide (DARO), androgen-deprivation therapy (ADT), and docetaxel (DOC) in patients with metastatic hormone-sensitive prostate cancer (mHSPC) in the ARASENS study. J Clin Oncol (2023) 41(6_Suppl. l):148. doi:10.1200/jco.2023.41.6_suppl.148
31. Saad, F, Hussain, M, Tombal, B, Fizazi, K, Sternberg, CN, Crawford, ED, et al. 1784P Prostate-specific antigen (PSA) outcomes with darolutamide (DARO): androgen-Deprivation therapy (ADT) and docetaxel (DOC) in patients (pts) with high- and low-volume metastatic hormone-sensitive prostate cancer (mHSPC) in ARASENS. Ann Oncol (2023) 34(Suppl. 2):S964. doi:10.1016/j.annonc.2023.09.2734
32. Saad, F, Hussain, MHA, Tombal, BF, Fizazi, K, Sternberg, CN, Crawford, ED, et al. Association of prostate-specific antigen (PSA) response and overall survival (OS) in patients with metastatic hormone-sensitive prostate cancer (mHSPC) from the phase 3 ARASENS trial. J Clin Oncol (2022) 40(16_Suppl. l):5078. doi:10.1200/JCO.2022.40.16_suppl.5078
33. Saad, F, Tombal, B, Hussain, M, Fizazi, K, Sternberg, CN, Crawford, ED, et al. MP29-01 RAPID, DURABLE, AND DEEP PROSTATE-SPECIFIC ANTIGEN RESPONSE FOLLOWING ADDITION OF DAROLUTAMIDE TO ANDROGEN-DEPRIVATION THERAPY AND DOCETAXEL IN ARASENS. J Urol (2023) 209(Suppl. 4):e380. doi:10.1097/JU.0000000000003257.01
34. Shore, ND, Hussain, MHA, Saad, F, Fizazi, K, Sternberg, CN, Crawford, ED, et al. Abstract B131: efficacy and safety of darolutamide in combination with androgen-deprivation therapy (ADT) and docetaxel in Black/african-american patients from the phase 3 ARASENS trial. Cancer Epidemiol Biomarkers and Prev (2023) 32(Suppl. 1):B131. doi:10.1158/1538-7755.DISP22-B131
35. Shore, ND, Tombal, B, Hussain, M, Saad, F, Fizazi, K, Sternberg, CN, et al. MP29-02 EFFICACY AND SAFETY OF DAROLUTAMIDE IN COMBINATION WITH ANDROGEN-DEPRIVATION THERAPY AND DOCETAXEL IN THE NORTH AMERICAN POPULATION FROM ARASENS. J Urol (2023) 209(Suppl. 4):e380. doi:10.1097/JU.0000000000003257.02
36. Shore, ND, Tombal, BF, Hussain, MHA, Saad, F, Fizazi, K, Sternberg, CN, et al. Overall survival with darolutamide vs placebo in combination with androgen-deprivation therapy (ADT) and docetaxel: a sensitivity analysis from ARASENS accounting for subsequent therapy. J Clin Oncol (2024) 42(4_Suppl. l):166. doi:10.1200/jco.2024.42.4_suppl.166
37. Tombal, B, Saad, F, Fizazi, K, Sternberg, CN, Crawford, ED, Gratzke, C, et al. Efficacy and Safety of Darolutamide (DARO) in Combination with Androgen-Deprivation Therapy (ADT) and Docetaxel (DOC) in Patients (Pts) with Metastatic Hormone Sensitive Prostate Cancer (mHSPC) by Metastatic Burden: Subgroup Analyses of ARASENS [Congress Abstract]. Eur Urol (2023) 83(Suppl. 1):S1707–S8. doi:10.1016/S0302-2838(23)01221-6
38. Tombal, B, Smith, MR, Hussain, M, Saad, F, Fizazi, K, Sternberg, CN, et al. Tolerability and Pharmacokinetic Analyses of Combination Therapy with Darolutamide (DARO), Androgen-Deprivation Therapy (ADT), and Docetaxel (DOC) in Patients with Metastatic Hormone Sensitive Prostate Cancer (mHSPC) from ARASENS [Congress Abstract]. Eur Urol (2023) 83(Suppl. 1):S1709–S10. doi:10.1016/S0302-2838(23)01222-8
39. Wang, S, Fu, C, Li, Y, Xing, J, Zhou, L, Yang, Y, et al. 255O darolutamide (DARO) in combination with androgen-deprivation therapy (ADT) and docetaxel (DOC) in Chinese patients (pts) with metastatic hormone-sensitive prostate cancer (mHSPC) in the phase III ARASENS study. Ann Oncol (2023) 34(Suppl. 4):S1572. doi:10.1016/j.annonc.2023.10.381
40. Hussain, MHA, Tombal, BF, Saad, F, Fizazi, K, Sternberg, CN, Crawford, ED, et al. Efficacy and safety of darolutamide (DARO) in combination with androgen-deprivation therapy (ADT) and docetaxel (DOC) by disease volume and disease risk in the phase 3 ARASENS study. J Clin Oncol (2023) 41(6_Suppl. l):15. doi:10.1200/jco.2023.41.6_suppl.15
41. Davis, ID, Martin, AJ, Zielinski, RR, Thomson, A, Tan, TH, Sandhu, S, et al. Updated overall survival outcomes in ENZAMET (ANZUP 1304), an international, cooperative group trial of enzalutamide in metastatic hormone-sensitive prostate cancer (mHSPC). J Clin Oncol (2022) 40(17_Suppl. l):LBA5004. doi:10.1200/JCO.2022.40.17_suppl.LBA5004
42. Fizazi, K, Carles Galceran, J, Foulon, S, Roubaud, G, McDermott, R, Flechon, A, et al. LBA5 A phase III trial with a 2x2 factorial design in men with de novo metastatic castration-sensitive prostate cancer: overall survival with abiraterone acetate plus prednisone in PEACE-1. Ann Oncol (2021) 32(Suppl. 5):S1299. doi:10.1016/j.annonc.2021.08.2099
43. Horvath, LG, Davis, ID, Martin, A, Zielinski, R, Thomson, A, Tan, TH, et al. 1792P effects of enzalutamide on overall survival +/- early docetaxel in participants aged less than 70 yrs versus greater than or equal to 70 yrs in ENZAMET (ANZUP 1304). Ann Oncol (2023) 34(Suppl. 2):S968–S969. doi:10.1016/j.annonc.2023.09.2742
44. Mourey, L, Boyle, HJ, Roubaud, G, McDermott, RS, Supiot, S, Tombal, BF, et al. Efficacy and safety of abiraterone acetate plus prednisone and androgen deprivation therapy +/- docetaxel in older patients (≥70 years), with de novo metastatic-castration sensitive prostate cancer, compared to younger patients (<70 years): the PEACE-1 trial. J Clin Oncol (2023) 41(6_Suppl. l):20. doi:10.1200/jco.2023.41.6_suppl.20
45. Smith, MR, Hussain, MHA, Saad, F, Fizazi, K, Sternberg, CN, Crawford, ED, et al. Overall survival with darolutamide versus placebo in combination with androgen-deprivation therapy and docetaxel for metastatic hormone-sensitive prostate cancer in the phase 3 ARASENS trial. J Clin Oncol (2022) 40(6_Suppl. l):13. doi:10.1200/JCO.2022.40.6_suppl.013
46. Armstrong, AJ. Highlights in Advanced Prostate Cancer from the 2021 American Society of Clinical Oncology Annual Meeting. A Phase 3 Trial with a 2×2 Factorial Design of Abiraterone Acetate Plus Prednisone and/or Local Radiotherapy in Men with de novo Metastatic Castration-Sensitive Prostate Cancer: first Results of PEACE-1. Clin Adv Hematol Oncol (2021) 19(8 Suppl. 18):6–7.
47. Kafka, M, Giannini, G, Artamonova, N, Neuwirt, H, Ofner, H, Kramer, G, et al. Real-world evidence of triplet therapy in metastatic hormone-sensitive prostate cancer: an Austrian multicenter study. Clin Genitourinary Cancer (2024) 22(2):458–66.e1. doi:10.1016/j.clgc.2023.12.018
48. Ciccarese, C, Iacovelli, R, Sternberg, CN, Gillessen, S, Tortora, G, and Fizazi, K. Triplet therapy with androgen deprivation, docetaxel, and androgen receptor signalling inhibitors in metastatic castration-sensitive prostate cancer: a meta-analysis. Eur J Cancer (2022) 173:276–84. doi:10.1016/j.ejca.2022.07.011
49. Dou, M, Liang, H, Liu, Y, Zhang, Q, Li, R, Chen, S, et al. Based on ARASENS trial: efficacy and safety of darolutamide as an emerging option of endocrinotherapy for metastatic hormone-sensitive prostate Cancer—An updated systematic review and network meta-analysis. J Cancer Res Clin Oncol (2023) 149(10):7017–27. doi:10.1007/s00432-023-04658-6
50. Fiorica, F, Buttigliero, C, Grigolato, D, Muraro, M, Turco, F, Munoz, F, et al. Addition of new androgen receptor pathway inhibitors to docetaxel and androgen deprivation therapy in metastatic hormone-sensitive prostate cancer: a systematic review and metanalysis. Curr Oncol (2022) 29(12):9511–24. doi:10.3390/curroncol29120747
51. Hoeh, B, Garcia, CC, Wenzel, M, Tian, Z, Tilki, D, Steuber, T, et al. Triplet or doublet therapy in metastatic hormone-sensitive prostate cancer: updated network meta-analysis stratified by disease volume. Eur Urol Focus (2023) 9(5):838–42. doi:10.1016/j.euf.2023.03.024
52. Jian, T, Zhan, Y, Hu, K, He, L, Chen, S, Hu, R, et al. Systemic triplet therapy for metastatic hormone-sensitive prostate cancer: a systematic review and network meta-analysis. Front Pharmacol (2022) 13:955925. doi:10.3389/fphar.2022.955925
53. Lee, YS, Kim, SH, Tae, JH, Chang, IH, Kim, TH, Myung, SC, et al. Oral chemotherapeutic agents in metastatic hormone-sensitive prostate cancer: a network meta-analysis of randomized controlled trials. Prostate Int (2023) 11(3):159–66. doi:10.1016/j.prnil.2023.06.003
54. Menges, D, Yebyo, HG, Sivec-Muniz, S, Haile, SR, Barbier, MC, Tomonaga, Y, et al. Treatments for metastatic hormone-sensitive prostate cancer: systematic review, network meta-analysis, and benefit-harm assessment. Eur Urol Oncol (2022) 5(6):605–16. doi:10.1016/j.euo.2022.04.007
55. Riaz, IB, Naqvi, SAA, He, H, Asghar, N, Siddiqi, R, Liu, H, et al. First-line systemic treatment options for metastatic castration-sensitive prostate cancer: a living systematic review and network meta-analysis. JAMA Oncol (2023) 9(5):635–45. doi:10.1001/jamaoncol.2022.7762
56. Jian, T, Zhan, Y, Yu, Y, Yu, K, Hu, R, Wang, J, et al. Combination therapy for high-volume versus low-volume metastatic hormone-sensitive prostate cancer: a systematic review and network meta-analysis. Front Pharmacol (2023) 14:1148021. doi:10.3389/fphar.2023.1148021
57. Mandel, P, Hoeh, B, Wenzel, M, Preisser, F, Tian, Z, Tilki, D, et al. Triplet or doublet therapy in metastatic hormone-sensitive prostate cancer patients: a systematic review and network meta-analysis. Eur Urol Focus (2023) 9(1):96–105. doi:10.1016/j.euf.2022.08.007
58. Maiorano, BA, De Giorgi, U, Roviello, G, Messina, C, Altavilla, A, Cattrini, C, et al. Addition of androgen receptor-targeted agents to androgen-deprivation therapy and docetaxel in metastatic hormone-sensitive prostate cancer: a systematic review and meta-analysis. ESMO Open (2022) 7(5):100575. Epub 2022/09/22. doi:10.1016/j.esmoop.2022.100575
59. Roy, S, Sayyid, R, Saad, F, Sun, Y, Lajkosz, K, Ong, M, et al. Addition of docetaxel to androgen receptor axis-targeted therapy and androgen deprivation therapy in metastatic hormone-sensitive prostate cancer: a network meta-analysis. Eur Urol Oncol (2022) 5(5):494–502. doi:10.1016/j.euo.2022.06.003
60. Wang, L, Li, C, Zhao, Z, Li, X, Tang, C, Guan, Z, et al. Comparison of doublet and triplet therapies for metastatic hormone-sensitive prostate cancer: a systematic review and network meta-analysis. Front Oncol (2023) 13:1104242. doi:10.3389/fonc.2023.1104242
61. Wang, SS, Bian, XJ, Wu, JL, Wang, BH, Zhang, S, and Ye, DW. Network meta-analysis of combination strategies in metastatic hormone-sensitive prostate cancer. Asian J Androl (2024) 26(4):402–8. doi:10.4103/aja20242
62. Kyriakopoulos, CE, Chen, YH, Carducci, MA, Liu, G, Jarrard, DF, Hahn, NM, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: long-term survival analysis of the randomized phase III E3805 chaarted trial. J Clin Oncol (2018) 36(11):1080–7. doi:10.1200/JCO.2017.75.3657
63. Fizazi, K, Tran, N, Fein, L, Matsubara, N, Rodriguez-Antolin, A, Alekseev, BY, et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (latitude): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol (2019) 20(5):686–700. doi:10.1016/s1470-2045(19)30082-8
64. George, DJ, Halabi, S, Heath, EI, Sartor, AO, Sonpavde, GP, Das, D, et al. A prospective trial of abiraterone acetate plus prednisone in black and white men with metastatic castrate-resistant prostate cancer. Cancer (2021) 127(16):2954–65. doi:10.1002/cncr.33589
65. Alliance Foundation Trials, LLC. Androgen receptor directed therapy on cognitive function in patients treated with darolutamide or enzalutamide (ARACOG) (2021). Available online at: https://clinicaltrials.gov/study/NCT04335682 [Accessed July 1, 2024].
66. Francini, E, Gray, KP, Xie, W, Shaw, GK, Valença, L, Bernard, B, et al. Time of metastatic disease presentation and volume of disease are prognostic for metastatic hormone sensitive prostate cancer (mHSPC). The Prostate (2018) 78(12):889–95. doi:10.1002/pros.23645
67. Sutera, PA, Shetty, AC, Hakansson, A, Van der Eecken, K, Song, Y, Liu, Y, et al. Transcriptomic and clinical heterogeneity of metastatic disease timing within metastatic castration-sensitive prostate cancer. Ann Oncol (2023) 34(7):605–14. doi:10.1016/j.annonc.2023.04.515
68. Hoeh, B, Chun, FKH, and Mandel, P. Disease volume and risk subgroup analyses for darolutamide plus androgen-deprivation therapy and docetaxel in the phase III ARASENS: should triplet therapy become standard of care in certain metastatic hormone-sensitive prostate cancer patients? Chin Clin Oncol (2024) 13(1):14. doi:10.21037/cco-23-66
69. Kench, JG, Amin, MB, Berney, DM, Compérat, EM, Cree, IA, Gill, AJ, et al. WHO classification of tumours fifth edition: evolving issues in the classification, diagnosis, and prognostication of prostate cancer. Histopathology (2022) 81(4):447–58. doi:10.1111/his.14711
70. Pisano, C, Turco, F, Arnaudo, E, Fea, E, Vanella, P, Ruatta, F, et al. TEAM study: upfront docetaxel treatment in patients with metastatic hormone-sensitive prostate cancer: a real-world, multicenter, retrospective analysis. Clin Genitourinary Cancer (2024) 22(2):56–67.e16. doi:10.1016/j.clgc.2023.08.006
71. Barata, PC, Leith, A, Ribbands, A, Montgomery, R, Last, M, Arondekar, B, et al. Real-world treatment trends among patients with metastatic castration-sensitive prostate cancer: results from an international study. The Oncologist (2023) 28(9):780–9. doi:10.1093/oncolo/oyad045
72. Gillessen, S, Turco, F, Davis, ID, Efstathiou, JA, Fizazi, K, James, ND, et al. Management of patients with advanced prostate cancer. Report from the 2024 advanced prostate cancer consensus conference (APCCC). Eur Urol (2025) 87:157–216. doi:10.1016/j.eururo.2024.09.017
73. Mills, EJ, Thorlund, K, and Ioannidis, JP. Demystifying trial networks and network meta-analysis. BMJ (2013) 346:f2914. doi:10.1136/bmj.f2914
74. Cote, MP, Lubowitz, JH, Brand, JC, and Rossi, MJ. Understanding network meta-analysis (NMA) conclusions requires scrutiny of methods and results: introduction to NMA and the geometry of evidence. Arthrosc J Arthroscopic and Relat Surg (2021) 37(7):2013–6. doi:10.1016/j.arthro.2021.04.070
75. Song, F, Xiong, T, Parekh-Bhurke, S, Loke, YK, Sutton, AJ, Eastwood, AJ, et al. Inconsistency between direct and indirect comparisons of competing interventions: meta-epidemiological study. BMJ (2011) 343:d4909. doi:10.1136/bmj.d4909
Keywords: androgen deprivation therapy, androgen receptor-targeted therapy, docetaxel, hormone-sensitive prostate cancer, metastatic prostate cancer
Citation: Zapatero A, Alonso-Gordoa T, Rodríguez Antolín A, Couñago F, Sanmamed N, Domínguez Esteban M, López Valcárcel M, Manneh R, Borque-Fernando Á, Sala González N and Maroto P (2025) Triplet systemic therapy for hormone-sensitive prostate cancer: a critical review with a multidisciplinary approach. Oncol. Rev. 19:1599292. doi: 10.3389/or.2025.1599292
Received: 24 March 2025; Accepted: 10 July 2025;
Published: 25 July 2025.
Edited by:
Feifei Sun, Shandong University, ChinaReviewed by:
Xinpei Wang, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaTingting Feng, Shandong Academy of Medical Sciences (SDAMS), China
Copyright © 2025 Zapatero, Alonso-Gordoa, Rodríguez Antolín, Couñago, Sanmamed, Domínguez Esteban, López Valcárcel, Manneh, Borque-Fernando, Sala González and Maroto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pablo Maroto, am1hcm90b0Boc3Auc2FudHBhdS5lcw==